Paeds · nephrology-urology-fluids-and-electrolytes
Nocturnal enuresis
Also known as Bedwetting in children · Monosymptomatic nocturnal enuresis · Non-monosymptomatic nocturnal enuresis · Primary nocturnal enuresis · Secondary nocturnal enuresis · Sleep enuresis
Fellowship guide to nocturnal enuresis (bedwetting) in children: the International Children's Continence Society definition of involuntary voiding during sleep from age five, the split into monosymptomatic versus non-monosymptomatic and primary versus secondary, the three pathophysiological mechanisms of reduced arousal, nocturnal polyuria from inadequate vasopressin and reduced bladder capacity, the clinical assessment built on the voiding diary and urinalysis, first-line therapy with the enuresis alarm or desmopressin at 200 to 400 micrograms orally or 120 to 360 micrograms sublingually with mandatory evening fluid restriction, combination therapy for partial responders, and the red flags that reclassify the problem as organic or neurological disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The organising idea of this topic is that bedwetting is a treatable condition driven by three reconcilable mechanisms, and the first decision is always whether daytime symptoms are present. The International Children's Continence Society frames the whole pathway around that idea: confirm the child is five or older, separate monosymptomatic from non-monosymptomatic disease, exclude the red flags with a focused history and urinalysis, and then offer first-line therapy with the alarm or desmopressin. [1] [2] Almost every child with monosymptomatic enuresis does well; the danger sits in the child with daytime symptoms or systemic features who is mislabelled as a simple bedwetter and denied the daytime or organic work-up that changes the plan.
This page covers the ICCS definition, the monosymptomatic and primary-versus-secondary classification, the three-systems pathophysiology, the clinical assessment built on the voiding diary and urinalysis, first-line alarm and desmopressin therapy with exact doses and the fluid-restriction safety rule, combination therapy and the second-line agents, and the red flags that demand investigation. It links to the leaves on daytime urinary incontinence, constipation, polyuria and polydipsia, and obstructive sleep apnoea, because enuresis often coexists with each of these and the first step is to recognise when it does. [3]
Overview & Definition
A school-age child who wets the bed almost every night is the picture most clinicians carry of nocturnal enuresis, and it is the right place to start. The International Children's Continence Society defines nocturnal enuresis as intermittent involuntary voiding during sleep in a child aged five years or older. [1] The word intermittent matters: the child is continent by day and the wetting is a sleep phenomenon, which separates enuresis from continuous incontinence and from the wetting of a neurogenic bladder. The age threshold of five reflects the developmental point by which most children are reliably dry at night, so wetting below that age is usually normal variation rather than disease. [2]
Enuresis is common, which is part of why the definition carries an age threshold rather than treating any wetting as abnormal. About 15 per cent of five-year-olds wet the bed, falling to around 7 per cent at ten years and 1 to 3 per cent at fifteen, and each year about 15 per cent of affected children become dry without treatment. [3] This favourable natural history shapes the counselling: most children resolve spontaneously, but the psychosocial cost of waiting can be high, which is why active treatment is offered to the child who is distressed rather than watchful waiting alone.
The practical first question after confirming the diagnosis is whether the wetting is monosymptomatic. Monosymptomatic nocturnal enuresis is bedwetting with no daytime lower urinary tract symptoms, and it is the form that flows directly into alarm or desmopressin therapy. Non-monosymptomatic nocturnal enuresis adds daytime urgency, frequency, daytime incontinence, holding postures or an abnormal stream, and it demands a different first step in which the daytime symptoms and any constipation are addressed before the night. [1] Getting this single distinction right at the first consultation is what keeps the rest of the pathway on track.
Classification
Classification begins with the daytime history, because it is the daytime symptoms that decide the pathway. Monosymptomatic enuresis, with bedwetting and nothing else, is the commonest form seen in primary care and the form that responds to the standard first-line options. Non-monosymptomatic enuresis, with daytime symptoms layered on the bedwetting, behaves differently and is more likely to need urotherapy, an anticholinergic and a longer course to dryness. [1] [2]
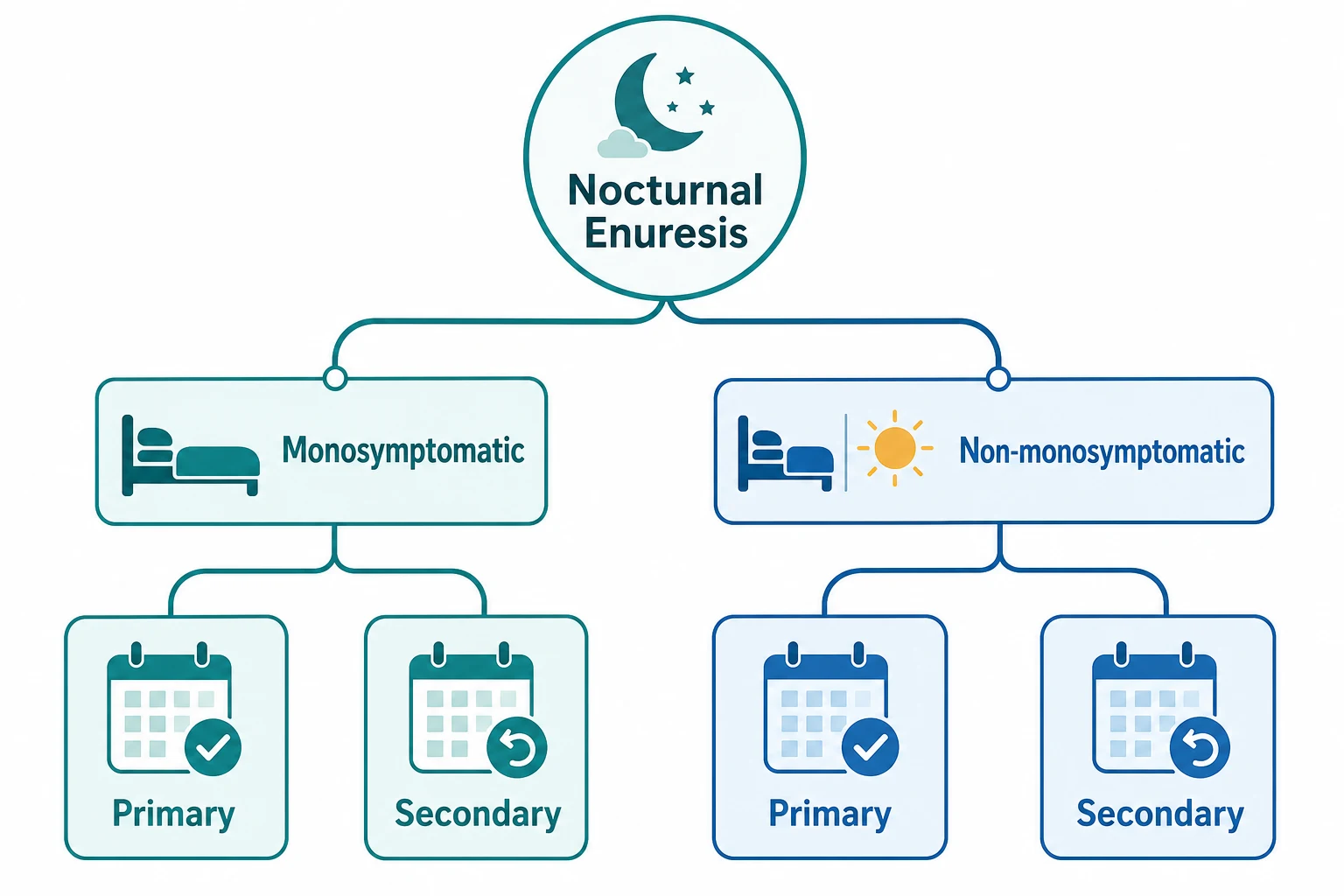
The second axis is the onset. Primary enuresis means the child has never been dry for a continuous six-month period, and it is the typical developmental form. Secondary enuresis means the child achieved dryness for at least six months and then relapsed, and it should prompt a search for a trigger such as urinary tract infection, constipation, diabetes, sleep-disordered breathing or a psychosocial stressor. [3] A previously dry child who starts wetting again is never assumed to be a simple variant, because the relapse often points to a remediable cause.
Monosymptomatic versus non-monosymptomatic nocturnal enuresis
Epidemiology & Risk Factors
The prevalence of bedwetting falls steadily through childhood, which is the single most useful epidemiological fact for counselling families. About 15 per cent of five-year-olds wet the bed, around 7 per cent of ten-year-olds, and only 1 to 3 per cent of fifteen-year-olds, with about 15 per cent of affected children resolving spontaneously each year. [3] Boys are affected about twice as often as girls in the early school years, and the sex difference narrows by adolescence.
The strongest risk factor is a positive family history, and the pattern is strikingly autosomal dominant. A child has about a 44 per cent chance of enuresis if one parent was enuretic and about a 77 per cent chance if both parents were, and the age at which the parent achieved dryness tends to predict the child's. [12] This family pattern is reassuring to share with parents, because it reframes the bedwetting as an inherited maturational delay rather than a behavioural failing.
The modifiable associations are the ones a clinician can act on. Constipation, often unrecognised, worsens bladder function and is present in a substantial minority of enuretic children. Urinary tract infection can precipitate or worsen wetting. Sleep-disordered breathing from adenotonsillar hypertrophy is a recognised contributor, and psychosocial stress frequently underlies secondary enuresis. [3] Identifying and treating each of these is part of every first assessment, because removing them can resolve the wetting before any specific therapy is started.
Pathophysiology
Bedwetting in the monosymptomatic child is best understood as a mismatch between how much urine the night produces and how much the bladder can hold, compounded by a brain that does not wake to the signal of fullness. These three mechanisms work together, and each one points to a treatment. [1]
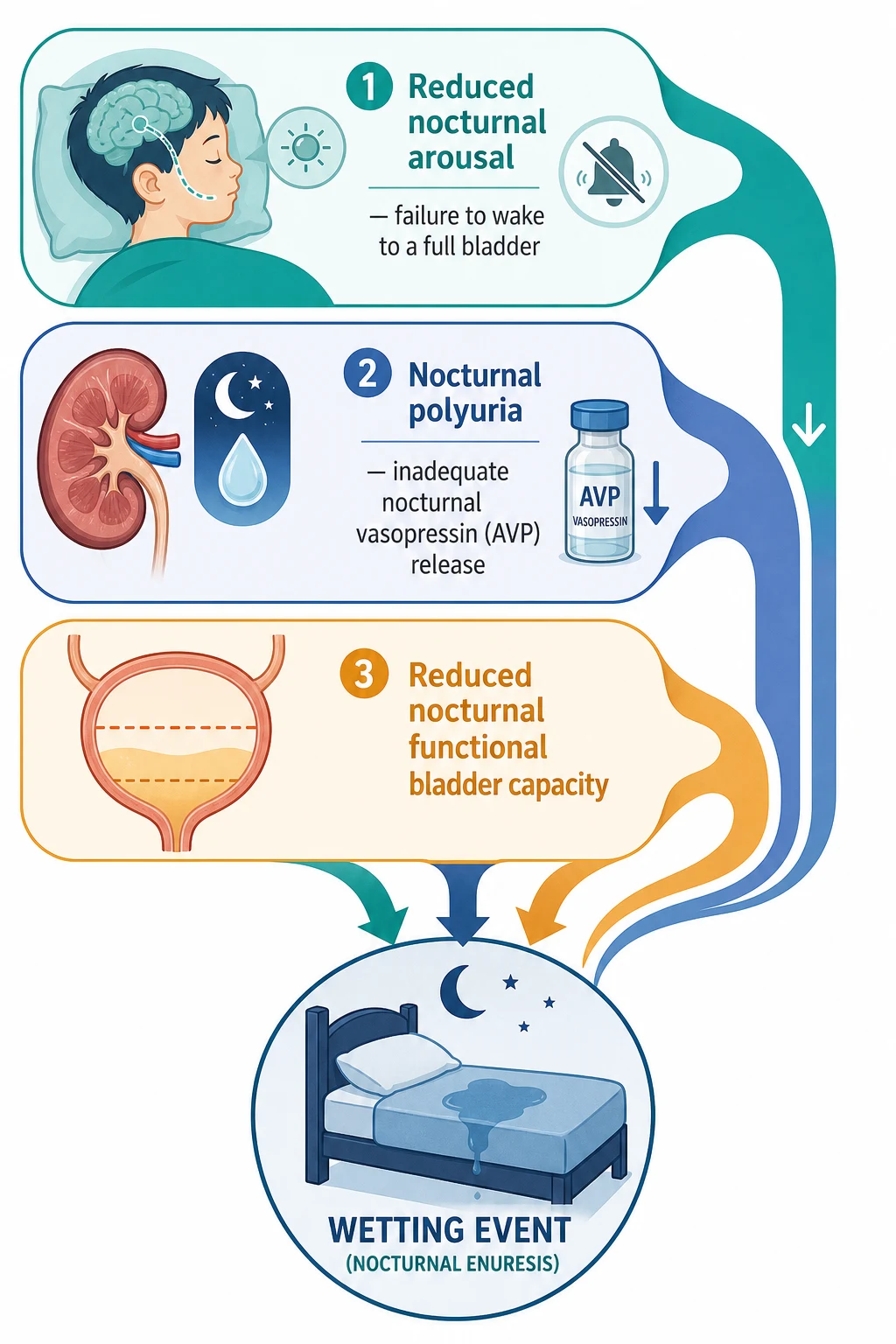
The first mechanism is nocturnal polyuria. Most children show a nocturnal rise in arginine vasopressin that concentrates the urine and reduces overnight volume, but many enuretic children do not mount this rise, so they produce a large volume of dilute urine through the night. When that overnight volume exceeds what the bladder can hold, the child wets. This is the mechanism that desmopressin targets directly, replacing the missing nocturnal vasopressin signal and concentrating the urine. [4]
The second mechanism is a reduced nocturnal functional bladder capacity. Some enuretic children have a bladder that overfills at a lower volume overnight, whether from detrusor overactivity or a genuinely small capacity, so they wet even when the overnight urine volume is normal. This mechanism is the rationale for urotherapy and, in selected children with non-monosymptomatic disease, an anticholinergic such as oxybutynin. [1]
The third mechanism is the arousal deficit. The enuretic child tends to be a deep sleeper who does not wake to the signal of bladder fullness, which is why bedwetting clusters in the first third of the night and why the alarm, which pairs the sensation of wetting with waking, can condition the child to arouse. [5] The three mechanisms rarely act in isolation, and most children have a combination, which is why combination therapy is so effective when a single agent gives only a partial response.
Clinical Presentation
The typical child presents at five to seven years with bedwetting on most nights, an otherwise normal history, and parents who are either worried or quietly resigned. A positive family history is common, and many families have tried restriction, lifting or rewards without success. The child is usually well, growing normally and dry by day. [2]
The presentation of non-monosymptomatic enuresis is different and must be actively sought, because families lead with the night-time problem and may not mention the daytime signs. Ask directly about daytime urgency, frequency, daytime wetting, crossing the legs or holding postures, a hesitant or interrupted stream, and posturing that suggests voiding dysfunction. Any of these changes the diagnosis and moves the daytime symptoms and constipation to the front of the plan. [1]
The psychological and social presentation is as important as the wetting itself. Children with enuresis commonly have lower self-esteem, shame and anxiety, and they may avoid sleepovers, school camps and overnight visits that their peers take for granted. Family conflict over the wetting is common, and punishment is harmful and never appropriate. A central reason to treat enuresis actively is that these psychological harms reverse when the wetting stops. [10]
Differential Diagnosis
The first differential is always between monosymptomatic and non-monosymptomatic enuresis, settled by the daytime history. A child with no daytime symptoms, a normal stream, a normal examination and a normal urinalysis has monosymptomatic enuresis and does not need further investigation. A child with any daytime symptom, an abnormal stream, recurrent infection or neurological signs has non-monosymptomatic or organic disease and enters a different pathway. [1]
The second differential is the cause of secondary enuresis, because a previously dry child who relapses is owed a search for a trigger. Urinary tract infection, constipation, diabetes mellitus, sleep-disordered breathing and psychosocial stress are the common explanations, and each is sought in the history and on urinalysis. [3]
Causes of secondary enuresis to consider and exclude
The third differential is the organic and neurological cause that masquerades as simple bedwetting. An abnormal urinary stream suggests obstruction such as posterior urethral valves. Continuous dribbling, faecal incontinence, a sacral dimple or hair tuft, asymmetrical buttock creases, or lower-limb neurological signs suggest occult spinal dysraphism and a neurogenic bladder. Recurrent urinary tract infection suggests an underlying structural or functional abnormality. Each of these demands imaging, specialist referral and a work-up, not alarm therapy. [3]
Clinical & Bedside Assessment
The assessment is built on a structured voiding and fluid history and a focused examination, and it is designed to detect the daytime and systemic red flags rather than to image an otherwise well child. Ask about the number of wet nights, the size of the wetting, daytime symptoms, bowel habit, the pattern of fluid intake through the day, sleep and snoring, the psychosocial context, and the family history of bedwetting. [1]
The voiding and fluid diary is the core assessment tool, kept over at least three and ideally seven days. It records the timing and volume of each void, the fluid intake, the wet and dry nights, and the morning void. From it the clinician can estimate the overnight urine volume and compare it with the expected bladder capacity for age, which identifies nocturnal polyuria and points to desmopressin, or a small functional bladder capacity, which points to urotherapy and possibly an anticholinergic. [2]
Focused assessment of the child with bedwetting
Confirm the child is five years or older and take a structured voiding, fluid, bowel, sleep and family history.
Ask explicitly about daytime urgency, frequency, daytime wetting, holding postures and the urinary stream.
Keep a voiding and fluid diary for at least three days to quantify overnight urine volume and bladder capacity.
Examine the abdomen, genitalia, spine and lower limbs, and measure growth and blood pressure.
Perform urinalysis to exclude infection, diabetes and a renal concentrating defect.
The physical examination is usually normal in monosymptomatic enuresis, and that normality is itself reassuring. Examine the abdomen for a distended bladder or faecal loading, inspect the genitalia, examine the spine for a sacral dimple, hair tuft or lipoma, and examine the lower limbs for tone, strength, reflexes and the feet for asymmetry or deformity. Measure the height and weight and plot them, and check the blood pressure. An abnormal finding in any of these redirects the child away from simple alarm or desmopressin therapy. [3]
Investigations
Urinalysis is the single most important investigation, and in monosymptomatic enuresis it is often the only one needed. A dipstick checks the specific gravity to assess concentrating ability, glucose to exclude diabetes mellitus, protein to screen for renal disease, and leucocytes and nitrites to screen for urinary tract infection. An abnormal result prompts culture or further testing; a normal result in the well child confirms that the bedwetting is functional. [2]
The voiding and fluid diary is the second investigation, and it is functional rather than laboratory. As well as guiding therapy, it documents the baseline wetting against which treatment response is judged, because a meaningful reduction in wet nights is the outcome that matters and it cannot be judged without a baseline count. [1]
Imaging and urodynamics are not routine, and ordering them reflexively in the well child with monosymptomatic enuresis is a pitfall. A renal tract ultrasound, urodynamics or further imaging is reserved for the non-monosymptomatic child, the child with recurrent urinary tract infection, the child with an abnormal examination, or the child who fails first-line therapy. [3]
[1] [3]Management — Resuscitation
Nocturnal enuresis is not a resuscitation diagnosis, but one presentation demands urgent action. The child with new polyuria, polydipsia and weight loss has diabetes mellitus until proven otherwise, and the assessment is capillary blood glucose and urinalysis for glucose and ketones without delay. Hyperglycaemia with ketonuria is diabetic ketoacidosis pending, and the child is managed along the diabetic emergency pathway rather than the continence pathway. [3]
Before any specific therapy, every child receives the foundational measures that apply across the whole pathway. These are education and reassurance that destigmatise the wetting, advice on a regular intake of most fluids earlier in the day with a reduction in the evening, regular daytime voiding, treatment of constipation, and treatment of any urinary tract infection. [6] No child is punished for bedwetting, and the family's expectation and motivation are gauged because they shape the choice between the alarm and desmopressin.
Active treatment is then offered to the school-age child whose bedwetting is distressing, rather than reassurance and watchful waiting alone. The favourable spontaneous resolution rate does not justify leaving a distressed child wet, because the self-esteem and social harms are real and reverse with treatment, and because effective first-line therapy exists. [10]
Management — Definitive & Stepwise
The choice of first-line therapy is shared with the family and turns on three questions: how quickly does the family need a result, is the child's wetting driven by nocturnal polyuria, and is the family motivated and able to use an alarm? The two first-line options are the enuresis alarm and desmopressin, and each fits a different answer to those questions. [1]
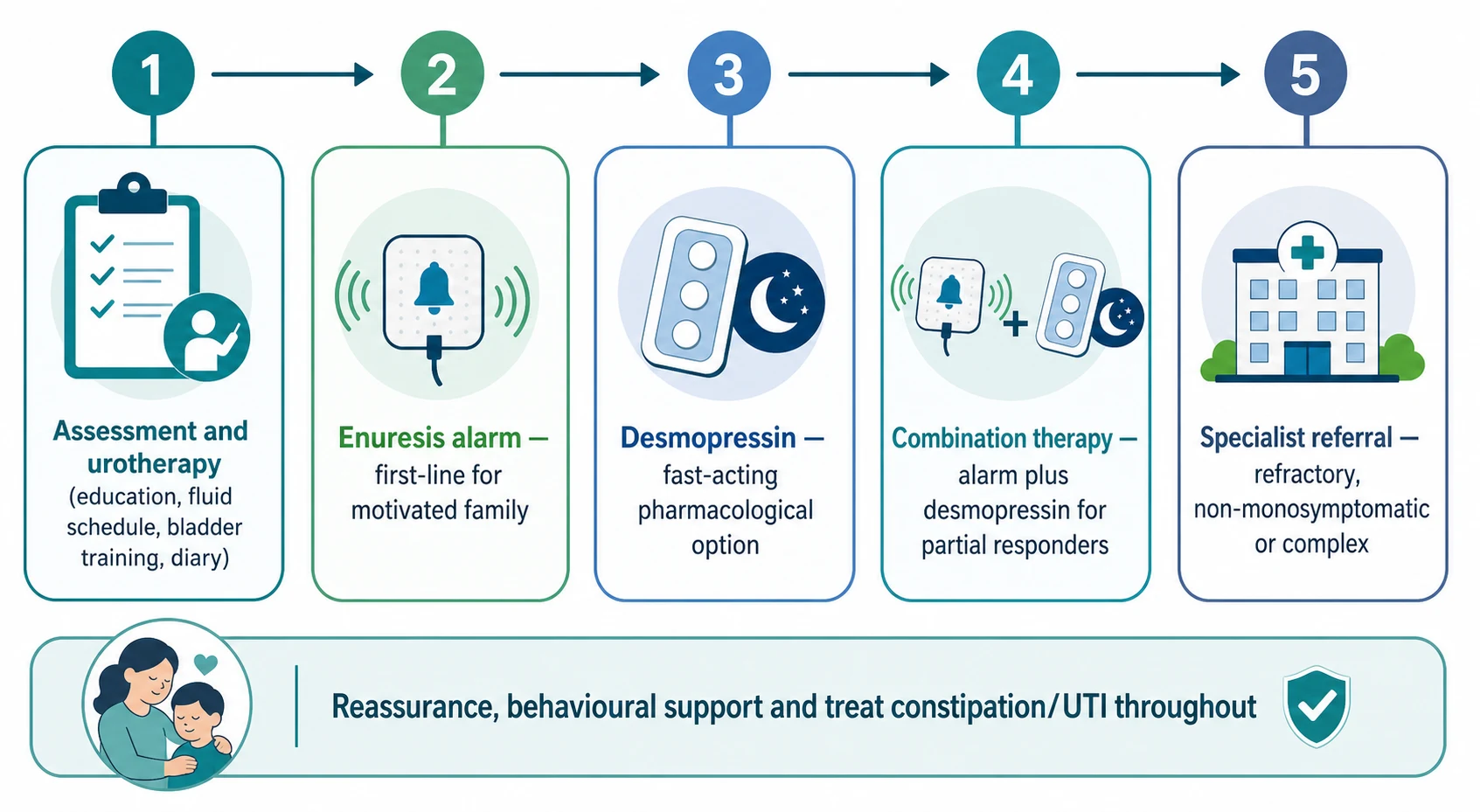
The enuresis alarm is first-line for the motivated family wanting a durable cure. It sounds at the first drops of urine and pairs the sensation of wetting with waking, conditioning the child to arouse to a full bladder, and about two-thirds of children who persist with it achieve dryness. [5] The alarm takes weeks to work and demands a committed family who will wake with the child, which is why it is offered to families who want a long-term cure rather than a quick result.
Desmopressin (first-line pharmacotherapy)
Dose
Oral tablets 200 micrograms at bedtime, titrated up to 400 micrograms if needed; OR sublingual lyophilisate (MELT) 120 micrograms at bedtime, titrated up to 360 micrograms
Desmopressin is first-line pharmacotherapy and has a rapid effect, which makes it the choice when nocturnal polyuria is the driver, when a quick result is needed for a sleepover or camp, or when the family cannot manage an alarm. The oral tablet starts at 200 micrograms at bedtime and is titrated to 400 micrograms, and the sublingual lyophilisate starts at 120 micrograms and is titrated up to 360 micrograms. [4] [9] Skoog's randomised trial established the dose-response and the superiority of desmopressin over placebo, and the MELT formulation offers a practical alternative for children who cannot swallow tablets. [8] [9]
Combination therapy with the alarm plus desmopressin is more effective than either alone and is the next step for the child who only partially responds to a single agent. The network meta-analysis of first-line therapies ranked the combination among the most effective options, and it is the standard approach for the partial responder. [11] When desmopressin alone is stopped, the relapse rate is high, so a structured taper or an overlap with the alarm is used to sustain dryness rather than an abrupt withdrawal. [4]
Specific Subtypes & Scenarios
The monosymptomatic child is the commonest scenario and the one for whom the standard pathway is built. The family chooses between the alarm and desmopressin guided by the urine-volume phenotype, the need for speed and the family's capacity to commit to an alarm, and combination therapy is held in reserve for the partial responder. [1]
The non-monosymptomatic child follows a different order. The daytime symptoms and any constipation are assessed and treated first, usually with urotherapy and an anticholinergic such as oxybutynin, and the night is addressed once the daytime pattern is improved. [3] Treating non-monosymptomatic enuresis as if it were monosymptomatic is a common error that delays dryness, because the daytime bladder dysfunction is the rate-limiting step.
The child who needs short-term dryness for a sleepover, a school camp or a holiday is served by desmopressin, which gives rapid and predictable control within days. [4] This is a legitimate and common use, provided the family is taught the fluid-restriction rule and the drug is used for the event rather than abandoned abruptly afterwards.
The adolescent and the treatment-resistant child need a more deliberate approach. Combination therapy, attention to adherence and comorbidity, a search for unrecognised daytime symptoms or constipation, and occasionally a third-line agent are considered, and referral to a continence or specialist service is appropriate for the child who has not responded to a well-conducted first-line course. [10]
Imipramine (third-line, with caution)
Dose
25 to 75 mg orally at night according to age and weight, short course with review
Imipramine, a tricyclic antidepressant, reduces wet nights while the child takes it, but the relapse rate on cessation is high and the drug is cardiotoxic in even modest overdose. [7] For these reasons it is a third-line option reserved for the resistant case under specialist guidance, used in short courses with secure storage, and never a first-line agent. The anticholinergic oxybutynin has a defined role in the non-monosymptomatic child with detrusor overactivity, where it is combined with urotherapy rather than used as a standalone bedwetting cure. [3]
Complications & Pitfalls
The principal harms of untreated enuresis are psychological and social rather than physical. Children with persistent bedwetting have lower self-esteem, higher rates of emotional and behavioural difficulty, and restricted participation in sleepovers, camps and social life, and these harms are reversible when the wetting is treated. [10] This is the clinical case for active treatment of the distressed school-age child rather than waiting for spontaneous resolution.
The first pitfall is misclassifying non-monosymptomatic enuresis as monosymptomatic. A child whose daytime urgency, frequency or wetting is missed is sent down the alarm-or-desmopressin pathway when the rate-limiting step is the daytime bladder dysfunction and constipation. [1] Asking explicitly about daytime symptoms at the first consultation is the safeguard, because families do not always volunteer them.
The second pitfall is the desmopressin fluid-restriction error. Giving desmopressin without restricting evening fluids, or continuing it through an illness with fluid imbalance, risks water intoxication and hyponatraemic seizures. [4] The rule is taught at every prescription: restrict fluids from one hour before the dose until eight hours after, and withhold during vomiting, diarrhoea or systemic illness.
The third pitfall is over-reliance on imipramine. Its cardiotoxicity in overdose, its high relapse rate on cessation and the availability of safer effective first-line options make it a drug to use sparingly and under supervision, with secure storage to protect siblings. [7] The fourth pitfall is investigating the well monosymptomatic child reflexively with ultrasound and urodynamics, when urinalysis and a diary are sufficient and therapy is the next step. [3]
Prognosis & Disposition
The prognosis of nocturnal enuresis is favourable. About 15 per cent of affected children resolve spontaneously each year, and the response rates to the alarm and desmopressin in motivated families are high. [3] The child who achieves dryness with the alarm tends to stay dry, while the child who responds to desmopressin relapses on withdrawal unless a structured taper or alarm overlap is used to sustain the gain. [4]
Most children are managed in primary care and general paediatric outpatient settings, and the family is empowered to monitor wet and dry nights at home and to lead the alarm therapy. Referral to a continence service, paediatric urology or nephrology is reserved for treatment-resistant disease, non-monosymptomatic enuresis that does not respond to urotherapy and an anticholinergic, and any child with an organic or neurological cause. [10] The child with an organic or neurological cause has a prognosis determined by that cause and requires specialist-led care from the outset.
Special Populations
Children with developmental disability and neurodiversity may need behavioural and alarm therapy adapted to their communication, toileting readiness and sensory profile. The principles do not change, but the pace, the rewards and the involvement of carers and educators are tailored, and a continence or developmental service often supports the plan. [3]
The child with constipation and faecal incontinence is a common and important overlap, because a loaded bowel impairs bladder function and bedwetting often persists until the bowel is managed. Treating the constipation with disimpaction and a maintenance regimen is a prerequisite for dryness, and the two problems are managed together rather than in sequence. [3]
The child with sleep-disordered breathing is another recognised overlap. Adenotonsillar hypertrophy and obstructive sleep apnoea contribute to enuresis in some children, so a sleep history looking for loud snoring and witnessed apnoeas is part of the assessment, and adenotonsillectomy resolves the enuresis in a proportion of these children. [3]
Families in rural and remote settings, and those from socioeconomically disadvantaged, migrant and refugee backgrounds, face practical barriers to the alarm, including disrupted sleep and shared rooms, and the cost and maintenance of equipment. Desmopressin, telehealth-supported review and language-appropriate education are practical priorities, and the threshold for offering an effective first-line option rather than watchful waiting is lower where access is constrained. [10]
Evidence, Guidelines & Regional Differences
The two frameworks that shape practice are the International Children's Continence Society updated standardization document of 2020 and the NICE clinical guideline on bedwetting in children and young people. The ICCS document sets the definition, the monosymptomatic and non-monosymptomatic classification, and the place of the alarm and desmopressin, and the NICE guideline translates this into a stepwise management pathway for primary and secondary care. [1] The Hjälmås evidence-based strategy and the Kuwertz-Bröking clinical review underpin the assessment and treatment framework. [2] [3]
The principal evidence points are that both desmopressin and the alarm reduce wet nights, that the alarm gives more durable dryness at the cost of slower and effortful treatment, and that combination therapy is the most effective option for the partial responder. [10] The network meta-analysis ranked the combination of alarm and desmopressin among the most effective first-line-based strategies, confirming the clinical practice of combining them when a single agent gives only a partial response. [11]
A regional and safety difference worth knowing is that the intranasal desmopressin spray is no longer recommended for enuresis because of a higher risk of hyponatraemia, and the oral tablet and sublingual lyophilisate routes are preferred. [4] The MELT formulation, compared with the tablet in the Lottmann trial, offers a practical alternative for children who cannot swallow tablets and has a comparable effect. [9]
Exam Pearls
Three rules that mark a fellowship answer
The high-yield minutiae an examiner rewards: enuresis is defined from age five; about 15 per cent of five-year-olds wet the bed with 15 per cent spontaneous resolution each year; boys exceed girls early on; the family risk is about 44 per cent with one parent and 77 per cent with both; the three mechanisms are arousal, nocturnal polyuria and bladder capacity; the alarm gives durable dryness in about two-thirds of committed families; desmopressin is 200 to 400 micrograms orally or 120 to 360 micrograms sublingually with strict evening fluid restriction; combination therapy is the most effective option for partial responders; imipramine is third-line because it is cardiotoxic in overdose and relapses on cessation; and the red flags are daytime symptoms, diabetes, an abnormal stream, neurological signs and recurrent infection. [1] [4] [11]
References
- [1]Nevéus T; Fonseca E; Franco I; et al Management and treatment of nocturnal enuresis-an updated standardization document from the International Children's Continence Society. J Pediatr Urol, 2020.PMID 32278657
- [2]Hjälmås K; Arnold T; Bower W; et al Nocturnal enuresis: an international evidence based management strategy. J Urol, 2004.PMID 15118418
- [3]Kuwertz-Bröking E; von Gontard A Clinical management of nocturnal enuresis. Pediatr Nephrol, 2018.PMID 28828529
- [4]Hahn D; Stewart F; Raman G Desmopressin for nocturnal enuresis in children. Cochrane Database Syst Rev, 2025.PMID 40728007
- [5]Glazener CM; Evans JH; Peto RE Alarm interventions for nocturnal enuresis in children. Cochrane Database Syst Rev, 2005.PMID 15846643
- [6]Caldwell PH; Nankivell G; Sureshkumar P Simple behavioural interventions for nocturnal enuresis in children. Cochrane Database Syst Rev, 2013.PMID 23881652
- [7]Caldwell PH; Sureshkumar P; Wong WC Tricyclic and related drugs for nocturnal enuresis in children. Cochrane Database Syst Rev, 2016.PMID 26789925
- [8]Skoog SJ; Stokes A; Turner KL Oral desmopressin: a randomized double-blind placebo controlled study of effectiveness in children with primary nocturnal enuresis. J Urol, 1997.PMID 9258137
- [9]Lottmann H; Froeling F; Alloussi S; et al A randomised comparison of oral desmopressin lyophilisate (MELT) and tablet formulations in children and adolescents with primary nocturnal enuresis. Int J Clin Pract, 2007.PMID 17655682
- [10]Moretti E; Barbosa L; da Silva IB; et al What do cochrane systematic reviews say about interventions for enuresis in children and adolescents? An overview of systematic reviews. J Pediatr Urol, 2022.PMID 35661613
- [11]Chen X; Zeng F; Tian N; et al Efficacy and safety of first-line therapies and first-line-based combination therapies for monosymptomatic nocturnal enuresis in children: a network meta-analysis. Pediatr Nephrol, 2026.PMID 41902910
- [12]von Gontard A; Heron J; Joinson C Family history of nocturnal enuresis and urinary incontinence: results from a large epidemiological study. J Urol, 2011.PMID 21511300