Paeds · neurology-neurodisability-and-neuromuscular
First seizure and seizure mimics
Also known as First afebrile seizure in a child · First unprovoked seizure · New-onset seizure in childhood · Seizure versus syncope and other mimics · First fit in a child · Psychogenic non-epileptic events in children
Fellowship guide to the child who presents after a possible first seizure: the first question is not what caused it but whether it was a seizure at all, because syncope, breath-holding spells, parasomnias and psychogenic non-epileptic events account for a large share of referrals and are harmed by antiseizure drugs. For a true first unprovoked seizure the work turns to seizure type by the 2017 ILAE classification, a focused cause search (EEG, neuroimaging, bloods), an honest recurrence-risk conversation, and the decision of whether to start daily treatment or wait — while never forgetting that an ongoing convulsion of five minutes or more is status epilepticus and needs a benzodiazepine now.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The organising idea of this topic is that the child after a first event is managed along three questions, in order: was it a seizure, what type and cause, and does it need a drug today. The first question is the one candidates most often skip, and it is the one that does the most harm when answered wrongly — because labelling a non-epileptic event as epilepsy exposes a child to unnecessary investigations, driving restrictions, stigma, and the cognitive and teratogenic burden of antiseizure medication. [9] [10]
This page covers the ILAE definition of epilepsy and its 2017 classification of seizure types, the recurrence risk after a first unprovoked seizure, the seizure-versus-mimic decision at the bedside, the tiered investigation strategy, the resuscitation of status epilepticus, and the shared decision about starting treatment. It links to the epilepsy syndromes, febrile seizures, syncope and status epilepticus leaves for the syndromic, febrile, cardiovascular and emergency-management depth that each demands. [1] [7]
Overview & Definition
A seizure is the transient occurrence of signs or symptoms produced by abnormal excessive or synchronous neuronal activity in the brain. The clinician at the bedside rarely sees the seizure itself — the event is usually over by the time the child arrives — so the diagnosis rests almost entirely on the account of a witness, ideally supplemented by a home video. [9] A provoked seizure is one driven by a transient systemic or metabolic insult such as fever, electrolyte disturbance, hypoglycaemia, head trauma, drug withdrawal or central nervous system infection; an unprovoked seizure occurs in the absence of such a trigger, and it is the unprovoked event that opens the epilepsy pathway. [4]
Epilepsy, by the 2014 ILAE practical definition, is a disease of the brain defined by any one of three conditions: two or more unprovoked seizures occurring more than twenty-four hours apart; a single unprovoked seizure with a recurrence risk of at least sixty per cent over the next ten years; or a recognised epilepsy syndrome. [2] The clinical consequence is that a single unprovoked seizure is not, by itself, epilepsy — the threshold for the diagnosis is high, deliberately, to protect children from a label that carries driving, occupational, insurance and psychosocial weight.
The practical corollary is that the first consultation after a possible seizure has two diagnostic aims. The first is to decide whether the event was epileptic; the second, only if it was, is to classify it and search for a cause. Jumping to the cause before settling the nature of the event is the single most common reason that a child is started on an antiseizure drug for a mimic. [9]
Classification
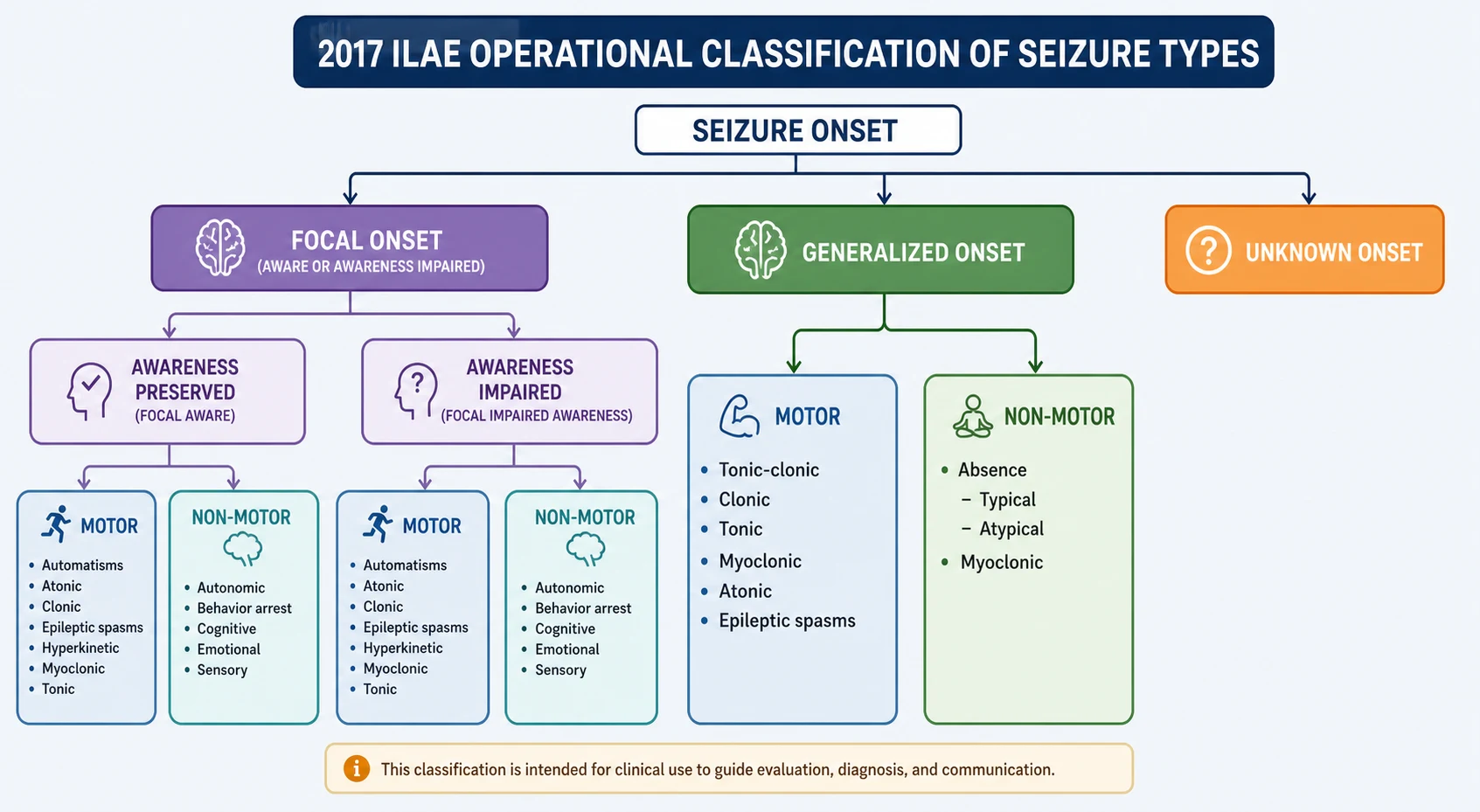
The 2017 ILAE operational classification is built around seizure onset. A focal seizure begins in one hemisphere, in a discrete neuronal network, and may occur with awareness preserved or with impaired awareness; it may have motor features (automatisms, clonic, tonic, atonic) or non-motor features (sensory, autonomic, cognitive, emotional), and it may evolve to a bilateral tonic-clonic seizure. [1] A generalised seizure engages bilateral distributed networks from the outset and is divided into motor types — tonic-clonic, clonic, tonic, myoclonic, atonic and epileptic spasms — and non-motor types, which are the absence seizures. A seizure of unknown onset is named as such until further information reclassifies it.
[4]Febrile seizures occupy a separate category and are the most common seizure entity of early childhood, affecting two to five per cent of children between six months and five years. A simple febrile seizure is generalised, lasts under fifteen minutes, does not recur within twenty-four hours, and occurs in a neurologically normal child; it needs no routine neuroimaging, electroencephalogram or lumbar puncture in a child who has recovered. [8] A complex febrile seizure is focal, prolonged beyond fifteen minutes, or recurrent within the same febrile illness, and it carries a higher risk of later epilepsy — a risk that rises further with each complex feature present. [12]
Epidemiology & Risk Factors
Seizures are among the most common reasons a child is brought to emergency care. The incidence of a first unprovoked seizure is highest in the first year of life, falls through childhood, and rises again in late adulthood. Roughly four to ten per cent of all children experience at least one afebrile seizure by adolescence, and around one per cent develop epilepsy. [4]
The recurrence risk after a first unprovoked seizure is the single number that governs the treatment decision, and it is not uniform. The baseline risk across all children is around forty to fifty per cent over two years, and it clusters around a small number of predictors: an epileptiform electroencephalogram, an abnormal neurological examination or developmental status, a structural lesion on imaging, a seizure that occurred during sleep, and a focal seizure type. [7] A child with several of these features carries a recurrence risk above sixty per cent and meets the ILAE definition of epilepsy after a single event; a child with none carries a risk nearer thirty per cent and is usually managed by waiting. [2]
Pathophysiology
A seizure arises when a population of cortical neurons loses its normal balance between excitation and inhibition and begins to fire in a hypersynchronous, excessive burst. In a focal seizure the discharge begins in a discrete network and may stay local or spread; in a generalised seizure it engages thalamocortical networks bilaterally from the outset, which is why the clinical onset is abrupt and symmetric. [1]
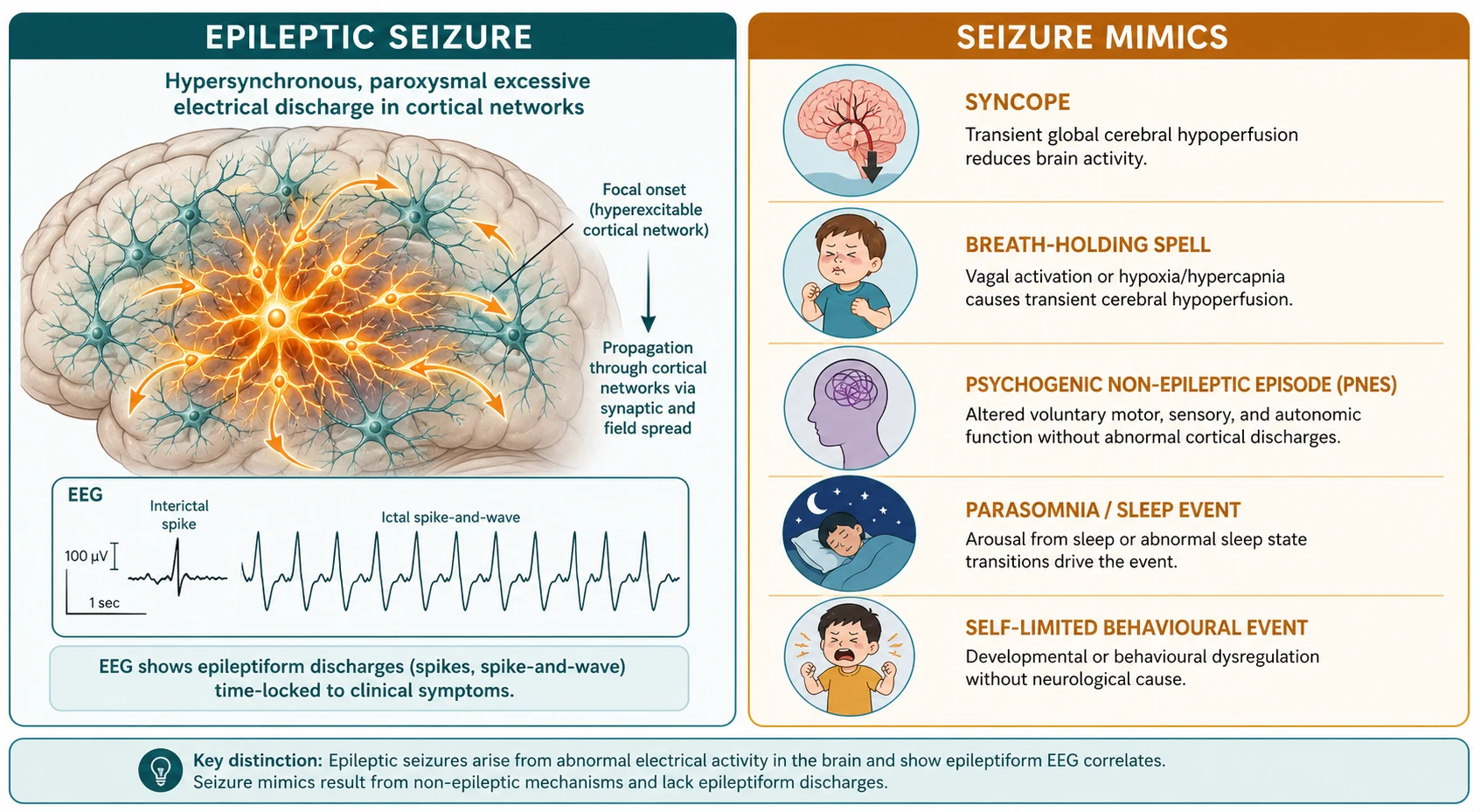
The mimics are valuable to understand mechanistically because the mechanism explains the distinguishing feature. Syncope is a transient global reduction in cerebral perfusion, which is why it is brief, upright-triggered, pale, and followed by rapid full recovery. A breath-holding spell is an intense autonomic, vagally mediated reflex in an infant or toddler provoked by crying, which is why it is cyanotic or pallid, precipitated by minor frustration, and ends with a brief loss of tone and rapid return to normal. [9] Psychogenic non-epileptic seizures are involuntary episodes of altered behaviour or movement generated by psychological distress rather than cortical epileptic discharge, which is why the motor pattern is atypical and variable, the eyes are closed with active resistance to opening, and there is no postictal confusion. [10]
Clinical Presentation
The clinical presentation of a first seizure is almost always a historical account rather than an observed event, so the quality of the history determines the quality of the diagnosis. A good history is taken from every available witness and is structured around the pre-ictal, ictal and post-ictal phases. The pre-ictal phase establishes the setting, any trigger or precipitant, the posture of the child, and any warning or aura. The ictal phase establishes the onset (focal versus generalised from the start), the evolution, the duration, the motor pattern, the state of awareness, and any automatisms, incontinence or tongue-biting. The post-ictal phase establishes the recovery — a true seizure is followed by a period of confusion, drowsiness or focal deficit such as Todd's paresis that resolves over minutes to hours. [9]
The features that favour an epileptic seizure over a mimic are a stereotyped onset, loss of awareness, an abrupt start and offset, a witnessed motor pattern of tonic or clonic activity, lateral tongue-biting, urinary incontinence, cyanosis, and a postictal phase of confusion or focal deficit. The features that favour a mimic are pallor preceding collapse, an upright or situational trigger, a brief duration with rapid complete recovery, eyes that are closed and resist opening, a waxing-and-waning rather than rhythmic motor pattern, recall of the event, and absence of a postictal state. [9] A home video is the single most useful investigation for the seizure-versus-mimic question, and parents should be asked to film any further events. [10]
Differential Diagnosis
The differential diagnosis of a first seizure is the differential of any sudden paroxysmal event in a child, and it is wide. The common mimics to be able to name and distinguish at the bedside are syncope, breath-holding spells, parasomnias, psychogenic non-epileptic seizures, migraine variants, Sandifer syndrome, benign paroxysmal vertigo, self-stimulatory or behavioural events, shuddering attacks, sleep myoclonus, tics and stereotypies, and rigors. [9]
True seizure versus the common mimics
Vasovagal syncope is the most frequent mimic in school-age children and adolescents. The attack is triggered by prolonged standing, heat, emotion or venepuncture, is preceded by prodromal pallor, nausea, blurred vision and ringing in the ears, lasts only seconds, and recovers fully within a minute. A cardiogenic syncope — from a long-QT channelopathy, hypertrophic cardiomyopathy or an arrhythmia — is suggested by syncope during exercise, on immersion in water, in response to a loud noise, or with a family history of sudden death in the young, and it demands an electrocardiogram before any other test. [9]
Breath-holding spells affect up to five per cent of infants and toddlers. The cyanotic type follows a brief period of crying that ends in breath-holding, cyanosis and loss of tone; the pallid type is a vagally mediated reflex, often after a minor head bump, that produces sudden pallor and limpness. Both resolve spontaneously within a minute and are benign, though an iron-deficiency screen is worthwhile because anaemia is associated with spells and treatment can reduce their frequency. [9]
Psychogenic non-epileptic seizures are the most important mimic to recognise in older children and adolescents, because they are commonly misdiagnosed as refractory epilepsy and exposed to escalating antiseizure drugs. The events are involuntary and distress-driven, not feigned, and are associated with anxiety, depression, trauma, family psychiatric illness and school difficulties. [10] The diagnosis is confirmed by video-electroencephalogram capture of a typical event with preserved conscious rhythm and no epileptiform correlate, and the treatment is cognitive behavioural therapy, not an antiseizure drug. [10]
Clinical & Bedside Assessment
The bedside assessment begins with the question of whether the child has returned to their normal conscious state. A child who is still drowsy, focal, or not at baseline is managed as an emergency: secure the airway, check the blood glucose, treat any ongoing seizure, and consider central nervous system infection. A child who has fully recovered moves to the structured history and examination. [4]
The first-seizure history
Establish that the child is back to baseline; if not, manage as an emergency and exclude hypoglycaemia and ongoing seizure.
Take a minute-by-minute account from every witness, covering the pre-ictal setting, the ictal onset and evolution, the duration, and the postictal recovery.
Ask specifically for triggers (fever, sleep deprivation, flickering light), for prior events that may have been missed, and for a family history of epilepsy, febrile seizures or sudden death.
Ask the family to video any further event — a home video resolves the seizure-versus-mimic question more often than any investigation.
Examine for neurocutaneous stigmata, focal neurology, developmental status, head circumference and signs of raised intracranial pressure.
The examination looks for three things. The first is a focal neurological deficit or a failure to return to baseline, which demands urgent imaging. The second is the stigmata of an underlying cause — the cafe-au-lait macules and axillary freckling of neurofibromatosis type 1, the hypopigmented ash-leaf macules and facial angiofibromas of tuberous sclerosis, the facial port-wine stain of Sturge-Weber syndrome, and the microcephaly, macrocephaly or dysmorphism that point to a structural or genetic cause. The third is the developmental and neurological baseline, because a child with established neurodisability or developmental delay has both a higher recurrence risk and a different differential, and the baseline establishes the post-event comparison. [4]
Investigations
The investigation strategy is selective and built around the nature of the event rather than ordered as a blanket panel. The American Academy of Neurology practice parameter for the child with a first nonfebrile seizure recommends a routine electroencephalogram and limits blood tests, glucose measurement and toxicology to children with specific indications, and reserves neuroimaging for the child with a focal deficit, a focal seizure, an abnormal electroencephalogram, or who has not returned to baseline. [4]
[4]The electroencephalogram is the highest-yield investigation after a first unprovoked seizure, both to classify the seizure type and to refine the recurrence risk. Population-based data show that an epileptiform abnormality is found in around half of recordings taken within twenty-four hours of a first seizure, and that the yield rises with sleep deprivation, with repeat recording, and when the study is done early. [6] A normal electroencephalogram does not exclude epilepsy, and an abnormal one does not prove it — the result is always interpreted in the clinical context. [6]
Neuroimaging is not needed for every child. A child with an idiopathic generalised epilepsy phenotype, a normal examination, a generalised seizure and a diagnostic electroencephalogram with a normal background does not require imaging. Magnetic resonance imaging is indicated for a focal seizure, a focal electroencephalogram or examination, a child who has not returned to baseline, and any child under two years or with developmental delay, because the yield of a treatable structural lesion is higher in these groups. Computed tomography is reserved for the emergency setting where a rapid structural or vascular cause must be excluded before magnetic resonance imaging is possible. [4]
Management — Resuscitation
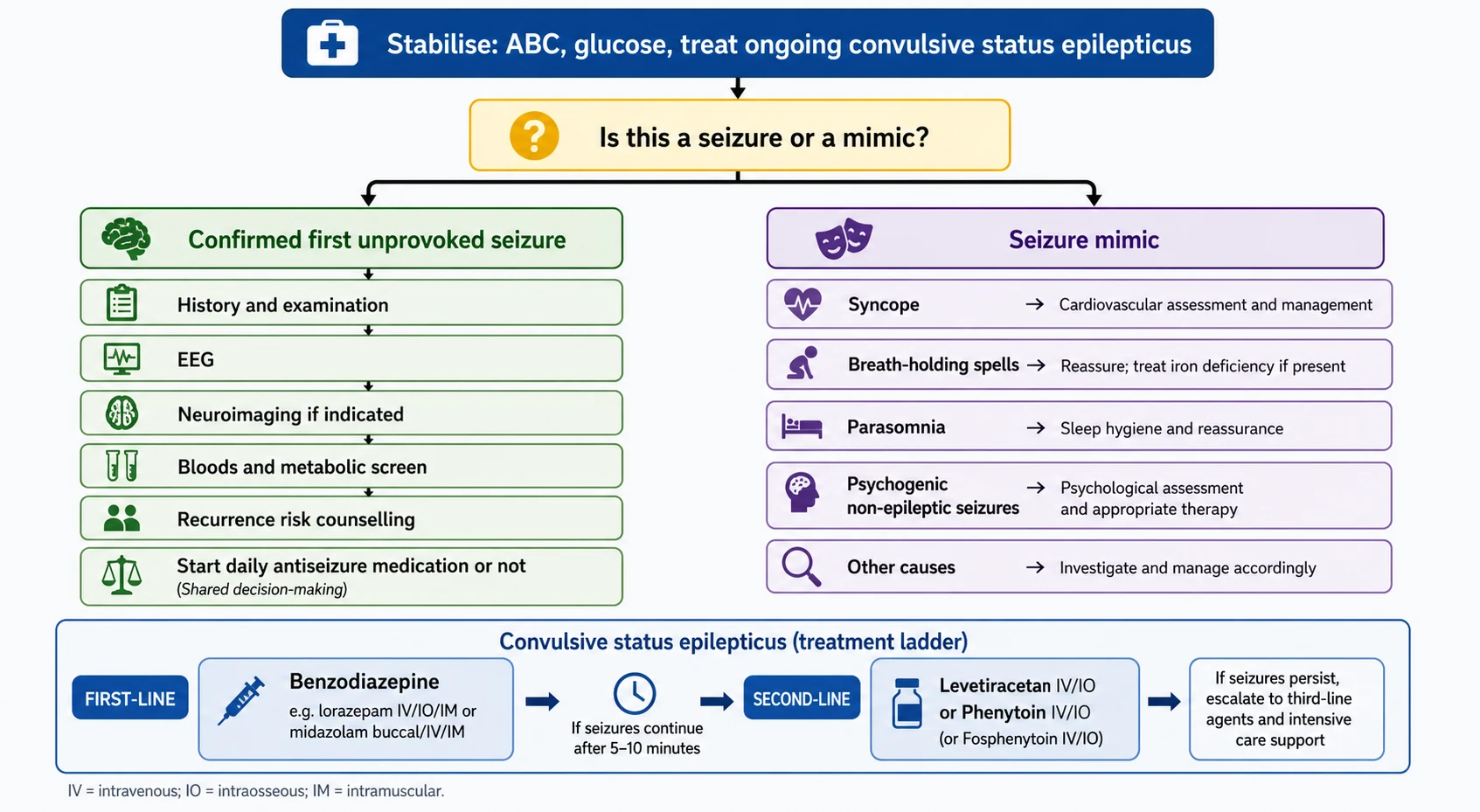
The one resuscitation scenario in this topic is the child who is still convulsing when they arrive, or who convulses again in the department. A convulsive seizure that has lasted five minutes or more meets the operational definition of convulsive status epilepticus, and the threshold exists because seizure termination becomes progressively less likely and neuronal injury progressively more likely the longer a convulsion runs. [3]
First-line treatment is a benzodiazepine. Intravenous lorazepam at 0.1 mg/kg, to a maximum of 4 mg, is the agent of choice when intravenous access is available, repeated once after five to ten minutes if the convulsion continues. When intravenous access cannot be obtained, buccal midazolam or intranasal midazolam is effective and avoids the delay of cannulating a convulsing child; rectal diazepam remains an option where the other routes are unavailable. [3] If the convulsion persists beyond a second benzodiazepine dose, a second-line agent is given — intravenous levetiracetam at 40 mg/kg to a maximum of 3 g, or intravenous fosphenytoin or phenytoin at 20 mg per kilogram. A large randomised trial in children found levetiracetam to be a safe and equivalent alternative to phenytoin for second-line treatment, which has shifted practice toward levetiracetam. [11]
Management — Definitive & Stepwise
Once the child has recovered and the event is confirmed as a first unprovoked seizure, the definitive decision is whether to start a daily antiseizure medication now or to wait for a recurrence. The decision is shared with the family and turns on the recurrence risk, the burden of a further seizure, and the risks of treatment. [7]
The American Academy of Neurology practice parameter concludes that treatment of a first unprovoked seizure reduces the risk of a second seizure in the short term but does not improve the long-term prognosis for seizure remission, which is why most clinicians advise waiting unless the recurrence risk is high. [5] Starting treatment is reasonable when the recurrence risk exceeds sixty per cent — which itself meets the definition of epilepsy — or when a further seizure would carry grave consequences, as for an adolescent driving or a child with a structural lesion. [2] When the decision is to wait, the family receives first-aid and safety advice, a plan for any recurrence, and clear safety-netting about when to return. [7]
Levetiracetam (broad-spectrum first-line antiseizure medication)
Dose
10 mg/kg orally twice daily, titrate to 30 mg/kg twice daily (adult max 1500 mg twice daily)
Counselling is part of treatment whether or not a drug is started. The family is taught first aid for a seizure — placing the child on their side, protecting the head, not putting anything in the mouth, and calling for help if a convulsion lasts five minutes. Recreational safety is addressed, particularly bathing, swimming, cycling and heights. When a diagnosis of epilepsy is made, the risk of sudden unexpected death in epilepsy is discussed honestly but proportionately, because it is low in childhood and higher in uncontrolled symptomatic epilepsies. [7]
Specific Subtypes & Scenarios
The febrile child deserves a separate assessment. A simple febrile seizure in a child who has recovered needs no investigation beyond the evaluation of the fever itself, and the family is reassured about the benign prognosis and the small risk of recurrence. [8] A complex febrile seizure — focal, prolonged, or recurrent within the same illness — is investigated for the cause of the fever, may warrant an electroencephalogram or imaging, and is reviewed for the higher risk of later epilepsy that rises with each complex feature. [12] A child who has not recovered, who is meningeal, or whose conscious level is falling is investigated for meningitis or encephalitis with a lumbar puncture, and the febrile label is withheld until central nervous system infection is excluded.
The infant presenting with a first seizure warrants particular care, because the differential includes inborn errors of metabolism, structural malformations of cortical development, and the early-onset epilepsy syndromes. Hypoglycaemia, hypocalcaemia and pyridoxine-dependent epilepsy are reversible causes that must be sought actively in an infant with seizures, and the work-up is broader and more urgent than in an older child. [4]
The adolescent with recurrent events that do not look like epilepsy is the scenario in which psychogenic non-epileptic seizures are most often missed. The clinician takes a careful psychosocial history, looks for the features of a non-epileptic event, and arranges video-electroencephalogram monitoring to capture a typical attack before committing to or escalating an antiseizure drug. The diagnosis is delivered with compassion and without stigma — the events are real and involuntary — and the path to recovery is psychological therapy. [10]
Complications & Pitfalls
The complications of a first seizure fall into two groups: the harm of the seizure itself and the harm of mislabelling it. The seizure may cause injury from a fall, aspiration, or prolonged convulsion; status epilepticus carries the risk of neuronal injury, respiratory compromise and, rarely, death. The harm of mislabelling is subtler and often larger — a child labelled with epilepsy for a mimic is exposed to unnecessary drugs, restrictions, stigma, investigations and anxiety, and a child with a missed treatable cause loses the window for early intervention. [9]
The diagnostic pitfalls cluster around the seizure-versus-mimic decision. Syncope is mislabelled as a seizure when the brief convulsive jerks of cerebral hypoperfusion — the myoclonic jerks that follow a faint — are taken for a generalised tonic-clonic seizure. Breath-holding is mislabelled when the colour change and brief loss of tone are not recognised. Parasomnias are mislabelled when stereotyped nocturnal events of frontal lobe epilepsy are dismissed as night terrors. And psychogenic events are mislabelled when the atypical motor pattern, the closed resisting eyes and the rapid recovery are not weighed against the diagnosis. [9] The investigative pitfalls are imaging every child, ordering an electroencephalogram without a sleep record or a repeat when the first is normal, and over-interpreting a single non-specific electroencephalogram abnormality as proof of epilepsy. [6]
Prognosis & Disposition
The prognosis of a first unprovoked seizure is, for most children, excellent. Around half will have a second seizure, and of those who do, most will enter remission; starting an antiseizure drug early reduces the short-term recurrence rate but does not change the long-term chance of becoming seizure-free. [5] The prognosis is least favourable in the child with a structural lesion, an abnormal neurological examination, developmental delay, or a focal epileptiform electroencephalogram, all of which raise both the recurrence risk and the chance of persistent epilepsy. [7]
The disposition is shared care. A child with a confidently diagnosed, low-risk first unprovoked seizure and a normal work-up can return to their general paediatrician or primary care with safety-netting advice and a plan for any recurrence. A child with a high recurrence risk, an abnormal electroencephalogram or imaging, an unclear diagnosis, or features of an epilepsy syndrome is referred to paediatric neurology. A child with a suspected psychogenic non-epileptic seizure is referred to the neurology and child psychology services for video-electroencephalogram confirmation and cognitive behavioural therapy. [10]
Special Populations
Children with neurodisability, developmental delay or a complex chronic neurological condition carry a higher recurrence risk after a first seizure and a broader differential, and their baseline examination is the benchmark against which any postictal change is judged. The seizure may be the first recognised manifestation of an underlying syndrome, the work-up is more likely to reveal a structural or metabolic cause, and the family often already navigates a complex care plan that the new diagnosis must be integrated into. [4]
Children in out-of-home care, in youth justice settings, and from migrant, refugee and socioeconomically disadvantaged backgrounds carry a higher burden of the psychosocial adversity that drives psychogenic non-epileptic seizures, and they may have limited access to the specialist video-electroencephalogram monitoring and psychological therapy that the diagnosis requires. [10] Trauma-informed assessment, attention to the social history, and equitable access to paediatric neurology and mental health services are the priority, because a misdiagnosis of refractory epilepsy in this group compounds existing disadvantage with the burden of unnecessary treatment.
Evidence, Guidelines & Regional Differences
The evidence base is anchored by the International League Against Epilepsy classification and definition papers — the 2017 operational classification of seizure types and the 2014 practical clinical definition of epilepsy — and by the American Academy of Neurology practice parameters on the evaluation and treatment of a first unprovoked seizure in children. [1] [2] [4] [5] The status epilepticus definition and the second-line treatment evidence come from the ILAE task force and from the ConSEPT trial comparing levetiracetam with phenytoin in children. [3] [11]
Regional and ethnic variation matters in this topic. Indigenous Australian, Maori and Pacific children, and children from migrant and refugee backgrounds, face barriers to specialist assessment, electroencephalogram access and psychological services, and carry a higher burden of the adversity associated with psychogenic non-epileptic events. [10] Controversies persist around the threshold for neuroimaging after a first seizure, the role of repeat electroencephalography, and the place of early antiseizure medication, but the consensus that a single unprovoked seizure is usually managed by waiting — unless the recurrence risk is high — is stable across guidelines. [5]
Exam Pearls
Three rules that mark a fellowship answer
The high-yield minutiae an examiner rewards: the operational threshold for status epilepticus is five minutes; the ILAE definition of epilepsy is two unprovoked seizures, or one with a recurrence risk of at least sixty per cent; the benzodiazepine first-line for status is intravenous lorazepam at 0.1 mg/kg to a maximum of 4 mg; buccal or intranasal midazolam is the no-access route; the second-line agent is levetiracetam at 40 mg/kg to a maximum of 3 g or fosphenytoin or phenytoin at 20 mg per kilogram; the electroencephalogram shows epileptiform activity in around half of first-seizure recordings; a simple febrile seizure needs no routine investigation; and psychogenic non-epileptic seizures are treated with cognitive behavioural therapy, not an antiseizure drug. [3] [11]
References
- [1]Fisher RS; Cross JH; French JA; et al Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology Epilepsia, 2017.PMID 28276060
- [2]Fisher RS; Acevedo C; Arzimanoglou A; et al ILAE official report: a practical clinical definition of epilepsy Epilepsia, 2014.PMID 24730690
- [3]Trinka E; Cock H; Hesdorffer D; et al A definition and classification of status epilepticus--Report of the ILAE Task Force on Classification of Status Epilepticus Epilepsia, 2015.PMID 26336950
- [4]Hirtz D; Ashwal S; Berg A; et al Practice parameter: evaluating a first nonfebrile seizure in children: report of the quality standards subcommittee of the American Academy of Neurology, The Child Neurology Society, and The American Epilepsy Society Neurology, 2000.PMID 10980722
- [5]Hirtz D; Berg A; Bettis D; et al Practice parameter: treatment of the child with a first unprovoked seizure: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society Neurology, 2003.PMID 12552027
- [6]Baldin E; Hauser WA; Buchhalter JR; et al Yield of epileptiform electroencephalogram abnormalities in incident unprovoked seizures: a population-based study Epilepsia, 2014.PMID 25041095
- [7]Haut SR; Shinnar S Considerations in the treatment of a first unprovoked seizure Semin Neurol, 2008.PMID 18777475
- [8]Subcommittee on Febrile Seizures Neurodiagnostic evaluation of the child with a simple febrile seizure Pediatrics, 2011.PMID 21285335
- [9]Leibetseder A; Eisermann M; LaFrance WC Jr; et al How to distinguish seizures from non-epileptic manifestations Epileptic Disord, 2020.PMID 33399092
- [10]Doss J Psychogenic non-epileptic seizures in youth: Individual and family psychiatric characteristics Front Psychiatry, 2022.PMID 36590633
- [11]Dalziel SR; Borland ML; Furyk J; et al Levetiracetam versus phenytoin for second-line treatment of convulsive status epilepticus in children (ConSEPT): an open-label, multicentre, randomised controlled trial Lancet, 2019.PMID 31005386
- [12]Berg AT; Shinnar S Complex febrile seizures Epilepsia, 1996.PMID 8635422