Paeds · nephrology-urology-fluids-and-electrolytes
Dehydration and oral or intravenous rehydration
Also known as Paediatric dehydration · Acute gastroenteritis dehydration · Oral rehydration therapy · Intravenous rehydration in children · Clinical dehydration scale
Fellowship guide to paediatric dehydration and rehydration: the clinical dehydration scale and the WHO and percentage-weight-loss severity bands, the assessment of volume status at the bedside, oral rehydration therapy with reduced-osmolarity oral rehydration solution as the first-line treatment for mild to moderate dehydration, the staged intravenous rehydration protocol with isotonic crystalloid and the slow correction of dysnatraemia, and the prevention of cerebral oedema that dominates the safe management of the severely dehydrated child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who has been vomiting and passing watery stools for two days, who is now listless with sunken eyes and a dry mouth, is the everyday face of dehydration and the most common paediatric fluid emergency. The defining problem is a net loss of body water and electrolytes that outruns intake, so the extracellular volume contracts and the circulating volume falls until the tissues are underperfused. Most episodes follow acute gastroenteritis, and most are mild, but the small proportion that progress to severe dehydration carry a real risk of shock, electrolyte crisis, and cerebral oedema. [11]
The degree of dehydration is expressed most usefully as a percentage of body weight lost, because a recent weight is the single most reliable measure of the water deficit. A loss below 5 percent of body weight is mild and usually clinically inapparent, a loss of 5 to 10 percent produces the recognisable signs of moderate dehydration, and a loss above 10 percent is severe and accompanied by shock and a threatened circulation. The clinical dehydration scale converts these weight bands into a reproducible bedside score, so the clinician can grade severity without waiting for a weight or a blood test. [4]
The treatment is simple in concept and exact in execution, which is the whole point of the topic for an examiner. Mild and moderate dehydration are managed with oral rehydration therapy using reduced-osmolarity oral rehydration solution, which works as well as intravenous fluid and avoids the cannula and the admission. Severe dehydration and shock need intravenous isotonic crystalloid in a staged protocol, and the dysnatraemic child needs that fluid given slowly, because the brain defends its volume and a rapid correction causes cerebral oedema. [7]
Classification
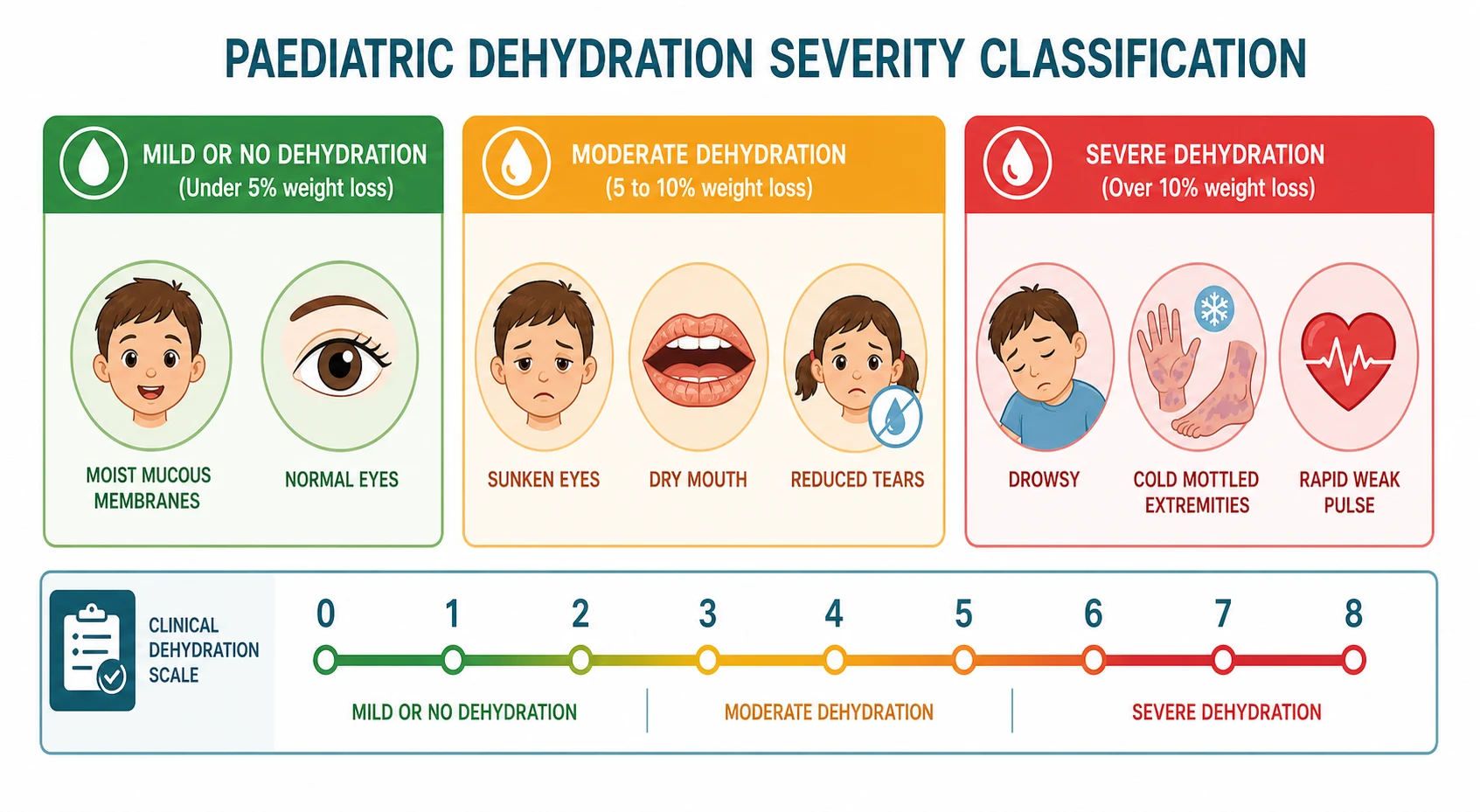
Severity is graded in three ways that each reinforce the others, and the exam rewards the candidate who can move between them. The percentage weight loss band is the reference standard and anchors the physiology, with mild below 5 percent, moderate 5 to 10 percent, and severe above 10 percent. The World Health Organization classification, built for resource-limited settings, groups children into no dehydration, some dehydration, and severe dehydration on a handful of bedside signs, and it drives the decision to use oral or intravenous fluid. The clinical dehydration scale, developed by Friedman and Goldman and validated by Parkin, adds a numerical score that is reproducible between observers and tracks the response to treatment. [5]
The clinical dehydration scale scores four findings, each from zero to two, for a total from zero to eight. General appearance is zero when the child is normal, one when thirsty or restless or lethargic but consolable, and two when drowsy or limp or poorly responsive. The eyes are scored as normal, slightly sunken, or very sunken, the mucous membranes as moist, sticky, or dry, and the tears as normal, reduced, or absent. A score of zero means no dehydration, one to four means some or moderate dehydration, and five to eight means moderate to severe dehydration. [4]
No or mild
- Weight loss below 5 percent
- Clinical dehydration scale zero
- Well, alert, moist mucous membranes
- Oral rehydration therapy at home
Moderate
- Weight loss 5 to 10 percent
- Clinical dehydration scale 1 to 4
- Sunken eyes, dry mouth, reduced tears, thirsty
- Oral rehydration therapy, consider ondansetron
Severe
- Weight loss above 10 percent
- Clinical dehydration scale 5 to 8
- Drowsy, cold peripheries, rapid weak pulse, deep acidotic breathing
- Intravenous isotonic crystalloid, watch the sodium
The severe band demands an immediate distinction between dehydration and shock, because the management diverges there. A child with severe dehydration is hypovolaemic, and the hypovolaemia becomes shock when the perfusion of vital organs fails, shown by altered consciousness, a prolonged capillary refill, and a weak rapid pulse. Shock is treated first with boluses and reassessed after each one, while uncomplicated moderate dehydration proceeds down the oral pathway, and the severity grade therefore selects the treatment arm at the point of the first assessment. [11]
Epidemiology & Risk Factors
Acute gastroenteritis is the engine of paediatric dehydration, and it remains one of the commonest reasons a child presents to an emergency department or is admitted to a ward. Viral causes predominate, with rotavirus historically the leading pathogen before vaccination and norovirus now prominent alongside adenovirus and sapovirus. Bacterial causes such as Campylobacter, Salmonella, and Shigella produce a smaller but important share, and the dysentery they cause carries its own management implications. The volume and the sodium content of the stool determine both the severity and the electrolyte picture, which is why profuse secretory diarrhoea dehydrates a small child so quickly. [11]
Infants and young children are the vulnerable group for a simple physiological reason. Their high body water fraction, their dependence on others for fluid intake, and their high surface area to weight ratio all magnify the effect of a given loss, so a toddler with gastroenteritis reaches 10 percent dehydration far faster than an adult with the same illness. Reduced intake from anorexia and vomiting compounds the loss, and the smaller the child the steeper the descent from moderate to severe dehydration. [3]
The risk of a poor outcome rises steeply in lower-resource settings and in specific populations. Worldwide, diarrhoeal disease remains a leading cause of child mortality where access to oral rehydration solution and clean water is limited, and the same children present later and more severely to health services. In Australia and Aotearoa New Zealand, Aboriginal and Torres Strait Islander children and children in remote communities carry a higher burden of severe gastroenteritis, and migrant and refugee families may face barriers to early oral rehydration. [9]
Pathophysiology
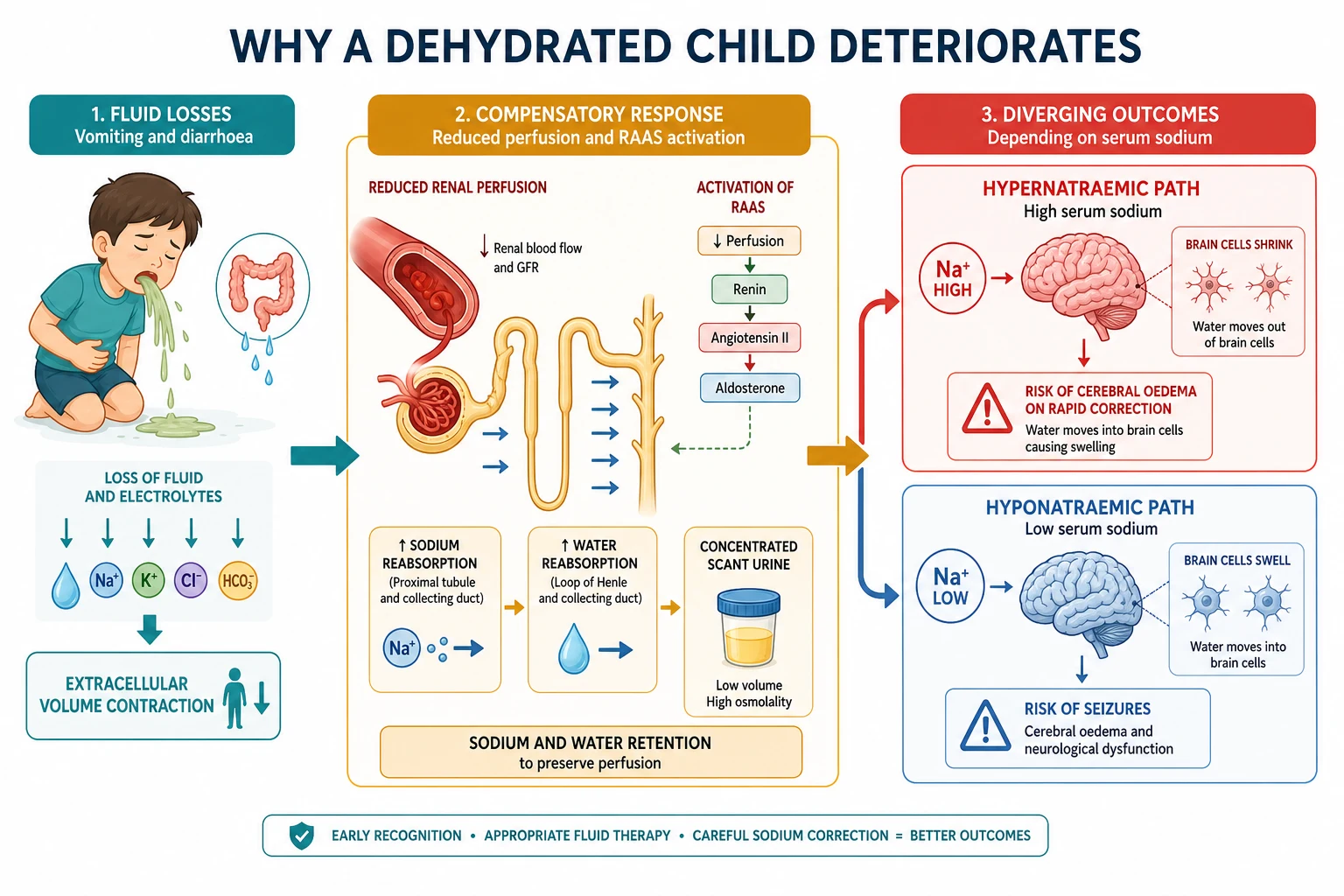
The mechanism unfolds along one pathway that the sodium level then splits into two. Fluid loss from vomiting and diarrhoea, or reduced intake, contracts the extracellular volume and lowers the effective circulating volume, so the perfusion of every tissue falls. The body defends the circulation by activating the renin to angiotensin to aldosterone system and by releasing antidiuretic hormone, which together retain sodium and water and produce the small volume of concentrated urine that is the hallmark of established dehydration. The same reflexes raise the heart rate and constrict the peripheral vessels, producing the tachycardia, the cool peripheries, and the prolonged capillary refill of the physical examination. [3]
The sodium level at presentation reflects the balance of salt and water loss, and it determines the danger of correction. When proportionally more water than sodium is lost, as in fever, poor intake, or some breastfeeding neonates, the serum sodium rises above 150 mmol per litre and the child becomes hypernatraemic, with shrunken brain cells that have generated idiogenic osmoles to defend their volume. When proportionally more sodium than water is lost, as in secretory diarrhoea or when a dehydrated child is given plain water, the serum sodium falls below 135 mmol per litre and the child becomes hyponatraemic, with brain-cell swelling that lowers the seizure threshold. [12]
The cerebral adaptation is the reason a rapid correction is dangerous and the reason the correction rate is the most testable number in the topic. In hypernatraemia the brain has defended its volume by taking on osmoles, so a sudden fall in serum sodium draws water into the brain and causes cerebral oedema, seizures, and death. In hyponatraemia the brain has shed water, so a sudden rise in serum sodium can cause osmotic demyelination. The safe correction rate, no faster than 0.5 mmol per litre per hour with a daily ceiling, applies to both, and the resuscitating fluid is isotonic rather than hypotonic so that the sodium is controlled rather than driven down. [10]
Clinical Presentation
The presentation spans the spectrum from a cheerful child with mild gastroenteritis and no clinical signs to a drowsy child in shock. The tempo is usually hours to a day or two of vomiting and watery diarrhoea, with a falling urine output and increasing thirst as the dehydration deepens. The history quantifies the intake, the stool and vomit frequency and volume, the urine output, and the presence of fever, and it seeks the red flags of an alternative diagnosis such as bilious vomiting, severe abdominal pain, or polyuria and polydipsia suggesting diabetes. [11]
The signs map onto the severity bands. A mildly dehydrated child looks well, with moist mucous membranes and normal eyes and tears. A moderately dehydrated child is thirsty and restless, with sunken eyes, a dry or sticky mouth, reduced tears, and a tachycardia. A severely dehydrated child is drowsy or floppy, with deeply sunken eyes, absent tears, cold mottled peripheries, a rapid thready pulse, a prolonged capillary refill, and deep acidotic breathing. The capillary refill, the mucous membranes, the eyes, and the tears are the four signs with the best discriminant value, and Gorelick and colleagues showed that three or more of these signs raises the probability of 5 percent or greater dehydration considerably. [3]
Recognising the deteriorating dehydrated child
Increasing thirst and reduced urine output with fewer wet nappies
Tachycardia, dry mouth, sunken eyes, and reduced tears
Prolonged capillary refill and cool peripheries signalling shock
Deep acidotic breathing and altered consciousness in severe dehydration
A serum sodium above 150 or below 135 defining a dysnatraemic crisis
Seizures from cerebral oedema or hyponatraemia as the feared complication
No single sign is reliable enough to stand alone, and Steiner and colleagues showed in their systematic review that the individual signs have only modest accuracy, so the diagnosis rests on a composite assessment rather than on any one finding. The clinician combines the history with several signs and, where possible, a recent weight, and uses the clinical dehydration scale to convert the composite into a number that guides the treatment. A normal urine output does not exclude early dehydration, and a child who is still passing some urine may still be moderately dehydrated. [2]
Differential Diagnosis
The first task is to confirm that the dehydration is from gastroenteritis and not from a mimicking illness, because the fluid plan is the same but the cause-directed treatment differs. Diabetic ketoacidosis presents with vomiting, dehydration, and deep breathing, but the history of polyuria and polydipsia, the high glucose, and the ketones distinguish it, and the fluid plan is gentler to avoid cerebral oedema. Sepsis produces tachycardia, poor perfusion, and shock, and the fever, the focus, and the inflammatory response separate it from simple dehydration. [11]
Within the loss of fluid, the differential considers where the water and electrolytes are going. Ongoing profuse diarrhoea may be infective, but it may also be lactose overload after a viral enteritis, a cow's milk protein enteropathy, or, rarely, a secretory tumour. Vomiting as the dominant feature raises surgical causes such as pyloric stenosis in the young infant with a hypochloraemic hypokalaemic metabolic alkalosis, intussusception with the redcurrant jelly stool, and malrotation with volvulus presenting with bilious vomiting. A reduced intake from stomatitis, pharyngitis, or a febrile illness explains dehydration in a younger child who refuses to drink. [11]
Gastroenteritis
- Vomiting and watery diarrhoea over hours to days
- Usually viral, supportive management
- Fluid loss drives the dehydration
- Oral rehydration therapy is first-line
Diabetic ketoacidosis
- Polyuria, polydipsia, weight loss, and vomiting
- High glucose and ketones, acidotic breathing
- Gentler rehydration to avoid cerebral oedema
- Insulin and glucose alongside the fluid
Sepsis
- Fever, tachycardia, poor perfusion, shock
- Identify and treat the source
- Broad antibiotics early
- Isotonic boluses for shock
Surgical
- Bilious vomiting in pyloric stenosis or volvulus
- Redcurrant jelly stool in intussusception
- Alkalosis or abdominal mass
- Surgical referral before fluids alone
The sodium level at presentation separates the dysnatraemic subtypes and is itself part of the differential, because it changes the fluid. Hypernatraemic dehydration, often from poor intake or a breastfed neonate, presents with a doughy skin feel and irritability rather than the expected flat affect, and the serum sodium above 150 mmol per litre marks the slow-correction pathway. Hyponatraemic dehydration, from salt loss or the dilution of plain water, presents with the more familiar picture of lethargy and may seize, and the serum sodium below 135 mmol per litre marks the cautious-correction pathway. [12]
Clinical & Bedside Assessment
The assessment runs in parallel with the start of treatment and answers three questions: how dehydrated is the child, is the child in shock, and what is the sodium doing. The airway, breathing, and circulation are assessed first, with a capillary refill, a pulse rate and character, a blood pressure, and a conscious level to detect shock at the bedside. A child in shock needs a fluid bolus before any further assessment, while a child without shock proceeds to the dehydration score and the oral pathway. [11]
A recent weight is the most useful single measure of the deficit, because the difference between a current and a pre-illness weight gives the percentage loss directly. Where no recent weight exists, the clinical dehydration scale and the percentage bands carry the assessment, and a weight measured now becomes the baseline against which the response to rehydration is tracked. The urine output, expressed as wet nappies or as millilitres per kilogram per hour in the catheterised child, is a sensitive marker of recovery, and a rising output confirms that the deficit is closing. [4]
The examination seeks the four high-yield signs and the signs of the complications. The eyes are inspected for sunkenness, the mouth for moisture, the peripheries for warmth and capillary refill, and the conscious level for irritability or drowsiness. The abdomen is examined for distension, tenderness, or a mass that would shift the diagnosis to a surgical cause, and the skin turgor is assessed, remembering that hypernatraemic dehydration can give a doughy rather than a tented feel. A deep sighing respiratory pattern points to acidosis from severe dehydration or to diabetic ketoacidosis. [3]
Investigations
Most children with mild dehydration need no investigation at all, and the over-investigation of a well child with simple gastroenteritis is itself a pitfall. The role of the tests is to confirm the severity, to detect the electrolyte disturbance, and to exclude the alternative diagnoses in the moderate and severe cases. A current weight, repeated at intervals, is the most important measurement and is treated as an investigation in its own right. [11]
The serum sodium is the single most important blood test, because it selects the speed of correction and the fluid. A sodium above 150 mmol per litre defines hypernatraemic dehydration and the slow-correction pathway, a sodium below 135 mmol per litre defines hyponatraemic dehydration and the cautious-correction pathway, and a normal sodium allows the standard protocol. Potassium is measured and monitored, and potassium is added to the intravenous fluid only once the serum sodium has normalised and the child has passed urine, because adding potassium to a hyperkalaemic or anuric child is dangerous. [10]
The urea, creatinine, and venous gas reveal the severity and the perfusion. A raised urea out of proportion to the creatinine reflects prerenal dehydration, a metabolic acidosis with a high anion gap reflects poor perfusion or diarrhoeal bicarbonate loss, and a rising lactate signals tissue hypoxia from shock. The glucose excludes hypoglycaemia from poor intake and the hyperglycaemia of diabetic ketoacidosis. The full blood count may show a haemoconcentration, and the urinalysis shows a high specific gravity and ketones in the fasting child, but neither changes the immediate management. [11]
Stool studies are sent selectively rather than routinely, for the child with bloody diarrhoea, a prolonged or severe course, immunocompromise, or a suspected outbreak. A renal ultrasound is reserved for the child in whom a post-renal or an intrinsic renal cause is suspected, and an abdominal film or ultrasound for the child with bilious vomiting or a mass. The principle is that the fluid resuscitation and the rehydration are never delayed for the tests, and the tests are interpreted in the light of the fluid plan rather than the reverse. [11]
Management — Resuscitation
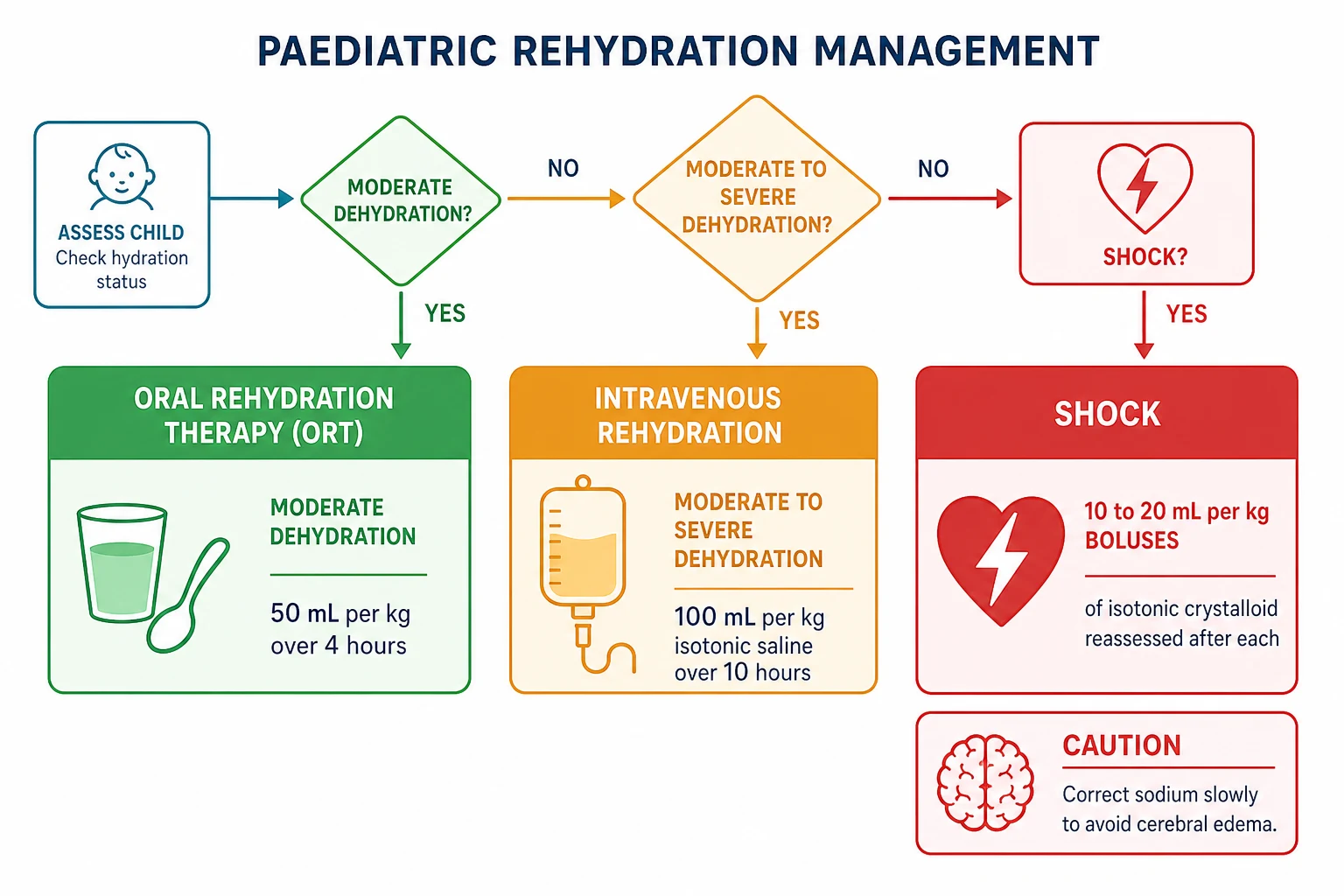
Resuscitation addresses the immediate threat of shock and runs in parallel with the assessment. The child in shock, defined by altered consciousness, a prolonged capillary refill, cold peripheries, and a weak rapid pulse, receives 10 to 20 mL per kg boluses of isotonic crystalloid, with reassessment after each bolus and repetition until the perfusion is restored. The fluid is 0.9 percent sodium chloride or a balanced crystalloid such as Hartmann solution, and the bolus is given over five to ten minutes rather than as a slow infusion, because the point is to restore the circulating volume promptly. [11]
Isotonic crystalloid bolus for shock in severe dehydration
Dose
10 to 20 mL per kg per bolus
The child who is dehydrated but not in shock does not receive a fluid bolus and instead proceeds to the oral or the intravenous rehydration pathway, because a bolus given to a non-shocked child adds no benefit and risks fluid overload. The single most common resuscitation error is to give repeated boluses to a child who is merely moderately dehydrated, mistaking the tachycardia of dehydration for shock, and the capillary refill, the pulse character, and the conscious level are the signs that separate the two. The bolus is reserved for the child whose perfusion has failed. [7]
Once shock is reversed, the resuscitation merges into rehydration, and the sodium level decides the rate. A child with a normal sodium continues on the standard intravenous protocol, while a child with hypernatraemic or hyponatraemic dehydration is managed on the slow-correction pathway with isotonic fluid and frequent sodium checks. Hypoglycaemia is sought and corrected with a bolus of 2 mL per kg of 10 percent glucose if present, and the blood glucose is monitored throughout, because the fasting dehydrated child is at risk. [10]
Management — Definitive & Stepwise
[11]Oral rehydration therapy is the first-line treatment for mild to moderate dehydration, and the Cochrane review by Hartling and colleagues confirmed that it is as effective as intravenous fluid in correcting the deficit while avoiding the cannula, the admission, and the complications. The principle is to replace the deficit and the ongoing losses with small, frequent volumes of reduced-osmolarity oral rehydration solution, given by spoon or syringe at 5 mL every one to two minutes, so that the absorption through the sodium-glucose cotransporter keeps pace with the losses even in the face of continuing diarrhoea. For moderate dehydration, 50 mL per kilogram is given over four hours, with ongoing losses added on top. [7]
The solution matters as much as the route. Reduced-osmolarity oral rehydration solution, with an osmolarity of about 245 mOsm per litre, a sodium of 75 mmol per litre, a glucose of 75 mmol per litre, and a potassium of 20 mmol per litre, was adopted worldwide after the rationale summarised by Duggan and colleagues showed that it reduces stool output and the need for intravenous fluid compared with the older standard solution. The lower osmolarity improves absorption without provoking the hypernatraemia that was feared with the original high-sodium solution, and it is the formulation recommended by the World Health Organization and NICE. [9]
Oral rehydration therapy for mild to moderate dehydration
Dose
50 mL per kg over 4 hours, plus ongoing losses
A single dose of oral ondansetron reduces vomiting and the need for intravenous rehydration in the child with gastroenteritis and mild to moderate dehydration, as Freedman and colleagues showed in their emergency department trial, and it is the standard adjunct that makes oral therapy feasible in the vomiting child. It is given once at the start of the oral attempt, and it is not repeated routinely. Diluted apple juice or the child's preferred fluid is an acceptable alternative to oral rehydration solution for the child with mild gastroenteritis and minimal dehydration, and the trial by Freedman and colleagues showed that it reduced treatment failure compared with an electrolyte maintenance solution in that group. [6]
The child who fails oral therapy, or who presents with moderate to severe dehydration, receives intravenous rehydration by the NICE staged protocol. Once any shock has been reversed, 100 mL per kilogram of 0.9 percent sodium chloride without potassium is given over 10 hours, the deficit is reassessed, and the child is moved onto maintenance fluid once the clinical signs have resolved. Potassium is added to the fluid only after the serum sodium has normalised and the child has passed urine, because adding potassium earlier risks hyperkalaemia. The maintenance volume follows the Holliday and Segar formula of 100 mL per kg for the first 10 kg, 50 mL per kg for the next 10 kg, and 20 mL per kg for each kilogram above 20 kg. [11]
Maintenance intravenous fluid for a dehydrated child
Dose
Holliday and Segar: 100/50/20 mL per kg per day
ORS for the four pillars of oral rehydration
Specific Subtypes & Scenarios
Hypernatraemic dehydration is the subtype that punishes a hurried correction, and it carries the highest risk of cerebral oedema. It arises when more water than sodium is lost, as in fever, poor intake, or a breastfed neonate with inadequate milk transfer, and the serum sodium is above 150 mmol per litre. The child is often irritable rather than flat, with a doughy skin feel, and the resuscitation uses isotonic crystalloid to lower the sodium slowly, at no faster than 0.5 mmol per litre per hour and with a daily ceiling of 8 to 12 mmol per litre, monitored with frequent sodium measurements. Free water and rapid correction are avoided because they draw water into the brain. [12]
Hyponatraemic dehydration presents with lethargy and may seize, and it arises when more sodium than water is lost or when a dehydrated child is given plain water. The serum sodium is below 135 mmol per litre, and the correction is likewise slow to avoid osmotic demyelination, with isotonic saline raising the sodium gently. A child with hyponatraemic seizures is the one exception to the slow rule, treated with 2 to 4 mL per kg boluses of 3 percent sodium chloride to raise the sodium by 3 to 5 mmol per litre and stop the seizures, after which the slow correction resumes. [10]
The breastfed neonate is a specific high-risk scenario for hypernatraemic dehydration, particularly in the first week of life when lactogenesis is still establishing. A weight loss above 10 percent, a high sodium, lethargy, poor feeding, and fever in a jaundiced neonate are the warning signs, and the management combines slow correction with lactation support, expressed milk, and formula supplementation as needed. The condition is preventable with early feeding assessment and weight monitoring, and Ozdogan and colleagues emphasised the importance of recognising it before the sodium is dangerously high. [12]
The child with diabetic ketoacidosis is rehydrated more gently than the child with simple gastroenteritis, because the risk of cerebral oedema during treatment is real and feared. The fluid is isotonic, the deficit is replaced over 24 to 48 hours rather than the 10 hours of the standard protocol, and insulin is started after the initial fluid rather than at the outset. The malnourished child is rehydrated cautiously with the specialised WHO rehydration solution for severe malnutrition, because the starved heart tolerates rapid fluid poorly and the electrolytes, especially phosphate and potassium, are already depleted. [11]
[11]Complications & Pitfalls
The complications divide into those of the untreated dehydration and those of its treatment. Untreated severe dehydration progresses to hypovolaemic shock, prerenal acute kidney injury, and death, and these are prevented by prompt rehydration. The complications of treatment are cerebral oedema from rapid sodium correction, hospital-acquired hyponatraemia from hypotonic fluid, and fluid overload from excessive boluses, and these are prevented by the disciplined use of isotonic fluid and a controlled correction rate. [10]
Cerebral oedema is the feared complication and it is iatrogenic, arising when the serum sodium is lowered too fast in hypernatraemic dehydration or when a hypotonic fluid is given to a child whose sodium is already low or normal. The child develops headache, vomiting, drowsiness, and seizures, and the condition can progress to coma and death, which is why the correction rate of 0.5 mmol per litre per hour is non-negotiable and why the resuscitating and maintenance fluid is isotonic. NICE advises an isotonic crystalloid with a sodium of 131 to 154 mmol per litre for maintenance and against the routine use of hypotonic fluids such as 0.45 percent sodium chloride or 5 percent glucose alone. [10]
The classic pitfalls are several. Treating a moderately dehydrated child with boluses rather than oral therapy overcorrects and overloads. Failing to check the sodium before starting intravenous fluid misses a hypernatraemic or hyponatraemic child who needs the slow pathway. Adding potassium before the sodium has normalised and urine has been passed risks hyperkalaemia. Using a hypotonic maintenance fluid causes hyponatraemia. Discharging a child before the oral intake is established risks readmission, and counselling the family on the warning signs is part of the treatment. [11]
Prognosis & Disposition
The prognosis of paediatric dehydration is excellent when it is recognised and treated promptly, and the great majority of children recover fully within a day or two of rehydration. Oral rehydration therapy succeeds in most children with mild to moderate dehydration, and the small proportion who need intravenous fluid recover as the deficit is closed. The mortality, where it occurs, is concentrated in the severely dehydrated child who presents late, the dysnatraemic child who is corrected too fast, and the child in a lower-resource setting without access to oral rehydration solution. [7]
Disposition follows the severity and the response. A child with mild dehydration and a reliable family is managed at home with oral rehydration solution and clear safety-netting advice, including the warning signs of drowsiness, persistent vomiting, reduced urine output, and bloody diarrhoea. A child with moderate dehydration who responds to oral therapy is observed until intake is established, and a child who fails oral therapy, who has severe dehydration, or who is dysnatraemic is admitted for intravenous rehydration and electrolyte monitoring. Intensive care is reserved for the child in refractory shock, with cerebral oedema, or with severe dysnatraemia. [11]
The discharge plan addresses the feeding, the fluids, and the prevention. Feeding, including breastfeeding, is restarted as soon as rehydration is underway, and the routine use of anti-motility agents is avoided. The family is taught how to mix and give oral rehydration solution, the warning signs that should bring the child back, and the general measures of hand hygiene and rotavirus vaccination that prevent the next episode. [11]
Special Populations
Neonates and young infants are the most vulnerable group, and they are managed with the greatest caution. Their high body water fraction and their dependence on a caregiver for intake mean that dehydration develops quickly and that the sodium can swing widely, and the breastfed neonate in the first week is the classic presentation of hypernatraemic dehydration. A weight loss above 7 to 10 percent, a poor feeding assessment, and a high sodium warrant admission, slow correction, and lactation support, and the threshold for investigation and intravenous fluid is lower than in the older child. [12]
The malnourished child is rehydrated cautiously and with a different solution. The starved heart tolerates rapid fluid poorly, the intracellular electrolytes are depleted, and refeeding is itself a risk, so the severely malnourished child receives the specialised rehydration solution for severe malnutrition at half the standard volume and is monitored for hypoglycaemia, hypothermia, and refeeding electrolyte shifts. The principles of oral first and isotonic fluid still apply, but the volumes are smaller and the monitoring is closer. [9]
Children in lower-resource settings bear the greatest burden of severe dehydration, and the management adapts to the resources available. The World Health Organization classification and the reduced-osmolarity solution were designed for this setting, and they remain among the most cost-effective interventions in medicine, with oral rehydration therapy and zinc together reducing diarrhoeal mortality substantially. The emphasis is on early oral therapy at home, clean water, sanitation, and rotavirus vaccination, and on the recognition of the severe dehydration that needs referral and intravenous fluid. [9]
Aboriginal and Torres Strait Islander children and children in remote communities carry a higher burden of severe gastroenteritis and dehydration, and the management uses a lower threshold for oral rehydration solution, ondansetron, and observation. Migrant and refugee families may face language and access barriers to early oral rehydration, and culturally appropriate education on the warning signs and the mixing of oral rehydration solution is part of the care. The retrieval services link the remote clinician to the tertiary centre, and the clinical dehydration scale gives both a shared language for severity. [11]
[9]Evidence, Guidelines & Regional Differences
The NICE guideline on diarrhoea and vomiting in children under five, summarised by Khanna and colleagues, is the standard reference for the assessment and the rehydration pathway in the United Kingdom and beyond, and it codifies the clinical dehydration scale, the oral-first principle, and the staged intravenous protocol. The NICE guidance on intravenous fluid therapy in children and young people, summarised by Neilson and colleagues, sets the maintenance standard of an isotonic crystalloid and the explicit warning against hypotonic fluids, and it carries the correction-rate rules that govern the dysnatraemic child. Together these two guidelines define the modern standard of care. [11]
The Cochrane review by Hartling and colleagues established that oral rehydration therapy is as effective as intravenous fluid for mild to moderate dehydration, with fewer admissions and fewer complications, and it is the evidence base for the oral-first principle. The rationale for the reduced-osmolarity solution, summarised by Duggan and colleagues, underpinned the worldwide switch to the 245 mOsm per litre solution, and the trials of ondansetron and of diluted apple juice by Freedman and colleagues refined the adjuncts that make oral therapy feasible. The systematic review by Steiner and colleagues and the validation study by Gorelick and colleagues defined the clinical signs and their limits. [7]
NICE gastroenteritis
- Oral rehydration first, staged intravenous protocol
- Clinical dehydration scale to grade severity
- 100 mL per kg isotonic over 10 hours after shock
NICE IV fluids
- Isotonic maintenance, avoid hypotonic
- Sodium 131 to 154 mmol per litre
- Correction no faster than 0.5 mmol per litre per hour
Cochrane ORT
- Oral as effective as intravenous for mild to moderate
- Fewer admissions and complications
- Foundation of the oral-first principle
Apple juice trial
- Diluted apple juice or preferred fluid for mild disease
- Reduced treatment failure versus maintenance solution
- Freedman and colleagues, JAMA 2016
The controversies are few but instructive. The speed of intravenous rehydration has been debated, with some units using a more rapid regimen for moderate dehydration, but the NICE standard of 100 mL per kg over 10 hours remains the default, and the dysnatraemic child is always corrected slowly. The choice between 0.9 percent sodium chloride and a balanced crystalloid is unsettled in dehydration as in other paediatric fluids, and either is acceptable for the initial resuscitation. The consistent message across the guidelines and the trials is that oral rehydration is first-line, that the fluid is isotonic, and that the sodium is corrected slowly. [10]
Exam Pearls
WET for the rehydration pathway
References
- [1]Holliday MA, Segar WE The maintenance need for water in parenteral fluid therapy. Pediatrics, 1957.PMID 13431307
- [2]Steiner MJ, DeWalt DA, Byerley JS Is this child dehydrated? JAMA, 2004.PMID 15187057
- [3]Gorelick MH, Shaw KN, Murphy KO Validity and reliability of clinical signs in the diagnosis of dehydration in children. Pediatrics, 1997.PMID 9113963
- [4]Friedman JN, Goldman RD, Srivastava R, Parkin PC Development of a clinical dehydration scale for use in children between 1 and 36 months of age. J Pediatr, 2004.PMID 15289767
- [5]Goldman RD, Friedman JN, Parkin PC Validation of the clinical dehydration scale for children with acute gastroenteritis. Pediatrics, 2008.PMID 18762524
- [6]Freedman SB, Willan AR, Boutis K, Schuh S Effect of Dilute Apple Juice and Preferred Fluids vs Electrolyte Maintenance Solution on Treatment Failure Among Children With Mild Gastroenteritis: A Randomized Clinical Trial. JAMA, 2016.PMID 27131100
- [7]Hartling L, Bellemare S, Wiebe N, Russell K, et al Oral versus intravenous rehydration for treating dehydration due to gastroenteritis in children. Cochrane Database Syst Rev, 2006.PMID 16856044
- [8]Freedman SB, Adler M, Seshadri R, Powell EC Oral ondansetron for gastroenteritis in a pediatric emergency department. N Engl J Med, 2006.PMID 16625009
- [9]Duggan C, Fontaine O, Pierce NF, Glass RI, et al Scientific rationale for a change in the composition of oral rehydration solution. JAMA, 2004.PMID 15173155
- [10]Neilson J, O'Neill F, Dawoud D, Crean P, et al Intravenous fluids in children and young people: summary of NICE guidance. BMJ, 2015.PMID 26662119
- [11]Khanna R, Lakhanpaul M, Burman-Roy S, Murphy MS, et al Diarrhoea and vomiting caused by gastroenteritis in children under 5 years: summary of NICE guidance. BMJ, 2009.PMID 19386673
- [12]Ozdogan T, Iscan M, Ellikcioglu C, Yildiz E Hypernatraemic dehydration in breast-fed neonates. Arch Dis Child, 2006.PMID 17119086