Paeds · nephrology-urology-fluids-and-electrolytes
Haematuria: diagnostic approach
Also known as Blood in the urine · Red urine · Cola-coloured urine · Microscopic haematuria · Macroscopic haematuria · Glomerular haematuria · IgA nephropathy · Post-streptococcal glomerulonephritis · IgA vasculitis nephritis · Alport syndrome · Hypercalciuria
Fellowship guide to the diagnostic approach to haematuria in children, built around the glomerular versus non-glomerular fork. The page works from confirming that red or brown urine really is blood, through the colour clue and red-cell morphology, to an age-anchored differential that runs from renal vein thrombosis in the neonate through post-streptococcal glomerulonephritis, IgA nephropathy, IgA vasculitis nephritis and haemolytic uraemic syndrome in the child to lupus nephritis and Alport syndrome in the adolescent, and on to complement patterns, the indications for renal biopsy and the red flags of hypertension, oedema and an abdominal mass.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old whose mother spots cola-coloured urine in the toilet, and a teenager who passes bright red urine after a long football session. Both have blood in the urine, yet the colour, the timing and the company the blood keeps point to completely different problems and demand different first moves. Haematuria is the presence of red blood cells in the urine, and in children its meaning is set by three things working together: whether the blood is visible, what colour it is, and whether the urine also carries protein, casts and the signs of kidney inflammation. [1] [2]
The first practical fork is not visible against invisible but visible against microscopic is only half the story. Microscopic haematuria means blood found on dipstick and confirmed as more than five red cells per high-power field on a centrifuged specimen, and it is usually picked up on a routine check. Macroscopic, or visible, haematuria means blood the family can see, and the colour they describe is immediately diagnostic of the broad source. [1]
The single trap at the door is the dipstick that lies. A urine dipstick detects haem, not intact red cells, so it turns positive for blood in the presence of free haemoglobin or myoglobin as well as whole red cells. A positive dipstick with no red cells on microscopy is therefore not haematuria at all; it points to myoglobinuria from rhabdomyolysis or haemoglobinuria from haemolysis, both of which can be rapidly dangerous. Confirming that red cells are really there, then reading their colour and their shape, is the discipline that turns an alarming symptom into a tractable problem. [1]
Classification
Classify every case on two axes at once: the source of the bleeding and the age of the child. The source decides whether you expect brown cola urine with casts and proteinuria in the glomerular column, or bright red urine with clots in the non-glomerular column, while the age decides which causes are statistically likely within that source. The classification figure sets these axes out as a grid, with the typical cause for each age and source in the cells. [2] [3]
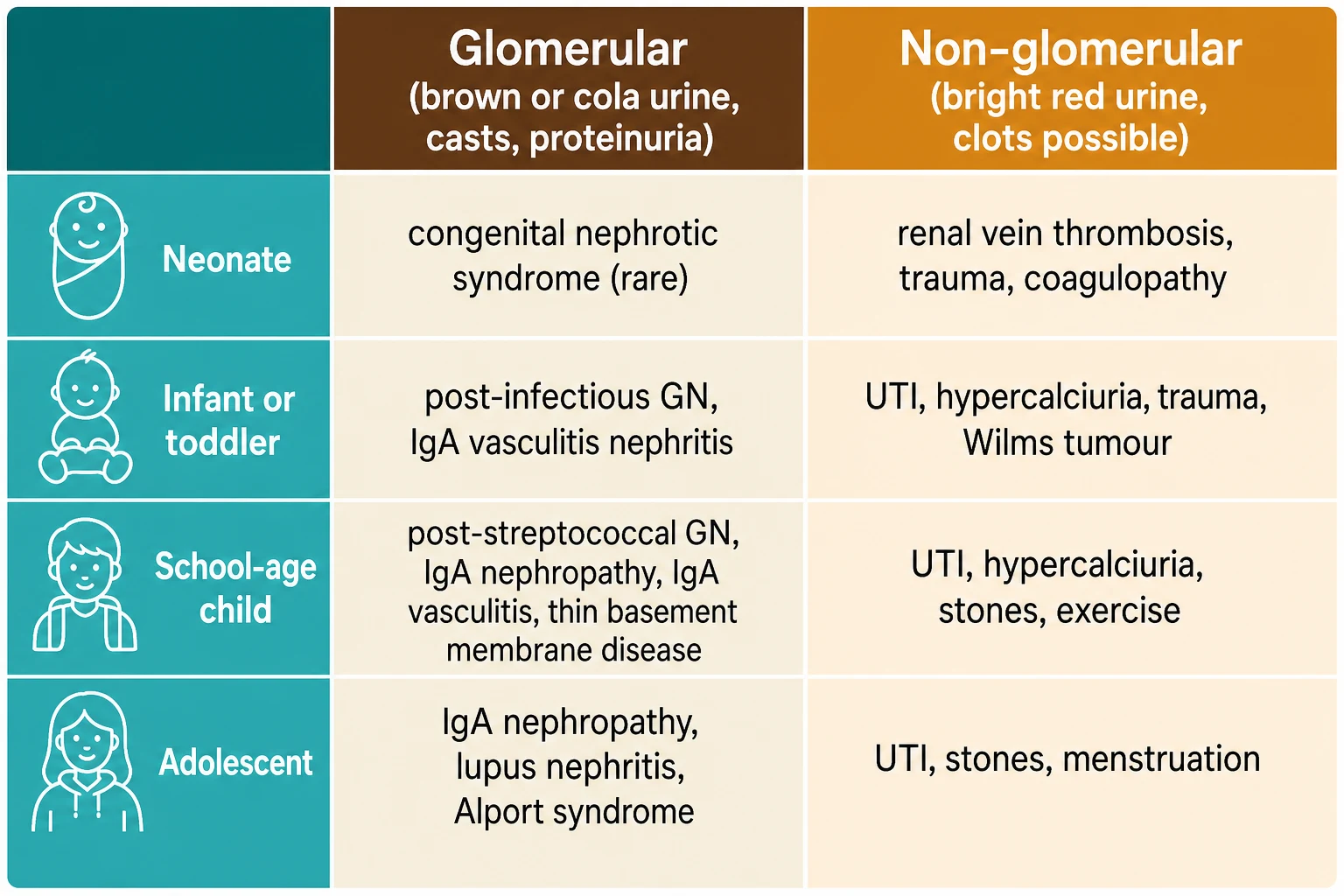
Within the glomerular column the causes shift with age and tempo. Recurrent cola-coloured urine at the same time as a sore throat is IgA nephropathy, the most common cause of chronic glomerular haematuria worldwide. A single episode of cola urine one to three weeks after a streptococcal throat infection is post-streptococcal glomerulonephritis. Persistent microscopic haematuria from early childhood with a family history of deafness and renal failure is Alport syndrome or thin basement membrane disease. [6] [8] [10]
The non-glomerular column has its own fingerprint. A neonate with gross haematuria and a flank mass may have a renal vein thrombosis. A febrile, dysuric child most often has a urinary tract infection. A well child with isolated microscopic haematuria and a family history of stones may have hypercalciuria, and a child with colicky flank pain may be passing a stone. A young child with a painless abdominal mass and haematuria raises the spectre of a Wilms tumour. [3] [11]
Glomerular source
- Brown, tea-coloured or cola-coloured urine
- Red-cell casts and dysmorphic red cells on microscopy
- Proteinuria and often hypertension, oedema or a rising creatinine
- Causes: IgA nephropathy, post-streptococcal GN, IgA vasculitis, lupus, Alport
Non-glomerular source
- Bright red or pink urine, clots possible
- Uniform intact red cells, no casts
- Pain, dysuria or a mass may point to the site
- Causes: UTI, hypercalciuria, stones, trauma, Wilms tumour, exercise
Not blood at all
- Dipstick positive but no red cells on microscopy
- Myoglobinuria from rhabdomyolysis, haemoglobinuria from haemolysis
- Red or pink urine from beets, blackberries, dyes, rifampicin
- Neonatal urate crystals stain the nappy pink but are not blood
Epidemiology & Risk Factors
Asymptomatic microscopic haematuria is a common incidental finding, turning up in roughly one to two per cent of school-age children on screening. The reassuring finding from the systematic review of 1092 children with asymptomatic microscopic haematuria is that benign or self-limited explanations, including hypercalciuria and mild glomerular disease, dominate, while dangerous causes are uncommon. The task of epidemiology is therefore to raise pre-test probability for the small minority who need urgent care, not to lower vigilance for the majority who do not. [4]
Age is the strongest epidemiological lever, because the statistical cause of haematuria moves predictably across childhood. Post-streptococcal glomerulonephritis remains the most common acute post-infectious glomerulonephritis in children and peaks in the early school years, while IgA nephropathy rises through late childhood and adolescence as the leading cause of recurrent visible glomerular haematuria. IgA vasculitis is the commonest childhood vasculitis and brings renal involvement in a significant proportion of cases. [8] [9]
Specific risk factors mark out the higher-risk child. A recent group A streptococcal throat or skin infection raises the chance of post-infectious glomerulonephritis, while a preceding bloody diarrhoeal illness raises the chance of haemolytic uraemic syndrome. A family history of renal failure, dialysis, transplant, consanguinity or hearing loss suggests Alport syndrome or thin basement membrane nephropathy, and a family history of stones suggests hypercalciuria. A child on anticoagulation, with a bleeding diathesis, or with recent abdominal trauma carries an added risk of urological bleeding. [10] [12]
Pathophysiology
The colour and shape of the red cells are not accidental; they are a record of where the blood has been. When blood crosses the glomerular basement membrane, the cells are physically distorted as they squeeze through the damaged filter, and they emerge as dysmorphic red cells, especially the spiky acanthocyte. Red cells that lodge in the tubules become trapped in protein secreted by the tubular cells, forming red-cell casts that are swept downstream and are pathognomonic of glomerular disease. The result is the brown, smoky, cola-coloured urine of nephritis, coloured by haem pigment and crowded with misshapen cells. [5] [1]
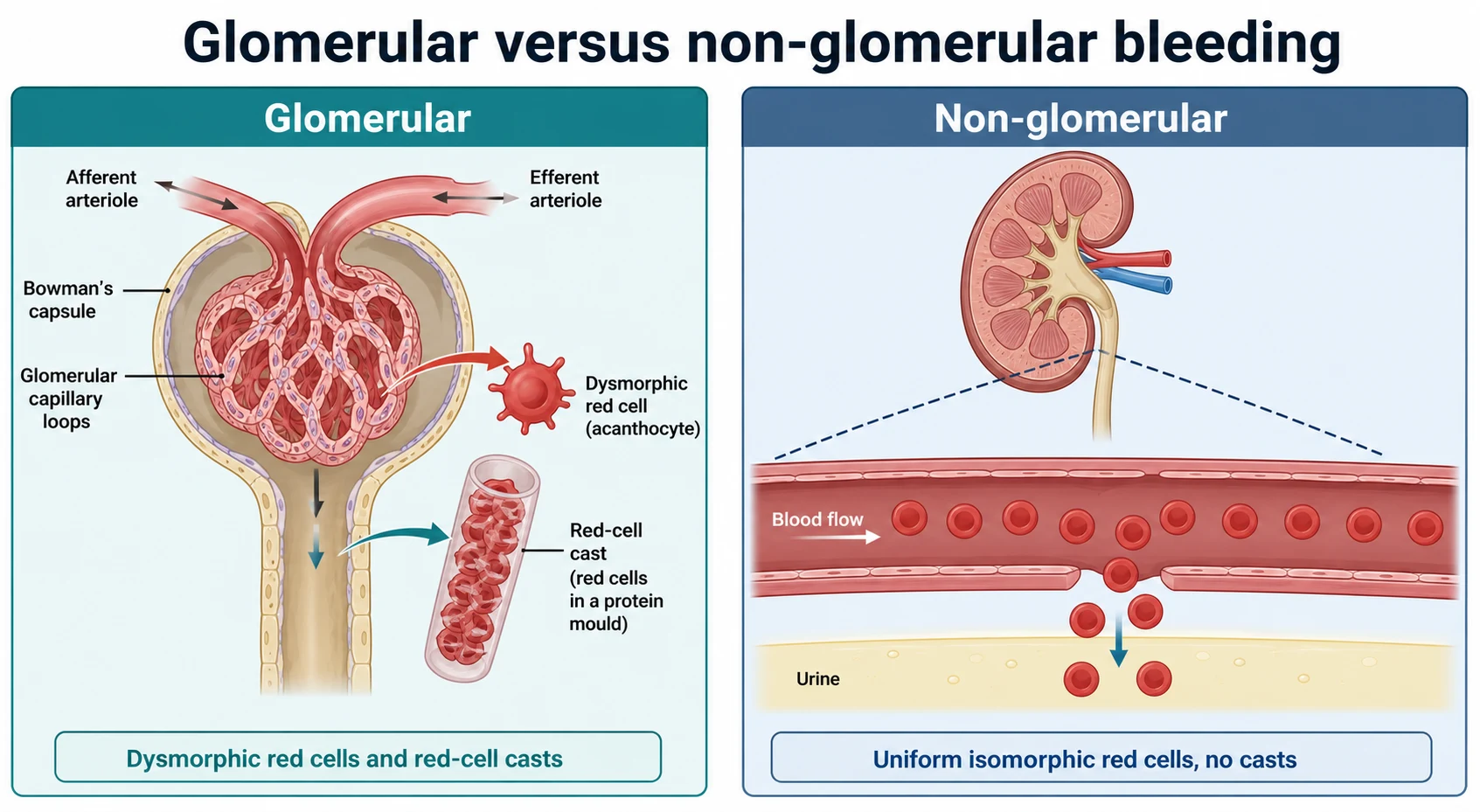
Non-glomerular bleeding behaves completely differently. Any break in the tract from the renal pelvis through the ureter, bladder and urethra releases intact, uniform red cells that have not crossed a filter and have not been moulded into casts. They keep their round shape, they may clot, and the urine stays bright red or pink. This is the pattern of a urinary tract infection eroding the mucosa, of a stone scraping the urothelium, of trauma, and of a tumour. [3]
The immunological mechanism of each glomerular cause is worth holding as a mental model, because it predicts the complement pattern. Post-streptococcal glomerulonephritis is driven by immune complexes deposited after group A streptococcal infection, activating the alternative complement pathway and dropping C3 while leaving C4 typically normal. IgA nephropathy is driven by mesangial deposition of aberrantly glycosylated IgA1 and usually leaves complement normal, which is why it presents as isolated haematuria rather than as a full nephritic crisis. Lupus nephritis activates the classical pathway and drops both C3 and C4. Holding these patterns lets you predict the cause from a single blood tube. [8] [7]
Clinical Presentation
The presentation divides first by whether the child looks well or sick, and second by the colour of the urine. A well child who happens to have blood found on a routine dipstick is a different problem from a child with brown urine, a swollen face and a headache, and the first minute of the encounter is spent telling them apart. The nephritic child shows oedema, hypertension, oliguria and a rising creatinine, and these signs demand urgent assessment rather than a delayed referral. [8]
The colour is the bedside clue that anchors the source. Brown, tea-coloured or cola-coloured urine points to a glomerular cause; bright red or pink urine points to a non-glomerular cause. The timing refines it further. Cola urine that appears at the same time as a sore throat, the synpharyngitic pattern, is the signature of IgA nephropathy, while cola urine appearing one to three weeks after a sore throat is post-streptococcal glomerulonephritis. Holding the colour and the latency together separates the two commonest glomerular diagnoses at the bedside. [6]
The accompanying features complete the picture. A palpable purpuric rash on the lower limbs and buttocks with arthritis and abdominal pain marks IgA vasculitis and its nephritis. Pallor, bruising, petechiae and oliguria after a diarrhoeal illness marks haemolytic uraemic syndrome. Persistent microscopic haematuria with a family history of hearing loss and renal failure marks Alport syndrome. A febrile, dysuric child points to infection, a child with colicky flank pain points to a stone, and a young child with a painless abdominal mass points to a Wilms tumour. [9] [12]
Differential Diagnosis
Build the differential from the source and the age together, because either alone is too broad to be useful. For a glomerular source, weigh IgA nephropathy, post-streptococcal and other post-infectious glomerulonephritis, IgA vasculitis nephritis, lupus nephritis, Alport syndrome and thin basement membrane nephropathy. For a non-glomerular source, weigh urinary tract infection, hypercalciuria, urolithiasis, trauma, exercise, coagulopathy, malignancy and, in adolescent girls, menstrual contamination. [2] [3]
Cola urine after infection
- Post-streptococcal GN if 1 to 3 weeks after a sore throat
- Low C3 with normal C4, raised streptococcal serology
- Oedema, hypertension, usually self-limited
- IgA nephropathy if concurrent with the sore throat
Bright red urine with pain
- Stone with colicky flank or abdominal pain
- Urinary tract infection with dysuria and fever
- Trauma, including non-accidental injury in a young child
- Hypercalciuria may be painless or colicky
Haematuria with systemic disease
- IgA vasculitis with palpable purpura and abdominal pain
- Haemolytic uraemic syndrome with pallor and oliguria
- Lupus nephritis in an adolescent girl
- Alport syndrome with familial deafness and renal failure
A few red-flag diagnoses must never be missed because they progress quickly or carry a high burden of disease. Haemolytic uraemic syndrome presents with the triad of microangiopathic haolytic anaemia, thrombocytopenia and acute kidney injury, and can deteriorate within hours. An acute nephritic emergency from severe hypertension or fluid overload can cause encephalopathy and pulmonary oedema. A renal vein thrombosis in a neonate can cost a kidney, and a Wilms tumour presenting as a painless mass with haematuria needs urgent imaging and a specialist referral, never a percutaneous biopsy first. [12] [3]
The benign and mimic causes still need to be named and distinguished, because reassuring a family correctly is itself a clinical skill. A positive dipstick with no red cells on microscopy is myoglobinuria or haemoglobinuria, not haematuria, and needs creatine kinase and a haemolysis screen. Red or pink urine from beets, blackberries, food dyes or rifampicin is not blood at all, and pink staining of a neonate's nappy from urate crystals is a benign mimic. Each benign cause is a diagnosis of reassessment, reached only after the dangerous ones have been considered. [1]
Clinical & Bedside Assessment
Run the assessment in parallel with the first urgent actions, because a nephritic child may need blood pressure control while the history is taken. Begin by judging whether the child looks well or sick, then measure the blood pressure in every case, because hypertension is the single most important vital sign in haematuria and its absence is not a licence to delay. Only once the child is stable and the blood pressure is known, turn to the focused history, examination and urine assessment. [2] [8]
The history should capture the colour and timing of the urine against any recent infection, sore throat or diarrhoeal illness, any pain, dysuria, fever, abdominal or flank pain, trauma, vigorous exercise, menstruation, and the child's medications. Ask specifically about a family history of renal disease, dialysis, transplant, deafness or consanguinity suggesting Alport syndrome or thin basement membrane disease, and of kidney stones suggesting hypercalciuria. In an adolescent girl, assess for pregnancy and systemic lupus erythematosus. [10] [9]
Examine for peri-orbital and peripheral oedema, pallor, petechiae or bruising, and measure the blood pressure against age-, sex- and height-specific centiles, where a pressure at or above the ninety-fifth centile signals hypertension. Palpate the abdomen for a mass or organomegaly, and look for the palpable purpura of IgA vasculitis on the lower limbs and buttocks, the arthritis, and the joint and skin findings. Assess hearing when Alport syndrome is suspected, and complete the bedside picture with a fresh urine sample for dipstick and microscopy. [8] [9]
Investigations
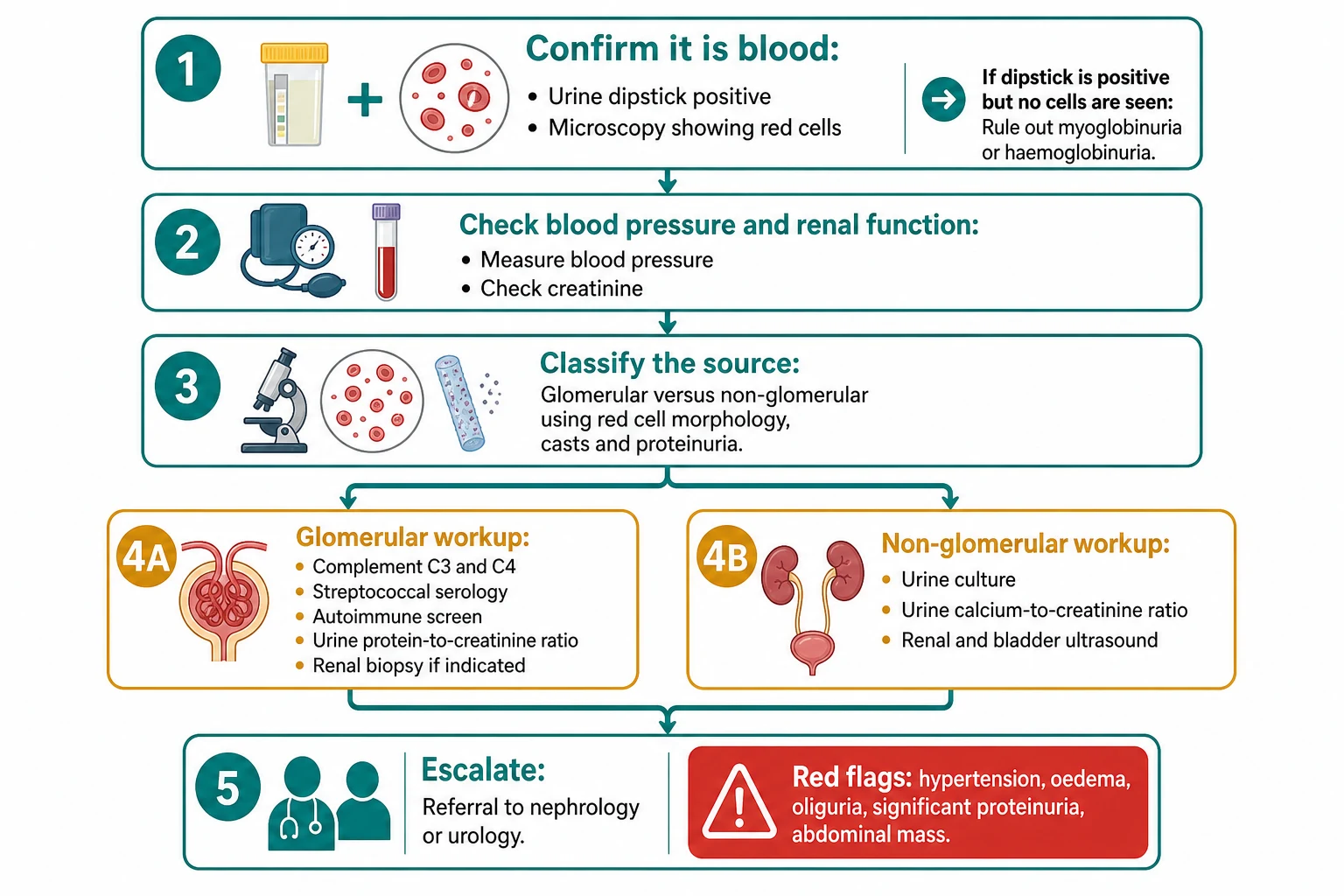
Choose investigations by the suspected source and the stability of the child, and never let a panel of bloods delay the control of a hypertensive emergency. The first test is the confirmation of blood itself: a urine dipstick positive for haemoglobin plus microscopy showing more than five red cells per high-power field confirms haematuria, while a positive dipstick with no red cells demands creatine kinase and a plasma free haemoglobin to chase myoglobinuria and haemoglobinuria. [1]
The baseline bloods in any significant haematuria are urea and electrolytes, creatinine, albumin, a full blood count and a coagulation screen. For a suspected glomerular source, add complement C3 and C4 and streptococcal serology such as anti-streptolysin O and anti-DNase B titres, which together distinguish post-streptococcal disease, where C3 is low and C4 is normal, from lupus nephritis, where both C3 and C4 are low. An autoimmune screen is added when lupus or a systemic vasculitis is plausible. [8] [7]
For a suspected non-glomerular source, the targeted tests are a urine culture to identify infection, an elevated urine calcium-to-creatinine ratio or a twenty-four-hour urinary calcium over four milligrams per kilogram per day to identify hypercalciuria, and a renal and bladder ultrasound to identify stones, obstruction or a mass. Renal ultrasound is also used in the glomerular pathway to exclude a structural or obstructive cause before biopsy. [11] [2]
The indications for a renal biopsy are the points where the diagnosis or the prognosis cannot be settled non-invasively. Biopsy is warranted for significant proteinuria, especially nephrotic-range proteinuria, a declining glomerular filtration rate, persistently low complement beyond the expected recovery of post-streptococcal disease, recurrent or persistent visible haematuria with significant proteinuria, and any atypical or progressive course. A well child with isolated microscopic haematuria, normal blood pressure and normal renal function does not need an urgent biopsy and is usually followed up. [6] [8]
The haematuria workup — the mnemonic CUBC
Management — Resuscitation
Most haematuria is not an immediate threat to life, but a small set of states is time-critical and must be recognised in the first hour. These are a hypertensive emergency from acute nephritis, severe fluid overload and hyperkalaemia from acute kidney injury, the multisystem failure of haemolytic uraemic syndrome, and massive urological bleeding with clots. The discipline is to look for these first, every time, before settling into a diagnostic workup. [8] [12]
A hypertensive emergency needs controlled blood pressure reduction, not an abrupt fall. Lower the pressure with a titratable antihypertensive infusion under close monitoring, because a sudden drop in a chronically hypertensive child can cause cerebral or retinal injury. Warn the nephrology and intensive care teams early, and treat the underlying nephritis with fluid and salt restriction, diuretics for overload, and management of hyperkalaemia, while the definitive diagnosis is pursued. [8]
Isotonic crystalloid
Dose
10 to 20 mL per kg
Fluid management is the recurring trap, because the nephritic and the haemolytic uraemic syndrome child is usually fluid overloaded rather than dehydrated. Restrict fluids and salt, use diuretics for overload, and correct hyperkalaemia and acidosis, reserving dialysis for refractory overload, uraemia or severe electrolyte disturbance. A child with an abdominal mass and haematuria is presumed to have a surgical or oncological cause and needs urgent imaging and a specialist referral, while a briskly bleeding urological source needs urology and a urinary catheter. [12] [3]
Management — Definitive & Stepwise
Once the child is stable, definitive care follows the source down a disciplined pathway. The management figure sets out the route from confirming blood and excluding mimics, through measuring blood pressure and classifying the source, to the branching glomerular and non-glomerular workups and the escalation triggers. The principle is to confirm and classify before you treat, and to escalate to nephrology, urology or oncology the moment a red flag appears. [2] [1]
Post-streptococcal glomerulonephritis is usually managed supportively and is self-limited. Balance fluid and salt, control the blood pressure, use diuretics for overload, and give antibiotic clearance of the group A streptococcus to prevent spread, while explaining to the family that the complement will recover within six to eight weeks and the long-term outlook is excellent. IgA nephropathy and IgA vasculitis nephritis are managed by a nephrologist, with blockade of the renin-angiotensin system for proteinuria and immunosuppression reserved for high-risk or severe disease. [8] [9]
Cause-specific treatment completes the picture. Hypercalciuria is managed with increased fluid intake and dietary modification, and urolithiasis is managed with urology, with lithotripsy or surgical removal as needed. A Wilms tumour is managed by the oncology and surgical teams, haemolytic uraemic syndrome is managed with supportive care and dialysis or complement blockade when indicated, and a urinary tract infection is treated with antibiotics guided by the culture. The definitive treatment always follows the diagnosis, which follows the resuscitation. [11] [12]
Specific Subtypes & Scenarios
Post-streptococcal glomerulonephritis is the subtype every candidate must own. The classic child is in the early school years, presenting one to three weeks after a streptococcal throat infection with cola-coloured urine, peri-orbital oedema and hypertension. The complement C3 is low with a normal C4, the streptococcal serology is raised, and the disease usually resolves completely with supportive care, the C3 normalising within six to eight weeks. The trap is to confuse its delayed onset with the synpharyngitic timing of IgA nephropathy. [8] [7]
IgA nephropathy is the subtype defined by its timing and its recurrence. An older child or adolescent has episodes of visible cola-coloured haematuria appearing at the same time as, or within a day or two of, an upper respiratory infection, with persistent microscopic haematuria between episodes. The complement is characteristically normal, the diagnosis is made by biopsy showing mesangial IgA deposition, and the Oxford classification stratifies the risk of progression. Not all children progress, but proteinuria, hypertension and a falling filtration rate mark those who will. [6]
IgA vasculitis nephritis is the subtype to remember in the child with a rash. A child with palpable purpura on the lower limbs and buttocks, arthritis and abdominal pain may have renal involvement that ranges from isolated haematuria to a full nephritic or nephrotic syndrome. The renal disease is managed by a nephrologist, with supportive care and, for severe disease, immunosuppression, and the family must be warned that renal involvement can appear or worsen even after the rash has settled. [9]
Alport syndrome is the subtype where the family history does the work. A child, usually a boy in the common X-linked form, has persistent microscopic haematuria from early childhood, with a family history of hearing loss and renal failure in male relatives. The biopsy shows thinning, lamellation and splitting of the glomerular basement membrane, and the management aims to delay the inexorable decline in renal function with renin-angiotensin blockade and ongoing surveillance. Screening of first-degree relatives is part of the care. [10]
Complications & Pitfalls
The complications flow from the underlying cause and from delay. An acute nephritis can cause hypertensive encephalopathy, pulmonary oedema, acute kidney injury and life-threatening hyperkalaemia, while IgA nephropathy and Alport syndrome carry a long-term risk of progression to chronic and end-stage kidney disease. Haemolytic uraemic syndrome can cause persistent hypertension, neurological involvement and chronic kidney disease, and a missed Wilms tumour can advance while a benign label is applied. [8] [12]
The pitfalls cluster around three avoidable errors. The first is to treat a dipstick-positive, cell-negative urine as haematuria and to miss rhabdomyolysis or haemolysis, both of which can be rapidly lethal. The second is to reassure a child with visible haematuria and no proteinuria without measuring the blood pressure, and so to miss a hypertensive emergency. The third is to attribute brown urine to dehydration, food or muscle damage without microscopy, and to miss a glomerular cause that needs complement testing and follow-up. [1] [8]
Prognosis & Disposition
Outcome depends on the cause and on the speed of recognition. Post-streptococcal glomerulonephritis usually resolves completely with an excellent long-term outlook, while IgA nephropathy and Alport syndrome carry a real risk of progressive chronic kidney disease that is modified by early treatment. Haemolytic uraemic syndrome has a variable outcome tied to the severity of the acute kidney injury and to neurological involvement, and a missed Wilms tumour carries the prognosis of its stage at diagnosis. [8] [10]
Disposition reflects the severity and the likely cause. A child with hypertension, significant proteinuria, a declining filtration rate, or an abdominal mass needs paediatric nephrology, urology or oncology referral and often admission, sometimes through a retrieval service with treatment continued in transit. A well child with isolated microscopic haematuria, normal blood pressure and normal renal function can be followed up in the outpatient setting with repeat urinalysis, provided the dangerous causes have been actively excluded. [1] [12]
Persistent microscopic haematuria, even when isolated, is not dismissed. It warrants long-term follow-up, because IgA nephropathy and Alport syndrome can declare themselves years later, and the screening of first-degree relatives is indicated whenever a familial cause is suspected. The safety-net for any child sent home is clear: return for visible haematuria, swelling, headache, reduced urine output or a swollen abdomen. [10]
Special Populations
The neonate is the population where the differential is most distinct and most time-critical. A neonate with gross haematuria may have a renal vein thrombosis, classically in an infant of a diabetic mother or a septic neonate, presenting with a flank mass and thrombocytopenia, or trauma from catheterisation, a coagulopathy including vitamin K deficiency bleeding, or a rare congenital cause. The early tools are renal ultrasound, a coagulation screen and a careful surgical review, and a well-looking neonate with haematuria is still assessed urgently. [2]
The adolescent girl is the population where systemic disease and contamination compete. Lupus nephritis enters the differential, and the assessment must include the joints, skin and an autoimmune screen, with pregnancy assessed where relevant. Menstrual blood can contaminate a urine sample and produce an apparent haematuria, so a clean-catch or catheter specimen and a menstrual history are needed before attributing the finding to renal disease. [9]
The child with a family history of renal failure, dialysis or transplant is the population where a single question changes the workup. Alport syndrome and thin basement membrane nephropathy are inherited causes of persistent microscopic haematuria, and the family history of hearing loss, consanguinity or early renal failure should trigger screening of first-degree relatives and long-term surveillance. Geography matters too, because a child with haematuria in a rural or remote community may be hours from a nephrologist, so early blood pressure measurement, urine microscopy locally and prompt retrieval when red flags appear are equity issues as much as clinical ones. [10] [2]
Evidence, Guidelines & Regional Differences
The evidence base blends diagnostic approach reviews with focused series on each glomerular cause. The approach to persistent microscopic haematuria, the approach to diagnosis and management of haematuria and the systematic review of asymptomatic microscopic haematuria together establish the glomerular versus non-glomerular split and the age-anchored differential. The Oxford classification of IgA nephropathy provides the consensus risk-stratification tool, and the clinical practice recommendations for Alport syndrome set the consensus for diagnosis and surveillance. [1] [6]
Where the evidence is softer, practice varies. The threshold for treating IgA vasculitis nephritis with corticosteroids, the role of routine screening of asymptomatic children, and the intensity of surveillance for isolated microscopic haematuria all show regional variation. The principles of confirming and classifying haematuria first, of measuring the blood pressure in every case, and of escalating for the red flags are consistent everywhere. [9] [10]
Regional practice is consistent in principle and variable in logistics. The rule that haematuria is confirmed with microscopy and split into a glomerular and a non-glomerular pathway is universal, but access to paediatric nephrology, timely renal biopsy and rapid complement testing differs between and within countries. In Australia and New Zealand, a child with haematuria in a rural or Indigenous community may be far from a tertiary centre, so early recognition, local blood pressure measurement and urine microscopy, and a prompt retrieval discussion are what protect the child during transfer. [2] [1]
Exam Pearls
Hold one sentence above all others: confirm that red or brown urine really is blood, then split it into a glomerular and a non-glomerular source, because that single fork decides the whole investigation pathway. State the reflex that follows, which is to confirm haematuria with microscopy showing more than five red cells per high-power field, to measure the blood pressure in every child, and to escalate for the red flags of hypertension, oedema, oliguria, significant proteinuria and an abdominal mass. This answer covers both the marks and the patient. [1] [8]
Get the frequently tested facts exactly right. Microscopic haematuria means more than five red cells per high-power field, and a positive dipstick with no red cells is myoglobinuria or haemoglobinuria, not haematuria. Red-cell casts and dysmorphic red cells point to a glomerular source, and uniform red cells point to a non-glomerular source. Post-streptococcal glomerulonephritis gives a low C3 with a normal C4 one to three weeks after a throat infection, while lupus nephritis gives a low C3 and a low C4. [5] [7]
The high-yield pairings do the work in a viva. Cola urine at the same time as a sore throat has IgA nephropathy with a normal complement. Cola urine one to three weeks after a sore throat has post-streptococcal glomerulonephritis with a low C3. Palpable purpura with abdominal pain has IgA vasculitis nephritis. Familial deafness with renal failure has Alport syndrome. Always confirm blood with microscopy and measure the blood pressure before you chase the cause. [6] [10]
References
- [1]Kallash M; Rheault MN Approach to Persistent Microscopic Hematuria in Children. Kidney360, 2020.PMID 35369549
- [2]Vedula R; Iyengar AA Approach to Diagnosis and Management of Hematuria. Indian J Pediatr, 2020.PMID 32026313
- [3]Tu WH; Shortliffe LD Evaluation of asymptomatic, atraumatic hematuria in children and adults. Nat Rev Urol, 2010.PMID 20212514
- [4]Clark M; Aronoff S; Del Vecchio M Etiologies of asymptomatic microscopic hematuria in children - systematic review of 1092 subjects. Diagnosis (Berl), 2015.PMID 29540037
- [5]Bottini PV; Andreguetto BD; Krempser K; et al UriSed as an Alternative to Phase-Contrast Microscopy in the Differentiation between Glomerular and Non-Glomerular Hematuria. Clin Lab, 2015.PMID 26118201
- [6]Trimarchi H; Barratt J; Cattran DC; et al Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group. Kidney Int, 2017.PMID 28341274
- [7]Iyengar A; Kamath N; Radhakrishnan J; et al Infection-Related Glomerulonephritis in Children and Adults. Semin Nephrol, 2023.PMID 38242806
- [8]Duong MD; Reidy KJ Acute Postinfectious Glomerulonephritis. Pediatr Clin North Am, 2022.PMID 36880922
- [9]Pillebout E; Sunderkötter C IgA vasculitis. Semin Immunopathol, 2021.PMID 34170395
- [10]Kashtan CE; Gross O Clinical practice recommendations for the diagnosis and management of Alport syndrome in children, adolescents, and young adults-an update for 2020. Pediatr Nephrol, 2021.PMID 33159213
- [11]MohammadKhawajah I; Shamshiri Khamene S; Mahboobipour AA; et al Investigating the Prevalence of Hypercalciuria in Children Aged 2-16 Years With Asymptomatic Microscopic Hematuria in 2020 in Tehran Children's Medical Center. Clin Case Rep, 2024.PMID 39545136
- [12]Gülhan B; Özaltın F; Fidan K; et al Management of pediatric hemolytic uremic syndrome. Turk J Pediatr, 2024.PMID 38523374