Paeds · nephrology-urology-fluids-and-electrolytes
Nephrolithiasis and nephrocalcinosis
Also known as Kidney stones · Renal calculi · Urolithiasis · Nephrocalcinosis · Medullary nephrocalcinosis · Paediatric stone disease · Hypercalciuria
Fellowship guide to paediatric nephrolithiasis (stones in the collecting system) and nephrocalcinosis (calcium deposits in the renal parenchyma), the rising incidence of childhood stone disease, hypercalciuria as the commonest metabolic risk factor, the stone-composition and nephrocalcinosis-cause classification, the supersaturation-and-inhibitor pathophysiology, the abdominal pain and haematuria presentation, the ultrasound-first imaging strategy, the acute analgesia and hydration pathway, medical expulsive therapy with tamsulosin for distal ureteric stones, the ESWL, ureteroscopy and PCNL surgical ladder, and prevention through fluids, diet, thiazides and potassium citrate.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Stone disease in a child is no longer the rare, exotic diagnosis it once was. Over the past two decades the incidence of paediatric nephrolithiasis has climbed steeply in parallel with adult disease, driven by diet, dehydration, rising obesity and better detection, so that a general paediatrician now sees it regularly. [1] [12] What distinguishes the child from the adult is the obligation to find a cause. A first stone in a child is far more likely than in an adult to reflect an underlying metabolic, anatomical or genetic predisposition, and roughly one in five children with stones carries a single-gene cause. [4] [3] Finding that cause is what prevents recurrence, protects kidney function, and occasionally changes a child's entire trajectory — which is why every paediatric stone deserves a metabolic workup.
This page treats nephrolithiasis and nephrocalcinosis as one subject with two expressions, because they share the same metabolic roots and the same preventive logic. Stones form in the lumen; calcium deposits form in the parenchyma; both arise when urine is supersaturated with calcium, oxalate or phosphate and the inhibitors of crystallisation fall short. [5] [3] The first half of the page is the acute and surgical management of the stone in the ureter; the second half is the metabolic and genetic detective work that stops the next one.
Overview & Definition
Nephrolithiasis is the presence of one or more stones (calculi) in the renal collecting system — the renal pelvis, calyces, ureter or bladder. Urolithiasis is the broader term that encompasses stones anywhere along the urinary tract. The stones themselves are crystalline aggregates of urinary solutes bound by a protein matrix, and their composition reveals the cause: calcium oxalate is the commonest in children as in adults, followed by calcium phosphate, then struvite (infection) stones, uric acid stones and cystine stones. [1] [3]
Nephrocalcinosis is a different but related entity — microscopic or macroscopic deposits of calcium salts within the renal parenchyma itself, in the tubular epithelium and interstitium rather than the lumen. [5] It is classified by location into medullary (by far the commonest, because the medulla is where calcium concentrates), cortical (rare, seen in cortical necrosis or chronic glomerular disease) and diffuse. The distinction matters at the bedside: a stone causes colic and haematuria by obstructing flow, whereas nephrocalcinosis is often an incidental ultrasound finding that points instead to a tubulopathy, a metabolic disorder or prematurity. [5] [6]
The two conditions overlap because they share risk factors. The same hypercalciuria that grows a calcium oxalate stone in the pelvis also seeds the medulla with calcium, so a child can have both at once. The unifying concept is urinary supersaturation — when the concentration of stone-forming solutes exceeds what the urine can keep dissolved, crystals nucleate, grow and either lodge as a stone or deposit in the tissue. [3] [5]
Classification
Stone disease in children is classified along two axes: what the stone is made of, and where the calcium deposits sit. Stone composition is the single most useful piece of information after a stone is retrieved or passed, because it narrows the cause immediately. Calcium oxalate dominates and points to hypercalciuria, hyperoxaluria or hypocitraturia; calcium phosphate points to a high urine pH and renal tubular acidosis; struvite points to infection by urease-splitting organisms such as Proteus; uric acid points to hyperuricosuria or a low urine pH; and cystine points to cystinuria, an inherited tubular transport defect. [1] [3]
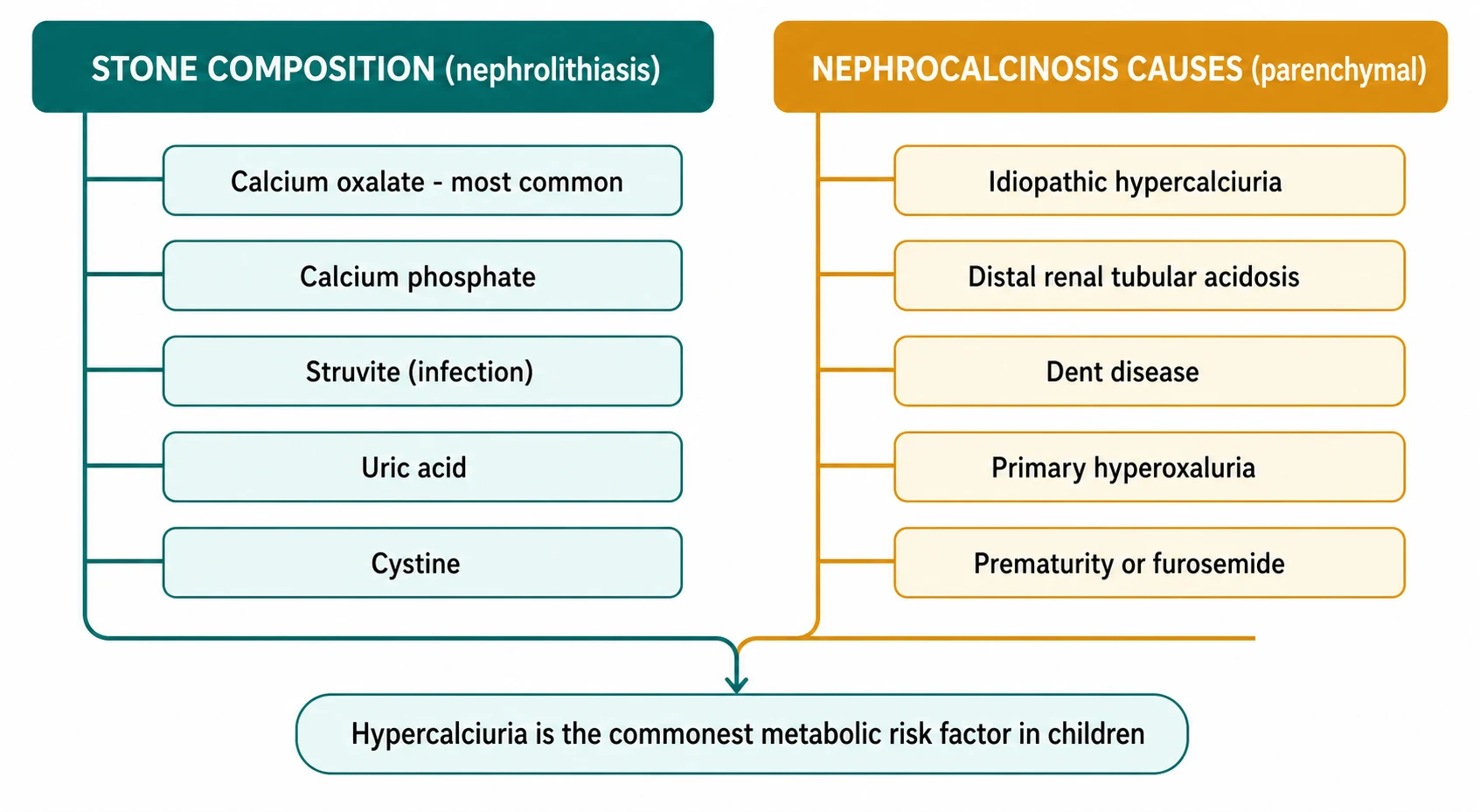
Nephrocalcinosis is classified by its parenchymal distribution, and that distribution is itself diagnostic. Medullary nephrocalcinosis is the common form and its causes read like a list of the inherited and metabolic diseases of the tubule: idiopathic hypercalciuria, distal renal tubular acidosis, Dent disease, primary hyperoxaluria, Bartter syndrome, and iatrogenic causes such as furosemide in the preterm infant and vitamin D intoxication. [5] [8] Cortical nephrocalcinosis is rare in children and follows cortical necrosis or chronic glomerular disease. Knowing whether the deposits are medullary or cortical therefore redirects the investigation before a single blood test is drawn.
Nephrolithiasis (lumen)
- Stone in pelvis, calyces, ureter or bladder
- Calcium oxalate most common, then calcium phosphate
- Struvite with urease-splitting infection (Proteus)
- Uric acid and cystine stones less common but important
- Presents with colic, haematuria or incidental finding
Nephrocalcinosis (parenchyma)
- Calcium deposits in renal tissue, usually medulla
- Distal renal tubular acidosis and Dent disease
- Primary hyperoxaluria and idiopathic hypercalciuria
- Furosemide and prematurity in the newborn
- Often an incidental ultrasound finding
Epidemiology & Risk Factors
Paediatric stone disease has become substantially more common. The global burden of paediatric urolithiasis rose steadily between 1990 and 2021, with the highest rates in the Middle East, South Asia and parts of North Africa, and forecasts suggest continued growth through 2040. [2] In high-income countries the increase has been attributed to rising rates of obesity and hypertension in children, diets high in sodium and low in fluid and citrate-containing fruits, and greater detection with ultrasound and computed tomography. [1] [12] Boys and girls are roughly equally affected in childhood, in contrast to the adult male predominance, and adolescents make up the largest share. [2]
The risk factors for recurrence are well mapped. In a multi-institutional analysis of children with a first stone, the strongest predictors of a subsequent stone event were a positive family history, an underlying metabolic abnormality (above all hypercalciuria), a larger index stone, anatomic abnormalities of the urinary tract, and a history of urinary tract infection. [11] Roughly half of children will form another stone within three to five years of the first if nothing changes, which is why the metabolic evaluation and preventive plan begin at the first presentation, not after a recurrence. [11] [12]
Pathophysiology
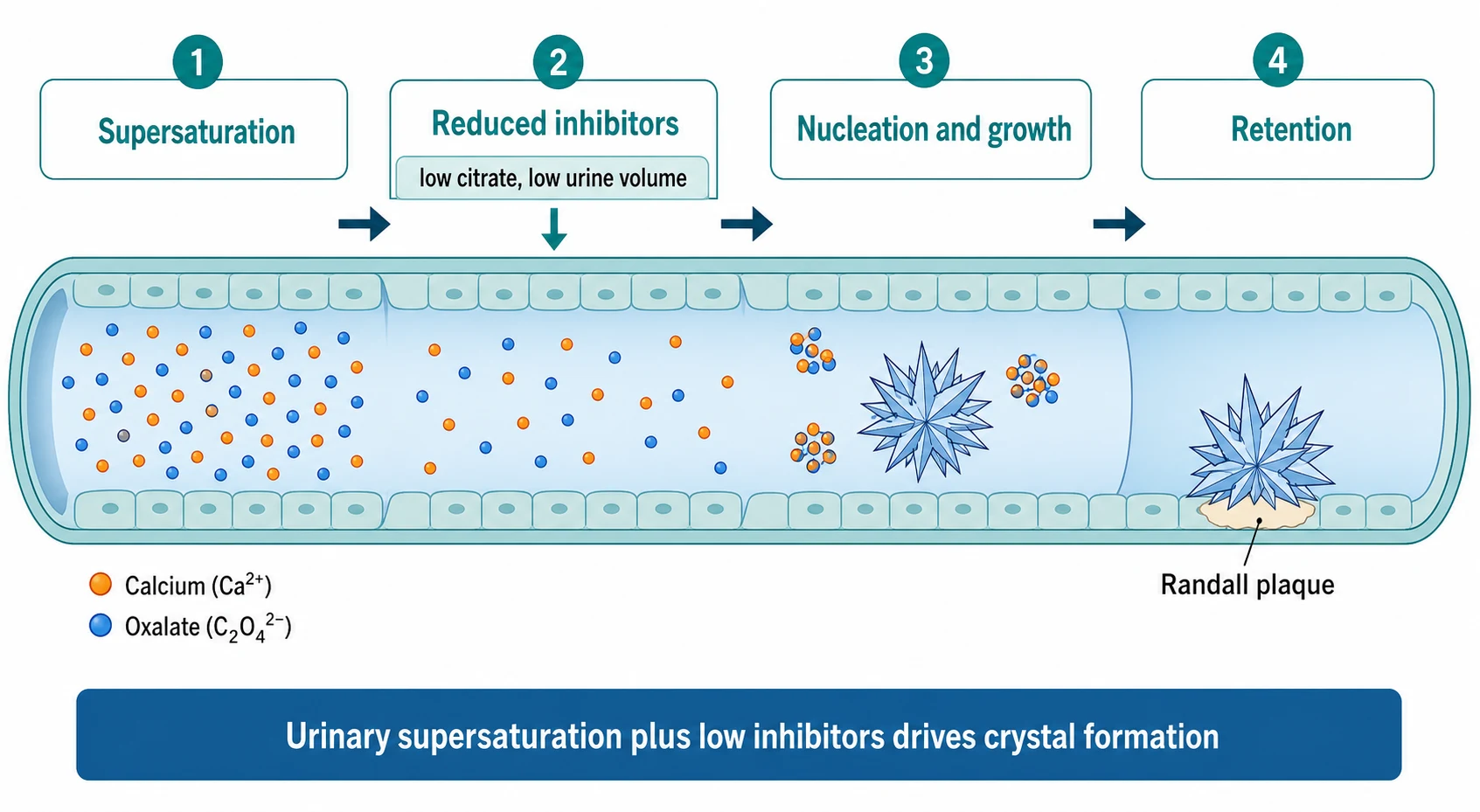
A stone forms when urine becomes supersaturated — when the concentration of a stone-forming salt exceeds the limit at which it can stay dissolved. Supersaturation is driven by three things: too much of the solute (calcium, oxalate, uric acid or cystine), too little urine volume (dehydration), and too little of the inhibitors that normally keep crystals from growing, chief among them citrate and magnesium. [3] [5] Once supersaturation passes a threshold, crystals nucleate, aggregate and grow. In calcium oxalate disease they often anchor to calcium phosphate deposits at the tips of the renal papillae known as Randall's plaques, which provide a surface for a clinical stone to take root. [3]
The metabolic drivers behind supersaturation are where paediatrics diverges from adult medicine. Hypercalciuria is the commonest abnormality and reflects either absorptive (gut over-absorption of calcium), resorptive (bone) or renal-leak mechanisms; hyperoxaluria may be primary (an inherited enzyme defect) or enteric (fat malabsorption binding calcium and freeing oxalate for absorption); hypocitraturia removes the main inhibitor of calcium crystallisation and often accompanies distal renal tubular acidosis or chronic diarrhoea. [5] [6] Distal renal tubular acidosis adds a high urine pH and systemic acidosis, which mobilises bone calcium and drives both calcium phosphate stones and medullary nephrocalcinosis. [6]
The genetic contribution is larger in children than is often assumed. Halbritter and colleagues screened a cohort of stone-forming patients against thirty known kidney-stone genes and found that a single monogenic cause explained roughly fifteen percent of all cases — and over twenty percent of the children. The cystinuria gene SLC7A9 was the most frequently mutated. [4] The implication is direct: a child with recurrent stones, bilateral disease, nephrocalcinosis or a positive family history carries a substantial chance of a treatable genetic diagnosis, and targeted gene panels are now part of the modern workup. [3] [4]
Clinical Presentation
Renal colic is the classic presentation of an obstructing stone, but in younger children the story is often vaguer. The school-age child or adolescent describes flank or loin pain that radiates to the groin, comes in waves, and is associated with nausea and vomiting — the same colic that adults report, though a child may localise it poorly as non-specific abdominal or back pain. [1] Haematuria is the other cardinal feature, and it is usually microscopic rather than visible; a child investigated for unexplained haematuria may turn out to have a small, non-obstructing stone. [12] Infants and preschool children present more variably — with irritability, feeding refusal, vomiting, or a urinary tract infection — and the stone is found on imaging done for these non-specific complaints. [1]
Nephrocalcinosis is usually silent. It is discovered when an ultrasound performed for another reason — a urinary tract infection, haematuria, failure to thrive, or screening of a preterm infant — shows echogenic medullary pyramids. [5] [8] When it does produce symptoms they are those of its cause: the polyuria, failure to thrive and rickets of distal renal tubular acidosis, the nephrocalcinosis itself being a signpost rather than the complaint. This is why nephrocalcinosis on an ultrasound is a trigger for a structured metabolic search, not a finding to be filed and forgotten. [6] [5]
The history that discriminates the cause runs through diet and fluids, bowel habit, medications, family history and the developmental context. Ask about fluid intake and diet (high sodium, low calcium, high oxalate foods), chronic diarrhoea or malabsorption (enteric hyperoxaluria), a personal or family history of stones, and in an infant the gestational history and any loop diuretic exposure. [5] [11] Examination adds growth parameters (failure to thrive points to a tubulopathy), blood pressure, evidence of rickets, the abdominal examination for a palpable mass or tenderness, and dysmorphic features that suggest a syndromic cause such as Williams syndrome. [6]
Differential Diagnosis
The acute differential of flank pain and haematuria in a child is wide, and stones must be distinguished from the surgical and medical causes of the same picture. Appendicitis, mesenteric adenitis, ovarian or testicular torsion, and a ruptured ectopic pregnancy in an adolescent girl can all mimic renal colic, while urinary tract infection, glomerulonephritis and Henoch-Schonlein purpura cause haematuria and abdominal pain without a stone. [1] [12] A urine dipstick, a full blood count and an ultrasound settle most of this at the bedside, but the message is that a child with abdominal pain needs the stone placed in a genuine differential, not assumed.
When a stone is confirmed, the differential shifts to its cause, and here the metabolic and anatomic causes are the target. Hypercalciuria is the commonest abnormality; others include hyperoxaluria, hypocitraturia, hyperuricosuria, cystinuria, and infection with urease-splitting organisms that produce struvite stones. [3] [5] Anatomic causes — ureteropelvic junction obstruction, megaureter, horseshoe kidney, posterior urethral valves, and bladder augmentation or diversion — slow urinary flow and let crystals settle, and they coexist with metabolic causes more often than chance. [1]
For medullary nephrocalcinosis the differential is a focused list of tubular and metabolic diseases. The principal causes are idiopathic hypercalciuria, distal renal tubular acidosis, Dent disease, primary hyperoxaluria, Bartter syndrome, hypophosphatasia and Williams syndrome, with furosemide-related hypercalciuria of prematurity leading the list in newborns. [5] [8] The blood gas, serum electrolytes, calcium, phosphate and urate, together with the urinary calcium-to-creatinine ratio and the urine pH, separate these efficiently at first contact. [6]
Commonest stone causes
- Idiopathic hypercalciuria
- Hyperoxaluria (primary or enteric)
- Hypocitraturia
- Anatomic obstruction stasis
- Infection with urease-splitting organisms
Medullary nephrocalcinosis causes
- Distal renal tubular acidosis
- Dent disease and Bartter syndrome
- Primary hyperoxaluria
- Furosemide and prematurity in infants
- Williams syndrome and hypophosphatasia
Clinical & Bedside Assessment
Begin with the analgesic and fluid needs of the child in pain, then screen for the red flags that change the tempo. Assess the severity and radiation of the pain, the presence of nausea and vomiting, the ability to tolerate oral fluids, and — most importantly — the presence of fever, which transforms a painful but stable stone into a potential emergency. [1] [12] A febrile child with an obstructing stone needs urgent imaging, urological referral and antibiotics, whereas an afebrile child with colic but preserved urine output can be managed stepwise. Check the urine output and the abdomen for a distended bladder or palpable kidney, and measure the blood pressure and look for signs of sepsis. [1]
Examine the growth and developmental context, because these point away from an incidental stone toward a systemic cause. Plot the height and weight: failure to thrive raises distal renal tubular acidosis, Dent disease or a chronic tubulopathy. Look for the bony signs of rickets (widened wrists, frontal bossing, leg bowing) that accompany chronic acidosis or phosphate wasting, and for dysmorphic features. [6] [5] A focused family history of stones, renal failure or consanguinity flags the genetic causes that account for a fifth of paediatric disease, and should be sought deliberately rather than as an afterthought. [4]
Take a careful dietary and pharmacological history. Low fluid intake is the commonest modifiable risk factor, and high dietary sodium, high oxalate intake (nuts, chocolate, spinach) with low calcium, and fad diets all contribute. Ask about loop diuretics in a preterm or cardiac infant, vitamin D or calcium supplementation, anticonvulsants (topiramate), and treatments such as indinavir that crystallise in urine. [5] [11] The bedside assessment is therefore not only about the pain in front of you but about assembling the clues that explain why this child formed a stone at all, because that is what the preventive plan will be built on.
Investigations
Imaging comes first, and ultrasound is the modality of choice in children. It shows stones as echogenic foci with an acoustic shadow, detects hydronephrosis that signals obstruction, and crucially does so without ionising radiation — a major consideration given that children are radiation-sensitive and stone disease is recurrent. [1] [12] Ultrasound is less sensitive than computed tomography for small ureteric stones, so a low-dose non-contrast CT is reserved for the child in whom ultrasound is non-diagnostic but the clinical suspicion remains high, or where the stone is refractory to conservative management. Plain abdominal radiography has a limited role but can track a known radio-opaque stone. [1]
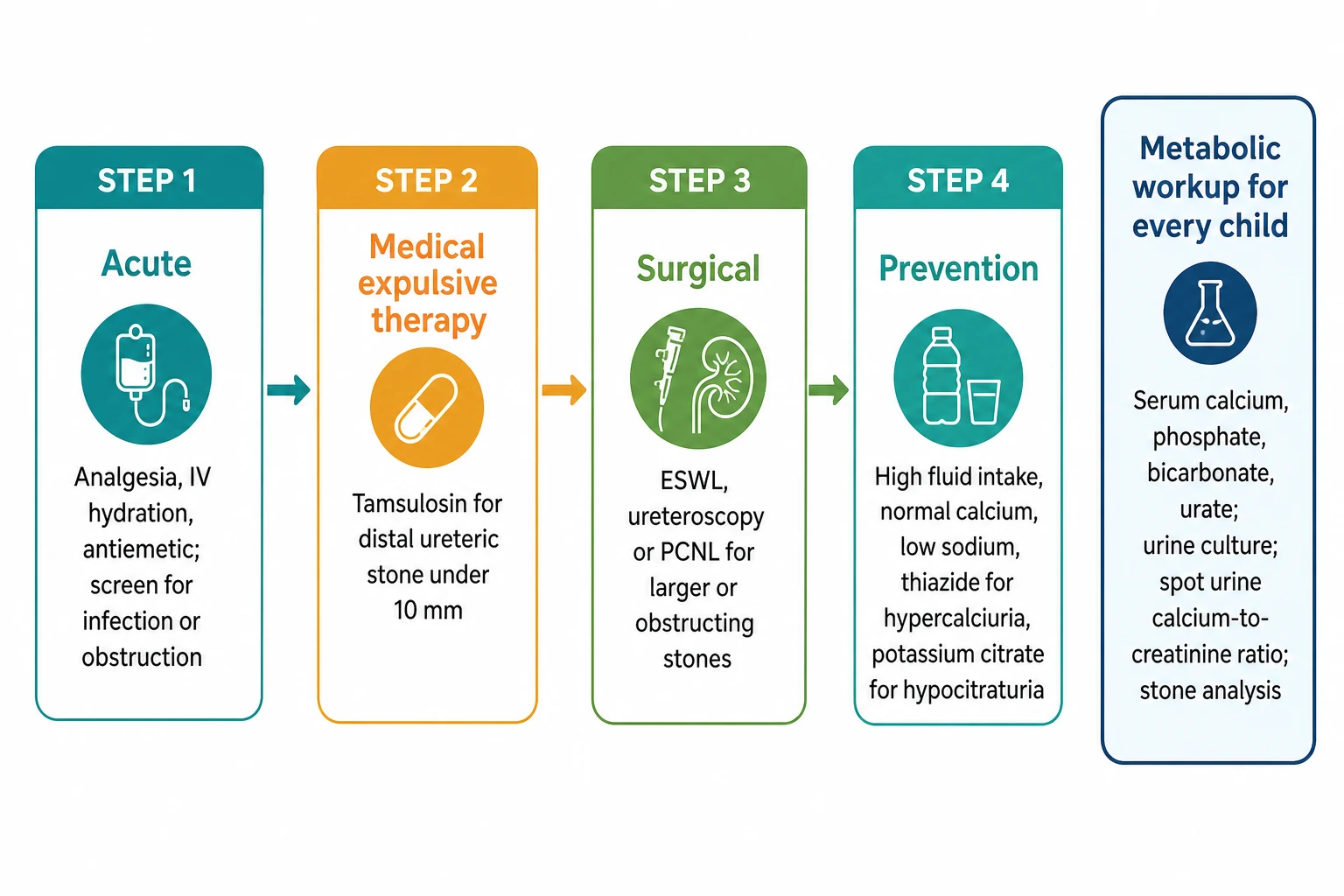
The metabolic workup is the heart of paediatric stone evaluation and should follow every confirmed stone. The blood panel includes calcium, phosphate, magnesium, bicarbonate (a venous blood gas captures the acid-base status), creatinine, urate, parathyroid hormone where the calcium is high or borderline, and vitamin D status. [3] [6] The urine panel includes a culture (to exclude urease-splitting infection), a urinalysis for pH and crystals (hexagonal crystals flag cystinuria), and a sodium nitroprusside screen for cystine. Stone analysis, when the stone is retrieved, gives the definitive composition and should always be requested. [1] [3]
STONES
The urinary metabolic evaluation hinges on calcium excretion. Hypercalciuria is confirmed when a 24-hour urine calcium collection exceeds 4 mg per kilogram per day (about 0.1 mmol per kilogram per day), and a random spot urine calcium-to-creatinine ratio is the practical screen — its upper reference limit falls with age, from about 0.8 mg/mg in infants to below 0.3 mg/mg in older children and adolescents, so an age-specific threshold must be applied. [5] [3] A full 24-hour urine adds oxalate, citrate, uric acid and cystine quantification, and a genetic panel is indicated for recurrent disease, bilateral stones, nephrocalcinosis or a positive family history. [3] [4]
Management — Resuscitation
Acute renal colic is managed with analgesia, hydration and the identification of complications. Non-steroidal anti-inflammatory drugs such as diclofenac or ibuprofen are first-line for renal colic, reducing the ureteric oedema and prostaglandin-mediated pain; intravenous paracetamol and, where needed, an opioid such as morphine are added for breakthrough pain. [1] [12] Give an antiemetic for nausea and vomiting, and encourage oral fluids where tolerated, with intravenous fluids reserved for the child who is dehydrated or vomiting. Forced high-volume intravenous hydration does not expedite stone passage and risks overload, so fluid resuscitation should aim to correct dehydration, not to flush the stone. [1]
The decisive early question is whether the stone is complicated. Fever with an obstructing stone is an emergency: it raises an infected obstructed system at risk of pyonephrosis and sepsis, and it mandates urgent urological decompression (usually ureteric stent or nephrostomy), blood and urine cultures, and intravenous antibiotics. [1] [12] A stone in a solitary kidney, bilateral obstruction, or any stone with acute kidney injury or anuria likewise needs urgent decompression rather than conservative observation. These complicated presentations bypass the conservative pathway and go straight to the urologist and theatre. [12]
For the uncomplicated ureteric stone, decide between observation with medical expulsive therapy and early intervention. The factors that favour conservative management are a small stone (under 5 to 10 mm), a distal location, the absence of infection or severe obstruction, and adequate pain control. [10] [1] Stones under 5 mm pass spontaneously in the majority of children, and the larger the stone and the higher it sits in the ureter, the lower the spontaneous passage rate, which is why size and location guide the threshold for intervention. [10] [9]
Management — Definitive & Stepwise
The definitive ladder for the ureteric stone begins with medical expulsive therapy. Tamsulosin, a selective alpha-1-blocker, is given as medical expulsive therapy for a distal ureteric stone under 10 mm, off-label in children, typically at 0.4 mg once daily in the RCT dose with lower doses for smaller children. The Aldaqadossi trial in children with distal ureteric stones under 1 cm showed that tamsulosin plus ibuprofen increased the spontaneous passage rate over ibuprofen alone, and a later comparison found silodosin comparable to tamsulosin. [10] [9] Alpha-blockade relaxes the smooth muscle of the distal ureter, and its use is confined to distal stones; it is continued for up to four weeks with a planned review, and reserved for older children given the small risk of hypotension. [10]
When the stone fails to pass, is too large, or is complicated, surgery takes over, and the paediatric ladder mirrors the adult one with attention to size and anatomy. Extracorporeal shock wave lithotripsy (ESWL) fragments upper-tract stones in a single session and suits renal and proximal ureteric stones of moderate size. Ureteroscopy with holmium laser lithotripsy is the workhorse for ureteric and renal stones, with a high stone-free rate and is increasingly first-line for most ureteric stones. Percutaneous nephrolithotomy (PCNL) is reserved for large (over 2 cm) or staghorn renal stones. [1] [12] Struvite staghorn calculi require complete clearance because residual fragments harbour infection and regrow, so PCNL rather than ESWL is preferred for these. [1]
Tamsulosin (medical expulsive therapy, distal ureteric stone under 10 mm)
Dose
0.4 mg once daily (RCT dose in children; lower doses for smaller children)
Prevention is the definitive treatment and it begins at the first episode, because without it roughly half of children recur. High fluid intake to keep the urine dilute is the cornerstone, with a practical target of urine output around 1.5 to 2 mL per kilogram per hour (about 2 litres per day in an adolescent). [1] [12] Dietary advice aims for normal calcium intake (calcium binds dietary oxalate in the gut and lowering calcium paradoxically raises oxalate absorption and stone risk), reduced sodium (sodium drives renal calcium excretion), and moderated oxalate. Thiazide diuretics are added for confirmed hypercalciuria to reduce renal calcium excretion, and potassium citrate is the specific treatment for hypocitraturia and raises urinary citrate, the main inhibitor of calcium crystallisation, while also alkalinising the urine in distal renal tubular acidosis. [5] [3]
Uncomplicated ureteric stone — the management ladder
Analgesia: NSAID first-line (diclofenac or ibuprofen), add paracetamol or opioid as needed
Hydration and antiemetic; screen for fever, obstruction and AKI
Medical expulsive therapy: tamsulosin for distal ureteric stone under 10 mm
Surgery if failure to pass, large stone, or complication: ESWL, ureteroscopy or PCNL
Prevention: high fluids, normal calcium, low sodium; thiazide or potassium citrate by metabolic defect
Specific Subtypes & Scenarios
Cystinuria is the inherited tubular transport defect every candidate should know. A defect in reabsorbing cystine (and the dibasic amino acids) in the proximal tubule causes high urinary cystine, which is poorly soluble and forms recurrent stones from childhood. The clues are a family history, recurrent stones in a child, and hexagonal crystals on urinalysis with a positive nitroprusside screen. Management is aggressive hydration, urinary alkalinisation with potassium citrate to a target urine pH above 7, and cystine-binding agents such as tiopronin for high excretors. [3] [4]
Struvite (infection) stones form when urease-splitting organisms — classically Proteus, also Klebsiella and Pseudomonas — hydrolyse urea to ammonia, alkalinise the urine and precipitate magnesium ammonium phosphate. They grow fast and often form staghorn calculi that fill the collecting system, and they are driven by chronic or recurrent infection, sometimes on an anatomic abnormality. [1] [5] Complete surgical clearance is the goal because residual fragments re-infect and regrow, combined with culture-directed antibiotics and correction of any anatomical cause. A struvite stone in a child is therefore a surgical and infectious-disease problem together, not a metabolic one. [1]
Distal renal tubular acidosis straddles stones and nephrocalcinosis and is the cause not to miss in the infant with failure to thrive. A failure of distal acid secretion produces a metabolic acidosis with a paradoxically alkaline urine (pH above 5.5), hypercalciuria and low citrate, which together drive calcium phosphate stones and medullary nephrocalcinosis and, over time, rickets and growth failure. [6] [5] An incomplete form exists in which the blood gas is normal but the urine cannot acidify after an ammonium chloride load, and it presents with nephrocalcinosis or stones alone. [6] Treatment is alkali (potassium citrate or bicarbonate) at doses sufficient to correct the acidosis and suppress the hypercalciuria, which usually halts stone growth and protects growth. [6]
Preterm infant nephrocalcinosis is the iatrogenic end of the spectrum. Loop diuretics, especially furosemide, drive hypercalciuria, and the immature kidney of the very preterm infant deposits calcium in the medulla; the deposits are often seen on routine cranial or renal ultrasound and frequently regress when the diuretic is stopped or a thiazide is substituted. [8] [7] A systematic review of furosemide in premature infants found the evidence linking it to nephrocalcinosis and hearing loss to be of low quality and confounded, but the association remains clinically important and warrants diuretic review and renal ultrasound surveillance in exposed infants. [7]
Complications & Pitfalls
The cardinal pitfall in the acute setting is under-recognition of the infected obstructed system. A child with a stone and a fever is not simply in pain — the concern is an infected, obstructed kidney progressing to pyonephrosis and sepsis, and delayed decompression is the avoidable harm. The safe practice is to treat any febrile stone as an emergency, obtain imaging and urology involvement early, and start antibiotics while cultures are pending. [1] [12] The mirror-image pitfall is over-imaging the uncomplicated child: computed tomography delivers ionising radiation to a radiation-sensitive, recurrence-prone child, so ultrasound should remain first-line and CT reserved for genuine diagnostic uncertainty. [12]
The cardinal pitfall in follow-up is failing to perform a metabolic workup after the first stone. Because a metabolic or genetic cause underlies the majority of paediatric stones and predicts recurrence, omitting the evaluation forfeits the chance to prevent the next stone — and in monogenic disease, to diagnose a treatable systemic condition. [3] [4] A related error is lowering dietary calcium in an attempt to reduce calcium stones: this raises gut oxalate absorption and increases stone risk, so the correct advice is a normal calcium intake with reduced sodium and oxalate. [5] [1]
The third pitfall, in nephrocalcinosis, is treating the radiological finding without pursuing its cause. Medullary nephrocalcinosis is a signpost to distal renal tubular acidosis, Dent disease, primary hyperoxaluria or prematurity-related hypercalciuria, each with a specific treatment that protects kidney function and growth. [5] [6] Filing the ultrasound report without the metabolic workup misses the underlying disease and, in primary hyperoxaluria, can delay a diagnosis that progresses to chronic kidney disease. [5]
Prognosis & Disposition
The prognosis of a single uncomplicated stone is excellent once it has passed or been removed, but the long-term outlook is dominated by recurrence. Without preventive measures, roughly half of children form another stone within three to five years, and recurrence rates climb with the number of metabolic abnormalities present. [11] [12] The strongest predictors of recurrence are a positive family history, hypercalciuria, a larger index stone, anatomic abnormalities and prior urinary tract infection, so the risk stratification built into the metabolic workup directly shapes the intensity and duration of preventive therapy. [11]
Disposition depends on the presentation. An afebrile child with an uncomplicated ureteric stone under 10 mm, controlled pain and preserved urine output can be managed with analgesia, medical expulsive therapy and outpatient review, with a safety-net for fever, uncontrolled pain or failure to pass the stone. [10] [1] Admit any child with fever and obstruction, a solitary kidney with obstruction, acute kidney injury, uncontrolled pain or vomiting, or a large stone requiring early surgery. After resolution, arrange a metabolic and genetic evaluation, a preventive plan tailored to the metabolic defect, and follow-up imaging to confirm stone-free status and detect recurrence. [3] [5]
For the chronic, genetically driven forms the prognosis depends on early diagnosis and sustained treatment. Distal renal tubular acidosis treated with adequate alkali preserves growth and kidney function; Dent disease and primary hyperoxaluria progress toward chronic kidney disease and demand nephrology follow-up and, in hyperoxaluria, consideration of liver-kidney transplantation. [5] [3] A clear safety-net for the family — seek help for fever, uncontrolled pain, reduced urine output or visible haematuria — closes the loop between episodes. [1]
Special Populations
Preterm and newborn infants are the population in whom nephrocalcinosis is most often an iatrogenic, self-limiting finding. Loop diuretics for chronic lung disease drive hypercalciuria, and the deposits form in the medulla of the immature kidney. [8] [7] Management is to review the indication for the diuretic, substitute a thiazide where a diuretic is still needed, ensure adequate fluid and phosphate, and monitor with renal ultrasound; in most cases the nephrocalcinosis regresses as the diuretic is weaned and the tubule matures. Primary hyperoxaluria must be excluded when the nephrocalcinosis is severe, bilateral or progressive in a newborn. [5]
Children with neurogenic bladder or reconstructed urinary tracts — bladder augmentation, ileal conduits, posterior urethral valves — form stones at high rates. The combination of stasis, recurrent infection, foreign bodies (catheters), and altered urinary chemistry (hyperchloremic acidosis from bowel segments drives bone calcium release and hypercalciuria) makes stones almost expected rather than incidental. [1] [5] Prevention centres on regular bladder emptying or catheterisation, treatment of infection, acid-base correction, and surveillance imaging; these children need a coordinated urology and nephrology plan. [1]
Children with inherited tubulopathies and metabolic disease — distal renal tubular acidosis, Dent disease, Bartter syndrome, cystinuria and primary hyperoxaluria — carry lifelong stone and nephrocalcinosis risk and require disease-specific therapy, growth and kidney-function surveillance, and a structured transition to adult nephrology care. [6] [3] Because monogenic causes account for roughly a fifth of paediatric stone disease, a genetic panel is part of the workup for recurrent, bilateral or syndromic presentations, and the result can change management — for example, confirming cystinuria and adding a cystine-binding agent. [4] [3]
Adolescents approaching transition are a high-risk group because lifestyle factors — sugar-sweetened drinks, low water intake, dieting, eating disorders and obesity — converge with any underlying metabolic predisposition to drive stones at exactly the age when follow-up tends to lapse. [12] Prevention at this stage is behavioural as much as pharmacological, with concrete fluid targets, dietary counselling, and a planned handover to adult care that carries the metabolic diagnosis and the prevention plan forward. [11] [12]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric stone disease has grown but still trails the adult literature. The Cao and Tasian overview in 2023 set out the steep rise in prevalence, the principles of metabolic assessment, and the observation-versus-medical-expulsive-versus-surgical decision, while noting that much of the treatment evidence is extrapolated from adults and that more paediatric-specific data are needed. [1] The Hu and Xu global epidemiology study quantified the rising burden of paediatric urolithiasis from 1990 to 2021 and forecast its continued growth, framing stone disease as a public-health problem in children rather than a curiosity. [2]
The genetics evidence is now central to the paediatric story. Singh and Lieske's review in Nature Reviews Nephrology consolidated the genetic basis of stone disease and nephrocalcinosis, and Halbritter and colleagues' gene-panel study established that monogenic causes explain roughly fifteen percent of all stone disease and over twenty percent in children — a finding that has pushed genetic testing into the mainstream workup of recurrent paediatric stones. [3] [4] The Gefen and Zaritsky review of childhood genetic nephrolithiasis and nephrocalcinosis laid out the parenchymal-versus-lumen distinction and the inherited and iatrogenic causes of medullary disease that anchor the differential. [5]
The medical expulsive therapy evidence in children is modest but consistent. The Aldaqadossi randomised trial showed tamsulosin increased the passage of distal ureteric stones under 1 cm in children, and the Soliman comparison found silodosin comparable to tamsulosin, supporting alpha-blockade for distal ureteric stones while leaving the optimal dose and the role in younger children less certain. [10] [9] The risk-factor evidence from the Medairos and Ellison multi-institutional analysis quantified the predictors of recurrence and underpinned the rationale for a first-episode metabolic workup. [11]
ANZ and UK practice follows international consensus that ultrasound is first-line imaging in children, with low-dose CT reserved for diagnostic uncertainty, and that every child with a confirmed stone receives a metabolic workup. Local variation exists in the threshold for medical expulsive therapy and in the exact metabolic panel and gene-panel selection; specialist paediatric nephrology and urology input guides these decisions. Always confirm the local protocol for tamsulosin dosing and for the surgical pathway before prescribing. [1] [5]
The evidence is weakest in three places: the optimal duration of medical expulsive therapy in young children, the long-term effect of thiazides and potassium citrate on the paediatric skeleton and growth, and the role and timing of genetic testing in first-presentation disease. These remain areas of active study, and a specialist nephrology discussion is appropriate for the complex or recurrent case. [3] [11]
Exam Pearls
Memorise the distinction between nephrolithiasis and nephrocalcinosis in one line: a stone sits in the lumen and obstructs, nephrocalcinosis sits in the parenchyma and is found on imaging. Examiners test this distinction relentlessly because it redirects the investigation — a stone toward composition and metabolic workup, nephrocalcinosis toward the inherited tubulopathies, distal renal tubular acidosis and prematurity. [5] [3] The second must-know is that hypercalciuria is the commonest metabolic risk factor in children, confirmed by a 24-hour urine calcium above 4 mg per kilogram per day, with the spot urine calcium-to-creatinine ratio as the screen using an age-specific threshold. [5]
The acute-management answer is ultrasound first, analgesia with a non-steroidal anti-inflammatory drug, and the fever-or-solitary-kidney red flag for urgent urological decompression. For the distal ureteric stone under 10 mm, tamsulosin as medical expulsive therapy is the high-yield pharmacology point, supported by the Aldaqadossi trial; ESWL, ureteroscopy and PCNL form the surgical ladder by size and location. [10] [1] The prevention answer is high fluids, normal calcium (not low), reduced sodium and oxalate, with thiazide for hypercalciuria and potassium citrate for hypocitraturia. [5]
The genetic angle is increasingly examiner-relevant: monogenic causes explain about fifteen percent of all stone disease and roughly twenty percent in children, with cystinuria (SLC7A9) the most frequent single gene, so a family history, recurrence or nephrocalcinosis prompts a gene panel. [4] [3] The one-cause-not-to-miss is distal renal tubular acidosis in the infant with medullary nephrocalcinosis and failure to thrive: an alkaline urine (pH above 5.5) with metabolic acidosis, treated with alkali to protect growth and kidney function. [6]
References
- [1]Cao B; Daniel R; McGregor R; Tasian GE Pediatric Nephrolithiasis. Healthcare (Basel), 2023.PMID 36833086
- [2]Hu J; Zhang J; Wang J; Tan Y; Zhou L; Xu K Global, Regional, and National Epidemiology of Pediatric Urolithiasis (1990-2021) and 2040 Forecast. J Urol, 2025.PMID 40532191
- [3]Singh P; Harris PC; Sas DJ; Lieske JC The genetics of kidney stone disease and nephrocalcinosis. Nat Rev Nephrol, 2022.PMID 34907378
- [4]Halbritter J; Baum M; Hynes AM; Rice SJ; Thwaites DT; Hildebrandt F Fourteen monogenic genes account for 15% of nephrolithiasis/nephrocalcinosis. J Am Soc Nephrol, 2015.PMID 25296721
- [5]Gefen AM; Zaritsky JJ Review of childhood genetic nephrolithiasis and nephrocalcinosis. Front Genet, 2024.PMID 38606357
- [6]Alonso-Varela M; Gil-Pena H; Santos F Incomplete distal renal tubular acidosis in children. Acta Paediatr, 2020.PMID 32212394
- [7]Jackson W; Taylor G; Selewski D; Smith PB; Tolleson-Rinehart S; Laughon MM Association between furosemide in premature infants and sensorineural hearing loss and nephrocalcinosis: a systematic review. Matern Health Neonatol Perinatol, 2018.PMID 30473868
- [8]Hoppe B; Duran I; Martin A; Kribs A; Benz-Bohm G; Roth B Nephrocalcinosis in preterm infants: a single center experience. Pediatr Nephrol, 2002.PMID 11956879
- [9]Soliman MG; El-Gamal O; El-Gamal S; Abdel Raheem A; Abou-Ramadan A; El-Abd A Silodosin versus Tamsulosin as Medical Expulsive Therapy for Children with Lower-Third Ureteric Stones: Prospective Randomised Study. Urol Int, 2021.PMID 33524970
- [10]Aldaqadossi HA; Shaker H; Saifelnasr M; Gaber M Efficacy and safety of tamsulosin as a medical expulsive therapy for stones in children. Arab J Urol, 2015.PMID 26413330
- [11]Medairos R; Paloian NJ; Pan A; Moyer A; Ellison JS Risk factors for subsequent stone events in pediatric nephrolithiasis: A multi-institutional analysis. J Pediatr Urol, 2022.PMID 34980558
- [12]Bonzo JR; Tasian GE The Emergence of Kidney Stone Disease During Childhood-Impact on Adults. Curr Urol Rep, 2017.PMID 28417430