Paeds · neurology-neurodisability-and-neuromuscular
Acute neuromuscular respiratory failure
Also known as Neuromuscular ventilatory failure · Respiratory pump failure · Respiratory muscle failure · Ventilatory failure from neuromuscular weakness
Fellowship guide to acute neuromuscular respiratory failure in children. Covers the respiratory pump from brainstem to diaphragm and bulbar muscles, the two mechanisms of failure, hypercapnic pump failure and hypoxaemic bulbar aspiration, the bedside forced vital capacity, maximum inspiratory pressure, and maximum expiratory pressure monitoring with the Lawn twenty-thirty-forty thresholds and the Durand and Sharshar predictors of ventilation, the differential across the motor unit from anterior horn cell to muscle including spinal muscular atrophy, Guillain-Barre syndrome, myasthenia gravis, infant botulism, and Duchenne muscular dystrophy, the airway decision between non-invasive ventilation when bulbar function is intact and intubation for bulbar weakness, the avoidance of suxamethonium and use of rocuronium one milligram per kilogram, cough augmentation with mechanical insufflation-exsufflation, and the disease-specific and long-term ventilation decisions.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A previously well seven-year-old who is recovering from a viral illness stops walking over three days. His legs are weak and floppy, his reflexes have vanished, and by day four he is struggling to finish a sentence and his cough is barely audible. His oxygen saturation reads ninety-eight percent. This child has a failing respiratory bellows, and if the team waits for the saturation to drop or the carbon dioxide to rise they will be intubating after an arrest rather than before one. The lungs are normal; the pump has failed. The whole art of managing acute neuromuscular respiratory failure is to recognise the failing pump early, measure it with a bedside forced vital capacity, and protect the airway before the blood gas decompensates. [4][1]
Overview & Definition
Acute neuromuscular respiratory failure is ventilatory failure caused by weakness of the respiratory pump, the chain that runs from the brainstem respiratory centre through the spinal cord and motor nerves to the neuromuscular junctions and the respiratory muscles, while the lung tissue itself is structurally normal. It is a bellows failure, not an alveolar failure. Because the failing pump moves less air, the defining physiological disturbance is progressive hypercapnia from under-ventilation, with a superimposed hypoxaemia once bulbar weakness lets secretions and feed pool and micro-aspirate. [4]
The clinical problem is that this failure is invisible to the monitors early on. The remaining alveoli still oxygenate the blood that reaches them, so the oxygen saturation stays high while carbon dioxide climbs; a normal saturation is therefore reassuring in the wrong direction. The single most important habit is to measure the respiratory reserve directly with a bedside forced vital capacity and to track it over time, because the trajectory of that number predicts arrest hours before the child looks sick. [1][3]
Classification
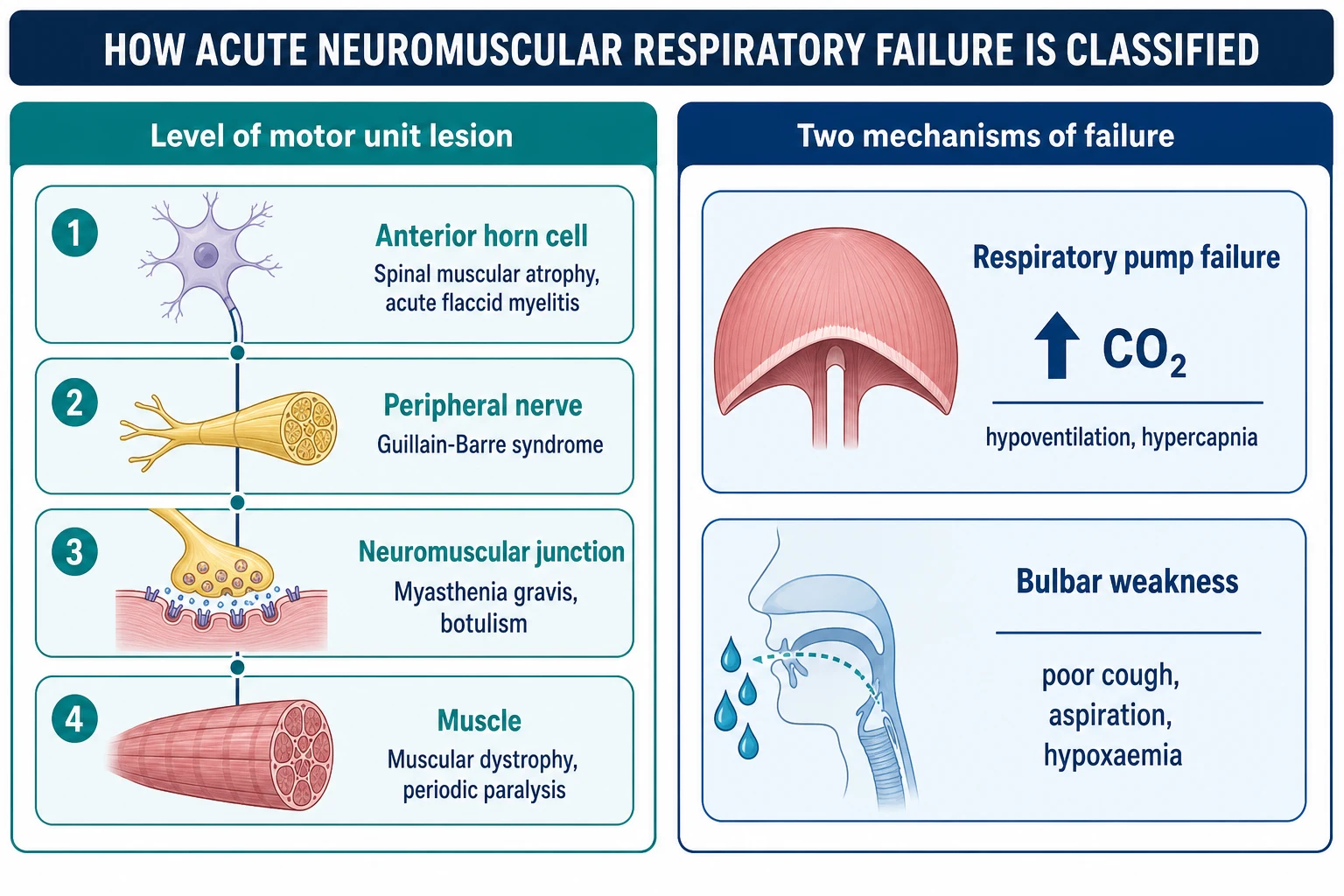
The classification answers two practical questions at once: where in the motor unit the disease sits, and which of the two mechanisms of failure is doing the killing. The motor-unit axis runs from anterior horn cell to muscle, and each level carries its own tempo and its own disease. [4]
- Spinal muscular atrophy (chronic, infant)
- Acute flaccid myelitis (acute, polio-like, asymmetric)
- Poliomyelitis
- Guillain-Barré syndrome (commonest acute cause)
- Tick paralysis (resolves on tick removal)
- Severe toxic neuropathy
- Myasthenia gravis (myasthenic crisis, fatigable)
- Infant botulism (descending, with constipation)
- Organophosphate poisoning
- Muscular dystrophies (Duchenne, chronic decompensation)
- Congenital myopathies
- Periodic paralysis (reversible, electrolyte-driven)
The functional axis separates the two ways the child decompensates. Respiratory pump failure is weakness of the diaphragm and intercostals: tidal volume falls, the chest goes quiet, and carbon dioxide rises. Bulbar failure is weakness of the cranial-nerve-driven muscles: the cough fails, secretions pool, and aspiration drives the oxygen down with atelectasis and infection. Most children have both by the time they reach intensive care, and the balance between them decides whether a mask can save them or whether they need a tube. [4][11]
Epidemiology & Risk Factors
Neuromuscular weakness is a substantial minority of paediatric intensive care respiratory admissions, and Guillain-Barré syndrome is the single commonest acute cause in a previously well child, with roughly a quarter of affected children needing mechanical ventilation. The chronic neuromuscular diseases, chiefly spinal muscular atrophy type one and Duchenne muscular dystrophy, account for the largest share of long-term ventilated children, although disease-modifying therapy is steadily changing that burden. [4][6][5]
The risk of respiratory failure clusters in three groups that the clinician can read at the bedside. Rapid progression to nadir within days, as in axonal Guillain-Barré syndrome and acute flaccid myelitis, gives little time to act. Established bulbar weakness, facial weakness, and a weak cough mark the child who will aspirate. And a falling forced vital capacity is the single most useful early signal, because it falls before the child looks sick. In chronic disease an intercurrent respiratory infection is the usual trigger that tips a marginal reserve into failure, and infants are over-represented because infant botulism, spinal muscular atrophy type one, and the congenital myopathies all present in the first year with weak suck, hypotonia, and chest infections. [2][3]
Pathophysiology
The respiratory pump is built from three linked parts that can each fail. The brainstem respiratory centre drives the spinal cord, the spinal cord drives the phrenic nerve from cervical roots C3 to C5 to innervate the diaphragm, the main muscle of inspiration, and it drives the intercostal nerves to the intercostal muscles, which contribute to expiration and cough. Separate cranial nerves, chiefly nine, ten, and twelve, drive the bulbar muscles that protect the airway, generate the cough, and coordinate swallowing. [4]
When weakness strikes anywhere along this chain the tidal volume falls and carbon dioxide climbs, and because the lungs are normal the oxygen exchange is preserved early, so the saturation reads high and the chest goes quiet. This is the trap: the child is failing while the monitor is calm. As the cranial nerves weaken the cough fails, secretions pool, micro-aspiration seeds atelectasis and infection, and oxygenation finally drops. Two failures therefore run in parallel, a hypercapnic pump failure and a hypoxaemic bulbar failure, and the patient who reaches intensive care usually has both. [4][9]
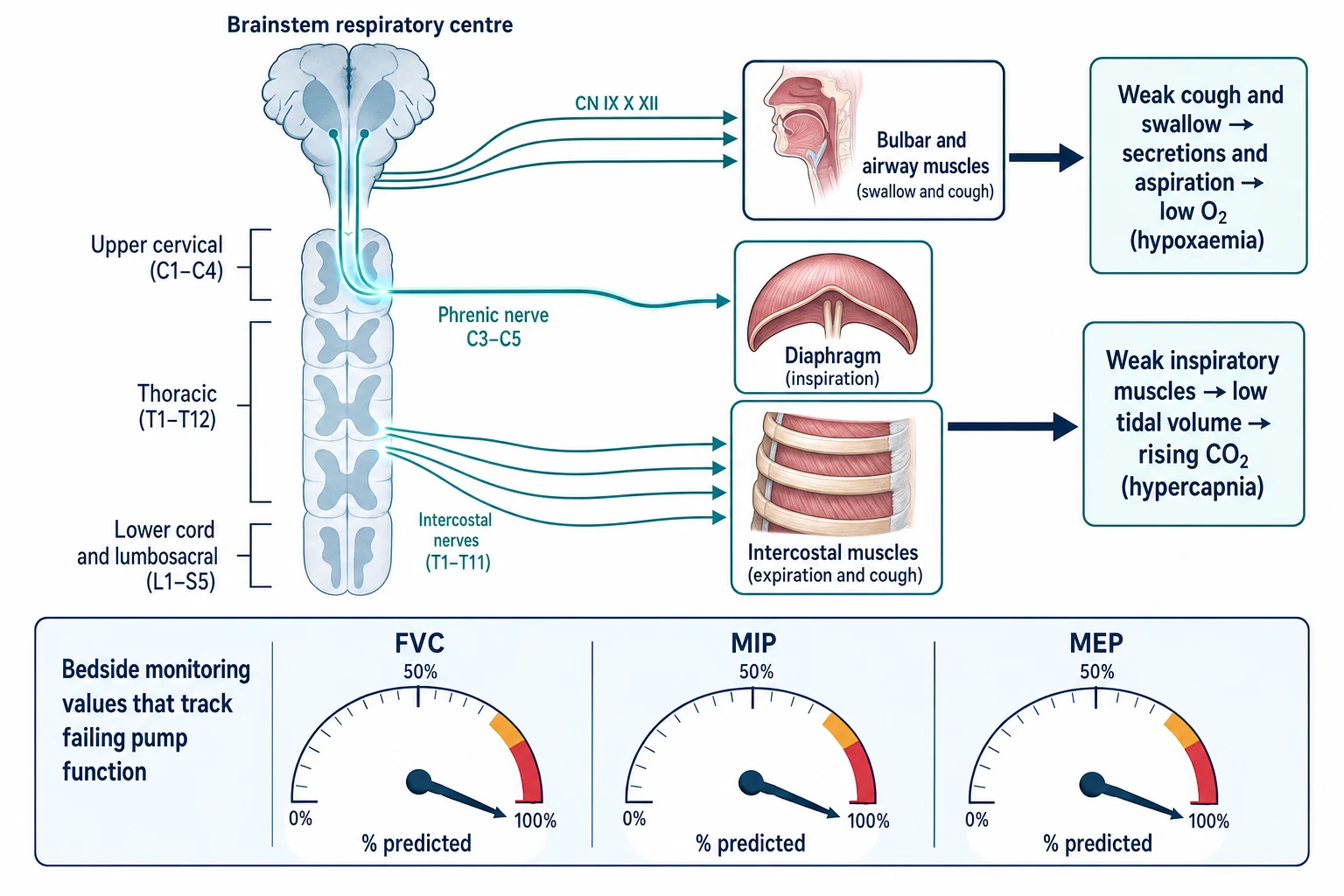
The forced vital capacity, the total volume a forced expiration can move, tracks the available muscle reserve, which is why serial bedside spirometry is the monitoring mainstay. The maximum inspiratory pressure probes inspiratory strength and the maximum expiratory pressure probes expiratory and cough strength, and both turn abnormal earlier than the vital capacity, so they are the more sensitive early-warning tests in a cooperative child. [1][11]
Clinical Presentation
The child is usually brought in for the underlying disease, and the respiratory failure is a complication the team must anticipate rather than wait for. The early signs are quiet, shallow breathing, speech that collapses to single words or short sentences, a weak or absent cough, and a voice that has gone soft or nasal. The chest moves little, the abdomen may paradox inwards on inspiration as the diaphragm fails, and the accessory muscles are conspicuously not recruiting because they are themselves weak. [4]
The cardinal trap is the reassuring saturation. Because the failing pump clears carbon dioxide poorly but the remaining alveoli still oxygenate blood, a child with a normal saturation and a rising carbon dioxide can arrest without warning. The bulbar signs that predict aspiration are cooing or nasal dysphonia, nasal regurgitation, pooled oral secretions, a weak gag and cough, and dysphagia. Autonomic instability with fluctuating blood pressure and heart rate is prominent in Guillain-Barré syndrome. In infants the chronic-disease presentation is weak suck, a feeble cry, poor head control, and frog-leg posture with recurrent chest infections, while acute infant botulism adds constipation, descending symmetrical weakness, and cranial-nerve palsies over hours to days. [7][1]
Differential Diagnosis
The practical differential is framed by the tempo of onset and the level of the motor unit, because both point to the cause and to whether a specific reversing therapy exists. A previously well child who worsens over hours to days raises Guillain-Barré syndrome, acute flaccid myelitis, infant botulism, myasthenic crisis, tick paralysis, and the periodic paralyses; chronic disease that decompensates with an infection raises spinal muscular atrophy, the muscular dystrophies, and the congenital myopathies. [4][6]
- Ascending, symmetrical, areflexic
- Days to nadir; post-infectious
- Treat with IVIG 2 g/kg
- Focal, asymmetric, polio-like
- After viral illness; anterior horn cell
- MRI shows anterior cord T2 change
- Fatigable ptosis, ophthalmoplegia, bulbar
- Worsens through the day
- Treat with IVIG or plasma exchange
- Descending, symmetrical, cranial nerves
- Constipation; dilated pupils
- Give botulism immune globulin early
The mimics outside the motor unit must be excluded because they change the management entirely. Central depression from opiates or sedatives reduces consciousness and respiratory drive rather than producing areflexic weakness, and responds to naloxone or reversal. A high spinal cord lesion or cord compression from tumour, abscess, or haematoma produces back pain and a sensorimotor level and is a surgical emergency needing urgent MRI. Hypokalaemic periodic paralysis can paralyse the respiratory muscles over hours and is fully reversible with potassium correction, so a serum electrolyte panel is part of the first bloods. Primary lung or airway disease, such as severe asthma or pneumonia, fails oxygenation early and changes the chest findings. [3][7]
Clinical & Bedside Assessment
The bedside assessment answers two questions in parallel: how much respiratory reserve remains, and can the child protect the airway. Reserve is measured by serial bedside spirometry, recording the forced vital capacity, maximum inspiratory pressure, and maximum expiratory pressure every two to six hours during acute progression, plotting them on a trend chart, and acting on the numbers rather than on how the child looks. [1]
Bulbar and airway protection is assessed at the bedside by the strength of the cough, the quality of the voice, the ability to handle secretions, the swallow, and the gag. The examination seeks paradoxical abdominal breathing, a quiet chest with reduced air entry, accessory-muscle recruitment that is conspicuously absent, and the cranial nerves with ptosis, ophthalmoplegia, and facial weakness. The deep tendon reflexes are lost early in Guillain-Barré syndrome and preserved or sluggish in myasthenia and in primary muscle disease, a single discriminator that is worth more than many investigations. [3][4]
PUMP
One bedside forced vital capacity or peak cough flow measurement changes the decision more than any blood gas in the early phase, because both the gas and the saturation stay normal until the child is already decompensating. The message to carry is that a normal gas never defers a decision already indicated by the spirometry. [1][2]
Investigations
The investigations divide into the monitoring that drives the airway decision and the diagnostic workup of the cause, and the two run together. For monitoring, serial bedside forced vital capacity is the cornerstone, with the thresholds drawn from the Lawn study of Guillain-Barré syndrome that anchor both paediatric and adult practice. [1]
The arterial or capillary blood gas is a late and confirmatory test. A rising PaCO2 with a respiratory acidosis confirms overt failure, but a normal gas never excludes impending failure and must never be used to defer a decision already indicated by the spirometry. Peak cough flow is increasingly used to assess expiratory and bulbar reserve, and a chest radiograph identifies atelectasis, consolidation, or aspiration that shift the balance toward intubation. [4]
- Earliest and most useful
- Drives the airway decision
- Track the trend, not one value
- Late and confirmatory
- Normal gas never excludes failure
- Rising CO2 means decompensation
- Assesses expiratory and bulbar reserve
- Falls as cough fails
- Guides cough augmentation
The diagnostic workup is disease-specific and runs in parallel with the monitoring. Cerebrospinal fluid is sent for albuminocytological dissociation and neurophysiology is requested to confirm Guillain-Barré syndrome; a spinal MRI excludes acute flaccid myelitis, transverse myelitis, and cord compression; repetitive nerve stimulation and acetylcholine-receptor antibodies test for myasthenia gravis; stool toxin assay and electrophysiology test for infant botulism; creatine kinase and genetic testing identify the muscular dystrophies; and SMN1 deletion testing confirms spinal muscular atrophy. [2][7][6]
Management — Resuscitation
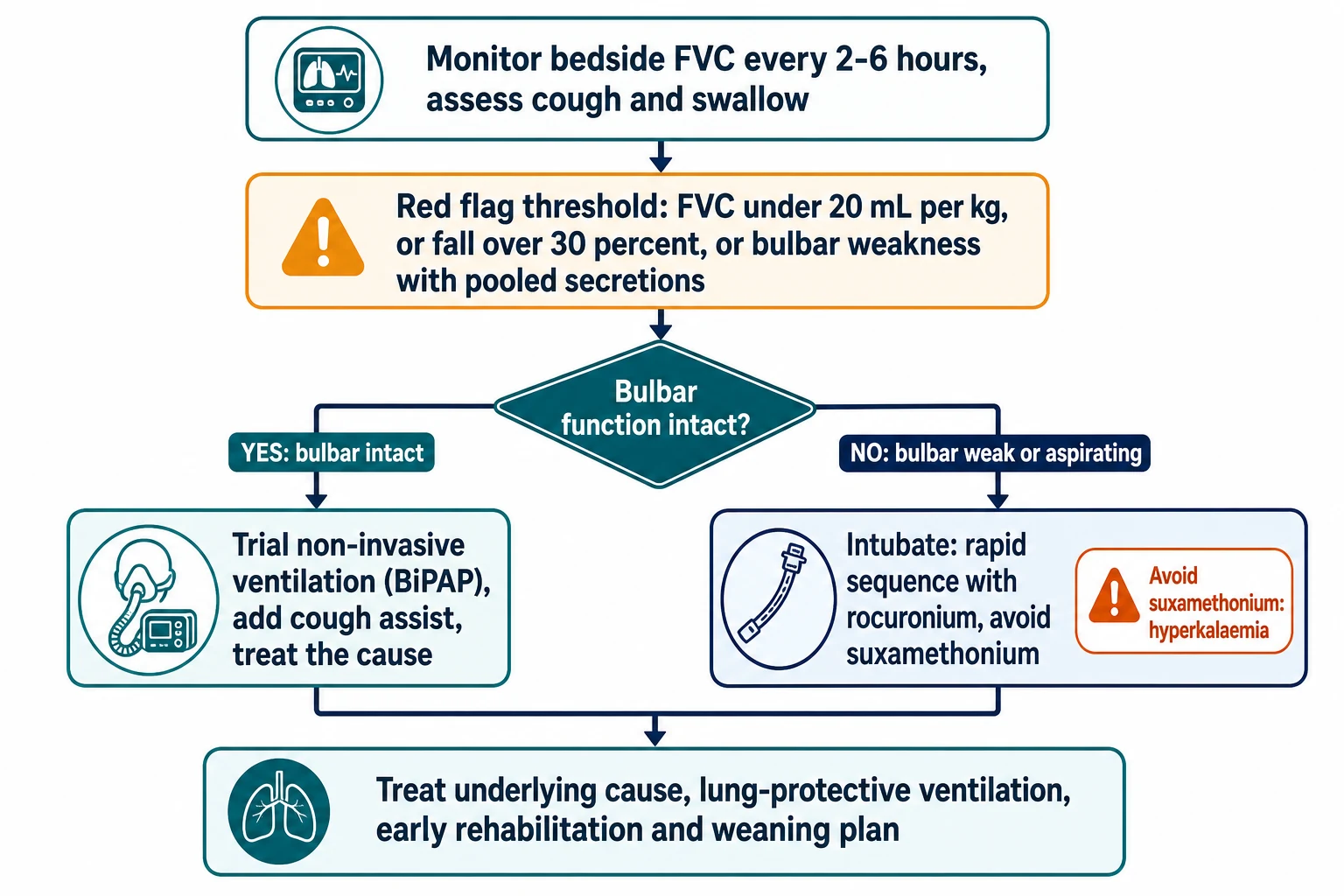
The immediate priority is to protect the airway and support the failing pump before blood-gas decompensation, because the child with a normal saturation and a rising carbon dioxide can arrest abruptly. Continuous cardiac and haemodynamic monitoring is set up for autonomic instability, oxygen is given only to maintain a target saturation and never as a substitute for ventilation, and the airway decision is made from the spirometry and the bulbar assessment, not from the gas. [4][1]
If the forced vital capacity is under twenty millilitres per kilogram or falling by over thirty percent, or if there is bulbar weakness with a weak cough and pooled secretions, the child is transferred to intensive care. If the bulbar function is intact and the failure is pure pump weakness, a trial of non-invasive bilevel positive airway pressure may avert or delay intubation; if bulbar weakness threatens aspiration, the child is intubated electively. [9][8]
Rocuronium (rapid sequence intubation)
Dose
1 mg per kg intravenous push
Management — Definitive & Stepwise
The definitive management is a ladder that moves from monitoring to non-invasive support to intubation and ventilation, and in chronic disease to tracheostomy and long-term ventilation. Each rung has an explicit escalation trigger, so the team never waits for an arrest to climb. [4]
Serial bedside spirometry every two to six hours with an explicit intensive-care threshold: FVC under 20 mL/kg, fall over 30 percent, MIP weaker than minus 30 cmH2O, or MEP under 40 cmH2O
Non-invasive bilevel positive airway pressure for pump failure with intact bulbar function, started early and weaned as the disease improves
Cough augmentation with mechanical insufflation-exsufflation, manually assisted coughing, and air stacking to clear secretions and reduce atelectasis
Intubation and lung-protective ventilation for bulbar failure, failing non-invasive ventilation, or overt hypercapnic failure, with rocuronium and never suxamethonium
Disease-specific therapy: IVIG 2 g/kg for GBS, IVIG or plasma exchange for myasthenic crisis, botulism immune globulin for infant botulism, nusinersen, risdiplam, or onasemnogene abeparvovec for SMA
The family-centred tracheostomy and long-term ventilation decision in chronic irreversible disease, balanced against quality of life
Cough augmentation is the centre of gravity of chronic neuromuscular respiratory care. Mechanical insufflation-exsufflation pushes a positive pressure in and then rapidly drops to negative pressure to simulate a cough, clearing secretions that the weak expiratory muscles cannot move, and observational data show it reduces hospitalisations and can avert intubation when bulbar function is adequate. [11][12]
Non-invasive ventilation is powerful but bounded. In pure pump failure with an intact bulbar mechanism it can carry the child through the nadir of a Guillain-Barré syndrome or a myasthenic crisis, and in Duchenne muscular dystrophy it is the foundation of long-term care. It fails when bulbar weakness develops, because it does not protect the airway, and trying to make it work in an aspirating child only delays the intubation that was always going to be needed. [9][8][5]
Specific Subtypes & Scenarios
Each cause carries its own tempo and its own decision points, and recognising the cause points to the specific therapy. Guillain-Barré syndrome is the prototype: weakness ascends over days, around a quarter of children need ventilation, the Lawn thresholds drive the decision, and intravenous immunoglobulin two grams per kilogram is the disease-modifying treatment, while non-invasive ventilation may fail when bulbar weakness develops. [1][2]
Acute flaccid myelitis produces focal, asymmetric, polio-like weakness after a viral illness and can involve the diaphragm; the limb prognosis is poor but the respiratory course is usually shorter, and management is supportive with meticulous airway clearance. Myasthenic crisis presents with fatigable bulbar and respiratory weakness and is managed with non-invasive ventilation as a bridge, intubation for bulbar failure, intravenous immunoglobulin or plasma exchange, and avoidance of the drugs that worsen myasthenia such as certain antibiotics and magnesium. [8]
Infant botulism is the great paediatric mimic to treat early. It produces descending symmetrical weakness over hours to days with cranial-nerve palsies, constipation, and dilated pupils, and the specific treatment is human botulism immune globulin intravenous, which shortens the duration of ventilation and hospital stay when given early on clinical suspicion rather than after toxin confirmation. Spinal muscular atrophy type one presents in the first months with severe hypotonia and a weak cough and is managed with proactive non-invasive ventilation, airway clearance, and disease-modifying therapy that has transformed a historically lethal prognosis. Duchenne muscular dystrophy loses respiratory reserve over years, with nocturnal hypoventilation and a falling peak cough flow, and its care is built around surveillance spirometry, nocturnal non-invasive ventilation, and cough augmentation. [7][6][5]
Complications & Pitfalls
The classic and dangerous pitfall is being reassured by a normal oxygen saturation, because in pure pump failure the saturation stays high while carbon dioxide climbs, and the child arrests with a gas that was reassuring an hour earlier. The airway pitfall is using non-invasive ventilation in bulbar weakness, where it does not protect the airway, hides the aspiration, and delays the intubation that was always going to be needed; non-invasive ventilation is for intact bulbar function. [9][4]
The monitoring pitfall is relying on a single blood gas or a single spirometry reading instead of a serial trend, because the trajectory is what predicts arrest. The disease pitfall is missing a treatable cause such as hypokalaemic periodic paralysis, myasthenic crisis, or infant botulism, each of which has a specific reversing therapy. The chronic-disease pitfall is failing to anticipate the silently eroded respiratory reserve in spinal muscular atrophy or Duchenne muscular dystrophy, so an intercurrent infection tips the child into failure. Ventilation-associated pneumonia, atelectasis, and prolonged weaning are the intensive-care complications that cough augmentation and lung-protective ventilation aim to prevent. [11][3]
Prognosis & Disposition
The prognosis is dominated by the underlying cause and the speed of the airway decision. Acute, reversible disease carries a good prognosis when the airway is protected early: most children with Guillain-Barré syndrome recover over weeks to months and the majority walk independently within a year, although residual fatigue and proximal weakness can persist. Acute flaccid myelitis carries a poorer limb prognosis, with persistent weakness in the most affected limb, but a shorter respiratory course. [1][4]
Myasthenic crisis responds to immunotherapy and has a good short-term outlook once the airway is secured, and infant botulism given early botulism immune globulin has a substantially shortened ventilation and hospital course with full recovery expected. The chronic diseases carry the heaviest burden. Spinal muscular atrophy type one was historically lethal in infancy, although disease-modifying therapy has transformed the outlook, and Duchenne muscular dystrophy progresses to respiratory failure and cardiomyopathy in early adulthood unless long-term ventilation is instituted. Disposition is always to a tertiary paediatric intensive care unit with retrieval, paediatric neurology, and access to neurophysiology and chronic-ventilation services, with a planned weaning and rehabilitation pathway and a clear safety-net for relapse or autonomic instability. [6][5][7]
Special Populations
Infants are the most vulnerable group, because infant botulism, spinal muscular atrophy type one, and the congenital myopathies all declare themselves in the first year, and because the soft, compliant infant chest wall and the small residual respiratory reserve make even modest weakness rapidly decompensating. In spinal muscular atrophy type one, proactive non-invasive ventilation and airway clearance from diagnosis, combined with disease-modifying therapy, have replaced the older palliative framing for many families. [6]
The technology-dependent child with an established tracheostomy and home ventilation presents to the emergency department with acute deterioration, and management focuses on the tracheostomy, the ventilator settings, and the usual infection or mucus-plug triggers rather than on the primary diagnosis. The adolescent with Duchenne muscular dystrophy nearing transition faces the long-term ventilation decision, which is explicitly family-centred and quality-of-life based, and which must be documented and shared with the adult service. The child with a chronic neuromuscular disease and an intercurrent respiratory infection needs early escalation of airway clearance and non-invasive ventilation, because the threshold for failure is lower than in the well child. [5][12]
Evidence, Guidelines & Regional Differences
The monitoring framework rests on the Lawn study of predictors of mechanical ventilation in Guillain-Barré syndrome, which established the forced vital capacity, maximum inspiratory pressure, and maximum expiratory pressure thresholds that anchor paediatric and adult practice, and on the Durand and Sharshar prospective predictor studies that refined which patients will need ventilation. [1][2][3]
Lawn et al, Arch Neurol 2001
Key finding
In 114 adults with Guillain-Barré syndrome, a forced vital capacity under 20 mL/kg, a maximum inspiratory pressure weaker than minus 30 cmH2O, a maximum expiratory pressure under 40 cmH2O, and a decline in vital capacity over 30 percent independently predicted the need for mechanical ventilation.
Practice change
These thresholds, the origin of the 20-30-40 rule, remain the bedrock of neuromuscular respiratory monitoring in adults and children.
The respiratory care of Duchenne muscular dystrophy is set by the international care considerations of Birnkrant and Bushby, which define surveillance spirometry, the threshold for nocturnal non-invasive ventilation at a forced vital capacity under thirty percent predicted or symptomatic hypoventilation, and cough augmentation at a falling peak cough flow. Spinal muscular atrophy care follows the Wang consensus standard, now overlaid by the disease-modifying era. [5][6]
Non-invasive ventilation and mechanical insufflation-exsufflation are championed by Bach and colleagues, whose multicentre observational data show that aggressive non-invasive management can avert or delay tracheostomy and improve survival, although randomised-trial evidence is limited and the technique is contested in severe bulbar weakness. The controversy in chronic disease is the tracheostomy-versus-long-term-non-invasive-ventilation decision, which turns on bulbar function, quality of life, and family values rather than on a single evidence threshold. Regional practice varies in the readiness to intubate versus to trial non-invasive ventilation, and in the adoption of peak cough flow monitoring. [11][12][4]
Australian and New Zealand practice follows the paediatric intensive care retrieval model: early escalation to a tertiary PICU, rocuronium-based rapid sequence intubation, and a low threshold to intubate once bulbar weakness is present. Non-invasive ventilation is used as a bridge in Guillain-Barré syndrome and myasthenic crisis with intact bulbar function, and long-term home ventilation programmes coordinate the tracheostomy decision for chronic disease. [4]
Exam Pearls
The single most testable fact is that neuromuscular respiratory failure is a hypercapnic pump failure in which the oxygen saturation is normal until late, so the decision is driven by forced vital capacity and the bulbar assessment, never by the saturation or a normal blood gas. The Lawn thresholds are the twenty-thirty-forty rule: forced vital capacity under twenty millilitres per kilogram, fall over thirty percent, maximum inspiratory pressure weaker than minus thirty centimetres of water, and maximum expiratory pressure under forty centimetres of water. [1][3]
Suxamethonium is contraindicated in any denervating or chronic neuromuscular disease because of hyperkalaemic arrest, and rocuronium one milligram per kilogram is the rapid-sequence alternative. Non-invasive ventilation is for intact bulbar function and fails in bulbar weakness, where the answer is intubation. [10][9]
Infant botulism is descending and symmetrical with cranial-nerve palsies and constipation, treated with human botulism immune globulin on suspicion, not after toxin confirmation. Guillain-Barré syndrome is ascending and areflexic, myasthenia is fatigable and ocular-bulbar, acute flaccid myelitis is focal and polio-like, and periodic paralysis is metabolic and reversible. The disease-modifying era has transformed the prognosis of spinal muscular atrophy, which was once the paradigm of infantile respiratory death and is now a treated chronic disease. [7][6][5]
Self-test: what forces intubation in a child with rising weakness?
A forced vital capacity under twenty millilitres per kilogram, a fall of over thirty percent in twenty-four hours, a maximum inspiratory pressure weaker than minus thirty centimetres of water, a maximum expiratory pressure under forty centimetres of water, or any bulbar weakness with a weak cough and pooled secretions. The decision is made from these numbers, not from the saturation or the blood gas. [1]
References
- [1]Lawn ND, Fletcher DD, Henderson RD, Wolanskyj AP, Wijdicks EF Anticipating mechanical ventilation in Guillain-Barré syndrome Arch Neurol, 2001.PMID 11405803
- [2]Durand MC, Porcher R, Orlikowski D, et al Clinical and electrophysiological predictors of respiratory failure in Guillain-Barré syndrome: a prospective study Lancet Neurol, 2006.PMID 17110282
- [3]Sharshar T, Chevret S, Bourdain F, Raphaël JC Early predictors of mechanical ventilation in Guillain-Barré syndrome Crit Care Med, 2003.PMID 12545029
- [4]Bach JR, Turcios NL, Wang L Respiratory Complications of Pediatric Neuromuscular Diseases Pediatr Clin North Am, 2021.PMID 33228931
- [5]Birnkrant DJ, Bushby K, Bann CM, et al Diagnosis and management of Duchenne muscular dystrophy, part 2: respiratory, cardiac, bone health, and orthopaedic management Lancet Neurol, 2018.PMID 29395990
- [6]Wang CH, Finkel RS, Bertini ES, et al Consensus statement for standard of care in spinal muscular atrophy J Child Neurol, 2007.PMID 17761659
- [7]Pifko E, Price A, Sterner S Infant botulism and indications for administration of botulism immune globulin Pediatr Emerg Care, 2014.PMID 24488164
- [8]Misra UK, Kumar S, Singh VK, et al Noninvasive Ventilation in Myasthenia Gravis Neurol India, 2020.PMID 32643679
- [9]Wijdicks EF, Roy TK BiPAP in early guillain-barré syndrome may fail Can J Neurol Sci, 2006.PMID 16583732
- [10]Martyn JA, Richtsfeld M Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms Anesthesiology, 2006.PMID 16394702
- [11]Bach JR, Choi WA Mechanical Insufflation-Exsufflation: The Rest of the Story Respiration, 2023.PMID 37040715
- [12]Gonçalves MR, Bach JR, Ishikawa Y, et al Continuous noninvasive ventilatory support outcomes for patients with neuromuscular disease: a multicenter data collaboration Pulmonology, 2021.PMID 34656524