Paeds · nephrology-urology-fluids-and-electrolytes
Scrotal pain and testicular torsion
Also known as Acute scrotum · Testicular torsion · Torsion of the spermatic cord · Torsion of the appendix testis · Acute epididymitis
Fellowship guide to scrotal pain and testicular torsion in boys. Covers the bell-clapper deformity and intravaginal torsion, the 6-hour salvage window, the TWIST score for the acute scrotum, the differentiation of torsion from torsion of the appendix testis and acute epididymitis, the role of colour Doppler ultrasound, immediate surgical exploration with detorsion and bilateral orchidopexy, manual detorsion as a bridge, the extravaginal perinatal form, intermittent torsion, and the fertility and medicolegal consequences of a missed diagnosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A boy who wakes in the night with sudden severe testicular pain has torsion until you have proved otherwise. Testicular torsion is the twisting of the spermatic cord on its long axis, which strangles the testicular blood supply and kills the testis within hours. It is the can't-miss diagnosis in any male with acute scrotal pain, because a missed torsion is a lost testis and a preventable medicolegal disaster. [1]
The cord carries the artery that feeds the testis and the veins that drain it. A twist compresses the thin-walled veins first, so the testis swells and congests, and then it collapses the artery, so the swollen organ becomes ischaemic. The whole process is governed by time. The salvageable window is short, and the testis that is not untwisted within hours becomes necrotic and has to be removed. [1]
Three facts make this topic central to the paediatric exam. The diagnosis is clinical, and a convincing picture goes straight to theatre without waiting for a scan. The determinant of outcome is the duration of torsion, which is why the 6-hour rule governs every decision. And the differential of the acute scrotum is narrow but high-stakes, because torsion sits beside the benign torsion of the appendix testis and the treatable acute epididymitis, and the only safe way to tell them apart at the bedside is a structured, time-critical assessment. Sharp and colleagues set out these principles in their widely cited review. [1]
Classification
Torsion is best understood by where on the cord the twist occurs and by its tempo. The classification matters because it predicts the age, the presentation, and whether the testis can be saved. Davis and Silverman set out the three patterns that examiners still ask about. [8]
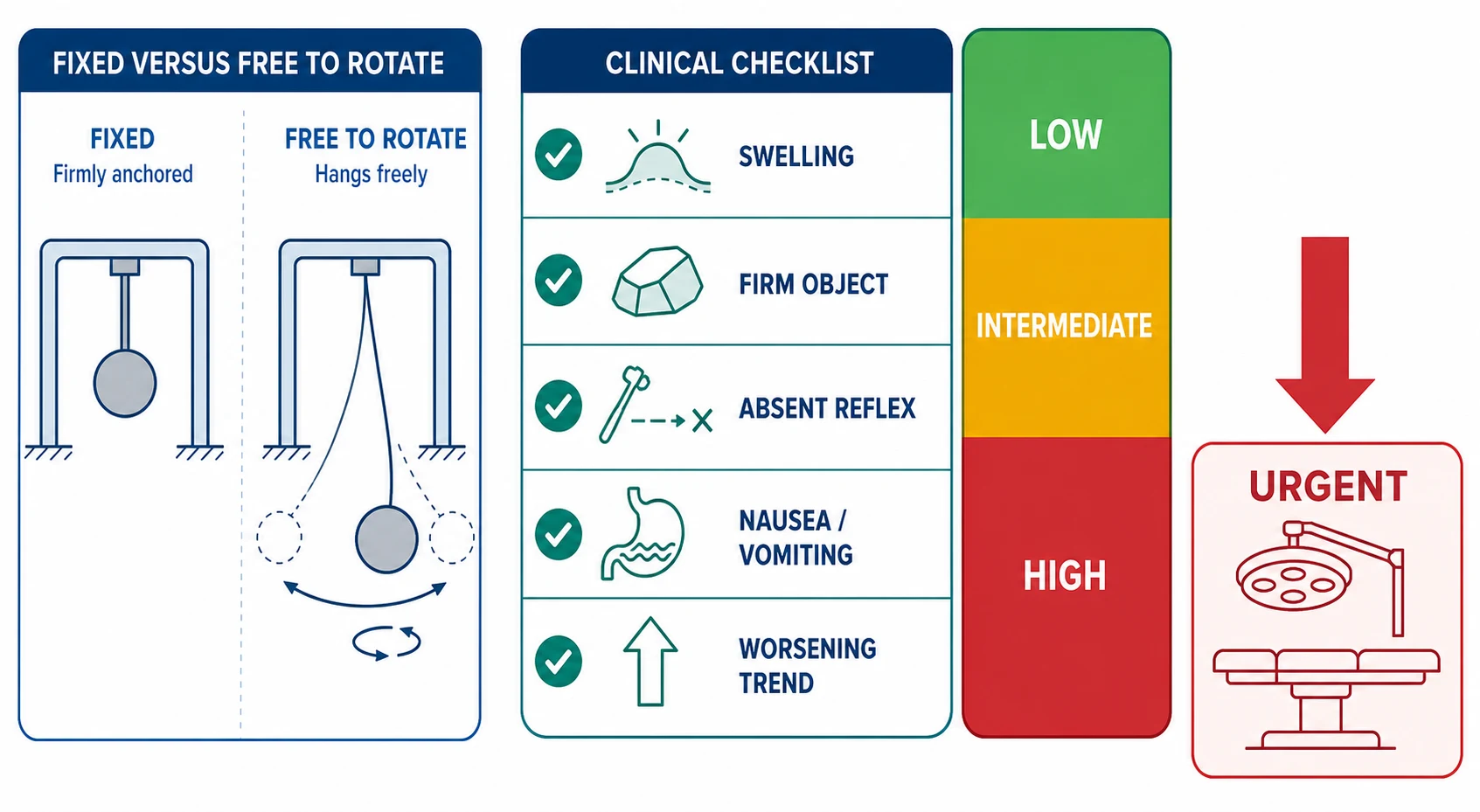
The common form is intravaginal torsion. The twist happens inside the tunica vaginalis, the thin sac that wraps the testis, because a developmental anomaly called the bell-clapper deformity lets the tunica invest too high on the cord. The testis then hangs freely inside its sac, like the clapper inside a bell, and can spin on the cord. This is the form of the adolescent boy, peaking between 12 and 18 years, and it is the one most relevant to the fellowship exam. [1]
The perinatal form is extravaginal torsion. The whole cord and its coverings twist as a unit before the tunica fuses to the scrotal wall, which is a normal event in late fetal life. This happens before or just after birth, the testis is usually already infarcted, and the baby presents with a hard, painless, discoloured scrotal mass. Salvage is rare, and the role of surgery is chiefly to fix and protect the contralateral testis. Erlich and colleagues described the clear-cut, the controversial, and the quiet scenarios of perinatal torsion. [12]
The third pattern is intermittent torsion. The boy describes repeated episodes of acute testicular pain that come on suddenly and resolve on their own as the testis detorses, often over minutes to a couple of hours. It is commonly mislabelled as epididymitis or growing pains, but it carries a high risk of a future complete, non-resolving torsion, and it is treated by elective bilateral orchidopexy rather than watchful waiting. [2]
Epidemiology & Risk Factors
Testicular torsion has a bimodal age distribution. A small neonatal peak reflects the perinatal extravaginal form, and a much larger adolescent peak between 12 and 18 years reflects intravaginal torsion, with most series placing the bulk of cases in males aged roughly 12 to 25 years. The annual incidence is about 1 in 4000 males under 25 years per year. [1][11]
The dominant risk factor is the bell-clapper deformity, which is bilateral in about 12 percent of boys, and this is the anatomical reason a torsion on one side threatens the other. A second risk factor is an undescended testis, which carries a roughly tenfold higher risk of torsion than a fully descended one, which is why a torsion in an undescended testis is a recognised reason to fix or bring down the contralateral gland. Sudden cremasteric contraction during cold, exertion, or minor trauma is the usual trigger, but many episodes are unprovoked and wake the boy from sleep. [11]
Mansbach and colleagues studied the risk factors for losing the testis, and the message for the clinician is sobering. The single strongest predictor of orchiectomy is the duration of symptoms before surgery, which is why every minute of delay, including delay for imaging, converts directly into lost testes. Ramachandra and colleagues confirmed the same finding in a tertiary paediatric centre, where the salvage rate tracked the time from pain onset to the operating room. [11][4]
Pathophysiology
To understand torsion you follow the blood. The spermatic cord carries the testicular artery, which feeds the gland, alongside the thin-walled pampiniform venous plexus, which drains it. A twist does not strangle everything at once. It compresses the low-pressure veins and lymphatics first, so the testis swells and congests inside its unyielding covering, the tunica albuginea. [1]
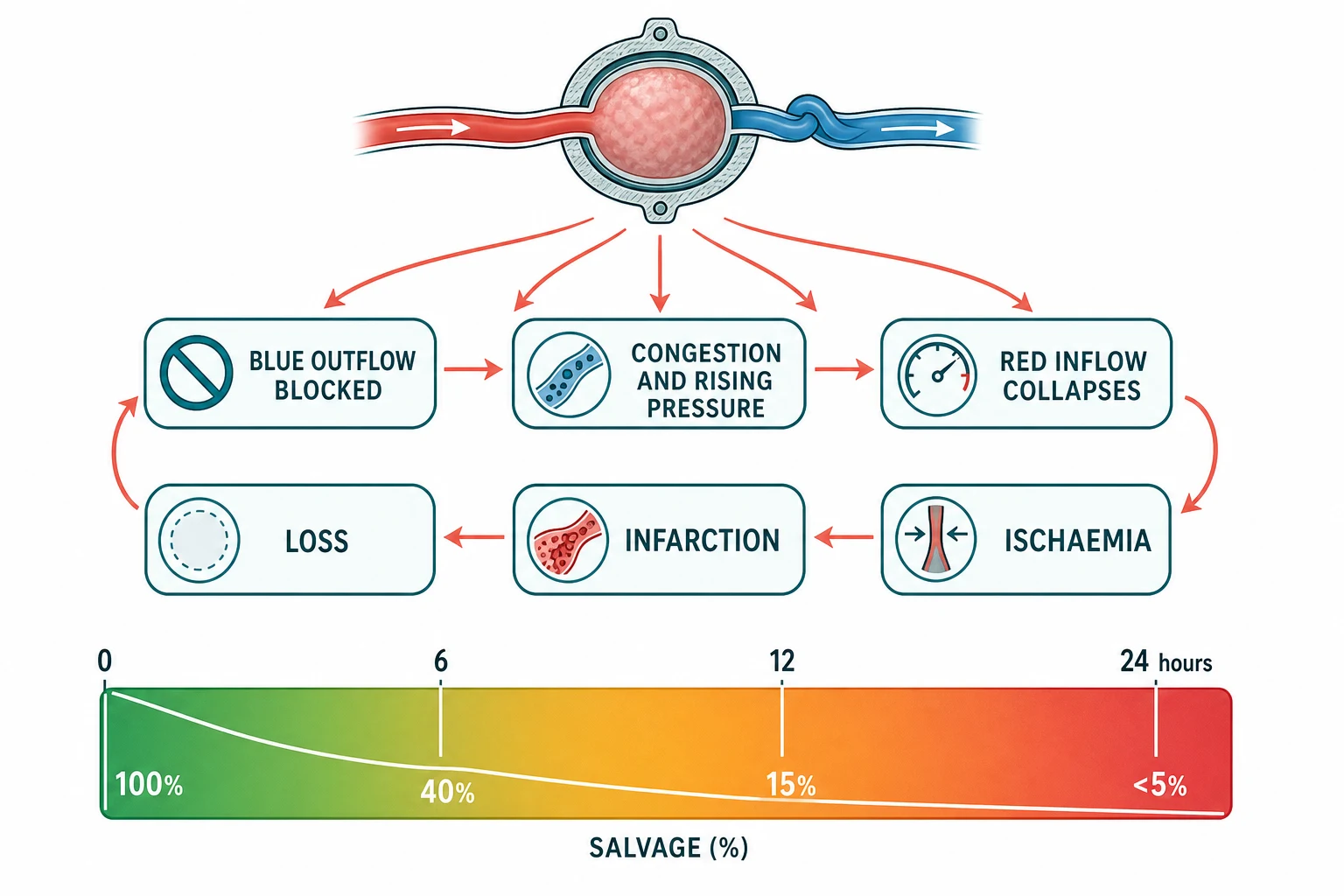
The rising tissue pressure inside the inelastic tunica then collapses the higher-pressure artery. This converts a congested but still-perfused testis into an ischaemic one, and it is the arterial occlusion that begins the irreversible injury. A complete torsion usually twists through 360 to 720 degrees, one to two full turns, and the tighter and longer the twist, the faster the artery fails. [1]
The result is the steep salvage curve that governs the whole topic. Detorsion within about 6 hours of the onset of pain salvages the testis in roughly 90 to 100 percent of boys. Between 6 and 12 hours the salvage rate falls to about 50 percent, between 12 and 24 hours to less than 20 percent, and beyond 24 hours it is near zero, when orchidectomy is the expected outcome. Sharp and colleagues emphasised that this curve is the reason time, not the scan, drives the decision. [1]
A subtlety worth knowing is that even a salvaged testis is not guaranteed to be normal. After an episode of torsion, the blood-testis barrier can be disrupted and antisperm antibodies may form, which is the proposed mechanism for the later subfertility seen in some boys despite a successful orchidopexy. Aggarwal and colleagues documented the long-term impact of torsion and its salvage on semen parameters and gonadal function, which is why fertility surveillance is part of the follow-up. [7]
Clinical Presentation
The classic story is unmistakable once you have heard it. A boy, usually an adolescent, develops sudden severe unilateral scrotal pain, often in the night or after exertion. The pain is often referred to the lower abdomen or the groin, because the nerve supply of the testis shares its roots with the abdominal wall, and this referral is a frequent trap. Nausea and vomiting are common and, together with the sudden severe pain, they raise the probability of torsion rather than a mimic. [2]
On examination the testis is swollen and exquisitely tender. It lies higher than its fellow, because the shortened twisted cord pulls it up toward the groin, and it often lies horizontally rather than vertically. The cremasteric reflex is absent on the affected side, and this is the single most sensitive sign of torsion, although its absence is not perfectly specific and its presence does not fully exclude torsion. The scrotum may be erythematous and oedematous, and a reactive hydrocele can develop within hours, making the examination harder. [1]
How torsion presents across the age spectrum
A perinatal extravaginal torsion presenting as a hard, painless, discoloured scrotal mass in a newborn
A prepubertal boy with acute scrotal pain that may be torsion or torsion of the appendix testis, distinguished by the bedside findings
An adolescent boy with sudden severe unilateral scrotal pain, a high-riding horizontal testis, and an absent cremasteric reflex, the classic picture
An older boy with recurrent self-limiting episodes of acute testicular pain suggesting intermittent torsion
A boy who has delayed presentation for many hours and arrives with a swollen, indurated, relatively painless testis that is likely already infarcted
Two atypical presentations are deliberately examined. The first is the boy whose abdominal pain hides a torsion, because the referred pain dominates and the scrotum is never examined. The rule is simple and load-bearing: any boy with unexplained lower abdominal or groin pain must have his scrotum examined. The second is intermittent torsion, in which the pain resolves before assessment and the examination is normal, so the diagnosis rests on the history of recurrent stereotyped episodes, and the management is elective bilateral orchidopexy. [2]
Differential Diagnosis
The acute scrotum has a short differential, and the task is to separate the surgical emergency from the conditions that can be managed conservatively. The discriminator is a combination of the onset, the lie of the testis, the cremasteric reflex, and the systemic features, brought together by the TWIST score. [8]
Testicular torsion
surgical emergency, adolescent
- Sudden severe onset, often waking the boy
- Absent cremasteric reflex, high-riding horizontal testis
- Nausea and vomiting common
- Urine usually clear; high TWIST score, go to theatre
Torsion of the appendix testis
self-limiting, prepubertal
- Gradual onset, less severe pain, typically aged 2 to 12 years
- Normal lie, cremasteric reflex usually present
- Blue dot sign at the upper pole of the testis
- Self-limiting, managed with rest and analgesia
Acute epididymitis
treatable, older boy
- Gradual onset, fever, dysuria, pyuria
- Tenderness localised to the epididymis initially
- Cremasteric reflex present; Prehn sign unreliable
- Prepubertal often viral or structural; adolescent often sexually transmitted
Torsion of the appendix testis is the commonest mimic in the prepubertal boy. The appendix testis is a small Mullerian remnant on the upper pole of the testis, and when it twists it produces a more gradual, less severe pain with a normal testicular lie and a usually intact cremasteric reflex. The hallmark is the blue dot sign, a small dark area at the upper pole where the infarcted appendix shows through the skin, and the condition is self-limiting, managed with rest and analgesia. [8]
Acute epididymitis is the other principal mimic, and it tends to affect the older, often sexually active, adolescent. The onset is gradual, fever and dysuria are common, the urine shows pyuria, and the tenderness begins in the epididymis rather than the testis itself. The cremasteric reflex is preserved, and the Prehn sign, relief of pain on elevating the scrotum, is classically taught but unreliable and should not be used to exclude torsion. In the prepubertal boy epididymitis is usually viral or associated with a structural urinary abnormality, while in the adolescent it is often sexually transmitted, which changes the investigation and the treatment. [2]
Less common causes round out the differential. Idiopathic scrotal oedema is a painless, bilateral, boggy oedema of the scrotal wall in young boys with a normal testis underneath. An incarcerated inguinal hernia presents with a groin mass extending into the scrotum and bowel obstruction. Trauma, a varicocele, and a Henoch-Schonlein purpura with scrotal vasculitis can each cause acute scrotal pain or swelling, but none produces the sudden severe pain, the high-riding testis, and the absent cremasteric reflex of torsion. [8]
Clinical & Bedside Assessment
The bedside assessment of the acute scrotum is a structured race against the clock, and it is examined directly in the clinical exams. You state that this boy has torsion until you have shown otherwise, you record the time the pain started, and you examine the scrotum gently and systematically. The assessment must take minutes, not hours, because every minute of delay erodes the salvage rate. [1]
The history focuses on the onset and the prior episodes. A sudden onset, pain that woke the boy, and associated nausea and vomiting all raise the probability of torsion, while a gradual onset with fever and dysuria points toward epididymitis. A history of recurrent short-lived episodes that resolved spontaneously is the signature of intermittent torsion, and a single such episode in an at-risk boy warrants elective orchidopexy. [2]
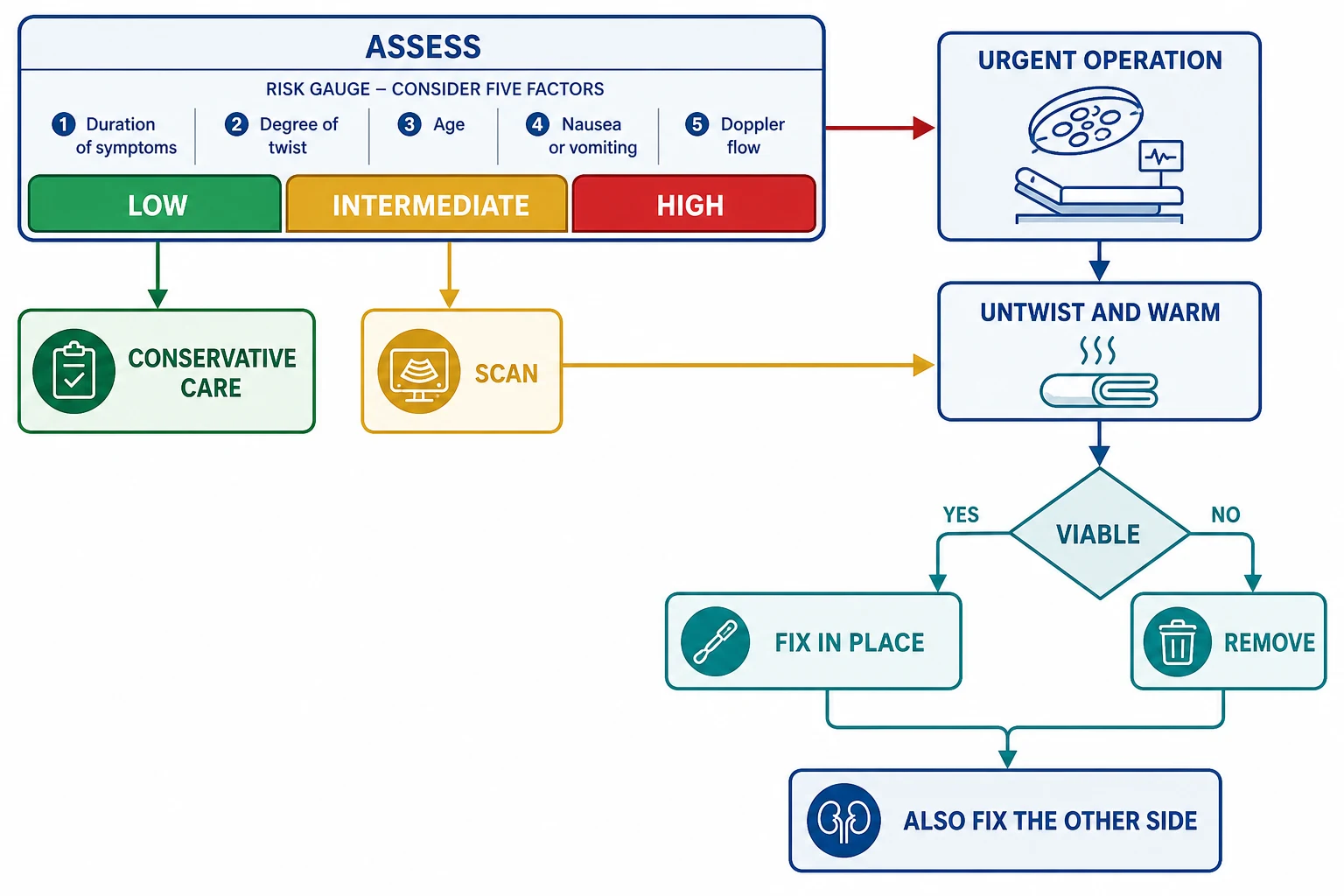
The TWIST score, the Testicular Workup for Ischemia and Suspected Torsion, is the validated way to turn the bedside findings into a probability of torsion. It assigns one point each for testicular swelling, a hard testis, an absent cremasteric reflex, nausea or vomiting, and a high-riding testis, for a maximum of five. A score of 0 to 2 is low risk, 3 to 4 is intermediate risk, and 5 is high risk. The systematic review and meta-analysis by Qin and Qu confirmed that the score discriminates torsion from its mimics, and the paediatric evaluation by Manohar and colleagues and the adult validation by Barbosa and colleagues support its use across the age range. [5][9]
Investigations
The investigation of the acute scrotum is governed by one principle: imaging must never delay exploration in a boy with high-probability torsion. A urinalysis and a urine culture are sent, because pyuria points toward epididymitis, but a clear urine does not exclude torsion, and an infected urine does not exclude it either, since a boy can have both. [1]
Colour Doppler ultrasound is the imaging test of choice when the diagnosis is genuinely in doubt, that is, in the intermediate-risk boy. The hallmark of torsion is reduced or absent intratesticular blood flow relative to the contralateral testis, and the scan can also show increased flow in epididymitis and the enlarged appendix in torsion of the appendix testis. The systematic review by McLaren confirmed that Doppler ultrasound has good diagnostic performance overall, but it is an adjunct and not a gatekeeper, and it can be falsely reassuring in the small prepubertal testis, in early or partial torsion, and in the hand of an inexperienced operator. [3]
Colour Doppler ultrasound in the acute scrotum
Dose
Intermediate-risk TWIST score (3 to 4) only
The 2024 ACR Appropriateness Criteria for the acute onset of scrotal pain reaffirm that colour Doppler ultrasound is the appropriate first-line imaging test for the equivocal presentation, but they also reinforce that a high clinical suspicion warrants surgical exploration without imaging. The blood tests are not diagnostic. A full blood count and a group and save are useful for the boy heading to theatre, but they do not distinguish torsion from its mimics, and they must not be allowed to delay the operation. [10]
The single most important investigation point is a communication one. If the probability of torsion is high, the next action is to call the surgical or urological team and transfer the boy to theatre, not to book a scan. The negative exploration rate, operating on a boy who turns out to have a mimic, is accepted and expected, and a senior clinician would always prefer a negative exploration to a missed torsion. Laher and colleagues emphasised that a low threshold for exploration is the standard of care. [2]
Management — Resuscitation
The resuscitation of suspected torsion is the preparation for theatre, and it happens in parallel with the surgical referral. You make the boy nil by mouth, you secure intravenous access, you give adequate analgesia, and you call the surgeon the moment torsion is on the differential. The aim is to have the boy in theatre inside the 6-hour window, which means the decision and the referral must be made within the first hour of arrival. [2]
Adequate analgesia is humane and it does not obscure the diagnosis, because the relief of pain does not restore the testicular lie or the cremasteric reflex. A simple analgesic such as paracetamol is started, and an opioid such as morphine is added for severe pain, with the doses adjusted to the child's weight. The analgesia is not a substitute for surgery, and the boy is reassessed after it takes effect, but the plan for theatre does not wait for the pain to settle. [1]
Analgesia for the boy with suspected torsion awaiting theatre
Dose
Paracetamol 15 mg per kg orally or intravenously, every 4 to 6 hours
Manual detorsion is a bedside manoeuvre that can be offered while the boy waits for theatre, but it is a bridge and not a substitute for surgery. The testis is gently rotated laterally, from the medial to the lateral side, described as opening the book, because most torsions twist the testis inward. The relief of pain and the return of a normal lie suggest success, but the boy still goes to theatre for definitive fixation, because the manoeuvre is incomplete and the testis can retorse. It is painful and often needs analgesia or a spermatic cord block, and it is never used to avoid the operation. [8]
Management — Definitive & Stepwise
The definitive treatment of torsion is urgent scrotal exploration, and it is both the diagnostic and the therapeutic standard. The scrotum is opened, the cord is delivered and untwisted, and the testis is wrapped in warm saline and observed. Viability is judged by the return of a pink colour and by bleeding from an incision in the tunica albuginea, and the decision to keep or to remove the testis rests on that viability assessment. [1]
[1]A viable testis is fixed to the scrotal wall with non-absorbable sutures, which is the orchidopexy. A necrotic testis is removed, which is the orchidectomy, and a prosthetic testis can be offered later for cosmesis. The critical step that is always performed, whether the testis is saved or removed, is the fixation of the contralateral testis, the contralateral orchidopexy, because the bell-clapper deformity is bilateral in about 12 percent of boys and a torsion on one side threatens the other. Ramachandra and colleagues confirmed that the duration of torsion before surgery is the dominant determinant of salvage, which is why the operation is urgent rather than semi-elective. [1][4]
The operative steps of scrotal exploration for torsion
Urgent scrotal exploration under general anaesthesia, ideally within 6 hours of pain onset
Delivery of the testis and the twisted cord, and detorsion by rotating laterally, opening the book
Wrapping the testis in warm saline and observing for the return of colour
Assessment of viability by bleeding from an incision in the tunica albuginea
Orchidopexy of the viable testis with non-absorbable sutures, or orchidectomy if necrotic
Contralateral orchidopexy in every case, because the bell-clapper deformity is often bilateral
The intermediate-risk boy, with a TWIST score of 3 to 4, undergoes urgent colour Doppler ultrasound, and if the scan shows reduced or absent flow he proceeds to exploration on the same pathway. The low-risk boy, with a score of 0 to 2 and a convincing alternative diagnosis such as torsion of the appendix testis, can be managed conservatively, but he is safety-netted and told to return immediately if the pain worsens, because a low score does not perfectly exclude torsion. Mansbach and colleagues showed that delayed presentation is the dominant driver of orchiectomy, which is why the threshold to explore is deliberately low. [11]
The management of the mimics runs alongside. Torsion of the appendix testis is managed with rest and simple analgesia such as a non-steroidal anti-inflammatory drug, and it resolves over days. Acute epididymitis is managed with antibiotics directed to the cause, with hydration and analgesia, and with investigation for a structural urinary abnormality in the prepubertal boy and for sexually transmitted infection in the adolescent. [8]
Antibiotics for acute epididymitis in the sexually active adolescent
Dose
Ceftriaxone 500 mg intramuscularly as a single dose plus doxycycline 100 mg twice daily for 10 to 14 days
Specific Subtypes & Scenarios
Perinatal torsion is the scenario that tests the candour of the clinician. The newborn presents with a hard, fixed, painless, discoloured scrotal mass, the testis is usually already infarcted at birth, and the salvage rate is low. Erlich and colleagues framed the perinatal form into the clear-cut case that is beyond salvage, the controversial case where the timing of the torsion is uncertain, and the quiet case that is found incidentally. The role of urgent exploration is chiefly to fix and protect the contralateral testis, because a synchronous or metachronous bilateral torsion is the catastrophic outcome that surgery is trying to prevent. [12]
Intermittent torsion is the second scenario, and it is the one most often missed. The boy describes recurrent episodes of acute testicular pain that resolve spontaneously, the examination between episodes is normal, and the temptation is to label the pain as epididymitis or growing pains. The correct response is to take the history seriously and to offer elective bilateral orchidopexy, because the natural history is a high risk of a future complete, non-resolving torsion that will cost the testis. [2]
Torsion in the undescended testis is the third scenario, and it presents as an acute groin or abdominal mass with an empty scrotum. The risk of torsion in an undescended testis is roughly tenfold that of a descended one, and the diagnosis is harder because the testis cannot be examined directly. The management is urgent exploration, with detorsion and orchidopexy if the testis is viable and orchidopexy or orchidectomy depending on the findings, and the episode reinforces the case for the elective surgical correction of the undescended testis. [11]
The delayed-presentation torsion is the fourth scenario, and it is the one that most often ends in orchidectomy. The boy who presents many hours after the pain, with a swollen, indurated, and now relatively painless testis, often has an infarcted gland, and the operation is as much about confirming the diagnosis and fixing the other side as about saving the testis. Mansbach and colleagues documented the strong link between delayed presentation and orchiectomy, which is why the public-health message of immediate presentation is part of the long-term management. [11]
Complications & Pitfalls
Orchiectomy, the loss of the testis, is the dominant complication, and it is the direct consequence of delayed exploration. The salvage rate tracks the duration of torsion, and a boy who reaches theatre beyond the 6-hour window has a steadily worsening chance of leaving with his testis. Ramachandra and colleagues confirmed that the duration of symptoms before surgery is the strongest predictor of salvage at a tertiary paediatric centre, which is why the prevention of delay is the prevention of orchiectomy. [4]
Subfertility is the second key complication, and it affects even the salvaged testis. After torsion, the disruption of the blood-testis barrier can trigger antisperm antibody formation and a degree of testicular atrophy, and the contralateral testis can be affected through a sympathetic or immunological mechanism. Aggarwal and colleagues documented the long-term impact on semen parameters and gonadal function, which is why the follow-up of a salvaged torsion includes a later assessment of the fertility, particularly if the boy had an orchidectomy or a prolonged torsion. [7]
The classic pitfalls are diagnostic and temporal. The first is attributing the pain to a mimic, such as epididymitis or growing pains, on the basis of a single reassuring feature, when the only safe stance is that torsion is present until excluded by exploration. The second is delaying the operation for a scan in a high-probability boy, which converts the salvageable testis into the necrotic one. The third is the boy with abdominal pain whose scrotum is never examined, which is why the rule that any boy with unexplained lower abdominal pain must have a scrotal examination is load-bearing. [2]
A subtler pitfall is the falsely reassuring Doppler ultrasound. In the small prepubertal testis, in early or partial torsion, and in low-flow states, the scan can show residual flow and the diagnosis can be missed. The scan is interpreted in the context of the clinical probability, and a convincing picture with a normal scan still warrants exploration. McLaren emphasised that ultrasound is an adjunct and not a gatekeeper. [3]
Prognosis & Disposition
The prognosis of torsion is almost entirely a function of the time to detorsion, and the salvage rate is the single number that encapsulates it. A boy explored within 6 hours has a 90 to 100 percent chance of keeping his testis, and that chance falls to about 50 percent from 6 to 12 hours and to less than 20 percent from 12 to 24 hours. Sharp and colleagues set out the salvage gradient that governs the counselling of the boy and the family. [1]
Disposition is to a paediatric surgical or urological service for every boy with confirmed or suspected torsion, and the transfer to theatre is immediate for the high-probability case. The boy who has an orchidectomy is offered a prosthetic testis in adolescence for cosmesis, and the boy who has a salvaged testis is followed for atrophy and for fertility. The psychological impact of the diagnosis, the operation, and the possible loss of a testis is real in the adolescent, and it is addressed with honest, age-appropriate communication and the offer of counselling. [7]
The long-term outlook includes the fertility surveillance. A salvaged testis can undergo some atrophy, and the boy who had a prolonged torsion or an orchidectomy is offered a later semen analysis in adulthood, with referral to a fertility service if the parameters are abnormal. The contralateral fixation protects the other testis, and the boy is reassured that a single healthy testis is sufficient for normal hormonal function and usually for fertility, provided the semen parameters are preserved. [7]
Special Populations
The newborn with perinatal torsion is the population at the frontier of candour. The testis is usually infarcted at birth, the salvage rate is low, and the role of urgent exploration is chiefly to fix the contralateral testis and to prevent the catastrophic synchronous or metachronous bilateral torsion. The family is counselled honestly about the likely loss of the testis and the rationale for operating on the other side, and the option of a contralateral fixation versus observation is discussed with the paediatric urology team. [12]
The adolescent is the second population, and the one for whom the communication is most delicate. The boy is frightened, the diagnosis carries the threat of losing a testis and the anxiety about future fertility, and the consent must be honest, age-appropriate, and delivered with the family. The offer of a prosthetic testis in the boy who has an orchidectomy, the reassurance about hormonal function, and the plan for later fertility surveillance are all part of the adolescent-centred care. [7]
The Aboriginal and Torres Strait Islander boy and the boy from a remote setting is the third population. The later presentation, with a longer duration of torsion and a lower salvage rate, is more common where the distance to a surgical centre is greater, and the public-health message of immediate presentation is part of the prevention. The culturally appropriate communication, the engagement with the family, and the coordination with the retrieval service are the elements that move the boy to theatre inside the window. [2]
The boy with an undescended testis is the fourth population, and the one with the highest baseline risk. The torsion in a groin testis presents as an acute groin mass with an empty scrotum, the diagnosis is harder, and the management is urgent exploration. The episode reinforces the case for the elective surgical correction of the undescended testis, which is the long-term prevention of the torsion in this high-risk group. [11]
Evidence, Guidelines & Regional Differences
The evidence base for torsion has been reshaped by the standardised risk-stratification studies. The systematic review and meta-analysis by Qin and Qu confirmed the diagnostic performance of the TWIST score across the published cohorts, and the paediatric evaluation by Manohar and colleagues and the adult validation by Barbosa and colleagues extended its use across the age range. The score has moved the assessment of the acute scrotum from an impressionistic judgement to a reproducible, evidence-based probability. [5][9]
The imaging evidence has been consolidated by the appropriateness criteria. The 2024 ACR Appropriateness Criteria for the acute onset of scrotal pain reaffirmed colour Doppler ultrasound as the appropriate first-line imaging test for the equivocal presentation, while the systematic review by McLaren quantified its diagnostic performance and its limits, particularly the falsely reassuring scan in early or partial torsion. The shared message is that the scan informs the intermediate-risk boy and must never gatekeep the high-probability one. [10][3]
Qin and Qu 2022
J Urol meta-analysis
- Systematic review and meta-analysis of the TWIST score
- Confirmed the diagnostic performance across the cohorts
- Moved the acute scrotum to a reproducible probability
Ramachandra 2015
West J Emerg Med
- Tertiary paediatric centre salvage factors
- Duration of torsion as the dominant determinant of salvage
- Quantified the cost of delay to imaging
Erlich 2022
J Pediatr Surg
- Perinatal torsion in clear-cut, controversial, and quiet scenarios
- Salvage is rare, role of surgery is contralateral protection
- Synchronous and metachronous bilateral torsion
Aggarwal 2022
Indian J Urol
- Long-term impact on semen parameters and gonadal function
- Antisperm antibodies and atrophy after torsion
- Fertility surveillance is part of the follow-up
The regional differences centre on the access to urgent surgical care and on the imaging pathway. In the high-resource settings, the near-immediate access to a surgical team and to Doppler ultrasound allows the rapid exploration of the high-probability boy and the timely imaging of the intermediate-risk one. In the lower-resource and remote settings, the longer time to theatre is the dominant driver of the lower salvage rate, which is why the retrieval pathways and the public-health message of immediate presentation are part of the regional management. The international consensus on the 6-hour window and on the low threshold for exploration applies across the settings. [2]
Exam Pearls
The four features of torsion for the short case
References
- [1]Sharp VJ, Kieran K, Arlen AM Testicular torsion: diagnosis, evaluation, and management. Am Fam Physician, 2013.PMID 24364548
- [2]Laher A, Ragavan S, Mehta P, et al Testicular Torsion in the Emergency Room: A Review of Detection and Management Strategies. Open Access Emerg Med, 2020.PMID 33116959
- [3]McLaren PSM A systematic review on the utility of ultrasonography in the diagnosis of testicular torsion in acute scrotum patients. Radiography (Lond), 2021.PMID 33451883
- [4]Ramachandra P, Palazzi KL, Holmes NM, et al Factors influencing rate of testicular salvage in acute testicular torsion at a tertiary pediatric center. West J Emerg Med, 2015.PMID 25671040
- [5]Qin KR, Qu LG Diagnosing with a TWIST: Systematic Review and Meta-Analysis of a Testicular Torsion Risk Score. J Urol, 2022.PMID 35238603
- [6]Barbosa JABA, de Freitas PFS, Carvalho SAD, et al Validation of the TWIST score for testicular torsion in adults. Int Urol Nephrol, 2021.PMID 32844355
- [7]Aggarwal D, Parmar K, Sharma AP, et al Long-term impact of testicular torsion and its salvage on semen parameters and gonadal function. Indian J Urol, 2022.PMID 35400863
- [8]Davis JE, Silverman M Scrotal emergencies. Emerg Med Clin North Am, 2011.PMID 21782069
- [9]Manohar CS, Gupta A, Keshavamurthy R, et al Evaluation of Testicular Workup for Ischemia and Suspected Torsion score in patients presenting with acute scrotum. Urol Ann, 2018.PMID 29416270
- [10]Expert Panel on Urological Imaging, Gerena M, Allen BC, et al ACR Appropriateness Criteria Acute Onset of Scrotal Pain-Without Trauma, Without Antecedent Mass: 2024 Update. J Am Coll Radiol, 2024.PMID 39488348
- [11]Mansbach JM, Forbes P, Peters C Testicular torsion and risk factors for orchiectomy. Arch Pediatr Adolesc Med, 2005.PMID 16330742
- [12]Erlich T, Ghazzaoui AE, Pokarowski M, et al Perinatal testicular torsion: The clear cut, the controversial, and the "quiet" scenarios. J Pediatr Surg, 2022.PMID 34753560