Paeds · nephrology-urology-fluids-and-electrolytes
Kidney transplantation in children
Also known as Paediatric renal transplantation · Kidney transplant in children · Preemptive kidney transplant · Living donor kidney transplant
Fellowship guide to paediatric kidney transplantation: why a transplanted kidney is the treatment of choice over lifelong dialysis for a child with end-stage kidney disease; the living-donor versus deceased-donor and preemptive versus dialysis-first classifications that predict graft survival; the standard tacrolimus, mycophenolate and steroid maintenance regimen with therapeutic drug monitoring; the distinction between T-cell-mediated and antibody-mediated rejection and how each is treated; and the leading threats to long-term graft survival including non-adherence in adolescence and chronic antibody-mediated rejection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child whose kidneys have failed has end-stage kidney disease, and the question becomes how to replace what the kidneys did. There are two ways: dialysis, which filters the blood by machine or through the abdomen, or a kidney transplant, in which a healthy kidney from a donor is surgically placed in the child's lower abdomen. A transplanted kidney is the treatment of choice for almost every child with end-stage kidney disease, because it does what dialysis cannot: it works continuously, frees the child from the machine, restores near-normal growth and development, and improves long-term survival. [1]
The new kidney does not replace the old ones. The child's own failed kidneys usually stay in place, and the donor kidney is placed in the iliac fossa, the lower abdomen, where its blood vessels are joined to the large pelvic vessels and its ureter is connected to the bladder. The operation is the easy part. The hard part, which dominates everything afterwards, is that the child's immune system sees the donor kidney as foreign and will attack and destroy it unless the child takes immunosuppressant medicines every single day for life. This balance, between protecting the graft and avoiding the infections and cancers that immunosuppression permits, is what paediatric transplant medicine is about. [2]
Classification
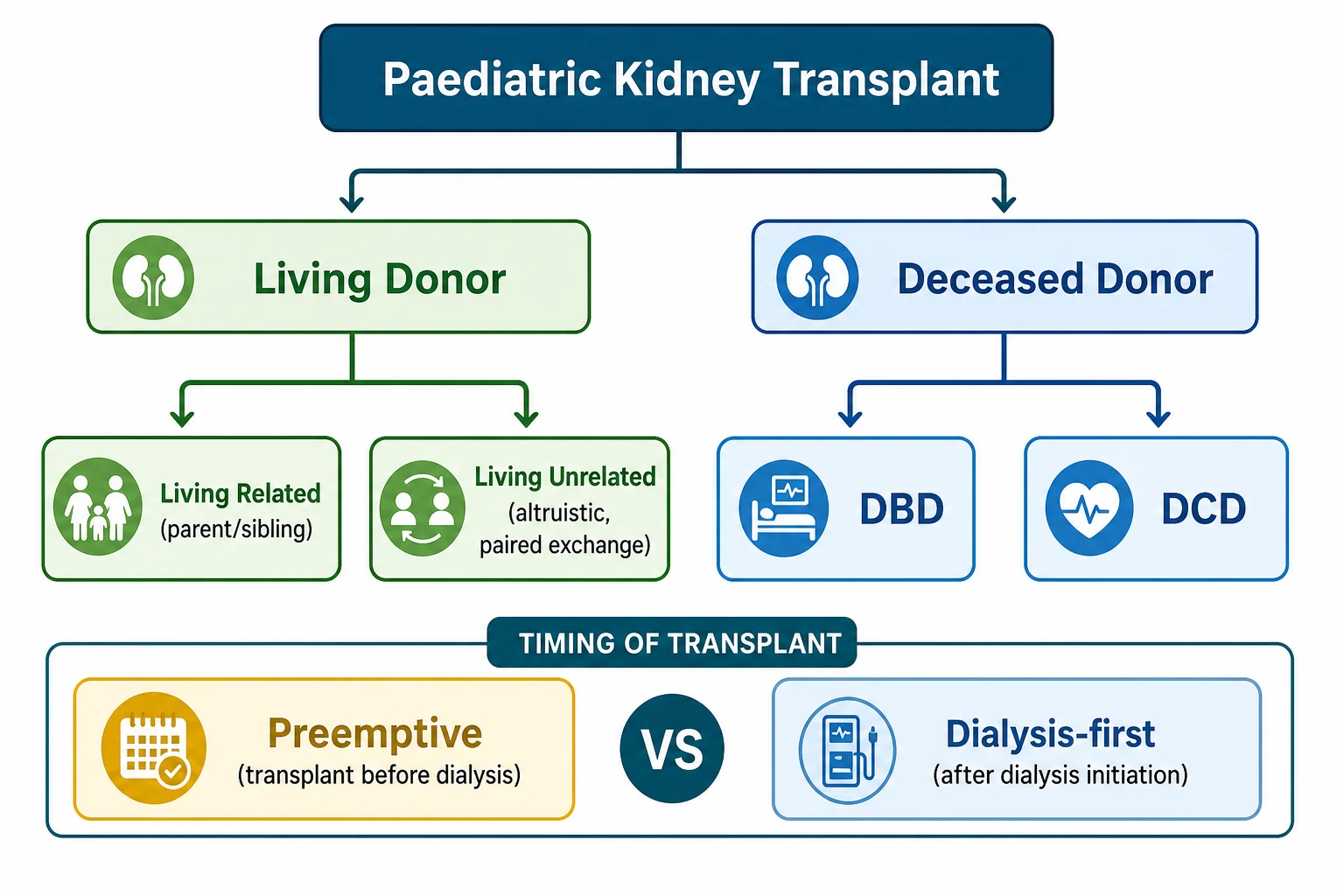
The reason classification matters is that two simple questions about the kidney a child receives predict how long that kidney will last: where did the kidney come from, and was the child already on dialysis when they received it. A kidney from a living donor, especially a parent, survives longer than one from a deceased donor, and a kidney placed before the child ever starts dialysis survives longer still. These are not minor differences; they are the dominant modifiable factors in paediatric graft survival, so every transplant assessment is built around optimising them. [3]
The first axis is donor source. A living donor is a healthy adult, usually the child's parent or an adult sibling, who donates one kidney and continues life with the remaining one. Living donation gives the best graft survival because the kidney is healthy, the surgery is planned, and the cold ischaemia time (the time the kidney spends out of the body between donor and recipient) is short. A deceased-donor kidney comes from a person who has died, either after brain death (donation after brain death, DBD) or after circulatory death (donation after circulatory death, DCD). Deceased-donor kidneys carry a higher risk of delayed graft function, where the kidney is slow to start working and dialysis is needed temporarily in the first week. [2]
[3]The second axis is timing, and this is where the concept of a preemptive transplant enters. A preemptive transplant means the child receives a kidney before they ever start dialysis. This is usually possible only when a living donor is available, because a deceased-donor kidney arrives unpredictably and the child is usually already on dialysis by then. Preemptive transplant matters because dialysis itself harms the child: it impairs growth, worsens neurodevelopment, damages blood vessels, and reduces long-term graft survival once the transplant finally happens. Every time dialysis can be avoided by timely living donation, the child benefits, which is why a child with progressive chronic kidney disease should be referred to a transplant centre and have a donor worked up early, before dialysis is needed. [2]
Epidemiology & Risk Factors
Kidney transplantation is far less common in children than in adults, but for the child who reaches end-stage kidney disease it is the single most important intervention available. The causes of kidney failure that bring a child to transplant are completely different from the causes in adults. In adults, diabetes and hypertension dominate. In children, the leading cause is structural: congenital anomalies of the kidney and urinary tract, a group that includes renal hypodysplasia, posterior urethral valves and obstructive uropathy, accounts for roughly 30 to 50 percent of paediatric transplants. [1]
After congenital causes, steroid-resistant nephrotic syndrome (usually focal segmental glomerulosclerosis) is the next most common indication, followed by inherited and metabolic diseases, reflux nephropathy, and the glomerulonephritides. In adolescents the pattern shifts toward acquired disease, with IgA nephropathy, lupus nephritis and other immune-mediated glomerular diseases becoming more prominent. Knowing the original disease matters because some diseases recur in the new kidney and change the prognosis and management, which is covered under recurrence below. [3]
Several factors predict whether a graft will survive well or fail. The strongest favourable factors are a living-donor kidney, a preemptive transplant, a good HLA match, and adherence to the immunosuppressant regimen. The strongest adverse factors are sensitisation (the child has many antibodies against donor tissue from previous transfusions, pregnancies in the mother, or a prior transplant), a high degree of HLA mismatch, delayed graft function, recurrence of the original disease, and non-adherence. Non-adherence, meaning the teenager who does not take their tablets, is the single most common cause of late graft loss in adolescents, which is why transition care is treated as a clinical priority rather than an administrative task. [12]
Pathophysiology
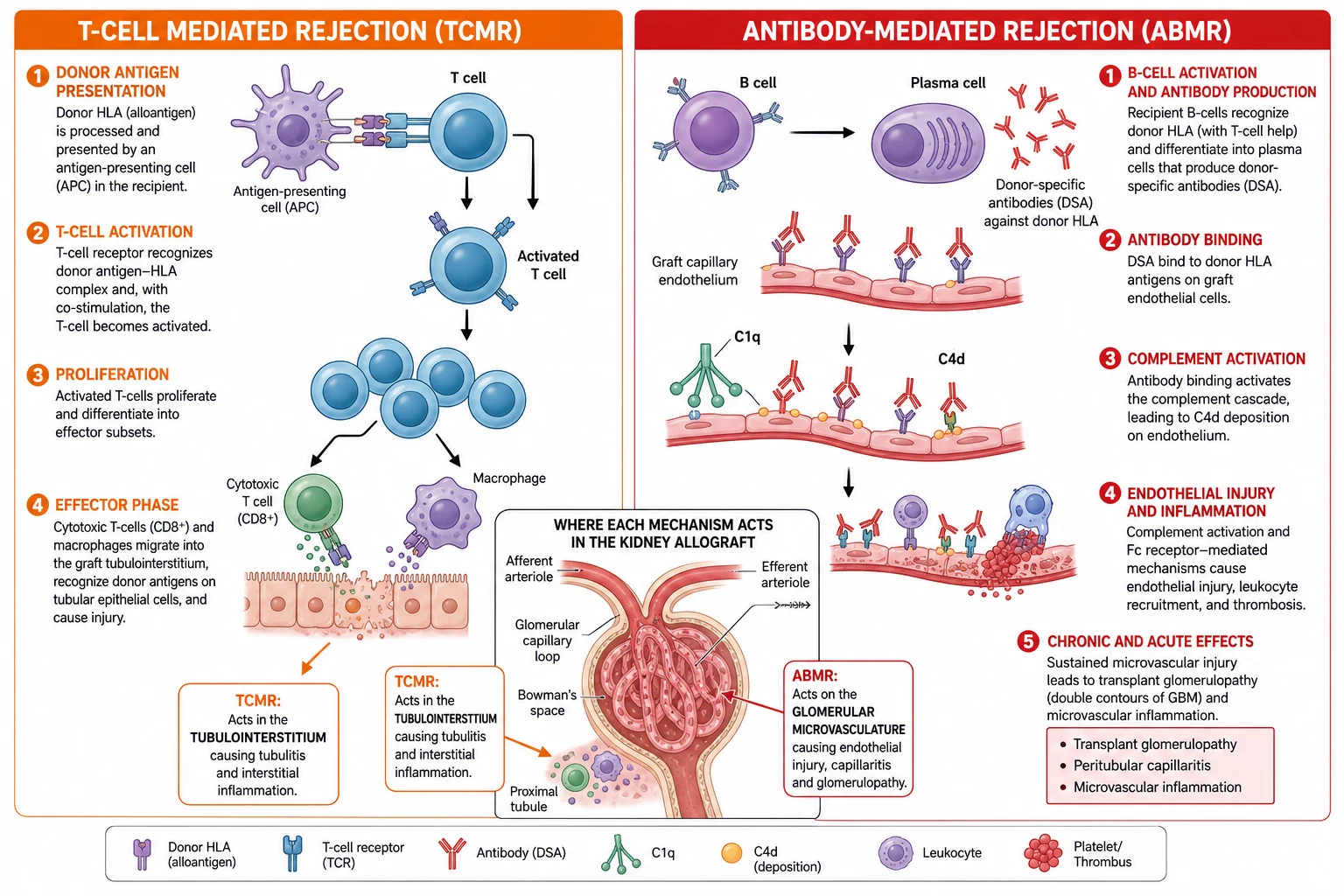
To understand rejection, picture the donor kidney as wearing a coat of badges. Those badges are the donor's human leukocyte antigen molecules, the tissue-type proteins that make each person's cells individually identifiable. The recipient's immune system inspects every cell it meets, and when it reads badges it does not recognise as self, it treats them as a threat. This recognition triggers one of two kinds of attack, and which attack occurs decides which treatment the child needs. [9]
The first attack is T-cell-mediated rejection. Recipient immune cells pick up fragments of donor tissue and show them to the recipient's T lymphocytes. With a second co-stimulatory signal, the T cells switch on, multiply, and turn into cytotoxic cells and inflammatory macrophages that storm into the graft. They invade the tubules and the walls of small arteries, causing tubulitis and intimal arteritis. This is the classic acute rejection of the first weeks and months after transplant. It responds well to steroids, which is why a creatinine rise in the early period is treated empirically with pulse methylprednisolone once infection and obstruction are excluded. [7]
The second attack is antibody-mediated rejection. Here the recipient's B lymphocytes, helped by T cells, mature into plasma cells that pour out donor-specific antibodies. These antibodies lock onto the donor HLA badges on the graft's capillary lining, switch on the complement cascade, and leave a tell-tale footprint called C4d in the peritubular capillaries. The result is microvascular inflammation, injury to the filtering surface, and over time a scarring pattern called transplant glomerulopathy that slowly chokes the graft. Antibody-mediated rejection is harder to treat, tends to be chronic, and is the leading cause of long-term graft loss. [9]
CIT
The maintenance drugs work by damping these two pathways at different points. Tacrolimus, a calcineurin inhibitor, blocks the T-cell activation step by preventing interleukin-2 transcription, so fewer T cells are switched on. Mycophenolate, an antimetabolite, stops lymphocytes multiplying. The corticosteroid dampens the broader inflammatory response. Understanding where each drug acts explains why all three are used together, and why removing or under-dosing any one of them reopens a pathway to rejection. [4]
Clinical Presentation
A child heading toward transplant shows the features of advanced chronic kidney disease: poor growth, fatigue, poor appetite, pallor from anaemia, bone deformity from renal osteodystrophy, and high blood pressure. If the child is on dialysis, the additional burden of restricted diet, intermittent treatment, and dialysis access (a fistula, line or peritoneal catheter) dominates the picture. The transplant is performed to lift all of this. [1]
After the transplant, the clinical picture shifts entirely to detecting complications, because a graft that is failing often does so silently. The child who was passing plenty of urine may pass less. The blood pressure may rise. The graft site may become tender. But the single most important sign of trouble is a rise in the serum creatinine, which is why creatinine is checked frequently after transplant and at every clinic visit for life. A creatinine rise is the alarm bell that triggers a search for the cause. [3]
The complications present in a recognisable timeline. In the first hours and days the threats are surgical: the renal artery or vein may thrombose and threaten the graft immediately, the ureter may leak or obstruct, and the kidney may be slow to wake up (delayed graft function) so that temporary dialysis is needed. Over the first weeks and months, acute rejection and opportunistic infection compete for attention. Beyond the first year, the slow burn of chronic antibody-mediated rejection, recurrence of the original disease, drug nephrotoxicity, and non-adherence in the teenager become the threats. [2]
Infection presents according to the organism and the timing, and this timeline is worth memorising. In the first month the infections are the same bacterial ones any surgical patient gets: wound, line and urinary infections. From one to six months, when the immunosuppression is at its peak, the opportunistic infections emerge: cytomegalovirus, BK virus, Epstein-Barr virus, and fungal infection. After six months the child faces ordinary community infections again. This timeline helps you guess the organism before the cultures return. [11]
Differential Diagnosis
When a transplanted child's creatinine rises, the question is never "is it rejection?" but "which of the five causes is it?" The five causes to work through every time are pre-renal (the graft is underperfused), intrinsic graft disease (acute tubular necrosis, rejection, drug toxicity, recurrence, or viral nephropathy), and post-renal (the urine is blocked). Going through them systematically prevents the common error of assuming every creatinine rise is rejection and treating it with steroids that may do harm. [3]
Acute tubular necrosis and delayed graft function are the commonest early cause, especially after a deceased-donor transplant with a long cold ischaemia time. The kidney is stunned rather than rejected, and it recovers with supportive care while dialysis bridges the gap. Calcineurin inhibitor nephrotoxicity is the great mimic of rejection: tacrolimus can injure the graft at the same time as it protects it. The tacrolimus trough level and the biopsy pattern separate the two, because treating toxicity means lowering the drug, while treating rejection means raising the immunosuppression. [8]
[9]Recurrence of the original disease is a transplant-specific differential that examiners test. Focal segmental glomerulosclerosis can recur within hours of transplant, presenting as sudden massive proteinuria, and is treated with plasmapheresis and rituximab. Primary hyperoxaluria recurs unless the child receives a combined liver-kidney transplant, because the liver is the source of the enzyme defect. Atypical haemolytic uraemic syndrome recurs aggressively and requires prophylactic eculizumab. Knowing whether the original disease can recur changes the pre-transplant plan. [9]
BK virus nephropathy deserves special mention because it is the infection that behaves like rejection. BK virus, which most people carry harmlessly, reactivates under immunosuppression and invades the graft tubules, causing inflammation and a rising creatinine that looks exactly like acute T-cell-mediated rejection on biopsy. The danger is treating presumed rejection with more immunosuppression, which feeds the virus. The discriminator is the BK viral load in the blood and the SV40 stain on biopsy, and the treatment is to reduce immunosuppression, not increase it. [11]
Clinical & Bedside Assessment
Assessment of graft dysfunction runs alongside investigation and targets the cause. The history is where most of the answer lies. Ask first about adherence, because a teenager who has stopped taking their tablets is the commonest reason for a late creatinine rise, and no test will show it if you do not ask. Ask about the timing and character of the creatinine rise, any dose changes or missed doses, whether the tacrolimus is being taken correctly (it must be taken on an empty stomach at consistent times), and any intercurrent illness, diarrhoea or dehydration. [12]
Ask about new medications, because tacrolimus is metabolised by the same liver enzyme pathway as many common drugs. Azole antifungals and macrolide antibiotics raise the tacrolimus level toward toxicity, while rifampicin, phenytoin and St John's wort lower it and precipitate rejection. A child prescribed one of these by a doctor unfamiliar with their transplant can lose the graft, so a full medication and supplement review is essential whenever the creatinine rises. [8]
Examination focuses on fluid status, blood pressure, and the graft. Volume depletion from vomiting or diarrhoea underperfuses the graft and raises creatinine, so look for the signs of dehydration. Hypertension suggests rejection or vascular compromise. Examine the graft site: a tender, swollen graft suggests rejection, infection or vascular thrombosis; a bruit suggests a vascular abnormality. Check the wound for a collection or leak, and look systematically for signs of infection. Daily weights and strict input-output charts are non-negotiable in the early post-transplant period, because a falling urine output is often the first sign of trouble. [1]
The synthesis is a problem representation: "a 14-year-old boy, three years post living-donor transplant, with a creatinine rise from 90 to 160 over two weeks, erratic tacrolimus levels, and no intercurrent illness, presenting with likely acute rejection from non-adherence." That one sentence sets the investigation and the management. The discriminator between the causes is rarely the history alone; it is the combination of the tacrolimus level, the donor-specific antibody result, the ultrasound, and, when needed, the biopsy. [10]
Investigations
The core investigations for graft dysfunction are a focused panel that you send on every creatinine rise. Serum creatinine and its trend tell you how fast the problem is moving. The tacrolimus trough level tells you whether the child is toxic or under-immunosuppressed. A full blood count detects leucopenia or anaemia from mycophenolate or from infection. Urinalysis and the urine protein-to-creatinine ratio detect proteinuria, which signals recurrence of focal segmental glomerulosclerosis or chronic antibody-mediated rejection. [3]
The graft ultrasound with Doppler is the first imaging test and excludes the surgical complications: a dilated collecting system means obstruction, a peri-graft collection means a leak or lymphocoele, and absent or altered flow means vascular thrombosis. If the cause is still unclear, the immunological tests come next. Donor-specific antibodies, measured by a single-antigen bead assay against the donor's HLA, are sent: a rise in donor-specific antibodies strongly suggests antibody-mediated rejection. A BK virus blood PCR is sent to detect BK nephropathy. [9]
The definitive investigation is the graft biopsy, interpreted against the Banff classification. Biopsy is not reserved for when everything else fails; it is the test that confirms rejection and tells you which type, because treating the wrong type causes harm. T-cell-mediated rejection shows tubulitis, interstitial inflammation and intimal arteritis. Antibody-mediated rejection shows microvascular inflammation, glomerulitis, and C4d deposition in the peritubular capillaries. Tacrolimus toxicity shows arteriolar hyalinosis and striped fibrosis. BK nephropathy shows tubulointerstitial inflammation with a positive SV40 stain. The biopsy pattern changes the treatment completely, which is why it is done before escalating immunosuppression in any but the clearest case. [9]
Routine monitoring extends beyond the creatinine rise. Epstein-Barr virus PCR is monitored in EBV-negative recipients of EBV-positive grafts, because a rising load warns of post-transplant lymphoproliferative disorder. Cytomegalovirus PCR is monitored based on serostatus. Metabolic surveillance looks for post-transplant diabetes (from tacrolimus and steroids), hypophosphataemia, hypercalcaemia, hyperlipidaemia, and the bone disease of chronic kidney disease. Growth is measured at every visit, because a child whose growth falters may need their steroid minimised. [2]
Management — Resuscitation
The immediate perioperative and early post-transplant period protects the graft from the insults that cause delayed graft function and early graft loss. The guiding principle is generous perfusion: the new kidney needs a well-filled vascular tree to function, so the child is given isotonic fluid to keep the circulation full and the urine output generous. Hypovolaemia is the enemy, because an underperfused graft develops acute tubular necrosis and may never recover. [1]
Fluid management demands precision because the new graft can produce enormous volumes of urine. In the first hours the graft may pass hundreds of millilitres per hour, and this output is replaced millilitre for millilitre with intravenous fluid matched to the urine electrolytes. Daily weight, strict input-output charts, and central venous pressure monitoring guide therapy. The trap is being too cautious with fluid in a child who looks oedematous from pre-existing renal failure, because the graft still needs to be perfused. [1]
Electrolyte disturbances are expected and corrected promptly. Hyperkalaemia, hypophosphataemia, hypomagnesaemia (which tacrolimus causes by urinary wasting) and metabolic acidosis all occur in the early period. Hypertension is common, driven by the new graft, the steroids, and pre-existing vascular disease, and is managed with a calcium channel blocker. The tacrolimus level is checked daily at first and the dose adjusted to stay within the target trough, because both toxicity and under-immunosuppression threaten the graft in equal measure. [8]
The patency of the renal vessels is confirmed in the first hours. Sudden oliguria with a swollen tender graft, falling haemoglobin, or haematuria suggests renal vein thrombosis, which is a surgical emergency because the graft can be lost within hours. An urgent Doppler ultrasound confirms the diagnosis, and the child returns to theatre for exploration. Vascular thrombosis is the commonest cause of early graft loss in young children, which is why the graft is monitored so closely in the first day. [1]
Delayed graft function, defined as the need for dialysis in the first week after transplant, is managed supportively. Dialysis bridges the gap while the stunned kidney recovers, and the child is investigated to exclude rejection and obstruction as alternative causes. Delayed graft function is more common after deceased-donor transplant and worsens long-term graft survival, which is another reason living donation is preferred. [2]
Management — Definitive & Stepwise
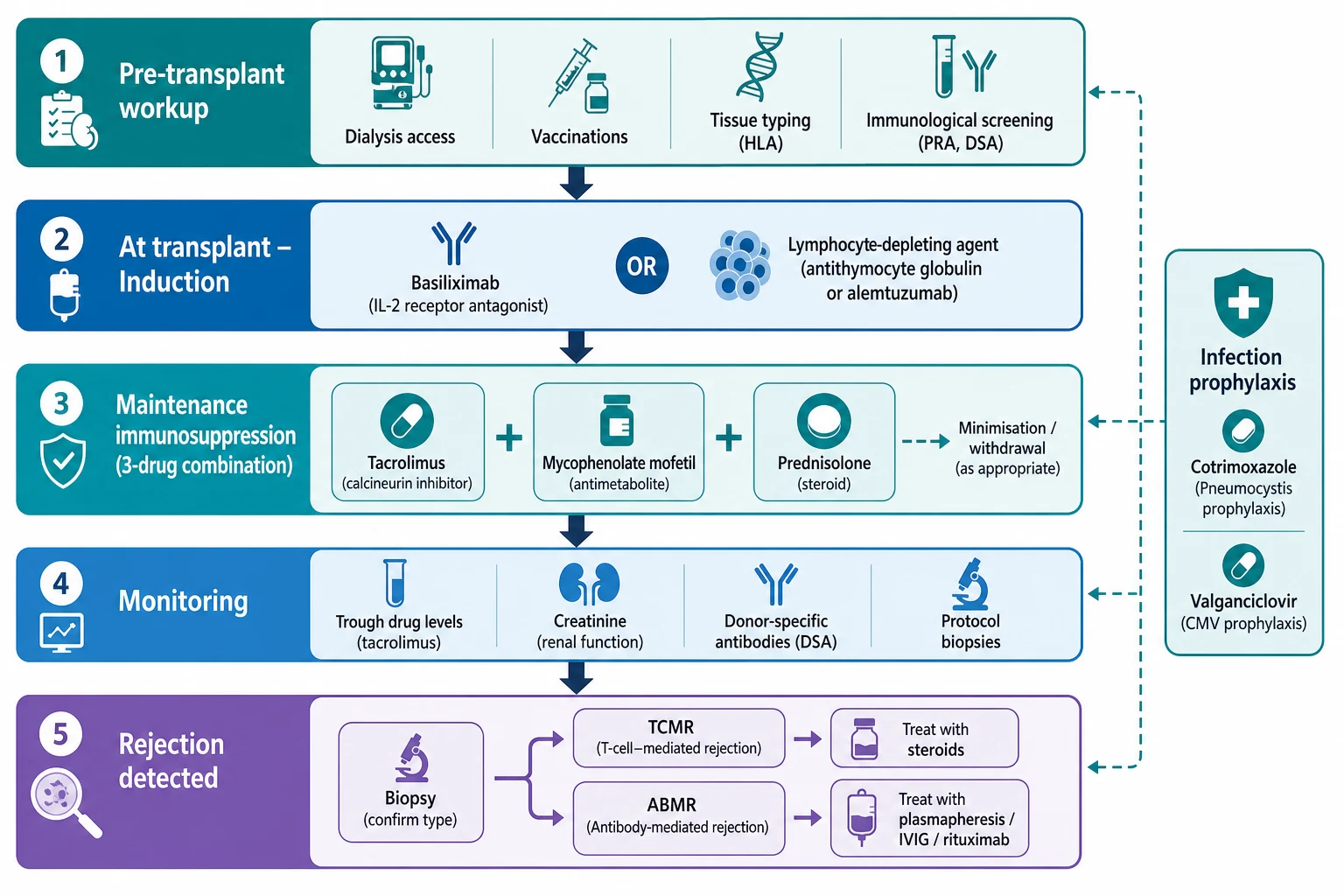
[4]Definitive management is lifelong immunosuppression, organised as two phases: a powerful induction dose given at the operation, and a maintenance regimen the child takes every day thereafter. The induction is chosen according to the child's immunological risk. A child at low risk, with a well-matched living-donor kidney and no sensitising antibodies, receives basiliximab, a gentle interleukin-2 receptor antibody. A child at higher risk, who is sensitised or receiving a deceased-donor kidney, receives a lymphocyte-depleting agent such as antithymocyte globulin or alemtuzumab, which more powerfully suppresses the T cells that would otherwise reject the graft. [7]
The maintenance regimen is a three-drug combination that has become the international standard because it protects the graft from both rejection pathways while keeping each drug's dose low enough to limit toxicity. Tacrolimus, the calcineurin inhibitor, blocks T-cell activation. Mycophenolate mofetil, the antimetabolite, blocks lymphocyte proliferation. Prednisolone, the corticosteroid, dampens the inflammatory response and is given at the lowest effective dose, and in selected low-risk recipients it is withdrawn entirely to protect the child's growth. [4]
Pre-transplant workup
Induction at transplant
Maintenance immunosuppression
Infection prophylaxis
Monitoring for life
Therapeutic drug monitoring of tacrolimus is the cornerstone of maintenance care, because tacrolimus has a narrow therapeutic window: too little and the child rejects, too much and the graft is poisoned. The trough whole-blood tacrolimus level is kept around 5 to 10 nanograms per millilitre in the early post-transplant period, then lowered to a long-term target to limit chronic nephrotoxicity. The level is affected by dozens of drug interactions and by the child's liver enzyme genetics, which is why it is checked frequently and the dose adjusted to the result rather than to a fixed prescription. [8]
Tacrolimus (maintenance)
Dose
Starting around 0.15 to 0.3 mg per kg per dose orally twice daily, then titrated to trough level
When rejection is confirmed by biopsy, the treatment depends on the type. Acute T-cell-mediated rejection is treated first with high-dose intravenous corticosteroids, typically pulse methylprednisolone. If the rejection is steroid-resistant, a lymphocyte-depleting agent such as antithymocyte globulin is added. Antibody-mediated rejection is harder to treat and combines therapies that remove and neutralise the antibodies: plasmapheresis to wash them out, intravenous immunoglobulin to block them, and rituximab to deplete the B cells that make them. In resistant cases, proteasome inhibitors such as bortezomib are used to target the antibody-producing plasma cells directly. [9]
Acute T-cell-mediated rejection treatment
Dose
Intravenous methylprednisolone, for example 10 mg per kg per day (maximum 500 mg) for 3 days, then an oral prednisolone taper
Infection prophylaxis runs in parallel with the immunosuppression. Co-trimoxazole is given for several months to prevent Pneumocystis jirovecii pneumonia. Valganciclovir prophylaxis is given to CMV-mismatched recipients (those who are CMV-negative receiving a CMV-positive graft) to prevent cytomegalovirus disease. In EBV-mismatched recipients, the Epstein-Barr virus viral load is monitored by quantitative PCR so that post-transplant lymphoproliferative disorder is detected early, at which point the first step is to reduce immunosuppression. [11]
Specific Subtypes & Scenarios
The infant and very small recipient deserves separate attention because the surgery and the perioperative care are harder. A child under roughly 15 to 20 kilograms receives an adult-sized kidney, because paediatric deceased-donor kidneys are scarce. The adult kidney is placed intraperitoneally, with its vessels joined to the aorta and inferior vena cava. This large kidney demands meticulous fluid and haemodynamic management in the first hours, and these small recipients carry a higher early graft-loss rate from vascular thrombosis. Once they survive the early period, their long-term graft function is excellent. [1]
Preemptive transplantation is the scenario that every transplant programme tries to maximise. By transplanting before dialysis begins, the child avoids the growth failure, neurodevelopmental harm, vascular damage, and mortality of dialysis, and the graft survives longer. It is feasible chiefly when a living donor is available, because the surgery can be planned for the moment dialysis would otherwise be needed. The practical trigger is the estimated glomerular filtration rate: once it falls toward 10 to 15 mL per minute per 1.73 square metres, dialysis is imminent, so the donor workup must already be complete. [3]
Preemptive transplant and graft survival
Key finding
Preemptive transplantation, performed before the initiation of maintenance dialysis, is associated with superior graft and patient survival compared with transplantation after dialysis, and is feasible primarily when a living donor is available. The benefits are attributed to avoidance of dialysis-related cardiovascular and infectious morbidity and to a shorter uraemic exposure.
Practice change
Refer children with progressive chronic kidney disease to a transplant centre early and work up a living donor so that dialysis can be avoided entirely, planning the transplant once eGFR approaches 10 to 15 mL per minute per 1.73 square metres.
Recurrent disease changes the transplant plan. Focal segmental glomerulosclerosis recurs in roughly 30 percent of first grafts, often within hours to days, presenting as massive proteinuria and a falling serum albumin; it is treated with plasmapheresis and rituximab, and a child with a history of aggressive recurrence may be listed for transplant with a plan to start plasmapheresis at the operating table. Primary hyperoxaluria recurs unless a combined liver-kidney transplant is performed, because the liver is the source of the missing enzyme. Atypical haemolytic uraemic syndrome recurs aggressively and requires prophylactic eculizumab before and after transplant. [9]
The highly sensitised child has a high panel-reactive antibody level and multiple donor-specific antibodies, usually from previous transfusions or a prior transplant, which makes finding a compatible kidney hard. These children may need desensitisation to lower their antibody burden, entry into a paired-exchange programme to find a better-matched donor, or acceptance of an HLA-incompatible graft with a higher rejection risk that requires augmented immunosuppression. The sensitised child waits longer and rejects more, which is why avoiding sensitising transfusions in children with chronic kidney disease is a preventive priority. [10]
Complications & Pitfalls
A transplanted child can run into trouble at any point, and the trouble looks different depending on when it strikes. In the first hours the danger is surgical: the renal artery or vein may thrombose, threatening the graft immediately, the ureter may leak or obstruct, and a lymphocoele may collect. Vascular thrombosis is the commonest cause of early graft loss in young children and presents with sudden oliguria and a swollen graft; recognising it within hours is the difference between saving and losing the graft. Wound infection rounds out the early surgical picture. [1]
The immunological complications are acute rejection, chronic antibody-mediated rejection, and recurrent disease. Acute rejection is now mostly preventable with modern induction and maintenance, and when it occurs it is usually steroid-responsive. Chronic antibody-mediated rejection, driven by persistent donor-specific antibodies, is harder to treat and is the leading cause of long-term graft loss; the strategy is prevention through adherence and monitoring of donor-specific antibodies rather than rescue. [9]
Infectious complications follow the predictable timeline: bacterial infections in the first month, opportunistic viral and fungal infections from one to six months, and community infections after six months. Post-transplant lymphoproliferative disorder, driven by Epstein-Barr virus in EBV-mismatched recipients, is the feared complication; it presents with fever, lymphadenopathy and a rising EBV load, and the first step is to reduce immunosuppression, with rituximab and chemotherapy reserved for progressive disease. [11]
Metabolic and drug complications are the long-term price of immunosuppression. Post-transplant diabetes mellitus is caused by tacrolimus and steroids and is screened for at every visit. Hypertension is almost universal and drives cardiovascular disease, the leading cause of death in long-term transplant survivors. Dyslipidaemia, growth impairment (which improves once the steroid is minimised), osteopaenia, and chronic calcineurin inhibitor nephrotoxicity all accumulate over the years. The practical point is that these complications are dose-dependent, so the long-term goal is the lowest immunosuppression that still protects the graft. [2]
The most preventable pitfall is non-adherence in the adolescent. The teenager who stops taking their tacrolimus rejects, often silently, and loses a graft that took years to arrange. Non-adherence is not a moral failing but a developmental and systems problem: the medicines are many, the side effects include acne and weight gain, the graft feels well so the motivation drops, and the transition to adult care severs the safety net. Detecting non-adherence, through erratic tacrolimus levels and missed appointments, and responding with structured support rather than blame, is the most important thing a paediatric transplant service does for its adolescents. [12]
Prognosis & Disposition
Kidney transplantation offers a transformed prognosis compared with dialysis. Five-year patient survival exceeds 95 percent, and the child returns to school, grows, and develops in a way that dialysis does not permit. Five-year graft survival is around 85 to 90 percent for living-donor grafts and 75 to 80 percent for deceased-donor grafts in paediatric series. The graft half-life is longest for living-related grafts received in childhood, which is why a parent's kidney is the gold standard. [2]
The sobering truth is that no graft lasts forever. Most paediatric recipients will outlive their first graft and need at least one retransplant, because chronic antibody-mediated rejection and the slow accumulation of damage eventually win. The aim of long-term care is therefore to maximise the years of function the graft gives, through adherence, monitoring of donor-specific antibodies, minimisation of nephrotoxicity, and aggressive management of hypertension and cardiovascular risk. [3]
Severity
Stable graft
Stable creatinine, therapeutic tacrolimus level, no donor-specific antibodies, adherent. Routine clinic follow-up every few months.
Severity
Acute rejection episode
Rising creatinine with biopsy-confirmed acute cellular or antibody-mediated rejection. Requires admission, pulse steroids or antibody-directed therapy, and a review of the maintenance regimen.
Severity
Graft loss or life-threatening complication
Refractory antibody-mediated rejection, vascular thrombosis, PTLD, or non-adherence-driven graft failure. Requires intensive management, possible return to dialysis, and retransplant assessment.
Disposition depends on the phase. The early post-transplant child is in a tertiary transplant centre, often in a high-dependency or intensive care setting for the first day. The stable graft recipient is followed in the transplant clinic, with the frequency of visits reducing over years as the graft stabilises. Every child needs lifelong specialist nephrology follow-up, and the transfer to adult care is a high-risk moment that demands a structured transition programme, because graft loss clusters around the handover. [12]
Special Populations
Adolescents are the population that transplant services worry about most, because the graft-loss rate rises sharply in the late teens and early twenties. The reasons cluster around development: the drive for autonomy conflicts with a regimen that demands absolute consistency, the side effects of steroids and immunosuppression threaten body image at exactly the age it matters most, and the move to adult care severs the paediatric team's relationship. The response is a structured transition programme that begins in early adolescence, teaches self-management, addresses mental health, and hands over to an adult team with a written summary and a warm introduction rather than a cold referral. [12]
Infants and very small children carry a higher early graft-loss risk from vascular thrombosis but, once past the early period, achieve excellent long-term graft function and growth. Their management demands a specialist paediatric transplant centre with the surgical and intensive care expertise to place and support an adult-sized kidney in a small body. Growth, which is often severely impaired by chronic kidney disease before transplant, accelerates after a successful transplant once the steroid is minimised. [1]
Children from Indigenous, socioeconomically disadvantaged, and migrant or refugee families face barriers that the transplant team must address actively. Donor availability may be limited by family logistics and geography. Adherence support is harder when housing is unstable, when English is a second language, and when the family lives far from the transplant centre. Telehealth, outreach clinics, dedicated transplant coordinators, and culturally appropriate education reduce these barriers and improve graft survival. These are not optional extras but core components of equitable transplant care. [3]
The EBV-seronegative child receiving an EBV-positive graft is a special population at risk of post-transplant lymphoproliferative disorder. These children are monitored with quantitative EBV PCR, and a rising load prompts a reduction in immunosuppression before the lymphoma declares itself. The highly sensitised child, with a high panel-reactive antibody, waits longer for a compatible kidney and faces a higher rejection risk, requiring desensitisation or paired-exchange strategies. Both groups need intensified surveillance and individualised immunosuppression. [11]
Evidence, Guidelines & Regional Differences
The KDIGO 2009 Clinical Practice Guideline for the Care of Kidney Transplant Recipients is the international framework for transplant management, covering immunosuppression, infection prophylaxis, cardiovascular risk, malignancy surveillance, and graft monitoring. Although written primarily for adults, its principles apply to children, and the paediatric-specific guidance from the International Pediatric Nephrology Association and the International Pediatric Transplant Association extends it for the developing child. [4]
In Australia and New Zealand, the KHA-CARI 2012 guideline adapts the KDIGO recommendations for local practice, and ANZDATA (the Australia and New Zealand Dialysis and Transplant Registry) provides outcome data that benchmark local programmes. Access to living donation and to the expensive biologics used for antibody-mediated rejection is funded through national transplant programmes, though the high cost of agents such as eculizumab and bortezomib requires individual approval. Preemptive transplantation is actively promoted, and paediatric candidates receive priority on the deceased-donor waiting list. [5]
In Australia and Aotearoa New Zealand, paediatric kidney transplantation is centralised in specialist tertiary centres, with ANZDATA providing comprehensive registry data on graft and patient survival. The KHA-CARI guideline adapts KDIGO for local practice, living donation is strongly encouraged, and paediatric recipients receive priority allocation on the deceased-donor waiting list. Transition to adult care is increasingly delivered through structured programmes, recognising that graft loss clusters around the transfer. [5]
Active controversies in the field include the optimal induction agent, the safety and timing of steroid withdrawal (favoured for growth but carrying rejection risk), the role of protocol surveillance biopsies in detecting subclinical rejection, and the best regimen for antibody-mediated rejection, where newer agents such as bortezomib, carfilzomib and tocilizumab are under investigation. Newer agents under development for children include belatacept, a co-stimulation blocker that aims to reduce calcineurin inhibitor nephrotoxicity, which is the leading cause of chronic allograft dysfunction. [7]
Exam Pearls
Kidney transplantation is the treatment of choice for a child with end-stage kidney disease, offering better survival, growth and neurodevelopment than dialysis. Congenital anomalies of the kidney and urinary tract are the leading cause of paediatric end-stage kidney disease leading to transplant. A living-donor kidney, especially from a parent, gives the best graft survival, and a preemptive transplant performed before dialysis is superior, so plan it once the eGFR approaches 10 to 15 mL per minute per 1.73 square metres. [3]
The standard maintenance regimen is tacrolimus plus mycophenolate mofetil plus low-dose prednisolone. Tacrolimus is a calcineurin inhibitor whose trough is kept around 5 to 10 nanograms per millilitre early, then lower long-term, and it is nephrotoxic, diabetogenic, and interacts with azoles (which raise the level) and rifampicin (which lowers it). Acute T-cell-mediated rejection is treated with high-dose intravenous methylprednisolone; antibody-mediated rejection is treated with plasmapheresis, intravenous immunoglobulin and rituximab. Focal segmental glomerulosclerosis recurs in about 30 percent of first grafts within days. [8]
BK virus nephropathy mimics acute rejection and is treated by reducing immunosuppression, not increasing it. Post-transplant lymphoproliferative disorder is Epstein-Barr virus driven in mismatched recipients and presents with fever, lymphadenopathy and a rising EBV load; the first step is to reduce immunosuppression. Co-trimoxazole prevents Pneumocystis and valganciclovir prevents cytomegalovirus. Non-adherence is the leading cause of late graft loss in adolescents, so structured transition to adult care, beginning in early adolescence, is essential. Remember the drug interactions: azoles and macrolides raise tacrolimus levels, while rifampicin and phenytoin lower them. [11]
References
- [1]Roach JP, Bock ME, Goebel J Pediatric kidney transplantation. Semin Pediatr Surg, 2017.PMID 28964479
- [2]Holmberg C, Jalanko H Long-term effects of paediatric kidney transplantation. Nat Rev Nephrol, 2016.PMID 26656457
- [3]Winterberg PD, Garro R Long-Term Outcomes of Kidney Transplantation in Children. Pediatr Clin North Am, 2019.PMID 30454748
- [4]Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant, 2009.PMID 19845597
- [5]Chadban SJ, Barraclough KA, Campbell SB, et al KHA-CARI guideline: KHA-CARI adaptation of the KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients. Nephrology (Carlton), 2012.PMID 22212251
- [6]Kizilbash SJ, Jensen CJ, Kouri AM, et al Steroid avoidance/withdrawal and maintenance immunosuppression in pediatric kidney transplantation. Pediatr Transplant, 2022.PMID 34786800
- [7]Balani SS, Jensen CJ, Kouri AM, et al Induction and maintenance immunosuppression in pediatric kidney transplantation-Advances and controversies. Pediatr Transplant, 2021.PMID 34216190
- [8]Weber LT Therapeutic drug monitoring in pediatric renal transplantation. Pediatr Nephrol, 2015.PMID 24763544
- [9]Ng YW, Singh M, Sarwal MM Antibody-mediated rejection in pediatric kidney transplantation: pathophysiology, diagnosis, and management. Drugs, 2015.PMID 25813498
- [10]Ashoor IF, Engen RM, Puliyanda D, et al Antibody-mediated rejection in pediatric kidney transplant recipients: A report from the Pediatric Nephrology Research Consortium. Pediatr Transplant, 2024.PMID 38602171
- [11]Scaggs Huang FA, Danziger-Isakov L Infectious disease risks in pediatric renal transplantation. Pediatr Nephrol, 2019.PMID 29626241
- [12]Holmberg C Nonadherence after pediatric renal transplantation: detection and treatment. Curr Opin Pediatr, 2019.PMID 30672821