Paeds · nephrology-urology-fluids-and-electrolytes
Posterior urethral valves
Also known as PUV · Posterior urethral valves · Congenital obstructive posterior urethral membrane · Lower urinary tract obstruction in male infants · Valve bladder syndrome
Fellowship guide to posterior urethral valves, the most common cause of lower urinary tract obstruction in male infants. Covers the Young classification of valve leaflets in the male posterior urethra, the back-pressure pathophysiology from the obstructed bladder through bilateral hydronephrosis and renal dysplasia to oligohydramnios and the Potter sequence, the antenatal and postnatal presentation, the micturating cystourethrogram as the diagnostic gold standard, the immediate catheter decompression and endoscopic valve ablation, the valve-bladder management with urodynamics and clean intermittent catheterisation, and the life-long chronic kidney disease surveillance driven by the nadir creatinine.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A boy who cannot empty his bladder has posterior urethral valves until imaging proves otherwise. The condition is a flap of tissue in the male urethra, just below the bladder, that blocks urine from getting out. Because the blockage sits below the bladder, the whole urinary tract above it is forced to work against high pressure, which damages the kidneys from before birth. Posterior urethral valves are the most common cause of lower urinary tract obstruction in male infants, and they carry a heavy life-long burden of kidney and bladder disease. [1]
The valve itself is a thin membrane-like fold in the posterior urethra. It forms during fetal development and is present from birth. Urine builds up behind it, the bladder thickens into a hard muscular wall, and the back-pressure travels up the ureters to the kidneys. In the worst cases the fetal kidneys fail to develop properly and produce too little urine, the amniotic fluid runs low, and the baby's lungs cannot grow, which is the Potter sequence. In milder cases the boy is well at birth and only turns up years later with a weak stream or repeated infections. [11]
Three facts make this condition central to paediatric fellowship exams. It occurs only in boys. The single most important thing you can do at the bedside is pass a urethral catheter. And even a perfect operation to remove the valves does not protect the kidneys for life, because the damage and the bladder problem were set up before birth. Robinson and colleagues showed in a population-based cohort that a large proportion of boys progress to chronic kidney disease despite successful valve ablation, which is why the management does not end when the valves are cut. [2]
Classification
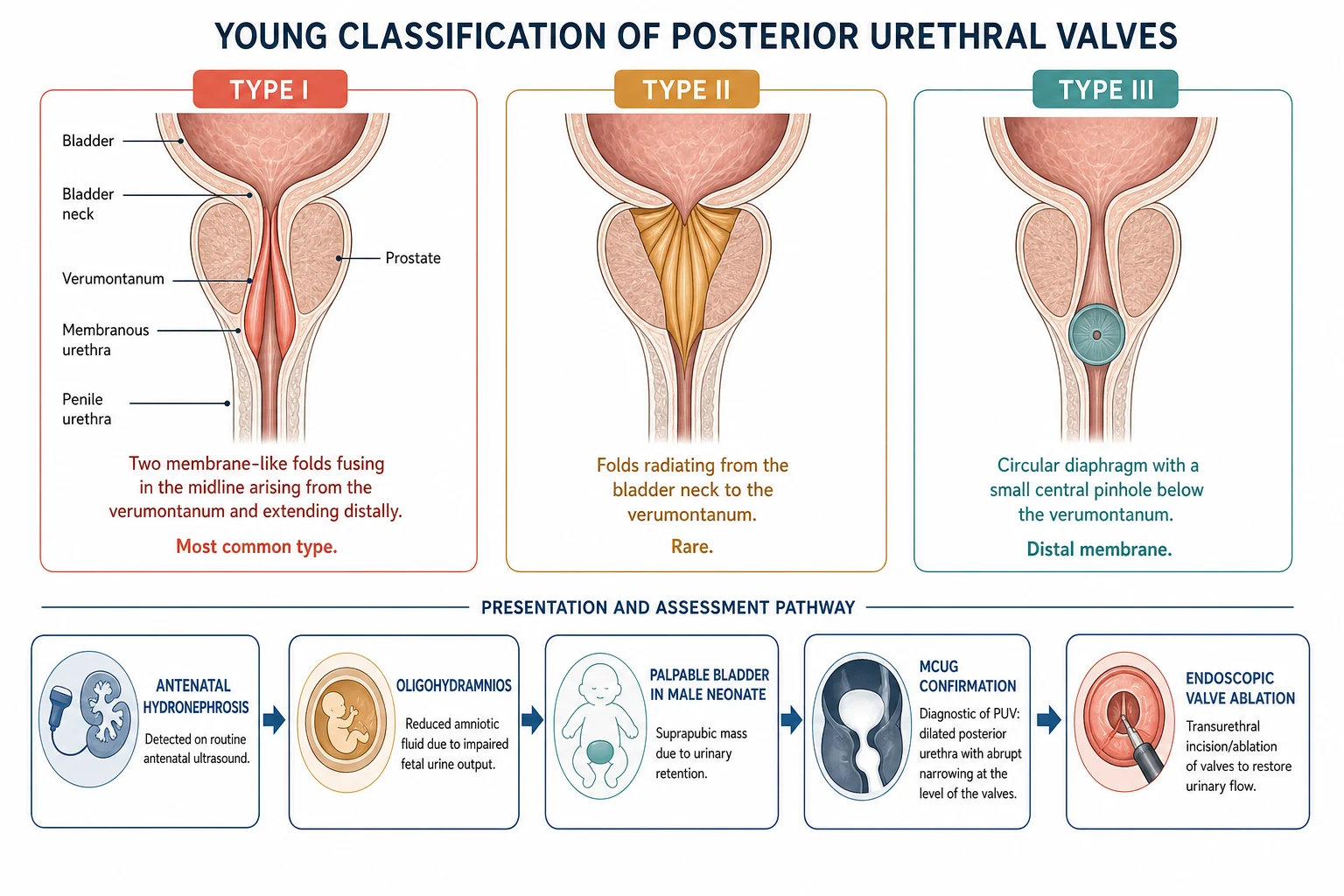
The Young classification, proposed a century ago, sorts the valves by where the obstructing tissue sits. It matters less for the operation than for the exam, because most boys have the same type and the surgery is the same. Hodges and colleagues set out the three types that examiners still ask about. [12]
The Type I valve is by far the most common. Two leaflets fuse in the midline and sweep down from the verumontanum, the small mound on the back wall of the urethra, so the tissue forms a sail that the urine pushes shut. The Type II valve describes folds running up from the verumontanum toward the bladder neck, but most urologists now regard these as non-obstructing mucosal ridges rather than true valves, and they are rare. The Type III valve is a round diaphragm with a tiny central hole sitting just below the verumontanum, which obstructs like a washer. [12]
A more useful way to think about valves for clinical decisions is by the severity of the obstruction, not the leaflet shape. A boy with a near-complete blockage presents as a sick newborn with Potter sequence, while a boy with a partial blockage may not be diagnosed until he is five years old with a dribbling stream. The severity of the obstruction, more than the Young type, predicts how badly the kidneys and bladder are damaged. [3]
Epidemiology & Risk Factors
Posterior urethral valves occur in approximately 1 in 4000 to 8000 live male births, and they occur only in boys. Caione and Nappo placed them as the single most common cause of lower urinary tract obstruction in male infants. The condition is sporadic in most families, but a small number of familial cases are recognised, which is why a family history of an affected male relative warrants a careful antenatal ultrasound. [1]
The risk factors that predict a poor outcome are the ones that tell you how badly the kidneys were injured before birth. Severe antenatal oligohydramnios signals that the fetal kidneys produced too little urine, which means dysplasia and the threat of pulmonary hypoplasia. Bilateral echogenic or cystic kidneys on the antenatal scan point to established dysplasia. A high nadir creatinine in the first year and persistent bladder dysfunction after the ablation both predict a downhill renal course. [3]
The near-universal antenatal ultrasound in high-income settings now means that most boys are identified before birth, which has shifted the clinical encounter from an emergency at the cot-side to a planned postnatal assessment. In remote and lower-resource settings, however, the late presentation with established kidney failure or severe infection is still common, and these children carry a worse prognosis because the damage is advanced by the time the valves are found. [2]
Pathophysiology
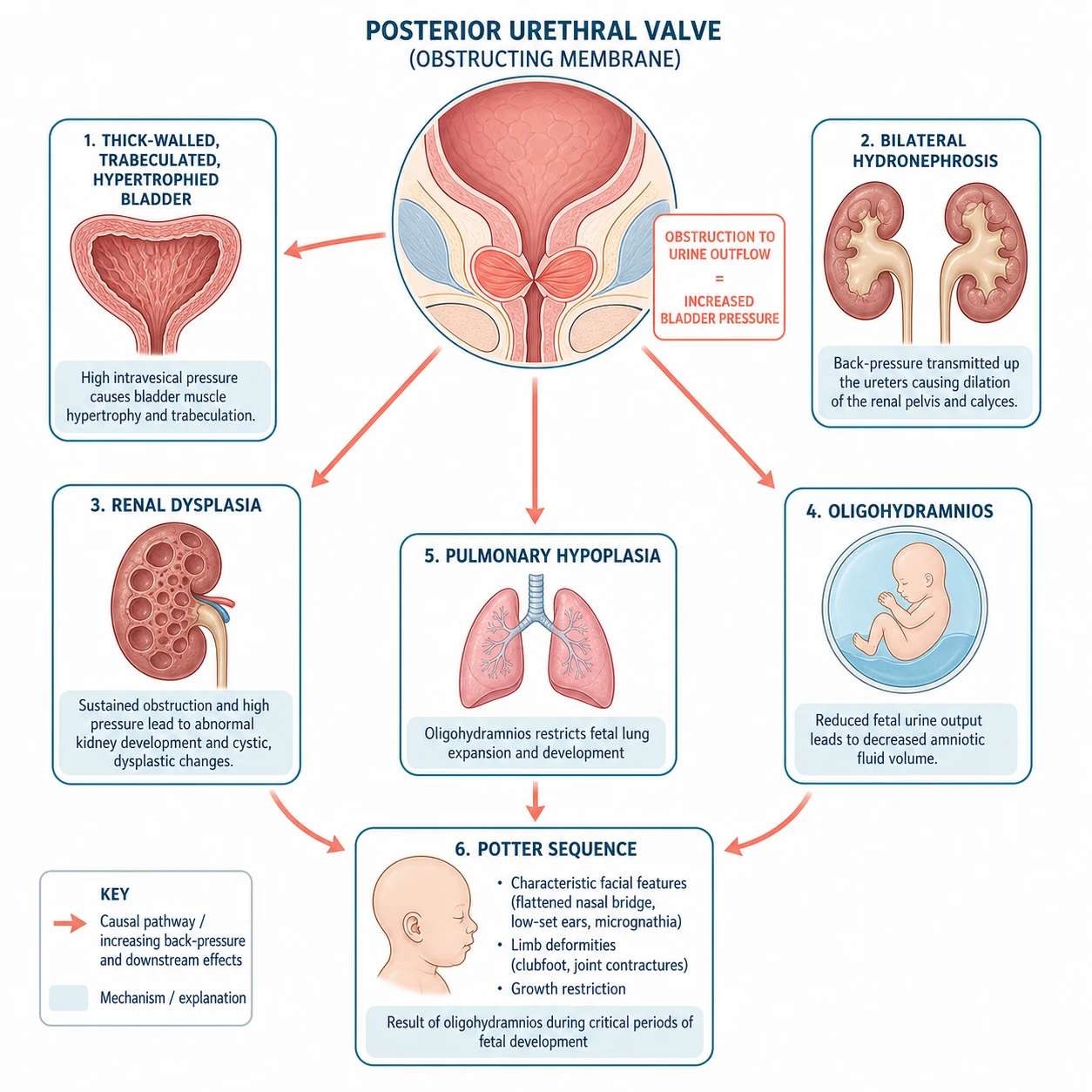
To understand the valves you follow the urine. The valve blocks the outflow, so the bladder has to squeeze harder to push urine past it. Over weeks and months in the fetus this builds a thick, muscular, trabeculated bladder wall that generates high pressures just to store a small volume. Those high pressures do not stay in the bladder. They travel straight up the ureters and into the kidney collecting systems, producing the bilateral hydronephrosis that is the first thing the antenatal scan sees. [11]
The pressure also damages the developing kidney tissue. The fetal kidney is still forming its nephrons when the obstruction begins, and sustained high pressure deranges that process, producing renal dysplasia, a kidney with disorganised tubules, cartilage, and cysts instead of working nephrons. Winyard and Chitty described how the timing and severity of the obstruction dictate the degree of dysplasia, because a kidney obstructed early in development never builds enough nephrons. The dysplastic kidney makes less urine, which sets off the next stage of the cascade. [11]
After about 16 weeks of gestation the fetal urine is the main ingredient of the amniotic fluid. When the obstructed, dysplastic kidneys produce too little urine, the amniotic fluid runs low, which is oligohydramnios. The fetus needs amniotic fluid to distend and grow its lungs and to move its limbs freely. Severe oligohydramnios causes pulmonary hypoplasia, the reason the worst-affected boys die of respiratory failure at birth, and it causes the limb contractures and characteristic facies of the Potter sequence. [5]
The final piece of the pathophysiology is the reduced nephron mass. A dysplastic kidney has fewer nephrons, and the surviving nephrons are forced to overwork, which raises the pressure inside each glomerulus and causes sclerosis over years. This hyperfiltration injury is the mechanism by which a boy whose valves were ablated in infancy can still drift into chronic kidney disease in adolescence, even when the operation was technically perfect. [2]
Clinical Presentation
The presentation splits into the antenatal finding and the postnatal picture. Most boys are now flagged before birth by a mid-trimester scan showing bilateral hydronephrosis, a thick-walled distended bladder, a dilated posterior urethra called the keyhole sign, and oligohydramnios. The antenatal team plans the place and mode of delivery, and the paediatric and urology teams are ready in the nursery. [5]
The severe postnatal presentation is the sick male newborn. He arrives in respiratory distress from the pulmonary hypoplasia, his abdomen is distended by a bladder you can feel above the pubis, and his urinary stream is weak or absent. He may already be in kidney failure with acidosis, hyperkalaemia, or fluid overload. This is the boy who cannot wait, because the airway and the bladder decompression compete for the first minute of your attention. [1]
The milder presentation is the boy who slipped through the antenatal net. He turns up in infancy or early childhood with recurrent urinary tract infection, a weak or dribbling stream, straining to void, daytime wetting, or simply poor growth and an incidental finding of hydronephrosis on an ultrasound done for another reason. These later presenters often have better kidneys, because the obstruction was partial, but their bladder dysfunction can be severe. [3]
How posterior urethral valves present across the age spectrum
Antenatal bilateral hydronephrosis with a thick-walled bladder and oligohydramnios, the most common mode today
A sick male newborn with respiratory distress from pulmonary hypoplasia and a palpable bladder
A male infant with a palpable distended bladder and a poor urinary stream
Recurrent febrile urinary tract infection in a male infant or toddler
A weak or dribbling stream, straining to void, or daytime wetting in an older boy
Failure to thrive or an incidental finding of hydronephrosis on imaging
A rare but exam-worthy presentation is the older child or adolescent with end-stage kidney disease whose valves were treated years ago and who now returns with hypertension, proteinuria, or a rising creatinine. Godlewski and colleagues reminded clinicians that the valve story does not end in childhood, and the adult with a history of valves needs ongoing renal and bladder surveillance. [10]
Differential Diagnosis
When a male fetus or neonate has bilateral hydronephrosis and a dilated bladder, posterior urethral valves head the list, but several other causes of lower urinary tract obstruction and bilateral upper tract dilation must be excluded, because the management differs. The micturating cystourethrogram is the single test that separates them, by showing the dilated posterior urethra that is specific to valves. [9]
Prune belly syndrome is the close mimic. It also occurs in boys and causes a dilated urinary tract, but it adds the two features that valves lack, an absent abdominal musculature so the belly looks wrinkled like a prune, and undescended testes. The abdomen of a prune belly infant is visibly lax, which is the opposite of the tensely distended abdomen of a boy with valves. [12]
A neurogenic bladder from occult spinal dysraphism, such as a tethered cord or a myelomeningocele, can also cause a thick-walled bladder and upper tract dilation. The clue is on the back, a sacral dimple, a hair tuft, a lipoma, or a sinus, and the lower limb neurology. Urethral atresia causes complete obstruction but is usually fatal without fetal intervention, and anterior urethral valves sit in the penile urethra and cause a cystic dilation of the urethra visible along the shaft. [3]
Posterior urethral valves
- Boys only, most common male LUTO
- Palpable distended bladder, poor stream
- MCUG: dilated posterior urethra with abrupt narrowing
- Normal abdominal wall and descended or undescended testes
Prune belly syndrome
- Boys, dilated urinary tract
- Absent abdominal musculature, wrinkled prune belly
- Bilateral undescended testes
- Often less severe renal dysplasia than valves
Neurogenic bladder
- Either sex, spinal cord lesion
- Sacral dimple, hair tuft, lipoma on the back
- Lower limb neurological signs
- MCUG: trabeculated bladder without a dilated posterior urethra
Severe bilateral vesicoureteral reflux and bilateral ureteropelvic junction obstruction can both mimic the hydronephrosis of valves, but neither produces the dilated posterior urethra on the MCUG, and neither typically gives the palpable bladder of an outflow obstruction. When the upper tracts are dilated but the bladder and urethra are normal, the problem lies above the bladder, not at the outlet. [9]
Clinical & Bedside Assessment
The bedside assessment of a boy with suspected valves answers three questions in order. Is he in danger now from lung failure or sepsis. What does his urinary tract look like. And how well are his kidneys working. You start with the airway and breathing, because the boy with Potter sequence may die of respiratory failure before the renal problem is addressed. [1]
The abdomen is the next focus. Feel for the bladder, which in a boy with valves is hard, rounded, and palpable above the pubis, and may reach the umbilicus. Feel for the kidneys, which may be enlarged and ballotable if they are hydronephrotic or dysplastic. The abdominal wall is normal in valves, which separates the condition from prune belly syndrome. Examine the external genitalia, because valves occur only in boys and the testes may be undescended, and examine the spine for the stigmata of occult dysraphism. [12]
The history focuses on the antenatal scans. The severity and the progression of the hydronephrosis, the amniotic fluid volume, and any fetal intervention all guide the urgency. A family history of an affected male relative raises the small possibility of familial recurrence. Ask about the urinary stream, any straining to void, and any previous urinary tract infection, because the late presenter often has a story of recurrent infection or a weak stream going back months. [3]
After you pass the catheter, watch the urine output closely. The relief of the obstruction can trigger post-obstructive diuresis, a large and sustained urine output that depletes the intravascular volume and drags out sodium and potassium. You replace the fluid and electrolytes hour by hour, guided by the urine output and the biochemistry, because an unrecognised post-obstructive diuresis can destabilise a neonate who was otherwise improving. [3]
Investigations
The investigation pathway is image-led, and each test answers one question. The first test after birth is the renal ultrasound, which confirms the antenatal finding and shows the bilateral hydronephrosis, the thick-walled bladder, and the dilated posterior urethra. The timing is flexible in valves, unlike in simple antenatal hydronephrosis, because the obstruction is already known and the ultrasound is done on the first day. [9]
The micturating cystourethrogram, abbreviated MCUG, is the diagnostic gold standard. A catheter fills the bladder with contrast and images are taken during filling and voiding. The MCUG shows the dilated posterior urethra with an abrupt narrowing at the level of the valves, the thick-walled trabeculated bladder, and any associated vesicoureteral reflux. Khondker and colleagues validated the posterior urethral morphology on the initial MCUG as a reliable predictor, confirming its central diagnostic role. [9]
Blood tests assess the renal function and the complications. The serum creatinine is the baseline marker, but in the first days of life it reflects the maternal creatinine and must be interpreted with care, so the trend over the first weeks matters more than any single early value. The electrolytes, the acid-base balance, and the full blood count screen for kidney failure and infection. Urinalysis and urine culture are essential, because a urinary tract infection may be the first sign and a catheter specimen is needed if the boy cannot void. [3]
The DMSA scan maps the renal cortex and shows the dysplasia and the split function between the two kidneys, but it is deferred until the neonate is older and the acute episode has settled. The MAG3 renogram assesses the drainage and the split function and is useful when an obstruction above the bladder is suspected. Urodynamics, the pressure-flow study of the bladder, are not part of the acute workup but are done later to characterise the valve bladder and to guide the bladder management. [6]
Management — Resuscitation
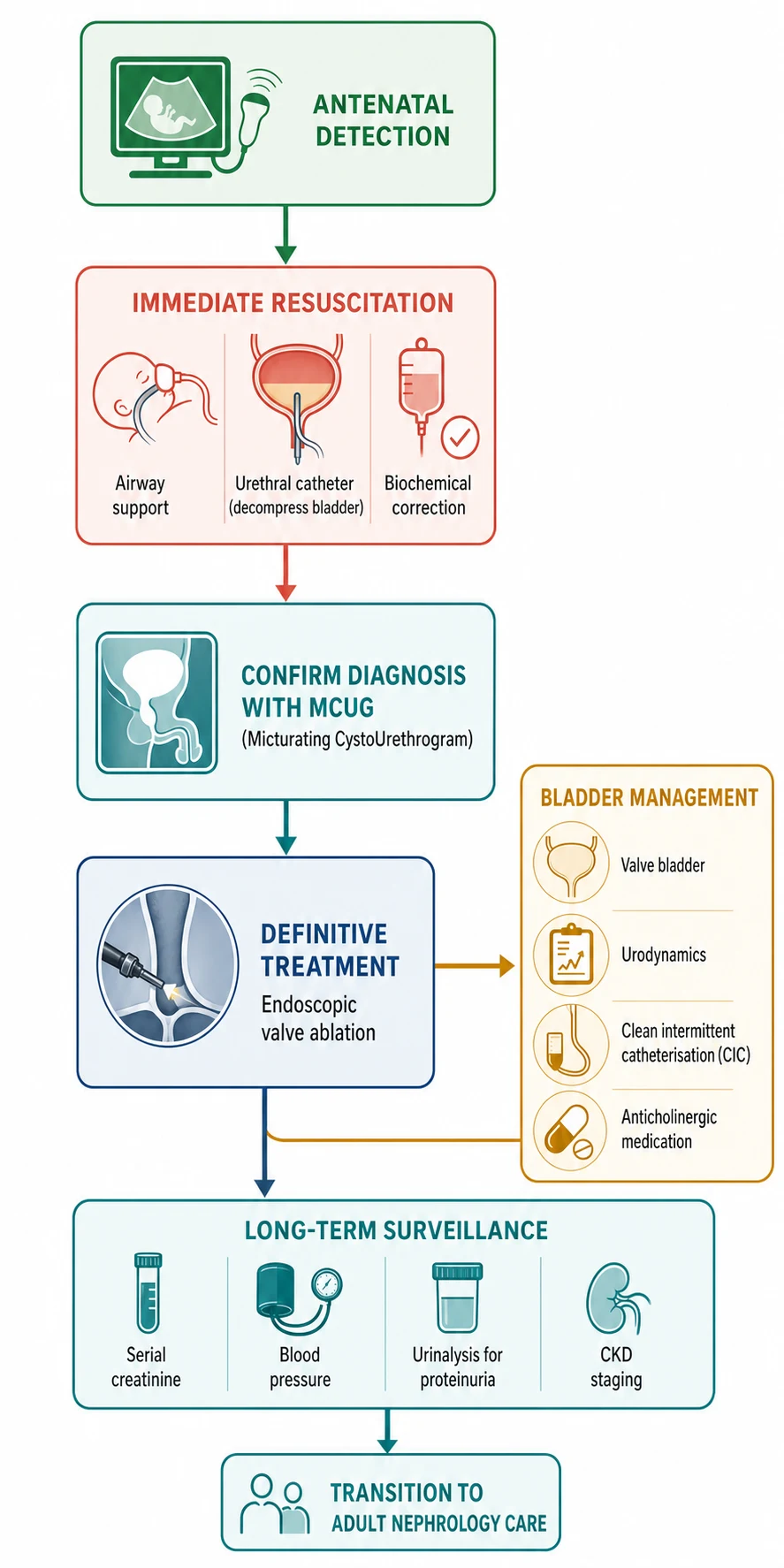
The resuscitation of a boy with suspected valves starts with the airway and the bladder, in that order. The neonate with pulmonary hypoplasia needs respiratory support first, because he will die of lung failure before renal failure if you do not breathe for him. Once the airway and breathing are secure, you decompress the bladder. [1]
Passing a urethral catheter is the first therapeutic intervention in any obstructive uropathy, and it is the one action that changes the renal perfusion within hours. A small feeding tube or a Foley catheter is passed gently into the bladder and left on free drainage. If the catheter will not pass, which can happen when the valve tissue or a tight urethra obstructs it, do not force it, because you will create a false passage, and call the urologist for a suprapubic catheter. The relief of the back-pressure improves the renal blood flow and allows the creatinine to fall toward its true baseline. [3]
The biochemical disturbances of renal failure are managed next. The obstructed, dysplastic kidneys may produce a metabolic acidosis, hyperkalaemia, or fluid overload, and these are corrected with the standard neonatal acute kidney injury protocols. Hyperkalaemia is treated first if it threatens the heart, the acidosis is corrected with bicarbonate, and fluid is restricted if the boy is overloaded. The nephrology team is involved early, and the renal replacement therapy pathway is readied for the boy whose disturbance is severe. [3]
Prophylactic antibiotic for the catheterised neonate with suspected valves
Dose
Trimethoprim 2 mg per kg at night
Prophylactic antibiotics are started at diagnosis, because the catheter and the obstructed system carry a high risk of urinary tract infection, which would compound the existing renal damage. The first choice is trimethoprim at 2 mg per kg at night, and the antibiotics are maintained until the definitive imaging is complete. Watch for the post-obstructive diuresis in the hours after decompression, and replace the fluid and electrolytes to keep the boy stable. [3]
Management — Definitive & Stepwise
[2]The definitive treatment is endoscopic valve ablation, performed once the neonate is stable and the renal function has been optimised. A small cystoscope is passed into the urethra, the valve leaflets are identified, and they are cut with a tiny electrode or a laser to restore the outflow. The catheter is maintained for a few days after the ablation, and the upper tracts are reassessed by ultrasound. The ablation is the beginning of the management, not the end, because the bladder and the kidneys need life-long attention. [1]
The boy who is too small or too unwell for an ablation, or the boy whose urethra will not take the cystoscope, needs a temporary diversion. A vesicostomy, a surgical opening of the bladder onto the abdominal wall, drains the urine at low pressure and buys time until the boy grows enough for a safe ablation. The vesicostomy is closed once the valves are ablated and the boy is ready for a normal voiding pathway. [3]
The valve bladder is the focus of the long-term urology care. The thick-walled, low-compliance bladder stores poorly and generates high pressures that damage the upper tracts, and de Jesus showed that the bladder dysfunction depends on many interacting variables. The bladder function is assessed by urodynamics after the ablation, and the management is tailored to the pattern. A poorly compliant bladder is managed with anticholinergic medication and, if that fails, with clean intermittent catheterisation. [7]
Oxybutynin for the poorly compliant valve bladder
Dose
0.2 to 0.4 mg per kg per dose, two to three times daily
Tang and colleagues emphasised the role of urodynamics in the boy with lower urinary tract symptoms after ablation, because the bladder pattern guides the choice between anticholinergic medication, clean intermittent catheterisation, and, in a few, bladder surgery such as augmentation. The aim is to keep the bladder storage pressure low enough to protect the kidneys, because a high-pressure bladder is the silent driver of the late renal decline. [6]
The chronic kidney disease surveillance runs in parallel. The blood pressure is measured at every visit, the urinalysis checks for proteinuria, and the serial creatinine and the estimated GFR track the renal trajectory. An ACE inhibitor or an angiotensin receptor blocker is commenced for the boy who develops hypertension or proteinuria, to slow the hyperfiltration injury. The transition to adult nephrology and urology care is planned in adolescence, because the CKD risk persists into adulthood. [2]
Specific Subtypes & Scenarios
The antenatally detected severe case, with oligohydramnios and bilateral echogenic kidneys, is the scenario that raises the question of fetal intervention. Cheung, Morris, and Kilby set out the rationale: the kidneys are still developing, and relieving the obstruction before birth might preserve the nephron mass and restore the amniotic fluid for lung growth. The candidate for fetal intervention is the male fetus with a favourable urine profile on serial sampling, performed in a tertiary fetal medicine centre. [5]
The fetal options are the vesicoamniotic shunt, a tube placed between the bladder and the amniotic cavity to bypass the obstruction, and the fetal cystoscopy, which ablates the valves directly in the fetus. Mustafa and colleagues produced an international Delphi consensus on the management of fetal lower urinary tract obstruction, which standardised the selection criteria and the core outcomes. The renal benefit of fetal intervention remains debated, and it is offered only in selected centres for the carefully selected fetus, because the procedure carries real risks. [4]
The late-presenting child is the second scenario. He comes in with a weak stream, daytime wetting, or recurrent infection at an age when his valves were never found. His renal prognosis is often better than the antenatally detected boy, because the obstruction was partial and the kidneys had time to develop, but his bladder dysfunction can be the dominant problem, and he needs the same urodynamic assessment and bladder management as the neonate. [7]
DUMP for the long-term complications of posterior urethral valves
The adult with a history of valves is the fourth scenario, and the one most often forgotten. Godlewski, Tekgul, and Gong reviewed the clinical considerations in adults, who present with hypertension, proteinuria, CKD, lower urinary tract symptoms, and issues of fertility and sexual function. The young man transferred from paediatric care needs an adult urology and nephrology team that understands the valve bladder, because the bladder and the kidneys keep aging together. [10]
Complications & Pitfalls
Chronic kidney disease is the dominant complication, and it is the one that defines the long-term prognosis. Robinson and colleagues showed in their population-based cohort that a large proportion of boys with valves progress to CKD over childhood and adolescence, with the risk influenced by the nadir creatinine in the first year, the degree of bilateral dysplasia, and the bladder function after ablation. The CKD may progress to end-stage kidney disease and the need for dialysis or transplantation, which makes the life-long nephrology surveillance essential. [2]
The valve bladder is the second key complication. The thick-walled, low-compliance bladder persists and often worsens after the ablation, because the bladder muscle learned to contract against the obstruction. The high storage pressures damage the upper tracts, the boy empties incompletely and wets by day, and the residual urine seeds recurrent infection. The valve bladder is the reason the urology follow-up is as important as the nephrology follow-up. [6]
The classic pitfalls are diagnostic and prognostic. Missing a male neonate with a palpable bladder, on the assumption that the distension is normal, delays the diagnosis and deepens the renal damage. Attributing the high neonatal creatinine solely to maternal transfer, rather than recognising the dysplasia, gives false reassurance in the first weeks. And assuming that a successful valve ablation has cured the boy, rather than committing him to life-long surveillance, misses the window to detect the early CKD and the high-pressure bladder. [3]
The post-obstructive diuresis is a pitfall of the decompression itself. In the hours after the catheter is passed, the kidneys dump the retained solute and water, and the urine output can exceed 5 mL per kg per hour. Without careful fluid and electrolyte replacement, the boy develops hypovolaemia, hyponatraemia, and hypokalaemia. The diuresis is self-limiting, but it must be managed hour by hour until it settles. [3]
Prognosis & Disposition
The prognosis is set largely before birth, by the severity of the renal dysplasia and the bladder remodelling, and the nadir creatinine in the first year is the single best predictor of the long-term renal outcome. Coleman and colleagues asked how high is low enough, and the widely used cut-off is a nadir creatinine below 0.8 mg per decilitre, which is about 70 micromoles per litre, in the first year of life. A boy below this threshold has a favourable prognosis, while a boy above it carries a high risk of progressive CKD. [8]
The bladder function modifies the prognosis over time. A boy with a well-managed, low-pressure bladder preserves his renal function longer than a boy with an unrecognised high-pressure bladder, which is why the urodynamics and the bladder therapy are prognostic as well as symptomatic. The recurrent infection and the hypertension each chip away at the remaining nephron mass, and the control of both is part of protecting the prognosis. [6]
Disposition is to a paediatric nephrology and urology service for every boy with confirmed valves, with the intensity of the follow-up tailored to the renal function and the bladder pattern. The boy with a good nadir creatinine and a low-pressure bladder may need only annual surveillance, while the boy with a high nadir and a poorly compliant bladder needs frequent review, imaging, and urodynamics. The transition to adult nephrology and urology care is planned in adolescence, because the CKD risk persists and may accelerate in adulthood. [10]
Special Populations
The fetus with severe oligohydramnios is the population at the frontier of care. The antenatal team of the maternal-fetal medicine specialist, the paediatric nephrologist, and the paediatric urologist counsels the family on the severity and the options, which range from fetal intervention in a selected case to palliative care in the most severe bilateral dysplasia. The fetus with a favourable urine profile may be offered a vesicoamniotic shunt or a fetal cystoscopy in a tertiary centre, while the fetus with established bilateral dysplasia and severe oligohydramnios is managed with honest counselling and a planned, compassionate approach. [4]
The Aboriginal and Torres Strait Islander child and the child from a remote setting present a different challenge. The higher background burden of kidney disease and the reduced access to antenatal ultrasound and specialist services compound the risk, and the late presentation with an advanced CKD is more common. The emphasis in these settings is on the early detection through the routine antenatal ultrasound, the prompt postnatal evaluation of any finding, and the culturally appropriate counselling and surveillance that keeps the family engaged with the long-term care. [2]
The boy with technology-dependent needs is the third population. The child on clean intermittent catheterisation, on overnight bladder drainage, or with a vesicostomy needs a coordinated package of education, equipment, and community nursing, and the family is taught the catheterisation and the recognition of infection before discharge. The technology supports the bladder and protects the kidneys, but it places a daily burden on the family that the team must acknowledge and resource. [7]
The young adult transitioning from paediatric to adult care is the final population. The valves may have been ablated in infancy, but the CKD risk and the valve bladder persist into adulthood. The transition plan addresses the blood pressure monitoring, the renal function surveillance, the bladder and continence management, the fertility and sexual function, and the coordination between the paediatric and the adult nephrology and urology services. Godlewski and colleagues reminded clinicians that the valve story does not end at the age of transfer. [10]
Evidence, Guidelines & Regional Differences
The evidence base for posterior urethral valves has been reshaped by the population-based outcome studies. The cohort by Robinson and colleagues quantified the substantial CKD progression over childhood and adolescence, which has intensified the surveillance and the bladder management after ablation. The nadir creatinine study by Coleman and colleagues established the prognostic threshold that guides the counselling of families and the intensity of the follow-up. [2]
The fetal management evidence is more contested. Cheung, Morris, and Kilby reviewed the congenital urinary tract obstruction and the rationale for fetal intervention, and the international Delphi consensus by Mustafa and colleagues standardised the selection criteria and the core outcomes. The renal benefit of fetal intervention remains debated, and the consensus emphasises the careful selection of the fetus with a favourable urine profile, performed only in tertiary fetal medicine centres. [4]
Robinson 2024
- JASN population-based cohort on long-term kidney outcomes
- Quantified the substantial CKD progression in childhood
- Intensified the surveillance after valve ablation
Coleman 2015
- J Pediatr Urol on the nadir creatinine threshold
- Established the prognostic cut-off under 0.8 mg per decilitre
- Guides the counselling and the intensity of follow-up
Mustafa 2024
- Ultrasound in Obstetrics and Gynecology Delphi consensus
- Standardised fetal lower urinary tract obstruction management
- Core outcome set for fetal intervention studies
Deshpande 2018
- Pediatric Nephrology review of current strategies
- Prediction and management of the valve sequelae
- Synthesised the prognostic and therapeutic approach
The regional differences centre on the access to antenatal ultrasound and specialist care. In the high-income settings, the near-universal antenatal detection and the standardised postnatal pathway allow the early catheter decompression and the planned valve ablation. In the lower-resource and remote settings, the later presentation with an advanced CKD or a severe infection is more common, and the emphasis shifts to the prompt decompression and the prevention of the reversible causes. The international consensus on the investigation of fetal lower urinary tract obstruction applies across the settings, with the intensity of the fetal and postnatal intervention tailored to the local resources. [4]
Exam Pearls
ABC for the immediate management of a male neonate with suspected valves
References
- [1]Caione P, Nappo SG Posterior urethral valves: long-term outcome. Pediatr Surg Int, 2011.PMID 21748651
- [2]Robinson CH, Rickard M, Jeyakumar N, de Carvalho M, Lorenzo AJ, Farhat WA, et al Long-Term Kidney Outcomes in Children with Posterior Urethral Valves: A Population-Based Cohort Study. J Am Soc Nephrol, 2024.PMID 39167453
- [3]Deshpande AV Current strategies to predict and manage sequelae of posterior urethral valves in children. Pediatr Nephrol, 2018.PMID 29159472
- [4]Mustafa HJ, Khalil A, Johnson S, Shen O, Sonek J, Lopriore E, et al Fetal lower urinary tract obstruction: international Delphi consensus on management and core outcome set. Ultrasound Obstet Gynecol, 2024.PMID 38748971
- [5]Cheung KW, Morris RK, Kilby MD Congenital urinary tract obstruction. Best Pract Res Clin Obstet Gynaecol, 2019.PMID 30819578
- [6]Tang LF, Bi YL, Fan Y Posterior Urethral Valves with Lower Urinary Tract Symptoms: Perspective on Urodynamics. J Invest Surg, 2021.PMID 32292072
- [7]de Jesus LE Bladder dysfunction depends on many variables in children with posterior urethral valves. Int Braz J Urol, 2022.PMID 34735084
- [8]Coleman R, King T, Nicoara CD, Madi M, Chandran H, Parashar K, et al Nadir creatinine in posterior urethral valves: How high is low enough? J Pediatr Urol, 2015.PMID 26292912
- [9]Khondker A, Chelliahpillai Y, Machado M, Jackson LI, Bruch D, Offorh C, et al External validation and reliability assessment of posterior urethral morphology on initial voiding cystourethrogram as a predictor for infants with posterior urethral valves. J Pediatr Urol, 2024.PMID 38129272
- [10]Godlewski K, Tekgul S, Gong E Clinical considerations in adults with history of posterior urethral valves. J Pediatr Urol, 2024.PMID 37806832
- [11]Winyard P, Chitty LS Dysplastic kidneys. Semin Fetal Neonatal Med, 2008.PMID 18065301
- [12]Hodges SJ, Patel B, McLorie G Posterior urethral valves. ScientificWorldJournal, 2009.PMID 19838598