Paeds · nephrology-urology-fluids-and-electrolytes
Hyponatraemia and hypernatraemia
Also known as Hyponatraemia · Hypernatraemia · Sodium disorders · Dysnatraemia · Low sodium · High sodium · Water balance disorders · SIAD
Fellowship guide to sodium and water disorders in children: hyponatraemia as a serum sodium below 135 and hypernatraemia as above 145 mmol/L, the volume-status classification of hypo-, eu- and hypervolaemic hyponatraemia and the water-loss versus sodium-gain classification of hypernatraemia, arginine vasopressin and thirst physiology, brain cell volume adaptation and its two failure modes, 3 percent hypertonic saline boluses for severe symptomatic hyponatraemia at a maximum correction of 8 mmol/L in 24 hours to avoid osmotic demyelination, and slow hypernatraemia correction at a maximum of 0.5 mmol/L per hour to avoid cerebral oedema.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Sodium sits in a narrow band. The body defends a serum sodium of 135 to 145 mmol/L with a system that is essentially a water-control machine: arginine vasopressin (also called antidiuretic hormone, ADH) from the posterior pituitarius, the thirst it generates, and the kidney's ability to dilute or concentrate the urine. When that system fails, the serum sodium drifts, and because sodium is an effective osmole that does not cross cell membranes easily, the water follows it — into the brain cells in hyponatraemia, out of them in hypernatraemia. The brain, locked inside a rigid skull, cannot tolerate either swing, and that is why every sodium disorder is at heart a brain-cell-volume problem. [1] [5]
This page treats the two disorders as a mirror image. Hyponatraemia is the commoner and the one most often made in hospital, so it gets the 3 percent saline resuscitation framework and the volume-status classification. Hypernatraemia is rarer on the ward but commoner in infants and at the extremes of illness, so it gets the free-water deficit and the slow-correction framework. Both share the same organising logic: classify by water balance, let the neurological examination set the tempo, and never correct faster than the brain can follow. [5] [2]
Overview & Definition
Hyponatraemia is a serum sodium below 135 mmol/L. It is graded by severity: mild (130 to 135), moderate (125 to 130), and severe (below 125). The number alone is a poor guide to danger — what matters is whether the brain is symptomatic. A child with a seizure or coma at any sodium level needs emergency treatment; a child who is alert and well may need only investigation and slow correction. [3] [1]
Hypernatraemia is a serum sodium above 145 mmol/L, with moderate disease from 150 to 160 and severe above 160. Like hyponatraemia, severity is neurological rather than numerical, but the danger here is cerebral dehydration and shrinkage, with the added risk of bleeding from torn bridging veins. Both thresholds are serum concentrations, and both demand a repeat sample to exclude artefact before you act on an asymptomatic, mildly abnormal result. [2] [5]
The serum sodium is a concentration, not a content. It tells you the ratio of body sodium (and its anions) to body water at that instant, not how much of either the body holds. A child may have hyponatraemia with excess total-body sodium — as in heart failure, where the problem is even greater excess water — or hypernatraemia with a normal or low total-body sodium, as in diabetes insipidus, where the problem is pure water loss. Treating the number without understanding the water balance is the root of most sodium-management errors. [1] [2]
Classification
Every cause of hyponatraemia lives in one of three volume-status buckets, and every cause of hypernatraemia lives in one of two water-balance buckets. The figure below lays the common paediatric causes onto these axes for both disorders. [5] [1]
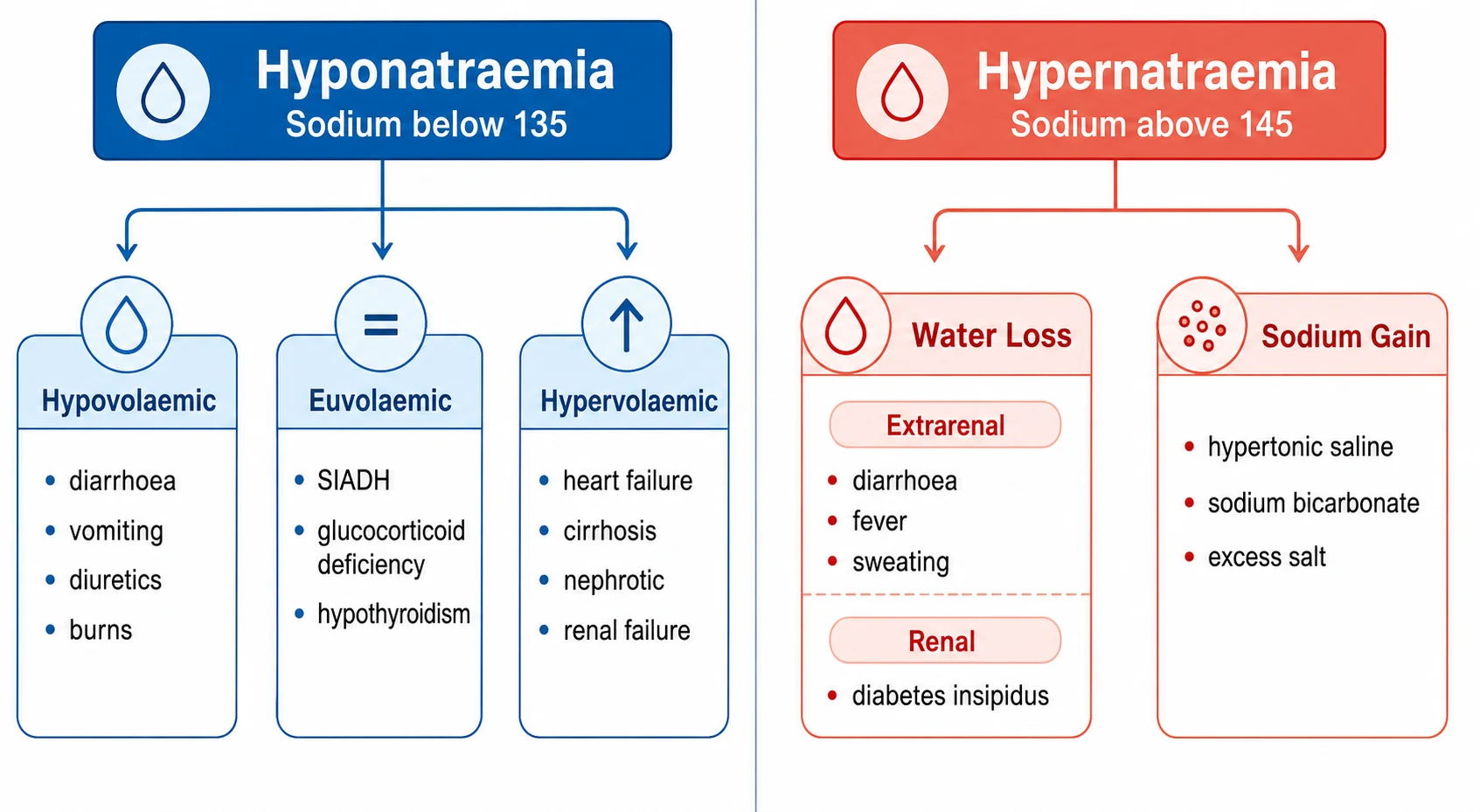
For hyponatraemia the decisive branch point is the child's volume status. Hypovolaemic hyponatraemia means both sodium and water have been lost, with more sodium than water — diarrhoea, vomiting, diuretics, burns, and cerebral salt wasting. Euvolaemic hyponatraemia means water excess without oedema — the syndrome of inappropriate antidiuresis (SIAD), glucocorticoid deficiency, hypothyroidism, and primary polydipsia. Hypervolaemic hyponatraemia means excess total body sodium but even greater excess water — heart failure, cirrhosis, nephrotic syndrome, and renal failure. The bedside examination of volume status, confirmed by the urine sodium and osmolality, sorts these within minutes. [3] [1]
For hypernatraemia the branch point is water loss versus sodium gain. Water loss is by far the commoner in children and splits into renal (central or nephrogenic diabetes insipidus, osmotic diuresis of DKA, diuretics) and extrarenal (fever, sweating, hyperventilation, diarrhoea, and the inadequate intake of a poorly feeding neonate). Sodium gain is iatrogenic or accidental — hypertonic saline, sodium bicarbonate, and salt poisoning. The urine osmolality is the key test: a dilute urine despite a high serum sodium points to diabetes insipidus; a concentrated urine points to extrarenal water loss or sodium gain. [2] [5]
Hyponatraemia (Na below 135 mmol/L)
- Hypovolaemic: diarrhoea, vomiting, diuretics, burns, cerebral salt wasting
- Euvolaemic: SIAD, glucocorticoid deficiency, hypothyroidism, primary polydipsia
- Hypervolaemic: heart failure, cirrhosis, nephrotic syndrome, renal failure
- Hospital-acquired: hypotonic maintenance fluid with non-osmotic ADH
Hypernatraemia (Na above 145 mmol/L)
- Water loss, renal: central or nephrogenic diabetes insipidus, osmotic diuresis, diuretics
- Water loss, extrarenal: fever, sweating, hyperventilation, diarrhoea, poor intake
- Sodium gain: hypertonic saline, sodium bicarbonate, salt poisoning
- Infant-specific: breastfeeding-associated hypernatraemia, immature concentrating ability
Epidemiology & Risk Factors
Dysnatraemia is the commonest electrolyte disturbance in hospitalised children, and hyponatraemia is by far the dominant end. The risk concentrates in a few well-defined groups: postoperative children, those with respiratory illness, children on diuretics, premature neonates, and — above all — any child receiving hypotonic maintenance fluid while ill. The shared mechanism is non-osmotic arginine vasopressin release: pain, nausea, respiratory illness, the postoperative state, and positive-pressure ventilation all drive ADH, and when that ADH acts on a kidney being given hypotonic fluid, the serum sodium falls. [7] [8]
The hospital-acquired hyponatraemia story is one of the great preventable-harm lessons of modern paediatrics. For decades children received 0.45 percent (or even 0.18 percent) saline with dextrose as maintenance fluid, following the Holliday-Segar rationale. Then the evidence shifted. Moritz and Ayus argued that non-osmotic ADH is near-universal in sick children, making any hypotonic fluid potentially dangerous; the McNab JAMA trial and the Padua systematic review then showed that isotonic maintenance fluid prevents hyponatraemia without increasing hypernatraemia or fluid overload. The practical result is that isotonic fluid (0.9 percent saline or balanced crystalloid with dextrose) is now the default in most paediatric units worldwide. [8] [9]
Hypernatraemia is rarer on the ward but commoner at the extremes of infancy and illness. The highest-risk groups are the newborn with inadequate breastfeeding (breastfeeding-associated hypernatraemia, presenting in the first week with weight loss over 10 percent and a sodium above 150), the child with diabetes insipidus who cannot access water, the child with severe diarrhoea and inadequate free-water replacement, and the critically ill child with large insensible losses. The neonate is especially vulnerable because the immature kidney cannot concentrate urine well, and a large surface-area-to-weight ratio drives insensible water loss. [2] [10]
Pathophysiology
Sodium controls where water goes, and the brain is where this matters most. Because sodium is an effective osmole that crosses cell membranes slowly, any change in serum sodium pulls water across the blood-brain barrier into or out of the brain cells. The body defends against this with a remarkable adaptation: over hours to days, the brain cells adjust their own intracellular osmole content to match the serum, protecting their volume. This adaptation is the key to understanding both why acute changes are so dangerous and why chronic changes must be corrected slowly. [5] [1]
Arginine vasopressin is the master regulator. Osmoreceptors in the hypothalamus sense a rise in serum osmolality of as little as 1 to 2 percent and trigger ADH release from the posterior pituitary; ADH then inserts aquaporin-2 water channels in the renal collecting duct, allowing water reabsorption and concentrating the urine. Thirst is triggered in parallel, protecting against water deficit. In hypernatraemia the ADH-thirst system is maximally active, urine is maximally concentrated, and thirst drives intake — unless the child cannot drink or the kidney cannot respond (as in diabetes insipidus). In hyponatraemia the system is suppressed, urine should be dilute, and the sodium falls only when water intake exceeds the diluting capacity or when non-osmotic ADH keeps the system switched on. [1] [5]
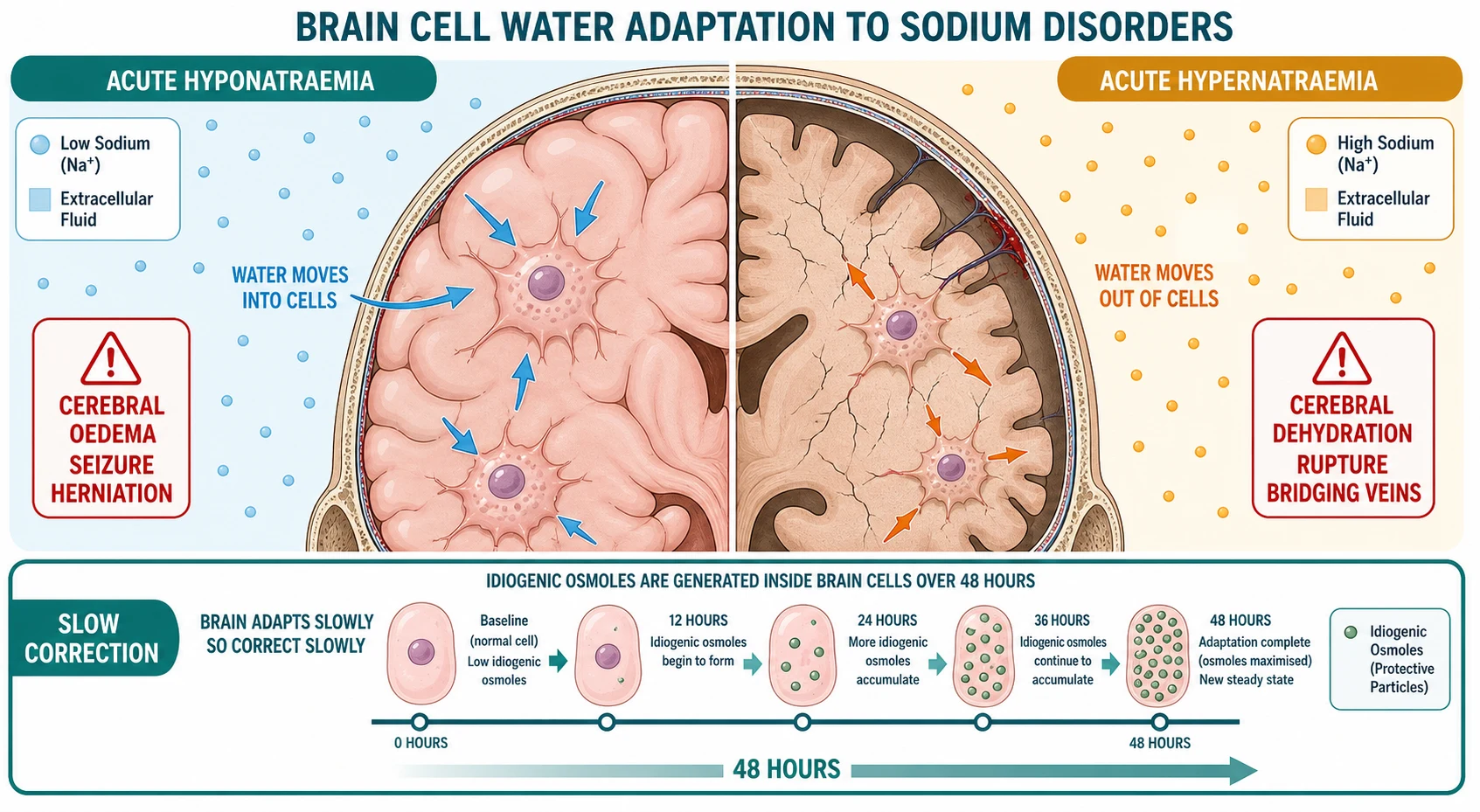
In acute hyponatraemia the serum sodium falls faster than the brain can adapt. Water moves into brain cells down the osmotic gradient, the cells swell, and the brain, trapped in the rigid skull, develops cerebral oedema and raised intracranial pressure. The clinical correlate is headache, vomiting, confusion, seizure, coma, and ultimately herniation with respiratory arrest. This is why acute severe hyponatraemia is a neurological emergency. [5] [11]
In acute hypernatraemia the mirror image occurs. Water moves out of brain cells, the cells shrink, and the brain pulls away from the dura, tearing the delicate bridging veins that run between the cortex and the venous sinuses. The result is cerebral dehydration, irritability, hyperreflexia, seizure, coma, and potentially catastrophic intracranial haemorrhage. The very young brain is most at risk, which is why neonatal hypernatraemia carries a particular burden of neurological injury. [2] [10]
The adaptation is the reason for the cardinal treatment rule. In chronic hyponatraemia (over 48 hours), the brain has extruded intracellular osmoles — first potassium, then organic osmolytes — to shed water and limit the swelling. If you now correct the sodium too quickly, the serum becomes hypertonic relative to the newly depleted brain cells, water rushes out, and the cells shrink and demyelinate, producing osmotic demyelination syndrome (central pontine myelinolysis). In chronic hypernatraemia the reverse holds: the brain has generated idiogenic osmoles to hold onto water, so rapid correction floods the adapted cells and causes cerebral oedema. In both cases the brain that has adapted to the abnormal sodium cannot follow a fast correction, and the injury is often worse than the original disorder. [3] [5]
Clinical Presentation
Hyponatraemia presents with the brain. Headache, nausea, and vomiting come first, then lethargy, confusion, and disorientation, and in severe disease seizure, coma, and respiratory arrest from cerebral oedema and raised intracranial pressure. Infants and young children present non-specifically — irritability, poor feeding, drowsiness, hypotonia — and the sodium is found on routine bloods. The tempo matters as much as the number: a sodium that has fallen over hours is far more dangerous than one that has sat at 120 for days, because the acute brain has not adapted. [5] [1]
Hypernatraemia also presents with the brain, but the picture is of dehydration rather than oedema. Irritability, lethargy, a high-pitched cry, hyperreflexia, and altered mental state give way in severe disease to seizure and coma. The child is characteristically thirsty, but an infant or an unconscious child cannot signal or meet that thirst, which is why hypernatraemia can advance to dangerous levels undetected. Bridging-vein haemorrhage may present as a rapid neurological decline or a seizure in the recovery phase. [2] [10]
The history discriminates the cause. For hyponatraemia, ask about fluid losses (diarrhoea, vomiting), recent surgery, respiratory illness, diuretic use, and drugs that cause SIAD (vincristine, SSRIs, carbamazepine, cyclophosphamide, desmopressin). For hypernatraemia, ask about polyuria and polydipsia (diabetes insipidus), diarrhoea, fever, sweating, poor feeding in a neonate, head injury or CNS tumour, and any sodium-containing fluid given. Examination adds the volume status — the single most useful discriminator for hyponatraemia — and the neurological state, which sets the tempo of treatment. [1] [2]
Differential Diagnosis
For hyponatraemia, branch first on volume status, confirmed by the urine sodium and osmolality. Hypovolaemic hyponatraemia shows clinical dehydration with a low urine sodium (below 20) if the loss is extrarenal (diarrhoea, vomiting, burns, third spacing) or a high urine sodium (above 40) if the loss is renal (diuretics, cerebral salt wasting, mineralocorticoid deficiency). Euvolaemic hyponatraemia shows no oedema and no dehydration, with an inappropriately concentrated urine (above 100 mOsm per kg) and a urine sodium above 40 — classic for SIAD, and also for glucocorticoid deficiency and hypothyroidism. Hypervolaemic hyponatraemia shows oedema and a low urine sodium (below 20, because the effective circulating volume is low and aldosterone is high) — heart failure, cirrhosis, nephrotic syndrome, and renal failure. [3] [1]
For hypernatraemia, branch on the urine osmolality. A dilute urine (below 250 to 300 mOsm per kg) despite a high serum sodium identifies diabetes insipidus: central if it responds to desmopressin, nephrogenic if it does not. A concentrated urine (above 700 to 800 mOsm per kg) means the kidney is doing its job and the loss is extrarenal (fever, sweating, hyperventilation, diarrhoea, poor intake) or due to sodium gain. An intermediate urine osmolality (300 to 700) suggests partial diabetes insipidus, osmotic diuresis (DKA, mannitol), or a kidney that is concentrating poorly (chronic kidney disease, sickle cell). [2] [5]
SIAD and cerebral salt wasting are the two euvolaemic-to-hypovolaemic hyponatraemias that examiners love, and they are separated by the volume status and the response to saline. SIAD is truly euvolaemic: concentrated urine, high urine sodium, low uric acid, normal blood urea, and it responds to fluid restriction. Cerebral salt wasting is truly hypovolaemic: high urine sodium, low to normal uric acid, signs of dehydration, and it responds to saline and salt replacement. In practice SIAD is commoner (meningitis, pneumonia, pain, drugs) and cerebral salt wasting clusters after neurosurgery, traumatic brain injury, and subarachnoid haemorrhage. [3] [5]
SIAD (syndrome of inappropriate antidiuresis)
- Euvolaemic: no oedema, no dehydration
- Inappropriately concentrated urine above 100 mOsm per kg with high urine sodium above 40
- Low serum uric acid, normal to low blood urea
- Responds to fluid restriction; common causes are meningitis, pneumonia, pain, and drugs
Cerebral salt wasting
- Hypovolaemic: clinical dehydration, tachycardia, oliguria responding to volume
- High urine sodium above 40 with concentrated urine
- Low to normal uric acid, high blood urea from dehydration
- Responds to saline and salt replacement; clusters after neurosurgery, head injury, subarachnoid haemorrhage
Clinical & Bedside Assessment
Begin with airway, breathing, and circulation, and attach cardiac and neurological monitoring immediately. The first question in any dysnatraemia is not "what is the cause" but "is this child's brain in danger", and the answer is the neurological examination. Assess the conscious level (AVPU or GCS), the pupils, the posture, and whether there is seizure activity. A seizing or comatose child with severe hyponatraemia needs 3 percent hypertonic saline now; an alert child with a chronic, mild abnormality needs investigation and slow correction. [5] [11]
Assess volume status at the bedside, because it decides the classification and the fluid strategy for hyponatraemia. Look and feel for the dry signs — cool peripheries, prolonged capillary refill (over 2 seconds), tachycardia, low blood pressure, dry mucous membranes, reduced skin turgor, sunken fontanelle in the infant — which mark hypovolaemia. Look for the wet signs — peripheral and sacral oedema, raised jugular venous pressure, pulmonary crackles, ascites — which mark hypervolaemia. A child who is clinically euvolaemic, with concentrated urine and a high urine sodium, is in the SIAD/euvolaemic group until proven otherwise. [1] [3]
Take a focused history aimed at the cause and the tempo. Run through the fluid losses, the recent surgery, the respiratory and neurological illness, the medication list (diuretics, desmopressin, vincristine, SSRIs, carbamazepine, thiazides, lithium), the intake (poor feeding, polydipsia, salt ingestion), and the head injury or CNS event. Review every fluid prescription on the chart — a child on hypotonic maintenance fluid with a falling sodium has hospital-acquired hyponatraemia until proven otherwise. In parallel, screen for the precipitating emergency — meningitis, head injury, the postoperative state, sepsis with SIAD physiology, diabetic ketoacidosis — because treating the sodium without the cause will fail. [7] [8]
Investigations
The core panel can be drawn from one cannula and is the same for both disorders: a repeat serum sodium on a free-flowing sample, serum osmolality, urine sodium, urine osmolality, urea, creatinine, glucose, potassium, and a venous blood gas for pH. Send the serum and urine osmolality simultaneously — they are only interpretable together. The blood gas tells you about acid-base and DKA within seconds, and the glucose tells you whether hyperglycaemia has translocated the sodium. [3] [1]
WATER
For hyponatraemia, the serum osmolality splits the problem into three. Hypotonic (below 275 mOsm per kg) is the clinically important group — the brain is at risk. Isotonic (275 to 295) is pseudohyponatraemia from hyperlipidaemia or hyperproteinaemia, where the sodium is artefactually low and the brain is not at risk. Hypertonic (above 295) is translocational — the sodium is low because another osmole, usually glucose, has pulled water into the plasma. Correct for glucose by adding roughly 2 mmol/L to the sodium for every 4 mmol/L of glucose above 5.5 mmol/L; the corrected sodium tells you whether a true hyponatraemia coexists. Within the hypotonic group, the urine osmolality and sodium then classify by volume status as above. [1] [5]
For hypernatraemia, the urine osmolality is the key test. A maximally concentrated urine (above 700 to 800 mOsm per kg) confirms the kidney is responding normally and the loss is extrarenal or due to sodium gain. A dilute urine (below 250 to 300) identifies diabetes insipidus; a water deprivation test with a desmopressin response separates central from nephrogenic. Targeted tests follow the screen: cortisol and a short synacthen test for adrenal insufficiency (a cause of both hyponatraemia and, rarely, hypernatraemia), thyroid function, uric acid (low in SIAD and cerebral salt wasting), and where indicated a drug screen and a head imaging for central causes. [2] [10]
Management — Resuscitation
Severe symptomatic hyponatraemia — seizure, coma, or respiratory distress from cerebral oedema — is a neurological emergency, and the treatment is intravenous 3 percent hypertonic saline. Give 2 mL per kg over 10 minutes, repeated up to two or three times if seizures continue, aiming for a rise of 4 to 6 mmol/L or cessation of seizures, whichever comes first. The goal is not to normalise the sodium; it is to raise the serum osmolality just enough to pull water out of the swollen brain and relieve the cerebral oedema. A 2 mL per kg bolus of 3 percent saline raises the sodium by roughly 2 to 4 mmol/L. Maximum single bolus is about 100 mL. [6] [11]
The evidence and advocacy for 3 percent saline in symptomatic hyponatraemic encephalopathy is strong. Ayus and Moritz have argued for two decades that the fear of osmotic demyelination has caused more deaths from under-treated cerebral herniation than over-correction has ever caused ODS — a small, targeted rise with boluses is safe, effective, and life-saving. The key is that bolus therapy is self-limiting: a 2 mL per kg bolus gives a measured, modest rise, and the target is seizure control, not normalisation. Once the brain is safe, the slow correction begins. [11] [6]
3% hypertonic saline (severe symptomatic hyponatraemia with seizure or coma)
Dose
2 mL/kg bolus
For severe hypernatraemia the resuscitation is gentler but no less urgent. If the child is shocked, restore intravascular volume with isotonic saline boluses (10 to 20 mL per kg) until perfusion is restored — the immediate threat is shock, and isotonic saline does not significantly change the sodium. Once perfused, begin the calculated free-water correction over 48 hours at the rate limit below. Oral or nasogastric free water is preferred wherever feasible, because the gut controls the rate far better than an intravenous line, and the risk of cerebral oedema is lower. [2] [10]
Management — Definitive & Stepwise
The definitive ladder for hyponatraemia has five rungs, applied in order. First, assess severity and symptoms and give 3 percent saline boluses for severe symptomatic disease. Second, correct slowly for chronic or asymptomatic disease — the ceiling is 8 mmol/L in 24 hours (some guidelines allow 10 to 12, but 8 is the safer figure for the high-risk child). Third, stop hypotonic fluids and use isotonic maintenance fluid — this alone corrects many hospital-acquired hyponatraemias. Fourth, treat the cause: fluid-restrict SIAD (typically 60 to 80 percent of maintenance), give glucocorticoids for adrenal insufficiency, restore volume for hypovolaemia, and salt-restrict and loop-diurese the hypervolaemic child. Fifth, monitor the sodium every 2 to 4 hours during active correction and adjust the rate to stay within the ceiling. [3] [5]
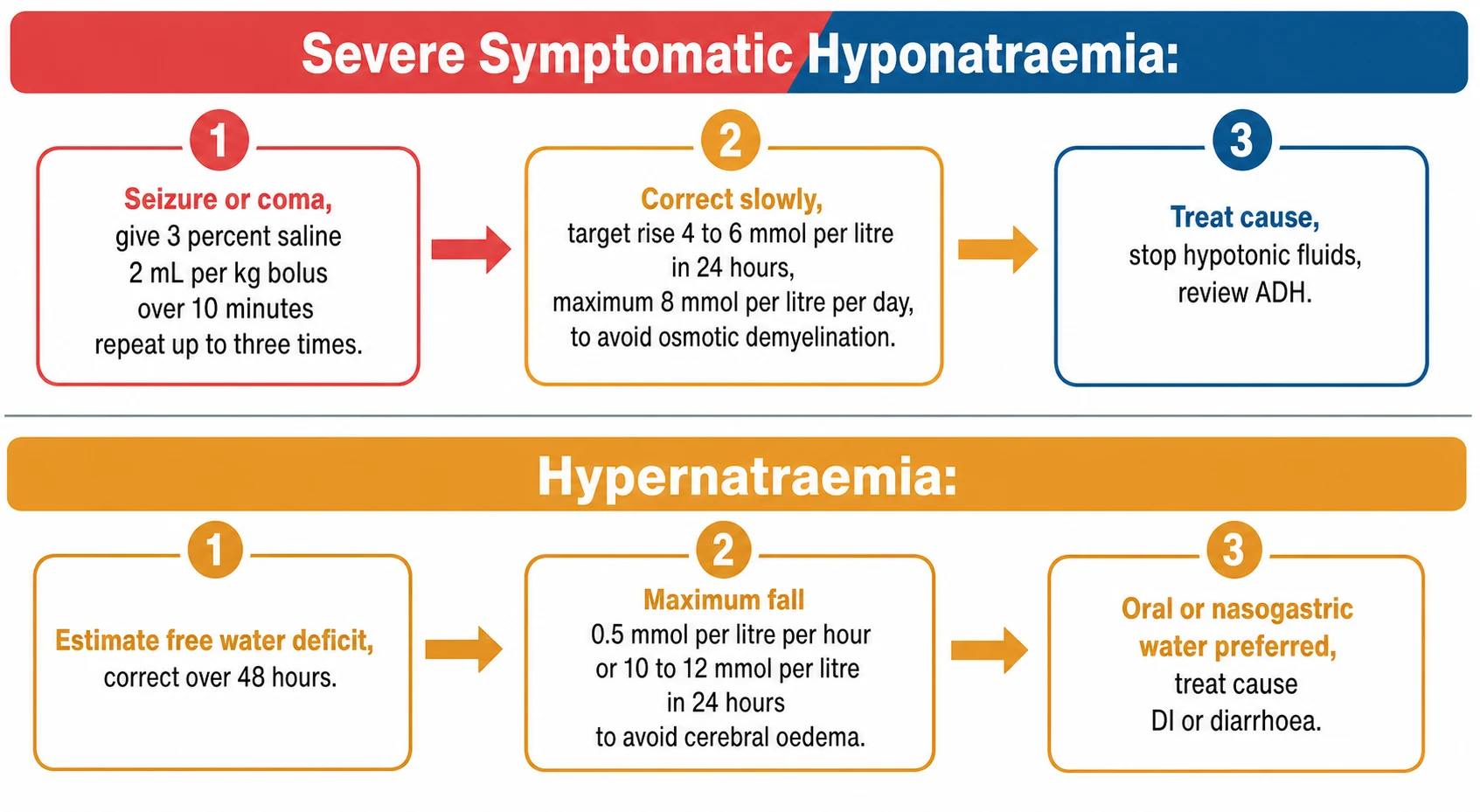
The definitive ladder for hypernatraemia has four rungs. First, assess severity and cause, and restore intravascular volume with isotonic saline if shocked. Second, estimate the free-water deficit: in older children the deficit is roughly 0.6 times body weight (in kg) times the sodium minus 140 divided by 140, with infants using a higher water fraction. Third, correct over 48 hours at a maximum of 0.5 mmol per litre per hour (10 to 12 mmol/L in 24 hours) — the hard rate limit that prevents cerebral oedema. Fourth, treat the cause: give desmopressin for central diabetes insipidus, reduce solute load and use hydrochlorothiazide or indometacin for nephrogenic DI, replace ongoing losses, and ensure adequate intake. [2] [10]
Severe symptomatic hyponatraemia — the five-rung ladder
Assess severity and symptoms; secure cardiac and neurological monitoring
Give 3% saline 2 mL/kg bolus over 10 min for seizure or coma; repeat up to 3 times for a 4 to 6 mmol/L rise
Switch to slow correction: target no more than 8 mmol/L rise in 24 hours
Stop hypotonic fluids, use isotonic maintenance; fluid-restrict SIAD, give steroids for adrenal insufficiency
Treat the cause and monitor sodium every 2 to 4 hours, adjusting rate to stay within the ceiling
Hypernatraemia — the four-rung ladder
Restore intravascular volume with isotonic saline boluses if shocked
Estimate free-water deficit (0.6 x weight x (Na minus 140) / 140); add ongoing losses
Correct over 48 hours at max 0.5 mmol/L per hour (10 to 12 in 24 hours); prefer oral or nasogastric water
Treat the cause: desmopressin for central DI, solute reduction and thiazide for nephrogenic DI
Specific Subtypes & Scenarios
Hospital-acquired hyponatraemia is the scenario that changed paediatric fluid practice. A sick or postoperative child releases non-osmotic ADH, and if given hypotonic maintenance fluid, the kidney retains the free water and the sodium falls — sometimes to seizure within hours. The treatment is to stop the hypotonic fluid and switch to isotonic maintenance fluid, which corrects most cases. The prevention is the evidence-based default of isotonic fluid for all hospitalised children, established by the McNab trial and the systematic reviews. This single policy change has prevented countless seizures and is one of the highest-yield pieces of knowledge in paediatric fluids. [7] [8]
SIAD is the commonest euvolaemic hyponatraemia. It presents with concentrated urine (above 100 mOsm per kg), a urine sodium above 40, a low uric acid, and no oedema or dehydration. Causes in children include meningitis, pneumonia (especially respiratory syncytial virus), pain, nausea, the postoperative state, and drugs (vincristine, SSRIs, carbamazepine, cyclophosphamide, desmopressin). Management is fluid restriction (60 to 80 percent of maintenance), oral urea or salt, and treatment of the cause; severe symptomatic disease still needs 3 percent saline first. [3] [5]
Diabetes insipidus is the hypernatraemia of water loss. Central DI is a deficiency of ADH from head injury, CNS tumour, pituitary surgery, septo-optic dysplasia, or an inherited defect; it presents with polyuria, polydipsia, and dilute urine despite hypernatraemia, and it responds to desmopressin. Nephrogenic DI is renal resistance to ADH, from lithium, hypercalcaemia, hypokalaemia, or an inherited AVPR2 or AQP2 defect; it does not respond to desmopressin and is managed with solute reduction, adequate water, and thiazide or indometacin (which paradoxically reduce urine output by inducing mild volume depletion). Any child with DI who loses access to water — an infant, an unconscious child, a child with impaired thirst — can develop lethal hypernatraemia within hours. [2] [5]
Cerebral salt wasting is the hyponatraemia that is managed by the opposite of SIAD. It is a true hypovolaemic state from renal salt loss, seen after neurosurgery, traumatic brain injury, meningitis, and subarachnoid haemorrhage. The urine sodium is high, the volume is depleted, and the treatment is saline and salt replacement — fluid restriction, the treatment of SIAD, would worsen it. The distinction from SIAD rests on the volume status and the response to volume. [3] [5]
Breastfeeding-associated hypernatraemia presents in the first week of life in a poorly feeding neonate. The infant shows weight loss over 10 percent, lethargy, poor feeding, jaundice, and a serum sodium above 150. The danger is twofold: the acute dehydration itself, and the risk of cerebral oedema if corrected too rapidly. Correction is oral or intravenous free water over 48 hours at the standard rate limit, with close neurological monitoring. The prevention is early feeding assessment and weight monitoring in the first week. [2] [10]
Complications & Pitfalls
The cardinal pitfall in hyponatraemia is correcting too fast. Osmotic demyelination syndrome (central pontine myelinolysis) is a devastating quadriparesis, pseudobulbar palsy, seizure, and sometimes a locked-in state that appears days after an over-rapid correction of chronic hyponatraemia. The mechanism is the stripping of protective brain osmoles faster than the brain can reacquire them, causing cellular dehydration and demyelination. The risk factors that lower the safe ceiling are chronicity, malnutrition, alcoholism, liver disease, hypokalaemia, and burns — in these, aim for the lower end of the correction range. If you over-correct, the rescue is to lower the sodium back down with desmopressin and free water or 5 percent dextrose, re-establishing a controlled fall. [5] [6]
The mirror-image pitfall in hypernatraemia is correcting too fast, which causes cerebral oedema. Because the brain has generated idiogenic osmoles to protect itself against the chronic hypernatraemia, rapid correction floods the adapted cells with water, the brain swells inside the rigid skull, and seizure, herniation, and death follow. This is why the 0.5 mmol per litre per hour ceiling is absolute. The infant brain is at particular risk, and the neonate with hypernatraemia needs especially careful, slow correction. [2] [10]
The third pitfall is failing to treat the symptomatic brain for fear of the asymptomatic complication. Ayus and Moritz have documented that the fear of osmotic demyelination has caused clinicians to withhold 3 percent saline from children with active cerebral oedema, leading to preventable herniation and death. The 3 percent saline bolus is self-limiting (a 2 mL per kg bolus gives a measured 2 to 4 mmol/L rise), and the risk of ODS is from sustained over-correction, not a single bolus given to a seizing child. When the brain is in danger, treat it; when it is safe, correct slowly. [11] [6]
Prognosis & Disposition
Prognosis in dysnatraemia is governed by four things: the severity and acuity of the level, the presence of neurological symptoms, the reversibility of the cause, and — above all — the rate of correction. A child whose sodium has fallen from 140 to 118 over hours is at far greater risk than one who lives chronically at 125, because the acute brain has not adapted. Mortality in severe symptomatic hyponatraemia is driven by cerebral herniation, which is why early 3 percent saline is the highest-yield intervention; the major iatrogenic harm is osmotic demyelination from over-correction. [5] [11]
Admit to a high-dependency or intensive care setting any child with severe symptomatic hyponatraemia needing 3 percent saline, hypernatraemia with seizure or shock, a child undergoing active rapid correction with frequent sodium checks, and any child needing desmopressin or dialysis. The stable child, after correction, goes to the ward with serial monitoring while the cause is addressed. On discharge, identify and treat the cause, ensure isotonic maintenance fluid is prescribed if fluids are needed, arrange follow-up electrolytes, and for chronic causes (diabetes insipidus, an inherited tubulopathy, adrenal insufficiency) set up the long-term regimen. Give the family a clear safety-net: the warning signs (seizure, drowsiness, poor feeding, excessive thirst or urination), the importance of medication adherence, and when to return. [3] [2]
Special Populations
Neonates are a law unto themselves. The glomerular filtration rate is low, the concentrating and diluting ability is immature, and the body-water fraction is large. Breastfeeding-associated hypernatraemia in the first week is a recognised and dangerous entity, and hospital-acquired hyponatraemia from hypotonic fluid is a constant risk. All sodium therapy in neonates is weight-based, with the correction rate applied per kilogram and close neurological monitoring throughout, because the immature brain is especially vulnerable to both cerebral oedema and osmotic demyelination. [2] [10]
Postoperative children run the highest risk of hospital-acquired hyponatraemia. The surgical stress, pain, and nausea drive non-osmotic ADH, and if hypotonic fluid is given, the sodium falls — sometimes to seizure within hours. The prevention is the evidence-based default of isotonic maintenance fluid for all postoperative children, and the treatment is to stop the hypotonic fluid and switch to isotonic. This single policy is among the most important safety interventions in paediatric inpatient care. [7] [8]
Children with cerebral salt wasting after neurosurgery or head injury need saline and volume rather than fluid restriction. The key is to recognise the hypovolaemia and treat it, distinguishing it from SIAD (which is fluid-restricted). These children may need substantial salt and water replacement for days, with monitoring of the sodium and the volume status. [3] [5]
Children with diabetes insipidus need individualised management: desmopressin for central DI, solute reduction and thiazide or indometacin for nephrogenic DI, and careful water balance during intercurrent illness. A MedicAlert, a school plan, and clear guidance for emergencies are essential, because a child with DI who loses access to water can become critically hypernatraemic within hours. Transition to adult endocrinology or nephrology care is part of the long-term plan. [2] [5]
Evidence, Guidelines & Regional Differences
The evidence base for sodium disorders in children has shifted decisively over two decades, and the shift has changed practice. The Adrogue and Madias NEJM reviews of 2000 remain the foundational pathophysiology, framing sodium as a water-balance problem governed by total body water relative to sodium. The Spasovski European clinical practice guideline of 2014 and the Verbalis expert panel of 2007 systematised the correction-rate ceilings, the 3 percent saline recommendation for symptomatic disease, and the cause-specific therapy. The Sterns 2015 NEJM review and the Rondon-Berrios and Sterns 2022 hypertonic saline review synthesised the modern approach, with particular attention to avoiding over-correction and managing it with desmopressin if it occurs. [1] [5] [6]
The paediatric maintenance-fluid evidence is the clearest win. Moritz and Ayus argued that non-osmotic ADH is near-universal in sick children, making hypotonic fluid dangerous; the McNab JAMA trial and the Padua and later systematic reviews then proved that isotonic maintenance fluid prevents hyponatraemia without increasing hypernatraemia or fluid overload. This evidence underpins the now-standard default of isotonic fluid for hospitalised children across ANZ, the UK, and North America. [7] [8] [9]
The most contested evidence concerns hypertonic saline in symptomatic hyponatraemic encephalopathy. Ayus and Moritz, in their 2019 barriers review, documented that the fear of osmotic demyelination has led to the under-use of 3 percent saline, with more deaths from untreated cerebral herniation than from ODS. The argument is that a measured bolus (2 mL per kg, raising the sodium by 2 to 4 mmol/L) is safe and life-saving, and that the risk of ODS comes from sustained over-correction, not a single bolus in a seizing child. This has driven a move toward earlier, more confident use of 3 percent saline in paediatric and emergency protocols. [11] [6]
The Spasovski European guideline (PMID 24569496) and the Verbalis expert panel (PMID 17981159) provide the international consensus on hyponatraemia correction. ANZ resuscitation and RCPCH/NICE paediatric pathways, the American Academy of Pediatrics maintenance-fluid guidance, and the KDIGO water-and-sodium discourse give broadly concordant correction-rate ceilings and 3 percent saline conventions but differ in detail (for example the exact bolus maximum and the preferred isotonic fluid). Always confirm the local paediatric protocol before prescribing, and document the guideline you are following. [3] [4]
The evidence is weakest in three places: the exact safe correction ceiling in small children and neonates (where the physiological extrapolation is strongest and the trial data thinnest), the role of desmopressin to clamp the sodium during active correction, and the optimal fluid and rate for neonatal hypernatraemia correction. The Didsbury paediatric hypernatraemia paper of 2023 found that real-world correction in children is often slower and more variable than guidelines suggest, and that the evidence for the 0.5 mmol per litre per hour limit is largely physiological rather than from paediatric trials. These remain areas for specialist nephrology and intensive-care discussion. [10] [5]
Exam Pearls
Memorise the sodium-as-water principle first, because every question flows from it. Sodium is a concentration, and the serum level moves because of water: hyponatraemia means relative water excess, hypernatraemia means relative water deficit. This is why oedematous states have hyponatraemia with excess total-body sodium, and why diabetes insipidus has hypernatraemia with normal or low total-body sodium. Get this right and the classification, the investigation, and the management all fall into place. [1] [2]
The correction-rate mnemonic is examiner gold. Hyponatraemia: correct no more than 8 mmol/L in 24 hours to avoid osmotic demyelination. Hypernatraemia: correct no more than 0.5 mmol/L per hour, or 10 to 12 mmol/L in 24 hours, to avoid cerebral oedema. Know both ceilings and know why they exist — the brain that has adapted cannot follow a fast correction. For symptomatic hyponatraemia, the exception is the 3 percent saline bolus: 2 mL per kg over 10 minutes, repeated up to three times, for a 4 to 6 mmol/L rise or seizure control. [5] [6]
The hospital-acquired hyponatraemia answer is isotonic maintenance fluid. A sick child releases non-osmotic ADH, and hypotonic fluid drives the sodium down; the McNab trial proved that isotonic fluid is safer and is now the default. This is one of the most reliable single-right-answer stems in paediatric fluids. [7] [8]
Finally, the SIAD-versus-cerebral-salt-wasting distinction. Both show concentrated urine with a high sodium and a low uric acid. SIAD is euvolaemic and fluid-restricted; cerebral salt wasting is hypovolaemic and salt- and volume-replaced. Fluid-restricting a child with cerebral salt wasting would worsen them — the volume status is the tie-breaker. Add that central DI responds to desmopressin and nephrogenic DI does not, and you have answered the spine of every sodium viva. [3] [5]
References
- [1]Adrogué HJ; Madias NE Hyponatremia. N Engl J Med, 2000.PMID 10824078
- [2]Adrogué HJ; Madias NE Hypernatremia. N Engl J Med, 2000.PMID 10816188
- [3]Spasovski G; Vanholder R; Allolio B; et al Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol Dial Transplant, 2014.PMID 24569496
- [4]Verbalis JG; Goldsmith SR; Greenberg A; et al Hyponatremia treatment guidelines 2007: expert panel recommendations. Am J Med, 2007.PMID 17981159
- [5]Sterns RH Disorders of plasma sodium--causes, consequences, and correction. N Engl J Med, 2015.PMID 25551526
- [6]Rondon-Berrios H; Sterns RH Hypertonic Saline for Hyponatremia: Meeting Goals and Avoiding Harm. Am J Kidney Dis, 2022.PMID 34508830
- [7]Moritz ML; Ayus JC Hyponatraemia: Isotonic fluids prevent hospital-acquired hyponatraemia. Nat Rev Nephrol, 2015.PMID 25599620
- [8]McNab S Isotonic vs Hypotonic Intravenous Fluids for Hospitalized Children. JAMA, 2015.PMID 26284724
- [9]Padua AP; Macaraya JR; Dans LF; et al Isotonic versus hypotonic saline solution for maintenance intravenous fluid therapy in children: a systematic review. Pediatr Nephrol, 2015.PMID 25576065
- [10]Didsbury M; See EJ; Cheng DR; et al Correcting Hypernatremia in Children. Clin J Am Soc Nephrol, 2023.PMID 36888887
- [11]Ayus JC; Moritz ML Misconceptions and Barriers to the Use of Hypertonic Saline to Treat Hyponatremic Encephalopathy. Front Med (Lausanne), 2019.PMID 30931308