Paeds · nephrology-urology-fluids-and-electrolytes
Vesicoureteric reflux
Also known as Vesicoureteral reflux · VUR · Reflux nephropathy · Ureterovesical reflux · Primary vesicoureteric reflux
Fellowship guide to vesicoureteric reflux, the retrograde flow of urine from the bladder into the upper urinary tract that is the most common urological abnormality in children. Covers the International Reflux Study grading system from grade I to grade V, the pathophysiology of an incompetent ureterovesical junction with a short intramural tunnel, the role of the micturating cystourethrogram in diagnosis, the natural history of spontaneous resolution skewed toward low-grade reflux, the RIVUR trial evidence on antimicrobial prophylaxis, the management ladder from observation through continuous antibiotic prophylaxis to endoscopic injection and ureteric reimplantation, the critical modifier of bladder and bowel dysfunction, and the long-term risk of reflux nephropathy with renal scarring, hypertension, and chronic kidney disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who presents with a febrile urinary tract infection in infancy, or an infant found to have hydronephrosis on the antenatal scan, leads the clinician to the diagnosis of vesicoureteric reflux. The condition is the retrograde flow of urine from the bladder up into the ureter and the renal pelvis, and it is the most common urological abnormality in children, found in approximately 1 to 2 percent of all children and in up to 30 to 40 percent of those who present with a febrile urinary tract infection. The abnormality lies at the ureterovesical junction, where the ureter enters the bladder through a short or absent intramural tunnel that fails to act as a one-way valve. [8]
The clinical significance of reflux is twofold. First, it allows infected bladder urine to ascend to the kidney, which converts a lower urinary tract infection into pyelonephritis and causes renal scarring. Second, the refluxing urine creates a residual volume that predisposes to recurrent infection. The scarred kidney carries a life-long risk of hypertension, proteinuria, and chronic kidney disease, and in pregnancy it increases the risk of pre-eclampsia. This cascade from a febrile infection to permanent renal damage is the entire rationale for the investigation, grading, and management of reflux. [8]
Primary reflux is the congenital form, in which the ureterovesical junction is structurally abnormal from a short intramural tunnel, and it is the form that resolves spontaneously as the child grows. Secondary reflux arises from a high-pressure or abnormal bladder, such as posterior urethral valves, a neurogenic bladder, or bladder and bowel dysfunction, and it persists until the underlying cause is treated. The distinction is critical, because primary reflux is managed on the grade and the infection history, while secondary reflux is managed by treating the bladder. [3]
Classification
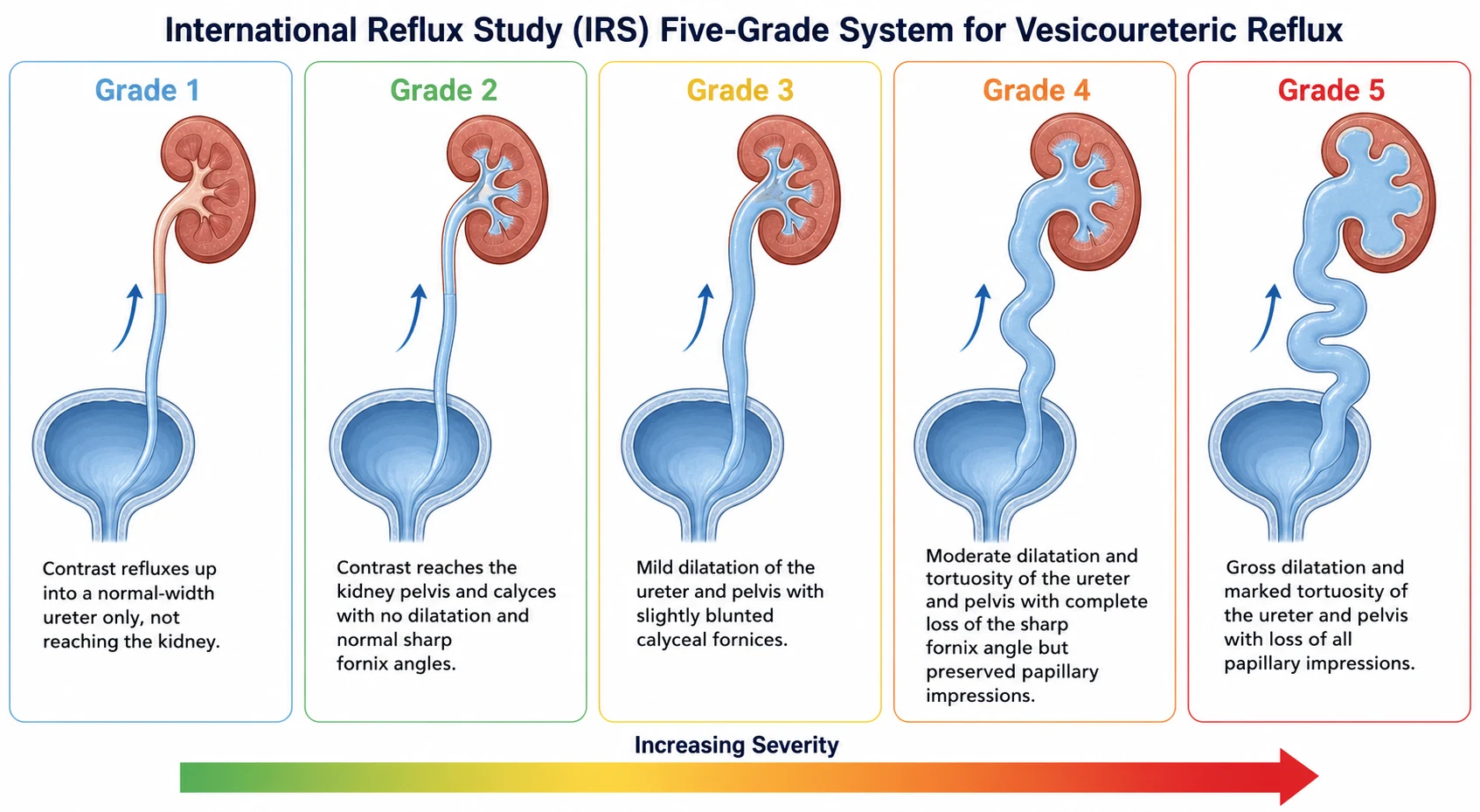
The classification of vesicoureteric reflux rests on the International Reflux Study system, published by Lebowitz and colleagues in 1985, which grades the reflux on the micturating cystourethrogram from grade I to grade V based on the extent of the reflux, the degree of dilatation, and the morphology of the calyces. The grading is the single most testable element of the topic, because the grade predicts the likelihood of spontaneous resolution, the risk of renal scarring, and the threshold for surgical intervention. [1]
Grade I reflux is the reflux of contrast into a non-dilated ureter only, without reaching the renal pelvis. Grade II reflux reaches the renal pelvis and the calyces, but there is no dilatation of the ureter, the pelvis, or the calyces, and the sharp angles of the calyceal fornices are preserved. Grade III reflux shows mild to moderate dilatation of the ureter with mild tortuosity, mild dilatation of the renal pelvis, and blunting of the sharp angles of the calyceal fornices. [1]
Grade IV reflux shows moderate dilatation and increased tortuosity of the ureter, moderate dilatation of the renal pelvis and calyces, and complete obliteration of the sharp angle of the fornices, though the papillary impressions of the calyces remain visible. Grade V reflux is the most severe, with gross dilatation and marked tortuosity of the ureter, massive dilatation of the renal pelvis and calyces, and loss of all papillary impressions. The distinction between grade IV and grade V rests on whether the papillary impressions are still visible, which is a favourite detail in written examinations. [1]
Low grade I to II
- Grade I: reflux into ureter only
- Grade II: reflux to pelvis and calyces, no dilatation
- High spontaneous resolution rate
- Low risk of renal scarring
Intermediate grade III
- Mild dilatation and tortuosity of ureter
- Mild blunting of calyceal fornices
- Moderate resolution rate over years
- Intermediate scarring risk
High grade IV to V
- Grade IV: moderate dilatation, fornices obliterated, papillary impressions preserved
- Grade V: gross dilatation, papillary impressions lost
- Low spontaneous resolution rate
- High risk of renal scarring and surgical referral
Epidemiology & Risk Factors
Vesicoureteric reflux is the most common urological abnormality in children. The overall prevalence in healthy children is approximately 1 to 2 percent, but the prevalence rises steeply in children who present with a urinary tract infection. Approximately 30 to 40 percent of children with a febrile urinary tract infection have reflux on a micturating cystourethrogram, and the proportion is even higher in infants under one year of age. This inverse relationship between age and the likelihood of reflux underpins the recommendation to investigate infants and young children after a febrile infection. [8]
The most important risk factors for reflux are young age, a history of febrile urinary tract infection, and a family history. Reflux is more common in infants because the intramural tunnel is shorter relative to the ureteric diameter in early life and lengthens as the bladder grows. Girls are more likely to be diagnosed after infancy because they have a higher rate of urinary tract infection, while boys are more likely to be diagnosed antenatally or in the neonatal period, often with higher-grade reflux associated with posterior urethral valves or a duplex system. [11]
Sibling reflux is a well-recognised phenomenon. Approximately 30 to 45 percent of siblings of a child with reflux also have reflux, which supports a genetic component with autosomal dominant inheritance in some families. The sibling screening strategy is selective rather than universal, targeting siblings with a history of urinary tract infection, antenatal hydronephrosis, or symptoms of bladder and bowel dysfunction, because the majority of asymptomatic siblings with low-grade reflux do not require intervention. [3]
Aboriginal and Torres Strait Islander children and other Indigenous populations carry a higher burden of recurrent urinary tract infection and renal scarring, which compounds the risk from reflux. Socioeconomic disadvantage, delayed presentation, and reduced access to imaging and specialist services all contribute to a later diagnosis and a higher rate of established reflux nephropathy at the time of presentation. [6]
Pathophysiology
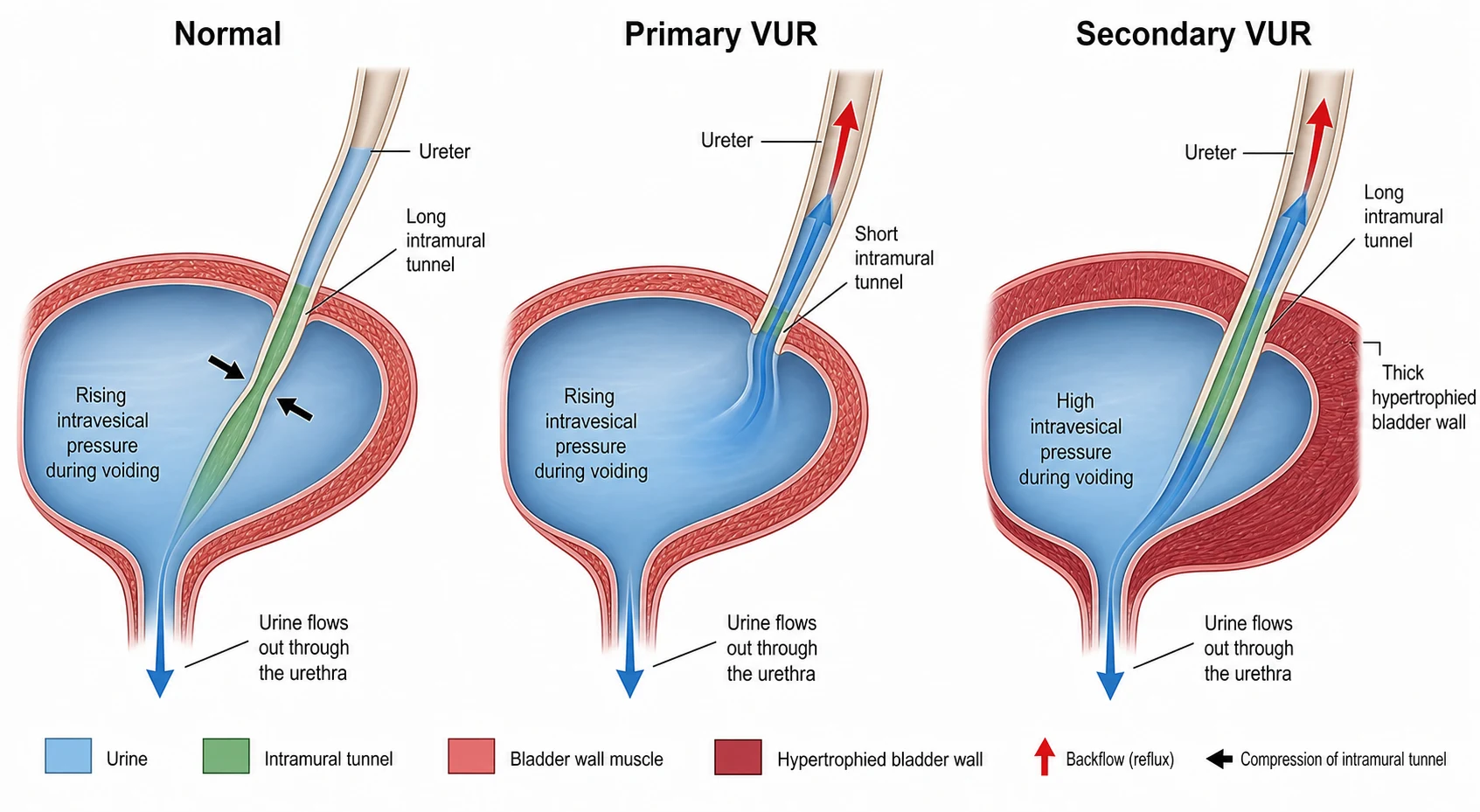
The normal ureterovesical junction functions as a passive flap-valve. The ureter enters the bladder wall obliquely and travels a distance through the detrusor muscle, the intramural tunnel, before opening into the bladder lumen. When the bladder contracts and the intravesical pressure rises during voiding, the rising pressure compresses the intramural tunnel against the bladder wall, collapsing it and preventing urine from flowing backwards. The ratio of the tunnel length to the ureteric diameter is critical, and a normal ratio of approximately 5 to 1 ensures a competent valve. [3]
Primary reflux arises when the intramural tunnel is abnormally short, the ureteric orifice is more lateral and cranial in the bladder, or the detrusor support of the tunnel is deficient. The tunnel fails to compress during voiding, and the urine flows retrogradely into the ureter. The reflux is a developmental anomaly of the ureteric bud origin, in which the bud arises too cranially on the Wolffian duct, producing an orifice that is displaced laterally and a tunnel that is short. As the child grows, the bladder enlarges, the tunnel lengthens, and the reflux resolves in many children, which is the anatomical basis for the natural history of spontaneous resolution. [11]
Secondary reflux arises from high intravesical pressure or a bladder that empties poorly. In posterior urethral valves, a neurogenic bladder, or bladder and bowel dysfunction, the bladder generates pressures during filling and voiding that overwhelm even a normal ureterovesical junction. The reflux does not resolve until the bladder problem is corrected, which is why the management of secondary reflux is entirely directed at the bladder rather than at the reflux itself. [5]
The consequence of reflux is the delivery of infected bladder urine to the renal parenchyma. When bacteria ascend through the refluxing ureter to the renal pelvis and enter the renal tubules, they trigger an inflammatory response that destroys the renal tubules and the surrounding interstitium. The resulting scar is permanent, and it is visible on a DMSA scan as a photon-deficient area of cortical loss. The scarring is uneven, concentrating at the renal poles where the papillae are of the compound type that allows intrarenal reflux. Each episode of pyelonephritis adds to the scar burden, and the cumulative loss of functioning nephrons drives the long-term risk of hypertension and chronic kidney disease. [8]
Clinical Presentation
The presentation of vesicoureteric reflux falls into three patterns that correspond to the three clinical pathways. The first and most common is the child who presents with a febrile urinary tract infection. The American Urological Association guideline and the European Association of Urology guideline both recommend that the child with a febrile urinary tract infection, particularly an infant under two years, is evaluated for reflux, because the probability of finding reflux is 30 to 40 percent. The infection is usually caused by Escherichia coli, it presents with fever, irritability, poor feeding, and sometimes vomiting, and the reflux is discovered on the subsequent micturating cystourethrogram. [3]
The second pattern is the child detected antenatally. The mid-trimester anomaly scan shows hydronephrosis, and the postnatal ultrasound confirms the dilation. Farhat and colleagues showed that a significant proportion of neonates with antenatal hydronephrosis have reflux on the postnatal micturating cystourethrogram, and these infants are often diagnosed before they ever have a urinary tract infection. The antenatally detected group tends to have higher-grade reflux, a higher proportion of boys, and a higher rate of associated congenital anomalies of the kidney and urinary tract. [11]
The three pathways to a diagnosis of vesicoureteric reflux
Febrile urinary tract infection in an infant or young child leading to micturating cystourethrogram
Antenatal hydronephrosis on mid-trimester scan with postnatal confirmation and micturating cystourethrogram
Sibling screening of a child with known reflux who has a history of urinary tract infection or symptoms
Incidental finding on imaging performed for another indication
Evaluation of bladder and bowel dysfunction with persistent daytime wetting and recurrent infection
The third pattern is the child with bladder and bowel dysfunction. This child presents with daytime urinary symptoms, including urgency, frequency, incontinence, and infrequent voiding, often accompanied by constipation and encopresis. The bladder and bowel dysfunction drives the reflux and the recurrent infection, and it is the most common reason for failure of conservative management. Elder and Diaz showed that bladder and bowel dysfunction is present in over 40 percent of children with reflux, and it reduces the spontaneous resolution rate and increases the risk of breakthrough infection. [5]
Differential Diagnosis
The primary differential is between reflux and other causes of urinary tract dilation on the ultrasound. Ureteropelvic junction obstruction produces hydronephrosis without ureteric dilation, and it is distinguished from reflux by the MAG3 renogram, which shows a delayed drainage from the renal pelvis without the reflux. A megaureter, whether obstructive or non-obstructive, produces a dilated ureter on the ultrasound, and the micturating cystourethrogram distinguishes a refluxing megaureter from an obstructive one. A duplex collecting system may be associated with reflux to the lower moiety and obstruction of the upper moiety, and it is identified on the ultrasound and confirmed on the micturating cystourethrogram. [3]
The second distinction is between reflux and the transient hydronephrosis of the newborn. Many neonates have mild hydronephrosis on the antenatal scan that resolves in the first months of life without any underlying pathology. The postnatal ultrasound at 5 to 7 days, followed by the micturating cystourethrogram if the hydronephrosis persists, separates the transient dilation from the reflux or obstruction. The threshold for the micturating cystourethrogram is a persistent renal pelvic diameter above 7 millimetres or a ureteric dilation on the postnatal ultrasound. [11]
VUR
- Retrograde flow on micturating cystourethrogram
- Dilated ureter and pelvis during voiding
- Diagnosed on MCUG, graded I to V
- Short intramural tunnel is the mechanism
PUJ obstruction
- Hydronephrosis without ureteric dilation
- Delayed drainage on MAG3 renogram
- No reflux on micturating cystourethrogram
- Congenital narrowing at the pelviureteric junction
Megaureter
- Dilated ureter on ultrasound
- Obstructive or non-obstructive variants
- Distinguished from reflux on MCUG
- May coexist with high-grade reflux
The third distinction is between reflux nephropathy and other causes of renal scarring. Renal scarring on the DMSA scan may result from reflux nephropathy, but it may also result from dysplasia associated with congenital anomalies of the kidney and urinary tract, from a previous episode of acute pyelonephritis without reflux, or from ischaemic injury. The distinction matters because reflux nephropathy is preventable with the control of infection, while congenital dysplasia is fixed and cannot be modified by the management of the reflux. [8]
Clinical & Bedside Assessment
The bedside assessment of a child with suspected or confirmed reflux answers three questions: is there an active infection, is there bladder and bowel dysfunction, and is there evidence of renal compromise. The child with a febrile urinary tract infection is assessed for the signs of pyelonephritis, including fever, flank pain, vomiting, and dehydration, and the urine is sent for culture before the antibiotics are started. The blood pressure is measured at every visit, because hypertension is the earliest sign of reflux nephropathy and it may be the first indication that the reflux has caused renal damage. [8]
The assessment of bladder and bowel dysfunction is the most often omitted element of the clinical assessment, and it is the key to the management. The clinician asks about the voiding pattern, including the frequency, the urgency, the stream, the daytime wetting, and the presence of constipation or encopresis. A voiding and bowel diary, kept for 3 days, is the most informative tool, and it reveals the infrequent voider, the child with urgency and incontinence, and the constipated child. The presence of bladder and bowel dysfunction changes the management, because it must be treated before any surgical intervention is considered, and its correction alone may resolve the reflux and the recurrent infection. [5]
The history should include the number and the characteristics of the previous urinary tract infections, including whether they were febrile, the causative organism, and the response to treatment. A history of breakthrough infection on prophylaxis is a red flag that may prompt surgical intervention. The family history of reflux in siblings or parents guides the screening of the family, and the developmental history screens for a neurogenic bladder from an occult spinal cord lesion, particularly in a child with a dimple, a hairy patch, or a foot deformity. [3]
Investigations
The investigation pathway for reflux is sequential, and each test answers a specific question. The renal ultrasound is the first test in any child with a urinary tract infection or an antenatal finding, and it screens for hydronephrosis, ureteric dilation, a duplex system, and renal size and morphology. The ultrasound does not diagnose reflux, because a child with low-grade reflux may have a normal ultrasound, and a child with high-grade reflux may have a dilated collecting system. The ultrasound identifies the child who needs the micturating cystourethrogram and the child with a renal anomaly that needs further investigation. [9]
The micturating cystourethrogram, also called the voiding cystourethrogram, is the gold standard for the diagnosis and grading of reflux. A catheter is passed into the bladder, the bladder is filled with iodinated contrast, and images are taken during filling and voiding. The reflux is graded from I to V using the International Reflux Study system, and the test also identifies posterior urethral valves, a diverticulum, and a duplex system. The test involves radiation exposure and carries a small risk of procedure-related urinary tract infection, so the child receives antibiotic prophylaxis around the procedure, and it is reserved for children with a high pre-test probability of reflux. [3]
The DMSA scan, or dimercaptosuccinic acid scintigraphy, is a static cortical scan that detects renal scarring, dysplasia, and the split renal function. It is performed 4 to 6 months after an acute pyelonephritis to allow the acute inflammatory changes to resolve, because an acute scan may overestimate the permanent scarring. The DMSA is the test that defines reflux nephropathy, and it is essential for the long-term surveillance of the child with high-grade reflux or recurrent infection. The MAG3 renogram is a dynamic scan that assesses the drainage and the split function, and it is used to distinguish reflux from ureteropelvic junction obstruction and to monitor the drainage after surgical correction. [8]
The selective imaging strategy has replaced the universal imaging of every child with a first febrile urinary tract infection. The American Academy of Pediatrics, in its 2011 clinical practice guideline on the initial urinary tract infection in febrile infants, recommended a renal and bladder ultrasound after the first febrile infection but reserved the micturating cystourethrogram for children with an abnormal ultrasound, an atypical organism, or a recurrent febrile infection. Mattoo and colleagues reviewed the contemporary management, noting that the selective approach reduces the number of invasive tests without missing the high-grade reflux that drives the scarring, and the strategy is endorsed by the European guidelines. [9]
Management — Resuscitation
The immediate priority in a child who presents with a febrile urinary tract infection and suspected reflux is the treatment of the infection, not the reflux. The child with pyelonephritis is treated with antibiotics, either orally with a cephalosporin or amoxicillin-clavulanate, or intravenously in the infant under 3 months, the toxic child, or the child who cannot tolerate oral medication. The urine culture is sent before the antibiotics are started, and the antibiotic is adjusted to the sensitivities when they become available. The reflux is investigated after the infection has been treated, because the micturating cystourethrogram is performed when the child is well. [6]
The child with breakthrough febrile infection on prophylaxis, or the child with high-grade reflux and a first febrile infection, is at the highest risk of progressive scarring. The resuscitation phase includes the prompt treatment of the infection, the assessment for dehydration and electrolyte disturbance, and the measurement of the renal function and the blood pressure. The child with bilateral high-grade reflux, a solitary functioning kidney, or established reflux nephropathy is managed jointly with the paediatric nephrologist from the outset, because the risk of acute kidney injury from severe pyelonephritis is real. [8]
Continuous antibiotic prophylaxis for vesicoureteric reflux
Dose
Trimethoprim 2 mg per kg at night
Continuous antibiotic prophylaxis is the cornerstone of the medical management of reflux, and its evidence base was transformed by the RIVUR trial. The Randomized Intervention for Children with Vesicoureteral Reflux trial, published in the New England Journal of Medicine in 2014 by the RIVUR Trial Investigators led by Hoberman, randomised 607 children aged 2 to 71 months with grade I to IV reflux after one or two febrile urinary tract infections to trimethoprim-sulfamethoxazole prophylaxis or placebo. The trial found that prophylaxis halved the rate of recurrent febrile or symptomatic urinary tract infection, from 23 percent in the placebo group to 13 percent in the prophylaxis group, but it did not reduce the rate of new renal scarring at two years, which was approximately 11 percent in both groups. [2]
The RIVUR trial also found a significant increase in trimethoprim-sulfamethoxazole-resistant Escherichia coli in the prophylaxis group, which is a trade-off that must be discussed with the family. Mathews and Mattoo reviewed the implications, noting that the subgroup of children who benefit most from prophylaxis are those with reflux and bladder and bowel dysfunction, who have the highest baseline risk of recurrent infection. Zhao and colleagues subsequently showed that the children with the highest baseline risk derive the greatest absolute benefit from prophylaxis, which supports a targeted rather than a universal approach. [4]
Management — Definitive & Stepwise
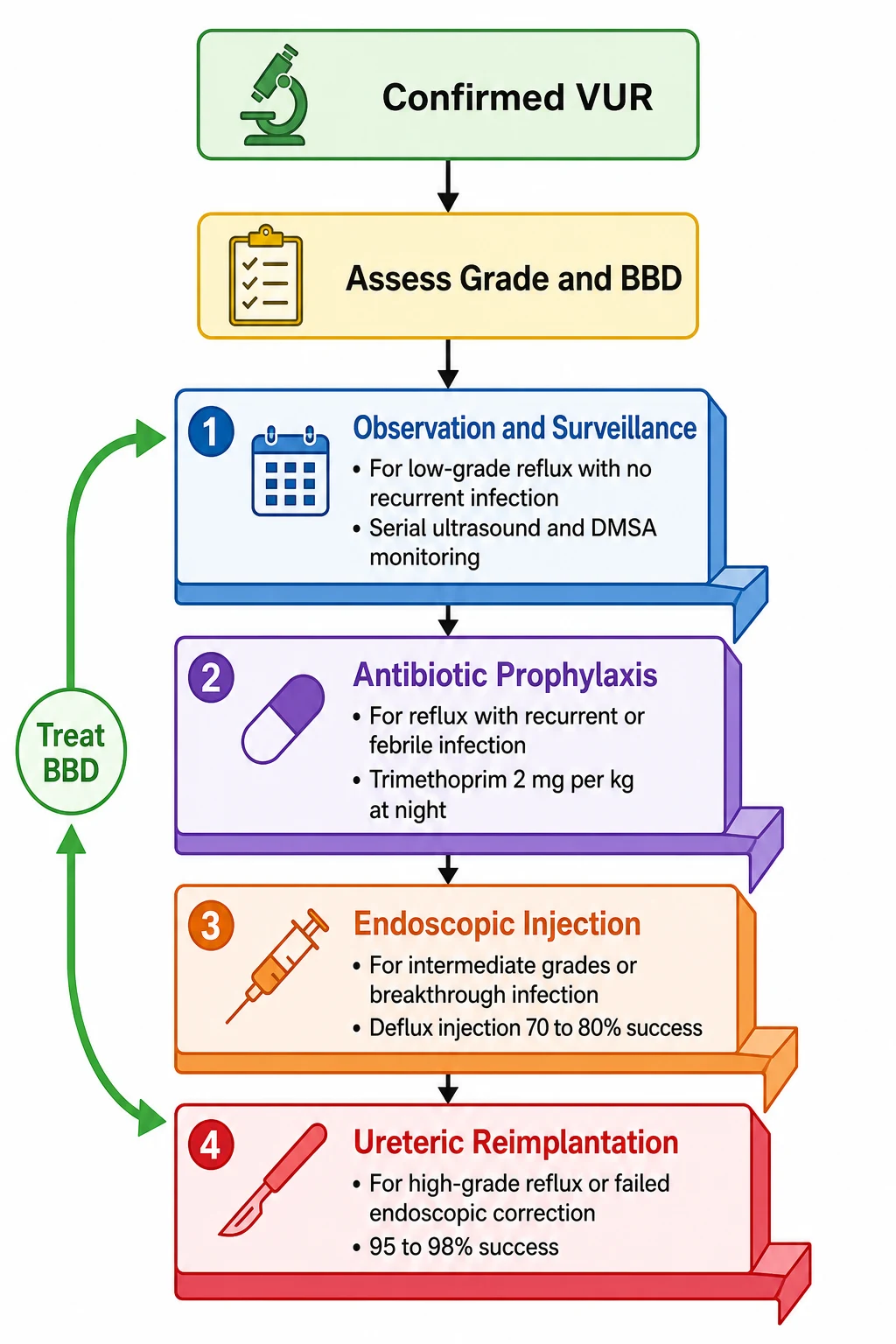
[3]The definitive management follows a ladder that escalates with the grade, the infection history, and the presence of bladder and bowel dysfunction. The overarching principles are to prevent renal scarring by controlling the infection, to treat the bladder and bowel dysfunction, and to reserve surgical correction for the child in whom the medical management has failed or the reflux is unlikely to resolve. The American Urological Association guideline, summarised by Peters and colleagues, provides the framework, and the decisions are made jointly by the paediatrician, the nephrologist, and the urologist. [3]
The first step is observation and surveillance for the child with low-grade reflux, no recurrent infection, and no renal scarring. This child is monitored with periodic ultrasound and DMSA scanning, the blood pressure is checked at every visit, and the family is counselled on the signs of urinary tract infection and the need to seek prompt treatment. The low-grade reflux has a high rate of spontaneous resolution, and the surveillance is the safety net that detects the child who develops breakthrough infection or progressive scarring. [12]
The second step is continuous antibiotic prophylaxis for the child with reflux and a febrile infection, or for the child with high-grade reflux that is unlikely to resolve. The first-line agent is trimethoprim at 2 mg per kg at night, with nitrofurantoin at 1 mg per kg at night or trimethoprim-sulfamethoxazole as alternatives. The prophylaxis is continued until the reflux resolves, is corrected, or the child is old enough that the risk of new scarring is low. The family is counselled on the RIVUR trial evidence, the reduced recurrence rate, the absent reduction in scarring, and the risk of resistant organisms. [2]
Nitrofurantoin prophylaxis for reflux
Dose
1 mg per kg at night
The third step is endoscopic injection for the child with intermediate-grade reflux, breakthrough infection on prophylaxis, or a family preference for a minimally invasive option. The injection of dextranomer and hyaluronic acid copolymer, known by the trade name Deflux, is placed beneath the ureteric orifice to augment the intramural tunnel and create a competent valve. Kirsch and colleagues reviewed the 20-year experience, showing success rates of approximately 70 to 80 percent per injection for grades I to III and lower rates for grades IV and V, with the option of repeat injection for the failures. The endoscopic approach is less invasive than open surgery but less durable, and it may require multiple procedures. [7]
The fourth step is ureteric reimplantation for the child with high-grade reflux, failed endoscopic correction, or a preference for a single definitive procedure. The open surgical reimplantation, using the Cohen transtrigonal or the Politano-Leadbetter technique, creates a new and longer intramural tunnel, and it has a success rate of approximately 95 to 98 percent, making it the most durable option. The robotic and laparoscopic approaches are increasingly used in specialist centres with comparable success rates and shorter hospital stays. The surgery is reserved for the child in whom the medical and the endoscopic management have failed or in whom the high-grade reflux is unlikely to resolve. [3]
Specific Subtypes & Scenarios
The child with antenatally detected reflux represents a distinct clinical scenario. These infants are diagnosed before they ever have a urinary tract infection, and they tend to have higher-grade reflux, a higher proportion of boys, and a higher rate of associated congenital anomalies. Farhat and colleagues showed that the neonatal reflux associated with antenatal hydronephrosis has a high rate of spontaneous resolution in the low grades, but the high grades have a lower resolution rate and a higher risk of renal dysplasia that is present from birth. The management of the antenatally detected group is prophylactic antibiotics from diagnosis, with the micturating cystourethrogram confirming the grade and the DMSA assessing the baseline cortical function. [11]
3 Ds for the management options in vesicoureteric reflux
The child with reflux and bladder and bowel dysfunction is the scenario that most often defeats the conservative management. Elder and Diaz showed that bladder and bowel dysfunction is present in over 40 percent of children with reflux, and it reduces the spontaneous resolution rate by half, doubles the risk of breakthrough infection, and halves the success rate of endoscopic injection. The management of this child begins with the treatment of the bladder and bowel dysfunction, using timed voiding every 2 to 3 hours, treatment of constipation with laxatives and a high-fibre diet, and anticholinergic medication or biofeedback for the overactive bladder. The reflux often improves or resolves once the bladder function is normalised, and the surgical correction is more likely to succeed when the bladder is compliant. [5]
The adolescent girl with reflux nephropathy is a critical scenario because of the reproductive implications. Connolly and colleagues documented the natural history of reflux in girls after age 5 years, showing that the reflux may persist into adolescence and adulthood, and the scarred kidney carries a risk of hypertension and pre-eclampsia in pregnancy. The surveillance includes the blood pressure monitoring and the urinalysis for proteinuria, and the young woman is counselled on the need for urinary tract infection prevention during pregnancy. The transition to adult nephrology care is planned in adolescence, because the reflux nephropathy does not resolve and the risk of chronic kidney disease persists. [12]
[6]Complications & Pitfalls
The complications of vesicoureteric reflux are the consequences of the recurrent pyelonephritis and the resulting renal scarring. Renal scarring is the central complication, and it is the direct cause of the long-term morbidity. Mattoo and Mohammad showed that the scarring risk is proportional to the number of febrile infections and the grade of the reflux, and that the scarring is permanent and progressive. Each episode of pyelonephritis adds to the scar burden, and the child with high-grade reflux and recurrent infection may accumulate enough scarring to reduce the renal function and drive the progression to chronic kidney disease. [8]
Hypertension is the most common long-term complication of reflux nephropathy, and it arises from the activation of the renin-angiotensin system in the scarred kidney. The hypertension is often asymptomatic in childhood and is detected only by the routine blood pressure monitoring, which is why every child with reflux has the blood pressure measured at every visit. The proteinuria and the declining renal function are the later signs of the hyperfiltration injury in the remaining nephrons, and they signal the progression to chronic kidney disease. [8]
The classic pitfalls are diagnostic and therapeutic. Failing to investigate a febrile urinary tract infection in an infant, on the assumption that the fever has another cause, delays the diagnosis of high-grade reflux and allows preventable scarring. Over-treating low-grade reflux that is destined to resolve, with unnecessary prophylaxis or premature surgery, exposes the child to the risks of the intervention without a corresponding benefit. Failing to identify and treat bladder and bowel dysfunction, in a child with reflux and recurrent infection, is the single most common reason for the failure of the conservative management, because the dysfunctional bladder drives both the reflux and the infection. [5]
Prognosis & Disposition
The prognosis of vesicoureteric reflux depends on the grade, the infection history, the presence of renal scarring at diagnosis, and the presence of bladder and bowel dysfunction. The low-grade reflux, grades I to III, has a high rate of spontaneous resolution, with up to 80 percent of grade I to II and approximately 50 percent of grade III resolving over 5 years. The high-grade reflux, grades IV to V, has a much lower resolution rate, and these children are more likely to require surgical correction. The child with scarring at diagnosis, or with breakthrough infection on prophylaxis, has a worse prognosis and a higher risk of long-term renal damage. [12]
The long-term data for reflux nephropathy show that the scarring is the determinant of the outcome. Mattoo and Mohammad reviewed the relationship between reflux and renal scarring, showing that the children who develop scarring are those who carry the risk of hypertension, proteinuria, and chronic kidney disease into adulthood. The child without scarring, regardless of the reflux grade, has a prognosis that is essentially normal, provided the infection is controlled and the reflux either resolves or is corrected. [8]
Disposition is to a paediatric nephrology and urology service for every child with confirmed reflux, with the intensity of the follow-up tailored to the grade, the infection history, and the scarring. The child with low-grade reflux and no scarring may be followed by the general paediatrician with the annual blood pressure and the periodic ultrasound and DMSA. The child with high-grade reflux, breakthrough infection, or established scarring is followed by the multidisciplinary team, with the consideration of surgical correction and the intensive surveillance for hypertension and declining renal function. The transition to adult nephrology care is planned in adolescence for every child with scarring, because the reflux nephropathy persists and the risk of chronic kidney disease continues into adulthood. [12]
Special Populations
The sibling of a child with reflux is the most common special population, because of the familial clustering of the condition. Approximately 30 to 45 percent of siblings of a child with reflux also have reflux, which supports a genetic component. The sibling screening strategy is selective, targeting siblings with a history of urinary tract infection, antenatal hydronephrosis, or symptoms of bladder and bowel dysfunction. The universal screening of all asymptomatic siblings is not recommended, because the majority of siblings with low-grade reflux do not require intervention and the micturating cystourethrogram is invasive. [3]
Children with bladder and bowel dysfunction form a distinct population that requires a combined urological and behavioural approach. Elder and Diaz showed that the bladder and bowel dysfunction is the strongest modifier of the reflux outcome, and the child with both conditions has a lower resolution rate, a higher breakthrough rate, and a lower surgical success rate. The management prioritises the treatment of the bladder and bowel dysfunction, using timed voiding, constipation management, anticholinergic medication, and biofeedback, before any surgical correction of the reflux is considered. [5]
Aboriginal and Torres Strait Islander children and children from lower-resource settings present a different challenge. The higher background burden of recurrent urinary tract infection and renal scarring, the reduced access to imaging and specialist services, and the later presentation all compound the risk. The emphasis in these settings is on the early detection through the prompt investigation of febrile infection, the culturally appropriate counselling of the family, and the close coordination between the primary care, the paediatric, and the specialist services. [6]
The young adult transitioning from paediatric to adult care is the final special population. The reflux may persist or may have been corrected, but the reflux nephropathy does not resolve, and the risk of hypertension and chronic kidney disease continues into adulthood. The transition plan addresses the blood pressure monitoring, the renal function surveillance, the reproductive counselling including the risk of pre-eclampsia in pregnancy, and the coordination between the paediatric and the adult nephrology services. [12]
Evidence, Guidelines & Regional Differences
The evidence base for vesicoureteric reflux has been transformed by the RIVUR trial. The Randomized Intervention for Children with Vesicoureteral Reflux trial, published by the RIVUR Trial Investigators led by Hoberman in 2014, was the definitive randomised controlled trial of antimicrobial prophylaxis, and it established that prophylaxis halves the rate of recurrent urinary tract infection but does not reduce the rate of new renal scarring. The trial also showed a significant increase in resistant organisms in the prophylaxis group, which is a trade-off that must be discussed with the family. [2]
The guideline framework is provided by the American Urological Association, summarised by Peters and colleagues in 2010, and the European Association of Urology and European Society for Paediatric Urology guidelines, reviewed by Stein and colleagues. The AUA guideline provides the risk-stratified management ladder, the indications for prophylaxis and surgery, and the framework for the surveillance. The EAU and ESPU guidelines integrate the reflux management into the broader urinary tract infection pathway, with the selective imaging strategy and the emphasis on the prevention of scarring. [6]
Lebowitz 1985
- International Reflux Study grading system I to V
- The single most testable element of the topic
- Published in Pediatric Radiology
RIVUR 2014
- NEJM randomised trial of prophylaxis
- Halved recurrence, no reduction in scarring
- Increased resistant organisms on prophylaxis
Peters 2010
- AUA guideline on primary reflux management
- Risk-stratified management ladder
- Framework for prophylaxis and surgery
Elder 2013
- Bladder and bowel dysfunction as modifier
- Present in over 40 percent of children
- Halves resolution rate and doubles breakthrough
The regional differences centre on the imaging strategy and the threshold for prophylaxis. The American Academy of Pediatrics, in its 2011 guideline on the initial urinary tract infection in febrile infants, recommended a selective imaging approach that reserves the micturating cystourethrogram for children with an abnormal ultrasound, an atypical organism, or a recurrent infection. The European guidelines, reviewed by Stein and colleagues, adopt a similar selective approach, with the additional emphasis on the micturating cystourethrogram in infants under 6 months with an atypical or recurrent infection, as endorsed by the NICE guideline in the United Kingdom. The international consensus is that the universal imaging of every child with a first febrile infection is no longer justified, because it identifies much low-grade reflux that would resolve without intervention. [9]
Exam Pearls
I-ING for the reflux grades on the micturating cystourethrogram
References
- [1]Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Mobius TE International system of radiographic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr Radiol, 1985.PMID 3975102
- [2]RIVUR Trial Investigators, Hoberman A, Greenfield SP, Mattoo TK, et al Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med, 2014.PMID 24795142
- [3]Peters CA, Skoog SJ, Arant BS Jr, et al Summary of the AUA Guideline on Management of Primary Vesicoureteral Reflux in Children. J Urol, 2010.PMID 20650499
- [4]Mathews R, Mattoo TK The role of antimicrobial prophylaxis in the management of children with vesicoureteral reflux--the RIVUR study outcomes. Adv Chronic Kidney Dis, 2015.PMID 26088078
- [5]Elder JS, Diaz M Vesicoureteral reflux--the role of bladder and bowel dysfunction. Nat Rev Urol, 2013.PMID 24126731
- [6]Stein R, Dogan HS, Hoebeke P, et al Urinary tract infections in children: EAU/ESPU guidelines. Eur Urol, 2015.PMID 25477258
- [7]Kirsch AJ, Cooper CS, Lackgren G Non-Animal Stabilized Hyaluronic Acid/Dextranomer Gel (NASHA/Dx, Deflux) for Endoscopic Treatment of Vesicoureteral Reflux: What Have We Learned Over the Last 20 Years? Urology, 2021.PMID 34411597
- [8]Mattoo TK, Mohammad D Primary Vesicoureteral Reflux and Renal Scarring. Pediatr Clin North Am, 2022.PMID 36880925
- [9]Mattoo TK, Shaikh N, Nelson CP Contemporary Management of Urinary Tract Infection in Children. Pediatrics, 2021.PMID 33479164
- [10]Zhao B, Ivanova A, Shaikh N, et al Antimicrobial prophylaxis for vesicoureteral reflux: which subgroups of children benefit the most? Pediatr Nephrol, 2024.PMID 38244067
- [11]Farhat W, McLorie G, Geary D, et al The natural history of neonatal vesicoureteral reflux associated with antenatal hydronephrosis. J Urol, 2000.PMID 10958740
- [12]Connolly LP, Zurakowski D, Connolly SA, et al Natural history of vesicoureteral reflux in girls after age 5 years. J Urol, 2001.PMID 11696785