Paeds · neurology-neurodisability-and-neuromuscular
Headache and migraine in children
Also known as Paediatric migraine · Childhood migraine · Migraine without aura in children · Migraine with aura in children · Tension-type headache in children · Primary headache in children · Chronic migraine in children
Fellowship guide to headache and migraine in children: the ICHD-3 criteria that separate migraine from tension-type headache, the primary-versus-secondary decision driven by the SNNOOP red flags, the acute abortive pathway built around ibuprofen and paracetamol with a triptan for moderate-to-severe attacks, the prophylaxis ladder that begins with lifestyle and cognitive behavioural therapy and confronts the CHAMP trial finding that amitriptyline and topiramate are no better than placebo, and the trap of medication-overuse headache.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the 11-year-old who has missed a day of school each fortnight for a year with a throbbing headache, nausea, and a need to lie in a dark room, and whose mother is now asking whether she needs a brain scan. That child carries the whole teaching point of paediatric headache: the diagnosis is almost always clinical, the workup is selective, and the management is built on lifestyle and behavioural medicine more than on drugs. The single most important first question is not which drug to give but whether the headache is primary or secondary, because missing a secondary cause is the catastrophic error and over-investigating a primary headache is the common one. [1] [2]
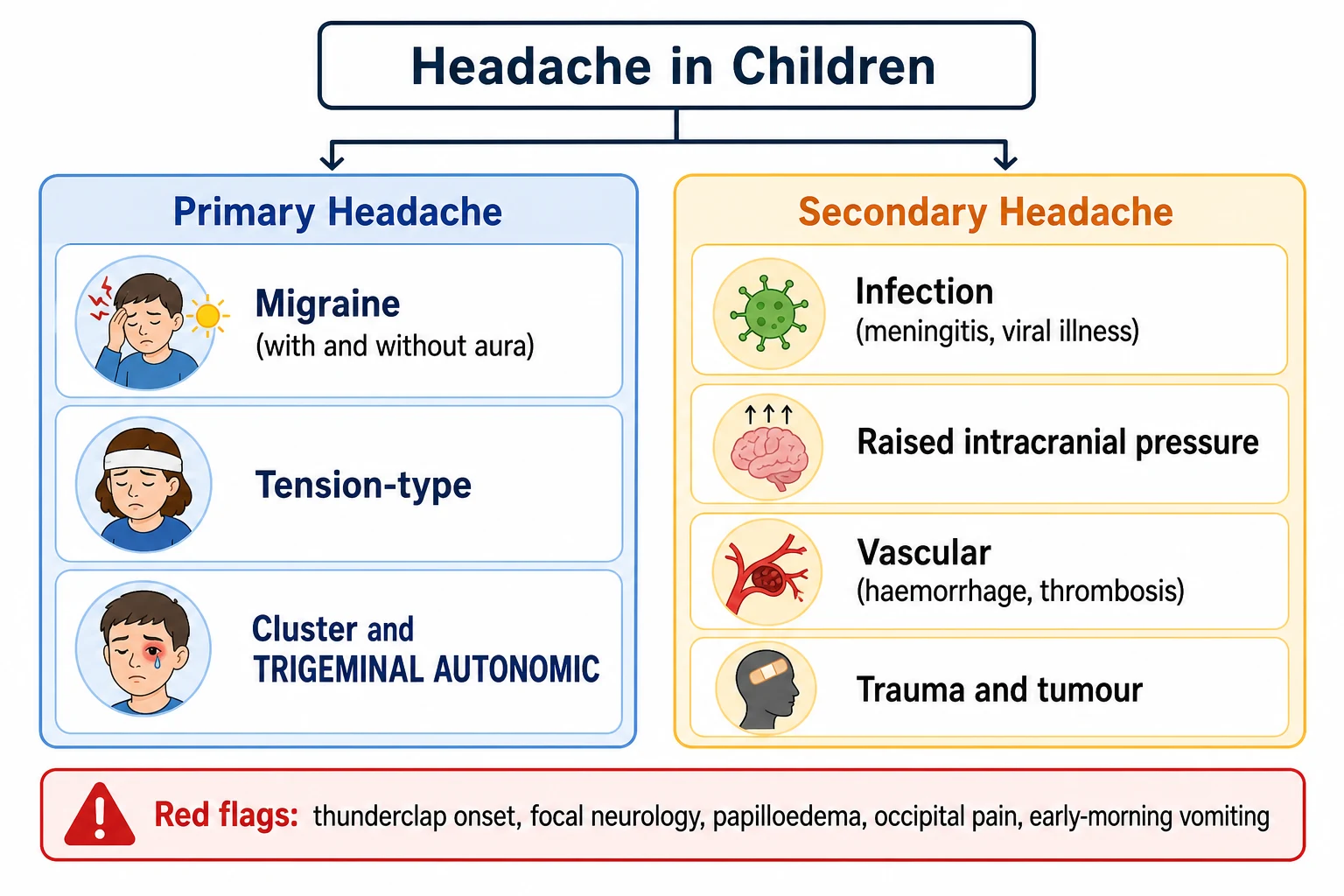
A headache is primary when it is the disease itself, and migraine and tension-type headache together account for the overwhelming majority of recurrent paediatric headache. Migraine is defined by the ICHD-3 as at least five attacks of headache lasting two to 72 hours with characteristic features, while tension-type headache is bilateral, pressing, mild to moderate, and lacks the nausea and aggravation that define migraine. A headache is secondary when it is a symptom of another disorder, whether infection, raised intracranial pressure, a vascular event, or a tumour, and the red-flag screen exists to separate these two worlds. [1]
Recurrent headache is common. The systematic review by Abu-Arafeh and colleagues put the overall prevalence of headache in children and adolescents at around 60 per cent over the preceding year and the prevalence of migraine at between 5 and 15 per cent, rising steeply through adolescence. Girls overtake boys after puberty, and the burden falls disproportionately on adolescents, who lose school days and quality of life to attacks that are often untreated. The challenge for the clinician is to make the diagnosis confidently, to exclude the dangerous minority, and to resist the reflex to scan every head that hurts. [2]
Classification
Classifying a paediatric headache begins with the primary-versus-secondary split, because it determines whether the next step is a management plan or an investigation. Once a headache is confirmed as primary, the ICHD-3 framework distinguishes migraine from tension-type headache and from the rarer trigeminal autonomic cephalalgias, and within migraine it separates attacks with and without aura. The features that drive this classification are the pain quality, the duration, the location, the accompanying symptoms, and the response to activity. [1]
Migraine without aura requires at least five attacks, each lasting two to 72 hours, with a throbbing quality, moderate or severe intensity, and aggravation by routine activity, accompanied by nausea or vomiting or by both photophobia and phonophobia. Migraine with aura adds fully reversible visual, sensory, language, or motor symptoms that develop over five minutes and last up to an hour, with a visual aura of scintillating scotoma or fortification spectra being the most common in children. The two share the same underlying biology and the same management, so the aura distinction matters for the diagnosis and for counselling, but it does not change the acute or preventive plan. [1]
Migraine (without aura)
ICHD-3
- At least 5 attacks lasting 2 to 72 hours
- Throbbing, moderate or severe, worse with activity
- Nausea or vomiting, or photophobia with phonophobia
- Often bilateral and frontotemporal in children
- Photophobia and phonophobia may be inferred from behaviour
Tension-type headache
ICHD-3
- Bilateral, pressing or tightening, non-throbbing
- Mild to moderate, not worsened by activity
- No nausea; photophobia or phonophobia but not both
- Lasts 30 minutes to 7 days
- Often the harder diagnosis to separate from migraine in children
Secondary headache
red flag
- Thunderclap onset, occipital location, or focal deficit
- Early-morning vomiting or papilloedema
- Progressive pattern or systemic features
- New headache in a child under 5 years
- Demands neuroimaging, not a diagnosis of migraine
A child with migraine differs from an adult in three testable ways. The attacks are shorter, lasting as little as two hours rather than the four-hour minimum of adult migraine. The pain is more often bilateral, especially in younger children, with the more recognisable unilateral, one-sided pain emerging through adolescence. And the accompanying features are more often expressed through behaviour, so a child who seeks a dark, quiet room and refuses food is showing photophobia and phonophobia even without the vocabulary to name them. Occipital pain, by contrast, is rare in primary paediatric migraine and should prompt imaging to exclude a posterior fossa lesion. [1]
Epidemiology & Risk Factors
Headache is one of the most common somatic complaints of childhood. The systematic review by Abu-Arafeh and colleagues pooled population-based studies and found that around 60 per cent of children and adolescents report a headache in the preceding year, that 5 to 15 per cent meet criteria for migraine, and that 15 to 20 per cent report frequent or recurrent tension-type headache. The prevalence of migraine rises with age, from a few per cent in primary-school children to its peak in late adolescence, and the sex ratio inverts around puberty: boys predominate before puberty and girls predominate after it, tracking the hormonal surge of menarche. [2]
A strong family history is the single most important risk factor. Migraine is highly heritable, and the child of a parent with migraine has a substantially higher risk of migraine than the general population, which is both a diagnostic clue and a counselling point when a parent recognises their own attacks in the child's story. Identified triggers cluster around sleep disruption, dehydration, skipped meals, stress, screen time, and the menstrual cycle, and recognising them is the first step of the lifestyle foundation of management. [12]
The numbers that anchor your viva
The transformation from episodic to chronic migraine is the pathway the clinician most wants to interrupt. Chronic migraine is defined as 15 or more headache days a month for over three months, of which at least eight have migrainous features, and the principal driver of that transformation in children is medication-overuse headache. A child taking acute medication on 10 or more days a month for triptans or 15 or more days a month for simple analgesics, sustained over months, is on the path to chronification, which is why an analgesic diary is part of every headache consultation. [1] [12]
Pathophysiology
Migraine is a disorder of brain excitability and sensory processing, not, as once taught, primarily a disorder of blood vessels. The attack begins in a brain whose threshold for activation is lowered, so that ordinary sensory input, a flashing light, a skipped meal, a change in sleep, becomes sufficient to trigger a cascade that ends in throbbing pain and nausea. Understanding this shift from the old vascular model to the modern neurovascular model matters because it explains why treatment aims at the brain and the trigeminovascular system rather than at vessel calibre alone. [1]
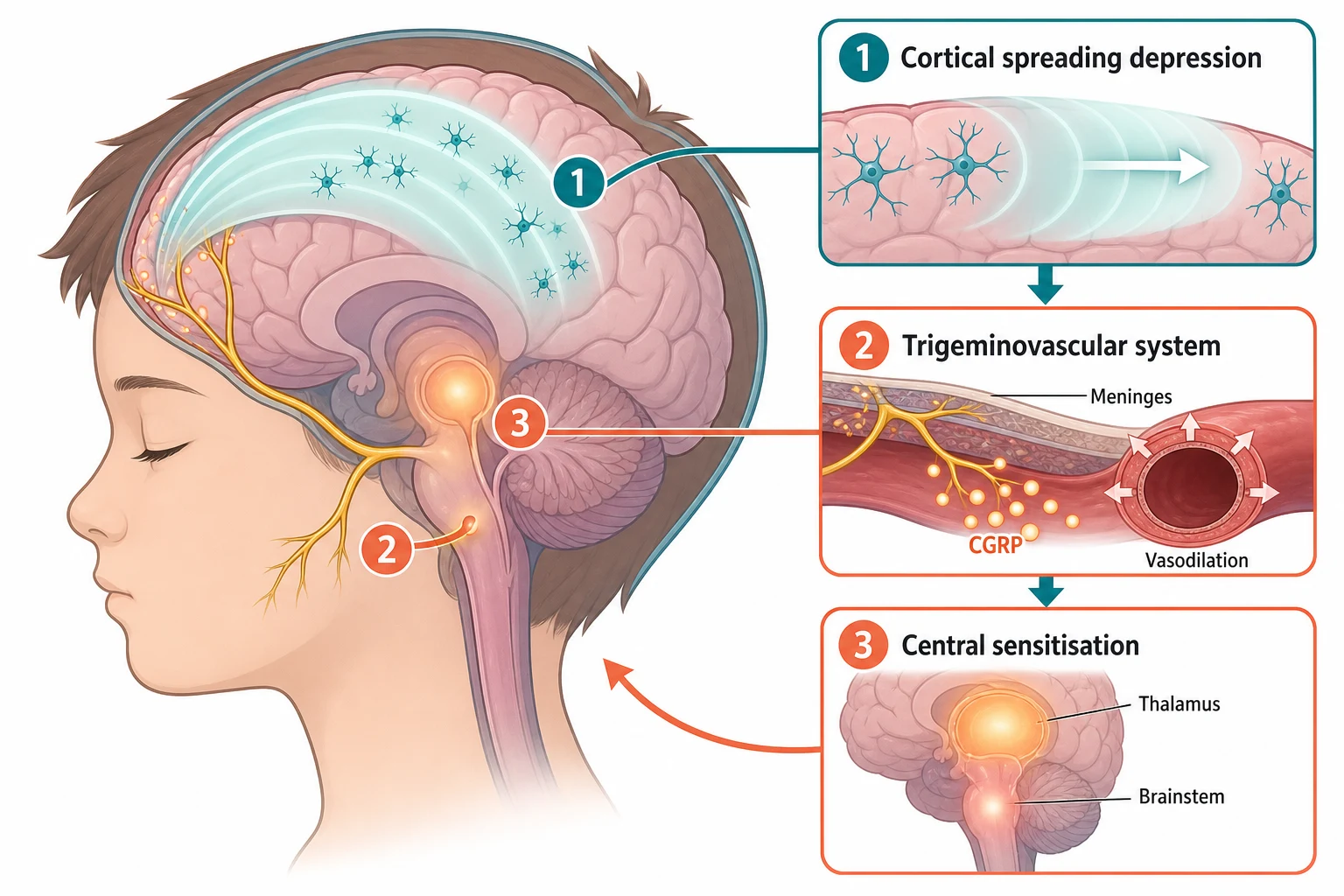
Three converging mechanisms produce an attack. Cortical spreading depression, a slow wave of depolarisation that spreads across the cortex, is thought to underlie the aura and to activate the trigeminovascular system. The trigeminovascular system, the network of nerves from the brainstem to the meninges and their vessels, releases inflammatory neuropeptides, chief among them calcitonin gene-related peptide (CGRP), which produces vasodilation and sensitises the pain pathway. And central sensitisation, the amplification of pain signalling at the brainstem and thalamus, is why light, sound, and movement become painful during an attack and why the headache throbs. [1]
[1]The high placebo response that defines paediatric migraine trials, and that explains the CHAMP trial result, has its own biology. The developing brain appears to mount a robust expectation-driven analgesic response, so that children on placebo report large reductions in headache days. This is not a nuisance of trial design but a real phenomenon, and it is part of why non-pharmacological interventions, lifestyle medicine and cognitive behavioural therapy, perform so well in children and form the foundation of prophylaxis. [6] [7]
Clinical Presentation
The typical story is a school-aged child or adolescent who describes a throbbing headache that builds over an hour, settles in the frontotemporal region, and forces them to stop their activity and lie still in a dark, quiet room. Nausea is common, vomiting may occur, and light and sound become unpleasant. The attack lasts a few hours and resolves with sleep, and the child is entirely well between attacks. In younger children the picture is less articulate: the child may be irritable, pale, withdrawn, or simply stop playing, and the photophobia and phonophobia are inferred from the seeking of a dark, quiet place. [1]
A child with migraine with aura describes a visual disturbance that precedes the headache, classically a shimmering zig-zag or scintillating scotoma that expands over several minutes and resolves within an hour, after which the headache begins. Less commonly the aura is sensory, with tingling spreading across one side, or dysphasic. The aura is fully reversible, and any fixed neurological deficit is not an aura but a red flag demanding imaging. A family history of migraine with aura strengthens the diagnosis. [1]
| Clinical picture | What it implies | Act |
|---|
The two histories that most change the plan are the frequency history and the analgesic history. A child having four or more headache days a month, or whose headaches are disabling their school and social life, crosses the threshold at which prophylaxis is considered. And a child taking acute medication on two or three days a week or more is at risk of medication-overuse headache, the single most reversible cause of a worsening primary headache. Asking how many days a week the child takes painkillers is the highest-yield question in the follow-up consultation. [1] [12]
Differential Diagnosis
The first differential question is which primary headache this is, because migraine and tension-type headache overlap in children and the boundary is sometimes blurred. Migraine is throbbing, moderate to severe, worse with activity, and accompanied by nausea or photo-phonophobia, while tension-type headache is pressing, mild to moderate, bilateral, and lacking the nausea and aggravation of migraine. A child with features of both is given the diagnosis that best fits the most disabling attacks, because the management of frequent headache of either type rests on the same lifestyle and behavioural foundation. [1]
The second and dangerous question is whether this is a secondary headache, and the red-flag screen exists to answer it. The SNNOOP framework names the features that demand investigation: systemic symptoms such as fever and weight loss, a history of neoplasia, a neurological deficit or depressed consciousness, a sudden or thunderclap onset, an older or very young age at first presentation, and a change in the headache pattern. In children, occipital location, a headache that wakes the child from sleep or is worse on waking with early-morning vomiting, papilloedema, ataxia, and a progressive course are added red flags that point to raised intracranial pressure or a posterior fossa lesion. [1]
Migraine
- Throbbing, moderate or severe, worse with activity
- Nausea, photophobia, phonophobia
- Fully well between attacks
- Family history common
- Normal examination, no red flags
Tension-type headache
- Bilateral, pressing, mild to moderate
- No nausea, not worsened by activity
- Often school-related, stress-linked
- Normal examination
- Lifestyle and stress management
Secondary headache
- Thunderclap, occipital, or focal deficit
- Early-morning vomiting, papilloedema
- Progressive or new under age 5
- Systemic features or altered consciousness
- Neuroimaging before any diagnosis of migraine
Headache mimic
- Sinusitis with facial tenderness and discharge
- Refractive error with squinting and eye strain
- Post-concussive headache after head injury
- Dental or temporomandibular pain
- Resolved by the targeted history and examination
A thunderclap headache, reaching maximum intensity within one minute, is subarachnoid haemorrhage until proven otherwise and is never a primary migraine. A child with a focal neurological deficit that does not resolve, with papilloedema, with ataxia, or with a depressed conscious state has a secondary headache and needs urgent neuroimaging. The migraine aura is the one element of primary headache that mimics a deficit, and the distinction is duration and reversibility: an aura resolves within an hour, a fixed deficit does not, and any deficit lasting beyond an hour warrants imaging. [1]
Clinical & Bedside Assessment
The headache history is the diagnosis. Ask when the headaches started, how often they occur and for how long, where they are and what they feel like, how severe they are and what brings them on, and what the child does during an attack. A child who seeks a dark, quiet room and stops eating is describing photophobia, phonophobia, and nausea through behaviour. Ask about triggers, about school attendance and the impact on daily life, and specifically about how many days a week the child takes acute medication. Record the family history of headache and migraine, and ask about recent head injury, infection, or visual change. [1]
The red-flag screen is a deliberate act, not an afterthought. Ask whether the headache has ever reached full severity within one minute, whether it is ever occipital, whether it wakes the child from sleep or is worse on waking, whether there is early-morning vomiting, and whether there has been any change in vision, balance, coordination, personality, or school performance. A single positive answer shifts the consultation from a management plan to an investigation pathway. [1]
[1]Examination confirms the absence of red flags. Check the blood pressure, examine the optic fundi for papilloedema, test the visual fields and acuity, and perform a full neurological examination including gait and coordination. Feel the sinuses and temporal-mandibular joints, examine the teeth, and look for signs of infection. A normal neurological examination in a child whose history meets the ICHD-3 criteria and whose red-flag screen is negative confirms a primary headache and closes the investigation loop. An abnormality in any of these is an indication for imaging. [1]
Investigations
The guiding principle for a primary paediatric headache is that neuroimaging is not routine. A child whose history meets the ICHD-3 criteria for migraine or tension-type headache, whose red-flag screen is negative, and whose neurological examination is normal does not need a scan, a blood test, or an electroencephalogram. Over-investigation of primary headache exposes children to radiation, generates incidental findings that increase anxiety, and delays the lifestyle and behavioural plan that is the real treatment. [1]
Neuroimaging is reserved for the child with a red flag. Magnetic resonance imaging is the preferred modality for a suspected posterior fossa lesion, a chiari malformation, or raised intracranial pressure, while computed tomography is reserved for the acute thunderclap or the child who needs an urgent image to exclude haemorrhage. An abnormal fundus with papilloedema is an indication for imaging and, where available, opening pressure measurement. Blood pressure measurement is part of every headache assessment because hypertension is a treatable secondary cause. [1]
The selective investigation pathway
Full headache history and ICHD-3 criteria; count headache days and analgesic days per week
Deliberate red-flag screen (SNNOOP: thunderclap, occipital, focal deficit, papilloedema, early-morning vomiting, progressive, under 5 years)
Blood pressure, fundoscopy, visual acuity and fields, full neurological examination including gait
Neuroimaging only if a red flag is present or the examination is abnormal
No routine blood tests, EEG, or imaging for a primary headache that meets criteria
PedMIDAS disability score to quantify the impact on school and daily life
The disability assessment is the investigation that belongs in every recurrent headache consultation. The Pediatric Migraine Disability Assessment, or PedMIDAS, is a six-item tool that quantifies the impact of headache on school, home, play, and social life over the preceding three months, and it guides the threshold for prophylaxis. A score in the moderate or severe range, alongside a frequency of four or more headache days a month, shifts the plan from acute treatment alone toward a stepped preventive approach. [1]
Management — Resuscitation
The acute attack is the moment the family needs a drug that works, and the evidence points clearly to a simple first step. Ibuprofen at 10 mg per kg or paracetamol at 15 mg per kg, given early in the attack while the pain is still building, is first-line acute treatment for paediatric migraine. The 2016 Cochrane review by Richer and colleagues found that ibuprofen and paracetamol are the best-supported acute agents, with a number needed to treat of around three for ibuprofen and around five for paracetamol to achieve two-hour pain freedom. [8]
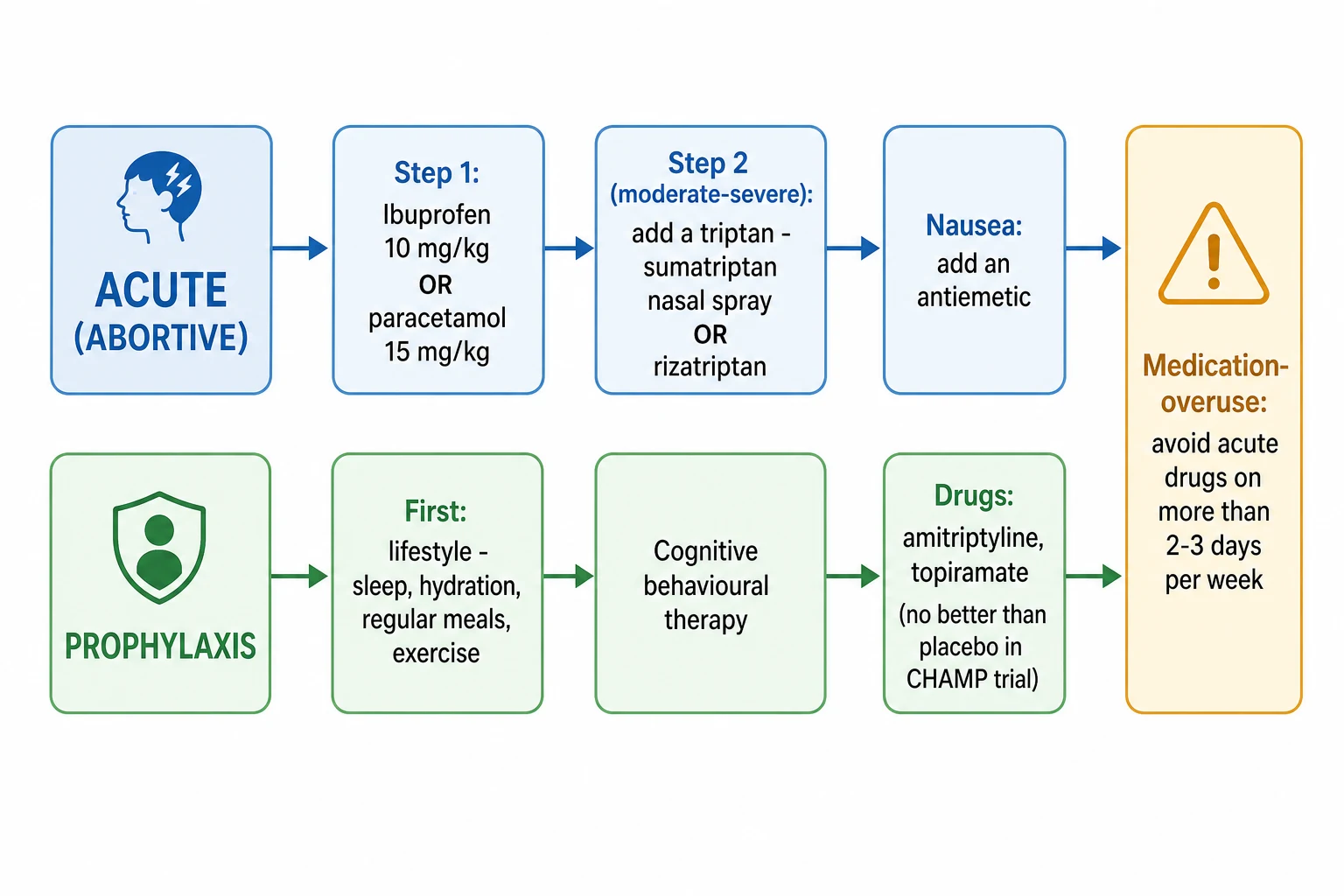
For the moderate-to-severe attack that does not respond to simple analgesia, a triptan is added. Sumatriptan nasal spray at 10 to 20 mg for adolescents, or rizatriptan as a dispersible tablet, are the triptans with the strongest paediatric evidence, supported by the trials of Ho and colleagues for rizatriptan and McDonald and colleagues for the sumatriptan and naproxen combination. Oral sumatriptan alone has weaker evidence in children than in adults, and the nasal and dispersible routes are preferred. An antiemetic such as ondansetron or domperidone is added when nausea or vomiting is prominent. [9] [10] [11]
HEAD-SMART
Two principles govern acute treatment. The first is that the dose is given early, because an analgesic taken while the pain is still building works far better than one taken once the attack is established. The second is restraint, because the road to medication-overuse headache is paved with daily analgesia. Opioids and codeine have no place in routine paediatric migraine: they are ineffective, sedating, and carry a high risk of dependence and overuse, and their prescription is a marker of a plan that has gone wrong. A child needing acute medication on two or three days a week or more is a child heading toward medication-overuse headache and toward a preventive plan, not toward stronger acute drugs. [1] [12]
Management — Definitive & Stepwise
Once the acute plan is in place, definitive management is built on a stepped foundation that begins with what is not a drug. Regular sleep, adequate hydration, meals that are not skipped, daily exercise, and the recognition and avoidance of triggers form the lifestyle platform on which everything else rests. The prospective cohort by Casanova and colleagues reinforced that embracing these protectors and adhering to healthy lifestyle recommendations is associated with fewer headache days in episodic migraine, and these interventions are effective, safe, and free. [12]
For the child with frequent or chronic migraine, cognitive behavioural therapy is the most effective single addition. The randomised trial by Powers and colleagues showed that cognitive behavioural therapy added to amitriptyline roughly halved the days of headache and the disability score compared with headache education added to amitriptyline in children and adolescents with chronic migraine. The effect is durable, and it positions behavioural therapy not as an adjunct but as a core treatment that outperforms drug alone. [7]
The stepped management arc of paediatric migraine
Drug prophylaxis is reserved for the child with four or more headache days a month or significant disability whose lifestyle and behavioural plan has not controlled the attacks. The two most-studied drugs are amitriptyline, given at night, and topiramate, titrated to a target weight-based dose, and the 2019 American Academy of Neurology and American Headache Society guideline frames these as options to consider. The framing matters because of the CHAMP trial, which found that neither amitriptyline nor topiramate was superior to placebo for paediatric migraine, a result driven by an exceptionally high placebo response of up to 60 per cent. Propranolol and the calcium-channel blocker flunarizine are alternatives used in some regions, with propranolol avoided in asthma. [4] [6]
The meta-analysis by El-Chammas and colleagues had earlier suggested a benefit for several preventive agents over placebo, but the CHAMP trial, with its rigorous blinding and large sample, reset expectations. The fellowship-correct position is that drug prophylaxis is tried when the lifestyle and behavioural platform has been built and the attacks remain disabling, that the family is counselled on the high placebo response and the uncertain drug benefit, and that the response is judged over eight to twelve weeks before a drug is continued, switched, or weaned. The goal is a return to function and school, not a headache-free child. [5] [6]
Specific Subtypes & Scenarios
Migraine with aura shares the acute and preventive plan of migraine without aura, and the aura itself needs no specific treatment because it resolves within an hour. The counselling point is the reversibility: an aura that persists, that produces a fixed deficit, or that is accompanied by a depressed conscious level is not an aura but a secondary event and demands imaging. The diagnostic value of aura is that it strengthens a diagnosis of migraine and often aligns with a family history of migraine with aura. [1]
Chronic migraine, defined as 15 or more headache days a month for over three months with at least eight migrainous days, is the point at which the preventive plan is intensified and the search for medication-overuse headache becomes urgent. The combination of cognitive behavioural therapy with a preventive drug is the evidence-based approach, drawn from the Powers trial, and referral to a paediatric neurology or headache service is appropriate when the chronic pattern is established or disabling. Reversal of medication overuse is often the single most effective intervention. [7]
Status migrainosus, a debilitating migraine attack lasting beyond 72 hours, is the acute severe end of the spectrum. The emergency management includes hydration, an antiemetic such as metoclopramide or prochlorperazine, a non-steroidal anti-inflammatory, and, in selected cases, an intravenous agent such as a dopamine antagonist or a low-dose ketamine infusion under specialist guidance. A child with status migrainosus needs assessment to exclude a secondary cause and is managed with senior paediatric and neurology input. [8]
Medication-overuse headache is the most common reason a primary headache becomes chronic, and it is the most reversible. The diagnostic threshold is acute medication on 10 or more days a month for triptans or 15 or more days a month for simple analgesics, sustained for over three months, in a child with a primary headache disorder. The treatment is weaning the offending analgesic, building the lifestyle and behavioural platform, and introducing cognitive behavioural therapy, with a preventive drug considered if the chronic pattern persists. Recognising it is the key, because no preventive drug works while daily analgesia continues. [1] [12]
Complications & Pitfalls
The complications of migraine are the complications of an untreated or over-treated disease rather than of the headache itself. A child whose attacks are poorly controlled loses school days, falls behind academically, withdraws from friends and sport, and develops anxiety and low mood, and these are the disabilities that the PedMIDAS captures and that the management plan exists to reverse. Status migrainosus brings acute dehydration, pain, and the need for emergency care. The most preventable complication is medication-overuse headache, which is iatrogenic and entirely reversible once recognised. [1] [12]
The risks that drive the consultation
The avoidable pitfalls are well described. The first is missing a secondary cause by accepting a thunderclap, an occipital headache, or a focal deficit as a primary migraine, which is the catastrophic error. The second is over-investigating a clear primary headache with unnecessary imaging, blood tests, or referrals, which is the common error and the one that increases anxiety and delays treatment. The third is prescribing drug prophylaxis before building the lifestyle and behavioural platform, which over-medicalises a condition whose foundation is behavioural. The fourth is failing to recognise medication-overuse headache, leaving a child on escalating analgesia with a worsening headache. [1]
A subtler pitfall is expecting a preventive drug to work as it does in adults. The CHAMP trial showed that the paediatric placebo response is so high that established adult preventives fail to separate from placebo in children, and a clinician who prescribes amitriptyline or topiramate expecting a clear adult-style benefit sets up the family for disappointment and the child for unnecessary drug exposure. The realistic goal of drug prophylaxis in a child is modest and is built on the behavioural foundation, not on the drug alone. [6] [4]
Prognosis & Disposition
The prognosis of paediatric migraine is good and is the foundation of the consultation. Most children improve over time with a structured plan, and many outgrow or substantially reduce their attacks through adolescence, though migraine persists into adulthood for a substantial proportion. The attacks do not damage the brain, and the child's cognition and development are unaffected by migraine itself. The disability that migraine causes is functional and reversible, which is why the management plan is built on return to school and daily life rather than on the absence of headache. [1] [2]
The prognosis shifts with frequency, disability, and medication overuse. A child with episodic migraine, a normal examination, and an intact lifestyle platform has an excellent outlook, while a child with chronic migraine, high disability on the PedMIDAS, and daily analgesia has a course that is harder but still reversible once the medication overuse is addressed and the behavioural plan is built. The family is counselled that the goal is control and function, not cure, and that relapses during stress, sleep disruption, or examination periods are expected and manageable. [7] [12]
Disposition after a first or follow-up consultation for primary headache is to the general practitioner or paediatric outpatient service with a written acute plan, a headache diary, and a follow-up PedMIDAS. Admission is reserved for status migrainosus, for the child in whom a secondary cause is being actively excluded, or for the rare refractory case needing intravenous therapy. Every family leaves with a clear plan covering what to do during an attack, how to avoid medication overuse, and when to return. [1]
Special Populations
Adolescent girls deserve particular attention because migraine peaks in this group after menarche, menstrual triggers are prominent, and the risk of medication-overuse headache rises with the frequent use of over-the-counter analgesia. A menstrual migraine diary, the recognition of perimenstrual triggers, and the avoidance of daily combination analgesics are the key interventions, and the contraceptive choices that interact with migraine prophylaxis are discussed where relevant. [2] [12]
Children with disability and neurodiversity may struggle to articulate the quality and location of their pain, so the behavioural signs of photophobia, phonophobia, and nausea take on greater diagnostic weight, and the assessment of disability relies more on carer report and observation. The lifestyle and behavioural plan is the same, and cognitive behavioural therapy is adapted to the child's developmental level and communication style. [1]
Aboriginal and Torres Strait Islander children, and children in rural and remote settings, may have reduced access to paediatric neurology, cognitive behavioural therapy, and magnetic resonance imaging. Culturally safe communication, the use of telehealth and retrieval networks, and the delivery of the high-yield lifestyle and behavioural interventions by the primary clinician support equitable care. The red-flag screen and the acute plan are unchanged, but the threshold for transfer is held higher when distance separates the family from specialist services. [1]
Children from migrant, refugee, and asylum-seeking families, and those facing socioeconomic disadvantage, may face language barriers, lower health literacy around headache and analgesia, and limited access to consistent follow-up. A trained interpreter, written information in the family's language, and a simple, reinforced acute and lifestyle plan are essential. The over-the-counter availability of codeine-containing analgesics in some settings makes the medication-overuse warning especially important. [12]
Evidence, Guidelines & Regional Differences
| Region | Key guidance | Acute treatment | Prophylaxis strategy |
|---|
The principal controversy has been largely resolved by the CHAMP trial, and a candidate should know where the field has settled and where uncertainty remains. The case for ibuprofen and paracetamol as first-line acute treatment is settled. The case for cognitive behavioural therapy in frequent and chronic migraine is settled and strong. The case for drug prophylaxis is unsettled: amitriptyline and topiramate are the most-studied options and may be tried, but the CHAMP trial showed no superiority over placebo, and the 2019 guideline frames them as options rather than established preventives. The remaining uncertainty concerns the newer CGRP-directed monoclonal antibodies, which are effective in adults but have limited paediatric evidence and are not yet first-line in children. [6] [4]
The most common point of genuine practice variation is the preferred triptan and the age at which it is introduced. Sumatriptan nasal spray and rizatriptan have the strongest paediatric evidence and are widely used in older children and adolescents, while the choice between them is driven by availability, route preference, and regional subsidy. The early introduction of an acute plan, built on simple analgesia with a triptan for moderate-to-severe attacks and an explicit cap on analgesic days, is the one habit a candidate must carry into practice. [9] [10]
Exam Pearls
References
- [1]Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 2018.PMID 29368949
- [2]Abu-Arafeh I, Razak S, Sivaraman B, Graham C Prevalence of headache and migraine in children and adolescents: a systematic review of population-based studies. Dev Med Child Neurol, 2010.PMID 20875042
- [3]Lewis D, Ashwal S, Hershey A, Hirtz D, Yonker M, Silberstein S Practice parameter: pharmacological treatment of migraine headache in children and adolescents: report of the American Academy of Neurology Quality Standards Subcommittee and the Practice Committee of the Child Neurology Society. Neurology, 2004.PMID 15623677
- [4]Oskoui M, Pringsheim T, Billinghurst L, Smith A, Mesterman R, Ghasia M, et al Practice guideline update summary: Pharmacologic treatment for pediatric migraine prevention: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology, 2019.PMID 31413170
- [5]El-Chammas K, Keyes J, Thompson N, Vijayakumar J, Langer E, Lasser D, Suresh S, Szperka C, Cleves C, Mauskop A, Kabbouche MA Pharmacologic treatment of pediatric headaches: a meta-analysis. JAMA Pediatr, 2013.PMID 23358935
- [6]Powers SW, Coffey CS, Chamberlin LA, Ecklund DJ, Klingner EA, Yan Y, Eby N, Dugan P, Morgenlander WL, Krane E, et al Trial of Amitriptyline, Topiramate, and Placebo for Pediatric Migraine. N Engl J Med, 2017.PMID 27788026
- [7]Powers SW, Kashikar-Zuck SM, Allen JR, LeCates SL, Slater SK, Zafar M, Kabbouche MA, O'Brien HL, Shenk CE, Rausch JR, Hershey AD Cognitive behavioral therapy plus amitriptyline for chronic migraine in children and adolescents: a randomized clinical trial. JAMA, 2013.PMID 24368463
- [8]Richer L, Billinghurst L, Linsdell MA, Russell K, Vandermeer B, Crumley ET, Durec T, Scott SD, Dryden DM Drugs for the acute treatment of migraine in children and adolescents. Cochrane Database Syst Rev, 2016.PMID 27091010
- [9]Ho TW, Pearlman E, Lewis D, Hämäläinen M, Connor K, Michelson D, Lesem E, Chappell A, Strawn J, Smith T, et al Efficacy and tolerability of rizatriptan in pediatric migraineurs: results from a randomized, double-blind, placebo-controlled trial using a novel adaptive enrichment design. Cephalalgia, 2012.PMID 22711898
- [10]McDonald SA, Hershey AD, Pearlman E, Lewis D, Winner P, Ruff D, Edwards K, Evans DC, Wilson M, Onishchenko A, Wen W, Schaeffler B, Schlotterbeck K Long-term evaluation of sumatriptan and naproxen sodium for the acute treatment of migraine in adolescents. Headache, 2011.PMID 21797863
- [11]Linder SL, Mathew NT, Cady RK, Finlayson G, Ishkanian G, Lewis DW Efficacy and tolerability of almotriptan in adolescents: a randomized, double-blind, placebo-controlled trial. Headache, 2008.PMID 18484981
- [12]Casanova A, Vives-Mestres M, Donoghue S, Asuni C, Onofrj M, Novelli S, Pitti-Cabrera E, Alarcon-Pell L, Guell V, Martelletti P The role of avoiding known triggers, embracing protectors, and adhering to healthy lifestyle recommendations in migraine prophylaxis: Insights from a prospective cohort of 1125 people with episodic migraine. Headache, 2023.PMID 36651502