Paeds · neurology-neurodisability-and-neuromuscular
Febrile seizures
Also known as Febrile seizure · Febrile convulsion · Simple febrile seizure · Complex febrile seizure · Febrile status epilepticus · GEFS+ (generalised epilepsy with febrile seizures plus)
Fellowship guide to febrile seizures: the age-locked definition (6 months to 5 years with fever, no CNS infection, no prior afebrile seizure), the simple-versus-complex split that drives every decision, the reassuring prognosis, the acute termination of a prolonged convulsion with a benzodiazepine, the case against routine antiepileptic prophylaxis and against antipyretics as prevention, the lumbar-puncture thresholds of the 2011 AAP guideline, and the FEBSTAT evidence linking febrile status epilepticus to hippocampal injury.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the 18-month-old brought to the emergency department in the arms of a frightened parent after a generalised convulsion that lasted two minutes and began with a fever that morning. The child is now alert, febrile to 39.2 degrees Celsius, and has a clear viral upper-respiratory infection. That child carries the entire teaching point of febrile seizures: a frightening event with a reassuring prognosis, where the task is to confirm the diagnosis, exclude meningitis, terminate any ongoing convulsion, and resist the impulse to over-investigate or over-treat. [1]
A febrile seizure is defined by four locked criteria. The child is aged between 6 months and 60 months (5 years). There is a fever, taken as a temperature over 38 degrees Celsius. There is no evidence of a central nervous system infection. And the child has no history of a prior afebrile seizure and no defined acute neurological cause. A convulsion with fever that falls outside any one of these criteria is not a febrile seizure and demands a different diagnostic path. [1] [2]
Febrile seizures are the most common neurological disorder of early childhood, affecting between 2 and 5 per cent of children in Western populations, with a peak incidence between 12 and 18 months of age and a slight male predominance. They are a developmental phenomenon of the immature brain, and they are benign. The teaching challenge is to hold three ideas together at once: the event is terrifying for families, the underlying diagnosis is usually benign, and a small minority of children have a dangerous mimic or a prolonged convulsion that needs active treatment. [2] [3]
Classification
The act of classification is the act that determines the workup, the counselling, and the prognosis. After the child has been stabilised and the diagnosis of a febrile seizure confirmed, the next question is always whether the seizure was simple or complex. The two categories are defined by three features: the mode of onset, the duration, and whether the seizure recurred within 24 hours. [1]
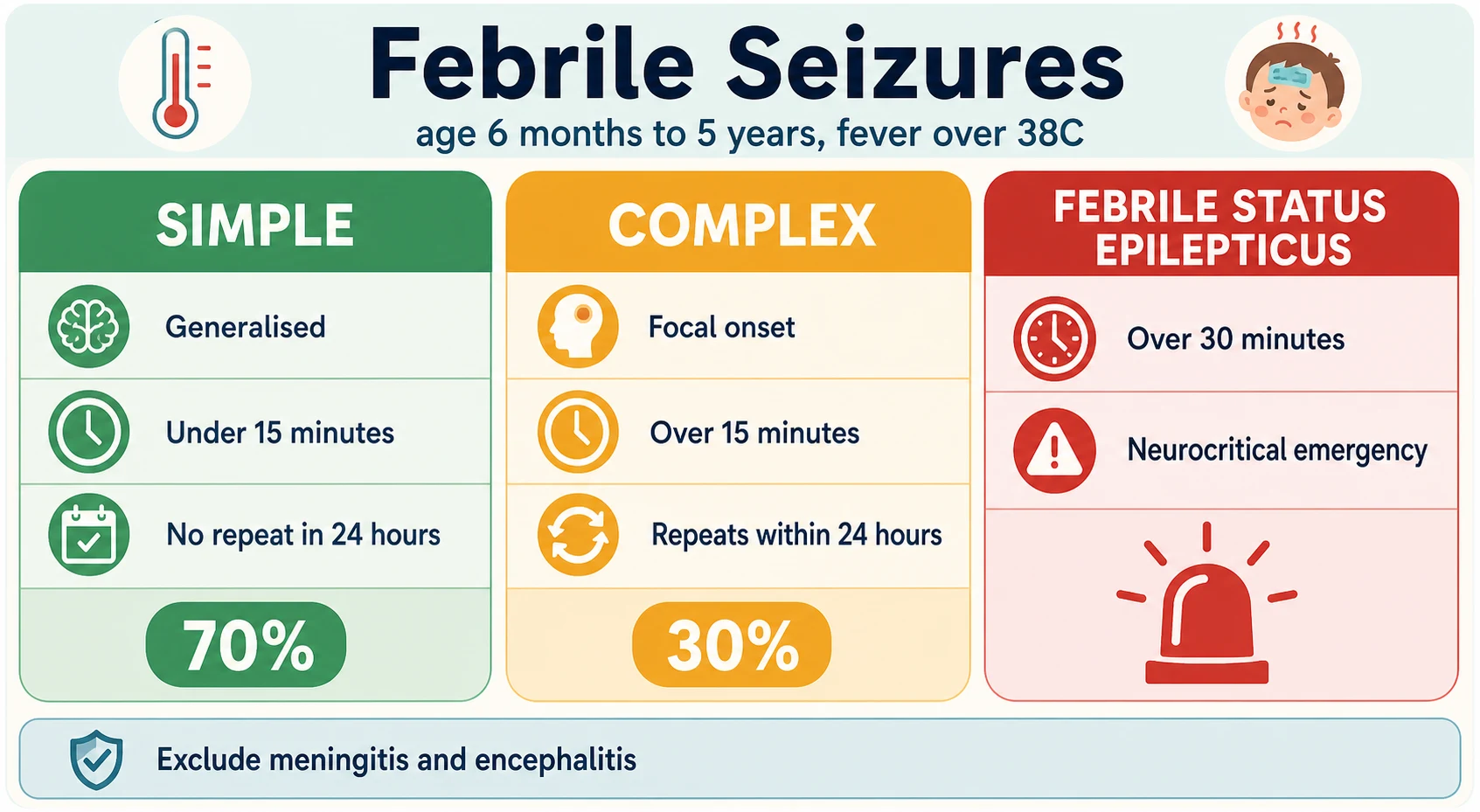
A simple febrile seizure is primary generalised from the onset, lasts under 15 minutes, and does not recur within the next 24 hours. It accounts for about 70 per cent of all febrile seizures, needs no routine neuroimaging or electroencephalogram, and carries the reassuring prognosis that defines the entity. A complex febrile seizure has any one of three features: a focal onset (observed or suspected), a duration over 15 minutes, or recurrence within 24 hours. Roughly 30 per cent of febrile seizures are complex, and they carry a higher recurrence rate and a higher subsequent epilepsy risk. [1] [2]
Simple febrile seizure
about 70 per cent
- Primary generalised tonic-clonic onset
- Lasts under 15 minutes
- No recurrence within 24 hours
- Child recovers quickly to baseline
- No routine EEG or neuroimaging needed
- Excellent prognosis, minimal epilepsy risk
Complex febrile seizure
about 30 per cent
- Focal onset, or focal features during the convulsion
- Lasts over 15 minutes
- Recurs within 24 hours
- Higher recurrence and subsequent epilepsy risk
- Consider EEG and neuroimaging
- Offer a rescue benzodiazepine plan
Febrile status epilepticus
over 30 minutes
- A febrile convulsion lasting over 30 minutes
- Neurocritical emergency - terminate urgently
- Higher risk of hippocampal injury (FEBSTAT)
- Admit for observation and investigation
- Search for a precipitant including HHV-6
The boundary at 15 minutes matters because it is the threshold at which a convulsion is unlikely to self-terminate and active treatment should begin, and the boundary at 30 minutes matters because it defines febrile status epilepticus. A child whose febrile convulsion is still ongoing at five minutes should be treated as heading toward status, not observed. The FEBSTAT study showed that febrile status epilepticus carries a real risk of acute hippocampal injury and of later temporal lobe epilepsy, which is why duration is a classification feature and not merely a descriptor. [8] [9]
Epidemiology & Risk Factors
Febrile seizures affect between 2 and 5 per cent of children in North America and Europe, with higher reported rates in some Asian populations. The peak age is 12 to 18 months, and the great majority of first febrile seizures occur between 6 months and 3 years. Boys are affected slightly more often than girls. The condition clusters in families, consistent with a strong genetic contribution, and a family history of febrile seizures is one of the strongest risk factors for having one. [2] [3]
Recurrence is common. About one in three children who has a first febrile seizure will have another, and the meta-analysis by Berg and Shinnar identified four predictors of recurrence: a young age at first seizure (under 12 months), a family history of febrile seizures, a relatively low fever at the time of the first seizure, and a short interval between the fever onset and the seizure. A child with all four risk factors has a recurrence risk approaching 70 per cent, while a child with none has a risk under 20 per cent. [7]
The numbers that anchor your viva
The risk of subsequent epilepsy is low after a simple febrile seizure, at around 2 to 5 per cent, which is only marginally above the 1 per cent background risk of epilepsy in the general population. The risk rises with complex features, with a pre-existing neurological or developmental abnormality, and with a family history of epilepsy. Febrile status epilepticus carries a meaningfully higher risk of later temporal lobe epilepsy, which the FEBSTAT study linked to acute hippocampal injury visible on magnetic resonance imaging. [8] [11]
Pathophysiology
Febrile seizures arise from the lowered seizure threshold of the developing brain during fever in a genetically susceptible child, rather than from the height of the fever itself. The phenomenon is locked to a developmental window because the immature brain has neuronal networks that are excitable and poorly inhibited, and fever destabilises them. The temperature at which a seizure occurs is usually lower in children who later have recurrences, which is one of the Berg and Shinnar predictors. [7] [3]
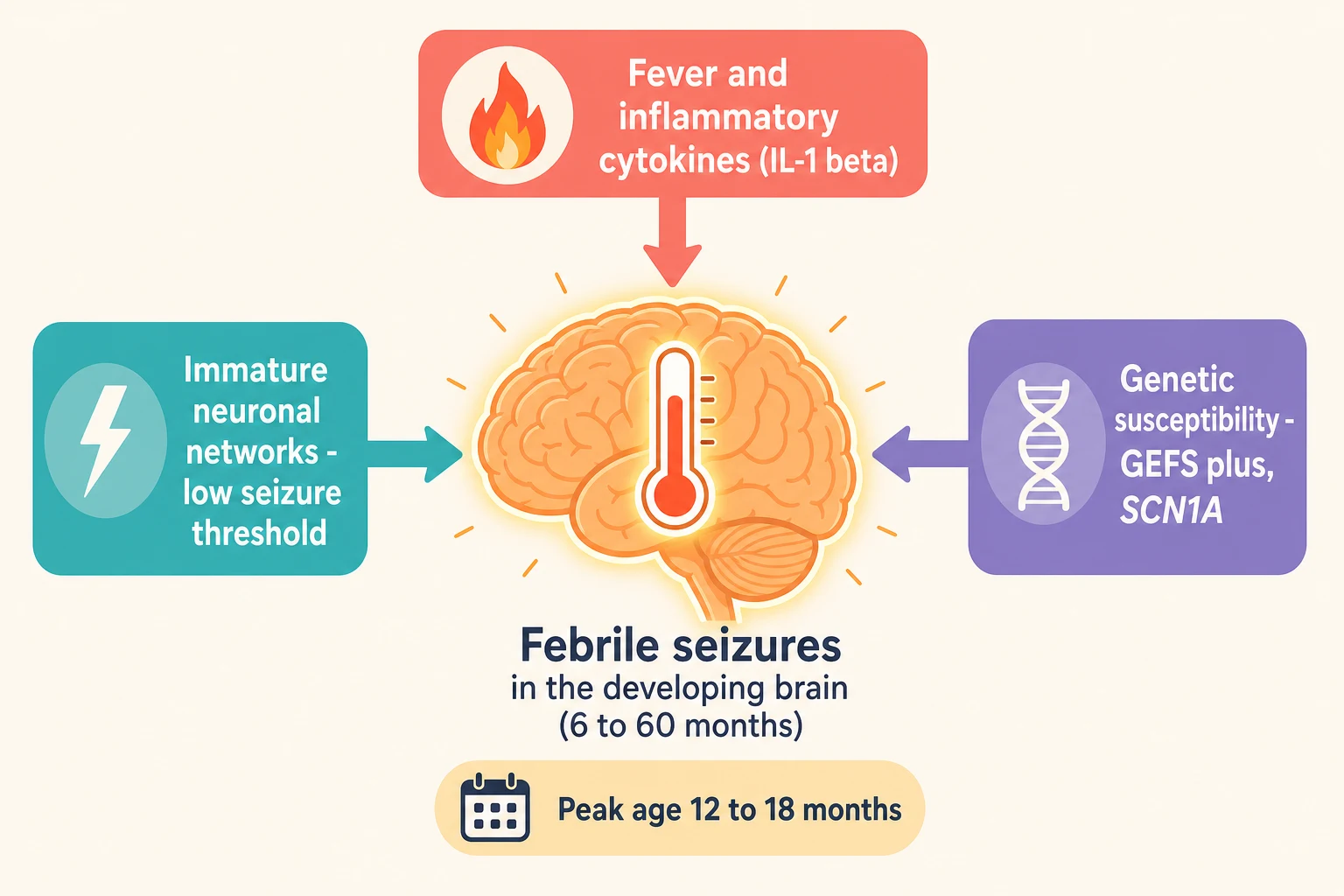
Three inputs converge on the developing brain. Fever, with its associated inflammatory cytokines, is the trigger; interleukin-1 beta in particular lowers the seizure threshold. The immature neuronal network provides the substrate, with incomplete inhibitory circuitry that matures through early childhood and explains the age-locked window. And genetic susceptibility sets the individual threshold, which is why a family history is so prominent and why specific syndromes such as generalised epilepsy with febrile seizures plus (GEFS+) map to channelopathy genes including SCN1A. [3]
[6] [3]Human herpesvirus 6 and 7, the agents of roseola, are over-represented among the fevers that precipitate febrile status epilepticus. The FEBSTAT study found that human herpesvirus 6 and 7 were more frequent in children with febrile status epilepticus than in those with simple febrile seizures, and the same cohort showed that febrile status epilepticus could produce acute hippocampal swelling that in some children evolved to hippocampal sclerosis and temporal lobe epilepsy. This is the mechanistic link between the most prolonged febrile seizures and a small but real long-term epilepsy risk. [10] [8]
Clinical Presentation
The typical story is a previously well child, usually between 12 and 18 months old, who develops a fever and within the first hours of the illness has a generalised tonic-clonic convulsion lasting under five minutes. The seizure is often the event that brings the family to hospital, and the fever source, such as an upper respiratory infection, otitis media, or a viral exanthem, is found on history and examination. The child recovers to a normal level of consciousness within minutes to an hour, which is a key feature distinguishing a simple febrile seizure from a more serious cause. [1] [3]
A complex febrile seizure presents with one of the defining features: a focal onset (for example twitching confined to one side of the body or face), a prolonged duration over 15 minutes, or a second convulsion within 24 hours. A child with a complex febrile seizure may have a slower recovery, a transient focal deficit (Todd paresis), or a more prolonged postictal state, and these features shift the differential toward a structural, inflammatory, or epileptic cause. [1] [2]
| Clinical picture | What it implies | Act |
|---|
A prolonged postictal state is the single most important red flag at the bedside. A child who has not returned to a normal baseline within an hour, who is persistently drowsy or irritable, or who has a focal neurological deficit should not be diagnosed with a simple febrile seizure until meningitis, encephalitis, a structural lesion, and a metabolic disturbance have been excluded. The same applies to any child outside the age window, whose convulsion with fever demands a separate diagnosis. [1] [12]
Differential Diagnosis
The first task is to confirm that the event was a seizure and that it was associated with fever, because several common events mimic a febrile convulsion. A rigor (shivering with a fever spike) can look alarming but produces a shaking child who is conscious throughout. A breath-holding spell with anoxic convulsive movements follows a brief crying and cyanotic phase. Syncope is briefer and followed by rapid, complete recovery. These mimics are resolved by a careful eyewitness account of the onset, the duration, and the recovery. [1] [3]
The second and more dangerous task is to exclude the serious causes of a convulsion with fever, which are the conditions that febrile seizures must not be confused with. Bacterial meningitis and viral encephalitis are the principal infectious threats, and they are excluded clinically and, when indicated, by lumbar puncture. Electrolyte disturbance, particularly hyponatraemia from gastroenteritis, hypoglycaemia, and hypocalcaemia, can present as a seizure with an incidental fever. Trauma, including non-accidental injury, and intoxication must be considered when the history is inconsistent. [1] [12]
Simple febrile seizure
- Age 6 months to 5 years, fever, generalised
- Under 15 min, recovers to baseline
- No meningeal or focal signs
- Self-limiting viral fever source
- Minimal investigation, no prophylaxis
Meningitis or encephalitis
- Ill-looking, prolonged postictal state
- Petechiae, bulging fontanelle, neck stiffness
- Complex or focal seizure
- Lower threshold for lumbar puncture in infants
- Empirical antibiotics and aciclovir
Seizure mimic with fever
- Rigor: shaking with preserved consciousness
- Breath-holding spell after crying
- Syncope: brief, rapid full recovery
- Respiratory infection with febrile twitching
- Resolved by a careful eyewitness history
A child outside the 6 month to 5 year window with a convulsion and fever is not having a febrile seizure. A neonate with a seizure and fever has a separate, much more dangerous differential dominated by serious bacterial infection, inborn errors of metabolism, and structural lesions. A child over five years with a convulsion and fever has, by definition, an afebrile seizure disorder or a provoked seizure, and needs an epilepsy and provoking-cause workup. Holding the age boundary firmly is one of the highest-yield exam points. [1] [2]
Clinical & Bedside Assessment
Assessment runs in parallel with termination, because a child who is still convulsing needs the seizure stopped while the diagnostic questions are answered. Secure the airway, give oxygen, check a bedside glucose, and obtain intravenous access. If the convulsion has lasted over five minutes, treat it now with a benzodiazepine rather than waiting for it to self-terminate. If the child has recovered, the assessment turns to confirming the diagnosis, finding the fever source, and excluding meningitis. [1] [4]
The history targets the fever onset, the seizure description (onset, duration, focal versus generalised, recovery), any recurrence within 24 hours, recent illness and antibiotic exposure, immunisation status, the developmental history, and the family history of febrile seizures and epilepsy. An account of a focal onset, a prolonged duration, or a failure to recover to baseline changes the diagnosis from simple to complex or displaces it altogether. [1] [12]
[1] [4]Examination looks for the fever source (ears, throat, chest, skin, urine), for meningeal signs (neck stiffness, bulging fontanelle, petechiae, photophobia), and for any focal neurological deficit or developmental concern. The general appearance of the child is informative: a well-looking, playful, febrile toddler who has fully recovered supports a simple febrile seizure, while an ill-looking, drowsy, or irritable child demands exclusion of serious infection. Prior antibiotic exposure can mask meningeal signs and lowers the threshold for lumbar puncture. [12] [1]
Investigations
The guiding principle for a simple febrile seizure is restraint. The well-looking child aged over 12 months who has had a short generalised convulsion with fever and has fully recovered needs no routine blood tests, no electroencephalogram, no neuroimaging, and no lumbar puncture beyond what the fever itself would prompt. Over-investigation of simple febrile seizures is a recognised cause of unnecessary radiation, hospital admission, and parental anxiety. [1] [3]
A bedside blood glucose is the one test that belongs in almost every assessment, because hypoglycaemia is a treatable cause of a convulsion and is easily missed. Blood tests for electrolytes, calcium, magnesium, and a full blood count are reserved for the child with a prolonged or complex seizure, an ill appearance, dehydration, or a failure to recover. A blood culture and inflammatory markers are driven by the suspicion of serious infection rather than by the seizure itself. [1] [12]
The selective investigation pathway
Bedside blood glucose on every child with a convulsion
Temperature and a search for the fever source (ears, throat, chest, skin, urine)
Lumbar puncture if meningeal signs, or if an infant under 12 months is ill-looking or incompletely immunised
Bloods (electrolytes, calcium, glucose, FBC, cultures) only for complex, prolonged, or ill-looking presentations
Electroencephalogram only for complex febrile seizure, focal features, or concern about epilepsy
Neuroimaging only for focal deficit, prolonged postictal state, or a failure to recover
The lumbar puncture decision follows the 2011 American Academy of Pediatrics guideline. Perform a lumbar puncture in any child with meningeal signs, and strongly consider it in any child aged 6 to 12 months who is incompletely immunised against Haemophilus influenzae type b or Streptococcus pneumoniae, or who has been pre-treated with antibiotics, because both situations can mask meningitis. A lumbar puncture is not routinely required for a well-looking, fully immunised child over 12 months with a simple febrile seizure. The study by Kimia and colleagues showed that bacterial meningitis is rare among well-appearing children aged 6 to 18 months presenting with a first simple febrile seizure. [1] [12]
An electroencephalogram is not recommended after a simple febrile seizure, because it does not predict recurrence or subsequent epilepsy and does not change management. It may be considered after a complex febrile seizure, when focal features or developmental concerns raise the question of an underlying epilepsy. Neuroimaging, whether computed tomography or magnetic resonance imaging, is reserved for the child with a focal deficit, a prolonged postictal state, a failure to recover, or signs of raised intracranial pressure, and is not part of the routine workup of a simple febrile seizure. [1]
Management — Resuscitation
Acute resuscitation addresses the airway, breathing, and circulation, and then answers the single time-critical question: is the child still convulsing. A febrile convulsion that has lasted under five minutes and has terminated needs no anticonvulsant. A convulsion that is ongoing at five minutes, or that recurs, needs active termination, because the longer a convulsion lasts the less likely it is to self-terminate and the greater the risk of progression to febrile status epilepticus. [1] [4]
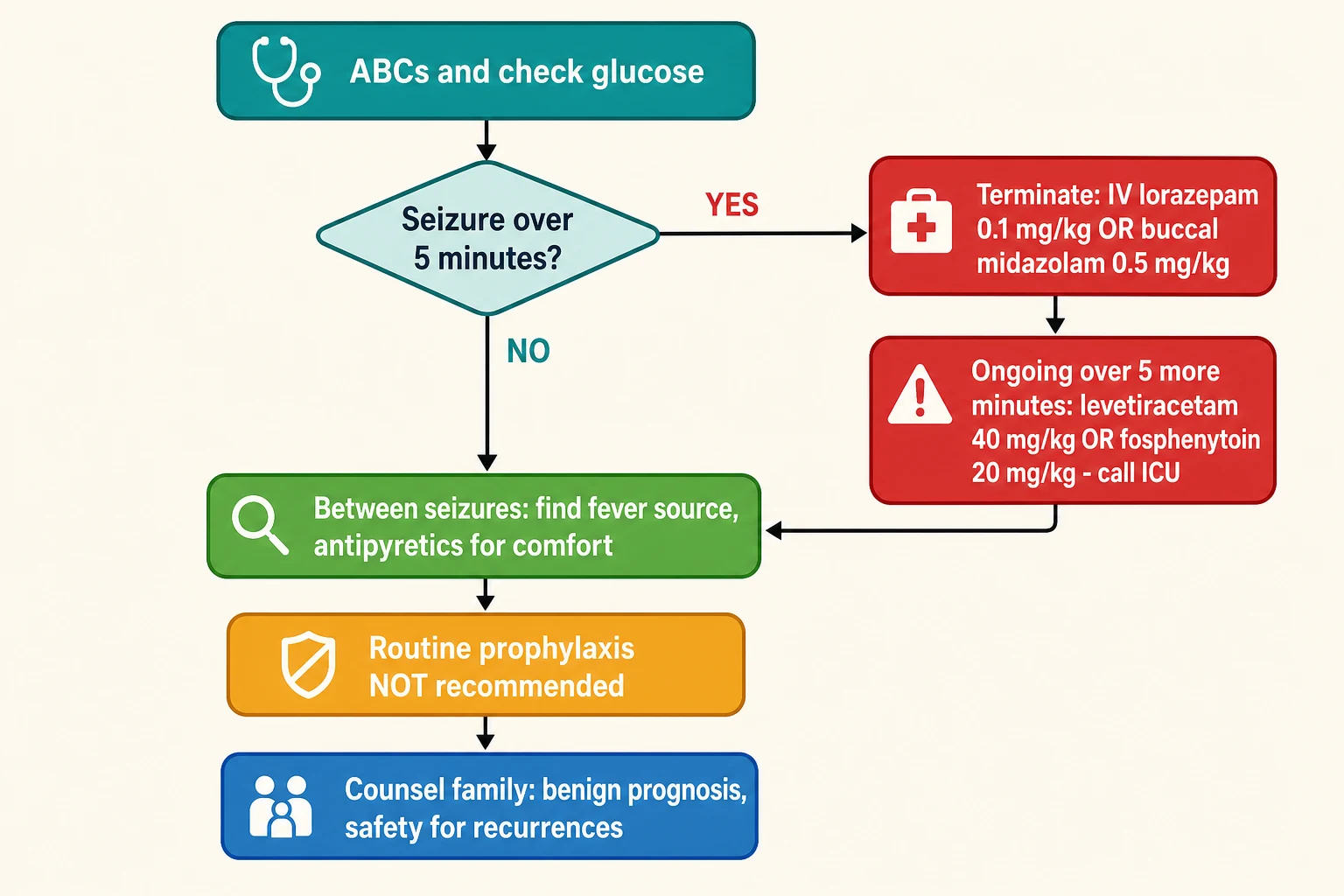
First-line termination is a benzodiazepine. Where intravenous access is available, give intravenous lorazepam at 0.1 mg/kg, to a maximum of 4 mg, repeated once after five minutes if needed. Where intravenous access is difficult, as it often is in a convulsing toddler, buccal midazolam at 0.5 mg/kg to a maximum of 10 mg is effective and was shown by the McIntyre randomised trial to terminate seizures at least as well as rectal diazepam. Rectal diazepam at 0.5 mg/kg to a maximum of 20 mg remains an option where no other route is available. [4] [1]
STOP-FIT
A convulsion that persists despite two doses of a benzodiazepine is refractory and demands second-line therapy and senior help. Intravenous levetiracetam at 40 mg/kg (maximum 2.5 g) or intravenous fosphenytoin at 20 mg PE/kg are the standard second-line agents for convulsive status epilepticus, and the child should be managed in a high-dependency or intensive care setting with preparation for airway support. A febrile convulsion lasting over 30 minutes is febrile status epilepticus, a neurocritical emergency that carries a risk of hippocampal injury. [1] [8]
Buccal midazolam
Dose
0.5 mg/kg (max 10 mg); may repeat once after 10 minutes
In parallel with termination, identify and treat the fever source, give antipyretics for comfort, and decide on disposition. Antipyretics (paracetamol 15 mg/kg or ibuprofen 10 mg/kg) relieve the child's distress but, critically, do not prevent a further febrile seizure. This distinction, between comfort and prevention, is the cornerstone of the counselling that follows. [6] [2]
Management — Definitive & Stepwise
Once the acute convulsion has terminated and the diagnosis of a simple febrile seizure is secure, the definitive management is built around three evidence-based decisions: do not prescribe continuous antiepileptic prophylaxis, do not prescribe intermittent prophylaxis routinely, and do not use antipyretics as prevention. Each of these has been tested and each has been found wanting. [2] [5]
Continuous prophylaxis with phenobarbitone, primidone, or valproate does reduce recurrence, but at the cost of substantial harms. Phenobarbitone causes hyperactivity, irritability, and impaired cognition and behaviour in up to a third of children; valproate carries a risk of fatal hepatotoxicity, thrombocytopenia, and (in later life) teratogenicity. The American Academy of Pediatrics 2008 guideline concludes that the potential harms of continuous prophylaxis outweigh the benefits for simple febrile seizures, and the 2021 Cochrane review reaches the same conclusion. [2] [5]
The life arc of a febrile seizure and its management
Intermittent oral diazepam given during fever does reduce recurrence, but the effect is small and the harms are real: ataxia, lethargy, and sedation that can mask a serious illness and erode a family's confidence in managing fever. For these reasons intermittent oral diazepam is not recommended for the routine child with simple febrile seizures. The exception is the child with prolonged or frequent recurrences, for whom a rescue benzodiazepine (buccal midazolam or rectal diazepam) given at the onset of a convulsion is a pragmatic and evidence-supported strategy that keeps the family out of hospital and shortens the seizure. [5] [4]
The antipyretic question is the single most common parental request and the single most common misconception. Rosenbloom and colleagues showed in their systematic review and meta-analysis that antipyretics, whether paracetamol or ibuprofen, given during a febrile illness do not prevent the recurrence of febrile seizures compared with placebo. Antipyretics are given to make the child comfortable, not to prevent another seizure, and families who understand this are spared the needless anxiety of believing that each fever must be aggressively suppressed to avert a convulsion. [6]
Specific Subtypes & Scenarios
Complex febrile seizures account for about 30 per cent of febrile seizures and carry a higher recurrence rate and a higher subsequent epilepsy risk than simple febrile seizures. The management shifts toward a more thorough evaluation: an electroencephalogram and neuroimaging are considered, and a longer period of observation is reasonable. A rescue benzodiazepine plan is offered to the family. The complex features, taken together with any developmental or neurological abnormality and the family history, allow the epilepsy risk to be quantified and the counselling to be tailored. [1] [11]
Febrile status epilepticus is a febrile convulsion lasting over 30 minutes and is the most severe end of the febrile seizure spectrum. It is a neurocritical emergency that requires urgent termination, second-line anticonvulsants, and intensive care. The FEBSTAT study established that febrile status epilepticus is associated with acute hippocampal injury, detectable as hippocampal swelling on magnetic resonance imaging, which in a proportion of children progresses to hippocampal sclerosis and temporal lobe epilepsy. Human herpesvirus 6 and 7 are over-represented as precipitants. [8] [10]
Generalised epilepsy with febrile seizures plus (GEFS+) is the bridge between febrile seizures and the genetic epilepsies. It describes a family in which affected members have febrile seizures that extend beyond the usual age window, together with afebrile generalised seizures of varying severity. It is commonly linked to SCN1A mutations, and the recognition matters because the severe end of the spectrum includes Dravet syndrome. A child with febrile seizures that persist beyond age 5, with developmental delay, or with a family history of severe epilepsy should trigger consideration of a genetic epilepsy rather than reassurance. [3]
The first febrile seizure outside the age window is, by definition, not a febrile seizure. A convulsion with fever under 6 months demands exclusion of serious bacterial infection, inborn errors of metabolism, and structural lesions, with a low threshold for lumbar puncture and septic workup. A convulsion with fever over 5 years is an afebrile seizure disorder with an incidental fever or a provoked seizure, and needs an epilepsy and provoking-cause evaluation. Holding the age boundary is the single most important safeguard against misdiagnosis. [1] [2]
Complications & Pitfalls
The complications of the convulsion itself are uncommon but important. A prolonged convulsion can cause hypoxia, aspiration, or injury, and febrile status epilepticus carries a risk of acute hippocampal injury and later temporal lobe epilepsy. Recurrence is common rather than dangerous: about one in three children will have another febrile seizure, and this is a source of family anxiety rather than of neurological harm. Simple febrile seizures do not cause brain damage, cognitive impairment, behavioural disturbance, or excess mortality, and this reassurance is central to the consultation. [2] [8]
The risks that drive the consultation
The avoidable pitfalls are clinical and well described. The first is missing meningitis or encephalitis by accepting a convulsion with fever as a simple febrile seizure in a child who is ill-looking, outside the age window, or not back to baseline. The second is over-investigating a straightforward simple febrile seizure with unnecessary blood tests, imaging, or admission. The third is prescribing prophylaxis, whether continuous antiepileptics or intermittent diazepam, against the evidence. The fourth is reinforcing the antipyretic misconception, leaving families to chase fevers aggressively and live in fear of the next convulsion. [1] [6]
A subtler pitfall is failing to recognise a genetic epilepsy behind the mask of recurrent or atypical febrile seizures. A child with prolonged or hemiconvulsive febrile seizures, developmental delay or regression, or a family history of severe epilepsy may have SCN1A-related disease such as Dravet syndrome, where some antiepileptics (notably sodium-channel agents) can worsen seizures. Early recognition allows appropriate genetic testing and the avoidance of harmful drugs. [3]
Prognosis & Disposition
The prognosis of simple febrile seizures is excellent and is the foundation of the consultation. The seizure does not cause neurological damage, and the child's cognition, behaviour, and mortality are no different from those of unaffected children. About one in three children will have a recurrence, and the recurrence risk is highest in the year after the first seizure and in children whose first seizure occurred under 12 months of age. The lifetime risk of subsequent epilepsy after a simple febrile seizure is around 2 to 5 per cent, only marginally above the background. [2] [7]
The prognosis shifts with complex features. A complex febrile seizure, a pre-existing neurological or developmental abnormality, and a family history of epilepsy each raise the subsequent epilepsy risk, and febrile status epilepticus carries a meaningfully higher risk of temporal lobe epilepsy linked to hippocampal sclerosis. These risks are quantified at the bedside and shared with the family so that the counselling is accurate rather than uniformly reassuring. [8] [11]
Disposition after a simple febrile seizure is usually discharge home with a clear safety-net. The child who has fully recovered, in whom the diagnosis is secure and meningitis excluded, and whose family understands the prognosis and the rescue plan does not need admission. Admission is reserved for the child with a complex seizure, a prolonged or incompletely resolved convulsion, an ill appearance, an uncertain diagnosis, or social circumstances that make safe discharge impossible. Every family leaves with a written plan covering what to do during a recurrence and when to call an ambulance. [1] [2]
Follow-up is with the general practitioner for most children, with paediatric outpatient review reserved for complex seizures, recurrent or prolonged attacks, developmental concerns, or an atypical picture suggesting a genetic epilepsy. The family is taught that fever is to be managed for comfort, that antipyretics do not prevent seizures, and that a recurrence, while frightening, is expected in a minority and is not harmful. [6]
Special Populations
Infants under 12 months deserve particular attention because their meningeal signs are unreliable and their risk of serious bacterial infection is higher. The 2011 American Academy of Pediatrics guideline sets a lower threshold for lumbar puncture in the 6 to 12 month age group, particularly when immunisation against Haemophilus influenzae type b or Streptococcus pneumoniae is incomplete or the child has received prior antibiotics. A well-looking, fully immunised infant with a clear fever source and full recovery can still be managed conservatively, but the index of suspicion for meningitis is held higher than in the older child. [1] [12]
Children with developmental or neurological abnormalities sit at the higher-risk end of the febrile seizure spectrum. A pre-existing abnormality is one of the strongest predictors of subsequent epilepsy, and these children are more likely to have complex features and to warrant electroencephalogram, neuroimaging, and closer follow-up. The reassuring message given to the family of a typically developing child is tempered here by an honest discussion of the elevated epilepsy risk. [2] [11]
Aboriginal and Torres Straiter Islander children, and children in rural and remote settings, may present to services with reduced access to rapid paediatric and neurology input. Culturally safe communication, the use of retrieval networks, and telehealth consultation support equitable care. The principles of management are unchanged, but the threshold for transfer and the reliance on structured safety-netting are higher when distance separates the family from specialist services. [1]
Children from migrant, refugee, and asylum-seeking families, and those facing socioeconomic disadvantage, may have incomplete immunisation records, language barriers, and lower health literacy around fever and seizures. A trained interpreter, written information in the family's language, and a clear, simple rescue plan are essential. The diagnosis and the management are identical, but the communication effort is greater, and the consequences of a missed meningitis or an unnecessary prophylactic prescription are amplified by inequity. [12]
Evidence, Guidelines & Regional Differences
| Region | Key guidance | Acute termination | Long-term strategy |
|---|
The principal controversies have largely been resolved by the evidence, and a candidate should know where the field has settled and where uncertainty remains. The case against continuous and intermittent prophylaxis is settled: the harms outweigh the benefits for simple febrile seizures. The case against antipyretics as prevention is settled. The remaining uncertainty concerns the long-term consequences of febrile status epilepticus, where the FEBSTAT study has established a link to hippocampal injury and temporal lobe epilepsy but where the magnitude of the risk and the role of surveillance imaging are still being defined. [8] [9]
The most common point of genuine practice variation is the preferred rescue benzodiazepine and its route. The McIntyre randomised trial established buccal midazolam as at least as effective as rectal diazepam and better accepted by families, and buccal midazolam has become the preferred community rescue in Australasia and the United Kingdom. Rectal diazepam remains in use where buccal midazolam is unavailable, and intranasal midazolam is an emerging alternative. The dose, 0.5 mg/kg buccal midazolam to a maximum of 10 mg, is the one number a candidate must carry into the examination. [4]
Exam Pearls
References
- [1]Subcommittee on Febrile Seizures, American Academy of Pediatrics Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics, 2011.PMID 21285335
- [2]Steering Committee on Quality Improvement and Management, Subcommittee on Febrile Seizures, American Academy of Pediatrics Febrile seizures: clinical practice guideline for the long-term management of the child with simple febrile seizures. Pediatrics, 2008.PMID 18519501
- [3]Baumann RJ Technical report: treatment of the child with simple febrile seizures. Pediatrics, 1999.PMID 10353983
- [4]McIntyre J, Robertson S, Norris E, Appleton R, Whitehouse WP, Phillips B, Martland T, Berry K, Collier J, Smith S, Choonara I Safety and efficacy of buccal midazolam versus rectal diazepam for emergency treatment of seizures in children: a randomised controlled trial. Lancet, 2005.PMID 16023510
- [5]Offringa M, Newton R, Nevitt SJ, Vraka K Prophylactic drug management for febrile seizures in children. Cochrane Database Syst Rev, 2021.PMID 34131913
- [6]Rosenbloom E, Finkelstein Y, Adams-Webber T, Kozer E Do antipyretics prevent the recurrence of febrile seizures in children? A systematic review of randomized controlled trials and meta-analysis. Eur J Paediatr Neurol, 2013.PMID 23702315
- [7]Berg AT, Shinnar S Predictors of recurrent febrile seizures: a metaanalytic review. J Pediatr, 1990.PMID 2137875
- [8]Lewis DV, Voyvodic J, Shinnar S, Chan S, Bello JA, Moshe SL, Nordli DR Jr, Frank LM, Pellock JM, Hesdorffer DC, et al, FEBSTAT Study Team Hippocampal sclerosis and temporal lobe epilepsy following febrile status epilepticus: The FEBSTAT study. Epilepsia, 2024.PMID 38606600
- [9]Hesdorffer DC, Shinnar S, Lewis DV, Moshe SL, Nordli DR Jr, Pellock JM, et al, FEBSTAT study team Design and phenomenology of the FEBSTAT study. Epilepsia, 2012.PMID 22742587
- [10]Epstein LG, Shinnar S, Hesdorffer DC, Nordli DR, Hamidullah A, Benn EK, et al, FEBSTAT study team Human herpesvirus 6 and 7 in febrile status epilepticus: the FEBSTAT study. Epilepsia, 2012.PMID 22954016
- [11]Hesdorffer DC, Shinnar S, Lax DN, Pellock JM, Nordli DR Jr, Seinfeld S, et al, FEBSTAT study team Risk factors for subsequent febrile seizures in the FEBSTAT study. Epilepsia, 2016.PMID 27265870
- [12]Kimia AA, Capraro AJ, Hummel D, Johnston P, Harper MB Utility of lumbar puncture for first simple febrile seizure among children 6 to 18 months of age. Pediatrics, 2009.PMID 19117854