Paeds · neurology-neurodisability-and-neuromuscular
Autoimmune encephalitis
Also known as Anti-NMDA receptor encephalitis · Antibody-mediated encephalitis · Post-herpes simplex autoimmune encephalitis · Limbic encephalitis · Cell-surface antibody encephalitis
Fellowship guide to autoimmune encephalitis in children. Covers the Graus 2016 diagnostic tiers of possible, probable, and definite disease with the specific anti-NMDA receptor criteria, the distinction between cell-surface antibody syndromes that respond to immunotherapy and intracellular onconeural syndromes that often do not, the pathophysiology of antibody-mediated NMDA receptor internalisation versus cytotoxic T-cell injury, the staged presentation from prodrome through psychiatric change to seizures, movement disorder, and dysautonomia, the first-line immunotherapy ladder of methylprednisolone, intravenous immunoglobulin, and plasma exchange and the second-line ladder of rituximab and cyclophosphamide at ten to fourteen days, the ovarian teratoma association and the search for and removal of occult tumours, the extreme delta brush EEG pattern and CSF pleocytosis, the Titulaer outcome data on early treatment and second-line therapy, and the prolonged multidisciplinary recovery with cognitive and school reintegration.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who changes over days to weeks from healthy to confused, agitated, and twitching, with seizures that will not settle and movements that look bizarre, is presenting one of the most treatable and most missed diagnoses in paediatric neurology. Autoimmune encephalitis is an immune attack on the brain in which antibodies or T cells target specific neuronal proteins, producing a subacute syndrome that straddles psychiatry, epilepsy, and movement disorder. The single most important fact for the exam, and for a real child, is that it is treatable and that early treatment changes lives. [1]
The disease was reframed for modern medicine by the description of anti-NMDA receptor encephalitis in 2008 by Dalmau and colleagues, who showed that an antibody against the NMDA glutamate receptor causes a stereotyped, recoverable, and often paraneoplastic encephalitis in young people. [3] That discovery opened the field: dozens of antibody targets are now known, and autoimmune encephalitis is recognised to be as common in children as infectious encephalitis. The Graus 2016 clinical approach gives a bedside framework that lets you treat on suspicion rather than wait weeks for a result. [1]
Three ideas hold this topic together. The diagnosis turns on a tempo, a pattern of brain involvement, and the exclusion of mimics, not on a single test. The treatment is a ladder from first-line steroids, immunoglobulin, and plasma exchange to second-line rituximab and cyclophosphamide, and the timing of that ladder is the chief determinant of outcome. And the antibody target predicts the response, because antibodies against cell-surface proteins like NMDAR are reversible while antibodies against intracellular antigens are T-cell mediated and often permanent. [2]
Classification
Autoimmune encephalitis is sorted in two ways that both change what you tell a family. The first sort is by the antibody target, which predicts whether the brain injury is reversible. The second sort is by how confident the diagnosis is, which sets when you treat. [1]
The antibody-target sort splits the disease into two families with different biology and different prognosis. Antibodies against cell-surface or synaptic proteins sit on the outside of the neuron and cause a functional, often reversible disturbance. NMDAR, LGI1, CASPR2, GABA-A, GABA-B, AMPA, DPPX, mGluR5, and the dopamine D2 receptor belong here. These syndromes usually respond to immunotherapy and a child can recover fully. Antibodies against intracellular antigens such as Hu, Yo, Ma2, Ri, GAD65, and CRMP5 cannot reach their target, so the real damage is done by cytotoxic T cells that kill neurons. These syndromes are often paraneoplastic and often respond poorly, and the prognosis is guarded. [1]
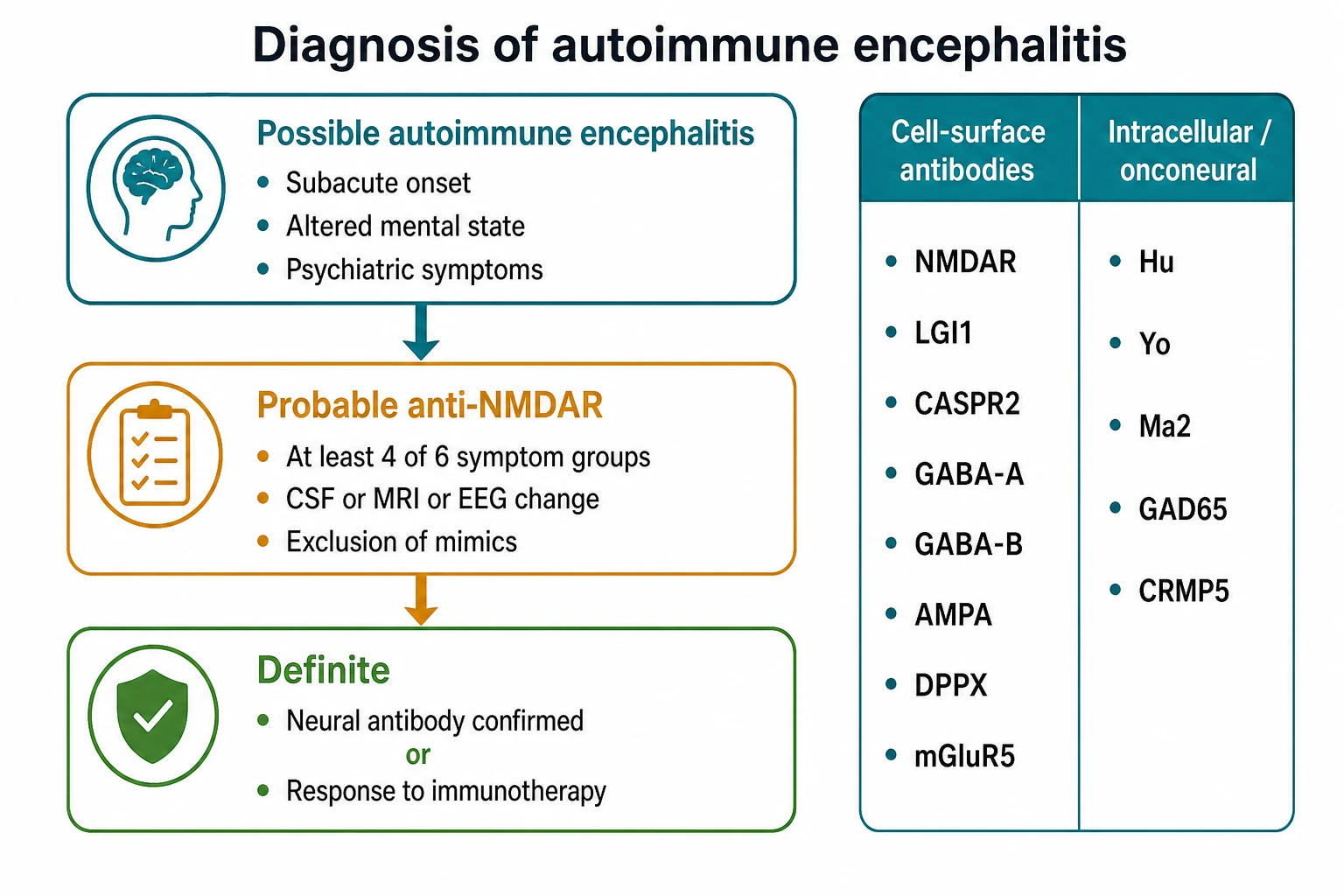
The diagnostic-confidence sort is the Graus tiering. A child meets possible autoimmune encephalitis when there is a subacute onset, under three months, of working-memory change, altered mental state, or psychiatric symptoms, with at least one supporting CSF, MRI, or EEG abnormality, after mimics are excluded. Probable anti-NMDAR encephalitis requires a rapid onset plus at least four of six symptom groups, plus a CSF or MRI or EEG change, plus either the antibody or a teratoma. Definite autoimmune encephalitis needs the antibody confirmed or a clear response to immunotherapy in the right clinical context. The point of the tiering is practical: a probable case is treated now, not when the antibody returns. [1]
Epidemiology & Risk Factors
Autoimmune encephalitis used to be considered rare, but it is now recognised to be as common in children as infectious encephalitis. Anti-NMDAR encephalitis is the dominant paediatric subtype, and the disease is more common in children and young women than in older adults. In large paediatric series the median age sits around twelve years, with a female predominance that is weaker in young children and stronger after puberty. [2]
The risk factors and associations matter because they steer the workup. A viral-like prodrome precedes many cases. An ovarian teratoma is found in a substantial minority, most often in post-pubertal girls, and its presence is both a clue and a treatment target. A recent episode of herpes simplex virus encephalitis is a specific trigger: in around twenty percent of survivors the virus exposes neuronal antigens and a secondary anti-NMDAR immune response develops weeks later. [11] Immune checkpoint inhibitors, used increasingly in adolescents with cancer, raise the risk of paraneoplastic and immune-related neurological syndromes. A personal or family history of autoimmunity is a softer clue. [1]
Pathophysiology
The mechanism of brain injury depends on where the antibody binds, and that single fact explains why some children recover and others do not. [3]
In anti-NMDAR encephalitis the antibody is IgG directed against the GluN1 subunit of the NMDA glutamate receptor on the postsynaptic membrane. Binding causes the receptors to clump together, fold into the cell, and be broken down, without complement lysis or cell death. The neuron survives but loses surface NMDA receptors, so NMDA-mediated signalling falls. Because NMDA receptors tune the balance of excitation and inhibition across the brain, their loss produces the psychiatric, cognitive, seizure, movement, and dysautonomic features that define the disease. The antibody titre is higher in CSF than in serum, which is why CSF testing is more sensitive, and the titre falls as the child recovers. The injury is functional and reversible, which is the biological basis of the good prognosis when treatment is prompt. [3]
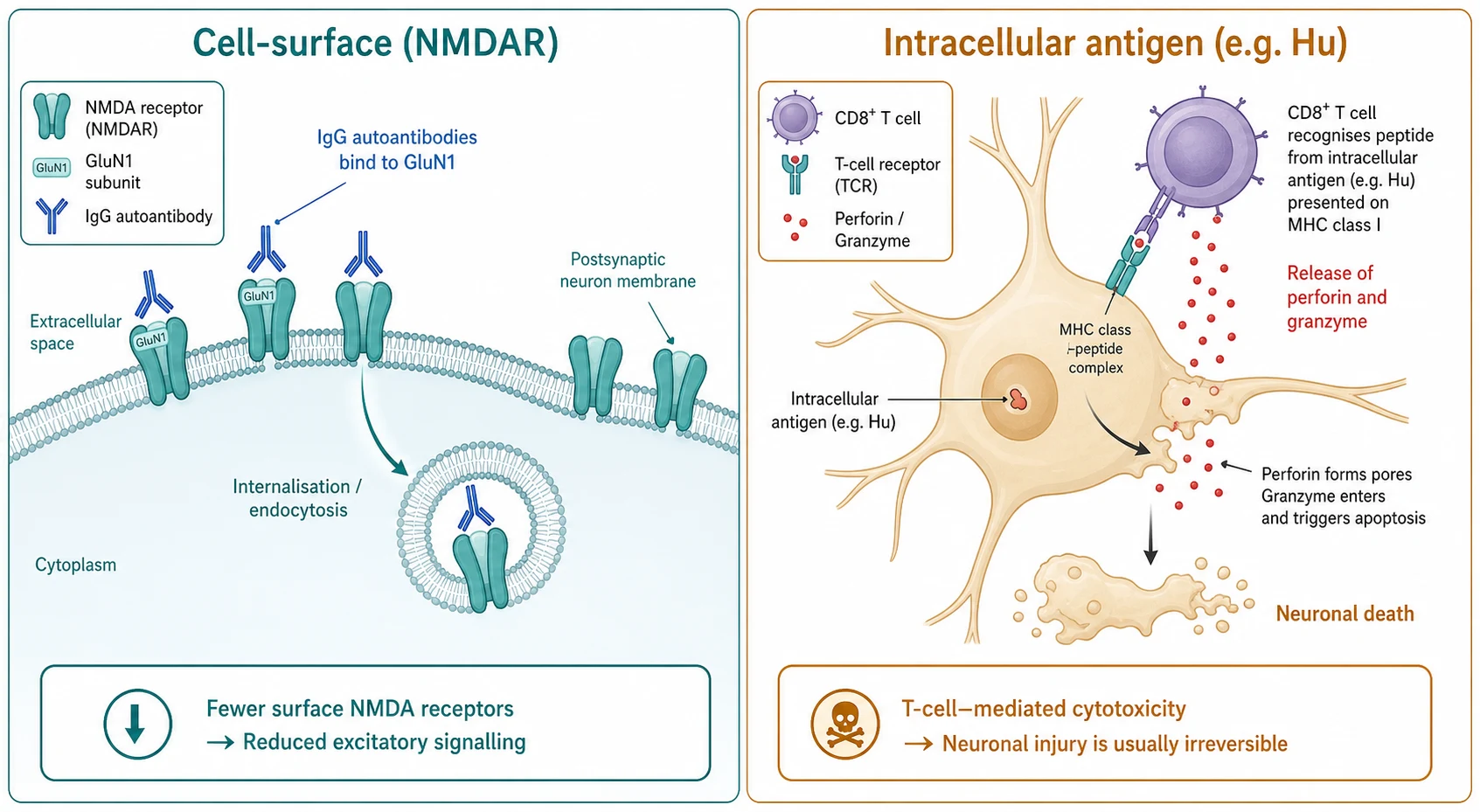
The other family works differently, and understanding it protects families from false hope. When the antigen is intracellular, the antibody never reaches it. The actual injury is done by cytotoxic CD8 T cells that infiltrate the nervous system, recognise the antigen presented on the neuronal surface, and release perforin and granzyme to kill the neuron. Neuronal loss accrues, the process is often paraneoplastic, and immunotherapy that removes antibody or B cells arrives too late to stop the T cells. This is why a child with a Hu, Yo, or Ma2 syndrome may not improve despite aggressive treatment. [1]
A trigger worth holding in mind is herpes simplex virus. After the virus damages temporal lobe neurons, the exposed antigens can break immune tolerance and provoke a secondary anti-NMDAR response in around a fifth of survivors. This explains the child who relapses weeks after seemingly successful treatment of HSE, and it is a mechanism rather than recurrent infection. [11]
Clinical Presentation
Anti-NMDAR encephalitis tells a story that unfolds over days to weeks, and the chapters are what you will be examined on. A viral-like prodrome of fever, headache, and malaise opens the illness in many children, lasting a few days. Then comes the psychiatric phase: anxiety, agitation, insomnia, hallucinations, bizarre or paranoid behaviour, catatonia, and in a younger child, regression, school refusal, or new psychosis. This phase is where the diagnosis is most often missed, because the child is sent to psychiatry before any neurological sign appears. [2]
The neurological phase follows and brings the disease into focus. Seizures are common, sometimes as the first clear sign. Speech disturbance ranges from pressured speech and verbal stereotypies to complete mutism. Abnormal movements are highly characteristic: orofacial dyskinesias with lip-smacking, grimacing, and chewing, choreoathetosis, dystonia, and rigidity. The child becomes cognitively impaired and the level of consciousness falls toward coma. Autonomic instability appears with tachycardia, fluctuating blood pressure, hypoventilation, hyperthermia, and bradycardic crises. [2]
The age of the child bends the presentation in ways examiners test deliberately. Young children more often present with seizures, movement disorder, and speech or developmental regression, and less often with overt psychiatric features, so the psychiatric anchor that flags the diagnosis in teenagers is absent and the workup is delayed. The post-pubertal girl with an ovarian teratoma may present with the full syndrome and a pelvic mass. The child recovering from herpes simplex encephalitis who relapses weeks later is the classic post-HSE autoimmune trigger. [11]
NMDAR
Differential Diagnosis
The differential is wide because the illness crosses psychiatry, infection, metabolism, and neurology, and the task is not to memorise a list but to separate the mimics that demand different treatment. [9]
The first fork is between autoimmune disease and a primary psychiatric disorder. Acute psychosis, catatonia, and a behavioural decompensation in a child with autism or intellectual disability can mimic the psychiatric phase. The discriminator is the appearance of seizures, movement disorder, dysautonomia, and CSF or EEG change, none of which belong to primary psychiatric disease. Any child with new psychiatric symptoms plus any neurological sign needs an EEG and an autoimmune workup, not a psychiatric admission. [9]
The second fork is between autoimmune and infectious encephalitis. Herpes simplex virus encephalitis presents with fever and altered consciousness, usually with temporal lobe MRI change and a positive CSF polymerase chain reaction. Because the two can overlap and because HSE itself can trigger autoimmune disease, the safe rule is to give empirical aciclovir and to start immunotherapy once infection is reasonably excluded. [11]
The remaining mimics each carry a specific pitfall. Drug intoxication or withdrawal, particularly neuroleptic malignant syndrome and serotonin syndrome, can mimic the dysautonomia and rigidity. Metabolic encephalopathy from a urea cycle defect, mitochondrial disease, or acute intermittent porphyria can present with psychiatric change and seizures. Mitochondrial encephalopathy, posterior reversible encephalopathy syndrome, and primary genetic epilepsy syndromes are considered when the antibody panel is negative. The clinching combination is rapid onset, multifocal central nervous system features, CSF pleocytosis, and a neural antibody. [9]
Clinical & Bedside Assessment
The bedside assessment runs in parallel with resuscitation, because a deteriorating child cannot wait for a sequential workup. Secure the airway and breathing first, because hypoventilation is common and can be fatal, and monitor the cardiac rhythm and blood pressure for autonomic instability. Treat ongoing seizures with the standard benzodiazepine then second-line then anaesthetic ladder used for status epilepticus. [5]
The focused history pins the tempo, which is the single most discriminating feature. Ask exactly when the child was last well, whether there was a fever or viral illness, whether there was a vaccine, what psychiatric and neurological features have appeared and in what order, and whether there is a family history of autoimmunity. In a post-pubertal girl, ask about menstrual and ovarian symptoms, and in any child, screen for toxin exposure and recent cancer or immunotherapy. [5]
Examination then looks for the pattern that flags the disease. Watch for the orofacial dyskinesia, the repetitive grimacing and chewing, the choreoathetoid movements, and the dystonic posturing. Take a cognitive and developmental snapshot, and note the speech pattern from pressured speech to mutism. Check for fever, rash, signs of infection, and focal neurological signs. Request the EEG early, because non-convulsive status is common and is easy to miss behind what looks like a postictal or psychiatric state. Plan the MRI, the lumbar puncture, and the paired CSF and serum antibody panels in parallel with the first dose of treatment. [5]
In ANZ practice, retrieval networks coordinate transfer of any child with suspected encephalitis to a tertiary paediatric centre with paediatric neurology, intensive care, and rapid antibody testing. Peripheral centres start empirical aciclovir and antibiotics and first-line immunotherapy on telephone advice, because the antibody result may take one to three weeks. The threshold to treat on suspicion is low. [5]
Investigations
The investigations are designed to confirm the disease, to exclude the mimics, and to find the tumour, and they run together rather than in sequence. [5]
Cerebrospinal fluid is central. It shows a lymphocytic pleocytosis, a mildly raised protein, and oligoclonal bands in many but not all children. A normal CSF does not exclude the diagnosis, but an inflammatory CSF in the right clinical context is powerful support. The CSF is also sent for viral polymerase chain reaction including herpes simplex virus, for bacterial studies when indicated, and for cytology when a paraneoplastic process is suspected. [1]
MRI brain is abnormal in roughly half of children, with fluid-attenuated inversion recovery hyperintensity in the medial temporal lobes or in cortical and subcortical regions. A normal MRI is entirely compatible with anti-NMDAR encephalitis, so a normal scan never delays treatment. EEG is almost always abnormal, showing a slow and disorganised background, and in around thirty percent of obtunded patients with anti-NMDAR disease it reveals the extreme delta brush pattern of rhythmic one to three hertz delta activity with superimposed beta activity. Extreme delta brush is not unique to the disease and is absent in most children, but it is highly suggestive when present. [4]
[5]The neural antibody panel is sent in paired CSF and serum. CSF is more sensitive for NMDAR and is the preferred sample, so a child with a negative serum but positive CSF is not a false negative. The panel covers the common cell-surface targets, NMDAR, LGI1, CASPR2, GABA-A, GABA-B, AMPA, and mGluR5, and the intracellular onconeural antigens when paraneoplastic disease is suspected. Antibody results take one to three weeks and must never delay treatment. [1]
Whole-body imaging searches for the tumour. A post-pubertal girl receives pelvic ultrasound followed by pelvic MRI to find an ovarian teratoma. Chest and testicular imaging is added according to the antibody syndrome and the clinical context. Infection, autoimmune, and metabolic screens and toxicology are sent to exclude mimics in parallel. [5]
Management — Resuscitation
Resuscitation protects the airway and breathing and controls seizures while the workup runs. Hypoventilation and autonomic instability are the life-threatening features, so any child with a falling level of consciousness, dysautonomia, or refractory seizures is admitted to intensive care with close ventilatory and haemodynamic monitoring. [5]
Seizures are treated with the standard status epilepticus ladder. A first-line benzodiazepine, lorazepam 0.1 mg per kg intravenously, maximum 4 mg, or buccal midazolam 0.15 mg per kg when there is no access, is followed by a second-line agent such as levetiracetam 40 mg per kg intravenously, maximum 4.5 g, and escalated to an anaesthetic infusion for refractory seizures. Continuous EEG is mandatory after paralysis, because non-convulsive status is common and invisible behind the paralysed patient. [5]
The workup is sent early and in parallel. The lumbar puncture, MRI, and EEG are obtained as soon as the child is safe, the antibody panels are drawn in paired CSF and serum, and empirical intravenous aciclovir and antibiotics are started until infection is excluded. First-line immunotherapy is started as soon as the diagnosis is suspected and infection is reasonably excluded, without waiting for the antibody result, because early treatment is the strongest predictor of good outcome. [2]
Management — Definitive & Stepwise
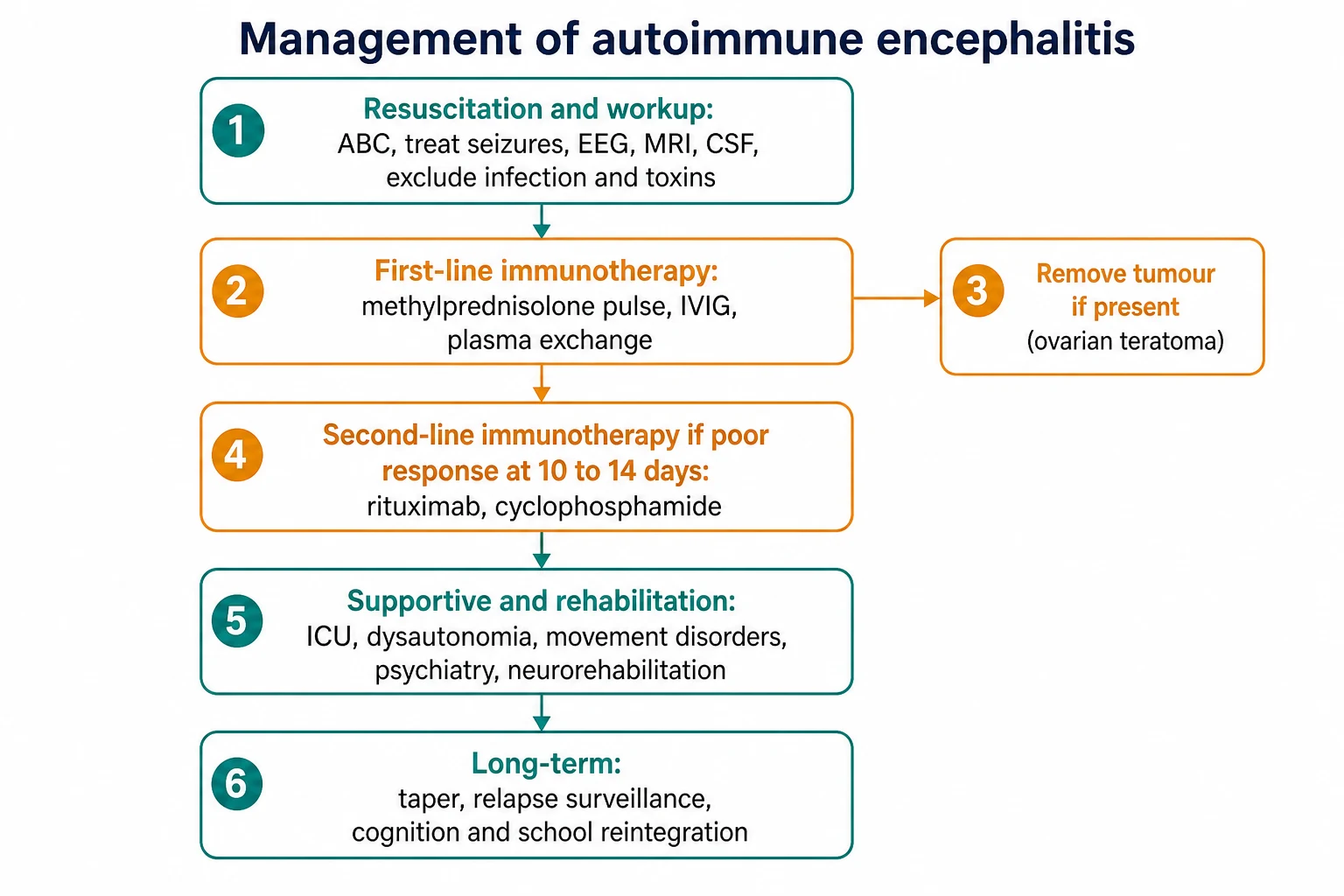
The definitive treatment is an immunotherapy ladder, and the rung the child reaches is the main determinant of how well they do. The ladder is built from first-line agents, tumour removal, and second-line agents, with supportive and rehabilitative care running throughout. [2]
First-line immunotherapy is intravenous methylprednisolone 20 to 30 mg per kg per day, maximum 1 g, for three to five days, combined with intravenous immunoglobulin 2 g per kg over two to five days, and plasma exchange, five cycles on alternate days, used alone or in combination. Many centres combine a steroid pulse with immunoglobulin to begin with, reserving plasma exchange for a non-responder. If an ovarian teratoma is found it is removed urgently, because tumour removal is the single most effective intervention in paraneoplastic anti-NMDAR disease and can transform the course. [7]
First-line immunotherapy (paediatric)
The decision to escalate to second-line therapy is the central judgement call of the disease, and the timing is fixed by the evidence. If the response to first-line therapy is poor at 10 to 14 days, as judged by persistent psychiatric, cognitive, seizure, movement, or dysautonomic features, second-line therapy is started. The second-line agents are rituximab 375 mg per m2 weekly for four weeks, and or cyclophosphamide 750 mg per m2 monthly, chosen by centre and by the side-effect profile. Titulaer showed that early immunotherapy and early second-line therapy within the first four weeks are independent predictors of good outcome, and the international paediatric consensus reinforces this approach. [2][7]
Second-line immunotherapy (paediatric)
Supportive care is not optional, and it dominates the hospital course. Dysautonomia is managed with haemodynamic support, careful fluid and electrolyte balance, and treatment of cardiac arrhythmia. Movement disorder and severe agitation may need careful sedation, with avoidance of dopamine-blocking antipsychotics where possible because of the risk of worsening movement disorder. Sleep is protected. Multidisciplinary neurorehabilitation, with physiotherapy, occupational therapy, speech and language therapy, and neuropsychology, runs throughout the prolonged recovery because the cognitive and functional burden outlasts the acute illness. [6]
Timing the immunotherapy ladder
Day 0: Suspect autoimmune encephalitis; secure ABC, treat seizures, send CSF/MRI/EEG and paired antibodies, start empirical aciclovir and antibiotics
Day 0-1: Start first-line immunotherapy once infection is reasonably excluded (methylprednisolone pulse plus IVIG)
Day 0-7: Search for and remove any ovarian teratoma if found
Day 10-14: Assess response; if poor, start second-line rituximab or cyclophosphamide
Weeks to months: Continue rehabilitation, manage dysautonomia and seizures, plan cognitive and school reintegration
Long-term: Relapse surveillance, neuropsychology, and structured school return with gradual immunotherapy taper
Specific Subtypes & Scenarios
Anti-NMDAR encephalitis is the archetype and the commonest paediatric subtype, and it is managed on the full ladder above. The tumour search and removal are central in post-pubertal girls, and the paediatric consensus gives a clear framework for first-line, second-line, and supportive care. [7]
Post-herpes simplex virus autoimmune encephalitis is the scenario examiners love because it is easy to miss. A child recovering from treated HSE relapses weeks later with new neurological or psychiatric features. This is not recurrent infection in most cases but a secondary autoimmune response, usually to NMDAR. The correct response is to repeat the MRI and CSF, to consider a new autoimmune workup, and to start first-line immunotherapy rather than simply prolonging aciclovir. [11]
LGI1 antibody encephalitis presents with the highly characteristic faciobrachial dystonic seizures, brief unilateral arm and face twitches, often with hyponatraemia, and responds well to immunotherapy but poorly to antiseizure drugs alone. GABA-A receptor encephalitis presents with refractory seizures and status epilepticus and often needs aggressive immunotherapy. GABA-B and AMPA receptor encephalitis are more often paraneoplastic in adults. Febrile infection-related epilepsy syndrome and new-onset refractory status epilepticus are refractory status syndromes in which autoimmune and inflammatory mechanisms are suspected and in which early immunotherapy and interleukin-1 blockade with anakinra are increasingly used. Intracellular antigen syndromes are usually paraneoplastic, poorly responsive, and demand a thorough tumour search and an honest early prognosis. [1]
Complications & Pitfalls
The complications of autoimmune encephalitis are both acute and long-term, and the pitfalls cluster around delayed diagnosis and under-treatment. [5]
The life-threatening acute complications are the direct features of the disease. Dysautonomia causes cardiac instability and blood pressure swings, hypoventilation can require weeks of mechanical ventilation, and refractory seizures may need an anaesthetic infusion. Intensive-care complications, including hospital-acquired infection, thrombosis, and critical-illness myopathy, add to the morbidity of a long admission. [5]
The classic pitfalls are the ones examiners reward a candidate for naming. The first is attributing the psychiatric phase to a primary psychiatric disorder and delaying the workup and treatment. The second is waiting for the antibody result before starting immunotherapy. The third is under-treating the first-line course, using a single agent at a low dose. The fourth is failing to search for and remove a tumour. The fifth is mistaking a post-HSE relapse for recurrent infection and prolonging aciclovir instead of starting immunotherapy. Relapse occurs in around twelve to fifteen percent of patients and may follow a premature taper of immunotherapy, so surveillance continues after discharge. [2]
The long-term complications dominate the lived burden of the disease. Cognitive impairment, especially of executive function and memory, psychiatric sequelae including anxiety, depression, and psychosis, residual epilepsy, and persistent movement disorder can outlast the acute illness by months or years. A child who looks recovered motorically may still carry a significant cognitive deficit, which is why formal neuropsychological assessment and a structured school reintegration plan are part of treatment, not an afterthought. [10]
Prognosis & Disposition
Most children with anti-NMDAR encephalitis recover well, but the recovery is long, and the milestones the family needs are the ones worth memorising. Good outcome, defined as a modified Rankin scale of zero to two, is achieved in around seventy-five percent within the first twenty-four months. Relapse occurs in around twelve to fifteen percent of patients. [2]
The predictors of outcome are the levers a clinician actually controls. Early immunotherapy and early second-line therapy within the first four weeks are independent predictors of good outcome. The absence of a need for intensive care and the removal of a tumour when present also favour recovery. Intracellular antigen syndromes carry a worse prognosis and a higher relapse risk, and an honest early conversation about prognosis is part of caring for these families. [2]
Disposition follows the tempo of the illness. Any child with dysautonomia, hypoventilation, a falling level of consciousness, or refractory seizures goes to intensive care. A child on the first-line course with stable physiology is managed on the ward with paediatric neurology input. As the acute phase settles, the child moves to neurorehabilitation, which may be inpatient or community-based, and to paediatric neurology follow-up for relapse surveillance, cognitive and psychiatric assessment, and a structured school reintegration plan. [6]
recovery trajectory
Sustained recovery toward 75% good outcome at 24 months
Special Populations
The post-pubertal girl has the highest chance of an ovarian teratoma and needs pelvic imaging and gynaecology input as part of the first-line workup. Tumour removal can transform the course, so the search is active rather than incidental. [7]
The young child more often presents with seizures, movement disorder, and speech or developmental regression and less often with overt psychiatric features. Because the psychiatric anchor is missing, the diagnosis is delayed, and a low threshold for an EEG and CSF study in a regressing child is essential. The child with an existing neurodisability or established psychiatric diagnosis is at particular risk of being mislabelled as a behavioural decompensation, and any change in the established baseline needs the same workup as a new presentation. [9]
The Aboriginal and Torres Strait Islander child and the child from a remote setting may present late after prolonged untreated symptoms, so retrieval pathways and early specialist input are central, and the threshold to treat on suspicion is even lower. The child from a refugee or migrant family needs an early interpreter and a broad workup that includes infection and nutritional deficiency. The immunocompromised child and the adolescent on an immune checkpoint inhibitor for cancer needs a high suspicion for paraneoplastic and immune-related encephalitis, a thorough tumour search, and early involvement of oncology and neurology. [9]
Evidence, Guidelines & Regional Differences
The diagnostic framework rests on the Graus 2016 clinical approach, which gave the field a usable set of tiers and the specific anti-NMDAR criteria, and on the cell-surface versus intracellular classification that predicts treatment response. [1] The original disease description by Dalmau in 2008 established the antibody mechanism and the reversibility of the receptor loss. [3]
The treatment evidence is dominated by the Titulaer observational cohort of 577 patients, which showed that good outcome is achieved in around seventy-five percent within the first twenty-four months and that early immunotherapy and early second-line therapy are the strongest predictors of good outcome. [2] The international consensus recommendations for paediatric anti-NMDAR encephalitis and the meta-analysis of immunotherapy safety in children translate that evidence into the first-line and second-line ladder used at the bedside. [7][8] The proposed best practice recommendations set out the diagnostic and acute management framework and the long-term symptomatic management. [5][6]
Titulaer 2013 — anti-NMDAR outcome cohort
Observational cohort of 577 patients with anti-NMDAR encephalitis
Key finding
Good outcome (mRS 0-2) in ~75% within first 24 months; relapse in ~12-15%
Practice change
Early immunotherapy and early second-line therapy within the first four weeks are independent predictors of good outcome and define the timing of the ladder.
Controversies remain. The exact timing and choice of second-line therapy, rituximab versus cyclophosphamide, is debated, though rituximab is increasingly favoured in children for its tolerability. The role of early tumour removal in non-paraneoplastic disease, the management of antibody-negative but clinically suspected disease, and the place of immunotherapy and anakinra in febrile infection-related epilepsy syndrome and new-onset refractory status epilepticus are all active areas. [7]
Regional differences are small in principle because the framework is international, but access matters in practice. Rapid antibody testing and rituximab are available promptly in tertiary centres in ANZ, the UK, and North America, but turnaround can stretch to weeks in remote settings, reinforcing the rule to treat on suspicion. The threshold to treat and the choice of second-line agent are broadly consistent across the RACP, RCPCH, ABP, and RCPSC contexts. [9]
Exam Pearls
Anti-NMDAR encephalitis is the commonest paediatric autoimmune encephalitis. The Graus 2016 tiers are possible, probable, and definite. Probable anti-NMDAR needs rapid onset of at least four of the six symptom groups: abnormal behaviour or cognition, speech dysfunction, seizures, movement disorder or abnormal postures, decreased consciousness, and autonomic dysfunction or hypoventilation, plus a CSF or MRI or EEG change, plus exclusion of mimics, plus the antibody or a teratoma. [1]
The CSF shows a lymphocytic pleocytosis and oligoclonal bands. Extreme delta brush is the characteristic EEG pattern but is absent in most children. MRI is normal in roughly half. Send the antibody panel in paired CSF and serum, because CSF is more sensitive for NMDAR and a negative serum does not exclude the disease. [4]
First-line immunotherapy is methylprednisolone 20 to 30 mg per kg per day, maximum 1 g, for three to five days, intravenous immunoglobulin 2 g per kg over two to five days, and plasma exchange for five cycles. Second-line therapy, started at 10 to 14 days for poor response, is rituximab 375 mg per m2 weekly for four doses and or cyclophosphamide 750 mg per m2 monthly. Search for and remove an ovarian teratoma in any post-pubertal girl. [7]
The outcome data worth quoting: good outcome in around seventy-five percent within twenty-four months, early treatment and early second-line therapy as predictors of good outcome, and relapse in around twelve to fifteen percent. Herpes simplex encephalitis triggers a secondary anti-NMDAR response in around twenty percent of survivors. The two rules that save children are to never delay immunotherapy for antibody results, and to remember that cell-surface antibodies respond while intracellular antigens often do not. [2][11]
References
- [1]Graus F, Titulaer MJ, Balu R, et al A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol, 2016.PMID 26906964
- [2]Titulaer MJ, McCracken L, Gabilondo I, et al Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol, 2013.PMID 23290630
- [3]Dalmau J, Gleichman AJ, Hughes EG, et al Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol, 2008.PMID 18851928
- [4]Schmitt SE, Pargeon K, Frechette ES, et al Extreme delta brush: a unique EEG pattern in adults with anti-NMDA receptor encephalitis. Neurology, 2012.PMID 22933737
- [5]Abboud H, Probasco JC, Irani S, et al Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management. J Neurol Neurosurg Psychiatry, 2021.PMID 33649022
- [6]Abboud H, Probasco JC, Irani S, et al Autoimmune encephalitis: proposed recommendations for symptomatic and long-term management. J Neurol Neurosurg Psychiatry, 2021.PMID 33649021
- [7]Nosadini M, Dalmau J, Anastasopoulou S, et al International Consensus Recommendations for the Treatment of Pediatric NMDAR Antibody Encephalitis. Neurol Neuroimmunol Neuroinflamm, 2021.PMID 34301820
- [8]Nosadini M, Lee T, D'Avino E, et al Use and Safety of Immunotherapeutic Management of N-Methyl-d-Aspartate Receptor Antibody Encephalitis: A Meta-analysis. JAMA Neurol, 2021.PMID 34542573
- [9]Olive-Cirera G, Solis-Garcia G, Sola-Valls N, et al Differential diagnosis and comparison of diagnostic algorithms in children and adolescents with autoimmune encephalitis in Spain: a prospective cohort study and retrospective analysis. Lancet Neurol, 2025.PMID 39706634
- [10]Guasp M, Gonzalez-Alegre P, Pujol A, et al Clinical characterisation of patients in the post-acute stage of anti-NMDA receptor encephalitis: a prospective cohort study and comparison with patients with schizophrenia spectrum disorders. Lancet Neurol, 2022.PMID 36115362
- [11]Armangue T, Leypoldt F, Malaga I, et al Herpes simplex virus encephalitis is a trigger of brain autoimmunity. Ann Neurol, 2014.PMID 24318406