Paeds · neurology-neurodisability-and-neuromuscular
Cerebral vascular malformations
Also known as Brain arteriovenous malformation · Vein of Galen aneurysmal malformation · Cerebral cavernous malformation · Cavernoma · Intracranial vascular malformation
Fellowship guide to cerebral vascular malformations in children. Covers the classification into high-flow arteriovenous malformation, vein of Galen aneurysmal malformation, low-flow cavernous malformation, and the developmental venous anomaly, the epidemiology with haemorrhage as the dominant paediatric presentation, the pathophysiology of the arteriovenous shunt versus thin-walled caverns versus the midline venous sac, the clinical presentation from a sudden intracerebral haemorrhage in the older child to neonatal high-output cardiac failure, the urgent MRI with MRA and MRV imaging pathway, the Bicetre neonatal evaluation score for vein of Galen, the Spetzler-Martin grade for arteriovenous malformation, the management of multidisciplinary treatment with microsurgery, embolisation and stereotactic radiosurgery, the transarterial embolisation of vein of Galen malformation, the surgical resection of symptomatic cavernoma, the familial CCM gene, and the long-term angiographic follow-up.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A cerebral vascular malformation is a developmental error of the intracranial blood vessels, and the four lesions the fellow must hold in mind are the high-flow arteriovenous malformation, the vein of Galen aneurysmal malformation, the low-flow cavernous malformation, and the developmental venous anomaly. The first principle is that these are not tumours and they are not strokes, but they cause both, because the high-flow lesions bleed and the low-flow lesions seize. The second principle is that the presentation tracks the flow: a high-flow arteriovenous malformation bleeds, a vein of Galen malformation fails the neonatal heart, and a cavernous malformation seizes or oozes. [1][2]
The dominant paediatric presentation is haemorrhage. Boulouis and colleagues showed that vascular malformations are a leading cause of nontraumatic intracerebral haemorrhage in children, which is why a sudden severe headache or a new focal deficit in a previously well child is a bleed until imaging proves otherwise. The incidence of a brain arteriovenous malformation in children is about one per one hundred thousand per year, and roughly half of these present with a haemorrhage. The vein of Galen malformation is rare but distinctive, because it presents in the neonate with high-output cardiac failure rather than with a stroke. [9][2]
Three threads run through this topic and structure the exam answer. The diagnosis is an imaging diagnosis, and the urgent scan is an MRI brain with MRA and MRV, with a catheter angiogram reserved for confirmation and treatment planning. The management is multidisciplinary and lesion-specific, with the high-flow lesions treated by a neurovascular team using surgery, embolisation, or radiosurgery, the vein of Galen by transarterial embolisation, and the cavernoma by surgical resection when it is symptomatic. And the long game is follow-up, because the paediatric arteriovenous malformation recurs and the cavernoma re-bleeds. Karim and colleagues set out the modern imaging and treatment framework that governs paediatric practice. [1]
Classification
Cerebral vascular malformations classify along two axes, and both axes matter at the bedside because they direct the imaging and the treatment. The first axis is the flow: the arteriovenous malformation and the vein of Galen malformation are high-flow lesions with a direct artery-to-vein connection, and the cavernous malformation is a low-flow lesion with no arterial input. The second axis is the structure: the arteriovenous malformation is a tangle called a nidus, the vein of Galen malformation is a dilated midline venous sac, and the cavernous malformation is a cluster of thin-walled blood cavities. The developmental venous anomaly sits apart, because it is a normal drainage pattern and not a true malformation. [1][2]
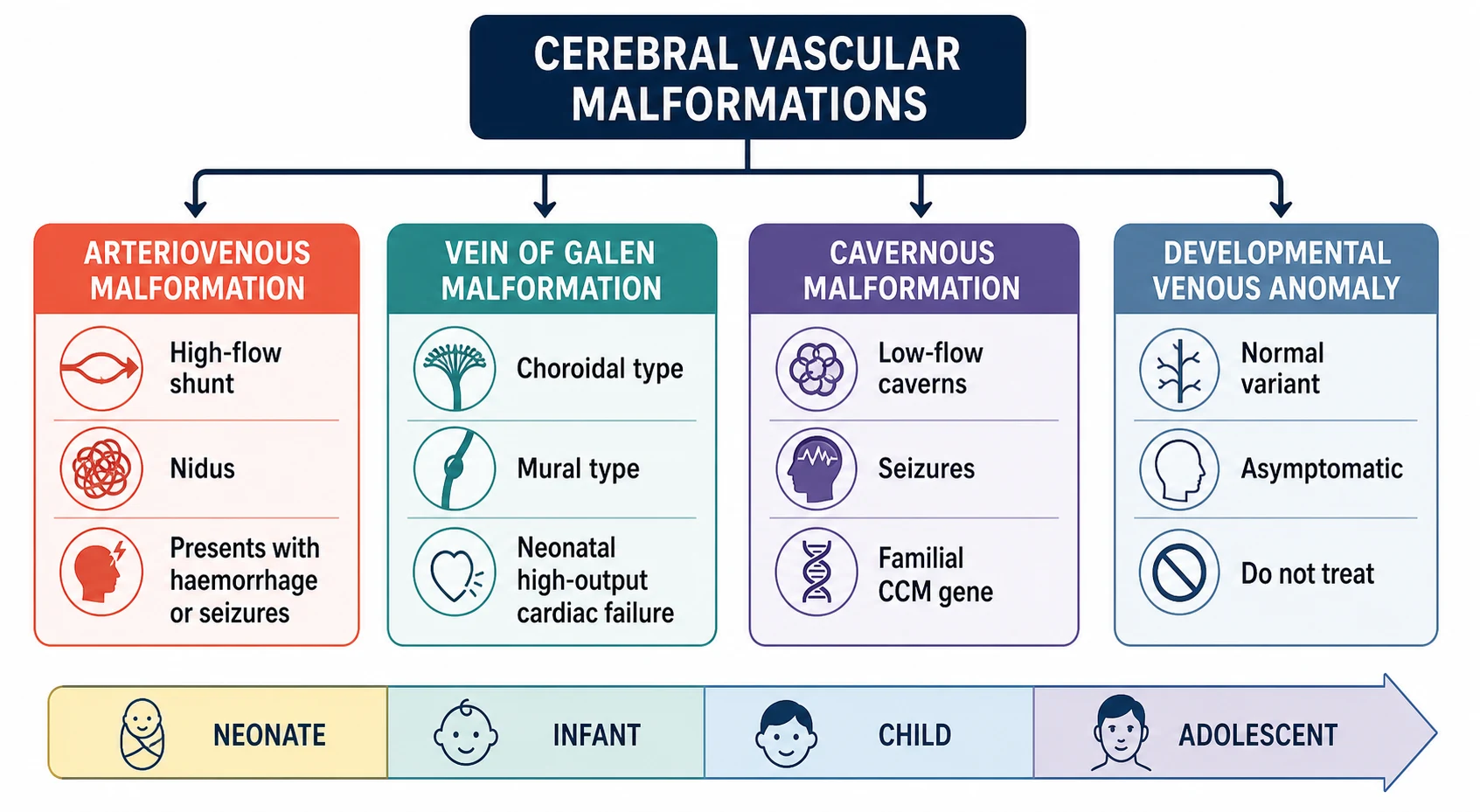
The arteriovenous malformation splits by angioarchitecture into a nidus type, a fistulous type, and a mixed type, and the fellow should know that the paediatric lesion is more often fistulous than the adult lesion. The vein of Galen malformation splits into the choroidal type, which is a complex network of choroidal arteries draining into the median prosencephalic vein, and the mural type, which is a simpler direct fistula into the wall of the venous sac, and the mural type carries the better prognosis. The cavernous malformation splits into the sporadic form, which is usually a single lesion, and the familial form, which carries multiple lesions and a CCM gene mutation. [3][4][7]
Epidemiology & Risk Factors
Brain arteriovenous malformations are the commonest cerebral vascular malformation to present in childhood, and the incidence is about one per one hundred thousand children per year. Roughly half of paediatric arteriovenous malformations present with a haemorrhage, and the annual bleeding risk of an unruptured lesion is around two to four percent, which is higher than the adult figure. Boys are affected slightly more often than girls, and the presentation peaks in the school-age and adolescent years, when the lesion has had time to declare itself by bleeding or seizing. [2][9]
The vein of Galen malformation is rare, accounting for less than one percent of all cerebral vascular malformations, but it is the commonest extracardiac cause of high-output cardiac failure in the newborn. It is a congenital lesion that develops in the first trimester, and the severity of the presentation is driven by the size of the shunt and the maturity of the cardiopulmonary circulation. Alvarez and colleagues established the modern understanding of the lesion, and the fellow should know that the choroidal type is more severe than the mural type. [4][5]
The cavernous malformation is the second commonest lesion to present in childhood after the arteriovenous malformation, and the familial form is concentrated in Hispanic populations through the founder mutation in the CCM1 gene. The risk factors for haemorrhage from any malformation are the deep or brainstem location, the small nidus size, and a prior bleed, and the fellow should be able to list these because they drive the decision to treat. Smith and Scott set out the cavernous malformation framework, and the familial form demands family screening once the index case is confirmed. [12][7]
Pathophysiology
The arteriovenous malformation is a congenital tangle of thin-walled arteries and veins connected through a nidus with no capillary bed, and the high-pressure arterial blood is delivered directly into the thin-walled veins. The veins are not built for arterial pressure, and over time they weaken and rupture, which is the mechanism of the intracerebral haemorrhage that dominates the paediatric presentation. The shunt also steals blood from the surrounding brain, which can produce a focal deficit or a seizure even before the lesion bleeds. [2]
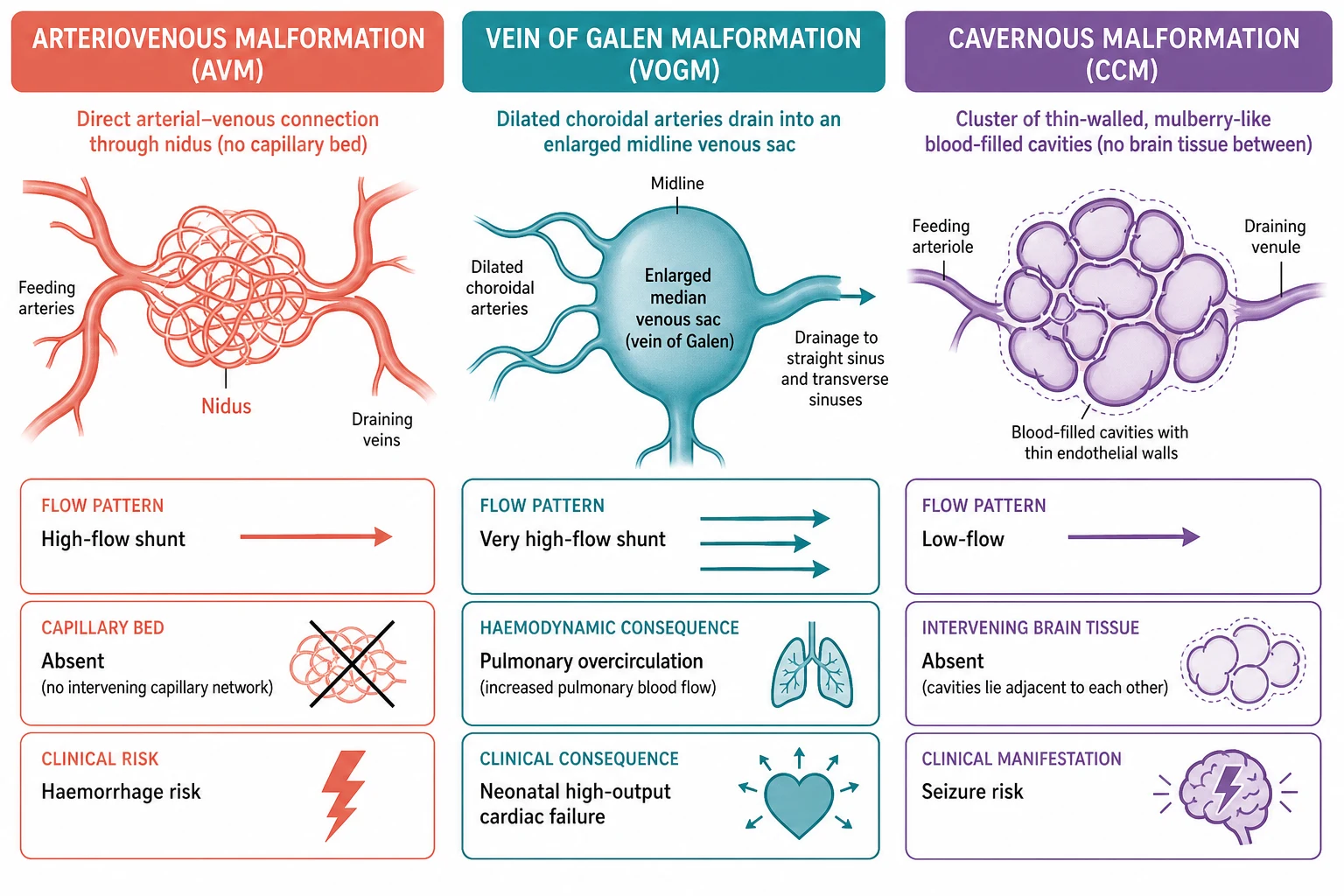
The vein of Galen malformation is a congenital arteriovenous fistula between the choroidal arteries and the median prosencephalic vein, which is the embryonic precursor of the vein of Galen. The high-flow shunt returns a large volume of blood to the heart, and in the neonate, whose myocardium and pulmonary vascular bed are immature, this volume overload produces severe high-output cardiac failure with pulmonary hypertension. The shunt also raises the pressure in the cerebral venous system, which impairs the absorption of cerebrospinal fluid and produces an obstructive pattern of hydrocephalus and a loss of brain tissue from venous congestion. Cory and colleagues rationalised the medical management of the neonatal heart failure, and the fellow should know that the cardiac failure is a consequence of the shunt volume, not of an intrinsic cardiac lesion. [5][3]
The cavernous malformation is a cluster of thin-walled endothelial-lined blood cavities with no intervening neural tissue, and the cavities leak small amounts of blood into the surrounding brain over time. The leaked blood and the surrounding haemosiderin ring irritate the cortex, which is the mechanism of the epilepsy that dominates the cavernous malformation presentation. A larger rupture produces a focal haematoma, and because the malformation is low-flow the bleed is usually less catastrophic than the arteriovenous malformation bleed, though a brainstem cavernoma can still be devastating. The familial form carries multiple lesions, and the CCM1, CCM2, and CCM3 gene mutations produce a loss of the endothelial junction integrity that allows the cavities to form and to grow. [12][7]
Clinical Presentation
The arteriovenous malformation in the older child presents with a sudden intracerebral haemorrhage, and the onset is the abrupt severe headache, the vomiting, the focal deficit, and the depressed consciousness of any expanding intracranial mass. The deficit reflects the location, with a hemiparesis from a motor-cortex lesion, a visual field loss from an occipital lesion, and an ataxia from a posterior-fossa lesion. Seizures are the second commonest presentation, and the seizure may be the first sign in a child who has not yet bled. Prablek and colleagues showed that arteriovenous malformation-associated epilepsy in children is driven by the location, the haemorrhage, and the cortical irritation. [10][9]
How cerebral vascular malformations present across the age spectrum
A fetus with an enlarged cerebral venous sac and cardiomegaly on the mid-trimester ultrasound, raising a vein of Galen malformation
A neonate in the first days of life with severe high-output cardiac failure, a loud cranial bruit, and cerebral venous congestion, the classic vein of Galen presentation
An infant or toddler with an enlarging head and developmental delay from the hydrocephalus of an untreated vein of Galen malformation
A school-age child with a sudden severe headache, vomiting, and a hemiparesis from a ruptured arteriovenous malformation
An adolescent with new focal epilepsy or an episodic severe headache from an unruptured arteriovenous or cavernous malformation
The vein of Galen malformation presents in the neonate with severe high-output cardiac failure, and the signs are tachypnoea, tachycardia, hepatomegaly, a gallop rhythm, and pulmonary oedema. A loud cranial bruit over the vertex is the bedside clue that the heart failure is driven by an intracranial shunt and not by an intrinsic cardiac lesion, and the neonate may also have prominent cerebral veins over the scalp and macrocephaly from the hydrocephalus. In the older infant the cardiac failure is less prominent, and the presentation shifts to developmental delay, an enlarging head, and seizures from the venous congestion. The choroidal type tends to present in the neonate, and the mural type tends to present later in infancy. [4][5]
The cavernous malformation presents with epilepsy in about half of children and with a haemorrhage in a substantial minority, and the presentation is shaped by the location. A supratentorial cavernoma presents with a focal seizure or a progressive deficit, and a brainstem cavernoma presents with a cranial nerve palsy or an ataxia from a small focal bleed. Because the bleed is low-flow, the cavernous malformation can present subtly, and the diagnosis is often made on an MRI performed for a seizure rather than for an acute collapse. Paddock and colleagues set out the paediatric cavernous malformation framework, and the fellow should know that a child with multiple lesions on the scan has the familial form until a gene test proves otherwise. [7][12]
Differential Diagnosis
The differential of a sudden intracerebral haemorrhage in a child separates the vascular malformation from the other causes of a paediatric bleed, and the separation rests on the imaging. The leading causes of a nontraumatic paediatric intracerebral haemorrhage are the arteriovenous malformation, the cavernous malformation, the aneurysm, the bleeding diathesis, and the tumour, and the imaging distinguishes them. Boulouis and colleagues established that vascular malformations are the dominant cause in the previously well child. [9]
Arteriovenous malformation
high-flow, bleeds
- Sudden haemorrhage with a tangle of vessels on MRA
- Roughly half of paediatric malformations present this way
- Confirmed by catheter angiography showing the nidus
- Treated by the multidisciplinary neurovascular team
Vein of Galen malformation
neonatal heart failure
- Neonate with high-output cardiac failure and a cranial bruit
- Enlarged midline venous sac on the MRV or ultrasound
- Treated by transarterial embolisation when the score allows
- Bicetre neonatal evaluation score guides the timing
Cavernous malformation
low-flow, seizes
- Seizures or a small focal haemorrhage
- Popcorn lesion with a haemosiderin ring on MRI
- Treated by surgical resection when symptomatic
- Familial form has multiple lesions and a CCM gene mutation
Developmental venous anomaly
do not treat
- Incidental finding on an MRI performed for another reason
- A medusa-head of draining veins with normal brain between
- Drains normal brain, so resection causes a venous infarct
- Leave alone and reassure the family
The aneurysm is a saccular outpouching of an arterial wall and is rarer in children than in adults, and the bleed is typically into the subarachnoid space rather than the parenchyma. The bleeding diathesis, whether from a coagulopathy, a leukaemia, or an anticoagulant, produces a bleed that is explained by the blood test, and the malformation is absent on the imaging. The tumour, particularly a high-grade glioma or a medulloblastoma, can bleed into its own substance, and the surrounding mass and the enhancement pattern on the MRI separate it from a malformation. When genuine doubt exists, the child is managed as a malformation and the catheter angiogram settles the question. [9][2]
Clinical & Bedside Assessment
The bedside assessment of a child with a suspected vascular malformation is a structured emergency that runs in parallel with the imaging request. The first move is to assess and support the airway, breathing, and circulation, because the child with a large haemorrhage or a failing neonatal heart can deteriorate quickly. The bedside glucose is checked in every child with a focal deficit or a seizure, and the time of onset is established, because these facts gate the imaging and the retrieval. [9][1]
The focused examination localises the lesion and seeks the cause. A hemiparesis points to a motor-cortex or internal-capsule lesion, a visual field defect points to an occipital lesion, and a cranial nerve palsy points to a brainstem or posterior-fossa lesion. The neonate with a suspected vein of Galen malformation is examined for the cardiac signs of high-output failure, including the hepatomegaly, the gallop, the pulmonary oedema, and the loud cranial bruit. The general examination seeks the cutaneous stigmata of a syndromic association, including a port-wine stain of Sturge-Weber, though the vascular malformations covered here are typically isolated. [4][5]
The history taken in parallel focuses on the family and the development. A family history of early stroke, haemorrhage, or a known cavernous malformation raises the familial form and triggers the genetic counselling. A developmental history that is delayed in an infant with an enlarging head raises an untreated vein of Galen malformation that has caused a chronic venous congestion. The medication history includes the antiepileptic drugs in a child presenting with a first seizure, and the retrieval is arranged early, because the definitive treatment is concentrated in a small number of paediatric neurosciences centres. [7][1]
Investigations
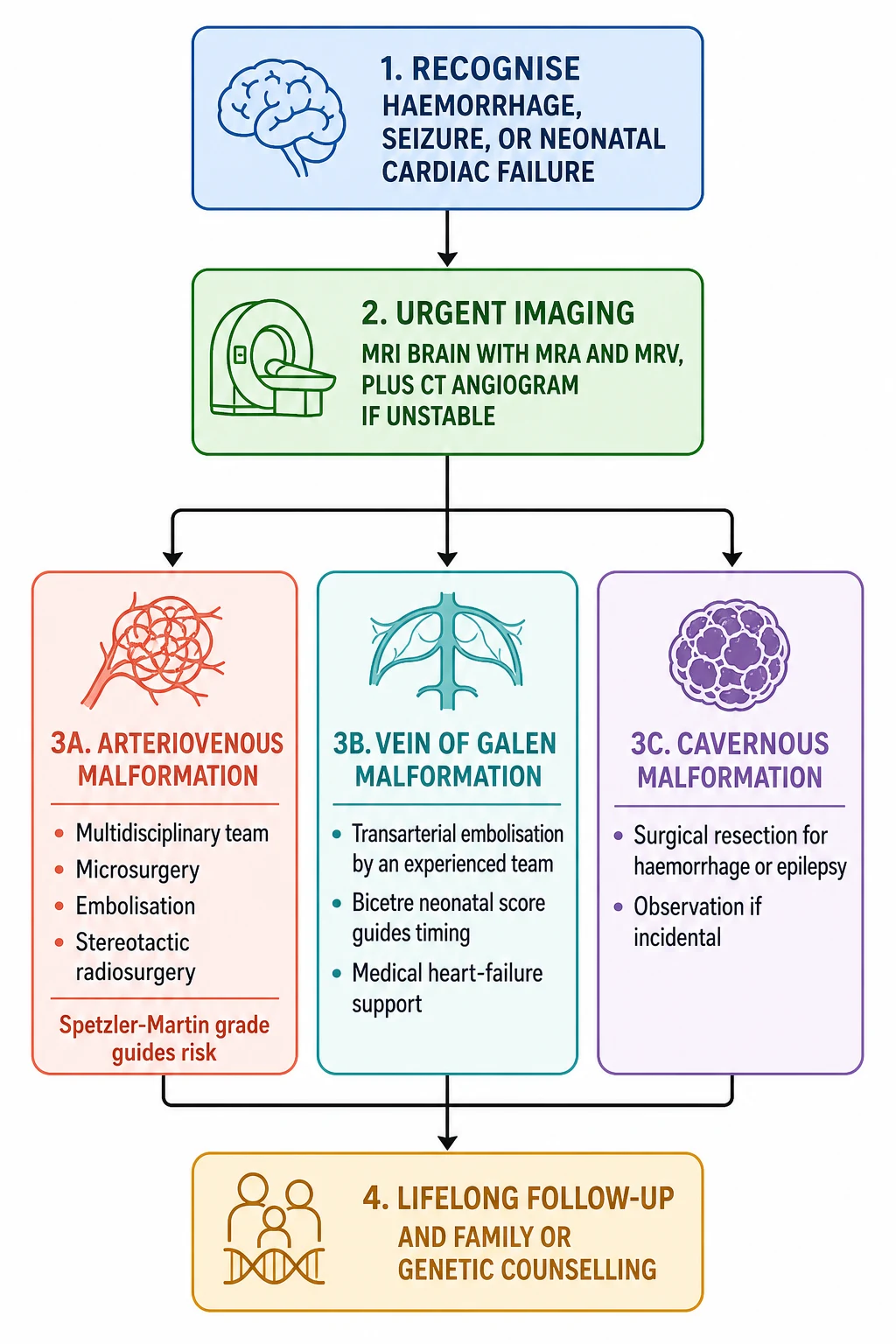
The investigation rests on urgent cross-sectional imaging, and the standard is an MRI brain with MRA and MRV. The MRI shows the lesion and the surrounding brain, the MRA shows the arterial supply of a high-flow lesion, and the MRV shows the venous drainage and the enlarged midline sac of a vein of Galen malformation. A computed tomography is the fallback when the child is unstable, and a CT angiogram can confirm the high-flow lesion quickly when the MRI is unavailable. The catheter angiogram remains the gold standard for the confirmation of an arteriovenous malformation and the planning of its treatment, because it resolves the nidus and the draining veins that the cross-sectional imaging may miss. [1][2]
The cavernous malformation has a distinctive MRI appearance, and the fellow should know it because it is a high-yield exam fact. The lesion is a popcorn-like mixed-signal mass on the T1 and T2 sequences with a complete low-signal haemosiderin ring on the gradient-echo or susceptibility-weighted sequences, and the angiogram is typically normal because the lesion is low-flow. The vein of Galen malformation is seen on the fetal or neonatal ultrasound as an enlarged midline cystic structure with prominent feeding vessels, and the MRI confirms the enlarged median prosencephalic vein and the arterial feeders. The developmental venous anomaly shows the classic medusa-head of draining veins on the contrast MRI, and it is critical to recognise and to leave alone. [1][7]
Imaging pathway for a suspected paediatric cerebral vascular malformation
Dose
MRI brain with MRA and MRV as the first-line standard
The cause search is limited in the sporadic malformation, because most lesions are isolated and developmental. The familial cavernous malformation is the exception, and a child with multiple lesions or a positive family history is offered a genetic test for the CCM1, CCM2, and CCM3 genes, and the family is counselled once the mutation is confirmed. The electroencephalography is performed in the child who presents with a seizure, and it helps to localise the epileptogenic cortex around a cavernous malformation. The echocardiogram is performed in the neonate with a suspected vein of Galen malformation, because it confirms that the cardiac failure is driven by the intracranial shunt and assesses the cardiac function before the embolisation. [7][5]
Management — Resuscitation
The resuscitation of a child with a suspected vascular malformation follows the airway, breathing, and circulation framework, and the priority is to keep the brain perfused while the imaging and the retrieval proceed. The airway is secured in the child with a depressed consciousness, and the ventilation is adjusted to maintain a normal carbon dioxide, because both hypoventilation and hyperventilation shift the cerebral blood flow. The circulation is supported with isotonic fluids and, in the child with a large haemorrhage, with a cautious transfusion to maintain the haemoglobin without raising the blood pressure excessively. [9]
The neonate with a vein of Galen malformation and high-output cardiac failure is a special resuscitation, and the priority is to support the failing heart while the transfer to a paediatric interventional neuroradiology centre is arranged. The medical management combines the ventilation, the diuretics such as furosemide to reduce the volume overload, the inotropes to support the cardiac output, and the careful management of the pulmonary hypertension, because a profound acidosis or a multi-organ failure from the steal phenomenon is the mode of death. Cory and colleagues rationalised this approach, and the principle is that the medical therapy buys time for the definitive embolisation, which is the only treatment that addresses the shunt. [5]
The child with a haemorrhage from an arteriovenous malformation or a cavernous malformation is managed for the raised intracranial pressure, and the neurosurgical team is involved early. A haematoma that is large and compressing the brainstem is evacuated, and the malformation itself is treated after the child has stabilised, because the urgent operation is the decompression and not the cure. The seizures are treated with standard anticonvulsants, and the child is kept nil by mouth until the swallow is assessed. The retrieval to the paediatric neurosciences centre is arranged with a team that can manage the airway and the haemodynamics, because the journey is part of the treatment. [9][1]
Management — Definitive & Stepwise
The definitive management of a brain arteriovenous malformation is multidisciplinary, and the team is made up of the paediatric neurologist, the neurosurgeon, the interventional neuroradiologist, and the radiation oncologist. The choice between microsurgery, embolisation, and stereotactic radiosurgery depends on the size, the location, the deep or superficial drainage, and the eloquence of the surrounding brain, and these features are captured by the Spetzler-Martin grade. A small superficial lesion in non-eloquent brain is a low-grade lesion and is treated by microsurgery, and a large deep lesion in eloquent brain is a high-grade lesion that may be observed rather than treated, because the procedural risk exceeds the natural history. [2][11]
[2] [1]Embolisation is the transarterial injection of a glue or a coil into the nidus or the feeding artery, and it is used to cure a small lesion or to reduce a large lesion before the surgery or the radiosurgery. Stereotactic radiosurgery delivers a focused radiation dose to the nidus, and it obliterates the lesion over two to three years, which is the drawback in a child because the lesion remains at risk of bleeding during that latent period. Hak and colleagues showed in their meta-analysis that the paediatric arteriovenous malformation recurs in up to eight percent of children after an apparent cure, which is higher than the adult figure, and this drives the mandatory post-treatment angiogram and the years of imaging follow-up. [11][2]
The definitive management of a vein of Galen malformation is transarterial embolisation, and the procedure is performed by an experienced paediatric interventional neuroradiology team. The embolisation closes the fistula with a glue or a coil, and it is staged over several sessions to avoid the haemodynamic shift that a single large occlusion can produce. Lasjaunias and colleagues set out the modern management framework, and the timing is guided by the Bicetre neonatal evaluation score, which combines the cardiac, the cerebral, the respiratory, the hepatic, and the renal function into a score that ranges from zero to twenty-one. A high score allows the neonatal embolisation, and a low score mandates the medical stabilisation and the delay to around five to six months. Orbach and colleagues reported the first in-utero embolisation for a fetal vein of Galen malformation, which opened a new frontier for the most severe cases. [3][6]
The definitive management of a cavernous malformation is surgical resection, and the indication is the symptomatic lesion that has bled or that causes a drug-resistant epilepsy. A supratentorial cavernoma in a non-eloquent area is resected with a low morbidity, and a brainstem cavernoma is resected only by an experienced team when it has bled and reaches a pial surface, because the procedural risk in the brainstem is high. An incidental cavernous malformation that has not bled and does not seize is observed, because the natural history is benign and the surgical risk is not justified. Rauschenbach and colleagues showed that the functional outcome after the paediatric cavernous malformation surgery is good in the majority, which supports the surgical approach for the symptomatic lesion. [8][12]
Specific Subtypes & Scenarios
The Spetzler-Martin grade is the anchor of the arteriovenous malformation management, and the fellow should be able to assign it at the bedside. The grade sums three features: the size, with one point for a nidus under three centimetres, two for three to six centimetres, and three for over six centimetres; the eloquence of the surrounding brain, with zero for non-eloquent and one for eloquent; and the venous drainage, with zero for superficial and one for deep. The total ranges from one to five, and the grade one and two lesions are generally surgical, while the grade four and five lesions are generally observed because the procedural risk exceeds the natural history. [2][11]
Spetzler-Martin grade of a brain arteriovenous malformation
Grade III
Medium or deep in non-eloquent brain — Moderate risk, multimodal treatment
The vein of Galen malformation with the choroidal angioarchitecture is the severe form, because the complex network of choroidal feeders produces a large shunt volume that overwhelms the neonatal heart. The mural type is the simpler form, with a direct fistula into the wall of the venous sac, and it carries a smaller shunt and a better prognosis. The neonate with the choroidal type often presents in the first days of life with the severe cardiac failure, and the infant with the mural type often presents later with the hydrocephalus and the developmental delay. The Bicetre neonatal evaluation score guides the timing of the embolisation across this spectrum. [4][3]
The familial cavernous malformation is the third high-yield subtype, and the fellow should know it because it changes the counselling. The familial form is autosomal dominant and is driven by the CCM1, CCM2, and CCM3 genes, and the CCM3 mutation carries a higher haemorrhage risk and a higher risk in childhood. The child presents with multiple lesions on the MRI, and the family history is positive for early haemorrhage or known cavernous malformation. The genetic test confirms the mutation, and the first-degree relatives are offered the screening, because a known carrier is followed with the serial MRI rather than waiting for a bleed. [7][12]
Complications & Pitfalls
The acute complications of a paediatric vascular malformation are driven by the haemorrhage or the cardiac failure, and the long-term complications are driven by the recurrence and the re-bleed. The acute haemorrhage from an arteriovenous malformation produces the raised intracranial pressure, the focal deficit, and the seizures, and a large posterior-fossa bleed can compress the brainstem and kill the child. The acute cardiac failure from a vein of Galen malformation produces the multi-organ failure from the steal phenomenon, and the pulmonary hypertension is the mode of death in the untreated neonate. [9][5]
The long-term complication of the treated arteriovenous malformation is the recurrence, and Hak and colleagues showed that the recurrence rate in children reaches up to eight percent after an apparent cure. The recurrence is driven by the residual nidus that is below the resolution of the angiogram and that grows in the developing brain, and it is the reason every child receives a post-treatment angiogram and years of imaging follow-up. The long-term complication of the cavernous malformation is the re-bleed, and the brainstem cavernoma carries a re-bleed rate that is several times higher than the supratentorial lesion, which supports the surgical resection once it has declared itself. [11][7]
The classic pitfalls are diagnostic and therapeutic. The diagnostic pitfall is attributing a sudden headache in a child to a migraine or a minor fall, and missing the haemorrhage and the underlying malformation. The second is failing to recognise the neonatal high-output cardiac failure as a vein of Galen malformation, and treating it as an intrinsic cardiac lesion while the intracranial shunt runs on. The therapeutic pitfalls are resecting a developmental venous anomaly, which drains normal brain and whose removal causes a venous infarct, and embolising a sick neonate with a low Bicetre score, which can be fatal on the table. The follow-up pitfall is discharging a treated arteriovenous malformation without the post-treatment angiogram and the years of imaging, because the recurrence is silent until it bleeds. [1][3][11]
Prognosis & Disposition
The prognosis of a paediatric arteriovenous malformation is shaped by whether it has bled and whether it has been cured. A low-grade lesion that is completely resected carries a good prognosis, with a low recurrence and a return to the normal function in most children. A high-grade lesion that is observed carries an ongoing annual bleed risk, and the counselling balances this against the procedural risk. The overall mortality of a paediatric arteriovenous malformation is low in the modern era, but the morbidity of a haemorrhage, with its hemiparesis, its epilepsy, and its cognitive effects, is substantial and drives the early and the complete treatment. [2][9]
The prognosis of a vein of Galen malformation is shaped by the severity of the shunt and the timing of the embolisation. The neonatal mortality of the severe choroidal type reaches up to a third in some series, and the survivors carry a burden of developmental delay, epilepsy, and cognitive impairment from the cerebral venous congestion and the steal. The mural type carries a better prognosis, and the staged embolisation in the older infant allows the normal development in a substantial proportion. The long-term follow-up is mandatory, because the persistent hydrocephalus and the residual shunt can declare themselves years after the initial treatment. [3][4]
The prognosis of a cavernous malformation is shaped by the location and the bleeding behaviour. A supratentorial cavernoma that is resected after a seizure or a bleed carries a good functional outcome in the majority, and the epilepsy is often cured by the resection. A brainstem cavernoma carries a higher procedural risk and a higher re-bleed rate, and the decision to operate is individualised. The familial form carries the ongoing risk of a new bleed from a new lesion, and the serial MRI is the surveillance. The disposition for all three lesions is to a paediatric neurosciences centre, because the treatment and the follow-up are concentrated there. [8][12]
Special Populations
The neonate with a vein of Galen malformation is the population that defines the urgency of the topic, because the cardiac failure can be fatal in the first days of life. The retrieval to a paediatric interventional neuroradiology centre is arranged early, and the medical heart failure therapy is optimised in the referring unit while the transfer proceeds. The family is counselled in honest terms about the severity of the lesion and the staged nature of the treatment, and the long-term developmental follow-up is built into the plan from the outset. [5][3]
The child with the familial cavernous malformation is the population that defines the genetic counselling, because the autosomal dominant transmission means the first-degree relatives are at risk. The genetic test confirms the mutation, and the screening of the parents and the siblings is offered, because a known carrier is followed with the serial MRI. The child with multiple lesions is counselled about the ongoing risk of a new bleed and the need for the long-term surveillance, and the transition to the adult neurology service is planned as the child grows. [7][12]
The child from a remote or a refugee family is the population for whom the access shapes the outcome, because the definitive treatment is concentrated in a small number of paediatric neurosciences centres. The longer time to the presentation, the language barrier, and the distance to the centre all conspire to delay the diagnosis and to narrow the treatment window. The retrieval pathway and the interpreter are part of the acute care, and the engagement with the family and the local health service is part of the long-term follow-up, because the adherence to the serial imaging is the key to catching the silent recurrence. [1][9]
The pregnant adolescent with a known arteriovenous malformation is the population that raises the counselling about the pregnancy and the delivery, because the haemodynamic changes of the pregnancy can increase the bleed risk. The neurovascular team is involved in the antenatal planning, and the mode and the timing of the delivery are individualised. The transition to the adult neurovascular service is planned as the adolescent leaves the paediatric system, because the lifelong follow-up continues. [2][11]
Evidence, Guidelines & Regional Differences
The guideline evidence for paediatric cerebral vascular malformations is drawn from the major centre series and the systematic reviews rather than from a single paediatric guideline, because the rarity of the lesions has limited the randomised trial evidence. The management framework reported by Lasjaunias and colleagues for the vein of Galen malformation, with the Bicetre neonatal evaluation score and the staged transarterial embolisation, remains the standard that governs the practice worldwide. The Morshed and colleagues review of the high-flow vascular malformations in children sets out the arteriovenous malformation framework, and the Karim and colleagues review of the intracranial vascular malformations in children integrates the imaging and the treatment across the spectrum. [3][2][1]
Vein of Galen management
Lasjaunias, Bicetre
- Bicetre neonatal evaluation score guides the timing
- Transarterial embolisation by an experienced team
- Medical heart failure therapy supports the neonate
- In-utero embolisation for the most severe fetal cases
Arteriovenous malformation management
multidisciplinary
- Spetzler-Martin grade guides the treatment choice
- Microsurgery, embolisation, or stereotactic radiosurgery
- Post-treatment angiogram and years of imaging follow-up
- Recurrence rate in children higher than in adults
Cavernous malformation management
surgical when symptomatic
- Surgical resection for haemorrhage or drug-resistant epilepsy
- Observation for the incidental lesion
- Familial form needs a CCM gene test and family screening
- Serial MRI for the multiple-lesion familial form
The recurrence evidence rests on the meta-analysis of Hak and colleagues, which showed that the paediatric arteriovenous malformation recurs in up to eight percent of children after an apparent cure, and which set the standard for the mandatory post-treatment angiogram and the years of imaging follow-up. The neonatal heart failure evidence rests on the work of Cory and colleagues, which rationalised the medical management of the vein of Galen malformation in the neonate. The in-utero frontier rests on the report of Orbach and colleagues, which described the first in-utero embolisation for a fetal vein of Galen malformation and opened a new option for the most severe cases. [11][5][6]
The regional differences are small and centre on the concentration of the expertise. The treatment of a paediatric vascular malformation is performed in a small number of paediatric neurosciences centres in Australia and New Zealand, in the United Kingdom, and in North America, and the retrieval pathway is part of the standard care. The Bicetre neonatal evaluation score and the Spetzler-Martin grade are used worldwide, and the staging of the vein of Galen embolisation follows the Lasjaunias framework across the regions. The long-term follow-up is the consistent principle, because the paediatric malformation recurs and the re-bleed is the silent threat. [1][3][11]
Exam Pearls
The four malformations and what to do with them
References
- [1]Karim S, Jain S, Martinez ML, et al Intracranial Vascular Malformations in Children. Neuroimaging Clin N Am, 2024.PMID 39461764
- [2]Morshed RA, Winkler EA, Kim H, et al High-Flow Vascular Malformations in Children. Semin Neurol, 2020.PMID 32252098
- [3]Lasjaunias PL, Chng SM, Sachet M, et al The management of vein of Galen aneurysmal malformations. Neurosurgery, 2006.PMID 17053602
- [4]Alvarez H, Garcia Monaco R, Rodesch G, et al Vein of galen aneurysmal malformations. Neuroimaging Clin N Am, 2007.PMID 17645970
- [5]Cory MJ, Durand P, Sillero R, et al Vein of Galen aneurysmal malformation: rationalizing medical management of neonatal heart failure. Pediatr Res, 2023.PMID 35422084
- [6]Orbach DB, Shamshirsaz AA, Wilkins-Haug L, et al In Utero Embolization for Fetal Vein of Galen Malformation. JAMA, 2025.PMID 40788723
- [7]Paddock M, Lanham S, Gill K, et al Pediatric Cerebral Cavernous Malformations. Pediatr Neurol, 2021.PMID 33494000
- [8]Rauschenbach L, Santos AN, Dinger TF, et al Functional outcome after pediatric cerebral cavernous malformation surgery. Sci Rep, 2023.PMID 36759693
- [9]Boulouis G, Blauwblomme T, Hak JF, et al Nontraumatic Pediatric Intracerebral Hemorrhage. Stroke, 2019.PMID 31637968
- [10]Prablek M, LoPresti MA, Du R, et al Arteriovenous Malformations-Associated Epilepsy in Pediatrics. Childs Nerv Syst, 2021.PMID 33895871
- [11]Hak JF, Boulouis G, Kerleroux B, et al Pediatric brain arteriovenous malformation recurrence: a cohort study, systematic review and meta-analysis. J Neurointerv Surg, 2022.PMID 34583986
- [12]Smith ER, Scott RM Cavernous malformations. Neurosurg Clin N Am, 2010.PMID 20561497