Paeds · nephrology-urology-fluids-and-electrolytes
Oliguria, anuria and urinary obstruction
Also known as Paediatric oliguria · Anuria in children · Post-renal obstruction · Obstructive uropathy · Post-obstructive diuresis · Urinary tract obstruction in children
Fellowship guide to oliguria, anuria and urinary obstruction in children: the urine output thresholds that define oliguria and anuria, the pre-renal, renal and post-renal framework with post-renal obstruction the focus, the pathophysiology of obstructive nephropathy where raised hydrostatic pressure collapses filtration, the emergency decompression of the urinary tract by catheter or nephrostomy, and the diagnosis and fluid management of post-obstructive diuresis that follows relief of a chronic obstruction.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child whose urine output has fallen to a trickle, or stopped altogether, is sending a signal that demands an answer before the biochemistry turns dangerous. Oliguria and anuria are not diagnoses but clinical signs measured at the bedside, and the first question is always whether the drop in output reflects a kidney that is under-perfused, a kidney that is injured, or a kidney that is blocked. This page focuses on the third possibility, the obstructed urinary tract, because it is the most readily reversible cause of acute kidney injury in children and because it carries a distinctive and testable complication in the period after the block is relieved. [1]
The thresholds that frame the whole assessment come from the KDIGO acute kidney injury criteria, summarised by Kellum and Lameire. Oliguria is a urine output below 0.5 mL per kg per hour for six hours or more, and anuria is the more severe reduction, defined by KDIGO as a urine output below 0.3 mL per kg per hour for 24 hours or more, or complete absence of urine for 12 hours or more. A stricter bedside convention defines anuria as below 0.1 mL per kg per hour or below 1 mL per kg per day, and the absence of any urine on catheterisation is the practical red flag that distinguishes true anuria from retention or a missed collection. [1]
The urgency comes from the speed with which a blocked kidney fails and the completeness with which it can recover if the obstruction is relieved early. Obstructive nephropathy is the term for the structural and functional injury that follows a block anywhere from the renal pelvis to the urethra, and it is the only major cause of paediatric acute kidney injury in which a single intervention, decompression, can reverse the entire process within hours. Delay converts a reversible problem into permanent scarring, which is why the obstructed child is a surgical and not merely a medical emergency. [3]
Classification
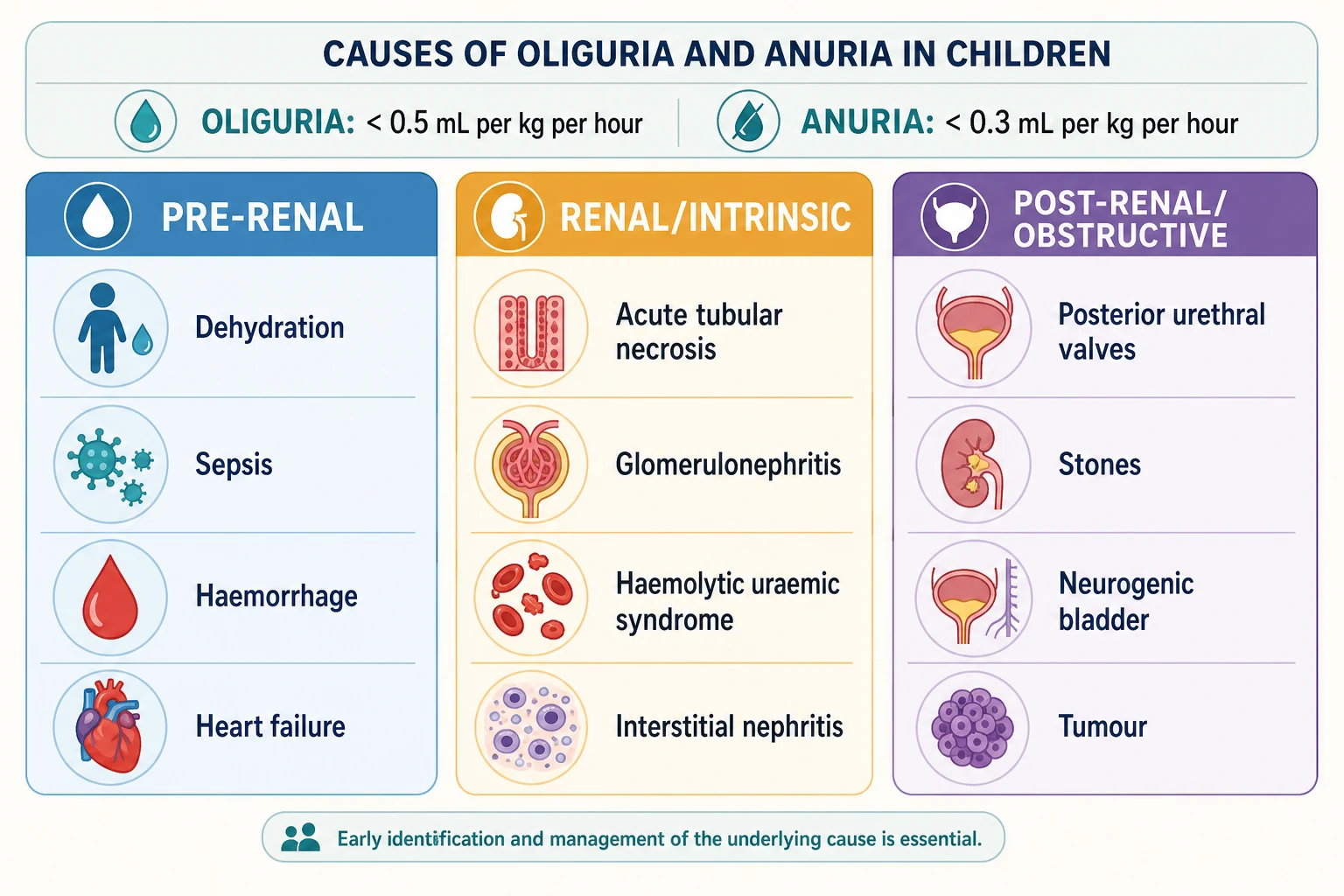
Oliguria and anuria are triaged by where the failure to make or pass urine originates, and the three anatomical levels carry different treatments. Pre-renal causes reduce the effective blood flow to a structurally intact kidney, so the output falls because the filtration pressure drops, and the injury reverses when perfusion is restored. Renal or intrinsic causes damage the nephron itself, from acute tubular necrosis through the glomerulonephritides and the haemolytic uraemic syndrome, and the recovery is slow and often incomplete. Post-renal causes obstruct the outflow tract, and this page makes the post-renal category its focus because obstruction is the reversible surgical emergency that a general paediatrician must not miss. [2]
Within the post-renal category the level of the block determines the cause and the approach. Lower tract obstruction, at the bladder outlet or urethra, is dominated in male infants by posterior urethral valves and in older children by a neurogenic bladder or a urethral stricture, and it presents with a palpable distended bladder and a poor stream. Upper tract obstruction, at the ureteropelvic or ureterovesical junction, presents with hydronephrosis and flank pain rather than a palpable bladder, and it causes anuria only when it is bilateral or affects a solitary kidney. A stone or a blood clot can lodge at either level and produce acute obstruction in a previously well child. [10]
Pre-renal
- Reduced effective renal perfusion with a structurally intact kidney
- Causes: dehydration, sepsis, haemorrhage, heart failure, third-space loss
- Rapidly reversible with fluid resuscitation
- Fractional excretion of sodium below 1 percent
Renal or intrinsic
- Structural damage to the tubules, glomeruli, or interstitium
- Causes: acute tubular necrosis, glomerulonephritis, haemolytic uraemic syndrome
- Recovery over days to weeks, may be incomplete
- Fractional excretion of sodium above 1 percent
Post-renal or obstructive
- Blockage of urinary outflow anywhere from renal pelvis to urethra
- Causes: posterior urethral valves, stones, neurogenic bladder, tumour
- Reversible with prompt decompression if relieved early
- Ultrasound shows hydronephrosis or a palpable distended bladder
The single most useful bedside distinction in a child who is not passing urine is whether the bladder is full. A distended, palpable bladder in an anuric or oliguric child points to lower tract obstruction and changes the immediate management from fluid resuscitation to catheterisation. A bladder that is empty and impalpable, by contrast, directs the search toward a pre-renal or renal cause, because the kidney is failing to make urine rather than being unable to pass it. This one physical sign, assessed before any imaging, often settles whether the first action is a catheter or a fluid bolus. [6]
Epidemiology & Risk Factors
Congenital obstructive uropathy is the single largest contributor to end-stage renal disease in children of urological origin, which is why Woolf and Thiruchelvam placed obstruction at the centre of the paediatric nephrology curriculum. Posterior urethral valves are the most common cause of lower urinary tract obstruction in male infants, with an incidence of roughly 1 in 4000 to 1 in 8000 male births, and they account for a substantial share of childhood chronic kidney disease attributable to a structural lesion. The burden falls heaviest on the youngest patients, because the obstructed fetal kidney develops fewer nephrons and the deficit is permanent. [10]
The long-term outcome data for posterior urethral valves now define the stakes. A systematic review and meta-analysis by Hafizar and colleagues found that a significant proportion of boys with posterior urethral valves progress to chronic kidney disease, and the population-based cohort study by Robinson and colleagues confirmed that the kidney outcomes remain poor even in the era of antenatal diagnosis and early valve ablation. These studies establish that obstruction in infancy is a life-long kidney disease, not an episode that ends when the valves are ablated. [4]
The risk factors for an obstructive presentation group by age and anatomy. In the neonate and young infant the dominant causes are congenital: posterior urethral valves, ureteropelvic junction obstruction, ectopic ureteroceles, and the neurogenic bladder of spina bifida. In the older child the causes shift toward acquired and acute events: urolithiasis causing ureteric obstruction, a clot from gross haematuria, and a pelvic or retroperitoneal tumour such as a rhabdomyosarcoma or lymphoma compressing the ureters. A child with a solitary kidney who develops an obstructing stone is at particular risk because a unilateral block produces complete anuria. [9]
Pathophysiology
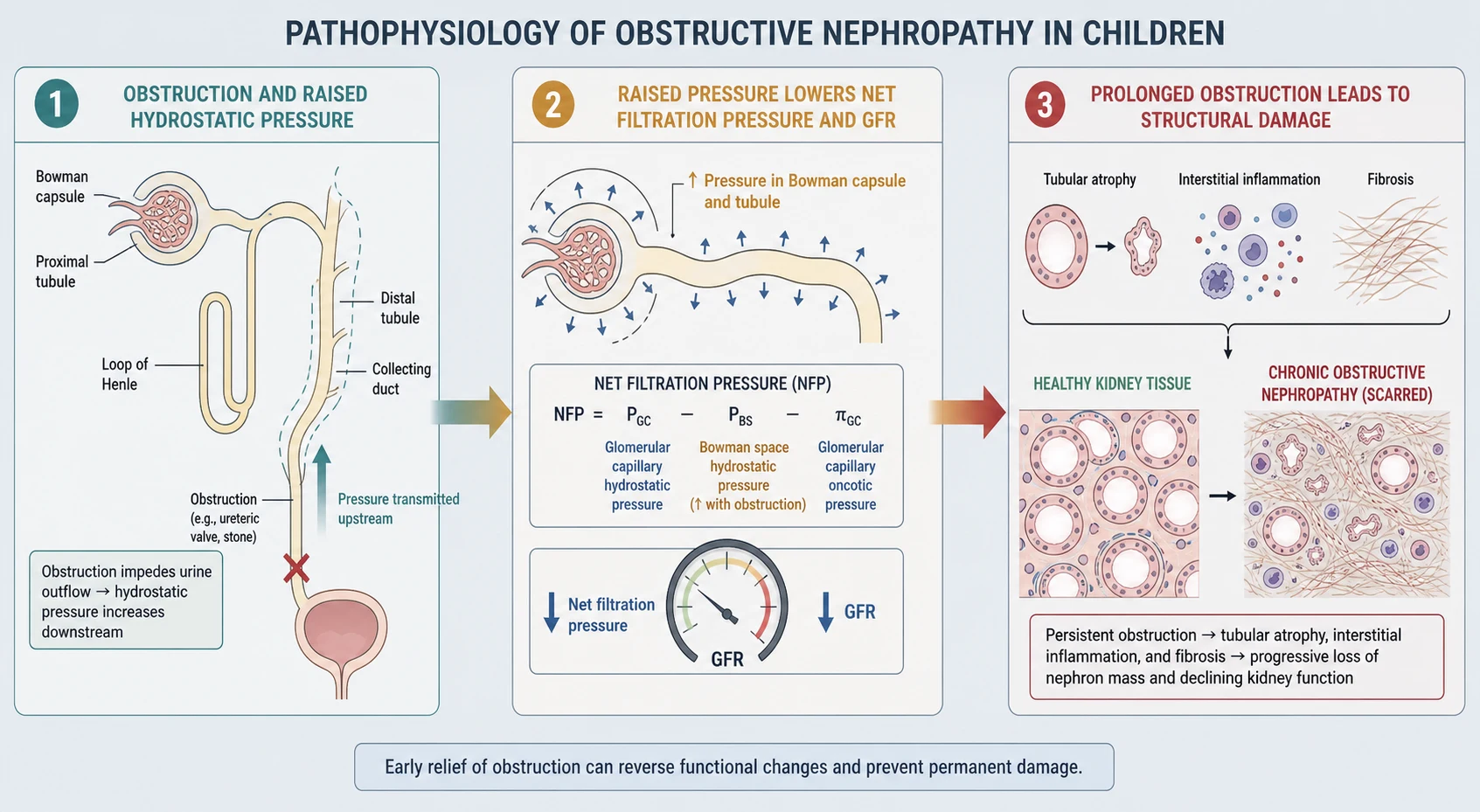
The mechanism by which obstruction injures the kidney is a story of pressure, and Molitoris framed it within the low-flow acute kidney injury paradigm alongside prerenal azotemia and abdominal compartment syndrome. A block anywhere in the outflow tract raises the hydrostatic pressure upstream, and that pressure transmits backwards through the collecting system into the tubules and the Bowman capsule. Because filtration depends on the pressure gradient between the glomerular capillary and the Bowman space, raising the pressure on the Bowman side narrows the gradient and the glomerular filtration rate falls. The kidney is structurally intact at this early stage, so relieving the obstruction restores the gradient and the filtration within hours. [2]
If the obstruction persists, the pressure-driven fall in filtration progresses to structural injury, and the molecular pathophysiology has been charted by Nørregaard and colleagues. Sustained raised pressure reduces the renal blood flow, triggers tubular cell apoptosis, and recruits an inflammatory cascade in the renal interstitium. The chronic obstruction also alters the renal tubular handling of sodium and water, which is the foundation of post-obstructive diuresis: the tubules lose their concentrating ability and their sodium-retaining capacity, so that once the obstruction is relieved they excrete large volumes of dilute urine rich in sodium. [3]
The duration of the obstruction is the critical determinant of whether the injury is reversible. Experimental and clinical data show that complete obstruction relieved within hours to a few days recovers fully, while obstruction lasting weeks causes tubular atrophy and interstitial fibrosis that do not recover. Partial obstruction, as in a ureteropelvic junction obstruction, may be tolerated for months because the pressure rise is gradual, but it too causes progressive nephron loss. This time-dependence is why a child with acute anuria from obstruction is a surgical emergency, not a problem to be observed overnight. [3]
Clinical Presentation
The presentation of an obstructed child spans the spectrum from a male infant discovered to have a palpable bladder on a routine check to an older child in acute renal failure with a stone lodged in a solitary ureter. The common thread is reduced or absent urine output in the presence of a structural block, and the tempo ranges from the acute anuria of a stone to the chronic partial obstruction of a ureteropelvic junction abnormality that presents with flank pain and hydronephrosis rather than anuria. [9]
The lower tract obstruction of posterior urethral valves presents in the male infant with a weak urinary stream, a palpable distended bladder, and sometimes a palpable abdominal mass from the distended bladder or the hydronephrotic kidneys. The antenatal history may reveal bilateral hydronephrosis, a thick-walled bladder, and oligohydramnios, and the postnatal course includes failure to pass urine in the first 24 hours of life, poor weight gain, or a febrile urinary tract infection. A neonate who has not passed urine by 24 hours of life must be assessed for obstruction, renal agenesis, and severe dysplasia. [6]
The upper tract obstruction of a ureteropelvic junction abnormality presents differently, because the block is above the bladder and the bladder empties normally. The child passes urine but develops hydronephrosis, flank or abdominal pain, and sometimes a palpable flank mass in infancy. Anuria occurs only when the obstruction is bilateral or affects a solitary kidney, and it presents as acute oliguria with flank pain, the picture of a renal emergency. A stone obstructing a ureter produces the acute, colicky flank pain of renal colic, and bilateral stones or a stone in a solitary kidney produce anuria. [9]
Recognising the obstructed child at the bedside
Reduced or absent urine output, or failure to void in the first 24 hours of life
Palpable distended bladder suggesting lower tract obstruction
Poor or dribbling urinary stream in a male infant suggesting valves
Flank or abdominal mass from a hydronephrotic kidney
Flank pain or renal colic suggesting an upper tract stone
Bilateral hydronephrosis on antenatal or postnatal ultrasound
Oliguria or anuria with a known solitary kidney
The neurogenic bladder of spina bifida or a spinal cord lesion presents with a different pattern: chronic retention with overflow incontinence, recurrent urinary tract infections, and a palpable bladder, rather than acute anuria. The child may be mislabelled as having primary incontinence when the bladder is in fact obstructed at the outlet by detrusor-sphincter dyssynergia. A careful history of the voiding pattern, the bowel function, and the neurological status, and an examination of the spine and the lower limbs, direct the clinician to the neurogenic cause before the kidneys are damaged. [12]
Differential Diagnosis
The first distinction in the oliguric or anuric child is between obstruction and the pre-renal and renal causes, because the management diverges immediately. A pre-renal cause is suggested by the signs of volume depletion or shock, a renal cause by the casts and the pattern of a glomerulonephritis or a haemolytic uraemic syndrome, and a post-renal cause by the palpable bladder and the hydronephrosis on ultrasound. The abdomen and the renal ultrasound do most of the work of separating the three, and a urinary catheter both diagnoses and treats a lower tract obstruction. [2]
Within obstruction, the differential is by the level and the cause. Lower tract causes include posterior urethral valves, a urethral stricture, a prolapsing ureterocele, a neurogenic bladder, and a pelvic tumour such as a rhabdomyosarcoma of the bladder base. Upper tract causes include ureteropelvic junction obstruction, ureterovesical junction obstruction, an obstructing stone, a retroperitoneal tumour, and retroperitoneal fibrosis. The age of the child, the antenatal history, and the imaging pattern narrow the differential rapidly. [9]
Lower tract obstruction
- Block at the bladder outlet or urethra
- Causes: posterior urethral valves, neurogenic bladder, urethral stricture
- Palpable distended bladder and a poor stream
- Catheterisation both diagnoses and treats
Upper tract obstruction
- Block at the ureteropelvic or ureterovesical junction
- Causes: ureteropelvic junction obstruction, stones, tumour, retroperitoneal fibrosis
- Hydronephrosis and flank pain, bladder empties normally
- Anuria only if bilateral or in a solitary kidney
Acquired acute obstruction
- Sudden block in a previously well child
- Causes: obstructing stone, clot from gross haematuria, fungal ball
- Acute colicky pain or abrupt anuria
- Emergency decompression or urology referral
The key mimics of obstruction are the conditions that produce a falsely low urine output. A missed or incomplete urine collection in an infant, a child who has just voided, and a dry nappy that was changed late can all mimic oliguria, which is why the anuric child must be catheterised to confirm the diagnosis. Acute tubular necrosis produces oliguria or anuria without obstruction, and the renal ultrasound is normal. Bilateral renal vein thrombosis in a neonate produces anuria with enlarged tender kidneys, and bilateral renal agenesis produces anuria with absent kidneys and a Potter sequence, both of which the ultrasound distinguishes from obstruction. [2]
Clinical & Bedside Assessment
The bedside assessment of the oliguric or anuric child runs in parallel with the first interventions and answers two questions in order: is there a palpable bladder, and is the child in immediate biochemical or haemodynamic danger. The airway, breathing, and circulation are assessed and stabilised, the volume status is judged clinically, and the abdomen is palpated for a distended bladder and flank masses. A strict fluid balance chart, a daily weight, and an accurate measurement of the urine output are essential, and a urinary catheter is placed early both to measure the output and to relieve a suspected lower tract obstruction. [1]
The abdominal examination is the highest-yield bedside manoeuvre in the obstructed child. A palpable, dull, suprapubic mass that does not empty with gentle pressure is a distended bladder, and in a male infant it points to posterior urethral valves until proven otherwise. A ballotable flank mass suggests a hydronephrotic kidney, and bilateral flank masses in a neonate suggest bilateral hydronephrosis or polycystic kidneys. The spine is examined for the sacral dimple, hair tuft, or lipoma of occult spinal dysraphism that accompanies a neurogenic bladder, and the lower limb reflexes and tone are checked. [12]
The cardiovascular examination seeks the signs of shock or dehydration that would make the cause pre-renal and volume-responsive, and the hypertension that accompanies volume overload or renal disease. The blood pressure is checked against age-appropriate centiles, because a raised blood pressure in an oliguric child suggests renal disease or volume excess. A 12-lead ECG is performed immediately if hyperkalaemia is suspected or confirmed, looking for the peaked T waves and the widened QRS that herald cardiac arrest, because the obstructed child with an acute kidney injury is at risk of the same hyperkalaemia that complicates any acute kidney injury. [1]
Investigations
The investigations confirm the obstruction, locate the level, and detect the complications. The cornerstone is the renal tract ultrasound, which is the first-line imaging in any child with oliguria, anuria, or a palpable bladder. It shows the hydronephrosis that confirms an upper tract obstruction, the dilated ureter that locates the level, the distended thick-walled bladder of a lower tract obstruction, and the post-void residual that quantifies incomplete emptying. It also distinguishes obstruction from the medical causes of acute kidney injury, where the ultrasound is typically normal, and from chronic kidney disease, where the kidneys are small and echogenic. [11]
The urinary tract dilation classification system, updated by Nguyen and colleagues, standardises the reporting of hydronephrosis and guides the decision between surveillance and intervention. The system grades the anteroposterior renal pelvic diameter and the presence of calyceal or ureteral dilation, peripheral cortical thickness, and bladder abnormalities, into low-risk and increased-risk categories that determine the follow-up imaging and the threshold for a diuresis renogram or surgical referral. A standardised report allows the clinician to compare serial ultrasounds and to communicate the severity consistently across centres. [11]
The blood tests reveal the complications that drive the acute danger, and they are identical to the panel for any acute kidney injury. The serum creatinine is checked against a baseline, the potassium is checked urgently because the obstructed child can develop hyperkalaemia, and the venous or arterial blood gas reveals the metabolic acidosis. The sodium may be low from water retention, and the full blood count shows anaemia in chronic kidney disease or a high white cell count in pyelonephritis or pyonephrosis behind an obstructed system. The urinalysis and urine microscopy may show haematuria and crystals in a stone, or pus cells and bacteria in an infected obstructed system. [1]
Where the ultrasound confirms a dilated system but the functional significance is unclear, a diuresis renogram with a radiotracer and a diuretic challenge distinguishes an obstructed from a non-obstructed dilation, as reviewed by Bayne and colleagues. This is reserved for the older infant and child with a ureteropelvic junction obstruction in whom the decision to operate depends on the functional impairment, not for the acute anuric child who needs immediate decompression. A computed tomography without contrast is occasionally used in the older child with a suspected stone when the ultrasound is nondiagnostic, but it is avoided in the young child because of the radiation dose and the risk of contrast nephropathy. [9]
Management — Resuscitation
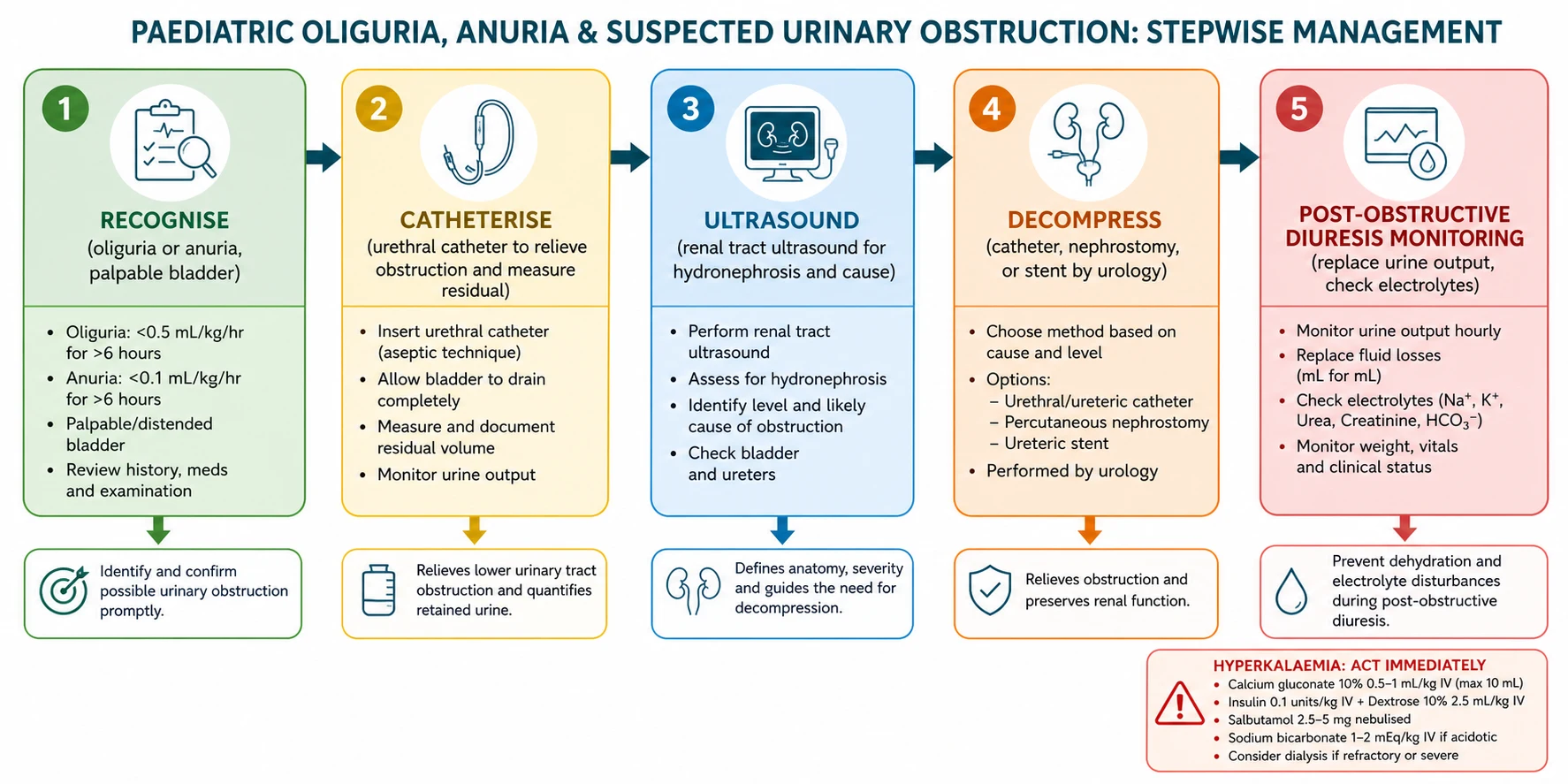
Resuscitation addresses the immediate threats to life and the obstruction in parallel. The airway and breathing are stabilised and the intravenous access is established, and a bedside glucose is checked. The central early intervention in the obstructed child is the urinary catheter, which both confirms the diagnosis and relieves a lower tract obstruction. A urethral catheter is passed, and if it drains a large volume of retained urine the diagnosis of lower tract obstruction is confirmed and the bladder is decompressed. [1]
If a urethral catheter cannot be passed, as in posterior urethral valves where the catheter coils at the obstruction, the clinician does not persist traumatically but escalates to a suprapubic catheter or to urgent urological referral. The decompression must be achieved by whatever route reaches the bladder, because the relief of the obstruction is the single most important intervention for preserving renal function. A child with an upper tract obstruction that cannot be relieved by a bladder catheter, such as a ureteric stone or a tumour, needs urgent urological or interventional radiology referral for a nephrostomy or a stent. [6]
Urethral catheter for suspected lower urinary tract obstruction
Dose
An appropriately sized paediatric Foley catheter, 6 to 8 French for an infant and 8 to 12 French for an older child
Hyperkalaemia complicates an obstructive acute kidney injury as it does any acute kidney injury, and it is treated as an emergency in the same staged approach. A 12-lead ECG is checked, and if there are ECG changes, intravenous calcium gluconate is given to stabilise the myocardial cell membrane, followed by the agents that shift potassium into the cells. The potassium is rechecked after each intervention because the effect is transient, and the decompression of the obstruction addresses the underlying cause of the potassium retention. A child with refractory hyperkalaemia despite decompression needs renal replacement therapy. [1]
Volume resuscitation is given only if the child is clinically hypovolaemic or shocked, and not simply because the urine output is low, because the obstructed child who is volume-overloaded or in renal failure is harmed by further fluid. The volume status is assessed clinically, and a hypovolaemic child receives an isotonic crystalloid bolus of 10 to 20 mL per kg with reassessment after each bolus. Once the obstruction is relieved, the management shifts to the monitoring for post-obstructive diuresis and the replacement of the fluid and electrolyte losses, which is where the distinctive management of obstruction begins. [1]
Management — Definitive & Stepwise
[6]Definitive management is cause-specific and centres on the relief of the obstruction and the prevention of its recurrence. The lower tract obstruction of posterior urethral valves is treated by primary valve ablation, or by a temporary vesicostomy in the small or unstable infant who cannot tolerate the endoscopic ablation. The upper tract obstruction of a ureteropelvic junction abnormality is treated by a pyeloplasty, and an obstructing stone is treated by urological removal or medical expulsion therapy depending on the size and the position. A nephrostomy or a stent relieves an obstruction that cannot be treated definitively at the initial presentation, and a tumour receives oncological treatment alongside the relief of the obstruction. [6]
The distinctive post-decompression phase is the monitoring for post-obstructive diuresis, which is the hallmark of safe obstructive uropathy management. After the relief of a chronic obstruction, the kidney that has lost its concentrating ability produces a high volume of dilute, sodium-rich urine. A physiological diuresis is expected and lasts hours, but a pathological post-obstructive diuresis is defined as a urine output above 3 mL per kg per hour for several hours, or persisting beyond 24 hours, and it can deplete the intravascular volume and the electrolytes to the point of hypovolaemic shock, hyponatraemia, and hypokalaemia. [7]
The management of post-obstructive diuresis rests on measuring the urine output hourly and replacing a fraction of the losses. The urine output, the weight, the blood pressure, and the serum sodium and potassium are monitored every 6 to 12 hours, and the intravenous fluid is tailored to the urine output and the electrolytes. A common approach is to replace approximately half to two-thirds of the previous hour's urine output with an isotonic fluid, adjusted to the sodium content of the urine, so that the diuresis is controlled without provoking volume overload or allowing dehydration. The diuresis is self-limiting as the tubules recover their concentrating ability over days. [7]
Fluid replacement for post-obstructive diuresis
Dose
Replace approximately 50 to 75 percent of the previous hour's urine output with an isotonic fluid such as 0.9 percent sodium chloride
The classic error in post-obstructive diuresis is to replace the full urine output, which perpetuates the diuresis by maintaining the volume stimulus, or to under-replace, which allows hypovolaemia and electrolyte depletion. The other error is to miss the diuresis altogether, because the child who was oliguric and is now passing large volumes of urine is assumed to have recovered. The urine output is measured hourly, and any output above 3 mL per kg per hour that persists is treated as a post-obstructive diuresis until the concentrating ability recovers. [8]
A paediatric nephrologist and a paediatric urologist are involved early for any child with an obstructive uropathy, and the discharge plan addresses the definitive repair, the bladder and the bowel management in the neurogenic bladder, and the long-term nephrology follow-up. Every child who has had an obstructive episode is enrolled in kidney surveillance, because the meta-analysis evidence from the posterior urethral valves literature shows that the kidney risk persists long after the obstruction is relieved. [4]
Specific Subtypes & Scenarios
Posterior urethral valves are the prototype obstructive uropathy and the single most testable cause of lower tract obstruction in male infants. They present in the male neonate or infant with a palpable distended bladder, a poor urinary stream, and often a history of antenatal bilateral hydronephrosis and oligohydramnios. The immediate management is a urethral catheter to relieve the obstruction, followed by a voiding cystourethrogram to confirm the diagnosis and a primary valve ablation by a paediatric urologist. The long-term kidney outcome is the central issue: the systematic review by Hafizar and colleagues and the population-based cohort by Robinson and colleagues show that a substantial proportion progress to chronic kidney disease despite early ablation. [4]
Presentation
- Male infant with a palpable distended bladder
- Poor or dribbling urinary stream
- Antenatal bilateral hydronephrosis and oligohydramnios
- Failure to void in the first 24 hours of life
Diagnosis
- Renal ultrasound shows a dilated posterior urethra and thick-walled bladder
- Voiding cystourethrogram confirms the valve
- Bilateral hydronephrosis, often with renal dysplasia
- Creatinine elevated at presentation
Management
- Urethral catheter for immediate decompression
- Primary valve ablation by paediatric urology
- Vesicostomy in the small or unstable infant
- Life-long nephrology follow-up for chronic kidney disease
Ureteropelvic junction obstruction is the most common cause of upper tract obstruction and presents with hydronephrosis that is often detected antenatally. The block is at the junction of the renal pelvis and the ureter, and it produces a hydronephrosis without ureteral dilation. Most infants are managed conservatively with serial ultrasound and a diuresis renogram, and the obstruction is repaired by a pyeloplasty when the function declines or the dilation progresses. The child with a ureteropelvic junction obstruction presents with anuria only when the obstruction is bilateral or affects a solitary kidney, and that presentation is a surgical emergency. [9]
An obstructing urolithiasis produces acute upper tract obstruction and the colicky flank pain of renal colic, and bilateral stones or a stone in a solitary kidney produce anuria. The stone is located by a renal ultrasound, with a non-contrast computed tomography reserved for the older child when the ultrasound is nondiagnostic, and the management depends on the size and the position: a small stone may pass with hydration and analgesia, while a larger or an impacted stone needs urological removal or a nephrostomy to relieve the obstruction and protect the kidney. A rhabdomyolysis causing pigment nephropathy is a medical mimic that produces dark urine rather than an obstruction. [9]
The neurogenic bladder of spina bifida or a spinal cord lesion produces a chronic lower tract obstruction from detrusor-sphincter dyssynergia, and the EAU and ESPU guidelines by Stein and colleagues provide the framework for the conservative management. The child is managed with clean intermittent catheterisation, anticholinergic medication to lower the storage pressure, and regular surveillance of the renal tract, because a high-pressure bladder damages the kidneys over years. The presentation with anuria is uncommon, but the recurrent infections, the high-pressure storage, and the upper tract dilation are the everyday manifestations that the paediatrician must recognise and refer. [12]
[6]Complications & Pitfalls
The complications of an obstructive uropathy are the consequences of the raised pressure and the failed filtration, and they are the targets of the emergency decompression. Hyperkalaemia complicates an obstructive acute kidney injury as it does any acute kidney injury, and it can cause the cardiac arrest that the staged medical therapy and the decompression are designed to prevent. Metabolic acidosis develops as the failing kidney cannot excrete the acid, and fluid overload develops as the obstructed kidney cannot excrete the water, producing hypertension, pulmonary oedema, and a rising respiratory rate. [1]
Post-obstructive diuresis is the distinctive complication of relief, and it is the one most often missed. The kidney that has been obstructed loses its concentrating ability, and on decompression it produces a high volume of dilute, sodium-rich urine that can deplete the intravascular volume and the electrolytes. The classic error is to celebrate the return of the urine output and to miss the diuresis, so that the child develops hypovolaemic shock, hyponatraemia, and hypokalaemia hours after the successful decompression. The urine output is measured hourly after every decompression of a chronic obstruction. [7]
Infection behind an obstructed system is a surgical emergency. A pyelonephritis or a pyonephrosis in an obstructed kidney produces sepsis, and the management requires both the antibiotics and the decompression, because the antibiotics cannot reach an obstructed, pus-filled system. A child with a fever and an obstructed kidney is drained by a nephrostomy or a stent in addition to the antibiotic therapy, and the failure to decompress an infected obstruction is a classic and dangerous error. [6]
The classic diagnostic pitfalls begin with the assumption that a normal urine output excludes a problem. A child with an upper tract obstruction and a normal bladder passes urine normally, so the hydronephrosis is missed until the flank pain or the ultrasound brings it to light. The other error is to treat anuria with fluid boluses without palpating the bladder, when the cause is a lower tract obstruction that a catheter would relieve. Failing to catheterise the anuric child, and failing to monitor the urine output hourly after a decompression, are the two errors that most often lead to harm. [6]
Prognosis & Disposition
The prognosis of an obstructive uropathy depends on the duration of the obstruction before relief, the degree of the renal dysplasia in the congenital causes, and the occurrence of the complications. An acute obstruction that is relieved within hours to a few days recovers fully, because the early pressure-driven fall in filtration reverses when the gradient is restored. A chronic obstruction that is relieved after weeks causes tubular atrophy and interstitial fibrosis that do not recover, and the congenital causes such as posterior urethral valves carry a background of renal dysplasia that limits the recovery regardless of the timing. [3]
The long-term outcome of posterior urethral valves defines the prognosis of the whole category, and the evidence has shifted the practice toward life-long kidney surveillance. The systematic review by Hafizar and colleagues and the population-based cohort by Robinson and colleagues show that a substantial proportion of boys with posterior urethral valves progress to chronic kidney disease, and that the kidney outcomes remain poor even in the era of antenatal diagnosis and early valve ablation. This means that every boy with posterior urethral valves is enrolled in nephrology follow-up with serial blood pressure, creatinine, and urinalysis, because the kidney risk persists long after the valves are ablated. [5]
Disposition is to a paediatric intensive care unit for the child with severe hyperkalaemia, sepsis, or a complicated post-obstructive diuresis, and to a paediatric ward with a urology and a nephrology service for the child who is stable after decompression. The discharge plan addresses the definitive repair, the bladder and bowel management in the neurogenic bladder, and the long-term nephrology follow-up. The family is counselled on the prognosis honestly, with the emphasis on the likelihood of recovery of the acute injury and the importance of the life-long kidney surveillance. [5]
Special Populations
Neonates are the highest-risk group because the obstructed fetal kidney develops a permanent nephron deficit, and the congenital causes dominate the presentation. Posterior urethral valves, ureteropelvic junction obstruction, and ectopic ureteroceles present in the neonatal period, and the antenatal hydronephrosis directs the postnatal assessment. A neonate who has not passed urine by 24 hours of life is assessed for obstruction, renal agenesis, and renal dysplasia, and a palpable bladder is catheterised. The neonatal kidney is also more vulnerable to the hyperkalaemia and the fluid overload of an acute kidney injury, which is why the neonate with an obstruction is managed in a neonatal intensive care unit with nephrology and urology. [10]
Children with a neurogenic bladder from spina bifida or a spinal cord lesion are a special population because the obstruction is chronic and the management is lifelong. The EAU and ESPU guidelines frame the care around clean intermittent catheterisation, anticholinergic medication to lower the storage pressure, and the regular surveillance of the renal tract, because a high-pressure bladder damages the kidneys over years rather than acutely. The paediatrician's role is to recognise the high-pressure bladder, to support the catheterisation regimen, and to refer for the urological and the nephrological review when the upper tract dilation or the recurrent infections indicate a loss of the bladder control. [12]
Children in lower-resource settings present later and have less access to the paediatric urology and the nephrology, so the prevention through the antenatal diagnosis, the prompt catheterisation, and the early referral carries the greatest yield. Nasir and colleagues reported the short-term outcomes of boys with posterior urethral valves in a resource-limited setting, and the late presentation with sepsis and established renal failure was the dominant challenge. Aboriginal and Torres Strait Islander children and other Indigenous populations carry a higher background burden of chronic kidney disease and recurrent urinary tract infection, so an obstructive presentation warrants a lower threshold for the tertiary referral and the long-term follow-up. [5]
[6]Evidence, Guidelines & Regional Differences
The KDIGO acute kidney injury criteria, summarised by Kellum and Lameire, provide the international standard for the urine output thresholds that define oliguria and anuria, and they apply to the obstructed child as to any child with an acute kidney injury. The thresholds of oliguria below 0.5 mL per kg per hour and anuria below 0.3 mL per kg per hour are the foundation of the bedside assessment, and the staging by the urine output criteria drives the intensity of the monitoring and the urgency of the decompression. [1]
The pathophysiology of the obstructive nephropathy is charted by two landmark reviews. Molitoris framed the obstructive uropathy within the low-flow acute kidney injury paradigm, alongside the prerenal azotemia and the abdominal compartment syndrome, and explained the pressure-driven fall in the filtration that defines the early, reversible phase. Nørregaard and colleagues provided the molecular pathophysiology of the renal interstitial fibrosis that defines the late, irreversible phase, and the duration-dependence that underpins the urgency of the decompression. [2]
KDIGO 2012
- Urine output thresholds for oliguria and anuria
- The international standard for the acute kidney injury definition
- Staging by the urine output and the creatinine criteria
Low-flow AKI
- Molitoris 2022: obstructive uropathy as a pressure-driven low-flow injury
- Explains the early reversible fall in filtration
- Frames obstruction with prerenal azotemia and compartment syndrome
Obstructive nephropathy
- Nørregaard 2023: molecular pathophysiology of interstitial fibrosis
- Duration-dependence underpins the urgency of decompression
- Late phase is irreversible tubular atrophy and fibrosis
UTD classification
- Nguyen 2022: standardised hydronephrosis grading
- Risk-stratifies for surveillance versus intervention
- Enables consistent serial comparison across centres
The urinary tract dilation classification system, updated by Nguyen and colleagues, is the contemporary standard for the grading and the risk-stratification of the hydronephrosis that confirms an upper tract obstruction, and it has superseded the older society for fetal urology grading in most centres. The post-obstructive diuresis literature is anchored by the classic review by Baum and colleagues and the contemporary series by Leinum and colleagues, which define the threshold and the management of the pathological diuresis. The EAU and ESPU guidelines by Stein and colleagues provide the framework for the neurogenic bladder, and the long-term outcome data from the posterior urethral valves literature, including the systematic review by Hafizar and colleagues and the cohort by Robinson and colleagues, define the prognosis. [11]
The controversies centre on the timing of the intervention in the partial upper tract obstruction, the threshold for the nephrostomy in the infected obstruction, and the optimal fluid replacement strategy in the post-obstructive diuresis. The partial obstruction that is tolerated for months is watched with the serial ultrasound and the diuresis renogram, and the surgery is reserved for the declining function. The infected obstruction is drained without delay, because the antibiotics cannot reach the obstructed system. The fluid replacement in the post-obstructive diuresis replaces a fraction of the urine output rather than the full amount, to allow the tubules to recover their concentrating ability without provoking a volume depletion or a volume overload. [7]
Exam Pearls
O B S T R U C T for the obstructive uropathy assessment
References
- [1]Kellum JA, Lameire N, KDIGO AKI Guideline Work Group Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care, 2013.PMID 23394211
- [2]Molitoris BA Low-Flow Acute Kidney Injury: The Pathophysiology of Prerenal Azotemia, Abdominal Compartment Syndrome, and Obstructive Uropathy. Clin J Am Soc Nephrol, 2022.PMID 35584927
- [3]Nørregaard R, Mutsaers HAM, Frøkiær J, Kwon TH Obstructive nephropathy and molecular pathophysiology of renal interstitial fibrosis. Physiol Rev, 2023.PMID 37440209
- [4]Hafizar, Wahyudi I, Situmorang GR, Risky Raharja PA, Rodjani A Long-term renal outcomes in children with posterior urethral valves: a systematic review and meta-analysis. Pediatr Surg Int, 2026.PMID 42323785
- [5]Robinson CH, Rickard M, Jeyakumar N, Smith G, Richter J, Van Mieghem T, et al Long-Term Kidney Outcomes in Children with Posterior Urethral Valves: A Population-Based Cohort Study. J Am Soc Nephrol, 2024.PMID 39167453
- [6]López Pereira P, Martinez Urrutia MJ, Jaureguizar E Initial and long-term management of posterior urethral valves. World J Urol, 2004.PMID 15558286
- [7]Leinum LR, Berthelsen C, Azawi N Post-obstructive diuresis; underlying causes and hospitalization. Scand J Urol, 2020.PMID 32449436
- [8]Baum N, Anhalt M, Carlton CE Jr, Scott R Jr Post-obstructive diuresis. J Urol, 1975.PMID 1142500
- [9]Cai PY, Lee RS Ureteropelvic Junction Obstruction/Hydronephrosis. Urol Clin North Am, 2023.PMID 37385700
- [10]Woolf AS, Thiruchelvam N Congenital obstructive uropathy: its origin and contribution to end-stage renal disease in children. Adv Ren Replace Ther, 2001.PMID 11533916
- [11]Nguyen HT, Phelps A, Coley B, Darge K, Rhee A, Chow JS 2021 update on the urinary tract dilation (UTD) classification system: clarifications, review of the literature, and practical suggestions. Pediatr Radiol, 2022.PMID 34981177
- [12]Stein R, Bogaert G, Dogan HS, Hoen L, Kocvara R, Nijman RJM, et al EAU/ESPU guidelines on the management of neurogenic bladder in children and adolescent part I diagnostics and conservative treatment. Neurourol Urodyn, 2020.PMID 31724222