Paeds · neurology-neurodisability-and-neuromuscular
Hypoxic-ischaemic brain injury
Also known as Post-cardiac-arrest brain injury · Hypoxic-ischaemic encephalopathy in the infant and child · Asphyxial brain injury · Post-arrest neurological injury · Drowning-related brain injury
Fellowship guide to hypoxic-ischaemic brain injury in the infant and child beyond the neonatal period. Covers the primary versus secondary injury split, the causes from drowning and asphyxia to cardiac disease and sepsis, the ischaemia-reperfusion cascade, the THAPCA out-of-hospital and in-hospital trials and the Bayesian reanalysis, the targeted temperature management protocol at 32 to 34 degrees or 36 to 37.5 degrees with rewarming at no more than 0.5 degrees per hour, the neurocritical care bundle of normoxia, normocapnia, normotension, normoglycaemia, and normothermia, the high rate of non-convulsive seizures on continuous EEG, the multimodal neuroprognostication deferred to at least 72 hours, and the care of the child with pre-existing neurodisability.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
When a child is resuscitated from cardiac arrest and remains comatose, the brain has already suffered its primary injury. What the intensive care team does next decides whether a cascade of secondary damage spreads over the following hours and days. The discipline of post-arrest neurology is built around one idea: the secondary injury is preventable, and preventing it changes outcomes. This page covers the biology of that secondary injury, the two landmark trials that defined temperature management in children, the neurocritical care bundle, and the honest, deferred approach to prognostication. [7][1]
Overview & Definition
Hypoxic-ischaemic brain injury in the infant and child is global brain injury caused by a period of inadequate cerebral oxygen and substrate delivery, almost always in the context of a cardiorespiratory arrest or a profound asphyxial event. It is distinct from neonatal hypoxic-ischaemic encephalopathy, which is a perinatal encephalopathy with its own cooling criteria and is covered separately. After the neonatal period, the injury is overwhelmingly a post-cardiac-arrest problem, and the child who reaches intensive care comatose after return of spontaneous circulation is the patient at the centre of this topic. [7]
The conceptual division that organises everything that follows is the split between primary and secondary injury. The primary injury is the neuronal death at the moment of the arrest, when ATP fails, ion pumps collapse, and glutamate-driven excitotoxicity kills cells within minutes. It is already done by the time the child reaches the intensive care unit, and nothing can reverse it. The secondary injury is the reperfusion-driven cascade that unfolds over hours to days — mitochondrial dysfunction, oxidative stress, inflammation, and apoptosis — and it is amplified by every physiological insult the team fails to prevent. Intensive care can do nothing for the primary injury and almost everything it does targets the secondary injury. [7][12]
Classification
The injury is classified first by the temporal mechanism and then by the cause. The temporal classification into primary and secondary injury is the one that drives management, because every intervention in intensive care is aimed at a specific element of the secondary cascade. The cause classification drives the parallel search for and treatment of the precipitant, which is itself part of protecting the brain. [7]
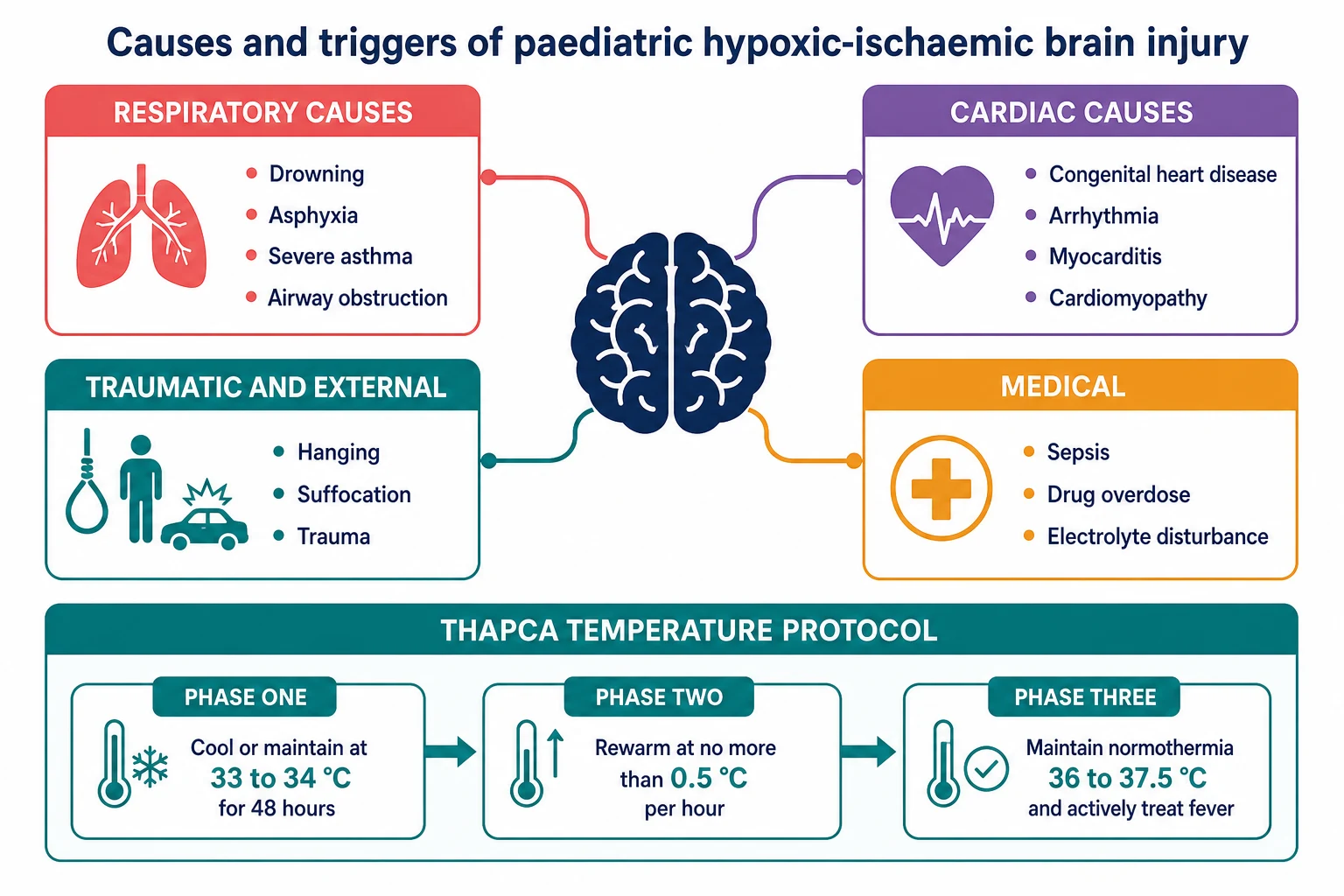
The causes divide into respiratory, cardiac, and other. Drowning is the dominant cause of out-of-hospital arrest in young children, followed by asphyxia from choking, suffocation, and hanging. Cardiac causes, including congenital heart disease, arrhythmia, myocarditis, and cardiomyopathy, dominate in-hospital arrest. Sepsis, trauma, and drug overdose complete the list. The distinction between out-of-hospital and in-hospital arrest matters because the two THAPCA trials recruited each group separately and reached different conclusions about temperature management, which is why the cause classification carries through to the treatment choice. [4][5]
Out-of-hospital arrest
respiratory cause, TTM 32 to 34 degrees
- Often drowning or asphyxia in a young child
- Frequently unwitnessed with a longer no-flow time
- Worse overall survival than in-hospital arrest
- THAPCA-OH: hypothermia is a reasonable option
In-hospital arrest
cardiac cause, TTM normothermia
- Often cardiac disease around surgery or arrhythmia
- Usually witnessed and monitored with a shorter no-flow time
- Better overall survival than out-of-hospital arrest
- THAPCA-IH stopped for futility; normothermia is standard
Asphyxial arrest
hanging, suffocation, foreign body
- Severe global ischaemia from complete airway obstruction
- Same neurocritical care bundle as other causes
- Adolescent hanging needs a mental-health and safeguarding response
- Cervical spine injury must be excluded in hanging
Epidemiology & Risk Factors
Paediatric cardiac arrest is uncommon compared with adult arrest, but it carries a high mortality, and the survivors who remain comatose are the population at risk of hypoxic-ischaemic brain injury. The outcome depends on a handful of factors that the team must establish in the first hour: whether the arrest was witnessed, whether bystander cardiopulmonary resuscitation was given, the duration of no-flow and low-flow, the initial rhythm, and the underlying cause. [7]
Out-of-hospital arrest is more often due to a respiratory cause such as drowning or asphyxia, is frequently unwitnessed, and carries a worse overall survival than in-hospital arrest, which is more often witnessed, monitored, and due to a cardiac cause in a child with known disease. The dominant risk factors are young age, male sex, pre-existing chronic illness or neurodisability, a respiratory cause in the community, and a prolonged resuscitation. Drowning accounts for a large share of out-of-hospital arrests in the one-to-four-year age group, which makes supervision, pool fencing, and early bystander resuscitation the public-health interventions that change the incidence at the population level. [4][5]
Pathophysiology
The injury begins at the moment of arrest when the heart stops delivering oxygen and glucose to the brain. Neurons lose their ATP within seconds, the sodium-potassium ATPase fails, and sodium and water flood into the cell to produce cytotoxic oedema. The membrane depolarises, glutamate floods the synapse, and the resulting calcium influx drives a cascade of enzyme activation, free-radical generation, and mitochondrial failure that kills neurons within minutes. This is the primary injury, and it is fixed at the moment of return of spontaneous circulation. [7]
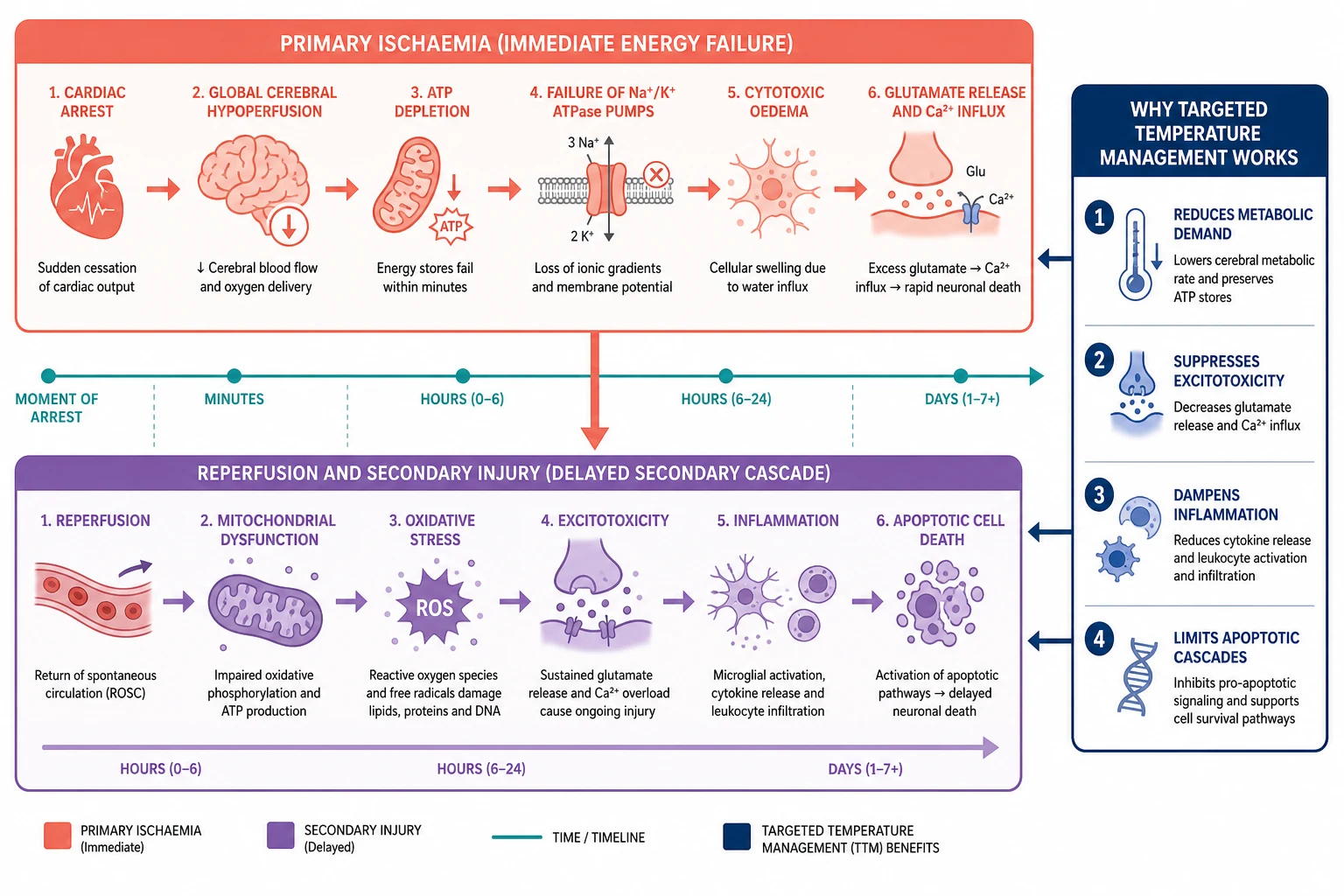
The secondary injury begins with reperfusion. The return of oxygen drives mitochondrial oxidative stress, the calcium influx perpetuates excitotoxicity, the blood-brain barrier opens to produce vasogenic oedema, and an inflammatory response amplifies the damage over hours to days. Secondary injury is also driven by anything the intensive care team fails to prevent: hypoxia, hypotension, hypercapnia, hypocapnia, fever, hyperglycaemia, and seizures all extend the lesion. This is the biological reason behind the neurocritical care bundle — each physiological target corresponds to a known amplifier of the secondary cascade. [7]
Cooling works because it attacks the secondary cascade at several points. A reduction in brain temperature reduces cerebral metabolic demand, suppresses excitotoxic neurotransmitter release, dampens the inflammatory response, and limits the apoptotic cascades that unfold over the first days. This multipoint action is why temperature management became the centrepiece of post-arrest care, and why the trials that tested it mattered so much to the field. [1][12]
Why does hyperventilation worsen the injured brain?
Aggressive hyperventilation lowers the carbon dioxide, which constricts the cerebral arterioles and reduces cerebral blood flow just when the injured brain is least able to tolerate it. Hypocapnia converts a salvageable region into an infarct. The target is normocapnia, and hyperventilation is reserved only for the transient management of impending herniation. [7]
Clinical Presentation
The child presents after return of spontaneous circulation, comatose and not following commands, and the clinical question is not whether brain injury has occurred but how severe it is and what the team can do to limit it. The examination is a structured coma assessment: the Glasgow Coma Scale or, in an intubated child, the motor component supplemented by the full outline of unresponsiveness score, the brainstem reflexes including pupillary, corneal, cough, and gag, the respiratory pattern, and the muscle tone and reflexes. [7]
The signs that raise a poor prognosis at seventy-two hours or beyond are an absent motor response, absent pupillary reflexes, or absent corneal reflexes, but none in isolation is sufficient, and none should be read before sedation has cleared. Seizures are common and often non-convulsive, which is why the examination must be paired with continuous EEG. Myoclonus, particularly status myoclonus in the first day, is a poor prognostic sign. The child with pre-existing neurodisability presents against a shifted baseline, and the team must establish the pre-arrest level of function from the family before interpreting the examination, because a deficit relative to the age norm may simply be the child's long-standing baseline. [11]
Differential Diagnosis
In the comatose post-arrest child the brain injury is almost always hypoxic-ischaemic, but the team must separate the contributors that drove the arrest and that continue to threaten the brain. The reversible threats are persistent hypoxia from pulmonary oedema or aspiration, persistent hypotension from cardiogenic shock or hypovolaemia, and persistent metabolic derangement such as hypoglycaemia or an electrolyte disturbance, all of which worsen the secondary injury and are corrected at the bedside. [6]
Hypoxic-ischaemic injury
the given diagnosis
- Global injury from the arrest, confirmed by the history
- No focal vascular territory, unlike stroke
- Secondary injury preventable with the bundle
- Outcome declared only at or beyond 72 hours
Non-convulsive status
a treatable mimic of coma
- Up to half of comatose post-arrest children
- Invisible to the bedside examination
- Detected on continuous EEG
- Treated with standard anticonvulsants
Drug effect and sedation
depresses the examination
- Sedatives and paralysers used in resuscitation
- Must clear before prognosticating
- Check a drug history and the timing of last dose
- Benzodiazepine reversal may confound seizures
Primary intracranial cause
may have caused or complicated the arrest
- Traumatic brain injury, haemorrhage, or meningitis
- Excluded by history, examination, and imaging
- May coexist with the hypoxic-ischaemic injury
- Sought actively in every case
A primary intracranial cause, such as traumatic brain injury, intracranial haemorrhage, or meningitis, may have caused the arrest or complicated it, and is excluded by the history, the examination, and a CT brain in the acute phase. Status epilepticus, often non-convulsive, may mimic ongoing coma and must be sought on continuous EEG. Sedation and paralysis from the drugs used in resuscitation can depress the examination, and the team must allow for their clearance before prognosticating. Sepsis and drug toxicity round out the reversible contributors that must be actively sought and treated alongside the neurocritical care. [7][9]
Clinical & Bedside Assessment
The bedside assessment runs in the first minutes after return of spontaneous circulation and repeats hourly throughout the admission. The airway is secured, the breathing is supported with mechanical ventilation, and the circulation is supported to an age-appropriate mean arterial pressure. The bedside glucose is checked and corrected, because hypoglycaemia both mimics and worsens brain injury. The temperature is measured continuously, because fever extends the lesion and must be prevented from the first hour. [7]
The focused neurological examination establishes the coma level, the brainstem reflexes, and the tone, and it is repeated over hours and days to detect change rather than to declare outcome. The history establishes the cause, the duration of no-flow and low-flow, whether the arrest was witnessed, and the pre-arrest neurological baseline, which is especially important in the child with known developmental delay. The general examination seeks the cause, including a cardiac murmur, signs of drowning or trauma, and evidence of infection. Continuous EEG is established early to detect non-convulsive seizures, which affect up to half of comatose post-arrest children and are invisible to the bedside examination. [9][8]
The post-arrest neurocritical care bundle
Investigations
The investigations serve three purposes: to monitor and support the brain, to find the cause, and to prognosticate. The cerebral monitor includes continuous EEG for seizures and background trends, near-infrared spectroscopy for cerebral oxygenation, and a continuous core temperature. The bloods include arterial blood gases for oxygenation, ventilation, and lactate, electrolytes, glucose, and a full blood count, with cardiac troponin when a cardiac cause is suspected. [7][8]
The cause search includes an echocardiogram and electrocardiogram for a cardiac source, blood cultures and inflammatory markers for sepsis, and a toxicology screen when ingestion is possible. Neuroimaging, usually a CT brain in the acute phase and an MRI brain later in the admission, excludes a primary intracranial cause and, over days, reveals the pattern and severity of the injury. The MRI may show cortical laminar necrosis, watershed-zone infarction, or basal-ganglia and thalamic injury, and the pattern carries prognostic weight — but it is never read in isolation. No single investigation defines the prognosis; the neuroprognostication is multimodal, combining the examination, the continuous EEG, the neuroimaging, and the biomarkers, and it is never made before 72 hours. [7]
Management — Resuscitation
Resuscitation is the immediate post-return-of-spontaneous-circulation stabilisation, and its single goal is to prevent secondary injury. The airway is secured and ventilated to normoxia and normocapnia. The oxygen is titrated down to the lowest concentration that avoids hypoxia, because hyperoxia drives oxidative stress in the reperfused brain. The ventilation targets a normal carbon dioxide, because both hypercapnia and hypocapnia harm the injured brain, and hypocapnia from over-ventilation constricts the cerebral vessels and worsens ischaemia. [7]
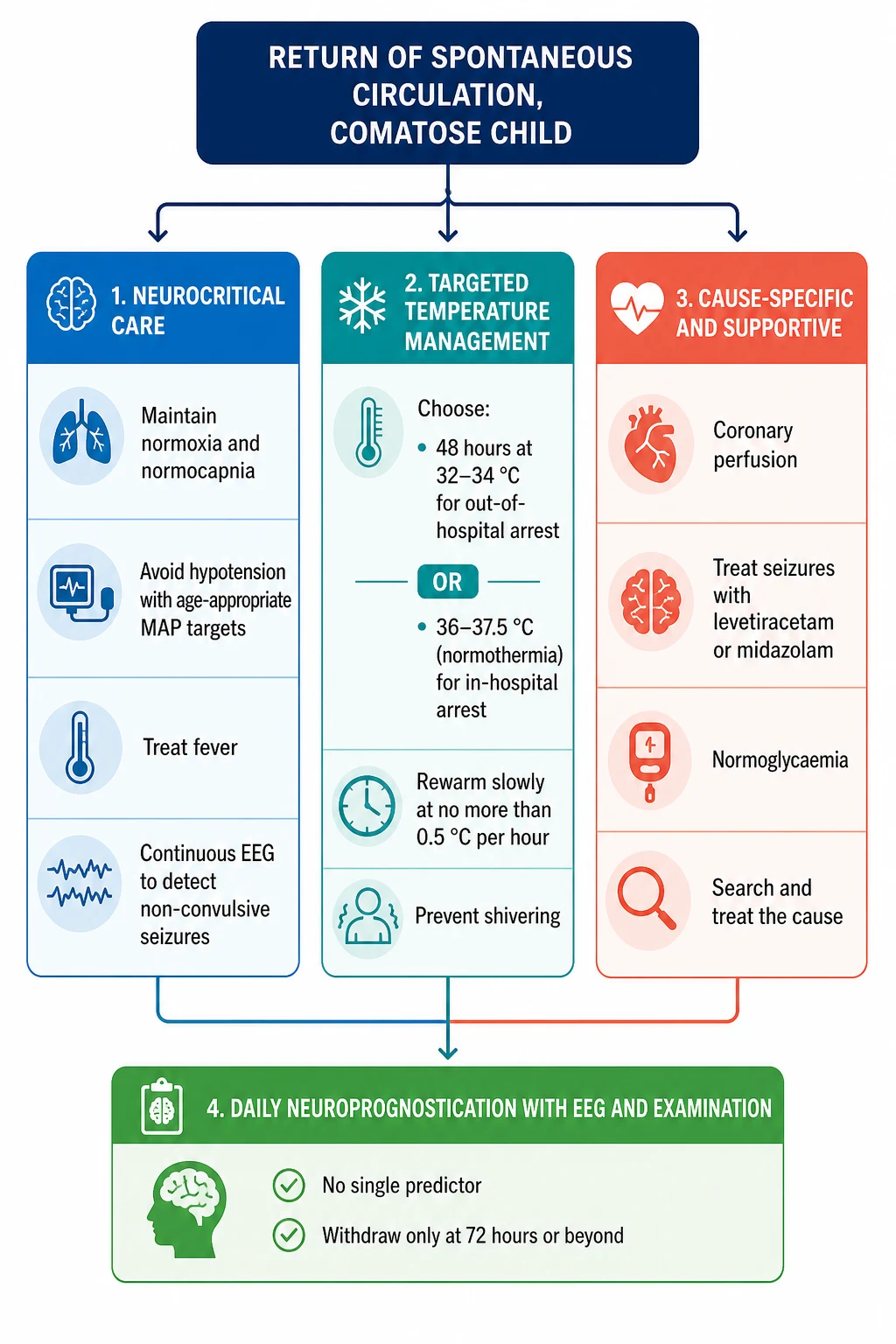
The circulation is supported with fluids and inotropes to an age-appropriate mean arterial pressure, because the injured brain has lost the autoregulation that normally protects it from blood-pressure swings. The bedside glucose is checked and maintained in the normal range, the temperature is measured and fever is treated, and seizures are sought on continuous EEG and treated with standard anticonvulsants. The child is transferred to the paediatric intensive care unit, the cause is sought and treated in parallel, and the family is informed of the critical illness and the genuine uncertainty of the early prognosis. The decision to initiate targeted temperature management is made in this window, and it is made as soon as the child is stable enough to begin cooling. [6][7]
Management — Definitive & Stepwise
The definitive management is targeted temperature management combined with the neurocritical care bundle. For a child who remains comatose after out-of-hospital arrest, targeted temperature management at 32 to 34 degrees Celsius for 48 hours is a reasonable choice, supported by a non-significant trend in the out-of-hospital trial and a favourable Bayesian reanalysis. For a child after in-hospital arrest, normothermia at 36 to 37.5 degrees with active fever prevention is the standard, because the in-hospital trial was stopped for futility. [1][2]
Targeted temperature management for paediatric hypoxic-ischaemic brain injury
Dose
Out-of-hospital arrest: 32 to 34 degrees Celsius for 48 hours. In-hospital arrest: normothermia at 36 to 37.5 degrees with active fever prevention
Rewarming is performed slowly, at no more than 0.5 degrees Celsius per hour, to avoid the rebound cerebral oedema, seizure burst, and metabolic stress that rapid rewarming provokes. Shivering is detected and treated, because it both raises the temperature and increases metabolic demand, defeating the purpose of cooling. The neurocritical care bundle maintains normoxia, normocapnia, normotension, normoglycaemia, and normothermia, runs continuous EEG with a protocol to detect and treat non-convulsive seizures within minutes, and treats the cause in parallel. The seizure management follows standard paediatric status epilepticus pathways, with a first-line agent and escalation as needed, all guided by the continuous trace. [7][9]
Targeted temperature management from return of circulation to prognostication
Stabilise the airway, breathing, and circulation; confirm normoxia, normocapnia, an age-appropriate MAP, and a normal glucose
Select the target: 32 to 34 degrees for 48 hours after out-of-hospital arrest, or 36 to 37.5 degrees normothermia after in-hospital arrest
Cool with a surface or intravascular device and a continuous core temperature; treat shivering with sedation and paralysis as needed
Maintain the target for 48 hours, running continuous EEG and treating non-convulsive seizures throughout
Rewarm at no more than 0.5 degrees Celsius per hour, then maintain normothermia and treat fever for the remainder of the admission
Run a multimodal neuroprognostication at 72 hours or beyond, combining examination, EEG, neuroimaging, and biomarkers
Specific Subtypes & Scenarios
The drowned child is the archetype of paediatric out-of-hospital arrest, and the management is the same post-arrest neurocritical care bundle with particular attention to three drowning-specific features. The first is the lung injury, because aspiration of water causes acute respiratory distress syndrome that complicates oxygenation and ventilation. The second is the hypothermia from immersion, which may have been protective during the arrest and which interacts with the temperature-management plan. The third is the possibility of cervical spine injury from a dive, which must be excluded before the collar is removed. [4][5]
The asphyxial arrest, from hanging, suffocation, or a foreign-body airway obstruction, follows the same neurocritical care pathway. The child with congenital heart disease arrests more often in hospital, usually around surgery or an arrhythmia, and the cause search drives the management toward cardiac optimisation, echocardiography, and discussion with the cardiology and cardiac surgery teams. The child with pre-existing neurobehavioural impairment presents against a shifted baseline, and Christensen and colleagues showed that these children have measurably different outcomes after cardiac arrest that must be judged against their pre-arrest function rather than an age-normative standard. The infant and the adolescent differ in physiology, pharmacology, and the likely cause, and the team adapts the temperature targets, the drug doses, and the rehabilitation plan to the age. [11][7]
Complications & Pitfalls
The acute complications are the secondary injury itself, status epilepticus which is often non-convulsive and detectable only on continuous EEG, posterior reversible encephalopathy, and the systemic complications of critical illness including acute kidney injury and myocardial stunning. The child is also at risk of the complications of immobility and intensive care, including pressure injury, venous thromboembolism, and critical-illness myopathy and neuropathy, which complicate the later rehabilitation. [7]
The classic diagnostic pitfalls are prognosticating too early — before 72 hours and before sedation has cleared — and relying on a single predictor such as an early EEG trace or a single biomarker. The classic therapeutic pitfalls are allowing hyperoxia or hyperventilation, accepting hypotension in the early post-arrest window, failing to detect and treat non-convulsive seizures, rewarming too fast, and failing to prevent fever during the maintenance phase. The communication pitfall is offering a definitive prognosis in the first days when the data are genuinely uncertain, which both misleads the family and biases the team's later assessment by anchoring it to an early, unreliable prediction. [8][6]
Prognosis & Disposition
The prognosis is determined by the duration of no-flow and low-flow, the cause, the early examination, the continuous EEG, the neuroimaging, and the biomarkers, and it is never declared before 72 hours. The continuous EEG background is among the strongest early predictors: Topjian and colleagues showed that early electroencephalographic background features predict the outcome in children resuscitated from cardiac arrest, and a normal or mildly abnormal background is reassuring while a suppressed or burst-suppressed background with electrographic seizures is worrying. [8]
Neuroprognostic indicators at 72 hours or beyond
Concerning
The overall survival to discharge for out-of-hospital arrest is lower than for in-hospital arrest, and a substantial minority of survivors are left with a cognitive or motor deficit, an epilepsy, or a movement disorder. Disposition is to the paediatric intensive care unit for the acute phase, to the ward for the recovery, and to a structured rehabilitation and neurodevelopmental follow-up programme that extends into the community. The family is supported through a structured communication that acknowledges the uncertainty of the early phase and the clarity that emerges over days, and that sets a date for the formal multidisciplinary prognostication. [7][5]
Special Populations
The child with pre-existing neurobehavioural impairment is the population whose baseline is shifted, and whose outcome must be judged against the pre-arrest function rather than an age-normative standard. Christensen and colleagues showed that these children have measurably different outcomes after cardiac arrest, and the practical implication is that the team must take a careful pre-arrest history from the family before interpreting any post-arrest assessment, because a deficit that looks new may be long-standing. [11]
The infant differs from the older child in the likely cause, the drug doses, and the temperature targets, and the team adapts the protocol to the age, with weight-based dosing and careful attention to the immature cerebral autoregulation. The Aboriginal and Torres Strait Islander child and the child from a remote setting presents after a longer no-flow time because of distance, and retrieval pathways and culturally appropriate communication are part of the care. The child from a refugee or migrant family needs an early interpreter and a sensitive discussion of the cause and the prognosis. The adolescent who arrests from a suicide attempt by hanging or overdose needs the same neurocritical care followed by a mental-health and safeguarding response, because the survival of the brain is only the first step in the survival of the young person. [7]
Evidence, Guidelines & Regional Differences
The evidence rests on the two THAPCA trials. The out-of-hospital trial of Moler and colleagues compared hypothermia at 33 degrees with normothermia at 36.8 degrees in 295 children and found a non-significant trend toward better survival with a good functional outcome in the hypothermia group, at 20 percent against 12 percent. The in-hospital trial was stopped for futility after 329 children, with no difference between the groups at 36 percent against 39 percent. The trials established that targeted temperature management is safe and that both targets are defensible, while leaving the choice between them to the clinician and the clinical context. [1][2]
THAPCA-OH (Moler, NEJM 2015)
Multicentre randomised trial of hypothermia at 33 degrees versus normothermia at 36.8 degrees in 295 comatose children after out-of-hospital cardiac arrest
Key finding
Survival with a good functional outcome at 1 year was 20 percent with hypothermia against 12 percent with normothermia, a non-significant difference. A later Bayesian reanalysis found a high probability of a modest hypothermia benefit
Practice change
Hypothermia is a reasonable and defensible option for the comatose child after out-of-hospital arrest; the result is non-significant but trended favourably
The controversy is the interpretation of the out-of-hospital trial. A frequentist reading concludes that hypothermia is not proven superior, while a Bayesian reanalysis by Harhay and colleagues concluded that there is a high probability that hypothermia provides a modest benefit in neurobehavioural outcome and survival at one year. This leaves the clinician with two defensible choices for the out-of-hospital child and is the reason that guidelines accept both. The 2020 American Heart Association guidelines of Topjian and colleagues recommend targeted temperature management for the comatose post-arrest child, accept both hypothermia and normothermia as reasonable, and make the prevention and treatment of fever a clear priority. The paediatric meta-analyses of Wieczorek and Buick and colleagues converge on the conclusion that neither strategy is clearly superior and that the quality of the neurocritical care bundle may matter more than the temperature target itself. [3][7][10][12]
Exam Pearls
Hypoxic-ischaemic brain injury after paediatric cardiac arrest splits into a primary injury that is fixed and a secondary injury that intensive care targets. The single neuroprotective intervention is targeted temperature management: 32 to 34 degrees for 48 hours after out-of-hospital arrest, or 36 to 37.5 degrees normothermia with active fever prevention after in-hospital arrest, with rewarming at no more than 0.5 degrees per hour. The THAPCA out-of-hospital trial showed 20 percent against 12 percent, a non-significant trend; the in-hospital trial was stopped for futility at 36 percent against 39 percent; and the Bayesian reanalysis found a high probability of a modest hypothermia benefit. [1][2][3]
Early postresuscitation hypotension is strongly associated with worse survival, so an age-appropriate mean arterial pressure is defended from the first hour. Up to half of comatose post-arrest children have non-convulsive seizures, so continuous EEG is mandatory. Neuroprognostication is multimodal and deferred to at least 72 hours, and no single predictor is sufficient. Drowning is the dominant cause of paediatric out-of-hospital arrest. The child with pre-existing neurodisability is judged against their pre-arrest baseline, not an age norm. [6][9][11]
References
- [1]Moler FW, Silverstein FS, Holubkov R, et al Therapeutic hypothermia after out-of-hospital cardiac arrest in children. N Engl J Med, 2015.PMID 25913022
- [2]Moler FW, Silverstein FS, Holubkov R, et al Therapeutic Hypothermia after In-Hospital Cardiac Arrest in Children. N Engl J Med, 2017.PMID 28118559
- [3]Harhay MO, Topjian AA, Karlawish J, et al A Bayesian Interpretation of a Pediatric Cardiac Arrest Trial (THAPCA-OH). NEJM Evid, 2023.PMID 38320098
- [4]Szpilman D, Webber J, Quan L, et al Drowning. N Engl J Med, 2012.PMID 22646632
- [5]Slomine BS, Silverstein FS, Christensen JR, et al Pediatric cardiac arrest due to drowning and other respiratory etiologies: Neurobehavioral outcomes in initially comatose children. Resuscitation, 2017.PMID 28274812
- [6]Topjian AA, French B, Sutton RM, et al Association of Early Postresuscitation Hypotension With Survival to Discharge After Targeted Temperature Management for Pediatric Cardiac Arrest. JAMA Pediatr, 2018.PMID 29228147
- [7]Topjian AA, Raymond TT, Atkins D, et al Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2020.PMID 33081526
- [8]Topjian AA, Sanchez SM, Shultz MJ, et al Early Electroencephalographic Background Features Predict Outcomes in Children Resuscitated From Cardiac Arrest. Pediatr Crit Care Med, 2016.PMID 27097270
- [9]Topjian AA, Gutierrez-Colina AM, Sanchez SM, et al Detection of electrographic seizures by critical care providers using color density spectral array after cardiac arrest. Pediatr Crit Care Med, 2015.PMID 25651050
- [10]Wieczorek W, Kedziora J, Smereka J, et al Efficacy of Targeted Temperature Management after Pediatric Cardiac Arrest: A Meta-Analysis of 2002 Patients. J Clin Med, 2021.PMID 33808425
- [11]Christensen JR, Silverstein FS, Holubkov R, et al Cardiac Arrest Outcomes in Children With Preexisting Neurobehavioral Impairment (from the THAPCA Trials). Pediatr Crit Care Med, 2019.PMID 30807545
- [12]Buick JE, Lin Y, Brooks SC, et al Paediatric targeted temperature management post cardiac arrest: A systematic review and meta-analysis. Resuscitation, 2019.PMID 30951842