Paeds · neurology-neurodisability-and-neuromuscular
Moderate and severe traumatic brain injury
Also known as Severe head injury · Severe TBI · Paediatric brain trauma · Intracranial hypertension after trauma · Diffuse axonal injury
Fellowship guide to moderate and severe traumatic brain injury in children. Covers the Glasgow Coma Scale severity bands of mild 13 to 15, moderate 9 to 12, and severe 3 to 8 with the paediatric verbal modification, the Monro-Kellie doctrine and the cerebral perfusion pressure equation, the primary versus secondary brain injury cascade from hypotension and hypoxia to herniation, the structured primary survey with cervical spine immobilisation and intubation for GCS 8 or less, computed tomography and intracranial pressure monitoring, the Brain Trauma Foundation pediatric guideline threshold of treating intracranial pressure over 20 mmHg while keeping cerebral perfusion pressure at least 40 mmHg, the stepwise ladder from head elevation and sedation through 3 percent saline and mannitol to barbiturate coma and decompressive craniectomy, the Hutchison hypothermia trial and the DECRA decompressive craniectomy trial, the recognition of Cushing triad and uncal herniation, and the neurorehabilitation and developmental follow-up.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who does not open the eyes, speak, or obey commands after a head strike has a serious brain injury, and the job at that bedside is to protect the brain from the second, preventable wave of damage. Traumatic brain injury is brain damage caused by an external mechanical force, and in moderate and severe cases the threat is not only the bruise or the bleed that the impact caused, but the swelling, the hypoxia, and the falling blood pressure that follow it. The clinical question at the bedside is always the same: which child is in danger, and what must be done in the next few minutes to keep the brain perfused. [4]
The severity of the injury is graded by the Glasgow Coma Scale, the practical scoring system introduced by Teasdale and Jennett that turns a bedside observation into a number that drives every decision. The scale scores eye opening, verbal response, and motor response, and the total places the child on a spectrum from mild to severe. The line that matters most is at a score of eight. A child at or below eight cannot protect the airway and is at high risk of rising pressure inside the skull, which is why the airway, the breathing, and the circulation come before any scan. [1]
Three ideas make this topic central to the paediatric exam. The damage done at impact cannot be undone, but the damage that follows can be prevented, and so every minute of resuscitation is brain salvage. The Glasgow Coma Scale is the universal currency that decides who is intubated, who is scanned, and who is monitored. And the intracranial pressure ladder, built on the cerebral perfusion pressure equation, is the framework a fellow must run when the brain begins to swell. The Brain Trauma Foundation set these principles out for children in its guidelines, which remain the single most testable source on the topic. [5]
Classification
The Glasgow Coma Scale turns the bedside observation of consciousness into a number, and that number sorts the child into a severity band that drives the entire plan. The scale has three parts. Eye opening is scored from one to four, verbal response from one to five, and motor response from one to six, giving a total from three to fifteen. The lower the number, the sicker the brain, and the score is reassessed often because the trend is more informative than any single reading. [1]
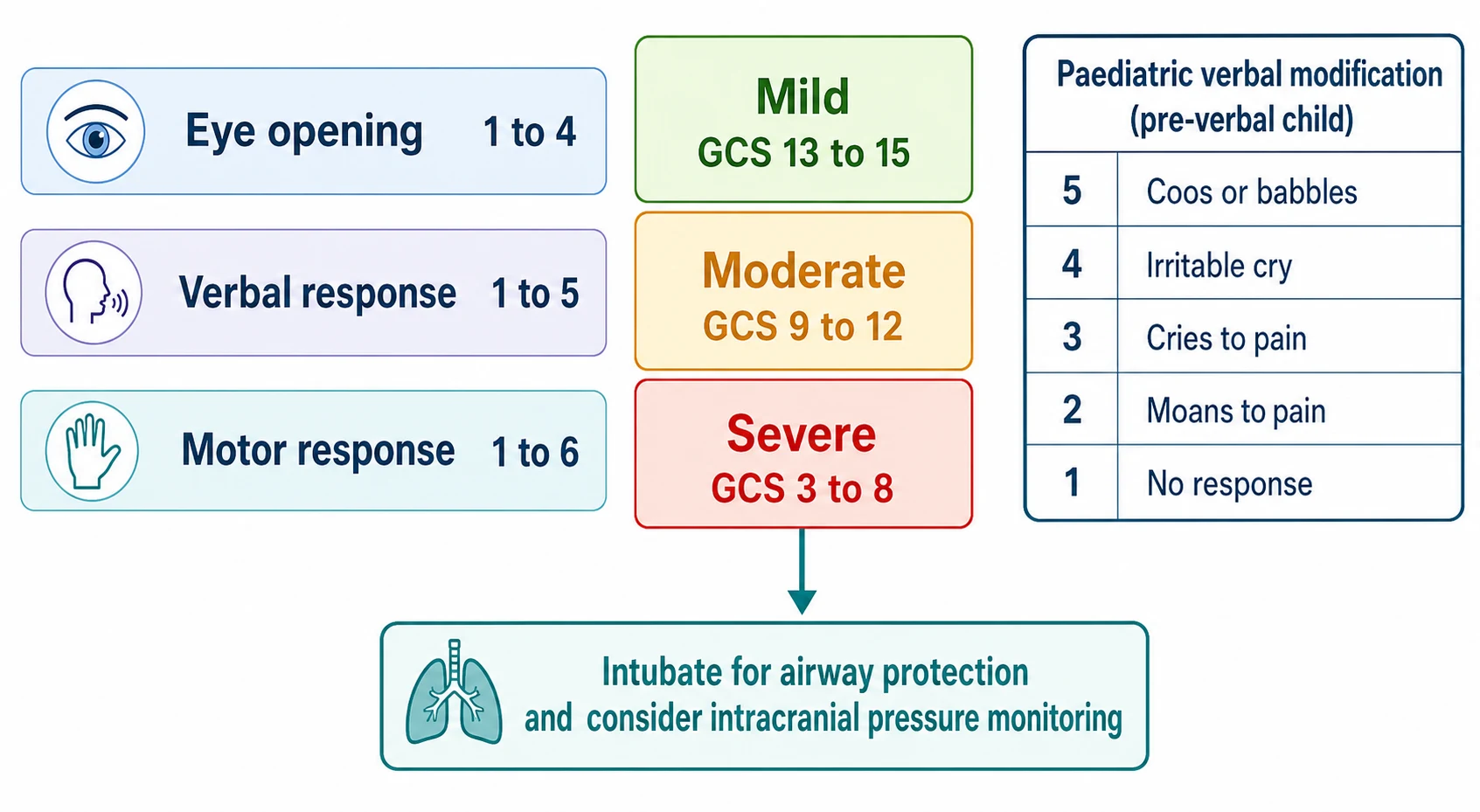
The total score sorts the injury into three bands, and the cut-off at eight is the one to remember. A score of 13 to 15 is mild injury, 9 to 12 is moderate, and 3 to 8 is severe. The child with a score of 8 or less cannot protect the airway and is at high risk of intracranial hypertension, so the number eight is the trigger to intubate, to scan, and to monitor. The moderate child, in the 9 to 12 band, is lethargic or confused and can deteriorate, which is why repeated scoring and a low threshold to escalate matter here too. [4]
The scale was built for adults, and the verbal component fails in the infant and the preverbal child who cannot speak. The paediatric modification keeps the structure but adapts the verbal score to what a young child can do. A score of five is a child who coos and babbles, four is an irritable cry that can be consoled, three is a cry only to pain, two is a moan to pain, and one is no response. The motor score also adapts for the small infant, but the eye and motor components are largely preserved. Kirkham and colleagues reviewed the paediatric coma scales and confirmed that the modified scale is the standard for young children in the emergency setting. [2]
Epidemiology & Risk Factors
Traumatic brain injury is the leading cause of death and disability in children older than one year across high-income countries, and the severe end of the spectrum, though less common than concussion, is where the mortality and the long-term disability concentrate. The mechanism shifts with age. Falls dominate in the toddler, road traffic crashes and sport in the school-age child and the adolescent, and non-accidental injury is a leading cause in the infant. The severe injury, with a score of 8 or less, carries a mortality of 10 to 30 percent in modern paediatric intensive care, and the majority of survivors carry some residual cognitive, behavioural, or motor disability. [6]
The risk factors for a poor outcome are the facts the fellow must seek at first contact, because each is preventable. A low systolic blood pressure at the scene or on arrival is the strongest predictor of death, and a single hypotensive episode doubles the mortality. Hypoxia, an abnormal computed tomography with a mass lesion or swelling, pupil abnormalities, and younger age each add to the risk. Ducrocq and colleagues, in a large paediatric trauma centre series, showed that hypotension, pupil abnormalities, and hypoxia were the dominant early predictors of both mortality and unfavourable outcome, which is why the prevention of these secondary insults is the entire rationale of resuscitation. [6]
Pathophysiology
The damage done by a head injury falls into two waves, and only the second can be treated. The first wave, the primary injury, is the mechanical damage at the instant of impact, the contusion, the diffuse axonal shearing, the haematoma, and the skull fracture. It is done before the child reaches hospital, and it cannot be reversed. The second wave, the secondary injury, is the cascade of swelling, ischaemia, and chemical injury that unfolds over the hours that follow, and it is the target of every intervention in this topic. [4]
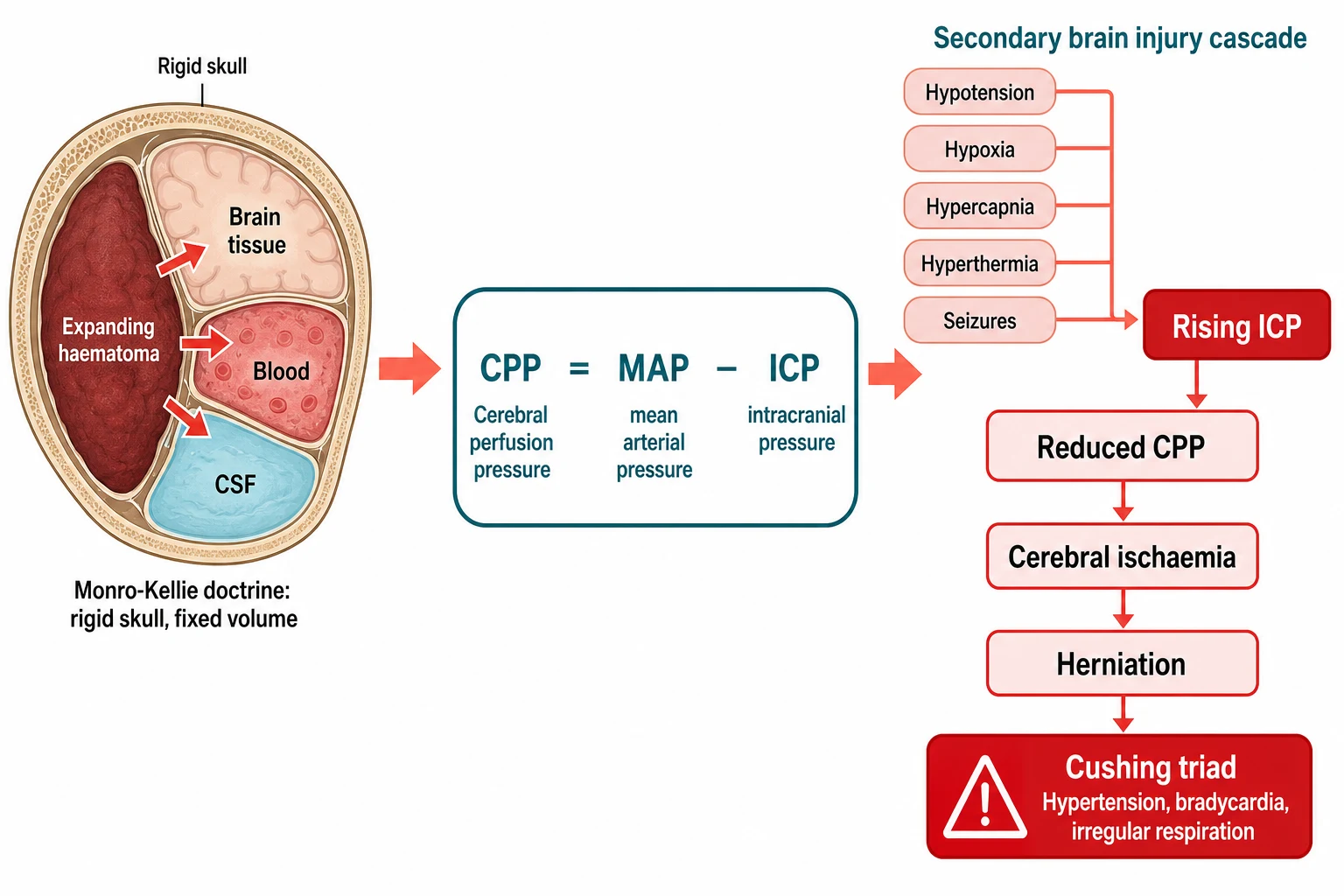
The reason the brain swells and fails sits in a simple physical fact about the skull. The skull is a rigid box that holds three things, the brain tissue, the blood, and the cerebrospinal fluid, in a fixed total volume, a principle known as the Monro-Kellie doctrine. When a haematoma expands or the brain swells, the volume inside the box rises, and because the box cannot expand, the pressure inside it rises instead. The compensatory reserve is soon exhausted, and beyond a critical point any further increase in volume causes a steep climb in pressure. [4]
The pressure that matters for the brain is not the intracranial pressure alone but the pressure that drives blood into it, and the two are linked by a single equation. Cerebral perfusion pressure is the mean arterial pressure minus the intracranial pressure. As the intracranial pressure climbs, the perfusion pressure falls, the cerebral blood flow drops, the brain becomes ischaemic, and the ischaemia worsens the swelling in a vicious cycle. The equation is the reason that a high intracranial pressure and a low blood pressure are both lethal, because together they collapse the perfusion pressure. [4]
The systemic insults compound the cascade, and each one is preventable. Hypotension lowers the mean arterial pressure and so the perfusion pressure. Hypoxia starves the already ischaemic brain. Hypercapnia from under-ventilation dilates the cerebral blood vessels and increases the cerebral blood volume, which raises the intracranial pressure. Hyperthermia and seizures raise the metabolic demand of the injured brain. This is the secondary brain injury cascade, and it is why the intensive care of severe traumatic brain injury is, in essence, the relentless prevention of hypotension, hypoxia, hypercapnia, hyperthermia, and seizures. [4]
The end of the cascade is herniation, when the swollen brain shifts within the skull and compresses the brainstem. The clinical sign is the fixed dilated pupil, the lateralised motor posturing, and, in the final stage, the Cushing triad of hypertension, bradycardia, and irregular respirations. The Cushing triad is a late and preterminal sign, and the fellow who waits for it before treating the intracranial pressure has left the run too late. [4]
Clinical Presentation
The severely injured child arrives unconscious, and the presentation is the depressed conscious state after a known or suspected head strike. The child does not open the eyes to pain, does not speak, and may localise poorly or posture to stimulation, giving a score of 8 or less after resuscitation. The breathing may be shallow or irregular, the airway may be compromised by secretions or vomit, and the child may show the systemic signs of associated injury. The moderate child, with a score of 9 to 12, is drowsy or confused and answers slowly, and the danger in this band is the child who deteriorates over the first hours. [1]
How moderate and severe injury presents across the age spectrum
An infant who is irritable then drowsy after a fall, with a bulging fontanelle and a possible expanding subdural or subgaleal bleed through the open sutures
A toddler who is obtunded after a fall from a height, with a score around 9 to 12 and a risk of deterioration from an evolving haematoma
A school-age child knocked unconscious in a road traffic crash, with a score of 8 or less and possible diffuse axonal injury
An adolescent with a brief lucid interval after a temporal blow followed by rapid loss of consciousness, the classic extradural haematoma
A child with a deteriorating score after an initially normal computed tomography, signalling an evolving mass or swelling that needs a repeat scan
The focused neurological examination looks for the signs that locate and grade the injury, and it runs once the airway and breathing are secured. The pupils are checked for size and reactivity, and a unilateral fixed dilated pupil is uncal herniation compressing the third nerve until proven otherwise. The motor response is checked for a lateralised weakness or an asymmetrical posturing, which localises the lesion. The head and neck are examined for the signs of skull fracture, for the racoon eyes and Battle sign of a basal skull fracture, and for cervical spine tenderness, because a significant head injury is assumed to carry a cervical spine injury until cleared. [4]
Two presentations are deliberately examined because they catch the unwary. The first is the lucid interval, the child who is briefly knocked out, wakes and talks, then slides back into coma as an extradural haematoma expands, and the recognition of this pattern is the trigger for an urgent scan and neurosurgical evacuation. The second is the infant, in whom the open sutures allow a subdural or subgaleal bleed to expand, so the child may present in shock or with a rapid fall in conscious state rather than the classic adult picture. In any infant with a subdural bleed, retinal haemorrhages, or an inconsistent story, non-accidental injury is the working assumption until excluded. [2]
Differential Diagnosis
The depressed conscious state after an apparent head strike has several explanations, and the task is to separate the surgical traumatic lesion from its mimics and from the medical causes that may coexist. The structural traumatic lesions are the extradural, subdural, and intraparenchymal bleeds and the diffuse axonal injury, and each has a pattern. The mimics and the coexisting medical causes must not be missed, because they change the treatment. [4]
Extradural haematoma
surgical emergency
- Lens-shaped bleed between skull and dura, often temporal
- Fracture across the middle meningeal artery
- Classic lucid interval then rapid deterioration
- Urgent neurosurgical evacuation
Subdural haematoma
common in infants
- Crescent-shaped bleed from bridging vein rupture
- Common in infants and in non-accidental injury
- Carries a poorer prognosis than extradural
- Often needs evacuation, safeguarding review
Diffuse axonal injury
no surgical mass
- Immediate coma from high-energy rotational force
- Computed tomography may look deceptively normal
- Magnetic resonance imaging shows white matter lesions
- Supportive intensive care, no evacuation
Postictal or metabolic
mimic
- Prolonged postictal state after a seizure
- Hypoglycaemia, intoxication, or diabetic ketoacidosis
- May coexist with a genuine head strike
- Treat the cause and recheck the score
The extradural haematoma is the surgical emergency, a lens-shaped bleed between the skull and the dura, most often temporal, from a fracture across the middle meningeal artery. The classic story is the lucid interval, and the response is an urgent computed tomography and neurosurgical evacuation, because the outcome is excellent if the bleed is evacuated before the brainstem is compressed. The subdural haematoma is a crescent-shaped bleed from a torn bridging vein, more common in infants and in non-accidental injury, and it carries a poorer prognosis. Diffuse axonal injury, from a high-energy rotational force, presents as immediate coma with a scan that may look deceptively mild, and the magnetic resonance imaging later shows the characteristic shearing lesions in the white matter. [4]
The mimics deserve a moment, because a head strike may be incidental to the real problem. A prolonged postictal state after a seizure, an alcohol or drug intoxication, a hypoglycaemic episode, and a diabetic ketoacidosis can each present as a depressed conscious state, and each may coexist with a genuine injury. The bedside glucose is checked in every child, the cause is sought in parallel with the scan, and the score is reassessed once the reversible factor is corrected. [4]
Clinical & Bedside Assessment
The assessment of the severely head-injured child is the structured primary survey, run in parallel with resuscitation rather than after it. The airway is assessed first and cleared, high-flow oxygen is applied, and the cervical spine is immobilised from the outset, because a significant head injury is assumed to carry a cervical spine injury until imaging clears it. The breathing is assessed for rate, effort, and oxygen saturation, and the circulation is assessed for perfusion and blood pressure, because the prevention of hypoxia and hypotension is the prevention of secondary brain injury. [4]
The Glasgow Coma Scale is scored repeatedly, because the trend matters more than any single number. The scale is applied with the paediatric verbal modification in the preverbal child, the best motor response is sought from a central stimulus, and the score is recorded with the time. A falling score by two points, a new pupil abnormality, or a rising blood pressure with a falling heart rate are each a signal of deterioration that demands an immediate reassessment and usually a repeat scan. [1]
The weight is needed for every drug and every fluid bolus, and it is obtained by weighing the child, asking the parent, or using a length-based tape when weighing is impossible. The drug doses in this topic are all weight-based, and an under-dose of a hyperosmolar agent or an under-resuscitation of a hypotensive child are common errors that worsen the secondary injury. The intravenous access is secured early, and blood is sent for glucose, electrolytes, coagulation, a full blood count, a venous gas, and alcohol and drug levels as the resuscitation proceeds. [4]
Investigations
The non-contrast computed tomography of the head is the key acute investigation, and it is performed once the airway, breathing, and circulation are stable enough for transfer. The scan looks for the surgical mass lesions that need evacuation, for the haemorrhage, the fractures, the swelling, and the midline shift that signal raised pressure. A child with a severe injury needs a scan regardless of the rules, and the rules exist to guide the decision in the mild case. [3]
The PECARN rule of Kuppermann and colleagues is the validated decision aid that identifies the child at very low risk of a clinically important brain injury after a mild head strike, in whom a scan can safely be deferred. The rule is built on the age, the mechanism, the history of loss of consciousness, the signs at the bedside, and the scalp and skull findings, and it operates in two age bands, under two years and two years and older. While the rule governs the mild case, the moderate and severe child is scanned without it, but the rule is the most testable single piece of imaging evidence on the topic and is frequently examined alongside the severe pathway. [3]
Blood is sent for a full panel that supports both the resuscitation and the search for the cause. Glucose excludes hypoglycaemia, electrolytes and a venous gas guide the fluid and ventilation, coagulation is checked because a bleeding child may need correction, and alcohol and drug levels are sent when intoxication is possible. A group and save is taken because the polytrauma child may need blood. A cervical spine computed tomography is performed with the head scan in the severely injured child, because the cervical spine is presumed injured until cleared. [4]
Intracranial pressure monitoring is placed in the severe injury with an abnormal scan, and it guides the therapy against the treatment threshold of 20 mmHg. The monitor is an intraparenchymal probe or an external ventricular drain, and the drain has the advantage that it allows cerebrospinal fluid to be drained as a therapy. The Brain Trauma Foundation pediatric guidelines also support monitoring in the severe injury with a normal scan when risk factors such as motor posturing or hypotension are present, because the pressure can still be high. [4]
Management — Resuscitation
The resuscitation of the severely head-injured child is the structured primary survey, and the single aim is to prevent the secondary brain injury that follows the impact. The airway is secured and the cervical spine immobilised, and any child with a score of 8 or less is intubated, because the unprotected airway and the underventilated lung are the immediate threats. The intubation is by a rapid sequence technique, and the drugs are chosen to avoid a fall in blood pressure, because the hypertensive response to laryngoscopy and the hypotensive effect of the induction agent both need to be managed. [4]
The breathing is controlled to keep the brain well oxygenated and the carbon dioxide in the normal range. The oxygen saturation is kept above 94 percent and the PaO2 above 80 mmHg, and the ventilation targets a PaCO2 of 35 to 40 mmHg, the normocapnic range that avoids the cerebral vessel dilation of hypercapnia and the cerebral vessel constriction of aggressive hypocapnia. Prophylactic hyperventilation is not used, because the constriction it causes reduces the cerebral blood flow and can worsen the ischaemia, and a brief period of hyperventilation is reserved only as a temporary measure for the acutely herniating child while the definitive therapy is prepared. [4]
The circulation is managed to keep the blood pressure age-appropriate, because the hypotensive child loses perfusion pressure and dies. Isotonic fluid boluses are given for hypovolaemia, blood is transfused for the bleeding child, and the cause of the hypotension, often an associated injury, is sought and treated. The glucose is checked and corrected, the seizures are treated with a benzodiazepine, and prophylactic anticonvulsants such as levetiracetam or phenytoin are given in the first seven days to prevent the early post-traumatic seizures that raise the metabolic demand and the intracranial pressure. Stulce and colleagues showed that fluid overload is itself associated with worse outcome, which is why the fluid is isotonic, goal-directed, and not excessive. [4][10]
The head is kept midline and elevated to 30 degrees to aid the venous drainage, and the temperature is kept normal, because fever raises the metabolic demand of the injured brain. Prophylactic hypothermia is not used, for reasons the evidence section explains, and the child is kept normothermic with antipyretics and cooling as needed. The hypoglycaemia is corrected, the pain is controlled, and the agitated child is sedated, because agitation and pain raise the intracranial pressure. [7]
Management — Definitive & Stepwise
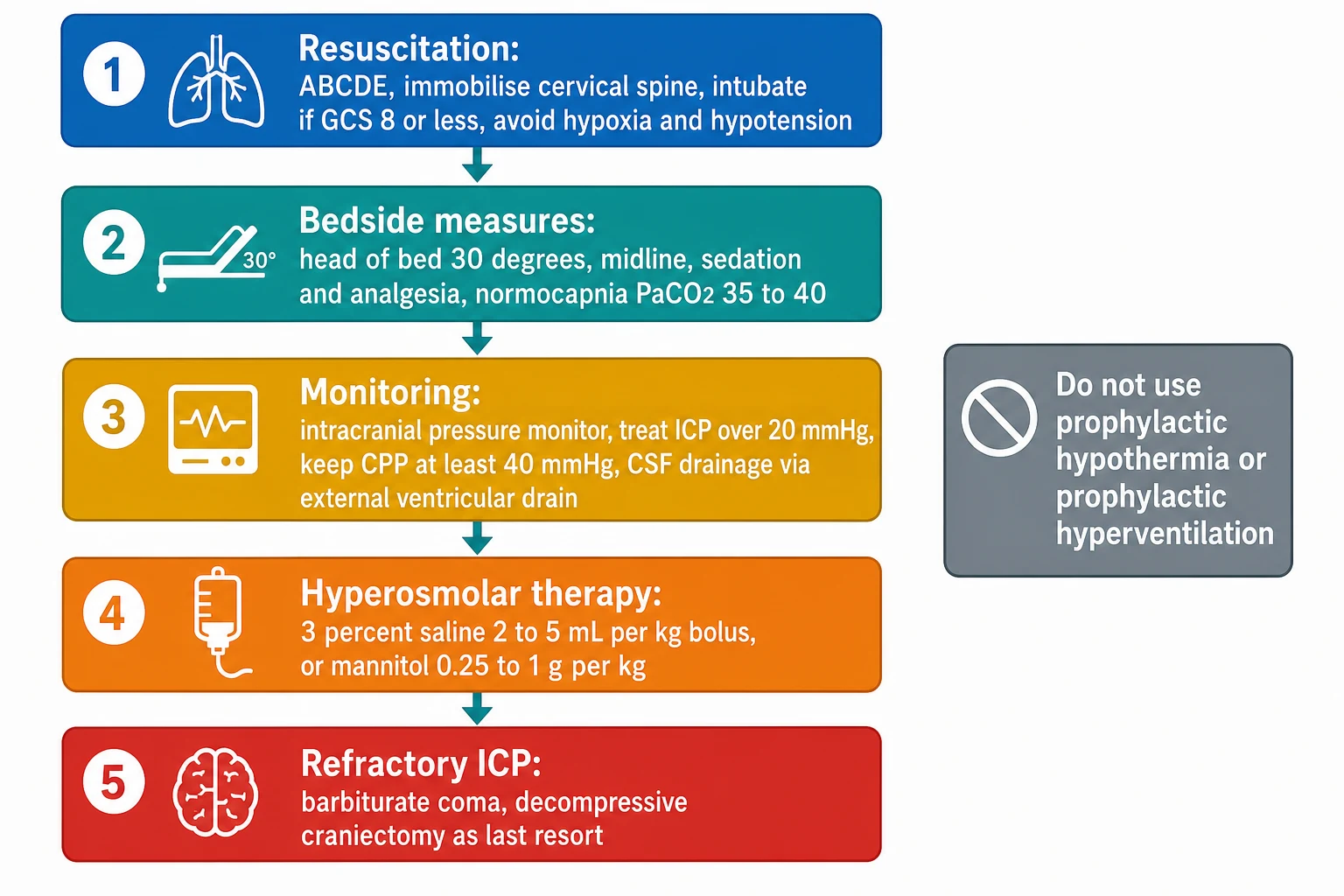
The definitive care is the stepwise intracranial pressure management ladder, and it is built on two numbers from the Brain Trauma Foundation pediatric guidelines. The intracranial pressure is treated when it rises above 20 mmHg, and the cerebral perfusion pressure is kept at least 40 mmHg. The ladder moves from the simple bedside measures to the hyperosmolar agents, and then to the refractory options, and each step is justified by the physiology. [4]
[4]The first steps are the bedside measures that lower the pressure without drugs. The head of the bed is elevated to 30 degrees and kept midline to improve the venous drainage, the child is sedated and given analgesia to reduce the metabolic demand and the agitation, and a neuromuscular blocker is added if the child fights the ventilator. If an external ventricular drain is in place, the cerebrospinal fluid is drained to lower the pressure directly. These measures are tried first because they are effective and carry the least risk. [4]
The next step is the hyperosmolar therapy, and the two agents are 3 percent saline and mannitol. A 3 percent saline bolus of 2 to 5 mL per kg lowers the intracranial pressure by drawing water out of the swollen brain, and it is the preferred first agent in many paediatric pathways because it also expands the circulating volume and supports the blood pressure. The serum sodium and osmolality are monitored, and the therapy is titrated to the pressure. Wu and colleagues confirmed that hypertonic saline reliably lowers the intracranial pressure in severe paediatric injury. The alternative is mannitol at 0.25 to 1 g per kg, which also draws water from the brain but can cause a diuresis and a fall in blood pressure, so it is given with attention to the circulating volume. [4][9]
Hyperosmolar therapy for raised intracranial pressure
Dose
3 percent saline 2 to 5 mL per kg bolus over 10 to 20 minutes, or mannitol 0.25 to 1 g per kg intravenously
If the pressure remains refractory, the ladder moves to the stronger options. A barbiturate coma, with pentobarbital or thiopentone titrated to burst suppression on the electroencephalogram, suppresses the cerebral metabolic rate and lowers the pressure, and it is used for the refractory case that has not responded to the simpler measures. Decompressive craniectomy, the removal of a large piece of skull to let the swollen brain expand, is the last-resort surgical option for the genuinely refractory case. The DECRA trial of Cooper and colleagues, though conducted in adults, showed that an early decompressive craniectomy for refractory pressure was associated with worse outcomes, which is why the operation is reserved for the case that has failed the medical ladder rather than used early. [5][8]
The stepwise intracranial pressure management ladder
Resuscitate with ABCDE, immobilise the cervical spine, intubate for a GCS of 8 or less, and maintain normoxia and normotension
Elevate the head of bed to 30 degrees, keep midline, give sedation and analgesia, and ventilate to a PaCO2 of 35 to 40 mmHg
Place an intracranial pressure monitor, treat the pressure over 20 mmHg, keep the cerebral perfusion pressure at least 40 mmHg, and drain CSF
Give hyperosmolar therapy with 3 percent saline 2 to 5 mL per kg or mannitol 0.25 to 1 g per kg
For refractory pressure, start a barbiturate coma titrated to burst suppression, and reserve decompressive craniectomy for the last-resort case
A subtlety in the refractory phase is the role of hyperventilation and hypothermia, both of which were once used and are now avoided. Prophylactic hyperventilation constricts the cerebral vessels and reduces the blood flow, and it is reserved only for the brief, temporary management of the acutely herniating child. Prophylactic hypothermia was tested by Hutchison and colleagues in a large multicentre trial, and it did not improve the outcome and raised concern about harm, which is why normothermia is the target and hypothermia is not used as a treatment. [7]
Specific Subtypes & Scenarios
The extradural haematoma is the scenario in which the right operation cures the child, and the recognition of its pattern is a high-yield exam point. The bleed sits between the skull and the dura, most often in the temporal fossa, from a fracture that crosses the middle meningeal artery. The classic story is the lucid interval, in which the child is briefly knocked out, wakes and talks, then slides back into coma as the bleed expands. The response is an urgent computed tomography and neurosurgical evacuation, and the outcome is excellent when the bleed is removed before the brainstem is compressed. [4]
The subdural haematoma is the scenario that is common in infants and in non-accidental injury, and it carries a poorer prognosis. The bleed comes from a torn bridging vein and sits in the crescent-shaped subdural space, and in the infant the open sutures allow it to expand. The clinical picture in the infant may be shock, seizures, or a rapid fall in conscious state, and the finding of a subdural bleed with retinal haemorrhages or an inconsistent story mandates a safeguarding workup alongside the neurocritical care. [2]
Diffuse axonal injury is the scenario of the high-energy rotational crash, and it presents as immediate coma without a surgical mass. The computed tomography may look deceptively mild, and the diagnosis is confirmed by the magnetic resonance imaging, which shows the characteristic shearing lesions in the corpus callosum and the brainstem white matter. The management is supportive intensive care on the standard ladder, and the outcome is driven by the severity of the axonal damage and by the prevention of secondary insults. [4]
The abusive head trauma scenario is the one in which the mechanism and the safeguarding are as important as the neurocritical care. An infant with a subdural bleed, retinal haemorrhages, rib or long-bone fractures, or an inconsistent history is managed for the brain injury on the standard ladder, and in parallel the safeguarding pathway is activated, the ophthalmology review is sought, the skeletal survey is performed, and the social work and child protection teams are engaged. The recognition of the pattern is the first step, because the brain injury will recur if the child returns to an unsafe environment. [2]
Complications & Pitfalls
Herniation is the feared intracranial complication, and it is the failure mode that every step of the ladder is designed to prevent. The clinical sign is the fixed dilated pupil, the lateralised motor posturing, and the Cushing triad, and it is a neurosurgical emergency that demands an immediate reduction of the pressure. The systemic complications of the prolonged intensive care stay are also real, and they include the ventilator-associated pneumonia, the venous thromboembolism, the pressure injury, and the sodium disturbances of the syndrome of inappropriate antidiuretic hormone and the diabetes insipidus that often follow a severe brain injury. [4]
The classic pitfalls are the preventable errors that cost the brain. The first is the failure to protect the cervical spine while managing the head, because the child with a head injury is assumed to have a cervical spine injury until cleared. The second is the tolerance of hypotension or hypoxia during the transfer, when a single episode of either doubles the mortality. The third is the under-treatment of the intracranial pressure, the fellow who waits for the Cushing triad before acting, when the triad is a late and preterminal sign. The fourth is the use of prophylactic hyperventilation or prophylactic hypothermia in the belief that they help, when both can worsen the outcome. [6]
A subtler pitfall is the reliance on a normal early computed tomography in a child who is clinically deteriorating. The scan is a snapshot, and a bleed or a swelling can evolve over the first hours, so the deteriorating child needs a repeat scan or an intracranial pressure monitor even if the first scan was reassuring. The fellow who treats the scan rather than the child misses the evolving lesion. [4]
Prognosis & Disposition
The prognosis of severe paediatric traumatic brain injury is sobering, with a mortality of 10 to 30 percent in modern series and a residual disability in the majority of survivors. The determinants of the outcome are the initial score and pupil response, the presence of hypotension or hypoxia, the type of lesion, and the course of the intracranial pressure. A common misconception is that children always do better than adults, and the evidence does not support it, because the very young child may do worse, in part because the developing brain is vulnerable and in part because the infant can harbour an expanding bleed through the open sutures. [6]
The disposition is to a paediatric intensive care unit for any child with a severe injury, an abnormal scan with a mass lesion, or the need for intracranial pressure control. The paediatric neurosurgery and neurology teams are involved early, and the retrieval service is engaged for the child who presents to a centre without paediatric intensive care. Every child with a moderate or severe injury is followed up in a structured neurorehabilitation programme, because the cognitive and behavioural sequelae often emerge over the months that follow and are the dominant determinants of the long-term quality of life. [4]
The rehabilitation plan is multidisciplinary and addresses the cognition, the behaviour, the school reintegration, the motor function, and the family support. The child is reviewed by physiotherapy, occupational therapy, speech and language therapy, psychology, and the paediatric neurology and neuropsychology services, and the school is engaged early because the return to learning is a central goal. The family is supported through the prognostic uncertainty, because the full extent of the recovery often takes a year or more to declare itself. [6]
Special Populations
The infant is the population in whom the open sutures change the natural history, and the one in whom non-accidental injury is the constant question. A subdural or subgaleal bleed can expand through the open sutures, so the infant may present in shock or with a rapid fall in the conscious state rather than the classic adult picture. The finding of a subdural bleed, retinal haemorrhages, or an inconsistent story activates the safeguarding pathway, and the workup includes the ophthalmology review, the skeletal survey, and the child protection team. The brain injury is managed on the standard ladder, and the safeguarding runs in parallel. [2]
The Aboriginal and Torres Strait Islander child and the child from a remote setting is the population in whom the access to care shapes the outcome. The longer time to treatment, the greater exposure to secondary insults in the prehospital phase, and the distance to a paediatric intensive care unit all conspire to worsen the course, which is why the retrieval service, the early intubation, and the prevention of hypoxia and hypotension in transit are central. The culturally appropriate communication and the engagement with the family are part of both the acute and the follow-up care. [4]
The child with a pre-existing neurodisability or a complex chronic condition tolerates the secondary insults poorly and needs an early and a cautious intensive care course. The baseline neurological state may already be abnormal, which complicates the scoring and the prognostication, and the family is involved early in the decisions about the goals of care. The adolescent is at risk from the road traffic crash, the sport, the alcohol, and the risk-taking behaviour, and the transition to the adult neurorehabilitation services is part of the long-term plan, because the cognitive and behavioural sequelae often extend into the adult years. [6]
The child from a refugee or migrant family is the population in whom the communication and the continuity are the challenges. The language barrier can hide the mechanism and the past history, an interpreter is engaged early, and the family is connected to the local neurology and rehabilitation services before discharge. The socioeconomic context matters, because the return to school and the access to therapy shape the long-term recovery as much as the acute care. [4]
Evidence, Guidelines & Regional Differences
The evidence base for the management of severe paediatric traumatic brain injury is anchored by the Brain Trauma Foundation Guidelines for the Management of Pediatric Severe Traumatic Brain Injury. Kochanek and colleagues reported the second edition in 2012, a comprehensive document that set out the thresholds and the doses for every step of the ladder, and the third edition executive summary in 2019 reaffirmed and updated the key recommendations. The guidelines give the intracranial pressure treatment threshold of 20 mmHg, the cerebral perfusion pressure floor of 40 mmHg, and the hyperosmolar doses that this topic reproduces, and they remain the single most testable source on the topic. [4][5]
Hutchison 2008
NEJM, hypothermia trial
- Prophylactic hypothermia versus normothermia in children
- No improvement in outcome with cooling
- Trend toward higher mortality with rewarming
- Prophylactic hypothermia is not recommended
DECRA 2011
NEJM, adults, craniectomy
- Early bifrontal decompressive craniectomy for refractory pressure
- Worse outcome in the craniectomy group
- Craniectomy reserved for the refractory case
- Adult trial, applied cautiously to children
Two landmark trials reshaped the refractory end of the ladder, and both showed that an aggressive intervention could do harm. The Hutchison trial, reported in the New England Journal of Medicine in 2008, randomised children with severe injury to prophylactic hypothermia or to normothermia, and it found that the cooling did not improve the outcome and raised a concern about harm, which is why normothermia is the target and hypothermia is not used as a treatment. The DECRA trial, reported by Cooper and colleagues in 2011, randomised adults with refractory intracranial hypertension to an early bifrontal decompressive craniectomy or to the standard care, and it found that the early operation was associated with worse outcomes, which is why the craniectomy is reserved for the genuinely refractory case rather than used early. [7][8]
The imaging evidence is anchored by the PECARN rule of Kuppermann and colleagues, a large prospective cohort study that identified the children at very low risk of a clinically important brain injury after a mild head strike, in whom a computed tomography can be safely deferred. The rule governs the mild case, while the moderate and severe child is scanned without it, but the rule is the most testable single piece of imaging evidence on the topic and is frequently examined alongside the severe pathway. The epidemiology and the prognostic evidence come from series such as that of Ducrocq and colleagues, which defined hypotension, hypoxia, and pupil abnormalities as the dominant early predictors of mortality. [3][6]
The regional differences are modest, because the Brain Trauma Foundation guidelines are adopted internationally. The Australian and New Zealand practice follows the guideline thresholds and doses, and the shared foundation is the prevention of secondary brain injury, the 20 mmHg intracranial pressure threshold, the 40 mmHg cerebral perfusion pressure floor, and the avoidance of prophylactic hypothermia and prophylactic hyperventilation. The controversies that remain are the optimal cerebral perfusion pressure target for the individual child, the role of the continuous hypertonic saline infusion, and the threshold for the decompressive craniectomy in the paediatric refractory case, each of which is still being refined. [5]
Exam Pearls
The severe TBI ladder to the pressure
References
- [1]Teasdale G, Jennett B Assessment of coma and impaired consciousness. A practical scale. Lancet, 1974.PMID 4136544
- [2]Kirkham FJ, Newton CR, Whitehouse W Paediatric coma scales. Dev Med Child Neurol, 2008.PMID 18312424
- [3]Kuppermann N, Holmes JF, Dayan PS, et al Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet, 2009.PMID 19758692
- [4]Kochanek PM, Carney N, Adelson PD, et al Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents--second edition. Pediatr Crit Care Med, 2012.PMID 22217782
- [5]Kochanek PM, Tasker RC, Carney N, et al Guidelines for the Management of Pediatric Severe Traumatic Brain Injury, Third Edition: Update of the Brain Trauma Foundation Guidelines, Executive Summary. Neurosurgery, 2019.PMID 30822776
- [6]Ducrocq SC, Meyer PG, Orliaguet GA, et al Epidemiology and early predictive factors of mortality and outcome in children with traumatic severe brain injury: experience of a French pediatric trauma center. Pediatr Crit Care Med, 2006.PMID 16885795
- [7]Hutchison JS, Ward RE, Lacroix J, et al Hypothermia therapy after traumatic brain injury in children. N Engl J Med, 2008.PMID 18525042
- [8]Cooper DJ, Rosenfeld JV, Murray L, et al Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med, 2011.PMID 21434843
- [9]Wu AG, Samadani U, Slusher TM, et al 23.4% Hypertonic Saline and Intracranial Pressure in Severe Traumatic Brain Injury Among Children: A 10-Year Retrospective Analysis. Pediatr Crit Care Med, 2019.PMID 30664588
- [10]Stulce C, Reisner A, Kane JM, et al Fluid Overload in Pediatric Severe Traumatic Brain Injury. Pediatr Crit Care Med, 2020.PMID 31568241