Paeds · neurology-neurodisability-and-neuromuscular
Concussion and mild traumatic brain injury
Also known as Sport-related concussion · Mild traumatic brain injury · Cerebral concussion · Minor head injury · Post-concussion syndrome
Fellowship guide to concussion and mild traumatic brain injury in children and adolescents. Covers the consensus definition of concussion as a traumatically induced functional brain injury with rapid-onset short-lived impairment, the distinction from moderate and severe traumatic brain injury by a Glasgow Coma Scale of 13 to 15, the PECARN and CATCH clinical decision rules that safely reduce computed tomography in minor head injury, the Amsterdam 2022 consensus pathway of 24 to 48 hours of relative rest followed by graduated return to learn before return to sport, the Child SCAT5 and Child SCAT6 multimodal assessment, the natural recovery trajectory with most children symptom-free within four weeks, the predictors of persistent post-concussion symptoms, and the active rehabilitation of the child whose symptoms do not resolve.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who bumps the head on the playground, takes a knock in a football match, or falls off a bike is the everyday face of concussion. Concussion is a traumatically induced disturbance of brain function, and the job of the clinician is to recognise it, to rule out the structural brain injury that it is not, and to guide the child safely back to school and sport. The Amsterdam consensus, the product of the sixth International Conference on Concussion in Sport, defines concussion as a traumatic brain injury caused by a direct or indirect force to the head that produces a rapid onset of short-lived neurological impairment that resolves spontaneously, with no abnormality on standard structural neuroimaging. [5]
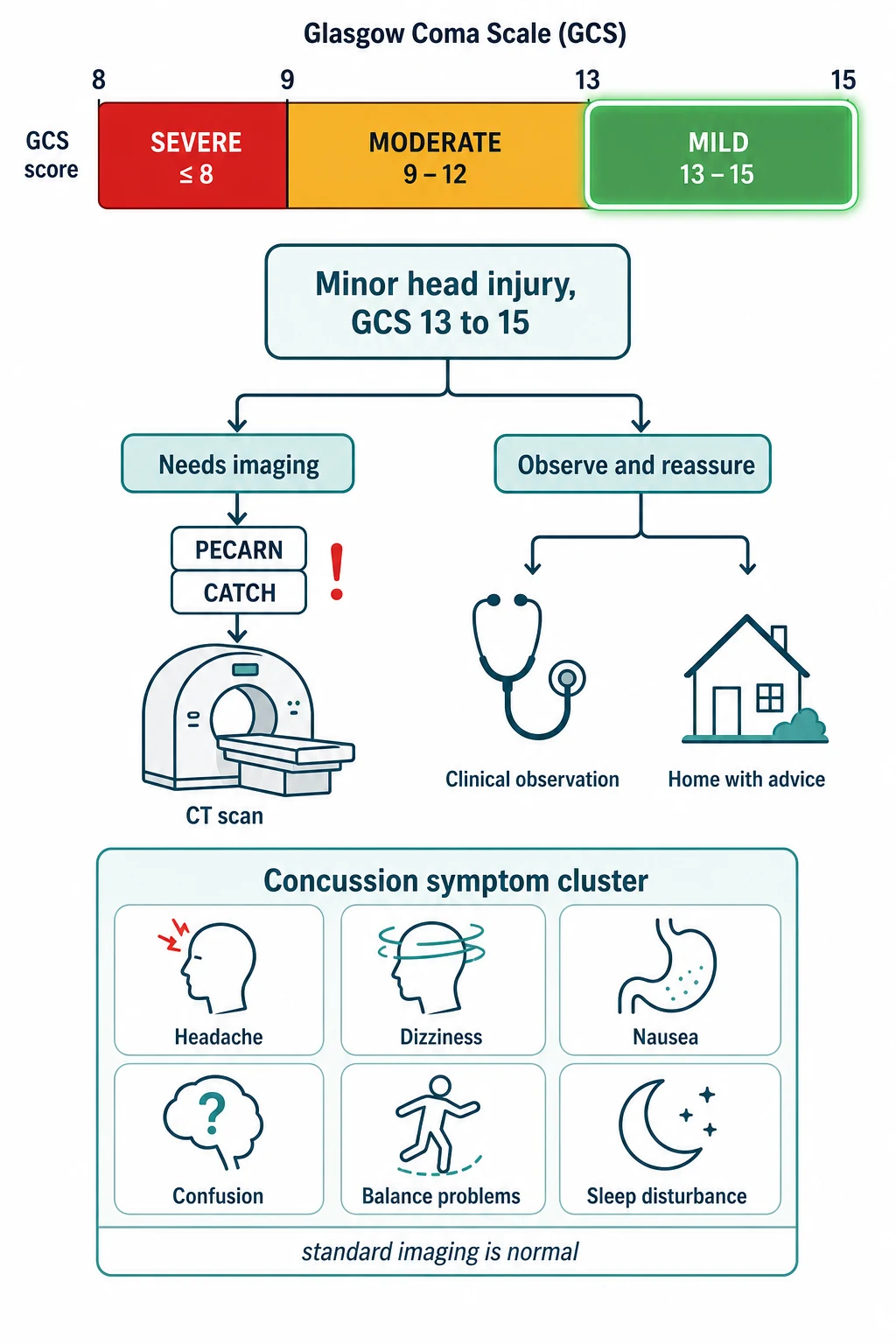
Mild traumatic brain injury is the broader medical term that brackets concussion, and it is defined operationally by the Glasgow Coma Scale. An injury with a Glasgow Coma Scale of 13 to 15 within 30 minutes of the event, with any period of loss of consciousness, amnesia, or neurological change, is a mild traumatic brain injury. The two terms overlap heavily, but concussion carries the added sense of a functional disturbance that imaging does not capture, while mild traumatic brain injury is the administrative and research envelope. The Centers for Disease Control and Prevention guideline synthesised the paediatric evidence into a set of recommendations that frame the modern approach. [3]
Three facts make this topic central to the paediatric exam. The diagnosis is clinical and depends on recognising the symptom cluster after a plausible mechanism, because no scan and no blood test confirms a concussion. The first decision is not treatment but triage, separating the child who needs a computed tomography from the very large majority who can be observed, and the PECARN and CATCH rules make that decision explicit. And the management is a graduated return to activity, in which prolonged rest is no longer the answer and the recovery of most children within four weeks is the benchmark against which persistent symptoms are detected. [4]
Classification
Mild traumatic brain injury is classified by severity alongside the moderate and severe forms, and the Glasgow Coma Scale is the dividing line. A Glasgow Coma Scale of 13 to 15 is mild, 9 to 12 is moderate, and 8 or below is severe. The distinction matters because the mild form is managed with observation and graduated activity while the moderate and severe forms need neuroimaging, neurosurgical involvement, and often intensive care. A child with a Glasgow Coma Scale below 13 does not have concussion and must not be labelled or managed as such. [3]
The symptom presentation is classified next, because concussion is a syndrome of several domains rather than a single symptom. The four domains are somatic, with headache and dizziness at the head; cognitive, with feeling foggy, slowed, or forgetful; emotional, with irritability and sadness; and sleep, with drowsiness or disturbed sleep. The Child Sport Concussion Assessment Tool, now in its sixth edition as Child SCAT6, captures these domains in a standardised multimodal assessment for children aged five to 12 that combines symptom report, cognitive testing, and balance. [6]
The temporal classification follows the recovery course. Acute concussion is the first days to weeks, during which the symptoms are expected and the child rests then resumes activity. Persistent post-concussion symptoms are symptoms that endure beyond the expected recovery window, set at four weeks in children and adolescents, and they mark the transition from reassurance to active rehabilitation. The temporal classification drives the management step, because the treatment of an acute concussion is graduated activity while the treatment of persistent symptoms is targeted therapy. [10]
Epidemiology & Risk Factors
Concussion is one of the commonest injuries of childhood, and its incidence has risen with greater sports participation and better recognition. Falls, sport, and recreational play are the leading mechanisms across childhood, with motor vehicle crashes and assault contributing in adolescents. Sport-related concussion concentrates in contact and collision sports such as rugby, Australian rules football, soccer, and basketball, and the highest paediatric rates are seen in adolescent athletes. [9]
The risk of concussion after a head injury is shaped by the mechanism and the child. A higher-energy mechanism, a direct blow to the head, and a history of previous concussion each raise the likelihood. Sex and age modify both the incidence and the outcome, with adolescent girls reporting higher symptom burdens and slower recovery than boys in several sports cohorts. The pre-injury profile matters too, because a child with migraine, mood disorder, attention deficit hyperactivity disorder, or learning difficulty has a higher baseline symptom load and a higher risk of prolonged recovery. [12]
The dominant risk factors for a prolonged course divide into the intrinsic and the acute. The intrinsic factors are the pre-injury vulnerabilities, chiefly female sex in adolescence, a prior concussion, pre-existing migraine, anxiety or depression, and attention deficit hyperactivity disorder. The acute factors are the injury itself, where a high symptom burden in the first days and a loss of consciousness or amnesia predict a slower recovery. Howell and colleagues showed in a paediatric sports medicine clinic that these factors together identify the child whose symptoms are likely to persist beyond the expected window. [12]
Pathophysiology
A concussion begins with a biomechanical force that rotates or accelerates the brain inside the skull, and it ends with a cascade of metabolic disturbance that is invisible to a computed tomography. The rapid acceleration and deceleration stretch the axons and the cell membranes, and the immediate effect is a diffuse release of the excitatory neurotransmitter glutamate and a large flux of ions across the membrane. The injury is functional rather than structural, which is why standard imaging looks normal. [5]
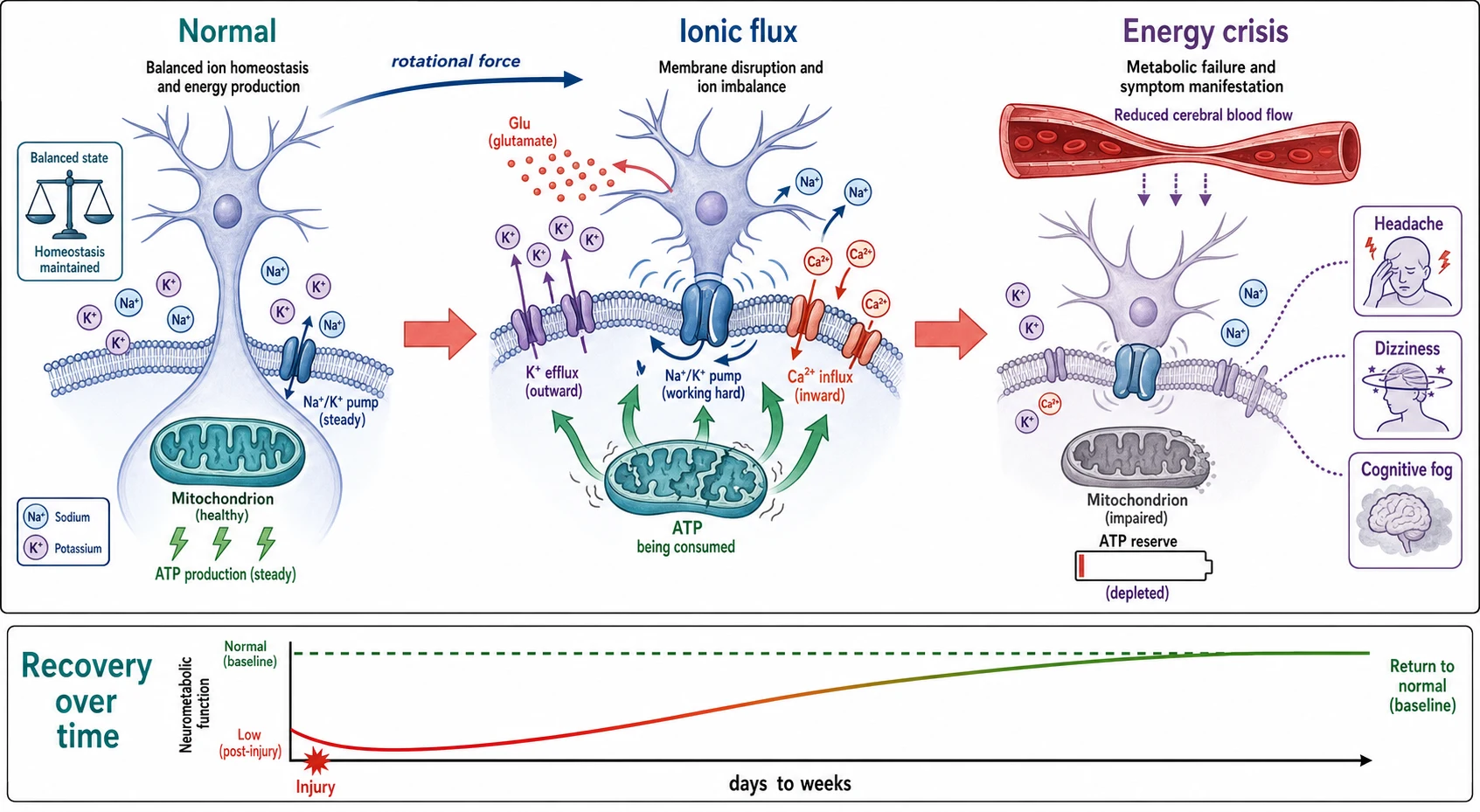
The ionic flux triggers an energy crisis. The outflow of potassium and the inflow of calcium drive the sodium-potassium pump to work hard to restore the gradients, and the pump consumes adenosine triphosphate at a rate the depleted cell cannot sustain. The calcium influx impairs the mitochondria, so the cell produces less energy precisely when it needs more. The mismatch between demand and supply is the metabolic bottleneck of the acute concussion, and it renders the brain vulnerable to a second injury in the days that follow, which is the rationale for removing the child from play and avoiding a second knock. [5]
The clinical consequence is the symptom cluster and the vulnerability window. The energy crisis and the reduced cerebral blood flow produce the headache, the fogginess, and the slowed thinking of the acute concussion. The vulnerability window, during which a second concussion carries a higher risk of prolonged or catastrophic outcome, is the biological basis of the graduated return to sport that prevents a repeat injury before the brain has recovered. The mismatch also explains why cognitive and physical exertion can worsen symptoms in the acute phase, and why a brief period of relative rest helps before activity resumes. [5]
Clinical Presentation
The presentation of a concussion is a child or adolescent who has taken a knock to the head or body and who now feels not right. The mechanism may be a fall, a collision in sport, a strike by a ball or an object, or a motor vehicle crash, and the onset of symptoms is rapid, within minutes to hours. Loss of consciousness occurs in only a minority, so its absence does not exclude a concussion, and a brief amnesia for the event is common. [9]
How concussion presents across the age spectrum
A preschool child who falls and then becomes quiet, clingy, or irritable, with vomiting once and a reluctance to play, the subtle presentation that is easily missed in the child who cannot describe symptoms
A school-age child who takes a knock in sport and complains of headache and dizziness, feels confused or foggy, and is slow to answer questions on the sideline
An adolescent rugby player who is briefly dazed after a tackle, plays on, and later reports headache, sensitivity to light, and poor concentration in class
A young child with a non-accidental head injury who presents with an altered conscious state and an inconsistent history, the scenario that shifts the focus to safeguarding
An adolescent who has had several concussions and now reports symptoms that persist for weeks, the presentation of persistent post-concussion symptoms
The symptom cluster spans four domains. The somatic symptoms are headache, dizziness, nausea, balance problems, and sensitivity to light and noise, and headache is the commonest of all. The cognitive symptoms are feeling foggy, slowed down, and having difficulty concentrating or remembering. The emotional symptoms are irritability, sadness, and nervousness. The sleep symptoms are feeling drowsy, sleeping more or less than usual, or having trouble falling asleep. The Child SCAT6 organises these into a structured report that the school-age child can complete. [6]
Two subtleties are deliberately examined. The first is that the symptoms of concussion overlap with everyday complaints, which is why a plausible mechanism and a temporal relationship are essential to the diagnosis. The second is that the symptoms evolve, so a child who looks well at the time of injury may develop symptoms over the following hours, and a child who is removed from play should be reassessed and should not return to play the same day. The rule of thumb is when in doubt, sit them out, because a concussed child who returns to play risks a second injury in the vulnerable window. [9]
Differential Diagnosis
The task at the bedside is to separate the child with a concussion, who needs observation and graduated activity, from the child with a structural brain injury, who needs imaging and possibly neurosurgery, and from the child whose symptoms have another cause. The discriminators are the red flags, the course of the conscious state, and the presence of focal signs, and the PECARN and CATCH rules formalise the imaging decision. [1]
Concussion / mild TBI
observe and graduate activity
- GCS 13 to 15 with rapid onset short-lived symptoms
- Headache, dizziness, fogginess, no focal signs
- Normal conscious state and no deterioration
- Symptoms evolve over hours then recover over days to weeks
Intracranial bleed / structural injury
urgent imaging and neurosurgery
- Deteriorating conscious state or focal neurological signs
- Repeated vomiting, seizure, or severe and worsening headache
- Signs of basilar skull fracture or a palpable skull fracture
- GCS below 13, managed as moderate or severe injury
Cervical spine injury
immobilise and image the spine
- Neck pain or midline tenderness after a high-energy mechanism
- Limb paraesthesia or weakness, or a distracting injury
- Fits the same trauma but demands spine clearance before discharge
- Concussion and spine injury can coexist after one event
Non-accidental head injury
safeguarding and imaging
The structural injuries to exclude are the intracranial bleeds and the fractures. An extradural haematoma presents with a lucid interval followed by deterioration, a subdural haematoma with a fluctuating conscious state, and a diffuse axonal injury with a prolonged coma. The basilar skull fracture shows with the raccoon eyes, the Battle sign, the haemotympanum, or the cerebrospinal fluid leak, and a palpable skull fracture is a sign that demands imaging. Any deterioration, any focal sign, or any seizure places the child in the imaging pathway, not the concussion pathway. [1]
The non-traumatic mimics are the conditions whose symptoms overlap with the concussion cluster. A migraine can produce headache, visual disturbance, and cognitive fog after a knock, and a post-traumatic seizure can be mistaken for a convulsive concussion. The key is that the diagnosis of concussion requires both a plausible mechanism and a compatible symptom cluster, and that the red flags are sought in every case to exclude the structural injury first. The cervical spine must be cleared in every head-injured child, because a spinal injury can coexist with a head injury. [3]
Clinical & Bedside Assessment
The bedside assessment of a head-injured child runs in two stages. The first is the immediate primary survey of the airway, breathing, and circulation, the cervical spine, and the conscious level, because a child with a falling Glasgow Coma Scale or a compromised airway is an emergency, not a concussion. The second is the focused concussion assessment, which uses a validated tool to capture the symptom cluster once the child is stable and the red flags have been excluded. [3]
The symptom assessment uses a validated tool rather than an open question. The Child SCAT6, for children aged five to 12, and the SCAT6 for those aged 13 and over, combine a symptom inventory with tests of cognition and balance. The tool is not used alone to make the diagnosis, which remains a clinical judgement, but it provides a structured baseline against which recovery is tracked and persistent symptoms are detected. The Child SCAT5 and its background rationale were set out by Davis and Echemendia and their colleagues, and the sixth edition refined the paediatric tool. [6][8]
The history captures the mechanism, the past, and the context. The mechanism is the energy, the direction, and the site of the force, and a high-energy mechanism such as a motor vehicle ejection or a fall from height raises the imaging threshold. The past history includes any previous concussion, the time to recovery, and any migraine, mood disorder, attention deficit hyperactivity disorder, or learning difficulty, each of which predicts a slower recovery. The context is the school, the sport, and the family, because the return to learn and the return to sport are negotiated with all three. [9]
Investigations
The investigation of a head-injured child turns on a single decision, whether to perform a computed tomography of the head, and the validated clinical decision rules make that decision explicit. The two rules examined in the paediatric curriculum are the PECARN rule from the United States and the CATCH rule from Canada, and both identify the children at very low risk of a clinically important brain injury in whom imaging can be safely withheld. [1][2]
The PECARN rule, reported by Kuppermann and colleagues, derives two prediction rules by age. For a child under two years, the risk of a clinically important traumatic brain injury is very low if all six of the following are absent: an altered mental status, a scalp haematoma other than frontal, a loss of consciousness of more than five seconds, a severe mechanism, not acting normally according to the parent, and any sign of a skull fracture. For a child aged two years and over, the risk is very low if all six are absent: an altered mental status, any sign of basilar skull fracture, a history of loss of consciousness, vomiting, a severe headache, and a severe mechanism. A severe mechanism in PECARN is a motor vehicle crash with ejection or rollover, a pedestrian or cyclist struck by a vehicle, or a fall of more than 0.9 metres for a child under two or more than 1.5 metres for a child over two. [1]
The CATCH rule, reported by Osmond and colleagues, applies to children from birth to 16 years with a minor head injury and a Glasgow Coma Scale of 13 to 15, and it recommends a computed tomography if any one of the high-risk factors is present: a Glasgow Coma Scale below 15 at two hours after the injury, a suspected open or depressed skull fracture, any sign of basilar skull fracture, vomiting four or more times, or a dangerous mechanism such as a fall from over three feet or five stairs or a motor vehicle crash. The rule identifies the small group at high risk of a brain injury requiring intervention, and it complements the PECARN rule across the paediatric age range. [2]
Beyond the imaging decision, no routine investigation confirms a concussion. The computed tomography, when performed, looks for a fracture or a bleed, and a normal scan does not confirm a concussion but excludes a structural injury. Blood biomarkers are under study as a means to reduce imaging, but they are not yet standard practice. The diagnosis of concussion remains clinical, based on the mechanism and the symptom cluster, and the return to activity is symptom-guided. [4]
Management — Resuscitation
The first move in a head-injured child is to exclude the emergency. The airway, breathing, and circulation are secured, the cervical spine is immobilised when a high-energy mechanism is suspected, and the Glasgow Coma Scale is recorded and repeated. A child with a falling score, a compromised airway, or a focal sign is managed as a moderate or severe injury, with urgent imaging and neurosurgical involvement, and the label of concussion is withheld until the structural injury is excluded. [3]
The child with a mild injury who is stable and alert moves to the imaging decision. The PECARN or CATCH rule is applied, and the child at very low risk is observed rather than scanned. Observation means serial assessment of the conscious state and the symptoms over a period of hours, and discharge is planned once the child is stable, improving, and able to tolerate oral intake. The family is given a clear safety net of the features that should bring them back, chiefly a deteriorating conscious state, repeated vomiting, a seizure, or a worsening headache. [1]
The acute symptom relief is simple and symptom-guided. Paracetamol is the preferred analgesic for the headache, given at the standard weight-based paediatric dose, and the child is advised to avoid substances that worsen symptoms or mask recovery, including alcohol and excessive caffeine. The non-steroidal anti-inflammatory drugs are avoided in the first 24 to 48 hours by convention because of the theoretical bleeding risk, though the evidence is limited. The acute period is one of relative rest, which is discussed in the next section. [9]
Management — Definitive & Stepwise
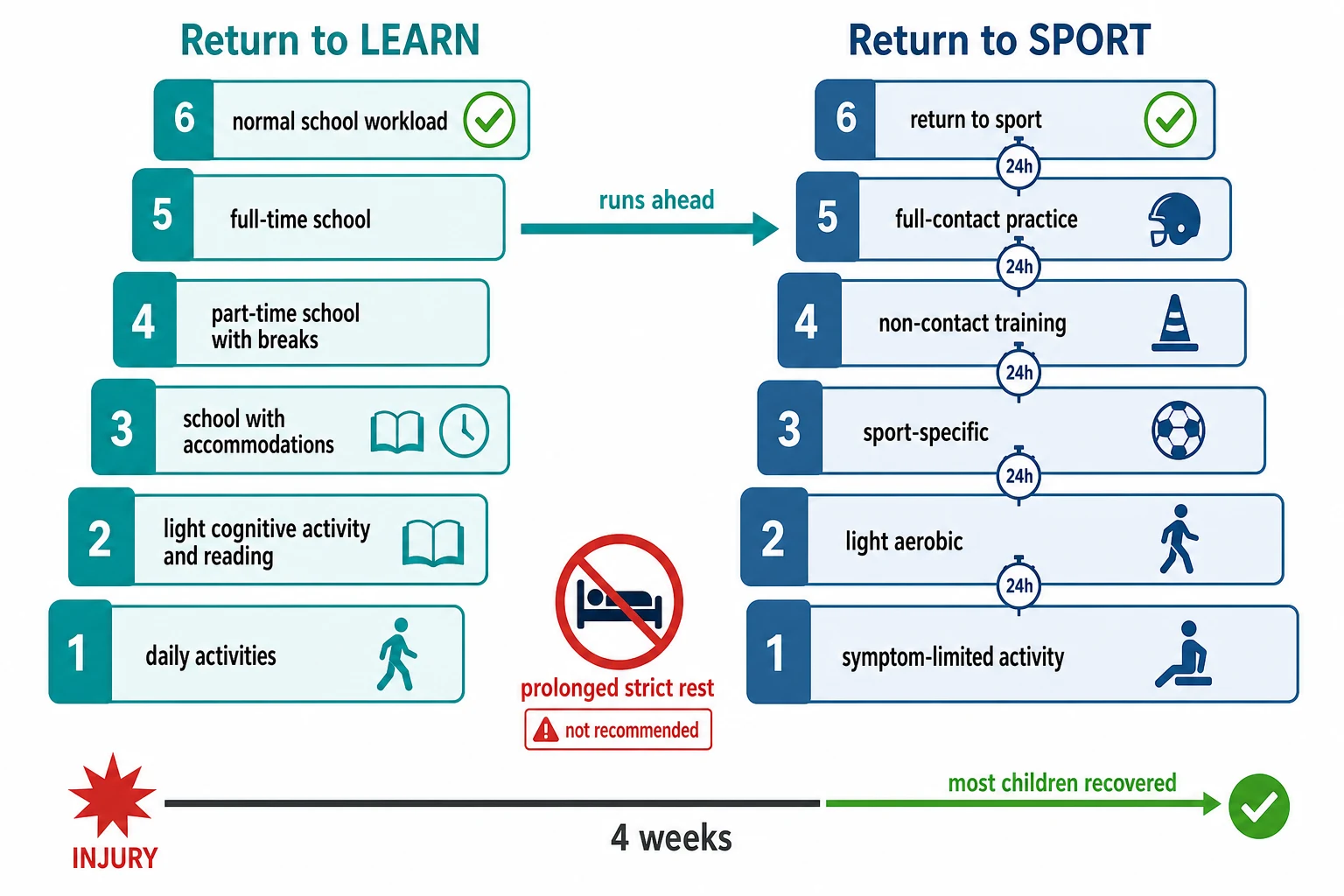
The definitive management of a concussion is the graduated return to activity, and the Amsterdam 2022 consensus reset the modern approach. The child is given 24 to 48 hours of relative rest, which means avoiding vigorous activity and limiting screen time and intense cognitive load, but it is emphatically not strict rest in a dark room. Prolonged strict rest beyond 48 hours worsens symptoms and slows recovery, and the consensus is clear that cocoon therapy is harmful and must be abandoned. [5]
[5]The return to learn comes before the return to sport, and this order is a frequent exam point. The child resumes cognitive activity in steps, beginning with light reading and screen time, then a return to school with accommodations such as breaks, reduced workload, and extra time, then a gradual increase to a full school day. The school cannot be skipped, because a child must be back to full cognitive participation before returning to contact sport. The return to sport then proceeds through six steps, each separated by a minimum of 24 hours, from symptom-limited activity through light aerobic exercise, sport-specific exercise, non-contact training drills, full-contact practice, and finally return to sport. [5]
The steps are paused if symptoms recur. If a symptom returns at any step, the child drops back to the previous asymptomatic step and tries again after 24 hours. The graduated pathway is designed to expose the recovering brain to increasing demands at a pace it can tolerate, and it is the practical embodiment of the metabolic recovery described in the pathophysiology section. The American Academy of Pediatrics clinical report reinforced that the return to learn is a collaborative process with the school, the family, and the clinician, and that accommodations are temporary and symptom-driven. [9]
Acute headache relief in concussion
Dose
Paracetamol 15 mg per kg orally every four to six hours as needed, maximum 60 mg per kg per day in children under 12
A persistent myth is that a concussed child must be woken every few hours through the night. The modern guidance is that a child who is stable and improving may sleep normally, and that the disturbance of frequent waking itself worsens recovery. The family is advised to check the child is breathing easily and rousable, and to return if the child cannot be woken or shows any red flag. The safety-net advice is the practical partner of the graduated pathway. [5]
Specific Subtypes & Scenarios
Sport-related concussion in the adolescent is the prototypical scenario and the one most tested. The athlete is removed from play at the time of the suspected injury and assessed on the sideline, because a concussed athlete who continues to play risks a second injury and a prolonged recovery. The athlete does not return to play the same day, and the graduated return to sport begins after 24 to 48 hours of relative rest. The scenario tests the principle that removal from play is non-negotiable and that return is symptom-gated. [9]
The preschool child with a minor head injury is the second scenario, and the one for whom the assessment is hardest. The young child cannot articulate the symptom cluster, so the presentation is behavioural, with irritability, clinginess, quietness, or a change in play, and vomiting may be the only somatic clue. The PECARN rule for the under-two age band is applied, and the family is given a careful safety net. The young child with an inconsistent history or an injury that does not fit the developmental stage raises the safeguarding scenario of non-accidental head injury, which shifts the focus to imaging and the child-protection workup. [1]
The child with persistent post-concussion symptoms is the third and most complex scenario, and it is the bridge to the next section. Symptoms that endure beyond four weeks mark the transition from acute management to active rehabilitation, and the child is assessed for the modifiable contributors, the sub-symptom threshold exercise deficit, the vestibular or ocular dysfunction, the mood disorder, and the school disengagement. The child with multiple concussions is a related scenario, in whom the cumulative risk and the longer recovery frame a cautious and individualised return to sport. [10]
Complications & Pitfalls
Persistent post-concussion symptoms are the principal complication, defined as symptoms that endure beyond the expected recovery window of four weeks in children. The syndrome affects an estimated 10 to 30 percent of children after a concussion, and its management is active rehabilitation rather than further rest. The shift in management is the key exam message, because the prescription of more rest to a child with persistent symptoms is the commonest and most harmful error, since it entrenches deconditioning, social isolation, and the symptom burden itself. [10]
Second impact syndrome is the rare and catastrophic complication, in which a second concussion sustained before the first has resolved triggers a rapid and fatal cerebral oedema. The syndrome is described chiefly in adolescents and is very rare, but its existence underpins the rule that a concussed child does not return to contact play until fully recovered. The cumulative effect of repeated concussions, with longer recovery times and the theoretical risk of long-term cognitive sequelae, is the broader concern that frames a cautious approach to the child with multiple injuries. [5]
The classic pitfalls are temporal, diagnostic, and therapeutic. The first temporal pitfall is returning a child to play the same day, which exposes the vulnerable brain to a second injury. The first diagnostic pitfall is treating a deteriorating child as a concussion, which delays the imaging and the neurosurgery that the structural injury demands. The first therapeutic pitfall is prescribing prolonged strict rest to a child with persistent symptoms, which deepens rather than resolves the syndrome. Each of these errors is preventable by adherence to the graduated pathway and by the vigilance for the red flags. [9]
A subtler pitfall is attributing every symptom after a knock to the concussion. A persistent headache may be a medication-overuse headache from frequent analgesia, a dizziness may be a vestibular dysfunction that responds to specific rehabilitation, and a persistent low mood may be a primary mood disorder unmasked by the injury. The management of persistent symptoms requires the clinician to identify the dominant contributor for each child and to target it, rather than to apply a blanket label of post-concussion syndrome. [10]
Prognosis & Disposition
The prognosis of a paediatric concussion is, in the main, excellent, with most children recovering fully within four weeks. Ledoux and colleagues tracked the natural progression of symptom change in a paediatric population and found that the symptom burden falls steeply in the first two weeks and that the majority of children are symptom-free by four weeks. The dominant determinants of a slower recovery are the pre-injury vulnerabilities, the acute symptom burden, and the early management, and a child with several risk factors is flagged for closer follow-up. [11]
Disposition is to home with a safety net for the child who is stable, alert, and improving, and to hospital for the child who needs imaging, observation, or the management of a structural injury. A child with a normal assessment and no red flags is discharged with written return to learn and return to sport guidance and a follow-up in the clinic or with the general practitioner at one to two weeks. A child whose symptoms persist beyond four weeks is referred to a multidisciplinary concussion service for active rehabilitation, where physiotherapy, psychology, and education liaison work together. [3]
The prognosis is framed for the family in terms of the expected trajectory and the signposts of recovery. The family is told that the symptoms are expected, that they will ease over days to weeks, and that the child will return to school before sport and to sport before contact play. The family is also told the features that should prompt review, chiefly a failure to improve, a return of symptoms at a particular step, or any red flag. The framing manages the anxiety that drives the demand for more rest and more imaging, and it sets the expectation of a graduated return. [9]
Special Populations
The child with a neurodevelopmental disorder is the population at highest baseline risk of a prolonged recovery. A child with attention deficit hyperactivity disorder, autism, or a learning difficulty has a higher baseline symptom load and may find the symptom inventory harder to complete, and the pre-injury vulnerabilities that predict persistent symptoms cluster in this group. The management is the same graduated pathway, with closer follow-up and an earlier move to active rehabilitation, and with school accommodations tailored to the baseline learning need. [12]
The Aboriginal and Torres Strait Islander child and the child from a remote setting is the second population, and the one for whom the access to follow-up shapes the outcome. The distance to a concussion service, the higher burden of injury in some remote communities, and the cultural context of sport and school all shape the care. The culturally appropriate communication, the engagement with the family and the community, and the use of telehealth to bridge the distance are part of the management, and the safety net is given in a form the family can act on. [3]
The child from a refugee or migrant family is the third population, and the one for whom the language and the continuity are the challenges. The symptom inventory and the return to learn guidance depend on shared language, an interpreter is engaged early, and the school liaison is central to the reintegration. The safeguarding scenario is the fourth population, because a head injury in an infant with an inconsistent history is non-accidental until excluded, and the clinician holds the dual responsibility of the medical and the child-protection assessment. [1]
Evidence, Guidelines & Regional Differences
The evidence base for the imaging decision was transformed by the PECARN and CATCH studies. Kuppermann and colleagues reported the PECARN rule in a prospective cohort of over 42,000 children, deriving the two age-specific prediction rules that identify the children at very low risk of a clinically important traumatic brain injury in whom imaging can be withheld. Osmond and colleagues reported the CATCH rule across ten Canadian paediatric emergency departments, identifying the high-risk factors that predict a brain injury requiring neurosurgical intervention. Together the rules give the clinician a validated basis to reduce the computed tomography rate without missing the structural injury. [1][2]
PECARN
United States, Lancet 2009
- Two age-specific rules for under and over two years
- Identifies very low risk children for observation without CT
- Six negative predictors in each age band
- Validated in over 42,000 children
CATCH
Canada, CMAJ 2010
- Validated from birth to 16 years with GCS 13 to 15
- High-risk factors trigger computed tomography
- Vomiting four or more times is a trigger
- Identifies injuries needing neurosurgical intervention
Amsterdam 2022
International consensus, 6th conference
- 24 to 48 hours of relative rest then early symptom-limited activity
- Return to learn before return to sport
- Rejects prolonged strict rest
- Child SCAT6 for the multimodal assessment
The consensus on management is anchored by the Amsterdam 2022 statement, which is the sixth in the series of international consensus statements on concussion in sport and which reset the approach to rest and activity. The American Academy of Pediatrics clinical report on sport-related concussion, reported by Halstead and colleagues, reinforced the graduated return to learn as a school collaboration, and the Centers for Disease Control and Prevention guideline, reported by Lumba-Brown and colleagues, distilled the paediatric evidence into 19 recommendations across diagnosis, prognosis, and management. The shared foundation of all three is the rejection of prolonged strict rest and the endorsement of a symptom-guided graduated return. [3][5][9]
The regional differences centre on the preferred imaging rule and the tool. The North American pathway leans on the PECARN rule, the Canadian pathway on the CATCH rule, and the Australian and New Zealand pathway accepts both and often applies the PECARN framework given its shared derivation population. The Child SCAT6 has replaced the Child SCAT5 across all regions as the multimodal assessment tool. The shared foundation is the graduated return to learn before return to sport, the 24 to 48 hour period of relative rest, and the active rehabilitation of persistent symptoms. [5][6]
Exam Pearls
The PECARN predictors for a child over two years
References
- [1]Kuppermann N, Holmes JF, Dayan PS, et al Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet, 2009.PMID 19758692
- [2]Osmond MH, Klassen TP, Wells GA, et al CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. CMAJ, 2010.PMID 20142371
- [3]Lumba-Brown A, Yeates KO, Bethel J, et al Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children. JAMA Pediatr, 2018.PMID 30193284
- [4]Lumba-Brown A, Yeates KO, Bethel J, et al Diagnosis and Management of Mild Traumatic Brain Injury in Children: A Systematic Review. JAMA Pediatr, 2018.PMID 30193325
- [5]Patricios JS, Schneider KJ, Dvorak J, et al Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport, Amsterdam, October 2022. Br J Sports Med, 2023.PMID 37316210
- [6]Davis GA, Purcell LK, Guskiewicz KM, et al Child SCAT6. Br J Sports Med, 2023.PMID 37316212
- [7]Echemendia RJ, Brett BL, Broglio S, et al Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and rationale. Br J Sports Med, 2017.PMID 28446453
- [8]Davis GA, Purcell L, Schneider KJ, et al The Child Sport Concussion Assessment Tool 5th Edition (Child SCAT5): Background and rationale. Br J Sports Med, 2017.PMID 28446452
- [9]Halstead ME, McAvoy K, Devore CD, et al Sport-Related Concussion in Children and Adolescents. Pediatrics, 2018.PMID 30420472
- [10]Makdissi M, Schneider KJ, Davis GA, et al Approach to investigation and treatment of persistent symptoms following sport-related concussion: a systematic review. Br J Sports Med, 2017.PMID 28483928
- [11]Ledoux AA, Tang K, Yeates KO, et al Natural Progression of Symptom Change and Recovery From Concussion in a Pediatric Population. JAMA Pediatr, 2019.PMID 30398522
- [12]Howell DR, Kriz P, Mannix RC, et al Identifying Persistent Postconcussion Symptom Risk in a Pediatric Sports Medicine Clinic. Am J Sports Med, 2018.PMID 30265817