Paeds · nephrology-urology-fluids-and-electrolytes
Neurogenic bladder and dysfunctional voiding
Also known as Neuropathic bladder · Neurogenic lower urinary tract dysfunction · Detrusor-sphincter dyssynergia · Overactive bladder in children · Voiding dysfunction · Dysfunctional elimination syndrome
Fellowship guide to the neurogenic bladder and the dysfunctional voiding spectrum in children. Covers the neurological control of micturition and how a cord lesion such as spina bifida produces a hostile high-pressure bladder that threatens the upper tracts, the distinction from functional overactive bladder and dysfunctional voiding, the role of video-urodynamics, and the stepwise management from clean intermittent catheterisation and anticholinergics through intravesical botulinum toxin to bladder augmentation and a continent catheterisable channel, with the explicit goal of protecting renal function.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who dribbles urine day and night despite sitting on the toilet, or a newborn with myelomeningocele who never achieves a normal stream, has a disordered lower urinary tract. The bladder has only two jobs — to store urine at a low pressure and to empty completely on command — and when either job fails, the cause is either a neurological lesion disrupting the nerve pathways to the bladder, or a learnt functional problem in an anatomically intact nervous system. These two families of disorder look similar on the surface but demand completely different management, and the examiner will test whether you can tell them apart. [1]
A neurogenic bladder (also called a neuropathic bladder) is disordered bladder storage or emptying caused by a congenital or acquired lesion that interrupts the nerve pathways running between the brain, the pontine micturition centre, the sacral spinal cord, and the bladder. In children the dominant cause by far is spinal dysraphism, above all myelomeningocele, but sacral agenesis, a tethered cord, a spinal cord tumour or injury, cerebral palsy, and the aftermath of sacrococcygeal teratoma resection all produce the same picture. The unifying feature is that the bladder has lost the coordinated nerve control it needs. [3]
The term dysfunctional voiding describes a different entity entirely. It belongs to the family of non-neurogenic, functional lower urinary tract disorders that appear in the toilet-trained child, in which the nervous system is anatomically intact but the child has learnt to void against a tightened pelvic floor or to postpone voiding until desperate. Overactive bladder, dysfunctional voiding, and voiding postponement sit on this functional side of the divide. The distinction matters because the functional disorders are common, benign, and managed with behavioural therapy and constipation treatment, whereas a neurogenic bladder is a lifelong threat to the kidneys that needs urodynamics, catheterisation, and medication. [12]
The clinical importance of the neurogenic bladder is the damage it does upstream. A bladder that stores urine at high pressure, or that empties against a sphincter that will not relax, transmits those pressures to the ureters and kidneys. The result is hydronephrosis, vesicoureteral reflux, recurrent pyelonephritis, renal scarring, hypertension, and progressive chronic kidney disease. Spina bifida is one of the commonest causes of paediatric end-stage kidney disease from a urological mechanism, which is why every child with a cord lesion needs urodynamic surveillance from infancy and a bladder kept low-pressure for life. [6]
Classification
The clearest way to classify these disorders is by whether a cord lesion is present. A neurogenic bladder is defined by a demonstrated or suspected lesion in the nervous system, while the functional disorders are defined by the absence of such a lesion. Within each group, urodynamics then sorts the bladder into patterns that drive treatment. The figure below summarises the two sides of the divide. [1]
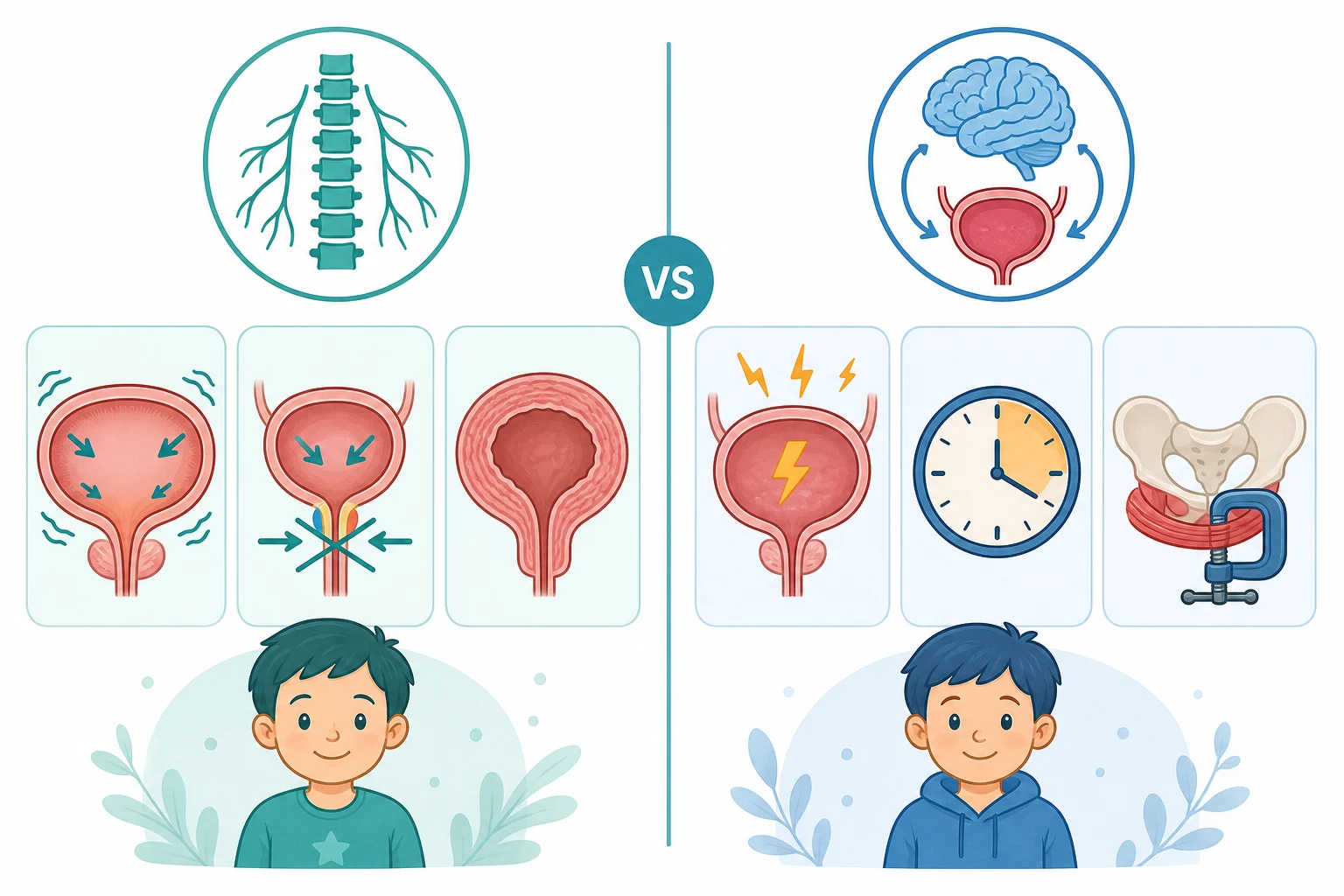
Neurogenic bladder
- A spinal cord or brain lesion interrupts the nerve pathway to the bladder
- Classic cause: myelomeningocele (spina bifida)
- Urodynamics shows detrusor overactivity, dyssynergia, or impaired compliance
- Threatens the upper tracts and kidneys through high storage pressures
- Managed with catheterisation, anticholinergics, and botulinum toxin
Overactive bladder
- No cord lesion; a functional storage problem in a toilet-trained child
- Urgency, with or without urge incontinence, usually with frequency
- Small frequent voids and holding manoeuvres such as leg crossing
- Benign; managed with bladder training, fluid advice, and anticholinergic if severe
- Often coexists with constipation
Dysfunctional voiding
- No cord lesion; the child learnt to contract the pelvic floor during voiding
- Staccato or interrupted stream on uroflowmetry, with a raised post-void residual
- Frequent urinary tract infection and daytime incontinence
- Strongly linked to constipation and the bowel-bladder loops
- Managed with biofeedback, timed voiding, and constipation treatment
Voiding postponement
- No cord lesion; the child defers voiding due to distraction or behavioural factors
- Infrequent voiding, often fewer than four times a day, with incontinence
- Common in children with behavioural or neurodevelopmental disorders
- Behavioural and psychological input is central
- Treated with timed voiding schedules and management of constipation
The neurogenic bladder is then classified urodynamically by what the bladder does during storage and emptying, because these patterns predict the risk to the kidneys and direct the treatment. Detrusor overactivity is involuntary detrusor contraction during filling, which produces urgency and incontinence and raises the storage pressure. Detrusor-sphincter dyssynergia is contraction of the urethral sphincter at the same time as the detrusor contracts during voiding, so the bladder empties against a closed outlet. Impaired compliance is a stiff, low-compliance bladder wall that allows pressure to climb steeply as it fills, and it is the pattern most dangerous to the upper tracts. A single child may show more than one pattern, and the pattern can change over time, which is why the urodynamics are repeated. [2]
Epidemiology & Risk Factors
Spina bifida (myelomeningocele) remains the prototype and the commonest cause of a paediatric neurogenic bladder, with a birth prevalence of around 3 to 4 per 10000 live births in populations with folate fortification. The majority of children born with myelomeningocele develop a hostile, high-pressure bladder that will damage the upper tracts if left alone, which is the central reason for early urodynamic surveillance in infancy. Beyond spina bifida, the causes span a cord lesion at any level: sacral agenesis (the caudal regression syndrome of maternal diabetes), a tethered cord from a lipomeningocele or a tight filum, diastematomyelia, spinal cord tumour or trauma, and the neurogenic bladder that follows resection of a sacrococcygeal teratoma. [5]
Cerebral palsy produces a mixed picture of an overactive bladder with sphincter disinhibition, often compounded by immobility and constipation. An acquired cord lesion from trauma, transverse myelitis, or a spinal abscess can produce a neurogenic bladder at any age and presents acutely with retention or incontinence. The lesson for the candidate is that any child with bladder symptoms and a neurological finding in the legs or on the back must be assumed to have a cord lesion until imaging proves otherwise. [7]
On the functional side, the disorders are far commoner. Overactive bladder and dysfunctional voiding together affect a substantial minority of school-age children, and they are the leading cause of daytime urinary incontinence in the toilet-trained years. The risk factors for the functional disorders are constipation (the single most important, because a loaded rectum compresses the bladder and disrupts the learnt voiding reflex), behavioural and psychological factors, developmental delay, and a family history. The two sides of the divide therefore have very different epidemiologies, which the examiner uses to separate a benign functional problem from a cord lesion. [12]
Pathophysiology
To understand why a neurogenic bladder damages the kidneys, you need to picture how normal continence is wired. The bladder is a smooth-muscle reservoir that fills at low pressure while the urethral sphincter stays closed, and then empties completely when the detrusor contracts and the sphincter relaxes at the same moment. That precise handover between filling and emptying, and between the detrusor and the sphincter, is organised by a nerve pathway that runs from the brain to the sacral cord. [7]
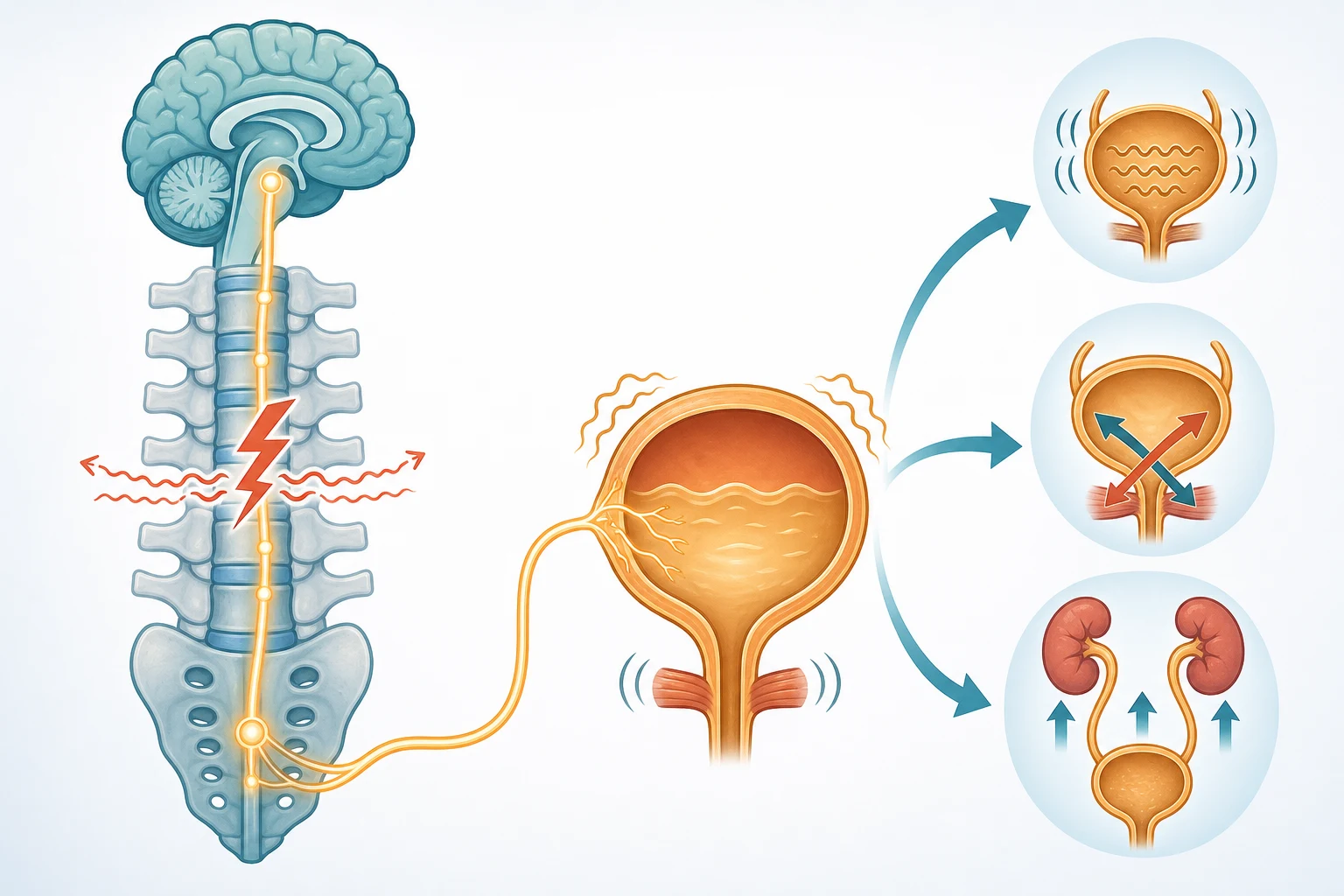
The control loop has three nodes. The sacral micturition centre at S2 to S4 carries the basic reflex: stretch of the bladder wall fires the pelvic nerve, the sacral centre sends the detrusor its contract command through the pelvic nerve, and it relaxes the sphincter through the pudendal nerve. The pontine micturition centre coordinates that reflex, ensuring the detrusor and sphincter act in concert rather than against each other. The cerebral cortex sits on top and provides inhibition, so the reflex fires only when the child chooses to void. A lesion anywhere along this loop changes what the bladder does, and the level of the lesion predicts the pattern. [7]
A cord lesion above the sacral centre, as in a thoracic or lumbar myelomeningocele, cuts the cortex and the pons off from the sacral reflex. The reflex is released from inhibition, so the detrusor fires involuntarily during filling — this is detrusor overactivity, the cause of urgency and incontinence. Because the pons can no longer coordinate the void, the detrusor and the sphincter contract together — this is detrusor-sphincter dyssynergia, the cause of incomplete emptying and a raised post-void residual. Over time the bladder wall, working against a closed outlet, becomes thick, collagen-laden, and stiff, so pressure climbs steeply as it fills — this is impaired compliance, the pattern most dangerous to the kidneys. [2]
The damage travels upstream because the bladder and the kidneys are a connected hydraulic system. When the storage pressure exceeds the pressure needed to push urine up the ureters, urine is forced back into the kidneys. The detrusor leak point pressure — the bladder pressure at which leakage occurs — is the single best predictor of this damage, and a pressure above 40 cm of water identifies the bladder that will develop hydronephrosis, reflux, and renal scarring. This is why the urodynamics, not the symptoms, decide whether a neurogenic bladder is safe. [2]
In the functional disorders the fault is learnt rather than structural. The child with dysfunctional voiding has learnt to contract the external sphincter and pelvic floor during voiding, perhaps initially to defer a void or to prevent leakage with cystitis, and the habit persists. The stream becomes staccato and interrupted, the post-void residual rises, and the stasis invites infection. The child with an overactive bladder has a sensitive, over-reactive detrusor that fires small involuntary contractions during filling, producing urgency. In both, the bowel is usually constipated, and a loaded rectum both compresses the bladder and reinforces the abnormal reflex. The pathophysiology points to the treatment: retrain the reflex, empty the bowel, and only then consider medication. [12]
Clinical Presentation
A neurogenic bladder announces itself differently at different ages. In the newborn, the clue is the spinal lesion itself — a myelomeningocele is obvious on the back at birth — and the bladder is silent because the newborn is in nappies. The first urinary signs may be a weak or dribbling stream, a palpable distended bladder, urinary retention, or a urinary tract infection in the first months of life. Because the newborn cannot report urgency, the urodynamics rather than the symptoms reveal the hostile bladder, which is why every infant with myelomeningocele is studied urodynamically in the first months. [3]
In the older child the presentation is incontinence, and the pattern of the incontinence is a clue. A neurogenic bladder produces continuous or stress incontinence that the child does not feel coming, because the detrusor and sphincter have lost sensation and coordination. Recurrent urinary tract infection is common, because the bladder empties poorly and stasis invites infection. Constipation and faecal soiling are nearly universal, because the cord lesion affects the bowel as well as the bladder, and the two must be managed together. [6]
The functional disorders present in the toilet-trained child and the history holds the diagnosis. The child with overactive bladder describes sudden, hard-to-defer urgency, with or without urge incontinence, and uses holding manoeuvres — crossing the legs, squatting on the heel, grabbing the genitals — to suppress the contraction. The child with dysfunctional voiding describes a stop-start stream, straining to void, and recurrent infection, and the parent reports the incontinence is worse with constipation. The child with voiding postponement voids infrequently, often fewer than four times a day, because play or distraction wins over the urge. [12]
The presentation that must not be missed is the occult cord lesion masquerading as a functional disorder. A child labelled as dysfunctional voiding who in fact has a tethered cord, a lipomeningocele, or diastematomyelia has a progressive, treatable cord lesion that will worsen until the cord is untethered. The clues are on the back and in the legs: a sacral dimple, a hair tuft, a lipoma, a deviated gluteal cleft, or a cutaneous haemangioma over the spine; and weakness, asymmetry, reflex change, gait abnormality, or a foot deformity in the lower limbs. Any such finding warrants an MRI of the spine. [7]
Differential Diagnosis
The first job is to separate the neurogenic from the functional, and then to find the cause within each. The features that distinguish the main entities are set out below, and the disciplined approach is to ask, for every child with bladder symptoms: is there a cord lesion, is there a structural urinary tract anomaly, and is there constipation driving the picture? [12]
Neurogenic bladder
- Spinal lesion on back examination or MRI: spina bifida, tethered cord, sacral agenesis
- Lower-limb neurological signs or foot deformity
- Video-urodynamics shows detrusor overactivity, dyssynergia, or impaired compliance
- Risk to upper tracts; needs lifelong renal surveillance
Overactive bladder
- No cord lesion; normal back and lower-limb exam
- Urgency, frequency, urge incontinence, holding manoeuvres
- Normal uroflowmetry or a bell-shaped curve with a small voided volume
- Benign; managed behaviourally and with anticholinergic if severe
Dysfunctional voiding
- No cord lesion; normal neurological exam
- Staccato or plateaued uroflow curve; raised post-void residual
- Strongly associated with constipation
- Biofeedback and constipation treatment are central
Structural anomaly
- Posterior urethral valves: male infant, poor stream, palpable bladder
- Urethral stricture or ectopic ureter: continuous dribbling in a girl
- Diagnosed on ultrasound and MCUG
- Surgical management of the underlying anomaly
Urinary tract infection
- Acute onset of urgency, frequency, dysuria, or incontinence
- Fever, malaise, or loin pain in pyelonephritis
- Urine culture confirms the diagnosis
- Treat the infection and reassess the bladder after recovery
Constipation
- Loaded rectum on abdominal and back exam
- Hard stools, infrequent defaecation, faecal soiling
- Bladder symptoms resolve or improve when the bowel is treated
- Treat the bowel first in any functional voiding disorder
The can't-miss diagnosis is the occult spinal dysraphism. A lipomeningocele, a tight filum terminale causing tethering, or diastematomyelia can all present as apparent dysfunctional voiding in a child whose back looks nearly normal, and the lesion is found only when a cutaneous stigmata or a lower-limb sign prompts an MRI. Missing it means the cord is progressively damaged and the bladder dysfunction worsens, whereas untethering can halt or reverse both. The rule the examiner rewards is simple: any child with new or progressive bladder dysfunction, or any child whose dysfunctional voiding does not respond to standard therapy, gets a careful back and lower-limb examination and an MRI if a stigmata or sign is found. [7]
The mimics of a neurogenic bladder presenting with retention include a posterior urethral valve in a male infant (a structural obstruction, not a cord lesion), a pelvic mass compressing the bladder or the sacral plexus, and an acute transverse myelitis or cord abscess that produces a sudden neurogenic bladder with back pain and a sensory level. Each needs urgent imaging, and the cord lesion causes demand an MRI of the spine on the day of presentation. [6]
Clinical & Bedside Assessment
The assessment begins with the back and the legs, not the bladder. Examine the spine and sacrum for a myelomeningocele (an open lesion, repaired at birth), a lipoma, a sacral dimple, a hair tuft (the faun's beard), a deviated gluteal cleft, or a cutaneous haemangioma — any of which signals an occult dysraphism and warrants an MRI. Examine the lower limbs for muscle bulk, tone, power, reflexes, and a foot deformity such as a talipes or a cavus foot, which localise the level of a cord lesion. Observe the gait, and check the anal tone and the sacral sensation. [7]
The abdominal examination looks for a palpable, distended bladder, palpable kidneys suggesting hydronephrosis, and a loaded colon suggesting constipation. Inspect the genitalia for an ectopic ureteral orifice in a girl with continuous dribbling, and assess the urinary stream by observation or by a flow rate where the child can cooperate. A post-void residual by bladder ultrasound after a natural void is the single most useful bedside measure: a residual above about 20 to 30 mL (or more than 10 percent of expected bladder capacity) in a toilet-trained child suggests incomplete emptying and prompts urodynamics. [2]
The history is structured by a bladder diary, in which the family records the time and volume of every void and every incontinence episode over three days, together with the fluid intake and the bowel actions. The diary quantifies the voided volumes, the frequency, and the incontinence pattern, and it distinguishes the small, frequent voids of an overactive bladder from the infrequent, large voids of voiding postponement. A validated symptom score for constipation and voiding completes the non-invasive assessment, because the bowel and the bladder are inseparable in the functional disorders. [4]
Investigations
The investigations are layered, and the layer chosen depends on whether a cord lesion is known, suspected, or excluded. The neurogenic bladder needs the gold-standard video-urodynamics; the functional disorders are worked up with non-invasive urodynamics; and both need surveillance of the upper tracts. The figure conceptually runs the pathway. [2]
Non-invasive urodynamics is the first step for the functional disorders and a useful baseline in all. Uroflowmetry records the urine flow rate over time, and the shape of the curve is diagnostic: a smooth bell-shaped curve is normal, a staccato or interrupted curve suggests dysfunctional voiding with pelvic-floor over-activity, a plateaued curve suggests a structural obstruction, and a tower-shaped curve with a high peak suggests an overactive bladder. Surface electromyography of the pelvic floor during voiding shows whether the sphincter relaxes, and it is the non-invasive test of dyssynergia. A bladder ultrasound with post-void residual completes the set. [12]
Video-urodynamics is the gold standard for the neurogenic bladder and is performed in infancy in spina bifida and whenever a hostile bladder is suspected. The bladder is filled through a catheter while the detrusor pressure is measured, the sphincter electromyogram is recorded, and fluoroscopy shows the bladder shape, the presence of vesicoureteral reflux, and the bladder outlet during voiding. The study defines the three patterns that drive treatment: detrusor overactivity (involuntary pressure rises during filling), impaired compliance (a steep pressure rise as the bladder fills, the most dangerous pattern), and detrusor-sphincter dyssynergia (sphincter activation during a detrusor contraction). The detrusor leak point pressure — the filling pressure at which leakage occurs — is the key number, because a pressure above 40 cm of water predicts upper-tract deterioration and mandates treatment to lower the pressure. [2]
The upper tracts are surveyed by renal ultrasound for hydronephrosis, bladder wall thickness, and post-void residual; by a DMSA scan for renal scarring and split function when reflux or infection has occurred; and by serum creatinine and blood pressure for renal function. An MRI of the spine is the test for the occult cord lesion and is obtained whenever a back stigmata or a lower-limb sign accompanies the bladder symptoms. A micturating cystourethrogram is reserved for suspected structural obstruction such as a posterior urethral valve or for the assessment of reflux, and is not a first-line test in the neurogenic bladder. [3]
Management — Resuscitation
A stable neurogenic bladder needs no acute resuscitation, but two situations are time-critical. The first is a child presenting in urinary retention with a palpable, distended bladder — pass a urethral catheter to drain the bladder immediately, because the obstruction and the back-pressure threaten the kidneys and the retained urine invites infection. The second is urosepsis in a child who cannot empty the bladder: drain the bladder with a catheter, send a urine culture, and treat the infection with intravenous antibiotics guided by local guidelines while the cause is found. [6]
The newborn with myelomeningocele is managed as a surgical and urological emergency in its own right. The open neural tube defect is closed by the neurosurgeon within the first 24 to 72 hours to prevent infection and preserve cord function, and the child is then assessed by the urology team. A baseline renal ultrasound and a urodynamic study are obtained in the first months of life, because a hostile high-pressure bladder can damage the upper tracts long before any symptom appears. A child found to have a high-pressure bladder is started on clean intermittent catheterisation and an anticholinergic from infancy, which is proactive management, not resuscitation, but it is the step that prevents the later renal failure. [3]
Management — Definitive & Stepwise
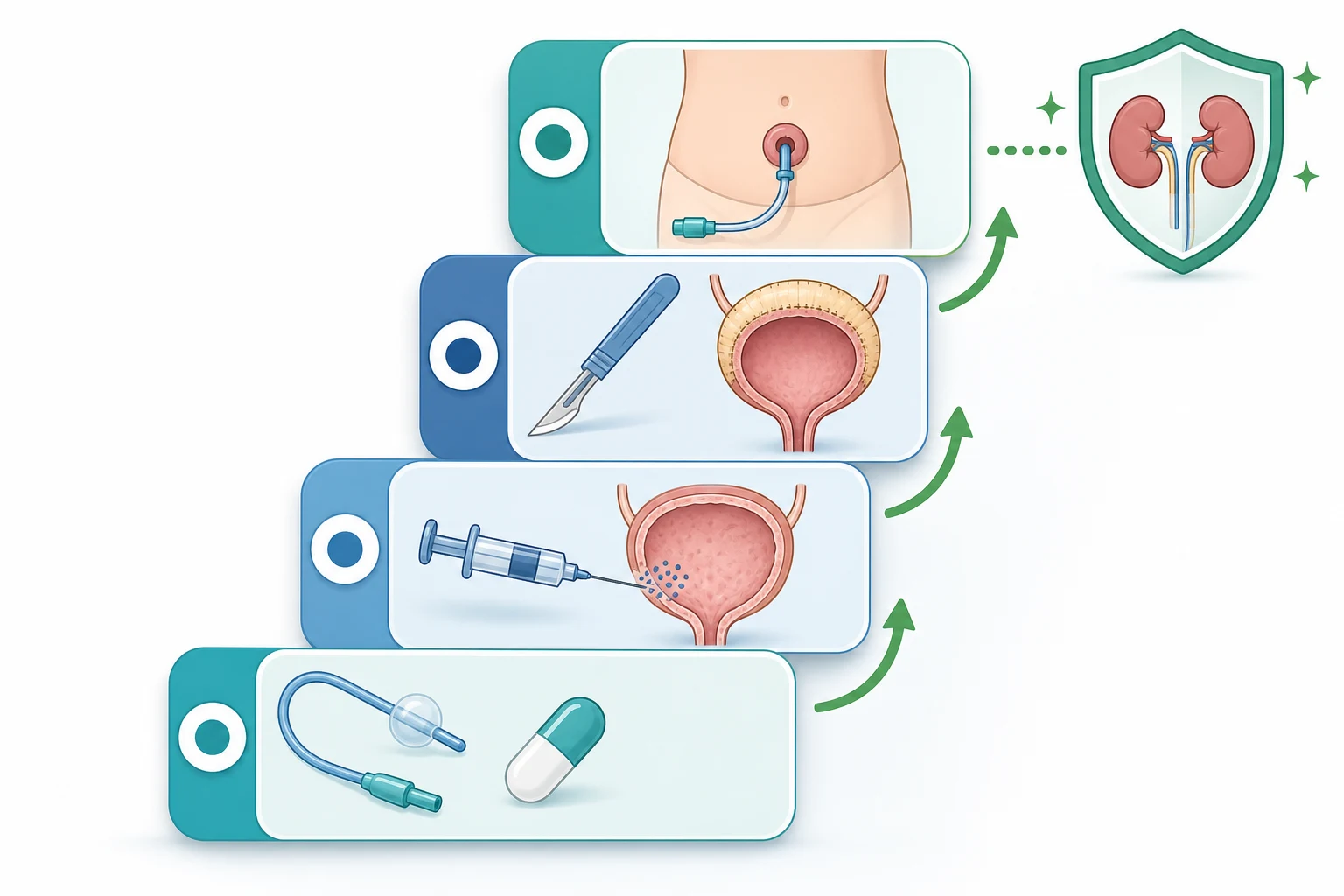
The goal of management is stated up front and repeated at every visit: a low-pressure, continent, completely emptied bladder that protects the kidneys. Every step in the ladder is judged against that goal, and the urodynamics rather than the symptoms decide whether the bladder is safe. The ladder for the neurogenic bladder and the simpler pathway for the functional disorders are shown in the management figure. [6]
The first-line treatment of the neurogenic bladder is clean intermittent catheterisation combined with an anticholinergic. Clean intermittent catheterisation, performed every 3 to 4 hours, empties the bladder completely and at low pressure regardless of the sphincter behaviour, and it is the single intervention that most preserves the upper tracts. It is begun in infancy in the child with a high-pressure bladder, and the parents are taught the technique so that it becomes routine. To make the bladder store at a low pressure while the catheterisation empties it, an anticholinergic is added to relax the detrusor and abolish the involuntary contractions. [8]
Oxybutynin for neurogenic detrusor overactivity
Dose
0.2 mg per kg per dose twice daily in the young child, titrated to a maximum of 5 mg per dose; or the extended-release formulation 5 to 15 mg once daily in the older child
The anticholinergics act by blocking the M3 muscarinic receptor on the detrusor, which abolishes the involuntary contractions and improves the bladder capacity and compliance. Noh and colleagues confirmed in their meta-analysis that anticholinergics are effective and generally well tolerated in children with overactive bladder, and the same class is the backbone of pharmacotherapy for the neurogenic bladder. The common side effects are dry mouth, constipation, and flushing, and in young children the central effects of oxybutynin — irritability and behavioural change — reflect its penetration of an immature blood-brain barrier, which is why tolterodine or solifenacin are sometimes preferred. [11]
Management ladder for the neurogenic bladder
Assess the bladder with video-urodynamics and the upper tracts with ultrasound in infancy in spina bifida
Start clean intermittent catheterisation every 3 to 4 hours and an anticholinergic such as oxybutynin
Repeat urodynamics to confirm the storage pressure has fallen and the upper tracts are protected
Add intravesical botulinum toxin for refractory detrusor overactivity despite anticholinergics and catheterisation
Reserve bladder augmentation and a continent catheterisable channel (Mitrofanoff or Monti) for the end-stage hostile bladder
Maintain lifelong surveillance of blood pressure, renal function, and the upper tracts, with transition to adult care
The second-line treatment for refractory detrusor overactivity is intravesical botulinum toxin. When the bladder remains high-pressure despite catheterisation and an anticholinergic, onabotulinumtoxinA is injected into the detrusor, typically at a dose of 200 units spread across about 30 injection sites and sparing the trigone, under general anaesthesia. Austin and colleagues showed that onabotulinumtoxinA reduces the detrusor overactivity, increases the bladder capacity, and lowers the storage pressures in children with neurogenic detrusor overactivity, and Franco and colleagues confirmed that the repeated treatments remain safe and well tolerated over the long term. The effect lasts for 6 to 9 months, so the injections are repeated, and the child stays on catheterisation throughout. [9]
The surgical options are reserved for the end-stage hostile bladder that cannot be controlled medically. A bladder augmentation (enterocystoplasty) enlarges the bladder with a segment of bowel to create a low-pressure reservoir, and a continent catheterisable channel such as a Mitrofanoff (appendix) or a Monti (reconfigured bowel) is fashioned on the abdominal wall so that the child or carer can catheterise easily and discreetly. An alpha-blocker such as doxazosin, or botulinum toxin of the external sphincter, is used when the problem is emptying failure from a dyssynergic or tight sphincter. A vesicostomy is a temporary diversion used in the infant whose bladder cannot be managed otherwise until the child is old enough for definitive surgery. These are major undertakings with lifelong consequences, and they are the last resort, not the first. [8]
The functional disorders are managed very differently, with behaviour first and medication only when behaviour fails. The pillars are bladder training and timed voiding (voiding by the clock every 2 to 3 hours regardless of urge), aggressive treatment of constipation (because a loaded rectum perpetuates the voiding dysfunction), adequate fluid intake, and biofeedback to teach the child to relax the pelvic floor during voiding. An anticholinergic is added for a severe overactive bladder that does not respond to behaviour, and the meta-analysis evidence supports its use, but it is never the first move. The functional disorders are benign and usually resolve with this approach, and the role of the clinician is to support the family, exclude a cord lesion, and treat the bowel. [4]
Specific Subtypes & Scenarios
The spina bifida neurogenic bladder is the scenario the examiner returns to. The infant needs urodynamics in the first months of life, and a high-pressure bladder is started on clean intermittent catheterisation and an anticholinergic from infancy. Joseph and colleagues, in the spina bifida urologic guidelines, emphasise that proactive management from birth preserves the upper tracts in the majority of children, and that the goal is continence and renal protection through childhood and into adulthood. The bowel is managed in parallel, because faecal incontinence is as important to the child's quality of life as urinary incontinence. [6]
The valve bladder is the hostile bladder that follows the ablation of posterior urethral valves, and it behaves like a neurogenic bladder even though the cord is intact. The chronic obstruction in utero remodels the bladder wall into a thick, low-compliance reservoir that stores poorly and generates high pressures, and these pressures damage the upper tracts over years. The valve bladder needs urodynamics after the ablation and management akin to the neurogenic bladder — anticholinergics, and clean intermittent catheterisation when the emptying fails. Snow-Lisy and colleagues highlight the valve bladder as a key driver of the long-term renal outcome in posterior urethral valves. [5]
Sacral agenesis, classically the caudal regression syndrome of maternal diabetes, produces a mixed neurogenic bladder whose pattern depends on the level of the agenesis, and it may coexist with anorectal and lower-limb malformations in the VACTERL association. Occult spinal dysraphism — a lipomeningocele, a tethered cord, or diastematomyelia — presents as apparent dysfunctional voiding with back or leg signs, and it needs an MRI and neurosurgical referral for untethering. The neurogenic bladder of cerebral palsy is usually an overactive bladder complicated by immobility and severe constipation, managed along the same principles. [7]
The adolescent with a neurogenic bladder is the transition scenario. The young person takes over the catheterisation and the continence management, the renal surveillance is continued, and the care is handed to adult urology and nephrology services. The transition is planned over years rather than at a single appointment, and the goals — continence, renal protection, and quality of life — are restated for the adult phase. Bladder cancer surveillance begins in adulthood, because the neurogenic bladder carries a long-term risk of malignancy that the adult service must own. [5]
Complications & Pitfalls
The dominant complication is progressive renal damage, and it is the reason the neurogenic bladder is taken so seriously. The mechanism runs from the high storage pressure to the upper tracts: hydronephrosis, vesicoureteral reflux, recurrent pyelonephritis, renal scarring, hypertension, and chronic kidney disease that may progress to end-stage kidney disease. The prevention is the maintenance of a low-pressure, completely emptied bladder from infancy, and the surveillance is the regular renal ultrasound, blood pressure, and creatinine. [6]
The other complications are the recurrent urinary tract infection from incomplete emptying and stasis, the bladder stones from the same stasis and from foreign bodies such as catheters, and the bladder cancer that appears in adulthood in the chronically catheterised or augmented bladder. The augmented bladder brings its own complications — mucus production, metabolic acidosis from the bowel segment, and a small but real risk of malignancy in the bowel — which is why surgery is the last resort. [5]
The classic pitfalls are diagnostic. The first is labelling a cord lesion as a functional disorder: a child with a tethered cord or a lipomeningocele presents as dysfunctional voiding, and the lesion is missed unless the back and legs are examined and an MRI obtained. The second is delaying the urodynamics in spina bifida, on the assumption that an infant in nappies needs no bladder assessment, when in fact the high-pressure bladder damages the upper tracts silently in the first months. The third is relying on symptoms rather than urodynamics to judge whether a neurogenic bladder is safe, because a bladder can be hostile and the child dry, or compliant and the child wet. The urodynamics, not the continence, decide whether the bladder is safe for the kidneys. [7]
Prognosis & Disposition
The prognosis for renal function is determined by whether the bladder is kept low-pressure and completely emptied from infancy. Proactive management with clean intermittent catheterisation and anticholinergics preserves the upper tracts in the majority of children with spina bifida, and the children who progress to chronic kidney disease are most often those whose hostile bladder was not identified and treated early. The renal surveillance — blood pressure, creatinine, and renal ultrasound at least annually — is the safety net that catches the child whose bladder is escaping control. [6]
The prognosis for continence is good with the modern ladder. Most children with a neurogenic bladder achieve social continence with catheterisation and anticholinergics, with botulinum toxin added when needed, and only a minority come to augmentation. The functional disorders have an excellent prognosis, resolving in the great majority of children with behavioural therapy and constipation treatment, and the role of the clinician is reassurance and the exclusion of a cord lesion. [4]
The disposition is lifelong surveillance. The child with a neurogenic bladder stays under the joint care of urology, nephrology, and the spina bifida or continence service, with the upper tracts monitored and the bladder management adjusted as the child grows. The transition to adult care is planned in adolescence, because the renal and continence needs persist into adulthood, and the adult service inherits the surveillance of renal function, blood pressure, and bladder cancer. [5]
Special Populations
The child with complex neurodisability, such as severe cerebral palsy or the technology-dependent child with spina bifida, needs an individualised continence plan that fits the child's mobility, cognition, and care arrangements. Clean intermittent catheterisation may be performed by the carer, the anticholinergic is titrated to the side-effect profile, and the bowel is managed in parallel, because the combination of urinary and faecal incontinence defines the quality of life. The coordination with rehabilitation and the community nursing service is as important as the medical prescription. [6]
Indigenous and remotely located children face real barriers to the urodynamic surveillance and the continence supplies that the neurogenic bladder demands. The urodynamics are a tertiary service, the catheter supplies are ongoing, and the travel burden is high, which is why the outreach and telehealth link the regional hospital to the tertiary centre and the continence programme. The higher background burden of renal disease in Aboriginal and Torres Strait Islander children lowers the threshold for nephrology involvement in any child with a neurogenic bladder. [6]
The adolescent needs a structured transition to adult continence and nephrology services, with the young person taking ownership of the catheterisation and the surveillance, and the adult service inheriting the bladder-cancer surveillance. The constipated child needs the bowel treated alongside the bladder, because untreated constipation perpetuates the voiding dysfunction and undermines the bladder management. The child in out-of-home care or with psychosocial adversity may have a functional voiding disorder driven by stress, and the behavioural and psychological input is central to the management alongside the medical care. [4]
Evidence, Guidelines & Regional Differences
The evidence base and the guidance are anchored by the International Children's Continence Society (ICCS), whose standardisation documents define the terminology, the urodynamics, the diagnostic evaluation of the congenital neuropathic bladder, and the treatment of daytime incontinence. Austin and colleagues set the terminology that the whole field uses; Bauer and colleagues standardised the urodynamics and the diagnostic pathway for the congenital neuropathic bladder and bowel dysfunction; and Chang and colleagues standardised the treatment of daytime urinary incontinence. These documents are the framework within which the neurogenic and the functional disorders are assessed and managed. [1]
OnabotulinumtoxinA for neurogenic detrusor overactivity in children (Austin 2021)
Key finding
OnabotulinumtoxinA injected into the detrusor reduced the detrusor overactivity, increased the bladder capacity, and lowered the storage pressures in children with neurogenic detrusor overactivity, with the effect sustained over repeated treatments.
Practice change
Intravesical botulinum toxin is the standard second-line agent for the neurogenic bladder that is refractory to an anticholinergic and clean intermittent catheterisation, and it has delayed or avoided bladder augmentation in many children.
The spina bifida guidance is set out by Snow-Lisy and colleagues in their update on the urological management of spina bifida from prenatal diagnosis to adulthood, and by Joseph and colleagues in the urologic guidelines for the care of people with spina bifida. Both emphasise the proactive approach — early urodynamics in infancy, clean intermittent catheterisation and anticholinergics for the high-pressure bladder, and lifelong renal surveillance. Sager and colleagues reviewed the medical treatment of the neurogenic bladder, and the botulinum toxin trials of Austin and Franco established the long-term safety of the repeated injections. [5]
[6]The regional differences are practical rather than conceptual. The folate fortification of food has reduced the birth prevalence of myelomeningocele, but the disease persists, and the access to urodynamics, continence supplies, and specialist surgery varies with the setting. In the well-resourced settings the proactive approach is the standard, while in the lower-resource settings the later presentation with established renal damage is more common, and the emphasis shifts to the prompt drainage of retention, the treatment of infection, and the maintenance of the renal function. The ICCS framework is global, but its application is adapted to the local resources. [3]
Exam Pearls
The single most testable fact is that spina bifida is the classic cause of a paediatric neurogenic bladder, and that the goal of management is a low-pressure, continent, completely emptied bladder that protects the kidneys. Clean intermittent catheterisation combined with an anticholinergic such as oxybutynin is the first-line treatment, intravesical botulinum toxin is the second-line agent for refractory detrusor overactivity, and bladder augmentation with a continent catheterisable channel is the last resort. The detrusor leak point pressure above 40 cm of water predicts upper-tract damage, and video-urodynamics is the gold-standard test, done in infancy in spina bifida. [6]
SAFE BLADDER for the management goals of the neurogenic bladder
Which child needs an MRI of the spine rather than biofeedback?
A child with new or progressive bladder symptoms, or any child whose dysfunctional voiding does not respond to standard behavioural therapy, needs a careful back and lower-limb examination. A sacral dimple, a hair tuft, a lipoma, a deviated gluteal cleft, lower-limb weakness, a foot deformity, or a gait abnormality are the findings that prompt an MRI of the spine to look for an occult dysraphism such as a tethered cord. Biofeedback is for the child with a normal back and legs.
[7]The examiner also rewards the dose knowledge. Oxybutynin is given at 0.2 mg per kg per dose twice daily in the young child, titrated to a maximum of 5 mg per dose, with the extended-release formulation 5 to 15 mg once daily in the older child. OnabotulinumtoxinA is injected into the detrusor at a typical dose of 200 units, sparing the trigone, and the effect lasts 6 to 9 months. Clean intermittent catheterisation is performed every 3 to 4 hours. The prophylactic antibiotic for the recurrent infection is trimethoprim 2 mg per kg at night. And the threshold that predicts the upper-tract damage is the detrusor leak point pressure above 40 cm of water. These are the numbers that turn a general answer into a fellowship answer. [8]
References
- [1]Austin PF, Bauer SB, Bower W, Chase J, Franco I, Hoebeke P, et al The standardization of terminology of lower urinary tract function in children and adolescents: update report from the Standardization Committee of the International Children's Continence Society. J Urol, 2014.PMID 24508614
- [2]Bauer SB, Nijman RJ, Drzewiecki BA, Sillen U, Hoebeke P International Children's Continence Society standardization report on urodynamic studies of the lower urinary tract in children. Neurourol Urodyn, 2015.PMID 25998310
- [3]Bauer SB, Austin PF, Rawashdeh YF, von Gontard A, Hoebeke P, Sillen U, et al International Children's Continence Society's recommendations for initial diagnostic evaluation and follow-up in congenital neuropathic bladder and bowel dysfunction in children. Neurourol Urodyn, 2012.PMID 22532312
- [4]Chang SJ, Van Laecke E, Bauer SB, von Gontard A, Bagli D, Sillen U, et al Treatment of daytime urinary incontinence: A standardization document from the International Children's Continence Society. Neurourol Urodyn, 2017.PMID 26473630
- [5]Snow-Lisy DC, Yerkes EB, Cheng EY Update on Urological Management of Spina Bifida from Prenatal Diagnosis to Adulthood. J Urol, 2015.PMID 25839383
- [6]Joseph DB, Baum MA, Tanaka ST, Hollatz P, Masand RP, Worley SE, et al Urologic guidelines for the care and management of people with spina bifida. J Pediatr Rehabil Med, 2020.PMID 33252091
- [7]Le HK, Cardona-Grau D, Chiang G Evaluation and Long-term Management of Neurogenic Bladder in Spinal Dysraphism. NeoReviews, 2019.PMID 31792158
- [8]Sager C, Barroso U Jr, Bastos JM Netto, Ortiz V, Macedo A Jr Management of neurogenic bladder dysfunction in children update and recommendations on medical treatment. Int Braz J Urol, 2022.PMID 33861059
- [9]Austin PF, Franco I, Dobremez E, Bauer SB, Lopez Pereira P, Hoebeke P, et al OnabotulinumtoxinA for the treatment of neurogenic detrusor overactivity in children. Neurourol Urodyn, 2021.PMID 33305474
- [10]Franco I, Hoebeke PB, Dobremez E, Fathallah S, Kline D, Naidich J, et al Long-term Safety and Tolerability of Repeated Treatments With OnabotulinumtoxinA in Children With Neurogenic Detrusor Overactivity. J Urol, 2023.PMID 36655470
- [11]Noh JW, Lee B, Kim JH Efficacy and safety of anticholinergics for children or adolescents with idiopathic overactive bladder: systematic review and meta-analysis. Int Urol Nephrol, 2019.PMID 31243632
- [12]Clothier JC, Wright AJ Dysfunctional voiding: the importance of non-invasive urodynamics in diagnosis and treatment. Pediatr Nephrol, 2018.PMID 28567611