Paeds · neurology-neurodisability-and-neuromuscular
Hydrocephalus and shunt emergencies
Also known as Ventriculoperitoneal shunt malfunction · Shunt obstruction · Shunt infection · Slit ventricle syndrome · Raised intracranial pressure in the shunted child
Fellowship guide to paediatric hydrocephalus and shunt emergencies. Covers the Rekate functional classification of hydrocephalus by the site of cerebrospinal fluid obstruction and overproduction, the cerebrospinal fluid pathway from choroid plexus to arachnoid granulations, the age-specific presentation of raised intracranial pressure from the bulging fontanelle and sunset sign in the infant to the early-morning headache and Cushing triad in the older child, the shunt series of skull, chest, and abdomen radiographs that traces the catheter from ventricle to peritoneum, the shunt tap that measures pressure and sends cerebrospinal fluid for culture, the hyperosmolar bridge to theatre with mannitol and hypertonic saline, the distinction of shunt malfunction from overdrainage, slit ventricle syndrome, and infection, the Hydrocephalus Clinical Research Network protocol that cut shunt infection, and the endoscopic third ventriculostomy and ETV Success Score work of Warf and Kulkarni as the non-shunt alternative.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who turns up unwell with a ventriculoperitoneal shunt has a shunt malfunction until proven otherwise, and the job is to prove it is not, fast. Hydrocephalus is the active distension of the cerebral ventricles from an imbalance between the production and the absorption of cerebrospinal fluid, and a shunt is the tube that drains that fluid from the ventricle to the peritoneum when the body cannot move it itself. When the shunt blocks, the original hydrocephalus returns, the intracranial pressure climbs, and the brainstem is threatened. Kahle and colleagues set out the modern understanding of paediatric hydrocephalus as a disorder of cerebrospinal fluid dynamics that is surgical in its emergency and lifelong in its management. [1]
Three facts make this topic central to the paediatric exam. The diagnosis is a clock and a clinical pattern, because the child with a blocked shunt and a falling conscious level is dying. The investigation is a shunt series and a head scan, which trace the tube and the ventricles. And the management is the early involvement of neurosurgery, because the definitive treatment is operative and no child with a threatened brainstem waits for it. The shunted child is one of the commonest technology-dependent children in general paediatric practice, and every fellow must hold the assessment and the safety-net without hesitation. [3]
Classification
Hydrocephalus has two working classifications, and both are worth holding. The first is the traditional divide into communicating and non-communicating forms, which tells you whether the block is inside or outside the ventricular system. The second is the Rekate functional classification by the site of the disturbance, which tells you exactly where the cerebrospinal fluid is held up and so guides the operation. [2]
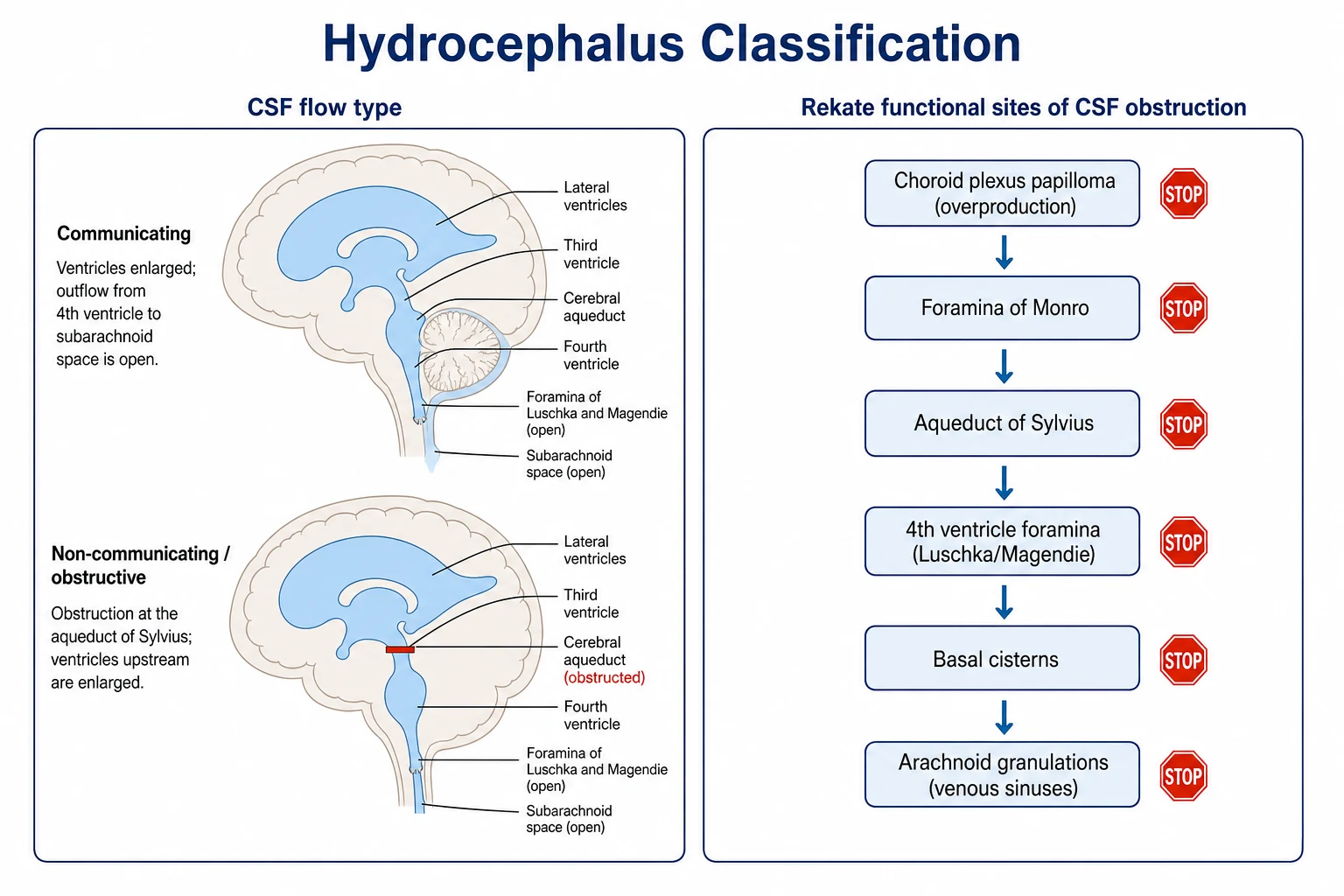
Communicating hydrocephalus means the ventricular outflow is open and the fluid reaches the subarachnoid space, but the defect lies downstream, most often at the arachnoid granulations where absorption fails. This is the pattern after a haemorrhage or a meningitis that gums up the granulations, and it is the pattern of the post-haemorrhagic hydrocephalus of prematurity. Non-communicating, or obstructive, hydrocephalus means a physical block halts the flow within or at the exit of the ventricular system, classically at the aqueduct of Sylvius in aqueductal stenosis or at the fourth ventricle outlets in a posterior fossa tumour or a Dandy-Walker cyst. The distinction matters because an obstructive cause may be curable by removing the block or by bypassing it with an endoscopic third ventriculostomy, while a communicating cause usually needs a shunt. [2]
The Rekate classification names six functional sites. Obstruction at the foramina of Monro, the aqueduct of Sylvius, the fourth ventricle outlets of Luschka and Magendie, the basal cisterns, and the arachnoid granulations each gives a distinct pattern, and overproduction from a choroid plexus papilloma is the sixth. The value of the functional approach is that it directs the surgeon to the right operation, because an aqueductal block is bypassed by a third ventriculostomy while an absorptive failure at the granulations is drained by a shunt. [2]
The clinical distinction that matters most at the bedside is not the anatomical label but whether the hydrocephalus is acute and uncompensated or chronic and compensated. Acute uncompensated hydrocephalus is the emergency, because the pressure is rising now and the brainstem is at risk. Chronic compensated hydrocephalus, where the ventricles are large but the pressure has settled, may tolerate a slow course and an elective plan, and the child who decompensates after years of stability is the one who presents as a shunt emergency. [1]
Epidemiology & Risk Factors
Congenital hydrocephalus affects roughly 1 in 1000 to 1 in 2000 live births, and shunted hydrocephalus is among the most common reasons a child sees a paediatric neurosurgeon. The shunt is the commonest neurosurgical implant in childhood, and because about a third to a half of all ventriculoperitoneal shunts fail within the first year after insertion, the shunted child is a recurring presence in the emergency department and on the ward. The lifetime burden is high, and a child implanted in infancy can expect several revisions across childhood. [1][4]
The causes of hydrocephalus in childhood divide into the congenital and the acquired. The congenital malformations include aqueductal stenosis, the Chiari II malformation with myelomeningocele, and the Dandy-Walker continuum, while the acquired causes include the intraventricular haemorrhage of prematurity, post-meningitic hydrocephalus, and the obstruction from a posterior fossa tumour. The cause shapes both the presentation and the prognosis, because the post-haemorrhagic hydrocephalus of the preterm infant carries the highest revision and infection burden, while the aqueductal stenosis of an older child may be managed with a single endoscopic third ventriculostomy and no shunt at all. [1]
The risk factors for shunt malfunction were defined by the prospective multicentre cohort of the Hydrocephalus Clinical Research Network, reported by Riva-Cambrin and colleagues. The strongest predictors of malfunction are young age at insertion, a post-haemorrhagic cause, and a prior revision, which means the preterm infant with post-haemorrhagic hydrocephalus is the child most likely to return. The risk factors for shunt infection are young age, long operative time, and a breach in the sterile protocol, which is why the same network built a standardised insertion protocol to cut the infection rate. [4][5]
Pathophysiology
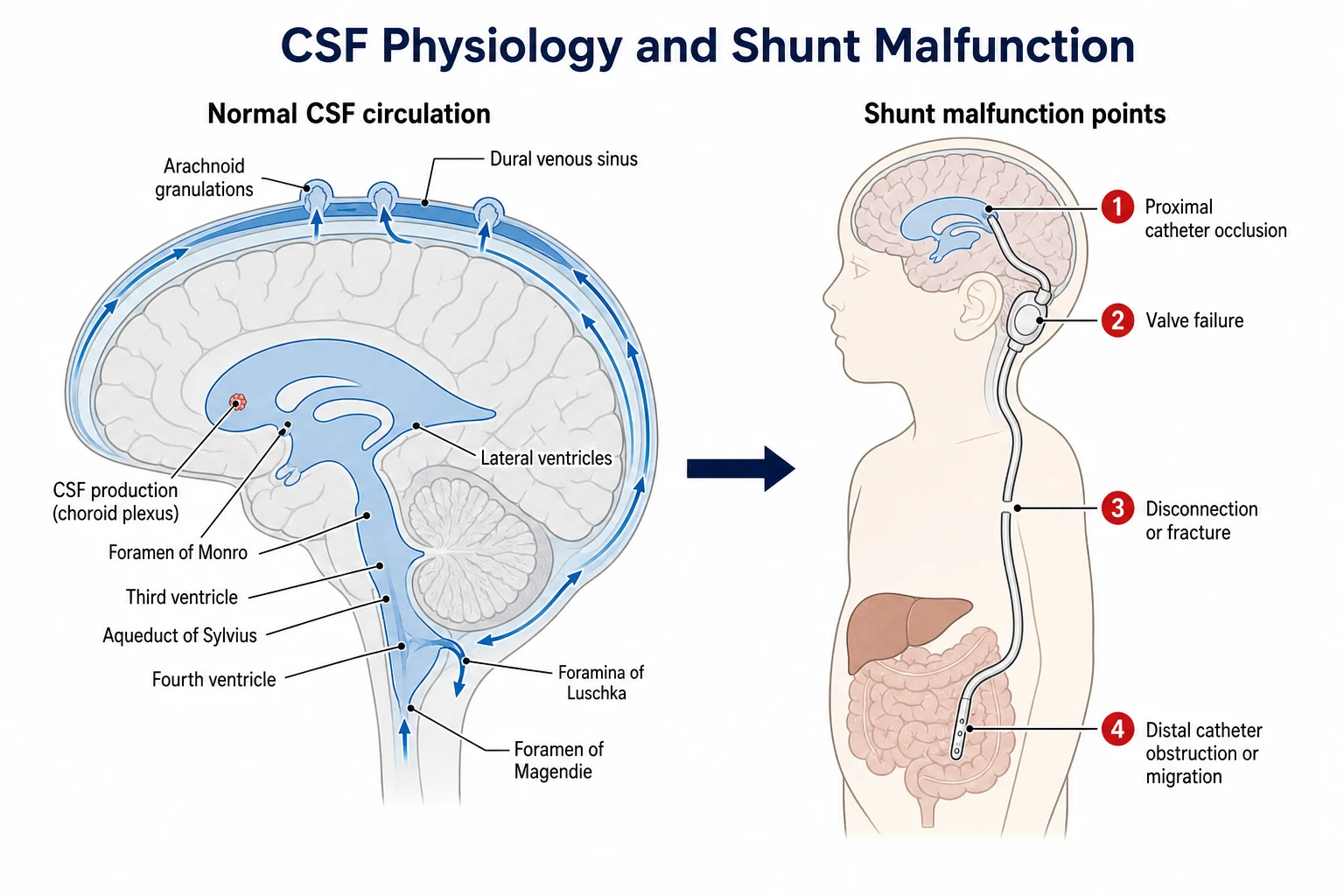
To understand the shunt, hold the normal circulation of the cerebrospinal fluid in mind. The fluid is made by the choroid plexus at about 0.3 millilitres per minute, and it flows from the two lateral ventricles through the foramina of Monro into the third ventricle, through the narrow aqueduct of Sylvius into the fourth ventricle, out through the foramina of Luschka and Magendie into the subarachnoid space, and up over the surface of the brain to the arachnoid granulations, where it is absorbed into the dural venous sinuses. Hydrocephalus is what happens when any link in that chain breaks. [1]
The mechanism is mechanical in three of the six Rekate categories, where a physical obstruction halts the flow at the foramina, the aqueduct, the fourth ventricle outlets, the basal cisterns, or the granulations, and the ventricles upstream of the block distend. In the absorptive failure of post-haemorrhagic and post-meningitic hydrocephalus, the granulations are blocked by protein and debris so the fluid reaches them but cannot pass. In the rare overproduction of a choroid plexus papilloma, the fluid is made faster than even healthy granulations can absorb. In every case the net result is the same, which is that the ventricles swell, the brain is compressed against the rigid skull, the intracranial pressure climbs, and when the pressure exceeds the cerebral perfusion pressure the brain is starved and the brainstem is pushed down. [2]
A shunt restores the balance by carrying the fluid past the block, from the ventricle through a valve to the peritoneum where it is absorbed. The shunt has three parts, which are the proximal catheter in the ventricle, the valve just under the scalp behind the ear, and the long distal catheter that runs under the skin of the neck and chest to the peritoneum. Shunt malfunction is the return of the original obstruction, because a blocked or broken shunt no longer drains the fluid and the hydrocephalus recurs. This is why the workup of the unwell shunted child is the workup of recurrent hydrocephalus, and why a blocked shunt reproduces the raised pressure that the shunt was placed to relieve. [11]
Clinical Presentation
The presentation of raised intracranial pressure divides by age, because the infant with open sutures accommodates the pressure by head growth while the older child with a fused skull cannot. The infant presents with a rapidly enlarging head circumference crossing the centiles, a tense or bulging fontanelle, splayed cranial sutures, distended scalp veins, irritability, vomiting, poor feeding, lethargy, and the sunset sign of impaired upgaze from pressure on the tectal plate of the midbrain. The head circumference is the single most sensitive sign in infancy, which is why it is measured and plotted at every visit. [3]
How raised intracranial pressure presents across the age spectrum
An infant with an enlarging head circumference crossing the centiles, a tense fontanelle, and the sunset sign of impaired upgaze
A toddler or preschool child with irritability, vomiting, and lethargy who cannot localise the headache
A school-age child with early-morning headache that may wake them, projectile vomiting, and a decline in school performance
An adolescent with a fused skull who develops papilloedema, a sixth nerve palsy with diplopia, and ataxia
A child of any age who reaches the preterminal Cushing triad of hypertension, bradycardia, and irregular respirations signalling brainstem herniation
The older child with a fused skull cannot expand the head, so the pressure is transmitted directly to the brain. The presentation is the classic triad of raised pressure, which is early-morning headache that may wake the child from sleep, vomiting that is often projectile and worse in the morning, and drowsiness. The headache is thought to ease as the day goes on because upright posture and activity improve the venous and cerebrospinal fluid drainage. Diplopia from a sixth nerve palsy is a false-localising sign of raised pressure, papilloedema is found on fundoscopy, and ataxia and a decline in school performance reflect the compression of the cerebellum and the cerebrum. [1]
The preterminal picture is Cushing triad, which is the combination of hypertension, bradycardia, and irregular respirations. Cushing triad is a late and preterminal sign of brainstem herniation, and the fellow must never wait for it. The child who reaches it needs an immediate hyperosmolar bridge, an airway, and a call to theatre, because the brainstem is being squeezed through the foramen magnum. The child with a shunt may additionally report that the pump or reservoir does not refill when compressed, and a parent may describe a visible swelling or fluid tracking along the shunt line, though neither sign is reliable enough to exclude malfunction. [1]
Differential Diagnosis
The differential of a child with a shunt and new symptoms is the heart of the exam question, because the commonest reason a shunted child presents unwell is not the shunt. The task is to separate shunt malfunction from its mimics without ever discharging a child with a missed block, and the discriminator is the combination of the clinical pattern, the shunt series, the head scan, and the shunt tap. [3]
Shunt malfunction (obstruction)
emergency, operate
- New headache, early-morning vomiting, drowsiness, and signs of raised pressure
- Enlarging ventricles on CT or rapid MRI compared to baseline
- Proximal catheter block is the commonest site
- Definitive treatment is shunt revision or external ventricular drainage
Gastroenteritis or viral illness
common mimic
- Vomiting and lethargy with a clear infectious context
- Normal shunt series and stable ventricles
- A diagnosis of exclusion in the shunted child
- Never assumed without excluding malfunction first
Slit ventricle syndrome (overdrainage)
chronic, positional
- Recurrent positional headache worse on standing and relieved by lying flat
- Small or slit ventricles on imaging despite the symptoms
- Reflects overdrainage from too low a valve pressure
- Managed by upgrading the valve, not by lowering it
Shunt infection
within months of surgery
- Fever, wound or track inflammation, abdominal pain, meningism
- Usually coagulase-negative staphylococci
- CSF from the shunt tap shows pleocytosis and a positive culture
- Managed by removal, external drainage, and antibiotics
The first mimic is a non-shunt cause of the same symptoms, and this is the trap that catches the unwary. Gastroenteritis causes vomiting, a viral illness causes lethargy, and migraine causes headache, and all three are common in childhood. The rule is that vomiting in a shunted child is gastroenteritis only after the shunt series is clear and the ventricles are stable, because a blocked shunt presents with exactly the same vomiting and the consequences of missing it are catastrophic. [3]
The second is shunt overdrainage and the slit ventricle syndrome, which Rekate described as the converse of obstruction. Here the shunt drains too well, the ventricles collapse to slits, and the child develops recurrent positional headache that is worse on standing and relieved by lying flat. The imaging shows small ventricles, not large ones, and the management is to raise the valve pressure, not to lower it, which is the opposite of what obstruction demands. [10]
The third is shunt infection, which presents with fever, inflammation along the shunt track or at the wound, abdominal pain from distal catheter infection, and meningism. Infection usually declares within months of the surgery, and the commonest organism is a coagulase-negative staphylococcus. The fourth is a new cause of raised pressure in a child who happens to have a shunt, such as a tumour, a venous sinus thrombosis, or a meningitis, which can coexist with a working shunt and which the workup will uncover. [6][9]
Clinical & Bedside Assessment
The bedside assessment of a child with a suspected shunt malfunction is a structured emergency, and it runs in parallel with the call to neurosurgery. You call for senior help and you alert the neurosurgical team at the outset, because the definitive treatment is operative and the child may need theatre within the hour. The assessment takes minutes, because the workup and the resuscitation move together. [3]
The head circumference is the first measurement, plotted against the centiles and against the child's own trajectory, because an upward deviation in a shunted infant is a sign of failing drainage. The fontanelle is palpated in the upright and the supine infant, and a tense or bulging fontanelle that does not settle when the child is calmed and upright is a sign of raised pressure. The eyes are examined for the sunset sign, in which the eyes are driven downward so the sclera shows above the iris, a sign of pressure on the tectal plate, and for the ocular movements, where a sixth nerve palsy causes an inability to abduct. [1]
The shunt itself is examined. The reservoir, usually felt as a small dome behind the ear or on the scalp, is compressed and watched to see whether it refills, because a reservoir that empties but does not refill suggests the proximal catheter is blocked and a reservoir that does not empty suggests the distal catheter is blocked. This sign is unreliable, and a normal refill never excludes a malfunction, but an abnormal finding adds weight to the suspicion. The abdomen is examined for distension or peritonism that suggests a distal catheter problem, and the wound and the shunt track are inspected for the redness, swelling, or discharge of infection. [11]
The conscious level is the single most important observation, because a falling conscious level is the sign that the brainstem is being threatened. The child who is drowsy, irritable, or unresponsive, or who reaches the preterminal Cushing triad, needs an immediate hyperosmolar bridge and a call to theatre, and the workup must not delay the resuscitation. Intravenous access is secured, and blood is sent for glucose, electrolytes, a full blood count, and blood cultures, because sepsis and electrolyte disturbance both mimic and accompany shunt malfunction. [1]
Investigations
The shunt series is the first imaging test for suspected malfunction, and it is the one every fellow must be able to describe. The shunt series is a set of plain radiographs, an anteroposterior and a lateral skull, a chest, and an abdomen, that together trace the shunt catheter from the ventricle to the peritoneum. The series looks for a disconnection, a fracture, a migration, or a pulled-back distal tip, and it is the test that tells you whether the hardware is still in one piece. A fracture is often found at the clavicle, where the catheter has fatigued over years of neck movement, and a migrated distal tip may lie anywhere from the peritoneum to the chest. [11]
A computed tomography of the head, or a rapid magnetic resonance imaging where a programme has it, is the test that shows the ventricles. The scan is compared to the child's own baseline from the last clinic visit, not to a population normal, because the relevant question is whether the ventricles have enlarged since the last time the child was well. An increase in ventricular size confirms an obstruction, while slit ventricles point to overdrainage. The trap is the child whose ventricles are large at baseline and have not changed, which is the stable compensated state and not a malfunction, and the child whose ventricles are small but whose pressure is high, which is slit ventricle syndrome. Rapid magnetic resonance imaging is preferred where available because it spares the shunted child a lifetime of cumulative radiation from repeated scans. [1]
Hyperosmolar bridge to theatre for impending herniation
Dose
Mannitol 0.5 grams per kilogram intravenously, or 3 percent hypertonic saline 2 to 5 millilitres per kilogram intravenously
The shunt tap is both a diagnostic and a therapeutic procedure, and Miller and colleagues set out its role. Performed by sterile puncture of the shunt reservoir with a fine needle, the tap measures the opening pressure, tests whether the shunt flows when the reservoir is depressed, and sends cerebrospinal fluid for cell count, protein, glucose, gram stain, and culture. A high opening pressure with poor flow points to obstruction, while a pleocytosis and a positive culture point to infection. By allowing fluid to be withdrawn, the tap also lowers the pressure and may temporarily relieve the block, which buys time on the way to theatre. [11]
The shuntogram, in which a small volume of contrast or isotope is injected into the reservoir to trace the flow on imaging, is reserved for cases where the shunt series, the head scan, and the tap are inconclusive. It can localise the exact site of obstruction but it is invasive and time-consuming, and it is not a first-line test. Blood cultures are sent whenever infection is suspected, and a lumbar puncture has no role in the workup of a shunted child with suspected malfunction, because it risks herniation and it does not sample the shunted system. [11]
Management — Resuscitation
The resuscitation of the child with an obstructed shunt and raised intracranial pressure begins with the airway, the breathing, and the circulation, and the early involvement of neurosurgery, because the definitive treatment is operative. The child with a falling conscious level or the preterminal Cushing triad needs an immediate bridge to theatre, and no child in that state waits for the scan. The first moves are to elevate the head of the bed to thirty degrees, to secure the airway and give high-flow oxygen, and to call the neurosurgical and anaesthetic teams. [1]
If herniation is imminent, a hyperosmolar agent is given to buy time. Mannitol at 0.5 grams per kilogram intravenously, or three percent hypertonic saline at 2 to 5 millilitres per kilogram intravenously, lowers the intracranial pressure within minutes by drawing water out of the brain and into the vascular compartment. The bridge is temporary, and it does not replace the operative revision or the external ventricular drain, but it keeps the brain perfused while the team is assembled and the theatre is prepared. The shunt tap, performed as part of the workup, may also relieve the pressure by allowing fluid to be withdrawn, which is why the tap is both diagnostic and therapeutic. [1]
The reversible contributors are sought and treated in parallel. Hypoglycaemia, electrolyte disturbance, and sepsis all accompany and mimic shunt malfunction, so the bedside glucose is checked, the electrolytes are sent, and the blood cultures are drawn when infection is suspected. The child is monitored continuously for the conscious level, the heart rate, the blood pressure, and the oxygen saturation, because a deterioration is the trigger to escalate from the workup to the bridge to theatre. [3]
Management — Definitive & Stepwise
The definitive management depends on the cause, and the cause is defined by the workup. An obstructed shunt is revised in theatre, where the blocked component is cleared or replaced and the system is tested for flow. If the child is unstable or the infection is suspected, the shunt is externalised, which means the distal catheter is brought out through the skin and connected to an external drainage system, and the cerebrospinal fluid is drained and sampled until the child is ready for a fresh shunt. [11]
[3]A shunt infection is managed in two stages. The infected shunt is removed and an external ventricular drain is placed, intravenous antibiotics are started and guided by the culture, and intraventricular antibiotics are added in selected cases. A fresh shunt is reinserted only once the cerebrospinal fluid is sterile, because reinserting into an infected system almost guarantees a recurrence. Konrad and colleagues set out the modern approach to cerebrospinal fluid shunt infections in children, and Simon and colleagues described the emerging paradigms of pathogenesis that shape the prevention and the treatment. [6][9]
Slit ventricle syndrome from overdrainage is managed by upgrading the valve to a higher pressure, which slows the drainage and lets the ventricles re-expand, or by replacing a fixed valve with a programmable one that can be adjusted externally with a magnet. A programmable valve allows the pressure setting to be tuned to the child over time, which is a particular advantage in the overdrainage states. Some children need a period of temporary external drainage to let the ventricles recover before a new valve is chosen. [10]
Endoscopic third ventriculostomy, with or without choroid plexus cauterisation in the infant, is the non-shunt alternative, and it is best in obstructive hydrocephalus where the block is at the aqueduct. The procedure creates a stoma in the floor of the third ventricle that opens into the prepontine cistern, bypassing the obstruction and restoring the natural flow. The likely success is predicted by the ETV Success Score, reported by Kulkarni and colleagues, which combines the child's age, the cause, and any prior shunt into a single percentage, so an older child with aqueductal stenosis and no prior shunt scores highly while a young infant with post-haemorrhagic hydrocephalus scores poorly. Warf and colleagues showed that adding choroid plexus cauterisation to the third ventriculostomy in infants improves the success rate and offers a shunt-free option in the very young. [7][8]
The stepwise pathway for the child with a suspected shunt malfunction
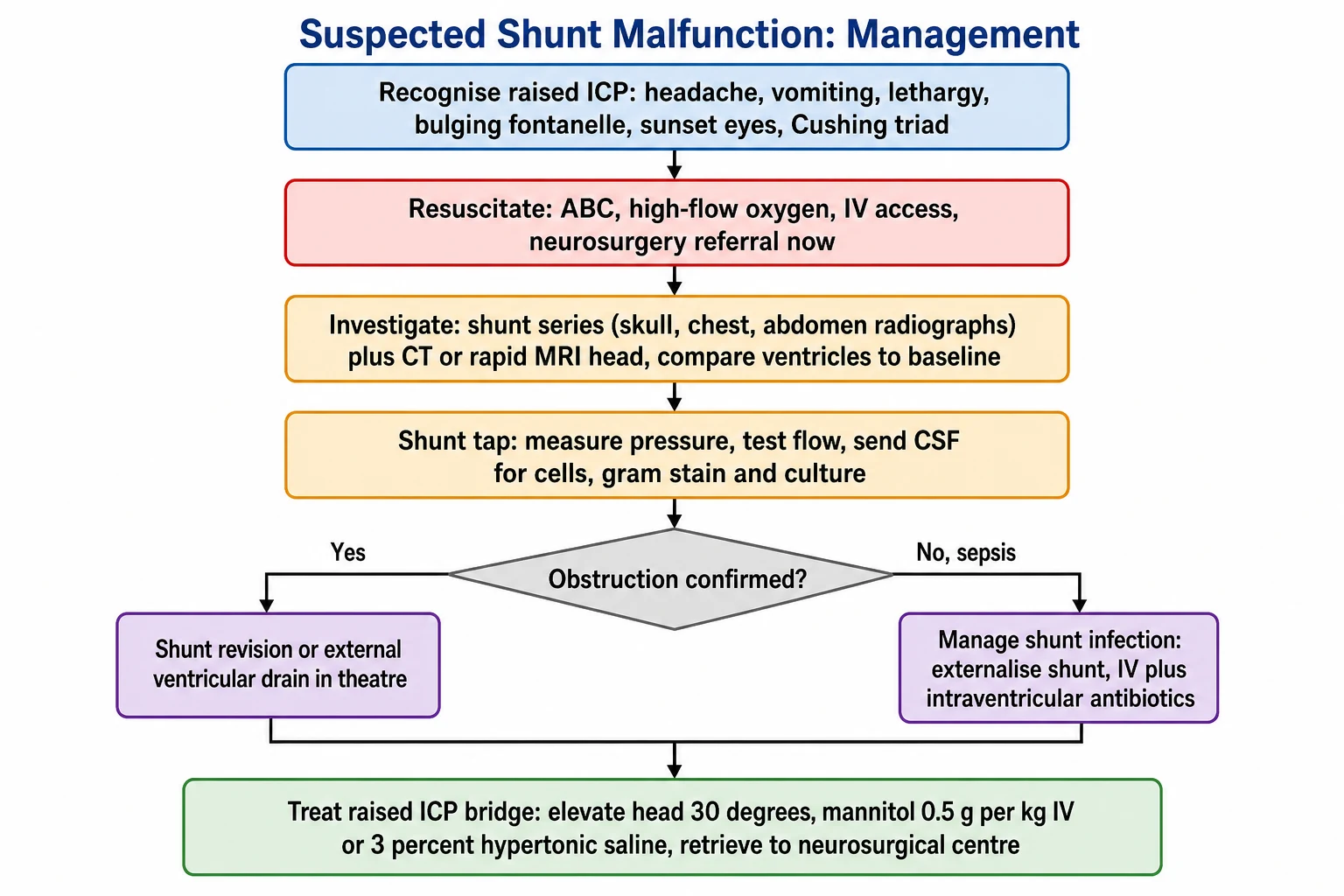
Recognise the red flags of raised intracranial pressure and measure the head circumference, fontanelle, eyes, and conscious level
Resuscitate with ABC, high-flow oxygen, intravenous access, and elevate the head of the bed to 30 degrees; call neurosurgery now
Investigate with the shunt series of skull, chest, and abdomen radiographs and a CT or rapid MRI of the head compared to baseline
Perform a shunt tap to measure the opening pressure, test the flow, and send cerebrospinal fluid for cells, gram stain, and culture
Give a hyperosmolar bridge of mannitol 0.5 grams per kilogram or 3 percent hypertonic saline if the conscious level falls or Cushing triad appears
Definitive care: shunt revision or external ventricular drainage for obstruction, removal and antibiotics for infection, valve upgrade for overdrainage
Specific Subtypes & Scenarios
Shunt malfunction is the commonest shunt emergency, and it usually reflects a mechanical obstruction. The proximal catheter is the commonest site of blockage, often by choroid plexus tissue or debris, and disconnection or fracture of the distal catheter and migration of the distal tip are the next most common. The child presents with the signs of raised pressure, the shunt series shows the hardware problem, and the head scan shows the enlarging ventricles, and the management is operative revision. [4]
Shunt infection is the second scenario, and it usually declares within months of the surgery. The child presents with fever, wound or track inflammation, abdominal pain from a distal infection, or the signs of meningitis. The commonest organism is a coagulase-negative staphylococcus, with Staphylococcus aureus, the gram negatives, and Propionibacterium acnes the other culprits. The diagnosis rests on the shunt tap, which shows a pleocytosis and a positive culture, and the management is the two-stage removal, external drainage, and antibiotics. [6]
Slit ventricle syndrome is the overdrainage phenotype, the third scenario, and Rekate described it as the converse of obstruction. The child develops recurrent positional headache that is worse on standing and relieved by lying flat, and the imaging shows small or slit ventricles despite the symptoms. The mechanism is overdrainage from a valve pressure set too low, so the ventricles collapse and the brain pulls on the pain-sensitive meninges. The management is to raise the valve pressure or to convert to a programmable valve, which is the opposite of what an obstruction would demand. [10]
The post-haemorrhagic hydrocephalus of the preterm infant is the fourth scenario, and it is the youngest and the most challenging. The intraventricular haemorrhage of prematurity damages the absorptive capacity of the arachnoid granulations, and the hydrocephalus is communicating and progressive. The preterm infant is often too small or too unstable for a definitive shunt at first, so a temporary reservoir is placed to drain the fluid until the child grows and stabilises, and the eventual shunt carries the highest revision and infection burden of any group. [1]
The Chiari II malformation with myelomeningocele is the fifth scenario, and it is a common congenital cause that Cavalheiro and colleagues described. The downward displacement of the cerebellum and the brainstem obstructs the cerebrospinal fluid flow, and most affected children need an early shunt. The child carries a combined neurosurgical, urological, and orthopaedic burden, and a shunt malfunction may first declare as a change in the brainstem signs of the Chiari II, such as new swallowing difficulty, stridor, or apnoea, rather than as the classic signs of raised pressure. [12]
A posterior fossa tumour is the sixth scenario, and it is the one that presents as an emergency before the tumour is even known. The tumour obstructs the fourth ventricle or the aqueduct and produces an acute obstructive hydrocephalus, which may need an emergency shunt, an external drain, or an endoscopic third ventriculostomy before the tumour itself is resected. The presentation is the raised-pressure triad in an older child, and the scan shows both the ventriculomegaly and the mass, and the management is the joint work of the oncology and the neurosurgical teams. [1]
Complications & Pitfalls
The feared complication of an obstructed shunt is brainstem herniation and death, which is why any child with a shunt and a falling conscious level is an emergency until proven otherwise. The herniation is the final step in the rising pressure, when the brain is forced down through the tentorial hiatus or the foramen magnum and the brainstem is crushed. A child who reaches this point may not recover, which is why the hyperosmolar bridge and the call to theatre must come before the scan. [1]
Repeated revisions carry their own burden. Each operation scars the abdomen and the ventricle, and each successive revision becomes technically harder, with a higher risk of injury to the brain and a longer operative time. The lifetime infection and revision burden shapes the child's development and schooling, and the child with a difficult shunt history is the one most likely to need intensive neurodevelopmental and educational support. Shunt infection adds weeks of antibiotics and a staged reinsertion, and it carries a real mortality, which is why the standardised insertion protocol was built to prevent it. [5][9]
The classic pitfalls are diagnostic and temporal. The first is to assume that vomiting in a shunted child is gastroenteritis and to discharge without a shunt series, which is the commonest route to a missed malfunction. The second is to be reassured by normal or stable ventricles on a single scan, because slit ventricle syndrome shows small ventricles and the relevant comparison is the change from the child's own baseline, not a population normal. The third is to under-treat the preterminal child while waiting for the neuroimaging, because the hyperosmolar bridge and the shunt tap must not wait for the scan, and the child who herniates in the scanner is the one who was not bridged first. [3]
A subtler pitfall is to confuse overdrainage with obstruction. The child with slit ventricle syndrome has small ventricles and a positional headache, and the correct move is to raise the valve pressure, but the unwary move is to assume the headache means obstruction and to lower the pressure, which worsens the overdrainage. The shunt tap and the comparison to the baseline scan distinguish the two, and the distinction is the one that decides whether the valve goes up or down. [10]
Prognosis & Disposition
The prognosis of a single shunt malfunction that is promptly recognised and revised is good, and most children return to their baseline within days. The episode is a crisis, but it is a treatable one when it is caught early, and the child who is revised before the brainstem is threatened recovers fully. The longer-term outlook is shaped by the underlying cause of the hydrocephalus, the cumulative number of revisions and infections, and any neurological injury sustained before or during the episodes. [1]
Children with shunted hydrocephalus are more likely than their peers to have learning and behavioural difficulties, seizure disorders, and visual impairment, and they need structured neurodevelopmental and educational follow-up. The cause drives the cognitive outcome, so the child with a post-haemorrhagic hydrocephalus of prematurity carries a heavier neurodevelopmental burden than the child with aqueductal stenosis, and the follow-up is tailored to the child's needs. The recurrence risk is high, with about a third to a half of shunts failing in the first year, and the family and the school must know the malfunction signs. [4]
Disposition after a revision is to the ward or the paediatric intensive care unit depending on the course, and every child goes home with a clear written safety-net describing the red flags and the route back to hospital. The safety-net names the symptoms that demand an immediate return, which are headache, vomiting, drowsiness, and a change in the eyes or the conscious level, and it gives the family the direct line to the neurosurgical service. The school and the respite carers receive the same plan, because the shunted child is a shared responsibility. [3]
Special Populations
The preterm infant with post-haemorrhagic hydrocephalus is the youngest population and the one most likely to need a reservoir before a definitive shunt. The preterm brain is fragile, the absorptive failure is severe, and the revision and the infection burden are the highest of any group, so the management is staged and patient, and the neurodevelopmental follow-up is intensive. [1]
The child with a Chiari II malformation and myelomeningocele carries a combined neurosurgical, urological, and orthopaedic burden, and the shunt is one part of a complex picture. A shunt malfunction in this child may first declare as a change in the brainstem signs of the Chiari II, such as new swallowing difficulty, stridor, or apnoea, rather than as the classic raised-pressure triad, which is why the fellow must know the atypical presentations of malfunction in this group. The management is multidisciplinary, and the neurosurgical, urological, and rehabilitation teams work together across childhood. [12]
The child with a neurodisability or technology dependence often cannot report a headache, and the carer's observation of irritability, vomiting, reduced tone, or a change in the seizure pattern becomes the red flag. The family knows the child's baseline better than any clinician, and a parental report that something is wrong is taken seriously and worked up, because the classic signs may be muted or absent. The management is the same shunt series and head scan and shunt tap, with extra attention to the airway and the swallowing in the child with baseline tone and bulbar abnormality. [3]
The child from a remote setting is at risk of a late presentation and a long retrieval, so a clear family action plan and a known retrieval pathway are central to the outcome. The family is taught to recognise the red flags and to call early, and the local service is linked to the neurosurgical centre by a documented escalation pathway that does not depend on a fresh referral each time. The culturally appropriate communication and the engagement with the family are part of the acute and the follow-up care, and the child from a refugee or migrant family is connected to an interpreter and to a local service before discharge. [3]
Evidence, Guidelines & Regional Differences
The modern evidence base is anchored by the Hydrocephalus Clinical Research Network, whose work has transformed both the prevention and the prediction of shunt complications. The network's standardised shunt insertion protocol, reported by Kestle and colleagues, reduced the shunt infection rate by a bundle that included a double-gloving, a strict operative protocol, and an antibiotic-impregnated catheter, and it is now the benchmark for shunt surgery. The network's multicentre cohorts have defined the risk factors for malfunction, with Riva-Cambrin and colleagues showing in a prospective study that young age, a post-haemorrhagic cause, and a prior revision carry the highest malfunction risk. [4][5]
HCRN insertion protocol
infection reduction
- Standardised bundle for shunt insertion
- Included double-gloving and a strict operative protocol
- Antibiotic-impregnated catheter as part of the bundle
- Reduced the shunt infection rate as a quality improvement initiative
HCRN malfunction cohort
risk prediction
- Multicentre prospective cohort of shunted children
- Young age at insertion is a strong risk factor
- Post-haemorrhagic cause carries the highest malfunction risk
- A prior revision predicts the next one
ETV Success Score
non-shunt option
- Combines age, cause, and prior shunt into a percentage
- Predicts the success of endoscopic third ventriculostomy
- Best in older children with aqueductal stenosis
- Adding choroid plexus cauterisation improves the infant rate
The non-shunt alternatives rest on the work of Kulkarni and Warf. The ETV Success Score, reported by Kulkarni and colleagues, combines the child's age, the cause, and any prior shunt into a single percentage that predicts the success of an endoscopic third ventriculostomy, so an older child with aqueductal stenosis and no prior shunt scores highly while a young infant with post-haemorrhagic hydrocephalus scores poorly. Warf and colleagues showed that adding choroid plexus cauterisation to the third ventriculostomy in infants improves the success rate and offers a shunt-free option in the very young, which has changed the practice in many centres, especially in resource-limited settings where the shunt burden is heaviest. [7][8]
The overdrainage states are set out in the work of Rekate, who described the slit ventricle syndromes and the headaches that arise from a shunt that drains too well. The controversy over the management of slit ventricle syndrome, whether by valve upgrade, by programmable valve, or by temporary external drainage, is alive in the literature, and the shared principle is that the treatment of overdrainage is the opposite of the treatment of obstruction. [10]
Regional practice differs in three areas. The choice between a shunt and an endoscopic third ventriculostomy varies by centre and by cause, with the high-volume centres more likely to offer the non-shunt option in suitable children. The routine use of rapid magnetic resonance imaging to spare the shunted child a lifetime of cumulative radiation is standard in many programmes but not universal. And the operative protocol for shunt insertion varies, though the HCRN bundle is widely adopted as the infection-reduction standard. The shared foundation is the early recognition of malfunction, the shunt series and the neuroimaging, the shunt tap, and the urgent neurosurgical referral, which no region disputes. [3]
Exam Pearls
The shunt malfunction workup to the letter
References
- [1]Kahle KT, Klinge PM, Koschnitzky JE, et al Paediatric hydrocephalus. Nat Rev Dis Primers, 2024.PMID 38755194
- [2]Rekate HL The definition and classification of hydrocephalus: a personal recommendation to stimulate debate. Cerebrospinal Fluid Res, 2008.PMID 18211712
- [3]Lu VM, Shimony N, Jallo GI Infant Hydrocephalus. Pediatr Rev, 2024.PMID 39085190
- [4]Riva-Cambrin J, Kestle JR, Holubkov R, et al Risk factors for shunt malfunction in pediatric hydrocephalus: a multicenter prospective cohort study. J Neurosurg Pediatr, 2016.PMID 26636251
- [5]Kestle JR, Riva-Cambrin J, Wellons JC 3rd, et al A standardized protocol to reduce cerebrospinal fluid shunt infection: the Hydrocephalus Clinical Research Network Quality Improvement Initiative. J Neurosurg Pediatr, 2011.PMID 21721884
- [6]Konrad E, Robinson JL, Hawkes MT Cerebrospinal fluid shunt infections in children. Arch Dis Child, 2023.PMID 36450441
- [7]Kulkarni AV, Riva-Cambrin J, Browd SR, et al Use of the ETV Success Score to explain the variation in reported endoscopic third ventriculostomy success rates among published case series of childhood hydrocephalus. J Neurosurg Pediatr, 2011.PMID 21284458
- [8]Warf BC, Weber DS, Day EL Endoscopic third ventriculostomy with choroid plexus cauterization: predictors of long-term success and comparison with shunt placement for primary treatment of infant hydrocephalus. J Neurosurg Pediatr, 2023.PMID 37178026
- [9]Simon TD, Schaffzin JK, Stevenson CB Cerebrospinal Fluid Shunt Infection: Emerging Paradigms in Pathogenesis that Affect Prevention and Treatment. J Pediatr, 2019.PMID 30528757
- [10]Rekate HL Shunt-related headaches: the slit ventricle syndromes. Childs Nerv Syst, 2008.PMID 18259760
- [11]Miller JP, Fulop SC, Dashti SR Rethinking the indications for the ventriculoperitoneal shunt tap. J Neurosurg Pediatr, 2008.PMID 18518692
- [12]Cavalheiro S, da Costa MDS, Barbosa MM, et al Hydrocephalus in myelomeningocele. Childs Nerv Syst, 2021.PMID 34435215