Paeds · nephrology-urology-fluids-and-electrolytes
Fluid maintenance and deficit replacement
Also known as Holliday-Segar · Maintenance fluids · Deficit replacement · 4-2-1 rule · Isotonic maintenance · Intravenous fluid therapy · Fluid prescription
Fellowship guide to prescribing fluids in children: the Holliday-Segar 100/50/20 mL/kg/day rule (the 4/2/1 hourly form) for maintenance water, the 2 to 3 mmol/kg/day sodium and 1 to 2 mmol/kg/day potassium requirement, the switch to isotonic maintenance fluids with dextrose and potassium to prevent hospital-acquired hyponatraemia and hyponatraemic encephalopathy, the percentage method for calculating a dehydration deficit with half replaced over 8 hours and half over 16 hours, and the slow correction of hypernatraemic dehydration at no faster than 0.5 mmol per litre per hour.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Fluid therapy is where physiology meets arithmetic, and both have to be right. A maintenance bag is not a generic drip. It is a calculated prescription of water, sodium, potassium and glucose, matched to a child's weight and to whatever the body is doing with ADH that day. The two classic errors are the opposite of each other: giving too little water, so the child slides into hypernatraemia, or giving too much free water, so the sodium falls and the brain swells. The Holliday-Segar rule solves the first problem, and the move to isotonic maintenance fluids solves the second. [1] [2]
This page treats prescription as a sequence of four questions. How much water does the child need each day? What tonicity should it be? How much deficit must be added back, and over how long? What ongoing losses must be matched? Answer all four and the fluid chart writes itself. The evidence base for the isotonic shift is now large and consistent, built on the Holliday and Segar observation, the McNab trial, the Cochrane and meta-analytic syntheses, and the American Academy of Pediatrics 2018 clinical practice guideline that made isotonic maintenance fluid the default for hospitalised children. [2] [3] [5]
Overview & Definition
Maintenance fluid is the daily intake of water and electrolytes needed to balance the obligatory losses a healthy child makes every day: urine, stool, sweat, and insensible loss from the skin and respiratory tract. Holliday and Segar derived it in 1957 from the metabolic observation that water need tracks energy expenditure, and their numbers have survived because they are simple and they work. [1]
The daily water requirement is 100 mL/kg for the first 10 kg of body weight, 50 mL/kg for the next 10 kg, and 20 mL/kg for every kilogram above 20. A 25 kg child therefore needs 1000 plus 500 plus 100, which is 1600 mL per day, or about 67 mL per hour. Expressed as the 4-2-1 hourly rule, the same child needs 4 mL/kg/hour for the first 10 kg, 2 mL/kg/hour for the next 10 kg, and 1 mL/kg/hour for each kilogram above 20 — giving 40 plus 20 plus 5, or 65 mL per hour. The two methods agree to within rounding. [1] [2]
Maintenance electrolytes ride along with the water. The daily sodium requirement is 2 to 3 mmol/kg/day, and the daily potassium requirement is 1 to 2 mmol/kg/day. Dissolved into the Holliday-Segar water volume, this lands the potassium at roughly 20 mmol per litre, which is why a standard maintenance bag adds 20 mmol/L of potassium chloride to its dextrose-saline base. [2]
Deficit is the fluid already lost before the child arrives, and it is separate from maintenance. It is estimated from the percentage dehydration: a clinically mild deficit is about 5 percent of body weight, a moderate deficit is 5 to 10 percent, and a severe deficit is at least 10 percent. Each 1 percent dehydration equals 10 mL/kg of lost fluid, so a 10 kg child at 10 percent dehydration has lost 1000 mL. [8]
Classification
A paediatric fluid prescription is built from four additive components, and classifying the child by which components apply is the first task. The figure lays the four components against the daily water tiers so the arithmetic is visible at a glance. [2] [10]
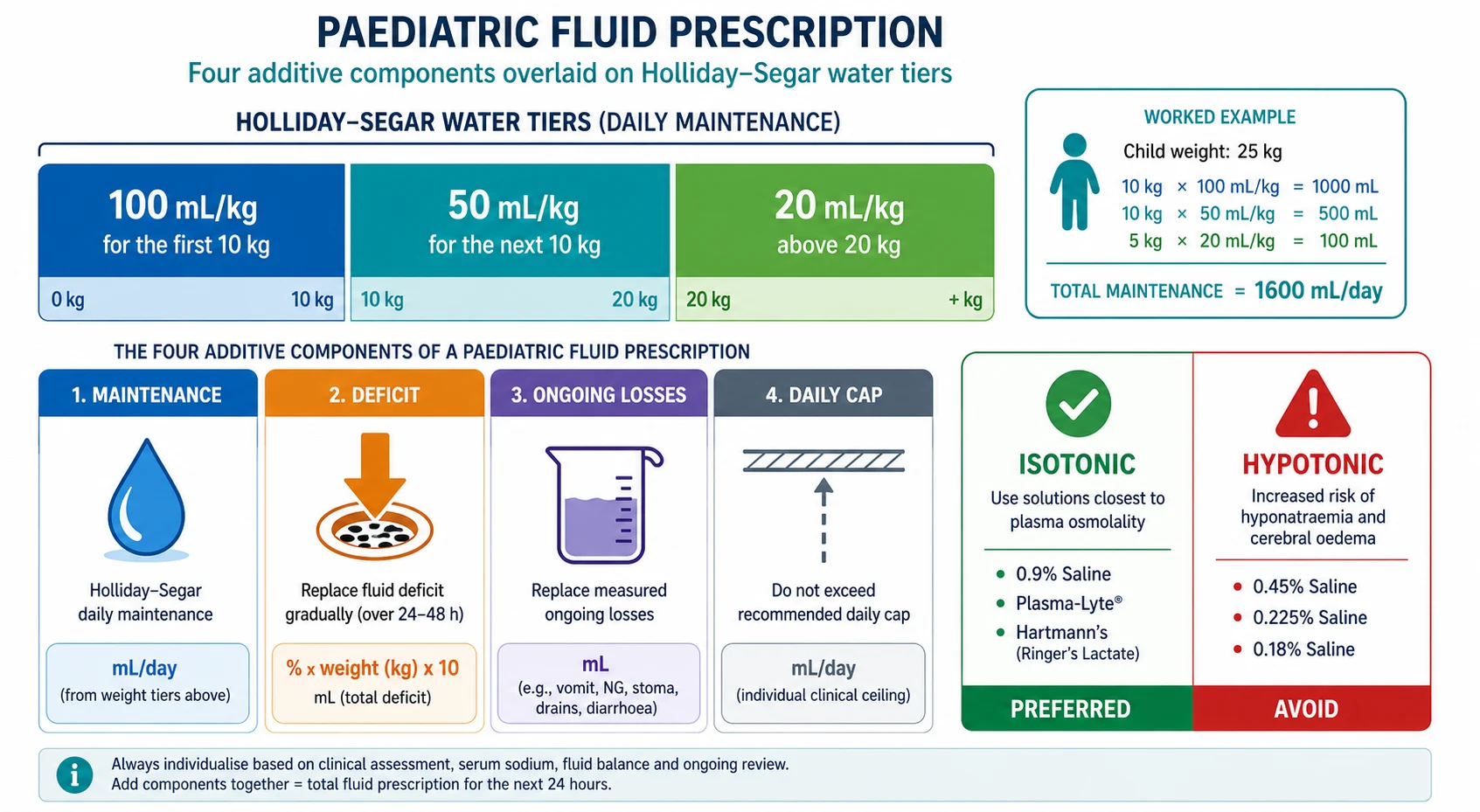
The four components are as follows. Maintenance is the Holliday-Segar daily water plus sodium and potassium, and it applies to every child who cannot meet their needs orally. Deficit is the percentage-based estimate of fluid already lost, added on top of maintenance. Ongoing losses are measured abnormal outputs — nasogastric aspirate, diarrhoea, drains, high stoma output — replaced volume for volume as they occur. The daily cap limits the weight-based maintenance rate for larger adolescents so they are not over-hydrated; beyond a sensible daily maximum the rate is held, not scaled further up by weight. [2] [10]
Fluid tonicity is the second axis of classification, and it is the one that carries the danger. Isotonic solutions have a sodium close to plasma: 0.9 percent saline at 154 mmol/L, or balanced crystalloids such as Plasma-Lyte, Hartmann's (Ringer's lactate) and Sterofundin, which sit around 130 to 140 mmol/L of sodium. Hypotonic solutions have a lower sodium: 0.45 percent saline at 77 mmol/L, 0.225 percent saline, 0.18 percent saline, and the old dextrose-saline mixtures. The modern default for maintenance is isotonic; hypotonic fluid is reserved for specific indications such as ongoing free-water deficit or sodium overload, and is avoided as routine maintenance. [2] [7]
Isotonic maintenance (preferred)
- 0.9% saline or balanced crystalloid (Plasma-Lyte, Hartmann's) with 5% dextrose
- Sodium 130 to 154 mmol/L — tonicity matches plasma
- Add 20 mmol/L potassium chloride once potassium and urine output confirmed
- Prevents hospital-acquired hyponatraemia in the sick child
Hypotonic fluids (avoid for routine maintenance)
- 0.45%, 0.225%, 0.18% saline, dextrose-water mixtures
- Sodium 30 to 77 mmol/L — excess free water when ADH is raised
- Causes hospital-acquired hyponatraemia and hyponatraemic encephalopathy
- Reserve for free-water deficit, sodium overload, or DKA protocols only
Epidemiology & Risk Factors
Almost every hospitalised child receives intravenous fluid at some point, so the population at risk is enormous. The children who come to harm from fluid are not a rare subset; they are ordinary ward and postoperative patients whose sodium drifts because a generic bag was hung and not reviewed. Quality-improvement work has shown that protocolised, isotonic prescribing reduces hyponatraemia across whole hospitals, which tells you the problem is systematic, not exotic. [9] [10]
The shared risk factor for hospital-acquired hyponatraemia is raised ADH. Anything that stresses a child turns on non-osmotic vasopressin: pain, nausea, anxiety, fever, respiratory illness, meningitis, the postoperative state, and almost every drug on the anaesthetic chart. The ADH tells the kidney to hold onto water, so the child excretes concentrated urine and retains free water. Hang a hypotonic bag in that state and the sodium falls predictably. [7] [11]
The perioperative child is the classic victim. Surgery raises ADH, NBM (nil by mouth) status removes dilute oral intake, and the legacy default of hypotonic maintenance combined to produce a generation of postoperative hyponatraemic seizures, some fatal. Roberts and colleagues, studying perioperative water balance in children having acute surgery, confirmed that the stress response shifts water handling toward retention and away from the free-water excretion a healthy child manages effortlessly. [11]
Children with pneumonia, bronchiolitis, meningitis and central nervous system infections are similarly vulnerable, because both the illness and the raised intracranial or intrathoracic pressure drive ADH. Smaller children and infants have less renal reserve to excrete a water load, and their brain fits a smaller cranial vault, so a given fall in sodium reaches symptomatic hyponatraemia faster than in an adult. [7] [9]
Pathophysiology
The body defends serum sodium through thirst, ADH, and the kidney's ability to dilute or concentrate the urine. In health, a child who drinks too much water simply excretes dilute urine: ADH switches off, the collecting duct becomes water-impermeable, and the spare water leaves within the hour. This diluting capacity is what makes a healthy child tolerant of a slightly generous fluid rate. [7]
The sick child has lost that safety margin. Non-osmotic ADH — released not because the blood is concentrated but because the body is stressed — keeps the collecting duct open to water, so the kidney cannot dilute the urine. Urine osmolality climbs, dilute urine stops, and every millilitre of free water given is retained. The figure shows how a hypotonic bag plus raised ADH converts to retained free water and a falling sodium. [7] [11]
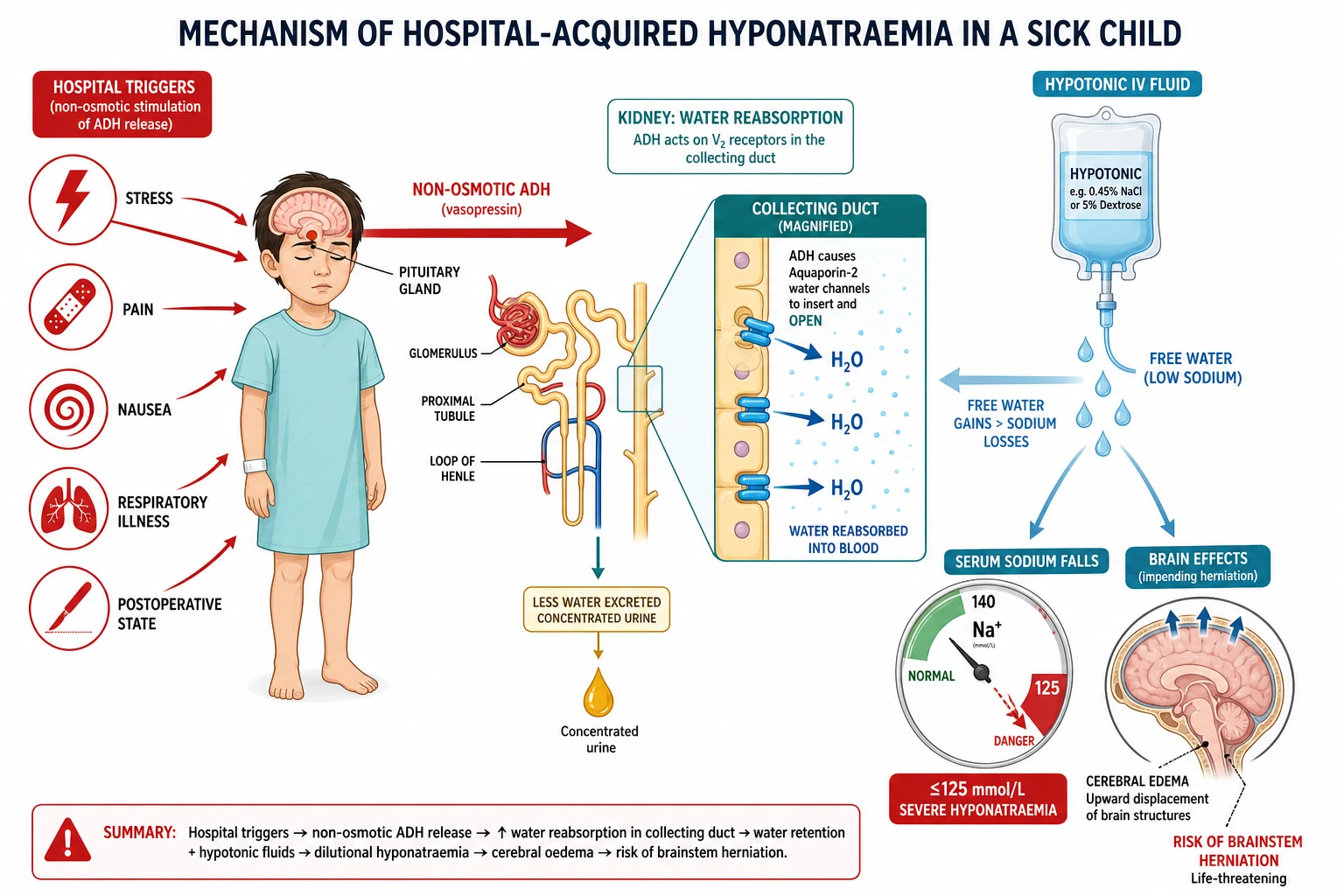
As sodium falls, water shifts by osmosis from the extracellular space into brain cells, and the brain swells within the rigid skull. Children are disproportionately vulnerable because their brain-to-cranial-vault ratio is higher, so they reach the symptomatic threshold earlier. The early signs are headache, nausea and vomiting, then lethargy and confusion, then seizures, and finally brainstem herniation, respiratory arrest and death. The whole cascade can unfold within hours of a misplaced hypotonic bag. [7]
The defence against this mechanism is tonicity. An isotonic fluid has the same effective osmolality as plasma, so even when ADH holds onto the water, no net free water moves into the brain. The sodium stays where it is. This single physical fact — tonicity, not the sodium number alone — is the entire justification for the isotonic-maintenance revolution. [2] [7]
Clinical Presentation
A child who needs fluid prescription is usually in hospital for something else — gastroenteritis, a surgical admission, pneumonia, or a complex chronic illness — and the fluid question is layered onto that presentation. The task is to estimate the dehydration deficit from the clinical picture, then write the maintenance that fits. [8]
Assess dehydration at the bedside using the percentage framework. A child with mild dehydration, around 5 percent, is thirsty, alert, has moist mucous membranes, normal perfusion, and may have slightly reduced urine output. A child with moderate dehydration, 5 to 10 percent, is restless or lethargic, has sunken eyes, a dry mouth, reduced skin turgor, tachycardia, and deep or rapid breathing. A child with severe dehydration, at least 10 percent, is drowsy or unconscious, has deeply sunken eyes and fontanelle, cold mottled skin, a weak rapid pulse, and little or no urine output, and is in or near shock. [8]
The history quantifies the deficit. Ask about the duration and frequency of vomiting and diarrhoea, the volume and frequency of urine, the last wet nappy, recent intake, fever, and any abnormal losses from drains or stomas. Weight is the most useful single measure: a recent weight compared with the child's usual weight gives the percentage loss directly, if a reliable pre-illness weight exists. [8]
The child with developing hyponatraemia from fluid looks different again. The early signal is a change in mental state — irritability, drowsiness, or nausea out of proportion to the primary illness — followed by headache and then vomiting. A child on intravenous fluid whose sodium is falling will often become sleepier before the blood result is back, which is why monitoring the sodium is mandatory, not optional. [7]
Differential Diagnosis
The differential here is not a list of diseases but a decision tree about which fluid to give and why. When a child needs a maintenance fluid, the first branch is whether they are genuinely euvolaemic with normal ADH, or whether they are sick enough to have raised ADH. In practice, almost every hospitalised child sits in the second group, which is why the default is isotonic. [2] [9]
The second branch concerns the sodium itself. A child whose sodium is normal and whose dehydration is isonatraemic gets the standard isotonic maintenance plus the deficit over 24 hours. A child with hypernatraemic dehydration — sodium above 145 mmol/L, usually from profuse watery diarrhoea in an infant — needs the deficit corrected slowly over 48 hours to avoid cerebral oedema. A child with hyponatraemic dehydration needs the deficit corrected more promptly and the sodium raised no faster than 8 mmol per litre per 24 hours. The sodium value at presentation decides the rate. [7] [8]
A few specific settings demand a different fluid altogether, and recognising them prevents error. Diabetic ketoacidosis has its own two-bag protocol and is beyond this leaf — but the principle is that DKA deliberately uses a measured sodium-containing fluid and adds potassium early, because total-body potassium is depleted. Burns use formula-based resuscitation, not Holliday-Segar. Cardiac and renal failure demand fluid restriction. Syndrome of inappropriate ADH demands fluid restriction, not more fluid. Each is a deviation from the default, and the default is isotonic maintenance. [2] [7]
ANZ hospital protocols (for example the Royal Children's Hospital Melbourne and the Sydney Children's Hospital guidelines) and the UK NICE guidance on intravenous fluid therapy for children and young people both now endorse isotonic maintenance fluids with dextrose and potassium. Local bag names and exact sodium concentrations vary — confirm the local preferred maintenance bag before prescribing, and document the guideline you are following. [2]
Clinical & Bedside Assessment
Start with weight, because every fluid calculation is per kilogram. Weigh the child unclothed or in a single layer, on calibrated scales, and record the weight on the fluid chart. If a recent pre-illness weight is available, the difference gives the percentage dehydration directly; if not, use the clinical signs to estimate mild, moderate or severe. [8]
Assess the volume status and the perfusion separately from the hydration. A child can be dehydrated but perfusing well, in which case the plan is deficit replacement over 24 hours. A child in shock — whatever the underlying hydration — gets isotonic boluses first. Feel the peripheries, measure the capillary refill, take the pulse and blood pressure, and look at the conscious level. These four signs decide whether the next move is a bolus or a bag. [8]
Record the urine output. A child passing urine at more than 1 mL/kg/hour is adequately perfused at the kidney, and potassium can be safely added to the maintenance fluid. A child who is oliguric or anuric is a different problem: hold the potassium, establish the cause, and reconsider the volume. Never write potassium into a bag for a child whose renal function and urine output you have not confirmed. [2]
Write the prescription as a structured order on the chart: the maintenance rate, the fluid type and tonicity, the dextrose and potassium content, the deficit volume and the time over which it will be replaced, the plan for ongoing losses, the daily weight, and the sodium and glucose monitoring schedule. A fluid chart that lists these elements defends the child against the slow drift that causes harm. [2] [10]
Investigations
The baseline bloods for any child on intravenous fluid are serum sodium, potassium, chloride, bicarbonate, urea and creatinine, and a venous or capillary glucose. These set the starting point against which every subsequent change is judged. If the sodium is already abnormal, the deficit-correction rate changes, and if the potassium is high or the child is oliguric, potassium stays out of the bag. [2]
Glucose matters because dextrose is part of every maintenance bag, and the child at risk of hypoglycaemia — the small infant, the starved surgical patient, the child with reduced intake — needs the dextrose confirmed rather than assumed. Check the glucose at baseline and again if the child becomes symptomatic, because hypoglycaemia is silent and harmful. [8]
WATER
Monitoring during maintenance therapy follows the clinical practice guideline. Check the serum sodium and chloride within 24 hours of starting intravenous fluid, then daily while the child remains on maintenance, and more often if the child is high-risk, postoperative, or has an abnormal baseline sodium. The point of monitoring is to catch the drift early, because the bag that was right yesterday can be wrong today once ADH shifts. [2] [10]
Urine output and urine specific gravity or osmolality help when the sodium is moving. A concentrated, high-osmolality urine in a child whose sodium is falling confirms inappropriate ADH activity and water retention, and signals that the free-water load, not the sodium loss, is the problem. The answer there is fluid restriction or isotonic fluid, never more hypotonic water. [7]
Management — Resuscitation
A child in hypovolaemic shock is resuscitated with isotonic fluid boluses of 20 mL/kg given rapidly, repeated as needed up to 60 mL/kg, until perfusion is restored. The fluid for the bolus is 0.9 percent saline or a balanced crystalloid such as Hartmann's — never hypotonic, never dextrose-containing for the bolus itself, because the goal is to expand the intravascular volume with an effective osmole. [8]
Boluses are not deficit replacement. They are a circulation rescue, given to the shocked child to restore perfusion, and the volume given in boluses is subtracted from the calculated deficit later. A child who needs three 20 mL/kg boluses to come out of shock has received 60 mL/kg of fluid already, and the remaining deficit is what is left after that. Only when the child is perfused and no longer needs boluses do you write the maintenance-plus-deficit prescription. [8]
Isotonic fluid bolus (hypovolaemic shock)
Dose
20 mL/kg
Management — Definitive & Stepwise
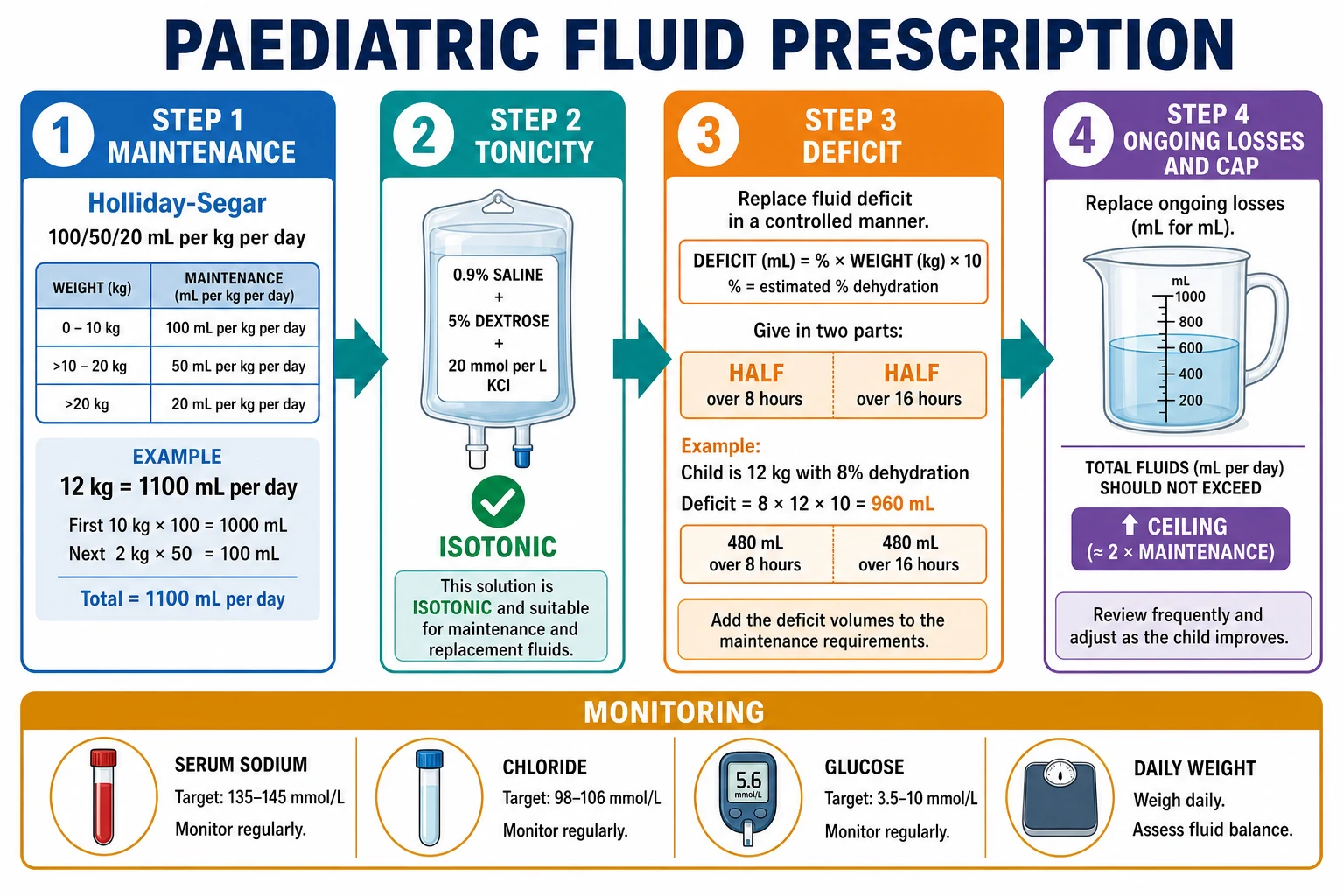
The definitive prescription answers four questions in order, and writing them out makes the arithmetic explicit. The figure walks through the four steps from the daily maintenance to the final bag. [2] [10]
Step one: maintenance. Calculate the daily water requirement by Holliday-Segar, then divide by 24 for the hourly rate. Add the sodium and potassium requirement by choosing a fluid that carries them. For a 12 kg infant the daily water is 1000 plus 100, or 1100 mL per day, which is about 46 mL per hour. [1] [2]
Step two: tonicity. Choose an isotonic maintenance fluid — 0.9 percent saline with 5 percent dextrose, or a balanced isotonic crystalloid with dextrose — and add 20 mmol/L of potassium chloride once you have confirmed the serum potassium is normal and the child is passing urine. This is the modern default for any child aged one month or older needing maintenance intravenous fluid, in the ward, the emergency department and the perioperative setting. [2] [5]
Step three: deficit. Calculate the deficit as the percentage dehydration times the weight in kilograms times ten. For a 10 kg child at 10 percent dehydration the deficit is 1000 mL. Replace half the deficit over the first 8 hours and the remaining half over the next 16 hours, added on top of the maintenance, and subtract any bolus volumes already given for shock. For hypernatraemic dehydration, extend the replacement to 48 hours and keep the sodium fall to no faster than 0.5 mmol per litre per hour, and no more than 10 to 12 mmol per litre in 24 hours. [7] [8]
Writing the fluid prescription
Maintenance: Holliday-Segar 100/50/20 mL/kg/day (or 4/2/1 per hour), plus sodium 2 to 3 mmol/kg/day and potassium 1 to 2 mmol/kg/day
Tonicity: isotonic — 0.9% saline or balanced crystalloid with 5% dextrose and 20 mmol/L potassium chloride once potassium and urine output confirmed
Deficit: percent dehydration times weight times ten; half over 8 hours, half over 16 hours, on top of maintenance; subtract any boluses
Hypernatraemic: correct over 48 hours, sodium fall no faster than 0.5 mmol per litre per hour and no more than 10 to 12 mmol per litre per day
Ongoing losses: replace measured abnormal output volume for volume; apply the daily weight cap for larger adolescents
Step four: ongoing losses and the cap. Replace ongoing abnormal losses — nasogastric aspirate, diarrhoea, drain output — volume for volume with an appropriate electrolyte composition, and reassess the prescription daily. For larger adolescents, cap the weight-based maintenance at a sensible daily maximum so the rate is not scaled up indefinitely by weight, which prevents over-hydration and sodium dilution. Re-weigh the child every morning and adjust the rate to the trend. [2] [10]
Specific Subtypes & Scenarios
The postoperative child is the scenario where hypotonic fluid historically killed. The surgical stress response raises ADH, the child is nil by mouth, and the legacy bag was often hypotonic. The prescription now is isotonic maintenance with dextrose and potassium, begun once intraoperative losses are accounted for, with the sodium checked within 24 hours. Roberts and colleagues confirmed that perioperative water homeostasis in children shifts toward retention, making isotonic fluid the correct default. [11] [2]
Hypernatraemic dehydration — sodium above 145 mmol/L, classically from profuse watery diarrhoea in a young infant — is the scenario where rapid correction kills. The brain has adapted to the hypernatraemia by accumulating idiogenic osmoles, so a fast fall in sodium pulls water into brain cells and causes cerebral oedema, seizures and death. Correct slowly, over 48 hours, keeping the sodium fall to no faster than 0.5 mmol per litre per hour and no more than 10 to 12 mmol per litre in 24 hours, and check the sodium every 4 to 6 hours while correcting. [7] [8]
The child with gastroenteritis and moderate dehydration is the everyday case for deficit replacement. Estimate the deficit as 5 to 10 percent, calculate the volume, and replace half over the first 8 hours and half over the next 16 hours on top of maintenance, preferring oral or nasogastric rehydration where the child can tolerate it and intravenous isotonic fluid where they cannot. Moritz and Ayus made the case that intravenous fluid therapy in gastroenteritis should default to isotonic saline to avoid the sodium falling in the child whose ADH is already raised. [8]
The child who is nil by mouth for a procedure needs straight isotonic maintenance, no deficit, with attention to glucose and potassium. A starved child is at risk of hypoglycaemia, so the dextrose in the bag is not ornamental; check the glucose if the fast is prolonged. [2]
Diabetic ketoacidosis is owned by its own leaf, but the fluid principle here applies: DKA uses a measured sodium-containing isotonic fluid, adds potassium early because total-body potassium is depleted, and corrects the deficit over 24 to 48 hours. Never use hypotonic fluid as DKA maintenance. [2]
Complications & Pitfalls
The cardinal pitfall is hanging a hypotonic bag as routine maintenance. In the sick child whose ADH is raised, that bag becomes retained free water and the sodium falls, sometimes into the range of hyponatraemic encephalopathy within hours. The defence is simple and absolute: prescribe isotonic maintenance fluid with dextrose and potassium for any child one month or older, and reserve hypotonic fluid for the specific indications that need it. [2] [7]
The mirror pitfall is adding potassium before confirming renal function and urine output. Potassium in a bag for a child who is oliguric, anuric, or already hyperkalaemic is a cardiac arrest waiting to happen. Confirm the serum potassium is normal and the child is passing urine before the potassium goes into the bag, and hold it if either is in doubt. [2]
The third pitfall is correcting hypernatraemia too fast. The brain has adapted to the high sodium, and a rapid fall causes cerebral oedema, seizures and death. Keep the sodium fall to no faster than 0.5 mmol per litre per hour and no more than 10 to 12 mmol per litre per 24 hours, and check the sodium frequently while correcting. The same discipline applies, in reverse, to chronic hyponatraemia, where over-rapid correction risks osmotic demyelination. [7]
The fourth pitfall is treating maintenance as a static prescription. ADH shifts, ongoing losses accumulate, and a bag that was correct in the morning can be wrong by the evening. Re-weigh the child daily, check the sodium and chloride at least daily, and rewrite the prescription to the trend. A fluid chart that is never reviewed is the one that harms. [10] [2]
Prognosis & Disposition
Prognosis in fluid therapy is overwhelmingly about avoiding iatrogenic harm. A child whose sodium stays within the normal range, whose potassium is added only when safe, and whose weight is tracked daily will do well, because the fluid is supporting the primary illness rather than adding to it. The children who come to grief are those whose prescription was written once and never reviewed, whose bag was hypotonic by habit, or whose hypernatraemia was corrected too fast. [7] [2]
Admit or escalate to a higher-acuity setting any child who needed boluses for shock, any child whose sodium is abnormal at baseline, any infant with hypernatraemic dehydration being corrected over 48 hours, and any child whose sodium is falling despite isotonic fluid. These children need frequent sodium and glucose checks and close observation of their neurological state. [7]
The stable child on isotonic maintenance stays on the ward with daily weight and daily electrolytes, and is stepped down to oral or enteral fluid as soon as tolerated. On discharge, the family is given a clear plan for oral rehydration if illness recurs, the indication for return is explained, and any underlying cause — gastroenteritis, a surgical recovery, a chronic condition — has its own follow-up arranged. [8]
Special Populations
Neonates are a separate prescribing world. The Holliday-Segar rule is used with caution in the first days of life, where water and sodium needs are lower and change daily, and where glucose stability is fragile. Neonatal fluid prescription is weight- and day-of-life-based, with glucose checked frequently and sodium added carefully. This leaf applies most cleanly to infants and children beyond the neonatal period. [2]
Children with complex chronic conditions, including cardiac, renal and neurological disease, need the maintenance prescription tailored to their physiology. Cardiac failure demands fluid restriction; renal failure demands potassium restriction and careful volume management; raised intracranial pressure interacts dangerously with hyponatraemia, making isotonic fluid essential. These children are over-represented among fluid-related adverse events, which is why their charts are reviewed daily and often. [2] [10]
Larger adolescents need the weight-based maintenance capped at a sensible daily maximum, because scaling 20 mL/kg indefinitely up the weight range over-hydrates a teenager. The prescription is still isotonic with dextrose and potassium, but the rate is held at the cap rather than rising with weight. [2] [10]
Children in rural and remote settings, and those undergoing retrieval, depend on a correctly written fluid chart that travels with them. The prescription written at the referring hospital must be isotonic, the sodium recorded, and the plan for deficit replacement explicit, so that the receiving team inherits a chart that is safe to continue. [2]
Evidence, Guidelines & Regional Differences
The evidence for the isotonic shift is now mature. Holliday and Segar's 1957 paper established the maintenance water requirement from energy expenditure, and the numbers have stood for seventy years. The transformation came later, when the harm from hospital-acquired hyponatraemia became clear and the randomised trials followed. [1] [9]
McNab summarised the landmark randomised evidence in JAMA, showing that isotonic maintenance fluid substantially reduces hyponatraemia compared with hypotonic fluid in hospitalised children. The Cochrane review by McNab and colleagues reached the same conclusion on pooled data, and two meta-analyses — by Wang and colleagues, and by Amer and colleagues in 2024 — confirmed that isotonic maintenance fluid reduces hyponatraemia without a compensatory rise in hypernatraemia or fluid overload. [3] [4] [6] [5]
Moritz and Ayus built the mechanistic and clinical case for why hypotonic fluids are unsafe in the acutely ill child, describing non-osmotic ADH and the pathogenesis of hyponatraemic encephalopathy, and applying the argument to the everyday setting of gastroenteritis. Karageorgos and colleagues reviewed the hospital-acquired hyponatraemia that follows hypotonic versus isotonic infusion in children, reinforcing the move away from hypotonic maintenance. [7] [8] [9]
The American Academy of Pediatrics 2018 clinical practice guideline on maintenance intravenous fluids in children (PMID 30478247) is the international reference standard: it recommends isotonic solutions with appropriate potassium chloride and dextrose for maintenance fluid in children aged one month and older, weight-based dosing, and monitoring of sodium and chloride. The UK NICE guideline on intravenous fluid therapy for children, the Royal Children's Hospital Melbourne and Sydney Children's Hospital protocols, and the Canadian and European paediatric society statements are broadly concordant, though local bag names and exact sodium concentrations vary. Confirm the local protocol before prescribing. [2]
The evidence is weakest in two places: the exact preferred isotonic solution (0.9 percent saline versus balanced crystalloid, which differ in their chloride load and risk of acidosis), and the daily maintenance volume cap for larger adolescents. Quality-improvement programmes, as reviewed by Sensing and colleagues, show that protocolised isotonic prescribing consistently reduces hyponatraemia across hospitals, which is the practical lesson. [2] [10]
Exam Pearls
Memorise the Holliday-Segar numbers cold, because the examiner will hand you a weight and expect the rate. 100 mL/kg for the first 10 kg, 50 mL/kg for the next 10, and 20 mL/kg above 20, giving the daily volume; divide by 24 for the hourly rate, or use the 4-2-1 rule (4 mL/kg/hour, 2 mL/kg/hour, 1 mL/kg/hour) which lands within rounding. Pair it with sodium 2 to 3 mmol/kg/day and potassium 1 to 2 mmol/kg/day. [1] [2]
The isotonic-first rule is examiner gold. Know that the modern maintenance fluid is isotonic — 0.9 percent saline or a balanced crystalloid with 5 percent dextrose and 20 mmol/L potassium chloride — and know why: non-osmotic ADH in the sick child makes hypotonic fluid dangerous by retaining free water and dropping the sodium. If asked why the bag changed, the answer is hospital-acquired hyponatraemia and hyponatraemic encephalopathy. [2] [7]
The deficit calculation is the arithmetic the examiner tests. Percentage dehydration times weight in kilograms times ten equals the deficit in millilitres; replace half over the first 8 hours and half over the next 16 hours, on top of maintenance, and subtract any bolus volumes given for shock. For hypernatraemic dehydration, correct over 48 hours with the sodium fall held to no faster than 0.5 mmol per litre per hour and no more than 10 to 12 mmol per litre per 24 hours. [8] [7]
Finally, the monitoring rule that closes the loop: check the sodium and chloride within 24 hours of starting intravenous fluid, then daily, and re-weigh the child every morning. The single most reliable marker of fluid balance on the ward is the daily weight, and the single most reliable cause of harm is the prescription that was never reviewed. [2] [10]
References
- [1]Holliday MA; Segar WE The maintenance need for water in parenteral fluid therapy. Pediatrics, 1957.PMID 13431307
- [2]Feld LG; Neuspiel DR; Foster BA; et al Clinical Practice Guideline: Maintenance Intravenous Fluids in Children. Pediatrics, 2018.PMID 30478247
- [3]McNab S Isotonic vs Hypotonic Intravenous Fluids for Hospitalized Children. JAMA, 2015.PMID 26284724
- [4]McNab S; Ware RS; Neville KA; et al Isotonic versus hypotonic solutions for maintenance intravenous fluid administration in children. Cochrane Database Syst Rev, 2014.PMID 25519949
- [5]Amer BE; Abdelwahab OA; Abdelaziz A; et al Efficacy and safety of isotonic versus hypotonic intravenous maintenance fluids in hospitalized children: an updated systematic review and meta-analysis of randomized controlled trials. Pediatr Nephrol, 2024.PMID 37365423
- [6]Wang J; Xu E; Xiao Y Isotonic versus hypotonic maintenance IV fluids in hospitalized children: a meta-analysis. Pediatrics, 2014.PMID 24379232
- [7]Moritz ML; Ayus JC New aspects in the pathogenesis, prevention, and treatment of hyponatremic encephalopathy in children. Pediatr Nephrol, 2010.PMID 19894066
- [8]Moritz ML; Ayus JC Improving intravenous fluid therapy in children with gastroenteritis. Pediatr Nephrol, 2010.PMID 20309584
- [9]Karageorgos SA; Kratimenos P; Landicho A; et al Hospital-Acquired Hyponatremia in Children Following Hypotonic versus Isotonic Intravenous Fluids Infusion. Children (Basel), 2018.PMID 30279348
- [10]Sensing W; Wenker M; Whitney E Maintenance fluid management in pediatrics: Current practice and quality improvement achievements. Curr Probl Pediatr Adolesc Health Care, 2021.PMID 34092514
- [11]Roberts DN; Vallen P; Cronhjort M; et al Perioperative water and electrolyte balance and water homeostasis regulation in children with acute surgery. Pediatr Res, 2023.PMID 36759747