Paeds · nephrology-urology-fluids-and-electrolytes
Polyuria and polydipsia
Also known as Polyuria · Polydipsia · Polyuria-polydipsia syndrome · Diabetes insipidus · Arginine vasopressin deficiency · Arginine vasopressin resistance · Primary polydipsia
Fellowship guide to the diagnostic approach to a child with polyuria and polydipsia, beginning with a blood glucose to exclude osmotic diuresis from diabetes mellitus, then a urine osmolality to split the water diuresis of diabetes insipidus from a solute diuresis, the three-way split of the water diuresis into central diabetes insipidus (arginine vasopressin deficiency), nephrogenic diabetes insipidus (arginine vasopressin resistance) and primary polydipsia, the serum sodium pointer, the vasopressin-aquaporin-2 axis, the water deprivation test with desmopressin response and the copeptin-based approach, the management of hypernatraemic dehydration with slow sodium correction, desmopressin for central disease, and a low-solute diet with thiazide for nephrogenic disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Polyuria and polydipsia together describe a syndrome every general paediatrician meets: a child who passes large volumes of urine and is driven to drink to keep up. The complaint sounds simple, but it conceals a fork that, once taken wrongly, causes real harm. The single most common cause of polyuria in a child is uncontrolled diabetes mellitus, where glucose spills into the urine and drags water with it — an osmotic diuresis. [1] [3] That diagnosis is missed by going straight to rare endocrine causes, so the discipline of this topic is to exclude glucose first, every time, before ever thinking about the water-balance disorders.
When the glucose is normal, the question becomes whether the kidney is failing to concentrate urine at all — a water diuresis — or whether it is being asked to excrete a load of solute. The urine osmolality answers that in a single number: dilute urine below 300 mOsm per kg is a water diuresis and leads to the three diabetes insipidus disorders. [1] [10] This page owns that diagnostic fork and the fluids-and-electrolytes consequences, while the companion endocrinology page carries the deep pituitary-tumour and congenital detail. The teaching spine is glucose first, osmolality second, sodium third, desmopressin response fourth, and slow correction of the sodium throughout.
Overview & Definition
Polyuria is defined quantitatively. In a child it means a urine output over 2 litres per square metre of body-surface area per day, or more simply over 40 to 50 mL per kilogram per day. [1] [3] Polydipsia is the compensatory intake that follows, because the body is defending its serum osmolality. The two together form the polyuria-polydipsia syndrome, and the first task is to decide whether the kidney is producing dilute urine because it cannot concentrate it (a water diuresis) or because it is being flooded with solute it must excrete (an osmotic or solute diuresis). [10] [5]
The urine osmolality is the single number that separates these. A water diuresis produces urine that is genuinely dilute — osmolality below 300 mOsm per kg — because the kidney cannot retain water against its concentration gradient. [1] [6] An osmotic diuresis produces a high volume of urine that is not dilute at all, because the obligate excretion of glucose, mannitol or urea carries water but keeps the urine relatively concentrated. This distinction is why a urine osmolality is measured alongside the glucose at first contact, rather than later. [5] [10]
Within the water diuresis sits diabetes insipidus, named centuries ago for the tasteless (insipid) urine that distinguished it from the sweet urine of diabetes mellitus. The 2022 Working Group position statement renamed central diabetes insipidus as arginine vasopressin deficiency (AVP-D) and nephrogenic disease as arginine vasopressin resistance (AVP-R), to remove confusion with diabetes mellitus and to describe mechanism rather than anatomy, though the older names remain in wide clinical use. [2] [1] Both describe a kidney that cannot concentrate urine; the difference is whether the problem is a lack of the hormone or a failure of the kidney to respond to it.
Classification
The classification of polyuria is the diagnostic algorithm itself, and it runs in two clean steps. The first step divides polyuria into an osmotic (solute) diuresis and a water diuresis, decided by the blood glucose and the urine osmolality. [10] [5] Osmotic diuresis means a solute is dragging water out — glucose in diabetes mellitus is the commonest, joined by mannitol, urea in recovering kidney injury, radiocontrast and loop diuretics. A water diuresis means the kidney cannot retain water, and that is the domain of the three diabetes insipidus disorders plus primary polydipsia. [1]
The second step splits the water diuresis into its three causes by asking where the vasopressin-aquaporin-2 axis breaks. Central diabetes insipidus is a deficiency of arginine vasopressin: the hormone is not made, so no signal reaches the kidney. Nephrogenic diabetes insipidus is resistance to arginine vasopressin: the hormone is present but the kidney cannot respond because the V2 receptor or the aquaporin-2 channel is defective. Primary polydipsia is neither — here the axis is intact, but chronic excess water intake suppresses vasopressin release so effectively that the kidney produces dilute urine by design. [1] [9]
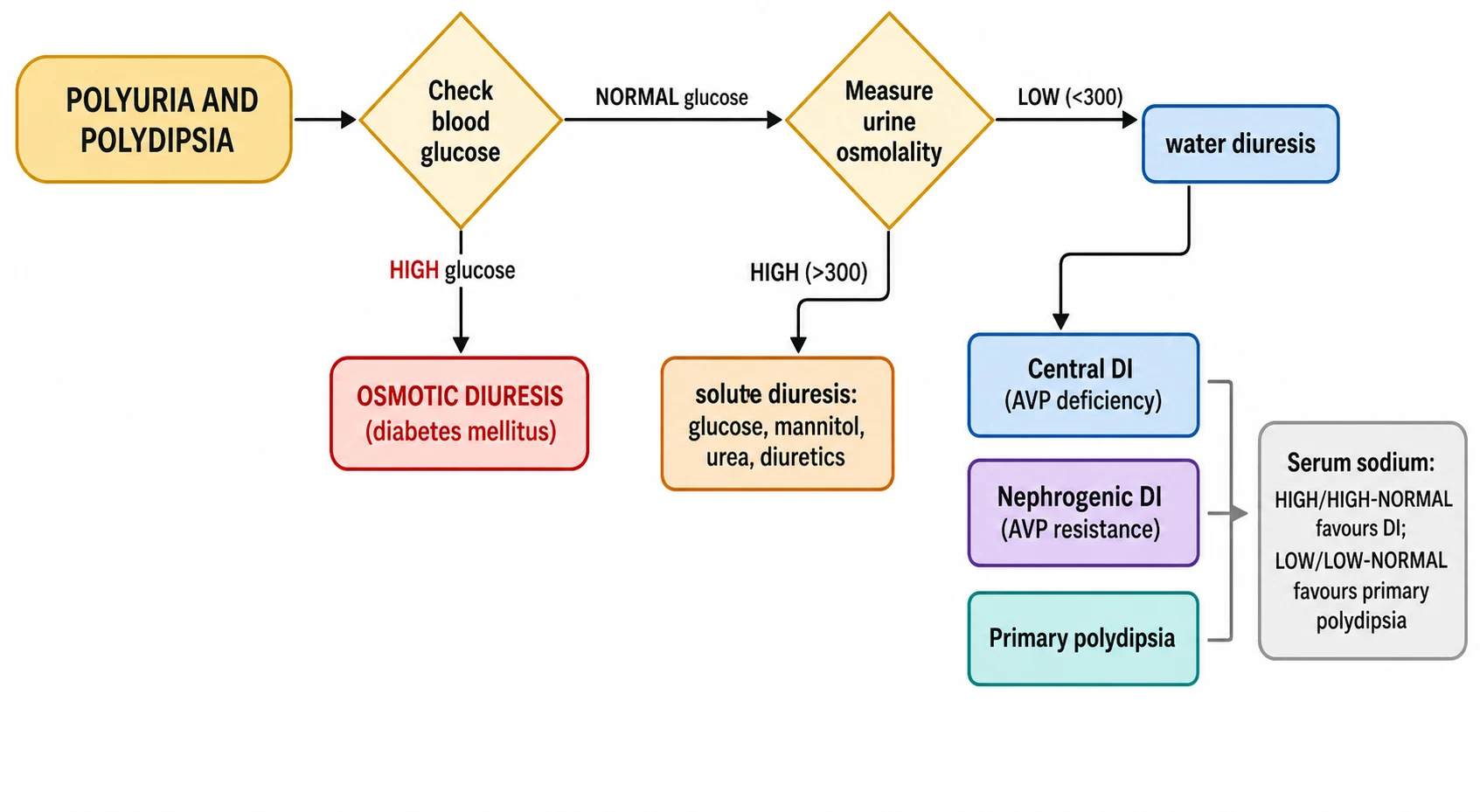
The serum sodium is the bedside pointer within the water diuresis, and it is worth memorising as a pair. Because diabetes insipidus loses free water, the serum sodium tends to sit at the high end of normal or frankly raised; because primary polydipsia overloads water, the serum sodium tends to sit at the low end of normal or frankly low. [1] [7] A sodium in the middle does not exclude either, but a high sodium with polyuria is diabetes insipidus until proven otherwise, and a low sodium with polyuria should make you very wary of giving desmopressin.
Central DI (AVP deficiency)
- No vasopressin reaches the kidney
- Causes: germinoma, craniopharyngioma, histiocytosis, surgery, trauma
- Serum sodium high or high-normal
- Concentrates urine after desmopressin
- Treated with desmopressin
Nephrogenic DI (AVP resistance)
- Vasopressin present but kidney cannot respond
- Congenital AVPR2 (X-linked) or AQP2, or acquired (lithium, hypercalcaemia)
- Serum sodium high or high-normal
- No response to desmopressin
- Treated with low-solute diet, thiazide, amiloride or indometacin
Primary polydipsia
- Axis intact but vasopressin suppressed by excess intake
- Psychogenic or habitual, occasionally hypothalamic
- Serum sodium low or low-normal
- Concentrates urine with dehydration (intact axis)
- Desmopressin is dangerous — treat the cause
Epidemiology & Risk Factors
The epidemiology of polyuria is the epidemiology of its causes, and one cause dominates. Diabetes mellitus is the single commonest reason a child presents with polyuria and polydipsia, because uncontrolled hyperglycaemia drives a glucose osmotic diuresis; this is why a blood glucose is the first test, not a pituitary hormone panel. [3] [1] Once osmotic diuresis is excluded, the water-diuresis disorders are individually uncommon but carry disproportionate exam and clinical weight because of the harm they do when missed.
Within the water diuresis, congenital nephrogenic diabetes insipidus is the dominant concern in infancy. It is usually an X-linked defect of the AVPR2 gene, accounting for about 90 percent of inherited cases and therefore affecting mostly boys, with the autosomal AQP2 form making up roughly the remaining 10 percent. [9] [3] A boy infant with polyuria, failure to thrive and a maternal family history of affected males carries congenital nephrogenic disease until proven otherwise. Central diabetes insipidus, by contrast, is most often acquired in older children, arising from a hypothalamic or pituitary germinoma, craniopharyngioma, Langerhans cell histiocytosis, head trauma or neurosurgery, and an idiopathic label should not be accepted until imaging has excluded an occult mass. [4] [11]
Primary polydipsia favours older children and adolescents and is often psychogenic, arising in the setting of psychiatric illness, behavioural disturbance or sometimes a hypothalamic lesion that disrupts the thirst centre. It is uncommon in infants, who cannot self-regulate their intake; the infant who drinks to excess usually does so because the kidney is losing water, not the reverse. [10] [1]
Pathophysiology
The kidney concentrates urine through the vasopressin-aquaporin-2 axis, and understanding where each disorder breaks this axis is the key to the whole topic. Arginine vasopressin is made in the hypothalamic supraoptic and paraventricular nuclei and travels down axons to the posterior pituitary, where it is released when serum osmolality rises. It then reaches the kidney, binds the V2 receptor on the basolateral membrane of the collecting-duct cell, raises intracellular cyclic AMP, and triggers the insertion of aquaporin-2 water channels into the apical (urine-facing) membrane. [1] [9] Water then flows through these channels back into the hypertonic medullary interstitium, and the urine is concentrated. Stop any one of those steps and the urine stays dilute.
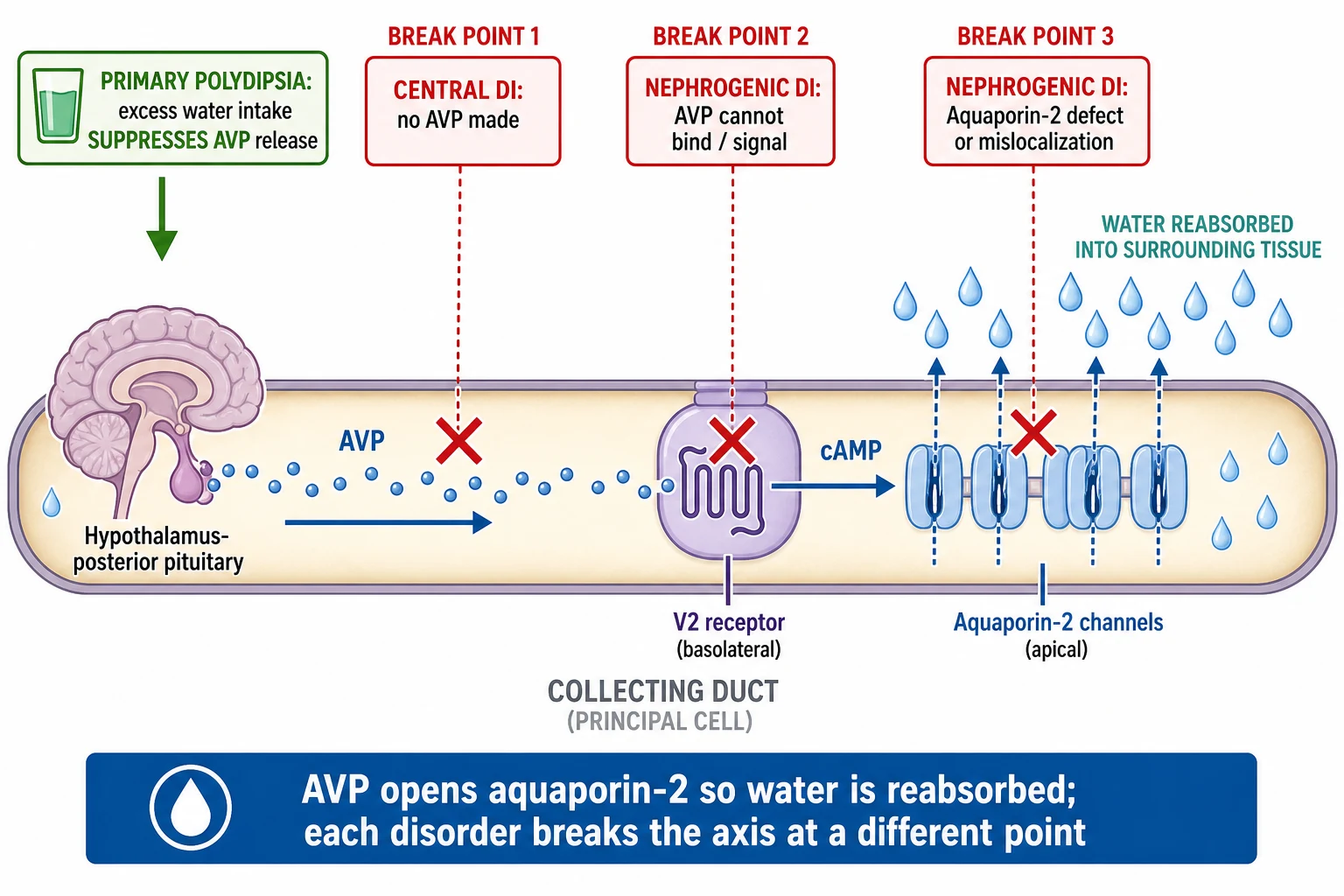
Central diabetes insipidus breaks the axis at its origin: there is no vasopressin to release, so the V2 receptor is never stimulated and aquaporin-2 stays out of the membrane. Nephrogenic diabetes insipidus breaks it at the kidney: vasopressin arrives but the V2 receptor or the aquaporin-2 channel is defective, so the signal cannot be transduced. [1] [9] Primary polydipsia breaks it at the top by a different mechanism — chronic over-hydration keeps the serum osmolality low, so vasopressin release is continually suppressed, and the axis is intact but switched off. [10]
The clinical consequence of a broken axis is the loss of free water. Because sodium and water are handled separately, pure water loss drives the serum sodium upward, producing the hypernatraemic dehydration that is the real danger of untreated diabetes insipidus. [12] [1] The infant is the highest-risk patient because they cannot report thirst or reach for water; they simply stop growing, become irritable and febrile, and present with a serum sodium that may exceed 160 mmol per litre. Osmotic diuresis, by contrast, does not produce dilute urine — the glucose carries water but keeps the urine concentrated, which is why the urine osmolality reliably separates the two. [5] [10]
Clinical Presentation
The school-age child or adolescent with a water diuresis describes the syndrome in their own words: passing huge volumes of pale urine through the day and night, waking repeatedly to drink and to void, a strong preference for cold water, and new bedwetting in a previously dry child. [3] [1] Nocturia and secondary enuresis are common presenting complaints, and a careful history often reveals that the drinking precedes the urination or vice versa in a way that the parents have not been able to disentangle — which is exactly what the tests are for.
Infants present very differently, and this is where diabetes insipidus is most often missed. An infant cannot complain of thirst, so the picture is of irritability, crying that resolves with feeding, poor weight gain, unexplained fever, constipation, and repeated presentations with hypernatraemic dehydration. [11] [3] Congenital nephrogenic diabetes insipidus classically appears in the first months of life in a boy with failure to thrive, and the family may describe a maternal uncle or brother with the same problem. Any infant with recurrent hypernatraemia or unexplained failure to thrive deserves a paired serum and urine osmolality, because the diagnosis will not declare itself otherwise. [9] [11]
The history and examination then carry the pointers to the cause. Ask about preceding neurosurgery or head trauma, visual symptoms, headaches and growth (pointing to a pituitary or hypothalamic lesion), and medications — lithium is the classic acquired nephrogenic cause, and hypercalcaemia can do the same. [4] [9] Examine the visual fields, growth parameters, hydration and neurological system. A child with central disease may have a bitemporal hemianopia from optic chiasm compression, growth failure from coexisting growth-hormone deficiency, or signs of raised intracranial pressure; a child with primary polydipsia may give a history of psychiatric illness or behavioural change. [11] [10]
Differential Diagnosis
The differential of polyuria runs along the same two steps as the classification, and the discipline is to work through them in order. The first branch is osmotic versus water diuresis. Osmotic diuresis is caused by a solute load: glucose in diabetes mellitus is by far the commonest, joined by mannitol, urea in the recovery phase of kidney injury or obstructive uropathy, radiocontrast agents, and loop diuretics. [5] [10] These all raise the urine osmolality rather than lower it, which is why a single urine osmolality at presentation places the child on the correct side of the fork.
The second branch, within the water diuresis, is the three-way split of central diabetes insipidus, nephrogenic diabetes insipidus and primary polydipsia, distinguished by the serum sodium, the water deprivation test and the response to desmopressin. The mimic that causes the most harm is primary polydipsia mislabelled as diabetes insipidus and treated with desmopressin: the intact kidney then retains the ingested water and the child develops acute water intoxication with severe hyponatraemia and seizures. [1] [7] This is why a low or low-normal serum sodium in a polyuric child is a warning to withhold desmopressin, not to give it.
A few other polyuric states sit alongside the main fork and should be considered when the picture is atypical. Post-obstructive diuresis follows relief of a chronic obstruction and is usually self-limiting but can dehydrate an infant. The polyuria of recovering acute tubular necrosis is transient and accompanied by the rising creatinine that tells the story. [5] [9] Rarely, a salt-wasting tubulopathy such as Bartter syndrome presents with polyuria, but it carries hypokalaemic metabolic alkalosis that points away from a pure water-loss disorder. The defining feature that keeps all of these off the main fork is that they do not produce maximally dilute urine in the setting of a rising serum sodium. [10]
Clinical & Bedside Assessment
Begin at the bedside with the two questions that change tempo: how dehydrated is the child, and is there a threat to the brain? Assess weight, perfusion, capillary refill, mucous membranes and fontanelle in the infant, and the conscious level throughout. [12] [3] A child who is clinically dehydrated with a high serum sodium needs intravascular volume restoration and slow correction, not a diagnostic fast; the water deprivation test is for the stable, well-hydrated child, and is deferred until the sodium is safe. Record the weight accurately, because serial weights during a deprivation test are both the safety and the endpoint measure. [7] [4]
The focused examination then hunts for the cause. Measure the growth parameters, because failure to thrive in a polyuric infant points to congenital nephrogenic disease or a missed central lesion with growth-hormone deficiency. [11] [9] Examine the visual fields by confrontation, because a bitemporal hemianopia signals a chiasmal lesion such as a craniopharyngioma or germinoma. Look for signs of raised intracranial pressure, pubertal delay, and the dysmorphic features of a syndromic cause. A medication history is mandatory: lithium and demeclocycline cause acquired nephrogenic disease, and hypercalcaemia from any cause impairs concentrating ability. [4] [9]
Take a deliberate family and developmental history. A maternal family history of affected males in a boy infant flags X-linked congenital nephrogenic diabetes insipidus. A psychiatric history in an adolescent flags psychogenic primary polydipsia. A recent neurosurgical or head-injury history flags acquired central disease and the possibility of the triphasic response. [3] [10] The bedside assessment is therefore not a single examination but the assembly of the clues — age, tempo, family, neurology, medications and hydration — that will steer the choice and timing of the investigations to follow.
Investigations
The first-line tests settle the pathway at the bedside and are done together: a blood glucose, a serum sodium and osmolality, a urine osmolality and specific gravity, and a serum urea and creatinine. [5] [1] The blood glucose excludes osmotic diuresis from diabetes mellitus. The paired serum and urine osmolality do the rest: a urine osmolality below 300 mOsm per kg in the face of a raised or high-normal serum osmolality is a water diuresis and defines diabetes insipidus, while a urine osmolality that is appropriately concentrated rules out a water-loss disorder and redirects to a solute cause. [10] [6]
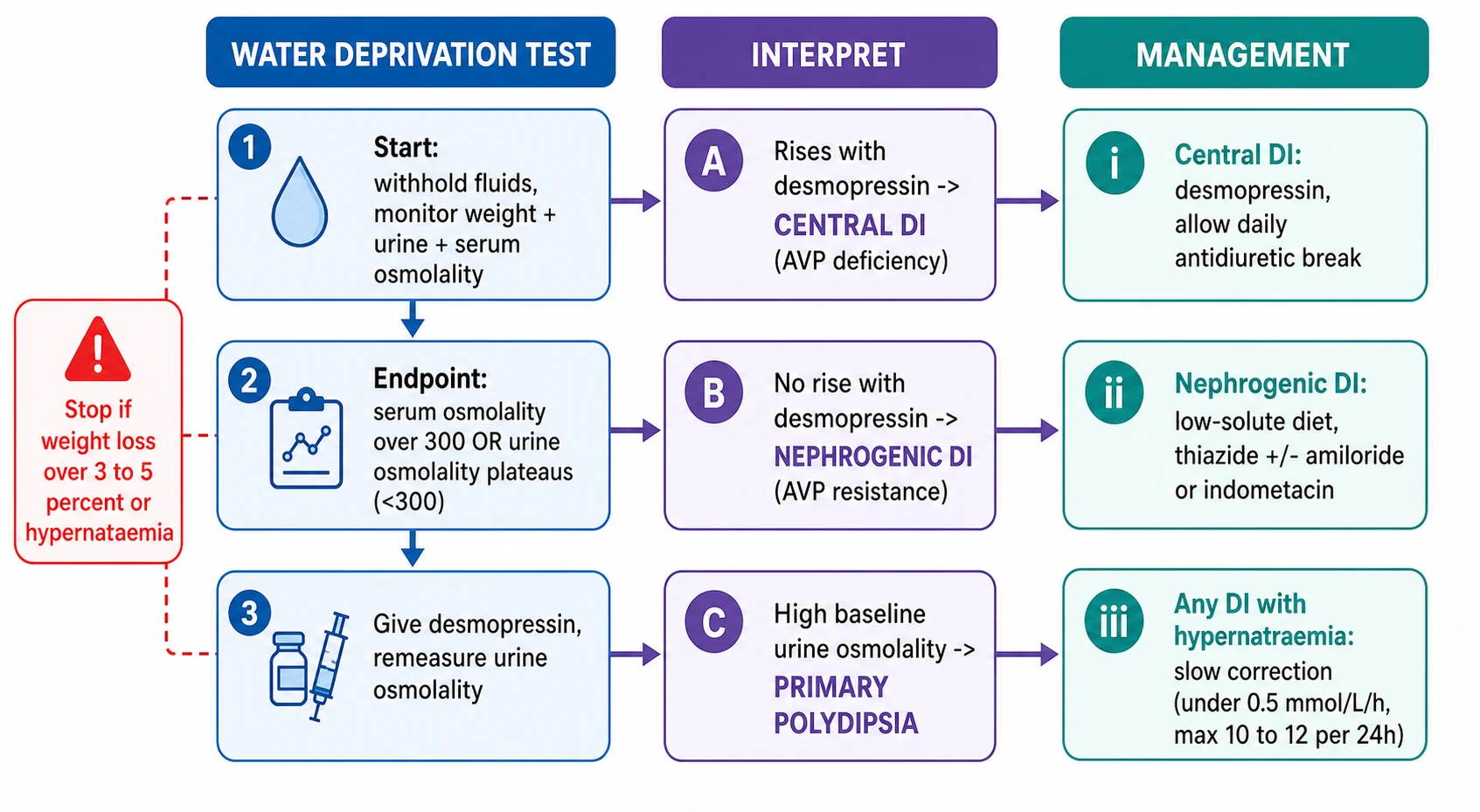
The water deprivation test is the classic dynamic investigation for the stable child in whom the first-line tests are equivocal, and it must be done under supervised observation. Fluids are withheld, and weight, urine output, urine osmolality and serum osmolality and sodium are measured at intervals. The test ends at one of two endpoints — the serum osmolality rises above 300 mOsm per kg with the urine osmolality still plateaus below 300, confirming diabetes insipidus — or at a safety limit, which is a weight loss over 3 to 5 percent or a rising serum sodium, at which point the test is stopped and desmopressin given. [4] [1] The response to desmopressin then splits central from nephrogenic disease: the urine osmolality rises by more than 50 percent in central diabetes insipidus, but does not rise in nephrogenic disease. [1] [9]
The copeptin-based approach has reshaped this testing in centres that can measure copeptin, the stable C-terminal fragment of the vasopressin precursor released in equimolar amounts with vasopressin. Because copeptin is stable in the serum and vasopressin is not, it can be measured directly. The Fenske trial in the New England Journal of Medicine showed that a hypertonic-saline-stimulated copeptin cut-off of 21.5 pmol per litre distinguished arginine vasopressin deficiency from primary polydipsia with greater accuracy than the indirect water deprivation test, and the Winzeler Lancet study showed that arginine-stimulated copeptin performed similarly and more conveniently. [7] [8] A baseline copeptin below 4 to 5 pmol per litre strongly suggests central diabetes insipidus, while a stimulated copeptin that fails to rise confirms it; nephrogenic disease shows a high baseline copeptin because the kidney is unresponsive. [6] [7]
When central diabetes insipidus is confirmed, the workup must find the lesion. An MRI of the hypothalamic-pituitary axis is mandatory, looking for a germinoma, craniopharyngioma, Langerhans cell histiocytosis or a thickened, absent pituitary stalk. [4] [11] Anterior pituitary hormones are measured, because central diabetes insipidus often coexists with growth-hormone, cortisol or thyroid deficiency — and cortisol deficiency in particular can mask diabetes insipidus, because glucocorticoids are needed for the kidney to excrete a water load. Visual fields are tested formally. A confirmed nephrogenic case in an infant warrants AVPR2 and AQP2 genetic testing with family counselling. [9] [11]
WATER
Management — Resuscitation
The resuscitation priority in a polyuric child is the hypernatraemic dehydration that uncontrolled water loss produces, and it overrides every diagnostic consideration. Secure the airway and breathing, then restore the intravascular volume with isotonic saline — 10 to 20 mL per kilogram boluses of 0.9 percent sodium chloride — to correct shock and tissue perfusion, because shock kills faster than hypernatraemia. [12] [3] Once perfusion is restored, the free-water deficit is replaced slowly, because the brain has adapted to the hypertonic state and a rapid fall in serum sodium risks cerebral oedema, herniation and death.
The rate of sodium correction is the single most important safety rule in this topic. The serum sodium should fall by no more than 0.5 mmol per litre per hour, to a maximum of 10 to 12 mmol per litre over 24 hours, with frequent monitoring. [12] [1] This is achieved by calculating the free-water deficit and replacing it over 48 hours using a hypotonic fluid such as 0.45 percent sodium chloride, adjusted to the measured sodium, while continuing to meet maintenance needs and ongoing losses. The infant is again the highest-risk patient because of a large surface-area-to-volume ratio and the inability to report thirst, so ongoing urinary water losses must be measured and replaced millilitre for millilitre. [3] [12]
While the sodium is being corrected, the cause is addressed in parallel. If central diabetes insipidus is suspected and the child is passing large volumes, desmopressin can be given to reduce ongoing water loss once cortisol status is known — because giving desmopressin before confirming the child can excrete a water load risks hyponatraemia, and because cortisol deficiency must be corrected first or the picture will be misread. [4] [1] In the infant with congenital nephrogenic disease, resuscitation means ensuring adequate free water by continuous access to feeds or a nasogastric drip, because no drug will reduce the urine output acutely. [9]
Management — Definitive & Stepwise
Definitive management is cause-specific and follows the three-way split. Central diabetes insipidus is treated with desmopressin, a synthetic vasopressin analogue that acts on the V2 receptor to restore concentrating ability. [1] [3] It is given orally, intranasally or sublingually, titrated to control symptoms and allow an uninterrupted night, and — crucially — a daily antidiuretic break is built in by allowing some breakthrough polyuria before the next dose, to permit the excretion of any excess water and prevent hyponatraemia. The family is taught that desmopressin is a water-retaining drug, not a fluid, so the child must not drink to excess around the dose. [3] [4]
Nephrogenic diabetes insipidus cannot be treated with desmopressin, because the defect is downstream of the receptor. The mainstay is a low-solute diet — reduced sodium and reduced protein — which lowers the obligate solute excretion and therefore the obligatory water loss, and this alone often improves symptoms and growth. [9] [3] Thiazide diuretics are added and work by a paradoxical mechanism: they produce mild volume depletion, which increases proximal tubular sodium and water reabsorption, so less filtrate reaches the collecting duct and the polyuria falls. A potassium-sparing diuretic such as amiloride is often combined, and indometacin, by reducing renal prostaglandin production, further enhances concentrating ability; the combination of thiazide, amiloride or indometacin with a low-solute diet is the standard regimen for congenital disease. [9] [3]
Primary polydipsia is treated by addressing the cause, not the kidney. In psychogenic polydipsia this means psychiatric assessment and behavioural restriction of fluid intake; in a hypothalamic thirst-centre lesion it means treating the lesion where possible. Desmopressin is contraindicated, because it converts the water overload into hyponatraemia, and it should never be started in a polyuric child whose serum sodium is low or low-normal without first excluding primary polydipsia. [10] [1] The osmotic diuresis of diabetes mellitus is managed with insulin and fluid resuscitation along the diabetic-ketoacidosis pathway, and the polyuria resolves as the glucose falls.
Desmopressin (central diabetes insipidus)
Dose
Titrate to symptom control; oral 0.05 to 1.2 mg per day in divided doses, sublingual or intranasal alternatives by age
Stable polyuria-polydipsia — the definitive ladder
First-line: blood glucose, serum sodium and osmolality, urine osmolality
Glucose high: manage osmotic diuresis (diabetes mellitus pathway)
Water diuresis with high or high-normal sodium: pursue diabetes insipidus
Water deprivation test or copeptin to confirm; desmopressin response splits central from nephrogenic
Central DI: desmopressin with a daily antidiuretic break; MRI and anterior pituitary workup
Nephrogenic DI: low-solute diet, thiazide with amiloride or indometacin; genetic testing in infants
Primary polydipsia: treat the cause; do not give desmopressin
Specific Subtypes & Scenarios
Congenital nephrogenic diabetes insipidus in the infant is the subtype that tests every part of this topic. A boy presenting in the first months of life with polyuria, failure to thrive, fever and constipation, often with a maternal family history, has the X-linked AVPR2 form until proven otherwise. [9] [3] The priority in infancy is not a drug but sufficient free water — frequent feeds, a nasogastric drip overnight, and a low-solute diet to reduce obligate water loss — because growth and brain development depend on avoiding chronic hypernatraemia. Thiazide, amiloride and indometacin are added to reduce urine volume, and genetic confirmation guides counselling. The parents are taught to respond to the infant's thirst and to seek help for intercurrent illness, which can precipitate dangerous dehydration. [9]
Central diabetes insipidus after pituitary surgery carries the triphasic response, and recognising it prevents both under- and over-treatment. The first phase is transient diabetes insipidus from shock to the posterior pituitary, lasting hours to days; the second is an antidiuretic phase from uncontrolled release of stored vasopressin, during which desmopressin is withheld to avoid hyponatraemia; the third is permanent diabetes insipidus if the neurons are destroyed. [4] [1] Cortisol status must be checked first, because cortisol deficiency impairs water excretion and can mask or mimic diabetes insipidus. Management is guided by measured serum sodium and urine output rather than a fixed schedule.
Adipsic diabetes insipidus is the rare but dangerous combination of vasopressin deficiency and absent thirst, usually from an extensive hypothalamic lesion. The child cannot defend their serum osmolality from either side, so management is a prescribed daily fluid intake plus desmopressin, with weight-based monitoring and a fixed sodium target. [11] [10] This is one of the hardest water-balance disorders to manage, because there is no internal feedback; it requires a disciplined regimen and close follow-up.
Osmotic diuresis from diabetes mellitus is the commonest polyuria of childhood and is managed along the diabetes pathway, not the water-diuresis pathway. The polyuria and polydipsia of new-onset type 1 diabetes resolve as the glucose falls with insulin and fluid resuscitation, and the urine osmolality — high rather than dilute at presentation — is the feature that keeps it on the osmotic side of the fork. [1] [5]
Complications & Pitfalls
The cardinal pitfall in resuscitation is correcting the sodium too fast. The brain adapts to chronic hypernatraemia by accumulating idiogenic osmoles, so a rapid fall in serum sodium shifts water into the brain and causes cerebral oedema, seizures and herniation. The safe rate — under 0.5 mmol per litre per hour, to a maximum of 10 to 12 mmol per litre over 24 hours — is the single rule that prevents this harm, and it requires frequent sodium monitoring and a willingness to slow the infusion if the sodium falls faster than intended. [12] [1] The mirror-image pitfall is under-correction, which leaves the child hypernatraemic and at risk of neurological injury; the discipline is to correct at the right rate, neither fast nor stalled.
The cardinal pitfall in diagnosis is giving desmopressin to a child with primary polydipsia. Because the axis is intact and only suppressed, desmopressin forces the kidney to retain the ingested water, and the serum sodium falls rapidly into the symptomatic hyponatraemia range with seizures and brain swelling. [10] [1] This is why a low or low-normal serum sodium in a polyuric child is treated as a warning against desmopressin until primary polydipsia is excluded, and why the water deprivation or copeptin test is done before any treatment is committed.
The third pitfall is mistaking nephrogenic for central disease and escalating desmopressin that cannot work. A child whose urine does not concentrate after an adequate desmopressin challenge has nephrogenic (or primary polydipsia) disease, not insufficient central treatment, and further desmopressin simply risks volume overload. [9] [7] The fourth pitfall is accepting an idiopathic label for central disease without an MRI — a proportion of these children harbour an occult germinoma or Langerhans cell histiocytosis that declares itself only on serial imaging, so a normal early scan warrants follow-up imaging if the diagnosis remains unexplained. [4] [11]
Prognosis & Disposition
The prognosis of the polyuria-polydipsia syndrome is governed by the cause, the speed of diagnosis and the avoidance of hypernatraemic brain injury. Treated central diabetes insipidus has an excellent prognosis for normal growth and development, because desmopressin restores water balance fully; the long-term outlook is then determined by the underlying tumour and its treatment. [3] [4] Congenital nephrogenic disease is a lifelong condition requiring sustained dietary and drug management, with the main determinants of outcome being early diagnosis, adherence to the low-solute regimen, and the prevention of recurrent hypernatraemia, which can cause cognitive impairment. [9]
Disposition depends on the presentation and the sodium. A child presenting with hypernatraemic dehydration is admitted for intravenous fluid management and frequent sodium monitoring, and is not discharged until the sodium is falling safely and the cause is being addressed. A stable, well-hydrated child with a clear diagnosis and a safe sodium can be managed as an outpatient with endocrinology or nephrology input, a clear treatment plan and safety-netting. [12] [1] The family is taught to recognise the signs of dehydration and water intoxication, to manage intercurrent illness, and to attend follow-up for sodium monitoring, growth and — in central disease — serial imaging.
The safety-net given to every family closes the loop between episodes. Seek urgent help for reduced urine output, drowsiness, irritability, fever with reduced intake, seizure, or any sign of dehydration in a child who cannot defend their own water balance. [9] [12] For the child on desmopressin, the additional warning is to avoid drinking to excess around the dose, because water retention is the mechanism of both its benefit and its harm.
Special Populations
Infants are the population in whom polyuria is most dangerous and most often missed. Unable to report thirst or reach for water, the infant with congenital nephrogenic or central disease presents with failure to thrive, irritability, fever and hypernatraemic dehydration rather than polydipsia, and the diagnosis is made only when a clinician thinks to measure a paired serum and urine osmolality. [11] [3] Management prioritises adequate free water by nasogastric drip if needed, a low-solute diet, and growth surveillance, with the drug regimen built around reducing obligate water loss. The parents become the frontline monitors of hydration and are taught to respond to the infant's behaviour and to seek help early with intercurrent illness.
Children after neurosurgery need careful distinction of the triphasic response and coexisting anterior pituitary deficits. Cortisol deficiency must be corrected before vasopressin action can be judged, because glucocorticoids are required for free-water clearance; a child who appears to have resolved diabetes insipidus may simply have untreated cortisol deficiency masking it. [4] [1] Management is guided by measured serum sodium and urine output rather than a fixed schedule, and the transition from the acute postoperative phase to long-term care is planned with the endocrine and neurosurgical teams together.
Adolescents with possible psychogenic primary polydipsia need psychiatric assessment as the central intervention, because the polyuria is driven by behaviour, not a renal or pituitary defect. The risk here is the same as at any age — giving desmopressin to a child with an intact axis and water overload causes hyponatraemia — so the diagnosis is confirmed by a low or low-normal serum sodium and an intact concentrating response to dehydration before any treatment is considered. [10] [1] The transition to adult care for congenital disease is planned early, carrying the diagnosis, the genetic result and the management plan forward so that adherence and growth are sustained.
Evidence, Guidelines & Regional Differences
The evidence base for the polyuria-polydipsia syndrome has been reshaped by the copeptin era. The Christ-Crain and Bichet primer in Nature Reviews Disease Primers consolidated the vasopressin-aquaporin-2 axis, the diagnostic algorithm and the management of the three disorders, and remains the reference overview. [1] The 2022 Working Group position statement recommended renaming central and nephrogenic diabetes insipidus to arginine vasopressin deficiency and arginine vasopressin resistance, a change that describes mechanism rather than anatomy and reduces confusion with diabetes mellitus — though it remains debated and the older names persist in practice. [2]
The diagnostic evidence has moved most. The Timper prospective multicentre study established that a baseline copeptin cut-off could distinguish the disorders, and the Fenske trial in the New England Journal of Medicine showed that a hypertonic-saline-stimulated copeptin cut-off of 21.5 pmol per litre distinguished arginine vasopressin deficiency from primary polydipsia with greater diagnostic accuracy than the indirect water deprivation test, which remains the standard where copeptin is unavailable. [6] [7] The Winzeler Lancet study showed that arginine-stimulated copeptin performed comparably and was more convenient and safer than hypertonic saline, positioning arginine-stimulation as a practical alternative in specialist centres. [8]
The paediatric and management evidence is anchored by the Dabrowski, Di Iorgi and Robertson reviews, which set out the infant and child presentation, the diagnostic pathway and the differential diagnosis. [3] [4] [10] The Bockenhauer and Bichet review in Nature Reviews Nephrology consolidated the pathophysiology and management of nephrogenic disease, including the low-solute, thiazide and indometacin regimen. [9] The Djermane infancy cohort established the importance of early identification of central disease with or without the adipsic hypernatraemia syndrome, and the Zieg Acta Paediatrica review set out the diagnosis and safe management of hypernatraemia in children, underpinning the slow-correction rule. [11] [12]
ANZ and UK practice follows international consensus that a blood glucose and a paired serum and urine osmolality are the first-line tests, that the water deprivation test remains the standard where copeptin is unavailable, and that hypernatraemic dehydration is corrected at no more than 0.5 mmol per litre per hour to a maximum of 10 to 12 mmol per litre over 24 hours. Copeptin testing is increasingly available in tertiary paediatric centres but not universally; local protocol governs its use. Always confirm the local desmopressin dosing and the slow-correction target before prescribing. [1] [12]
The evidence is weakest in three places: the optimal copeptin cut-offs in infants and young children, the long-term safety of indometacin in congenital nephrogenic disease, and the role and timing of arginine-stimulated copeptin in early infancy. These remain areas of active study, and a specialist endocrinology or nephrology discussion is appropriate for the complex or recurrent case. [8] [9]
Exam Pearls
Memorise the four-step discriminator as a chain: glucose first, osmolality second, sodium third, desmopressin fourth. A blood glucose excludes the osmotic diuresis of diabetes mellitus, the commonest cause of polyuria in childhood; a urine osmolality below 300 mOsm per kg marks a water diuresis; a high or high-normal serum sodium points to true diabetes insipidus while a low or low-normal sodium points to primary polydipsia; and the response to desmopressin splits central (concentrates) from nephrogenic (no response) disease. [1] [10] The single must-know definition is polyuria as over 2 L per m2 per day or over 40 to 50 mL per kg per day, and the must-know safety rule is slow sodium correction — under 0.5 mmol per litre per hour, max 10 to 12 over 24 hours — to avoid cerebral oedema. [12]
The pharmacology points are desmopressin for central disease with a daily antidiuretic break, and the paradox of thiazide reducing urine volume in nephrogenic disease through mild volume depletion and increased proximal reabsorption, combined with a low-solute diet and amiloride or indometacin. [3] [9] The high-yield physiology point is the vasopressin-aquaporin-2 axis: AVP binds the V2 receptor, raises cAMP and inserts aquaporin-2 into the apical collecting-duct membrane, and each disorder breaks it at a different point — no AVP in central disease, a receptor or channel defect in nephrogenic disease, and suppression by excess intake in primary polydipsia. [1] [9]
The danger point examiners reward is the recognition that desmopressin is contraindicated in primary polydipsia, because it converts water overload into acute hyponatraemia. The infant point is that congenital nephrogenic diabetes insipidus is X-linked AVPR2 in about 90 percent and presents in a boy with failure to thrive. [9] [11] The neurosurgery point is the triphasic response and the need to correct cortisol deficiency before judging vasopressin action. [4] Nail the four-step chain, the slow-correction rule, and the contraindication to desmopressin in primary polydipsia, and you have the spine of every polyuria-polydipsia viva.
References
- [1]Christ-Crain M; Bichet DG; Fenske WK; Goldman MB; Rittig S; Verbalis JG Diabetes insipidus. Nat Rev Dis Primers, 2019.PMID 31395885
- [2]Working Group for Renaming Diabetes Insipidus; Arima H; Cheetham T; Christ-Crain M; Crowley RK; Verbalis JG Changing the name of diabetes insipidus: a position statement of The Working Group for Renaming Diabetes Insipidus. Eur J Endocrinol, 2022.PMID 36239119
- [3]Dabrowski E; Kadakia R; Zimmerman D Diabetes insipidus in infants and children. Best Pract Res Clin Endocrinol Metab, 2016.PMID 27156767
- [4]Di Iorgi N; Napoli F; Allegri AE; Olivieri I; Bertelli E; Gallizia A; Rossi A; Maghnie M Diabetes insipidus--diagnosis and management. Horm Res Paediatr, 2012.PMID 22433947
- [5]Fenske W; Allolio B Clinical review: Current state and future perspectives in the diagnosis of diabetes insipidus: a clinical review. J Clin Endocrinol Metab, 2012.PMID 22855338
- [6]Timper K; Fenske W; Kühn F; Frech N; Arici B; Rutishauser J; Kopp P; Allolio B; Stettler C; Muller B; Katan M Diagnostic Accuracy of Copeptin in the Differential Diagnosis of the Polyuria-polydipsia Syndrome: A Prospective Multicenter Study. J Clin Endocrinol Metab, 2015.PMID 25768671
- [7]Fenske W; Refardt J; Chifu I; Schnyder I; Winzeler B; Drummond J; Rutishauser J; Kopp P; Landgraf R; Luger A; Christ-Crain M A Copeptin-Based Approach in the Diagnosis of Diabetes Insipidus. N Engl J Med, 2018.PMID 30067922
- [8]Winzeler B; Cesana-Nigro N; Refardt J; Vogt DR; Chifu I; Bassetti CL; Fenske WK; Kopp P; Christ-Crain M Arginine-stimulated copeptin measurements in the differential diagnosis of diabetes insipidus: a prospective diagnostic study. Lancet, 2019.PMID 31303316
- [9]Bockenhauer D; Bichet DG Pathophysiology, diagnosis and management of nephrogenic diabetes insipidus. Nat Rev Nephrol, 2015.PMID 26077742
- [10]Robertson GL Diabetes insipidus: Differential diagnosis and management. Best Pract Res Clin Endocrinol Metab, 2016.PMID 27156759
- [11]Djermane A; Elmaleh M; Simon D; Poidvin A; Souberbielle JC; Beltrand J; Brassier G; Houang M; Carel JC; Chomton M; Leger J Central Diabetes Insipidus in Infancy With or Without Hypothalamic Adipsic Hypernatremia Syndrome: Early Identification and Outcome. J Clin Endocrinol Metab, 2016.PMID 26588450
- [12]Zieg J Diagnosis and management of hypernatraemia in children. Acta Paediatr, 2022.PMID 34716953