Paeds · nephrology-urology-fluids-and-electrolytes
Kidney replacement therapy and dialysis in children
Also known as Renal replacement therapy · KRT · Peritoneal dialysis · Haemodialysis · Continuous renal replacement therapy · CRRT
Fellowship guide to kidney replacement therapy in children: the four modalities of peritoneal dialysis, haemodialysis, continuous renal replacement therapy, and kidney transplantation; the AEIOU indications for urgent dialysis in acute kidney injury; why peritoneal dialysis is preferred in infants and small children while continuous renal replacement therapy suits the haemodynamically unstable child in intensive care; and why transplantation remains the gold standard for end-stage kidney disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler in septic shock who has not passed urine for a day, whose potassium is climbing and whose chest is filling with fluid, cannot wait for his kidneys to recover. He needs kidney replacement therapy, the umbrella term for any treatment that takes over the work of the failing kidney by removing solute waste and excess water, and by correcting acid-base and electrolyte disturbance. The therapy does not heal the kidney. It buys time, either for the kidney to recover in acute kidney injury or for transplantation in end-stage kidney disease, and the choice of how to deliver it is one of the most consequential decisions in paediatric nephrology and intensive care. [12]
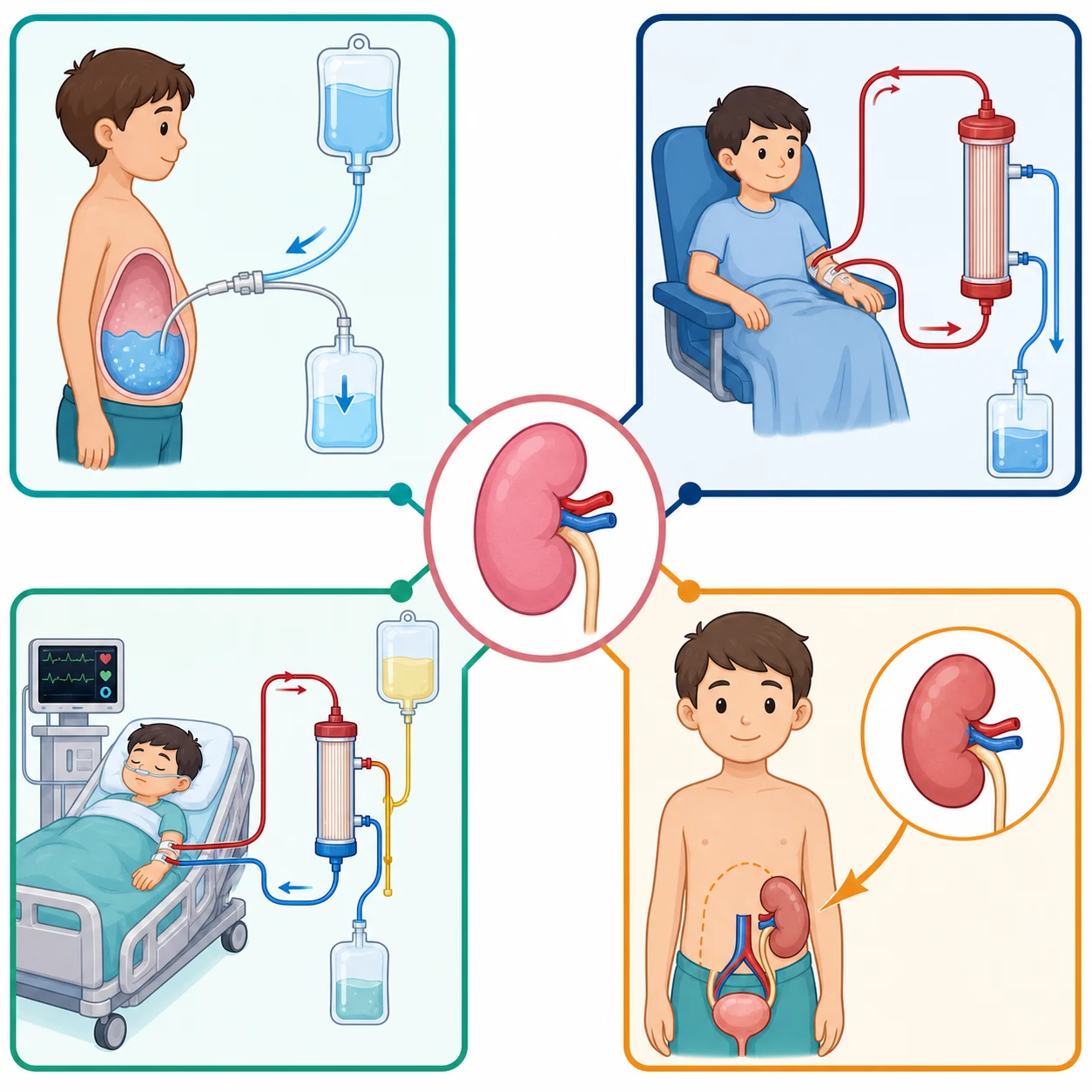
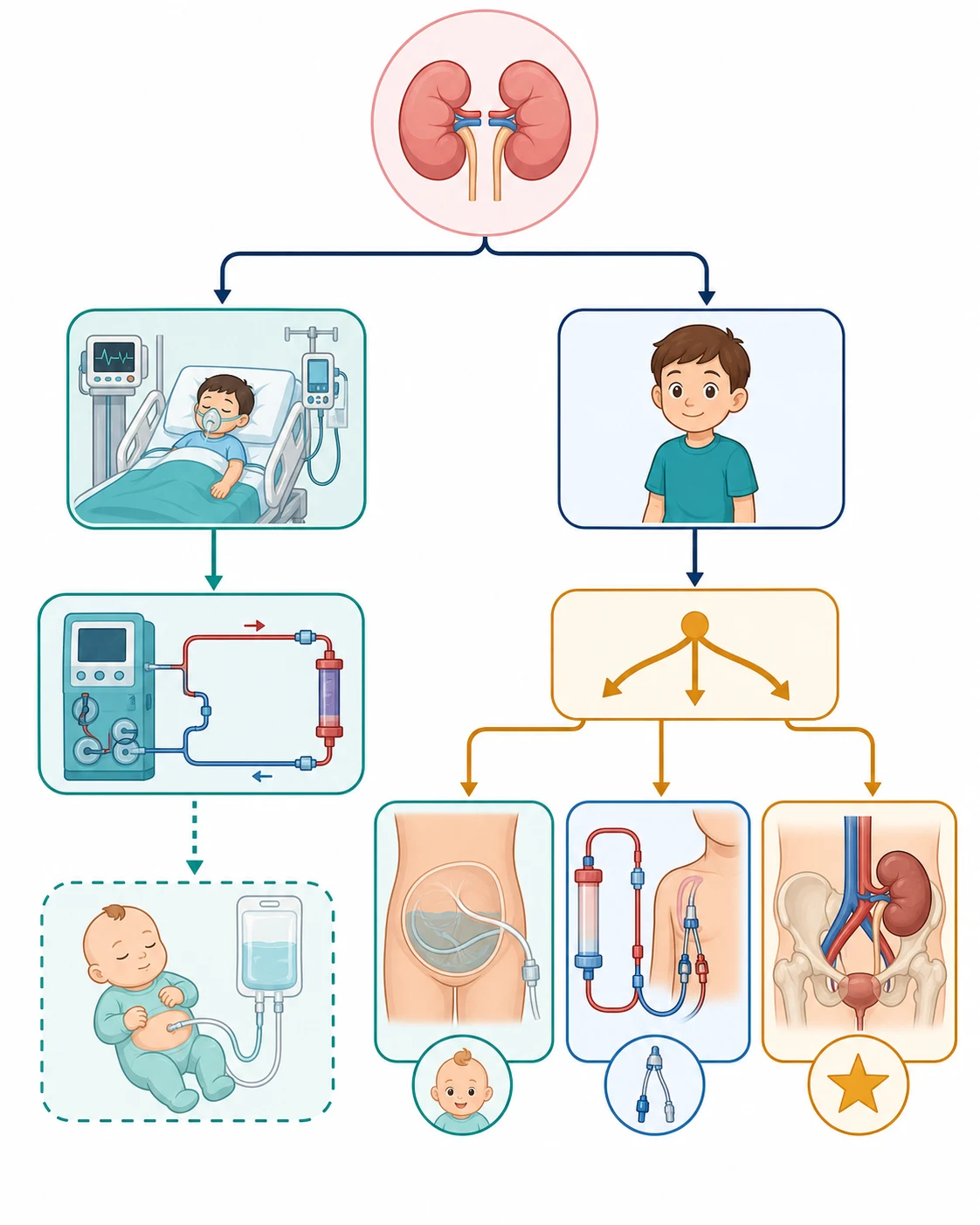
There are four ways to deliver kidney replacement therapy, and the differences between them are practical rather than philosophical. Peritoneal dialysis uses the lining of the child's own abdomen as the filter. Haemodialysis pumps blood through an artificial membrane in a machine and is fast and efficient but demands stable blood pressure and reliable vascular access. Continuous renal replacement therapy is a slower, gentler version of the blood circuit run continuously at the bedside for the child too unstable to tolerate intermittent haemodialysis. Kidney transplantation replaces the failing organ with a working one and is the definitive treatment for end-stage kidney disease, offering the best survival and quality of life. [5]
Classification
Classification matters because it drives the practical decision of which therapy to start. The first split is between therapy delivered across a membrane inside the child's body and therapy that takes blood out to an external filter. Peritoneal dialysis belongs to the first group: dialysate fluid is instilled into the peritoneal cavity, solutes and water move across the peritoneal membrane over hours of dwell, and the spent fluid is drained. Haemodialysis and continuous renal replacement therapy belong to the second group, both using an extracorporeal circuit and an artificial haemofilter, differing mainly in tempo and intensity. Transplantation is a separate category, an organ replacement rather than a filtration substitute. [12]
[1]Within peritoneal dialysis the prescription varies by technique. Continuous ambulatory peritoneal dialysis uses manual exchanges of dialysate through the day. Automated peritoneal dialysis, also called continuous cycling peritoneal dialysis, uses a machine to perform exchanges overnight while the child sleeps, which suits school-age children and gives them daytime freedom. Within continuous renal replacement therapy the modes differ by how clearance is generated: continuous venovenous haemofiltration removes solute by convection, continuous venovenous haemodialysis by diffusion, and continuous venovenous haemodiafiltration combines both. The choice between these continuous modes rarely changes outcome, so practice follows local expertise and the child's solute and fluid targets. [12]
Epidemiology & Risk Factors
The need for kidney replacement therapy in children divides into two populations with very different epidemiology. In the acute setting the trigger is severe acute kidney injury in critical illness, and this is far more common than once believed. The AWARE study by Kaddourah and colleagues found that acute kidney injury developed in nearly 27 percent of critically ill children within the first week of admission, and severe acute kidney injury in roughly 12 percent, though only a minority progress to the point of needing dialysis. The children who do need it are typically those with septic shock, multi-organ failure, post-cardiac surgery low cardiac output, or exposure to nephrotoxic drugs. [8]
The chronic dialysis population is smaller but lifelong in its demands. The incidence of end-stage kidney disease in children is approximately 5 to 10 per million children per year, with congenital anomalies of the kidney and urinary tract and hereditary nephropathies dominating in infants and young children, and glomerular diseases rising in older children and adolescents. Infants and very young children make up a disproportionate share of those starting chronic dialysis, and they carry the highest mortality, because their small size, comorbidity, and fragile cardiovascular and nutritional reserve amplify every complication of treatment. [6]
Several factors shape the risk of needing dialysis and the risk of doing badly on it. Young age, low body weight, and dependence on a central venous catheter rather than a fistula for haemodialysis access all predict poorer survival. Underlying multisystem disease, severe growth failure, and anaemia worsen long-term outcomes. For peritoneal dialysis, recurrent peritonitis and membrane failure over time threaten technique survival. Socioeconomic factors matter too, because home-based peritoneal dialysis depends on a reliable home environment, trained caregivers, and a clean water and storage supply that not all families can provide. [5]
Pathophysiology
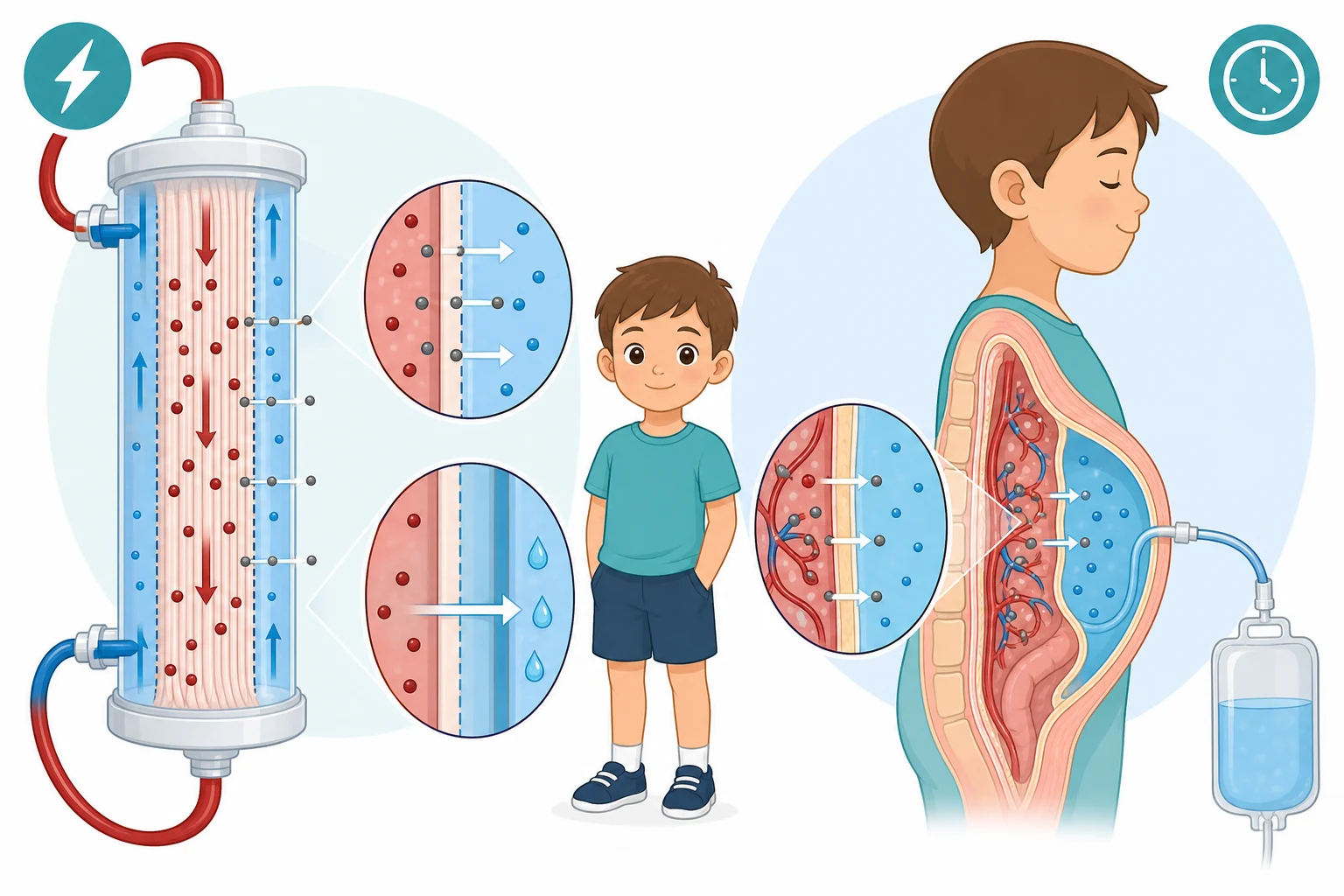
Every form of dialysis rests on the same physical principles operating across a semipermeable membrane. Solutes move by diffusion down their concentration gradient, so urea and potassium leave the blood where they are concentrated and enter the dialysate where they are absent. Water moves by ultrafiltration in response to a pressure or osmotic gradient, which is how excess fluid is removed. Larger solutes can also be dragged along with the water by convection, the mechanism that dominates in haemofiltration. The membrane, whether the artificial hollow fibres of a dialyser or the child's own peritoneum, holds back cells and large proteins while letting small molecules and water pass. [12]
The two main membranes behave differently and this shapes modality choice. The peritoneal membrane is a living capillary network with a large surface area roughly equal to body surface area, and it works slowly and gently over long dwells driven by a glucose osmotic gradient in the dialysate. An artificial haemofilter has a fixed surface area and works fast, clearing solute and water in hours rather than days, but it demands heparin anticoagulation and a blood pump that the smallest or most unstable children tolerate poorly. Understanding this trade-off between gentle slow clearance and rapid efficient clearance is the key to choosing the right therapy. [7]
AEIOU
The indications for urgent dialysis are remembered as AEIOU, and they map directly onto the pathophysiology. Refractory acidosis and hyperkalaemia reflect failure of the kidney's excretory and buffering roles that dialysis can restore. Intoxications with dialysable toxins such as salicylates, lithium, toxic alcohols, and metformin exploit diffusion to pull the drug out of the blood. Fluid overload that overwhelms the heart and lungs needs ultrafiltration. Uraemic complications threaten the pericardium and the brain and demand solute clearance. These five indications apply equally to children and adults, but the thresholds at which they trigger dialysis are lower and more fluid in children because the small child decompensates quickly. [8]
Clinical Presentation
A child who needs dialysis rarely presents with a single clear symptom. The picture is usually a deteriorating critically ill child in whom fluid, electrolyte, and acid-base problems are accumulating faster than the kidney can manage them. In acute kidney injury the signs are oliguria or anuria despite adequate fluid resuscitation, a rising creatinine, and the downstream consequences of failure to excrete: peripheral and pulmonary oedema from salt and water retention, a rising potassium with peaked T waves on the electrocardiogram, a worsening metabolic acidosis, and a falling conscious level from uraemia or from the hyponatraemia of fluid overload. [9]
The tempo is everything. A child who is haemodynamically stable with slowly progressive uraemia may tolerate planned haemodialysis in a dialysis unit, but a child in septic shock on multiple vasopressors with anuric fluid overload and worsening oxygenation needs gentle continuous removal at the bedside. A neonate with hyperammonaemia from a urea cycle disorder needs urgent clearance of ammonia before the brain is irreversibly injured. A child on chronic peritoneal dialysis who presents with cloudy effluent and abdominal pain has peritonitis until proven otherwise. Each presentation points to a different modality, and recognising the pattern is what drives the decision. [1]
Differential Diagnosis
Before committing a child to dialysis the clinician must distinguish genuine need from a reversible problem that will resolve with medical management. The first question is whether the acute kidney injury has a correctable prerenal or postrenal cause. A child who is simply volume-depleted from gastroenteritis may have oliguria and a rising creatinine that resolves with fluid resuscitation, and this reversible prerenal state should never be dialysed in haste. A child with obstructive uropathy may have postrenal failure that resolves once a catheter or nephrostomy drains the obstruction. These causes must be sought and treated before dialysis is considered. [9]
The second question is whether the child truly needs dialysis or only needs supportive care for a self-limiting injury. A single electrolyte disturbance, such as hyperkalaemia that responds to calcium, insulin-dextrose, and salbutamol, does not by itself mandate dialysis if the underlying kidney is expected to recover. The decision rests on whether the problems are refractory, accumulating, or accompanied by end-organ effects such as pericardial rub, uraemic seizures, or pulmonary oedema. When the disturbances are refractory and progressive, the differential collapses into the AEIOU indications and dialysis becomes the answer regardless of cause. [8]
In the chronic setting the differential is between end-stage kidney disease needing renal replacement and advanced chronic kidney disease that may be managed medically for a time. Children are often dialysed at a higher glomerular filtration rate than adults because growth failure, poor nutrition, and fluid overload appear early and respond poorly to conservative care. The decision to initiate chronic dialysis is therefore guided less by a single threshold number and more by the child's growth, metabolic control, and symptoms, with the goal of optimising the child for eventual transplantation. [5]
Clinical & Bedside Assessment
Assessment runs in parallel with resuscitation and targets three questions: does the child need dialysis now, which modality is feasible, and what access is available. The history establishes the cause and tempo of kidney failure, the premorbid baseline, and any prior dialysis or transplant. Recent surgery, sepsis, nephrotoxic drugs, and cardiac output states point toward acute kidney injury, while a known chronic kidney disease history, poor growth, and long-standing hypertension point toward end-stage disease. A careful fluid history, including all inputs and outputs and recent weights, is essential because volume status determines both the indication for dialysis and the safety of any chosen modality. [8]
Examination focuses on volume status and haemodynamics, the two determinants of modality. Tachycardia, cold peripheries, a narrow pulse pressure, and a rising lactate signal shock and instability that rule out intermittent haemodialysis in favour of a continuous therapy. Crackles, a gallop rhythm, hepatomegaly, and oxygen dependence signal fluid overload that needs ultrafiltration. Blood pressure may be high from volume overload or low from vasodilatory shock, and the trend matters more than any single reading. The abdomen is examined for any reason peritoneal dialysis might be unsuitable, such as recent abdominal surgery, a ostomy, hernia, or intra-abdominal infection. [9]
Vascular access assessment is practical and immediate. For urgent haemodialysis or continuous therapy the clinician looks for a usable central line, favouring the right internal jugular vein, and avoids subclavian lines wherever possible because they stenose the veins needed for a future fistula. For peritoneal dialysis the question is whether a Tenckhoff catheter can be placed, which depends on abdominal integrity and surgical availability. The child's size matters at every step: a two-kilogram neonate has different access options, blood prime needs, and anticoagulation risks than a fifty-kilogram adolescent, and the plan must be built around the individual child in front of you. [12]
Investigations
Investigations serve to confirm the need for dialysis, guide the prescription, and monitor the course. Blood tests quantify the uraemic and metabolic load: urea, creatinine, electrolytes, bicarbonate, calcium, phosphate, and magnesium. A rapidly rising urea above 35 to 40 mmol per litre raises the risk of dialysis disequilibrium if cleared too quickly, and a very high potassium with electrocardiogram changes is an emergency. Arterial or venous blood gas confirms the severity of metabolic acidosis and estimates the anion gap. In suspected intoxication the specific drug level, such as salicylate, lithium, ethylene glycol, or methanol, confirms the indication and the dialysability. [8]
For chronic dialysis, monitoring focuses on adequacy, nutrition, and the complications of long-term treatment. Dialysis adequacy in peritoneal dialysis is measured by the weekly Kt over V for urea and by the peritoneal equilibration test, which characterises the membrane as low, low-average, high-average, or high transporter and shapes the dwell prescription. Haemodialysis adequacy is judged by the single-pool Kt over V per session, targeted at around 1.2, and by achieving the estimated dry weight without symptomatic hypotension. Growth parameters, dietary intake, serum albumin, haemoglobin, iron stores, calcium, phosphate, parathyroid hormone, and bone mineral density are tracked at intervals because chronic dialysis is as much a nutritional and metabolic treatment as a filtration one. [7]
Imaging supports both planning and complication hunting. Renal ultrasound defines the size and structure of the native kidneys and may reveal obstruction that changes the plan. Echocardiography is essential in chronic dialysis because left ventricular hypertrophy and dysfunction are common and predict mortality. For peritoneal dialysis a plain abdominal film can confirm catheter position. When vascular access is being planned for chronic haemodialysis, vessel mapping by ultrasound guides creation of an arteriovenous fistula and avoids iatrogenic injury to future access sites. [11]
Management — Resuscitation
Resuscitation and the decision to start dialysis happen together, because the child needing dialysis is often the child in extremis. The airway and breathing are secured first, and circulatory access is established with at least one large-bore line. In a child with refractory hyperkalaemia, calcium gluconate is given to stabilise the myocardium while insulin-dextrose, salbutamol, and bicarbonate buy time by shifting potassium into cells, but these are bridges, not solutions, and definitive removal by dialysis follows. The aim is to support the child through the window in which dialysis is being prepared. [9]
Calcium gluconate 10 percent for hyperkalaemia
Dose
0.5 mL per kg slow intravenous push (max 20 mL), repeated as needed
The choice of urgent modality follows the child's haemodynamic state. The unstable child in the paediatric intensive care unit on vasopressors needs continuous renal replacement therapy, which removes fluid and solute gradually over hours to days and avoids the rapid shifts that would crash an already precarious circulation. The stable child with an intoxication or refractory electrolyte disturbance can tolerate intermittent haemodialysis, which clears solute fastest. Acute peritoneal dialysis is an excellent and often underused option for infants and small children, and it is the modality of choice in many resource-limited settings where the machinery and expertise for blood-based therapies are unavailable. [1]
Acute peritoneal dialysis is started with a temporary or Tenckhoff catheter and short dwells of 30 to 60 minutes, beginning with small fill volumes of around 300 to 500 mL per square metre in the first cycles and advancing as tolerated. It clears solute and removes fluid gently, tolerates low blood pressure well, and needs no anticoagulation, which is why the ISPD guidelines endorse it for paediatric acute kidney injury, including in neonates and after cardiac surgery. Its main limitations are lower efficiency than blood circuits in severe hypercatabolism, the risk of dialysate leak, and a learning curve for catheter placement and prescription. [2]
Continuous renal replacement therapy is delivered through a central venous circuit with a blood pump, a haemofilter, replacement or dialysate fluid, and anticoagulation. The effluent dose is typically targeted at 25 to 35 mL per kg per hour, balancing adequate clearance against the need to minimise filter clotting and the child's circulating volume. Anticoagulation is usually with heparin, but regional citrate anticoagulation is increasingly used because it avoids systemic heparin and lowers bleeding risk, though it requires careful monitoring of ionised calcium and total to ionised calcium ratio to avoid citrate accumulation, especially in liver failure. [12]
Management — Definitive & Stepwise
Definitive management is the long view, and it diverges sharply between the child who will recover and the child who has reached end-stage kidney disease. For acute kidney injury the goal is supportive dialysis until the kidney recovers, which may take days to weeks, with vigilance for the complications of critical illness. For end-stage kidney disease the goal shifts to maintaining health, growth, and quality of life while preparing for transplantation, because dialysis in children is fundamentally a bridge, not a destination. The modality chosen should fit the child, the family, and the local service, and it should be revisited as circumstances change. [5]
Decide acute versus chronic
Assess haemodynamic stability
Match modality to age and size
Plan vascular or peritoneal access
Set the prescription and monitor
The peritoneal dialysis prescription is built around dwell volume, dwell time, glucose concentration, and the number of cycles. Dwell volumes of 600 to 1100 mL per square metre are typical, beginning low and titrating to comfort and leak risk. Glucose-based dialysate provides the osmotic gradient for ultrafiltration, with higher dextrose concentrations used when more fluid removal is needed, and icodextrin reserved for the long overnight dwell to sustain ultrafiltration and spare glucose exposure. The peritoneal equilibration test personalises the prescription, because high transporters absorb glucose quickly and need shorter dwells while low transporters need longer dwells to reach adequacy. [7]
The haemodialysis prescription targets a single-pool Kt over V of around 1.2 over roughly three to four hours, three times weekly, with the blood flow rate and dialysate tailored to the child's size and access. Fluid removal is set to reach the estimated dry weight without symptomatic intradialytic hypotension, which is common in children and managed by slowing the ultrafiltration rate, using sodium profiling, and reviewing the dry weight. A reliable arteriovenous fistula is the preferred long-term access because it lasts longer and infects less than a catheter, consistent with the fistula-first principle, though catheters remain necessary in the acute setting and in small children too small for a fistula. [5]
Transplantation is the definitive therapy for end-stage kidney disease in children and should be planned from the moment chronic dialysis begins. Survival after transplantation is markedly better than on dialysis, growth and quality of life improve, and a preemptive transplant before dialysis is ever needed offers the best outcome of all. Living-related donation gives the best graft survival but must be approached carefully in inherited nephropathies so that the donor is not themselves at risk. Peritoneal dialysis and haemodialysis are both acceptable bridges to transplant, and the modality chosen should be the one that keeps the child healthiest while a graft is being arranged. [6]
Specific Subtypes & Scenarios
The infant on chronic peritoneal dialysis is one of the most challenging patients in paediatric nephrology. Congenital anomalies of the kidney and urinary tract and hereditary causes dominate, the child is small and fragile, and the margin for error in fluid, nutrition, and growth is narrow. Outcomes have improved over time, but infants still carry the highest mortality of any dialysis group, driven by infection, cardiovascular disease, and failure to thrive. The USRDS analysis by Sanderson and colleagues showed real gains in survival but persistent vulnerability, underscoring the need for specialist centres and aggressive nutritional support, often via gastrostomy, to deliver the calories these infants need to grow. [6]
The critically ill child on continuous renal replacement therapy in the paediatric intensive care unit represents the acute extreme. The typical patient has septic shock, post-cardiac surgery low cardiac output, or multi-organ failure, and cannot tolerate the rapid fluid shifts of intermittent haemodialysis. Continuous therapy removes fluid and solute gently over days, supports vasopressor weaning, and allows nutritional and blood product delivery without cumulative fluid overload. The trade-off is the demand on nursing and the need for anticoagulation, with filter clotting and circuit downtime the main practical obstacles. [12]
AWARE study of acute kidney injury in critically ill children
Key finding
In a prospective multicentre study of over 2000 critically ill children, acute kidney injury developed in about 27 percent within seven days and severe acute kidney injury in about 12 percent, and severe acute kidney injury was independently associated with higher mortality, supporting early recognition and timely kidney replacement therapy.
Practice change
Acute kidney injury is common and consequential in paediatric intensive care, and clinicians should anticipate the need for kidney replacement therapy early rather than waiting for biochemical or clinical collapse.
Intoxications and inborn errors of metabolism present a distinct scenario in which dialysis is not a bridge to recovery but a tool for rapid clearance of a specific molecule. Salicylates, lithium, toxic alcohols such as ethylene glycol and methanol, and metformin are removed efficiently by haemodialysis because they are small, water-soluble, and have a small volume of distribution. In inborn errors of metabolism such as urea cycle disorders, severe hyperammonaemia causes irreversible brain injury within hours, and emergency continuous therapy to clear ammonia is life-saving and neuroprotective when started before the ammonia peaks and the child sustains cerebral oedema. [10]
Complications & Pitfalls
Complications of dialysis span infection, haemodynamic instability, and the metabolic and vascular consequences of long-term treatment. Peritoneal dialysis-related peritonitis is the most frequent complication of chronic peritoneal dialysis and the leading reason for technique failure and catheter loss. It presents with cloudy effluent, abdominal pain, and fever, and the diagnosis rests on an effluent white cell count above 100 per microlitre after a dwell, with a positive culture in most cases. Empirical intraperitoneal antibiotic therapy covering gram-positive and gram-negative organisms is started immediately after culture, then narrowed to the organism, guided by the ISPD recommendations and the 2024 paediatric update by Warady and colleagues. [3]
Haemodialysis and continuous therapy carry their own risks. Intradialytic hypotension is common in small children and is managed by slowing the ultrafiltration rate and reviewing the target weight. Central venous catheters infect and thrombose, threatening the only access, and catheter-related bloodstream infection is a recurring source of sepsis and morbidity. Heparin anticoagulation risks bleeding, while citrate risks hypocalcaemia and accumulation in liver failure. Long-term, the dominant problem is cardiovascular disease, which is the leading cause of death in children on dialysis, driven by hypertension, fluid overload, dyslipidaemia, and disordered calcium-phosphate metabolism that accelerates vascular calcification from an early age. [11]
The most dangerous pitfalls are those of timing and modality mismatch. Delaying dialysis in a child with refractory hyperkalaemia while waiting for medical therapy to work can cost the child their life. Conversely, choosing intermittent haemodialysis for an unstable child precipitates circulatory collapse. Clearing a very high urea too quickly causes dialysis disequilibrium. Using a subclavian line destroys the veins needed for a future fistula. Failing to recognise peritonitis early, or giving inadequate empirical cover, lets an infection destroy the peritoneal membrane. And neglecting nutrition and growth in the chronic dialysis child guarantees a poor long-term outcome even when the dialysis itself is technically adequate. [5]
Prognosis & Disposition
Prognosis in kidney replacement therapy depends on whether the kidney failure is acute or chronic, the age and comorbidity of the child, and the modality used. For acute kidney injury requiring dialysis, the outlook is tied to the underlying illness: children who recover do so over days to weeks, and the mortality is driven by the primary disease rather than the dialysis. For end-stage kidney disease, dialysis is a holding measure whose outcomes are inferior to transplantation in every domain, from survival to growth to quality of life, which is why transplantation is the goal. [5]
Severity
Reversible acute kidney injury
Temporary dialysis for a clearly reversible cause such as a toxin or a self-limiting injury. The kidney recovers, dialysis is withdrawn, and long-term outlook is good.
Severity
Stable end-stage kidney disease on dialysis
Child on maintenance peritoneal or haemodialysis awaiting transplant. Survival is reasonable but inferior to transplant, with attention to growth, nutrition, and cardiovascular risk.
Severity
Infant on dialysis or unstable child on CRRT
Highest-risk group. Infants carry the greatest mortality, and unstable children on continuous therapy depend on the primary illness. Needs specialist centre and early transplant planning.
The NAPRTCS registry analysis by Weaver and colleagues showed that survival for children initiating chronic dialysis is worse than for those transplanted and is markedly affected by age and access type, with younger children and those dialysing through a catheter faring worst. Infants, in particular, have substantially higher mortality in the first months of dialysis, often from infection and cardiovascular events, though survival has improved over successive eras with better catheter design, nutrition, and infection prevention. The long-term burden of cardiovascular disease persists, which is why blood pressure, fluid status, and calcium-phosphate balance are tracked so closely. [5]
Disposition follows severity. Any child needing acute dialysis belongs in a paediatric intensive care unit with nephrology support, and a child needing chronic dialysis belongs in a specialist paediatric nephrology centre with multidisciplinary input from dietitians, nurses, social workers, and surgeons. Transfer to a transplant centre should be arranged early. At the transition to adult care, the adolescent on dialysis or with a transplant needs a structured handover, because the shift to adult services is a well-recognised point of graft loss and dropout that good transition planning can prevent. [6]
Special Populations
Infants are the population that defines paediatric dialysis. They are technically the hardest to dialyse, the most vulnerable to complications, and the most dependent on nutrition for brain growth and development. Chronic peritoneal dialysis is the modality of choice for infants because it preserves veins, needs no needles, and fits a small body, but it demands a skilled family and intensive multidisciplinary support. The USRDS data confirm that while infant outcomes have improved, they remain the group at greatest risk, and every effort must be made to optimise nutrition, prevent infection, and progress toward transplantation as early as the child is large and well enough. [6]
Adolescents on dialysis face a different set of challenges centred on adherence, identity, and transition. Non-adherence with fluid restriction, medications, and the dialysis schedule is common in adolescence and directly threatens technique survival and graft survival after transplant. Chronic dialysis during adolescence disrupts school, friendships, and the normal developmental task of independence, and the move to adult care is a high-risk period for loss to follow-up and graft failure. Structured transition programmes that build self-management skills and provide a warm handover to adult services improve outcomes and should begin years before the actual transfer. [11]
In resource-limited and remote settings, peritoneal dialysis has a particular and life-saving role. It needs no expensive machine, no continuous power, and no specialised water treatment, and it can be delivered safely by trained staff in district hospitals. The ISPD guidelines for peritoneal dialysis in acute kidney injury were written partly for this context, because the choice is often between acute peritoneal dialysis and no dialysis at all. In Australia and New Zealand, where distances are vast and children may be hundreds of kilometres from a tertiary centre, acute peritoneal dialysis at the referring hospital can stabilise a child for safe retrieval, and home-based chronic peritoneal dialysis allows remote children to live at home rather than relocate to a city. [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric kidney replacement therapy is a mix of registry data, consensus guidelines, and expert recommendation, because randomised trials are scarce in this small and heterogeneous population. The International Society for Peritoneal Dialysis guidelines on peritoneal dialysis in acute kidney injury, published in 2020 with separate paediatric and adult documents, established peritoneal dialysis as a valid and sometimes preferred modality for paediatric acute kidney injury, especially in infants and resource-limited settings. The 2024 update of the paediatric peritoneal dialysis infection guideline by Warady and colleagues consolidated the prevention and management of peritonitis and exit-site infection, building on the 2016 ISPD peritonitis recommendations. [3]
For chronic dialysis, the NAPRTCS registry and the International Pediatric Peritoneal Dialuation Network generate the outcome and prescription data that underpin practice. The Warady and Schaefer guidance on prescribing peritoneal dialysis for high-quality care in children translates these data into concrete prescription targets for dwell volume, dwell time, and adequacy. The KDIGO acute kidney injury guideline provides the staging and management framework that surrounds the decision to dialyse, and the nomenclature work by Neri and colleagues brings order to the bewildering array of names for the continuous therapies. [4]
In Australia and New Zealand, paediatric kidney replacement therapy is coordinated through specialist paediatric nephrology centres in each state and the ANZDATA registry tracks dialysis and transplant outcomes. Peritoneal dialysis is the first-line chronic modality for infants and young children, with transplantation planned early and living donor transplant encouraged where appropriate. The vast geography means that acute peritoneal dialysis at peripheral hospitals and home-based chronic dialysis are essential to equitable care, and retrieval services support the safe transfer of the critically ill child who needs a blood-based therapy only a tertiary centre can provide. [5]
Regional differences are most visible in access to transplantation and in the resources for blood-based therapies. In high-income settings, transplantation is readily available and living donation is common, giving children the best chance of dialysis-free survival. In lower-resource settings, the machinery, consumables, and trained staff for haemodialysis and continuous therapy may be scarce, and peritoneal dialysis carries a disproportionate share of the burden of both acute and chronic care. The International Pediatric Nephrology Association works to standardise and support dialysis delivery globally, and the principles of modality selection, infection prevention, and adequacy are universal even when the tools differ. [2]
Exam Pearls
Kidney replacement therapy replaces the filtration, fluid-removal, and acid-base roles of the failing kidney through four modalities. Peritoneal dialysis uses the peritoneal membrane and is preferred in infants and small children and in resource-limited settings. Haemodialysis uses an artificial membrane and is fast but demands stability and access. Continuous renal replacement therapy is the gentle continuous blood circuit for the haemodynamically unstable child in intensive care. Transplantation is the definitive treatment for end-stage kidney disease and offers the best survival. The AEIOU mnemonic captures the indications for urgent dialysis: refractory acidosis, electrolyte disturbance, intoxication, fluid overload, and uraemic complications. [12]
Modality choice hinges on three questions: is the failure acute or chronic, is the child stable, and what is the child's size. The unstable critically ill child gets continuous renal replacement therapy, the infant gets peritoneal dialysis, and the older stable child can have haemodialysis or peritoneal dialysis as a bridge to transplant. The peritoneal dialysis prescription uses dwell volumes of 600 to 1100 mL per square metre, and the continuous therapy targets an effluent dose of 25 to 35 mL per kg per hour. Peritoneal dialysis peritonitis presents with cloudy effluent and is treated with empirical intraperitoneal antibiotics covering gram-positive and gram-negative organisms, guided by the 2024 paediatric ISPD update. [3]
References
- [1]Nourse P, Cullis B, McCulloch M, Dias C, McCulloch I, Numanoglu A, et al ISPD guidelines for peritoneal dialysis in acute kidney injury: 2020 Update (paediatrics). Perit Dial Int, 2021.PMID 33523772
- [2]Cullis B, Al-Hwiesh A, Kilonzo K, Ponce D, Govindarajan S, Neri M, et al ISPD guidelines for peritoneal dialysis in acute kidney injury: 2020 update (adults). Perit Dial Int, 2021.PMID 33267747
- [3]Warady BA, Same R, Hebert D, Alexander SR, Schaefer F, Yavin H, et al Clinical practice guideline for the prevention and management of peritoneal dialysis-associated infections in children: 2024 update. Perit Dial Int, 2024.PMID 39313225
- [4]Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, et al ISPD peritonitis recommendations: 2016 update on prevention and treatment. Perit Dial Int, 2016.PMID 27282851
- [5]Weaver DJ Jr, Somers MJG, Martz K, Mitsnefes MM Clinical outcomes and survival in pediatric patients initiating chronic dialysis: a report of the NAPRTCS registry. Pediatr Nephrol, 2017.PMID 28762101
- [6]Sanderson KR, Yu Y, Vaidya S, Selewski DT, Kallash M, Akchurin O, et al Outcomes of infants receiving chronic peritoneal dialysis: an analysis of the USRDS registry. Pediatr Nephrol, 2019.PMID 30141177
- [7]Warady BA, Schaefer F, Bagga A, Cano F, Hijazi R, Yavascan O, et al Prescribing peritoneal dialysis for high-quality care in children. Perit Dial Int, 2020.PMID 32063210
- [8]Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL, AWARE Investigators Epidemiology of acute kidney injury in critically ill children and young adults. N Engl J Med, 2017.PMID 27959707
- [9]Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int, 2007.PMID 17396113
- [10]Raina R, Chakraborty R, Rappa K, Sethi SK, Kumar D, Hamdan D, et al Dialysis disequilibrium syndrome (DDS) in pediatric patients on dialysis: systematic review and clinical practice recommendations. Pediatr Nephrol, 2022.PMID 34609583
- [11]Querfeld U, Schaefer F, Zeller F, Warady BA Cardiovascular risk factors in children on dialysis: an update. Pediatr Nephrol, 2020.PMID 30382333
- [12]Neri M, Villa G, Garzotto F, Bagshaw S, Bellomo R, Cerda J, et al Nomenclature for renal replacement therapy in acute kidney injury: basic principles. Crit Care, 2016.PMID 27719682