Paeds · nephrology-urology-fluids-and-electrolytes
Vulvovaginal and common prepubertal gynaecological disorders
Also known as Prepubertal vulvovaginitis · Nonspecific vulvovaginitis · Labial adhesions · Labial fusion · Lichen sclerosus · Paediatric lichen sclerosus · Vulvar lichen sclerosus · Prepubertal vaginal discharge · Irritant vulvitis
Fellowship guide to the three common prepubertal gynaecological disorders: vulvovaginitis, labial adhesions, and lichen sclerosus. Covers the hypo-oestrogenic prepubertal vulval environment with its thin mucosa and neutral pH that predispose to nonspecific irritant vulvovaginitis as the commonest complaint, the fusion of the labia minora in labial adhesions that peaks between three months and six years and usually resolves at puberty, and the porcelain-white sclerotic plaques of lichen sclerosus treated with an ultra-potent topical corticosteroid, together with the red flags of vaginal foreign body, sexual abuse, and prepubertal bleeding that must never be missed.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Three conditions dominate the prepubertal vulval complaint in the general paediatric clinic, and all three share a common starting point in the hypo-oestrogenic state of the child before puberty. The first is vulvovaginitis, an inflammation of the vulva and the lower vagina that is the single commonest gynaecological complaint of prepubertal girls. [1] The second is labial adhesions, also called labial fusion, in which the labia minora fuse together along the midline to varying degrees, sometimes closing the vaginal introitus almost completely. [5] The third is lichen sclerosus, a chronic inflammatory skin condition that produces porcelain-white, atrophic, pruritic plaques on the vulval and perianal skin in the classic figure-of-eight distribution. [8]
The reason these conditions cluster in the prepubertal years is that the vulval skin and the vaginal mucosa of the young girl lack the protective maturation that oestrogen brings at puberty. [1] Before puberty the vulval epithelium is thin, the vaginal pH is neutral rather than acidic, and the lactobacilli that dominate the adult vaginal flora are absent, so the tissue is vulnerable to irritation, to fusion under mild inflammation, and to the immune-mediated changes of lichen sclerosus. Puberty reverses much of this vulnerability, which is why labial adhesions resolve spontaneously as oestrogen rises and why vulvovaginitis becomes far less common. [2]
The clinical task at the bedside is to recognise each condition, to treat it along the evidence-based pathway, and to identify the red flags that change a simple problem into an emergency or a child protection concern. A persistent or bloody discharge raises the question of a vaginal foreign body. A specific sexually transmitted organism on a vaginal swab raises the question of sexual abuse. Unexplained prepubertal bleeding demands evaluation for trauma, foreign body, precocious puberty, or a tumour. [12]
Classification
The three conditions are classified along their own clinical axes, and the classification guides the management. Nonspecific vulvovaginitis accounts for the majority of cases and is managed with hygiene alone, while specific vulvovaginitis is caused by an identified pathogen and needs targeted treatment. Labial adhesions are graded by the degree of fusion from partial to complete, and lichen sclerosus is staged by the severity of the skin change from early atrophy through established sclerosis to chronic scarring. [1] [5]
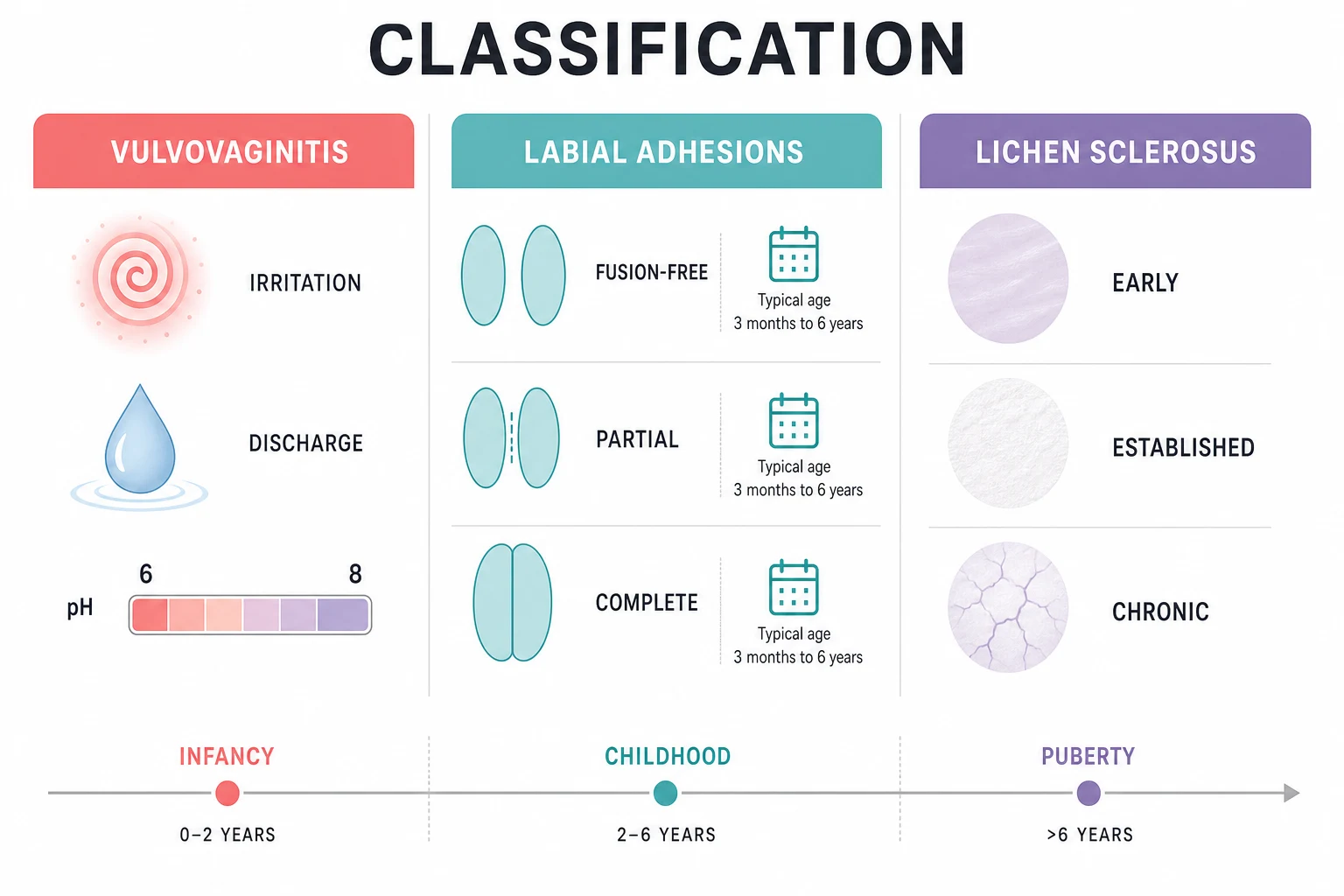
Vulvovaginitis is divided first into nonspecific and specific forms. Nonspecific, or irritant, vulvovaginitis accounts for roughly 50 to 75 percent of cases and has no single pathogen identified on culture; it reflects the vulnerability of the thin prepubertal mucosa to poor hygiene, tight clothing, bubble baths, and faecal contamination. [1] Specific vulvovaginitis is caused by an identifiable organism, most commonly Group A beta-haemolytic Streptococcus, but also Haemophilus influenzae, Streptococcus pneumoniae, Shigella, and, in the appropriate context, Neisseria gonorrhoeae or Chlamydia trachomatis. [3] Candida is rare in the healthy prepubertal girl because the neutral pH does not favour its growth, and its presence should prompt consideration of recent antibiotic use, diabetes, or immunocompromise. [2]
Labial adhesions are classified by the extent of the fusion along the midline. In partial adhesions the labia minora are fused over part of their length, leaving a visible or functional introitus, and the child is usually asymptomatic. In complete adhesions the fusion extends across the full length of the labia minora, closing the introitus and sometimes leaving only a small pinhole opening through which urine escapes. The severe form can cause urinary pooling, dribbling, recurrent urinary tract infections, or visible distension of the fused tissue on voiding. [5]
Lichen sclerosus is classified by the stage of the skin change, which ranges from early inflammation through established sclerosis to chronic scarring. Early disease shows erythema and mild atrophy that may be mistaken for vulvovaginitis or eczema. Established disease shows the classic porcelain-white, wrinkled, atrophic plaques with purpura and fissures in the figure-of-eight distribution around the vulva and the anus. Chronic disease shows resorption of the labia minora, scarring that narrows the introitus, and hyperkeratotic areas that may simulate lichen simplex chronicus from chronic scratching. [9]
Epidemiology & Risk Factors
Vulvovaginitis is the commonest gynaecological complaint in prepubertal girls and accounts for the great majority of paediatric gynaecology referrals in this age group. [1] The peak incidence is between the ages of two and seven years, the years when the child is toilet-training, wiping imperfectly, and exposed to irritants at day care and school. Risk factors include poor perineal hygiene, front-to-back wiping not yet mastered, tight or synthetic clothing, bubble baths and scented soaps, pinworm infestation, and the anatomical proximity of the anus to the vagina in the young child. [4]
Vulvovaginitis
- Commonest prepubertal gynaecological complaint
- Peak age 2 to 7 years
- Nonspecific irritant form dominates
- Hygiene measures are first-line
Labial adhesions
- Peak incidence 3 months to 6 years
- Hypo-oestrogenic origin
- Most are asymptomatic
- Resolve spontaneously at puberty
Lichen sclerosus
- Chronic inflammatory dermatosis
- Figure-of-eight distribution
- Intense pruritus is the hallmark
- Ultra-potent topical steroid first-line
Labial adhesions have an estimated prevalence of 0.6 to 3 percent in prepubertal girls, and the peak incidence falls between three months and six years of age. [5] The condition is rare in the neonatal period, when maternal oestrogens are still present, and rare after puberty, when endogenous oestrogen thins the adhesions. Norris and colleagues documented a high rate of spontaneous resolution, confirming that the natural history favours conservatism. [7] Risk factors include recurrent vulvovaginitis, which inflames the labial edges and promotes fusion, and any condition that causes chronic vulval irritation.
Lichen sclerosus is less common than the other two conditions but is an important cause of chronic vulval symptoms in girls. It accounts for 10 to 15 percent of all lichen sclerosus cases, the majority being postmenopausal women, and the prepubertal form presents most often between four and seven years of age. [8] The risk of progression to squamous cell carcinoma is well documented in adults but is very low in children, and the main long-term concerns in the paediatric patient are scarring, recurrence, and the persistence of symptoms into adult life in a proportion of cases. [9]
Pathophysiology
The unifying pathophysiology for all three conditions is the hypo-oestrogenic state of the prepubertal vulva and vagina, which leaves the tissue thin, vulnerable, and chemically unprotected. [1] Before puberty the vaginal epithelium is only a few cell layers thick, in contrast to the thick stratified squamous epithelium of the adult. The vaginal pH is neutral, between 6 and 8, rather than the acidic 3.8 to 4.5 of the adult, because the prepubertal girl lacks the glycogen-rich epithelium that lactobacilli ferment into lactic acid. Without this acidic barrier, the vagina is susceptible to colonisation by faecal and skin organisms that would not survive in the adult environment. [2]
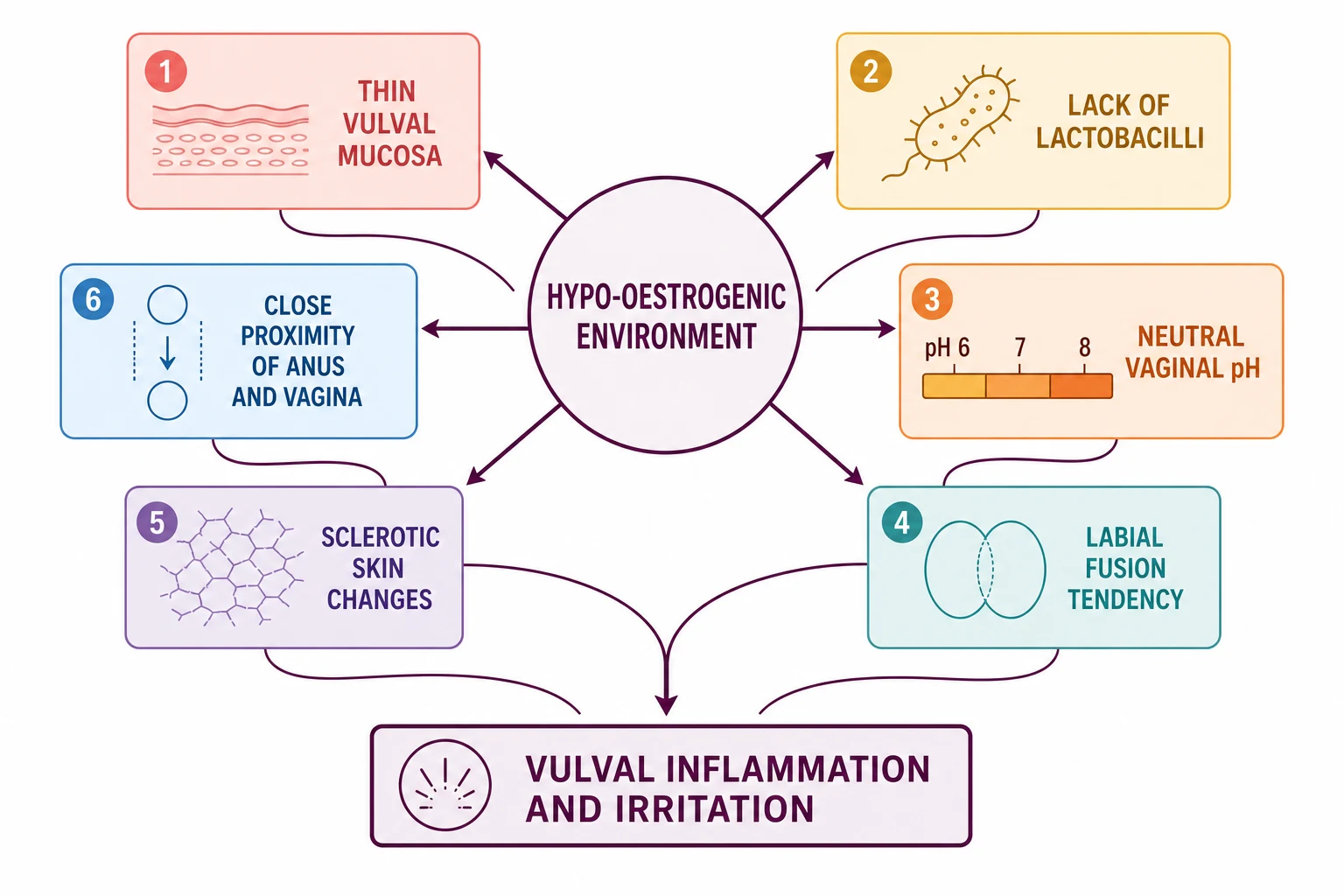
In nonspecific vulvovaginitis the thin mucosa is irritated by contact with urine, faeces, soap, and tight clothing, and the inflammation follows. In specific vulvovaginitis a pathogen gains entry through the same compromised barrier, and the neutral pH allows organisms such as Group A Streptococcus and Shigella to proliferate. [3] The anatomical proximity of the anus and the vagina in the young child means that faecal organisms reach the vulva easily, and poor wiping technique, which is normal at the developmental stage of two to four years, drives the recurrent cycle of contamination and inflammation. [4]
Labial adhesions form when the thin, inflamed edges of the labia minora lie in apposition and the irritated skin fuses along the midline. [5] The hypo-oestrogenic state is central: the low oestrogen level leaves the vulval epithelium thin and easily denuded, and any minor irritation from vulvovaginitis, scratching, or friction causes the raw edges to stick together. The fusion is not scarring in the mature sense but a thin membrane of apposed epithelium that oestrogen softens and dissolves, which is why both topical estrogen and the endogenous oestrogen of puberty are effective treatments. [6]
Lichen sclerosus is a chronic inflammatory dermatosis of unknown cause in which the upper dermis develops a band of lymphocytic inflammation beneath an atrophic epidermis, producing the characteristic sclerosis, collagen homogenisation, and loss of the rete ridges. [10] The result is the porcelain-white, wrinkled, fragile skin that bruises and tears with minimal trauma, producing the purpura and fissures that bring the child to medical attention. An autoimmune mechanism is suspected, given the association with other autoimmune conditions, and genetic and environmental triggers have been proposed. The disease is not caused by sexual abuse, but its bruising and scarring appearance can mimic abuse and demands careful assessment. [8]
Clinical Presentation
Vulvovaginitis presents with vulval redness, discomfort, itching, and a vaginal discharge that the parent has noticed on the underwear or the toilet paper. [1] The child may rub or scratch, may complain of pain on urination from the urine stinging the inflamed vulva, and may resist washing or wiping because of the soreness. The discharge in nonspecific vulvovaginitis is typically mild, greyish-yellow, and malodorous, while the discharge in specific vulvovaginitis may be purulent or bloody depending on the organism. Group A Streptococcus often produces a brisk, painful, erythematous vulvitis, while Shigella classically produces a bloody discharge. [3]
Labial adhesions are often discovered incidentally by the parent during bathing or nappy changing, or by the clinician on a routine examination, because the great majority are asymptomatic. [5] When symptoms occur they relate to the mechanical effect of the fused labia on the urinary stream. The parent may report that the child dribbles after voiding, that the urine stream is deflected upward or sprays, or that the child has had recurrent urinary tract infections from urinary pooling behind the adhesions. The examination finding is a flat, smooth, greyish membrane across the vulva where the labia minora have fused, with the clitoris visible above and the fused line running posteriorly from it. [7]
Lichen sclerosus presents with intense vulval itching, soreness, and sometimes bleeding or dysuria from skin fissures. [8] The parent may notice white patches on the vulva, and the child may have constipation from voluntary stool withholding because defecation is painful from perianal fissures. The examination shows the classic figure-of-eight distribution of porcelain-white, atrophic, wrinkled plaques around the vulva and the anus, with purpura, telangiectasia, and fissures in the active phase. The clitoris and labia minora may be resorbed or obscured by oedema in the acute presentation, and chronic scarring may narrow the introitus. [9]
Differential Diagnosis
The differential diagnosis of a vulval complaint in a prepubertal girl is broad, and the task is to separate the three common conditions from the rarer causes that need a different pathway. [1] Vulvovaginitis must be distinguished from a vaginal foreign body, which produces a persistent or bloody discharge, and from pinworm infestation, which causes nocturnal perianal itching. Labial adhesions must be distinguished from an imperforate hymen or a vaginal atresia, both congenital conditions that present differently, with a closed introitus from birth rather than an acquired fusion. [5]
Lichen sclerosus must be distinguished from vulval vitiligo, which is depigmented but not atrophic or pruritic, and from atopic or contact dermatitis, which is erythematous and itchy but lacks the porcelain-white sclerosis. [10] Sexual abuse produces bruising, laceration, and scarring that can closely mimic the purpura and fissures of lichen sclerosus, and the two conditions can coexist, so the assessment of any child with vulval signs must include a careful history and a child protection evaluation when the findings or the history are inconsistent. [8]
Prepubertal vaginal bleeding is the symptom that most demands a systematic differential. The causes range from the benign and common, such as vulvovaginitis, a foreign body, and urethral prolapse, to the serious and rare, such as a sarcoma botryoides of the vagina, a tumour of the ovary, or precocious puberty with oestrogen withdrawal bleeding. [12] Any girl with unexplained vaginal bleeding needs a careful examination under anaesthesia, imaging, and hormone measurements to find the cause, and the assumption should be that a cause exists and will be found rather than dismissed as unimportant. [12]
Clinical & Bedside Assessment
The examination of the prepubertal girl with a vulval complaint demands a gentle, unhurried approach and a trusted chaperone, usually the parent, positioned to reassure the child throughout. [1] The child is examined in the frog-leg position on the lap of the parent or on the couch, and the labia are gently separated to inspect the vulva, the introitus, and the hymenal rim. A speculum is never used in the prepubertal child in the outpatient setting. If a vaginal swab is needed, it is taken from the lower vagina or the introital area with a small-caliber swab moistened with saline, and the sample is sent for culture. [4]
For vulvovaginitis the examination documents the degree of erythema, the character and colour of any discharge, and the presence of skin excoriation from scratching. [1] A vaginal swab is sent for culture to identify a specific pathogen, and a sticky-tape test for pinworm ova is performed if nocturnal itching is the dominant symptom. The perianal skin is examined for the thread-like adult worms of Enterobius vermicularis, which are visible at night when the child is asleep. Growth parameters, the general examination, and the urinalysis are reviewed to exclude diabetes, immunocompromise, and a urinary tract infection as contributing factors. [4]
The vulvovaginitis assessment — what to check
For labial adhesions the examination documents the extent of the fusion, the size of the remaining opening, and any signs of urinary obstruction such as a distended bladder or dribbling. [5] The adhesion is inspected for the thin, grey, avascular membrane that distinguishes it from congenital obstruction, and the urethral meatus is sought above the fusion line. The degree of fusion guides the management: a partial, asymptomatic adhesion is observed, while a complete adhesion with urinary symptoms is treated with topical estrogen or, rarely, manual separation. [7]
For lichen sclerosus the examination documents the extent, the distribution, and the severity of the skin change. [8] The figure-of-eight pattern around the vulva and the anus is sought, and the active signs of purpura, fissuring, and erosions are distinguished from the chronic signs of scarring, introital narrowing, and labial resorption. A photograph is taken for baseline comparison and for medico-legal documentation. If the diagnosis is uncertain, a punch biopsy of the affected skin under local or general anaesthesia confirms the histology. [10]
Investigations
Nonspecific vulvovaginitis is a clinical diagnosis, and the first investigation is the introital swab sent for bacterial culture to identify or exclude a specific pathogen. [1] If the culture is negative, the diagnosis is nonspecific vulvovaginitis and no further investigation is needed in the first instance. If a pathogen is identified, the treatment is targeted to that organism. Group A Streptococcus is treated with oral penicillin or amoxicillin, Shigella with an appropriate oral antibiotic guided by sensitivities, and pinworm with a single dose of mebendazole repeated after two weeks. [4]
The persistent or bloody discharge that does not respond to treatment is the indication for vaginoscopy under anaesthesia to exclude a foreign body. [12] Imaging is not reliable for finding a radiolucent foreign body such as toilet paper, so direct visualisation is the standard. If a specific sexually transmitted organism such as Neisseria gonorrhoeae is identified, the child protection pathway is activated and full STI screening with nucleic acid amplification testing is performed under the appropriate protocol. [12]
Labial adhesions are a clinical diagnosis and need no investigation in the typical case. [5] A urinalysis is performed if the child has had urinary symptoms or recurrent infections, and a renal tract ultrasound is reserved for the child with a documented urinary tract infection to exclude an underlying anomaly. The distinction from an imperforate hymen or vaginal atresia is made on the history and the examination: the congenital conditions present from birth, while the adhesion is acquired and develops over months. [7]
Lichen sclerosus is a clinical diagnosis in the great majority of cases, based on the characteristic figure-of-eight distribution and the porcelain-white atrophic appearance. [8] A skin biopsy is reserved for cases where the diagnosis is uncertain, where the condition does not respond to an appropriate course of ultra-potent topical corticosteroid, or where there is concern about a premalignant or malignant change. The biopsy shows the characteristic epidermal atrophy, basement membrane thickening, upper dermal collagen homogenisation, and a band of lymphocytic inflammation beneath. [10]
Management — Resuscitation
None of the three conditions is typically a resuscitation emergency, but three presentations demand immediate action and must be recognised without delay. The first is the severe labial adhesions causing acute urinary obstruction, in which the child is unable to void or is retaining urine with a palpable distended bladder. [5] The management is the application of topical estrogen to the adhesion to soften it over several days, combined with bladder decompression if needed, and manual separation under anaesthesia is reserved for the case that does not resolve or that recurs despite treatment. [6]
The second is the vaginal foreign body producing a persistent or bloody discharge, which demands prompt examination under anaesthesia with vaginoscopy to find and remove the object. [12] Retained toilet paper is the commonest finding, and the discharge typically resolves once it is removed. The examination also allows the exclusion of a tumour such as a sarcoma botryoides, which presents as a grape-like mass at the vaginal introitus and is a rhabdomyosarcoma requiring urgent oncology referral. [12]
The foreign-body workup for persistent discharge
Recognise
Examine under anaesthesia
Exclude a tumour
Follow up
The third is the identification of a sexually transmitted organism on a vaginal swab, which activates the child protection pathway. The finding of Neisseria gonorrhoeae or Chlamydia trachomatis in a prepubertal girl is, in the absence of a clearly explained non-sexal mode of transmission, strong evidence of sexual abuse and mandates immediate referral to the child protection team and a formal forensic examination under the local protocol. [12] The urgency is to collect the forensic samples within the window in which they are recoverable and to ensure the safety of the child.
Management — Definitive & Stepwise
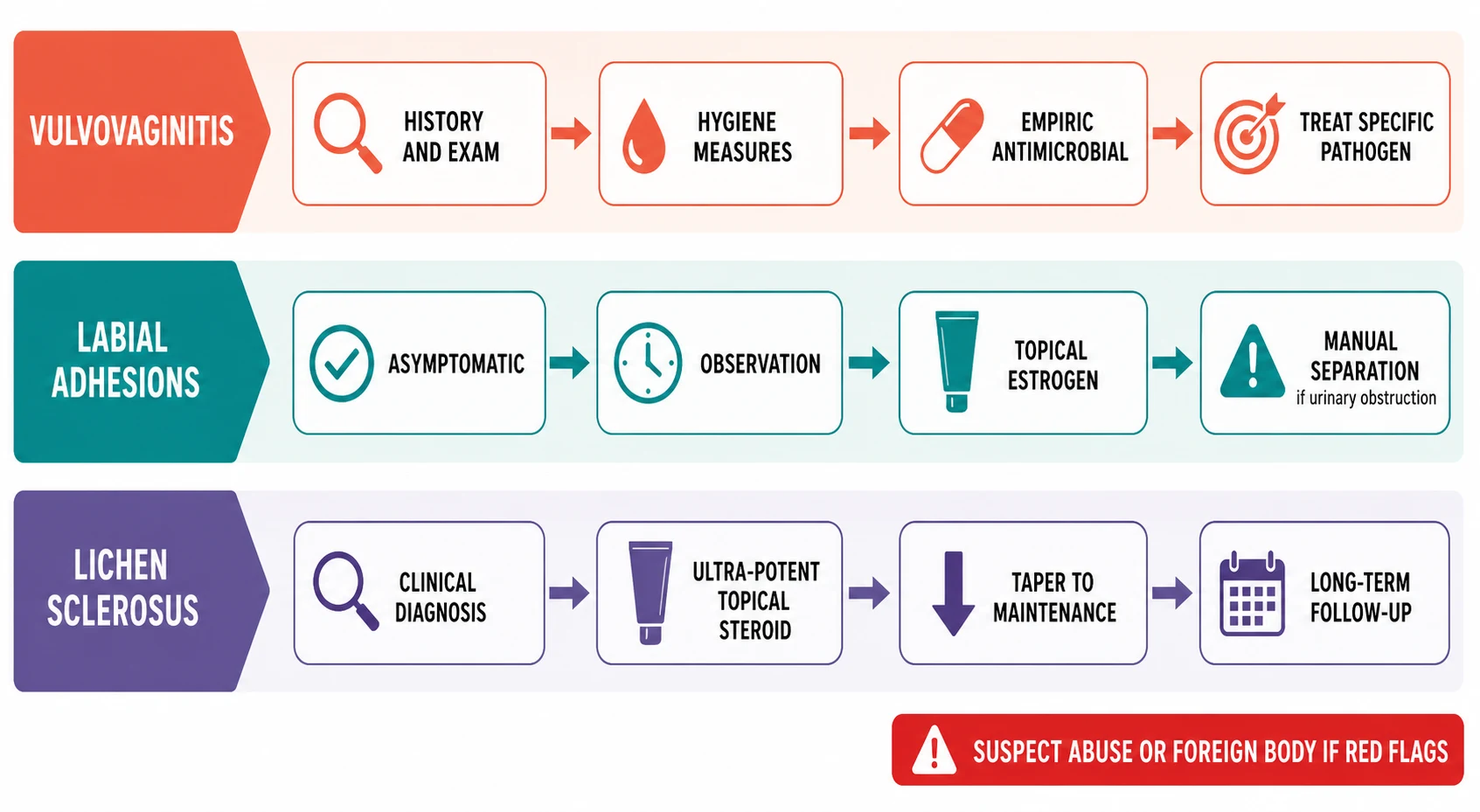
The definitive management of nonspecific vulvovaginitis begins with hygiene measures, which alone resolve the great majority of cases. [1] The family is advised to use plain water or a mild, non-soap cleanser for washing, to avoid bubble baths and scented products, to dress the child in loose cotton underwear, to teach front-to-back wiping, and to avoid tight-fitting clothing such as tights and leggings. [4] A short course of a barrier cream or a mild topical anti-inflammatory may soothe the acute inflammation. If a specific pathogen is identified on the introital swab, a targeted oral antibiotic is added, guided by the culture sensitivities. [3]
The management of labial adhesions is conservative and graduated, reflecting the high rate of spontaneous resolution and the benign natural history. [5] Asymptomatic partial adhesions are observed and the family is reassured that the fusion will almost certainly resolve at puberty. Symptomatic adhesions, or those causing urinary symptoms, are treated with a course of topical estrogen cream applied daily to the fusion line for two to six weeks, which softens the adhesion and allows the labia to separate. [6] Manual separation under anaesthesia is reserved for the rare case of urinary obstruction that does not respond to estrogen, and recurrence is common, so the family is warned and the child is followed. [7]
The management of lichen sclerosus is an ultra-potent topical corticosteroid, which is the first-line and evidence-based treatment at every age. [8] The standard regimen is clobetasol propionate 0.05% ointment applied to the affected skin once daily, typically for four to eight weeks for the induction of remission, followed by a tapering maintenance regimen of once or twice weekly for several months. [11] The family is counselled that the condition is chronic and relapsing, that the symptoms and signs may take weeks to improve, and that long-term follow-up is essential to detect recurrence, scarring, and the very rare progression to squamous cell carcinoma in adult life. [9]
The management of pinworm-related vulvovaginitis is a single dose of mebendazole repeated after two weeks to break the autoinfection cycle, combined with the hygiene measures for all family members. [4] The management of a confirmed vaginal foreign body is removal under anaesthesia followed by a short course of antibiotic cream if secondary infection is present, and the discharge resolves promptly. The management of sexual abuse, when identified, is the child protection pathway, and the medical treatment of the vulval condition is delivered alongside the safeguarding plan. [12]
Specific Subtypes & Scenarios
Group A streptococcal vulvovaginitis is the commonest specific form and presents with an acute, painful, bright-red vulvitis and a serosanguineous or purulent discharge. [3] The organism is the same Group A beta-haemolytic Streptococcus that causes pharyngitis and skin infection, and the child may have a concurrent upper respiratory or skin infection. The treatment is a 10-day course of oral penicillin or amoxicillin, and the response is usually rapid. The diagnosis is confirmed on the introital swab culture, and the family is reassured that the condition is not sexually transmitted. [4]
Shigella vulvovaginitis is notable for its bloody discharge, which can cause significant alarm, and for its association with gastrointestinal symptoms. [3] The organism reaches the vulva by faecal contamination, and the child may have a recent or concurrent diarrhoeal illness. The treatment is an oral antibiotic guided by the culture sensitivities, as Shigella resistance patterns vary by region. The bloody discharge is sometimes the presenting feature, and the finding should prompt a swab and a search for other causes of bleeding, including a foreign body, if the culture is negative. [12]
Nonspecific versus specific vulvovaginitis
The recurrent labial adhesion is the scenario that tests the clinician's patience and the family's confidence in conservative management. [7] Adhesions recur in up to 20 percent of girls after successful separation, whether by estrogen or by manual means, because the underlying hypo-oestrogenic environment persists until puberty. The management of recurrence is a repeated course of topical estrogen, and the family is counselled that the adhesions will eventually resolve with the endogenous oestrogen of puberty. Manual separation is repeated only if urinary obstruction recurs. [6]
Lichen sclerosus in the girl with concurrent bruising or behavioural concerns is the scenario that demands the most careful assessment. The skin changes of lichen sclerosus, with their purpura, fissures, and scarring, can mimic the signs of sexual abuse, and the two conditions may coexist. [8] The assessment includes a detailed history, a full skin examination to document the distribution, and, when the history or the findings are inconsistent with the explanation offered, a referral to the child protection team for a formal evaluation. The key message is that lichen sclerosus is not caused by abuse but that its presence does not exclude coexisting abuse, and the two diagnoses require separate, parallel assessments. [9]
Complications & Pitfalls
The complications of untreated or recurrent vulvovaginitis are discomfort, social embarrassment, and the rare progression to labial adhesions from chronic inflammation of the labial edges. [5] The principal pitfall is the misdiagnosis of a specific pathogen as nonspecific vulvovaginitis, which denies the child a targeted antibiotic and prolongs the symptoms. Another pitfall is the treatment of presumed Candida with an antifungal cream when the underlying cause is irritant or bacterial, which wastes time and may worsen the irritation. The third pitfall is the failure to investigate a persistent or bloody discharge for a foreign body, which leaves the cause unaddressed. [12]
The complications of labial adhesions relate to the mechanical effect on the urinary tract. Urinary pooling behind the adhesions predisposes to recurrent urinary tract infections, and in the severe case the child may develop acute urinary obstruction requiring emergency decompression. [5] The principal pitfall is the unnecessary manual separation of an asymptomatic adhesion that would have resolved spontaneously, which causes pain, risks further scarring, and has a high recurrence rate. The second pitfall is the failure to recognise urinary obstruction as the cause of the child's symptoms, which delays the appropriate treatment. [7]
The complications of lichen sclerosus are scarring with narrowing of the introitus, resorption of the labia minora, and the development of chronic pain or sexual dysfunction in adult life. [9] The very rare progression to squamous cell carcinoma is a long-term risk that is well documented in adults and that demands lifelong surveillance of the affected skin, although the absolute risk in the paediatric patient is very low. [10] The principal pitfall is the under-treatment with a weak topical steroid that fails to control the inflammation, which allows the sclerosis and scarring to progress. [11]
The misattribution of lichen sclerosus to sexual abuse, or the converse failure to recognise coexisting abuse, is the pitfall with the most serious consequences for the child and the family. [8] The skin changes of lichen sclerosus are not diagnostic of abuse, and a confident diagnosis of the dermatosis on clinical and histological grounds should reassure the clinician and the family, but a thorough child protection assessment is mandatory when the history or the findings are inconsistent. [9]
Prognosis & Disposition
The prognosis of nonspecific vulvovaginitis is excellent, and the great majority of cases resolve with hygiene measures alone or with a short course of targeted antibiotic for a specific pathogen. [1] Recurrence is common in the toddler and preschool years because the predisposing hygiene and the hypo-oestrogenic environment persist, so the family is counselled to maintain the hygiene measures and to return if the symptoms recur. The condition resolves definitively at puberty when the endogenous oestrogen thickens the mucosa and restores the acidic, lactobacillus-dominated flora. [2]
The prognosis of labial adhesions is excellent, with a high rate of spontaneous resolution at puberty and a good response to topical estrogen in the symptomatic case. [5] Recurrence is common before puberty, occurring in up to 20 percent of girls after successful separation, and the family is counselled to expect this and to return for repeat treatment if urinary symptoms recur. [7] The adhesions leave no long-term sequelae once they have resolved, and the vulval anatomy returns to normal. The disposition is back to the general paediatrician with a clear plan and a defined point of urological review. [6]
The prognosis of lichen sclerosus is more guarded, because the condition is chronic and relapsing and because a proportion of girls continue to have symptoms into adult life. [9] The prepubertal improvement that was once expected with the oestrogen surge of puberty is now recognised to be less reliable than previously thought, and up to two-thirds of girls may have persistent signs or symptoms into adulthood. [10] The long-term follow-up is essential to detect recurrence, to monitor for scarring, and to maintain the ultra-potent corticosteroid regimen at the lowest effective maintenance dose. [11]
The disposition for the girl with a confirmed foreign body, a specific sexually transmitted organism, or suspected abuse is to the child protection and forensic pathway, and the medical treatment of the vulval condition is integrated into the safeguarding plan. [12] The prognosis for the vulval condition itself is good once the cause is addressed, but the psychological and safeguarding outcome depends on the comprehensive assessment and the support provided to the child and the family through the child protection process.
Special Populations
The girl who has experienced sexual abuse is the population in whom the vulval complaint carries the highest stakes. The coexistence of vulvovaginitis, lichen sclerosus, or labial adhesions with the signs of abuse demands a coordinated evaluation by paediatrics, child protection, and forensic services, and the family needs careful and sensitive communication. [8] The principles of care are a full forensic examination under the appropriate protocol, the collection of samples within the window of recoverability, the treatment of any identified infection, and the safeguarding plan that ensures the ongoing safety of the child. [12]
Aboriginal and Torres Strait Islander children and children from rural and remote areas may present late with chronic vulval symptoms when the access to primary care and specialist services is limited. [1] The emphasis in these populations is on opportunistic examination at every primary care contact, on culturally safe communication about genital examination, and on the coordination of outreach paediatric and dermatology services so that the condition is not neglected because of distance. Pinworm infestation is common in remote communities and is a treatable cause of vulvovaginitis that should not be overlooked. [4]
[5]The girl with an underlying dermatological or immunological condition, such as atopic dermatitis or an autoimmune disease, may present with a more severe or refractory vulval condition. [10] The lichen sclerosus that coexists with an autoimmune thyroiditis or vitiligo follows the pattern seen in adults, and the child with lichen sclerosus should be screened for the associated autoimmune conditions. The girl with developmental delay or disability may have difficulty communicating her symptoms, and the clinician must rely on behavioural changes and a careful examination to identify and treat the vulval condition. [8]
Evidence, Guidelines & Regional Differences
The management of vulvovaginitis rests on the clinical reviews by Romano and by Brander, both of which emphasise the nonspecific, hygiene-driven nature of the great majority of cases and the targeted antibiotic approach for the specific pathogens identified on culture. [1] [2] The microbiological study by Baka and colleagues characterised the organisms cultured from prepubertal girls with vulvovaginitis and confirmed that Group A Streptococcus and the respiratory and gastrointestinal pathogens dominate, while Candida is rare. [3] The NASPAG clinical recommendation by Zuckerman and Romano formalised the stepwise approach of hygiene first, swab second, and targeted antibiotic third. [4]
The management of labial adhesions rests on the NASPAG clinical recommendation by Bacon and colleagues, which set out the conservative approach of observation for asymptomatic adhesions and topical estrogen for symptomatic ones, with manual separation reserved for urinary obstruction. [5] The study by Kim and colleagues compared topical estrogen cream with observation and supported the estrogen approach for symptomatic adhesions, while the study by Norris and colleagues documented the high rate of spontaneous resolution that underpins the conservative strategy. [6] [7]
The management of lichen sclerosus rests on the NASPAG clinical recommendation by Bercaw-Pratt and colleagues, which established the ultra-potent topical corticosteroid as the first-line treatment in children. [8] The 2023 update by De Luca and colleagues reviewed the current evidence, and the EuroGuiderm guideline by Kirtschig and colleagues provided the 2024 treatment recommendations for lichen sclerosus across all age groups, including the paediatric patient. [9] [11] The earlier review by Fistarol and Itin remains a comprehensive reference for the diagnosis and treatment, including the histological features and the long-term outlook. [10]
Controversies remain in the long-term prognosis of paediatric lichen sclerosus, with earlier reports suggesting that the condition resolved at puberty and more recent studies showing that a significant proportion of girls have persistent disease into adulthood. [9] The role of the maintenance corticosteroid regimen, the frequency of follow-up, and the approach to the girl who does not respond to an appropriate course of ultra-potent corticosteroid are areas of evolving practice. The controversy around the association with sexual abuse is settled in principle: lichen sclerosus is not caused by abuse, but the two conditions can coexist, and each demands its own assessment. [8]
Exam Pearls
The three highest-yield facts in this topic are the hypo-oestrogenic prepubertal environment, the hygiene-first approach to vulvovaginitis, and the ultra-potent corticosteroid for lichen sclerosus. [1] [8] The thin vulval mucosa, the neutral pH, and the absence of lactobacilli explain why vulvovaginitis is so common before puberty and why Candida is rare. The first-line treatment of nonspecific vulvovaginitis is hygiene measures, not antibiotics and not antifungals, and a targeted antibiotic is added only when a specific pathogen is cultured. [4]
The labial adhesion is the commonest examination trap in the opposite direction: the family and the inexperienced clinician see the fused labia and think of a congenital anomaly, but the adhesion is acquired and benign and resolves at puberty. [5] The management is observation for the asymptomatic case and topical estrogen for the symptomatic case, with manual separation reserved for urinary obstruction. Recurrence is common and expected, and the family is counselled accordingly. [6]
The red flags carry the most marks in the higher-order stems. A persistent or bloody discharge is a foreign body until proven otherwise and demands vaginoscopy. [12] A specific sexually transmitted organism on a vaginal swab activates the child protection pathway. The porcelain-white figure-of-eight plaques of lichen sclerosus are treated with an ultra-potent topical corticosteroid, and the condition is chronic and relapsing with long-term follow-up. [9] The bruising of lichen sclerosus mimics abuse, but the dermatosis is not caused by abuse, and the two conditions require separate assessments. [8]
References
- [1]Romano ME Prepubertal Vulvovaginitis. Clin Obstet Gynecol, 2020.PMID 32282354
- [2]Brander EPA, McQuillan SK Prepubertal vulvovaginitis. CMAJ, 2018.PMID 29970369
- [3]Baka S, Demeridou S, Kaparos G Microbiological findings in prepubertal and pubertal girls with vulvovaginitis. Eur J Pediatr, 2022.PMID 36163515
- [4]Zuckerman A, Romano M Clinical Recommendation: Vulvovaginitis. J Pediatr Adolesc Gynecol, 2016.PMID 27969009
- [5]Bacon JL, Romano ME, Quint EH Clinical Recommendation: Labial Adhesions. J Pediatr Adolesc Gynecol, 2015.PMID 26162697
- [6]Kim SW, Han JY, Han SJ Effect of topical estrogen cream compared with observation in prepubertal girls with labial adhesions. J Pediatr Urol, 2023.PMID 37179197
- [7]Norris JE, Elder CV, Dunford AM Spontaneous resolution of labial adhesions in pre-pubertal girls. J Paediatr Child Health, 2018.PMID 29436045
- [8]Bercaw-Pratt JL, Boardman LA, Simms-Cendan JS Clinical recommendation: pediatric lichen sclerosus. J Pediatr Adolesc Gynecol, 2014.PMID 24602304
- [9]De Luca DA, Papara C, Vorobyev A Lichen sclerosus: The 2023 update. Front Med (Lausanne), 2023.PMID 36873861
- [10]Fistarol SK, Itin PH Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol, 2013.PMID 23329078
- [11]Kirtschig G, Kinberger M, Kreuter A EuroGuiderm guideline on lichen sclerosus-Treatment of lichen sclerosus. J Eur Acad Dermatol Venereol, 2024.PMID 38822598
- [12]Bloomfield V, Iseyemi A, Kives S Clinical Review: Prepubertal Bleeding. J Pediatr Adolesc Gynecol, 2023.PMID 37301426