Paeds · neurology-neurodisability-and-neuromuscular
Neural tube defects and spinal dysraphism
Also known as Spina bifida · Myelomeningocele · Meningocele · Tethered cord syndrome · Occult spinal dysraphism · Lipomyelomeningocele
Fellowship guide to paediatric neural tube defects and spinal dysraphism. Covers the open and closed spectrum from anencephaly and myelomeningocele to spina bifida occulta and the occult dysraphic states, the periconceptional folic acid prophylaxis at 400 micrograms for the general population and 4 milligrams for the high-risk woman, the maternal serum alpha-fetoprotein and fetal ultrasound that make the prenatal diagnosis, the Chiari II malformation and the near-universal hydrocephalus of myelomeningocele, the Management of Myelomeningocele Study that established prenatal repair before 26 weeks, the cutaneous stigmata of occult dysraphism that prompt spinal imaging, the low-lying conus and the thickened filum of tethered cord syndrome, the clean intermittent catheterisation and anticholinergic management of the neurogenic bladder, and the latex-free environment that prevents sensitisation from birth.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Neural tube defects are the structural consequences of a failure of the neural tube to close during the third and fourth week of embryogenesis, and they span a spectrum from the lethal anencephaly at the cranial end to the occult dysraphic states that hide under the skin of the back. Copp and colleagues set out the modern understanding in their primer on spina bifida, framing the group as a disorder of primary neurulation whose severity tracks the level and the completeness of the failure of closure. The open defects, where neural tissue is exposed to the amniotic fluid, carry the heaviest burden, while the closed defects, where the skin covers the malformation, may declare only through the skin stigmata and the progressive neurological, urological, and orthopaedic deterioration of a tethered cord. [1]
Three facts make this topic central to the paediatric exam. The first is that most neural tube defects are preventable, and the periconceptional folic acid dose and the food fortification strategy are among the most testable facts in preventive paediatrics. The second is that the diagnosis is made prenatally for the open defects, by the maternal serum alpha-fetoprotein and the fetal ultrasound, and the prenatal counselling now includes the option of fetal surgery. The third is that the child with spina bifida carries a lifelong multidisciplinary burden across neurosurgery, urology, orthopaedics, and rehabilitation, and the fellow must hold the whole picture from the preventive dose to the adult transition. [2]
Classification
Neural tube defects have a working classification that divides by whether the lesion is open or closed and by its site along the neuraxis, and both axes matter for the clinical approach. The open defects expose neural tissue to the amniotic fluid, and they are the ones that leak alpha-fetoprotein into the maternal serum and declare on the prenatal ultrasound. The closed defects cover the malformation with skin, and they are the ones that hide under a skin stigma and present later with the tethered cord. [1]
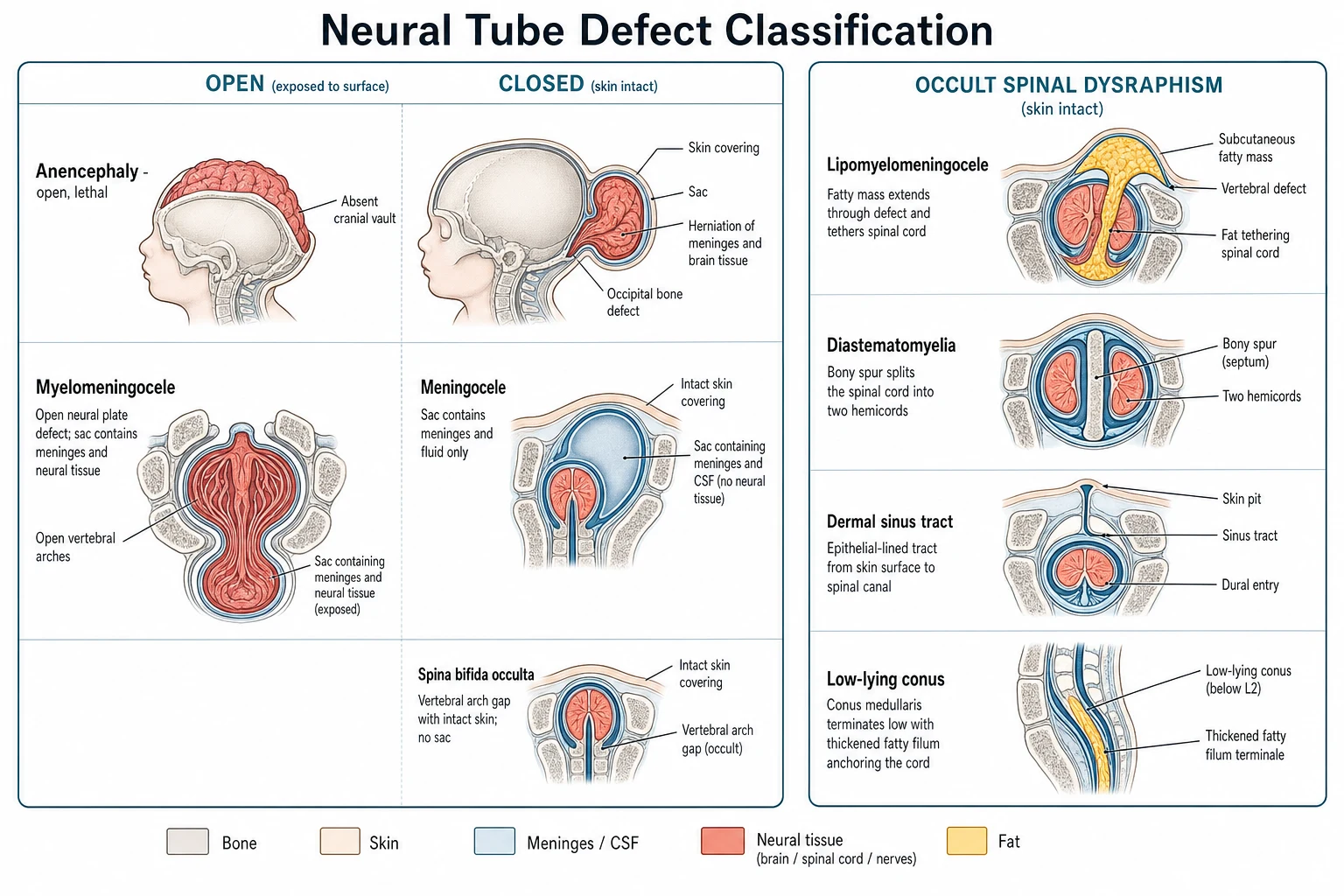
The open defects sit at the cranial and the spinal ends. Anencephaly is the failure of the anterior neuropore to close, the skull vault and the cerebral cortex do not form, and the condition is incompatible with life beyond the hours or days after birth. An encephalocele is a herniation of brain and meninges through a skull defect, most often in the occipital region, and its prognosis tracks the amount of herniated neural tissue. Myelomeningocele is the commonest and the most significant open spinal defect, where the neural placode is exposed on the back through a defect in the vertebrae and the skin, and the meninges and the neural tissue form a cystic sac in the midline of the lower back. A meningocele is a sac of meninges and cerebrospinal fluid protruding through the vertebral defect without neural tissue inside, and it carries a better neurological prognosis because the cord and the roots are spared. [1]
The closed defects are the occult spinal dysraphism group, where the skin covers the malformation and the cord is abnormal in its position, its structure, or its attachment. Spina bifida occulta is the mildest form, a failure of the posterior vertebral arch to fuse that is seen as a bony defect on the radiograph and that is usually an incidental finding in an asymptomatic child. The clinically significant occult dysraphic states are the lipomyelomeningocele, where a lipoma tethers the conus to the subcutaneous fat through a vertebral defect; the diastematomyelia, where a bony or fibrous spur splits the cord into two hemicords; the dermal sinus tract, where an epithelial track runs from the skin to the spinal canal and risks infection and tethering; and the tethered cord syndrome, where a thickened fatty filum or a low-lying conus anchors the cord and stretches it with growth. The value of this classification is that every occult dysraphic state is a candidate for surgical untethering, and the cutaneous stigmata are the sign that prompts the scan that finds it. [8]
The clinical distinction that matters most is not the label but whether the cord is open or tethered. An open myelomeningocele is the neonatal emergency, because the exposed neural tissue risks infection and further injury and the lesion needs closure within 24 to 72 hours. A tethered cord is the childhood and adolescence problem, because the cord is anchored and the growth of the spine stretches it, producing the progressive leg weakness, the foot deformity, the scoliosis, and the bladder and bowel deterioration that are the indications for untethering. The Chiari II malformation and the hydrocephalus belong almost exclusively to the myelomeningocele phenotype, which is why that subtype carries the heaviest multidisciplinary burden. [1]
Epidemiology & Risk Factors
The global prevalence of neural tube defects is about 1 to 2 per 1000 live births where food is not fortified, and mandatory folic acid fortification of flour has lowered that figure by between a quarter and a half wherever it has been introduced. Kancherla set out the global epidemiology in a recent review, framing neural tube defects as one of the most preventable congenital anomalies and one whose prevalence tracks the folate status of the population. The geographic and the ethnic variation is real, with higher rates in parts of Latin America, China, and among Celtic populations, and the lower rates in populations with mandatory fortification. [2]
The risk factors divide into the nutritional, the genetic, and the environmental. The dominant risk factor is a low maternal folate status in the periconceptional period, because the neural tube closes before most women know they are pregnant. A previous affected pregnancy carries a recurrence risk of 3 to 5 percent, which is ten times the background risk, and this is the group for whom the high-dose 4 milligram supplement is given. Maternal diabetes, maternal obesity, and the use of anticonvulsant drugs that interfere with folate metabolism, particularly valproate and carbamazepine, each raise the risk, and maternal hyperthermia in the early first trimester is a lesser contributor. The genetic contribution is polygenic with some syndromic overlap, and the recurrence risk after one affected child is the evidence that the tendency is inherited. [2]
The risk factors for a poor outcome in the child who already has a myelomeningocele are the level of the lesion and the presence of the Chiari II malformation. A higher lesion, above L2, predicts a worse motor outcome and a lower chance of community ambulation, while a lower lesion, at L3 to S1, predicts a better outcome. The Chiari II malformation is near-universal in myelomeningocele, and it drives the hydrocephalus that complicates 80 to 90 percent of cases and that makes the shunt a central feature of the child's life. [1]
Pathophysiology
To understand the neural tube defects, hold the normal closure of the neural tube in mind. The neural plate folds into a tube during the third and fourth week of embryogenesis, and the closure proceeds from multiple initiation sites along the neuraxis. The anterior neuropore closes at around day 24 and the posterior neuropore at around day 28, and a failure at any site leaves an open defect at that level. Anencephaly is the failure of the anterior closure, and myelomeningocele is the failure of the posterior closure at the lumbosacral region. The timing is critical, because the tube closes before the missed menstrual period, which is why folate must be taken before conception and not after the pregnancy is confirmed. [1]
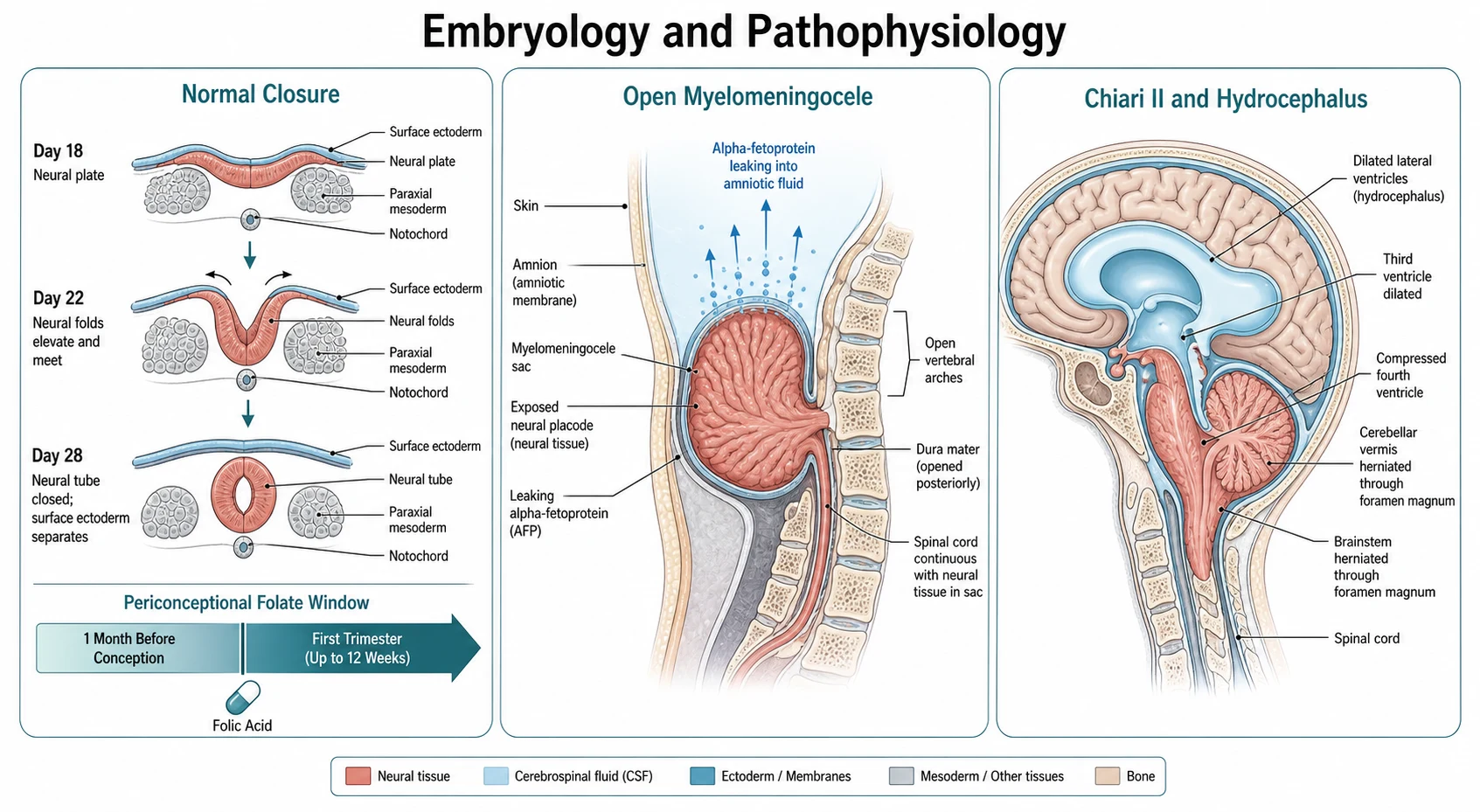
The mechanism of the open defect is a failure of the neural folds to elevate, meet, and fuse, and the exposed neural tissue suffers a two-hit injury. The first hit is the malformation itself, where the neural tube fails to form. The second hit is the mechanical and the chemical trauma to the exposed placode as it floats in the amniotic fluid through the remainder of the pregnancy, which is the rationale for the prenatal repair that removes the placode from the toxic amniotic environment and restores the cerebrospinal fluid cushion. The open defect leaks alpha-fetoprotein and acetylcholinesterase from the exposed neural tissue into the amniotic fluid and across the fetal skin into the maternal serum, which is the basis for the maternal serum screening that detects it. [6]
The mechanism of the Chiari II malformation is the loss of the cerebrospinal fluid pressure that normally inflates the developing brain. The open spinal defect allows the cerebrospinal fluid to leak out, the posterior fossa does not expand, and the cerebellar vermis and the brainstem are pushed downward through the foramen magnum as the brain collapses on itself. The herniated tissue obstructs the cerebrospinal fluid outflow and produces the hydrocephalus that complicates most cases of myelomeningocele, and the direct compression of the brainstem produces the stridor, the swallowing difficulty, the apnoea, and the arm weakness that are the life-threatening presentations of the Chiari II. Fons and Jnah set out the core concepts of the malformation. [7]
The mechanism of the tethered cord in the occult dysraphic states is the anchoring of the spinal cord to a structure that does not move with growth. In the lipomyelomeningocele, a lipoma tethers the conus to the subcutaneous fat. In the thickened fatty filum, a fat-infiltrated filum anchors the cord and does not allow the normal ascent of the conus from the L3 level at birth to the L1 to L2 level by three months. In the diastematomyelia, a bony spur splits the cord and restricts its movement. In every case the growth of the spine stretches the anchored cord, and the ischaemic and the mechanical injury to the lumbosacral cord produces the progressive leg weakness, the foot deformity, the scoliosis, and the bladder and bowel dysfunction that are the clinical signature of the tethered cord. [8]
Clinical Presentation
The presentation of a neural tube defect divides by whether it is open or closed and by whether it is found prenatally or after birth. The open defects are usually detected prenatally by the maternal serum alpha-fetoprotein and the fetal ultrasound, and the newborn with a myelomeningocele presents with a visible cystic lesion in the midline of the lower back. The closed defects declare after birth through the cutaneous stigmata over the spine and the progressive neurological, urological, and orthopaedic deterioration of the tethered cord, and some are found only on the spinal magnetic resonance imaging ordered for a skin stigma or a foot deformity. [1]
How neural tube defects present across the timeline
A prenatal maternal serum alpha-fetoprotein above two and a half multiples of the median at 15 to 20 weeks that raises an open defect until the fetal ultrasound resolves it
A fetal ultrasound at 18 to 20 weeks showing the open spinal defect, the lemon and banana signs of the Chiari II, and the ventriculomegaly of the hydrocephalus
A newborn with a visible cystic lesion in the midline of the lower back, the myelomeningocele, needing neurosurgical closure within 24 to 72 hours
An infant or child with a midline back skin stigma such as a hair tuft, a lipoma, a dermal sinus, or a deviated gluteal cleft that prompts the spinal magnetic resonance imaging
A child or adolescent with progressive leg weakness, foot deformity, scoliosis, or bladder and bowel dysfunction from a tethered cord that needs untethering
The newborn with a myelomeningocele has a cystic mass in the midline of the lower back, most often in the lumbosacral region, that may be covered by a thin membrane or that may leak cerebrospinal fluid. The motor and the sensory level is defined by examining the legs, because the lowest functioning muscle group predicts the ambulation potential, and the level usually corresponds to the vertebral level of the lesion. The head is measured for the macrocephaly of the hydrocephalus, and the baby is watched for the stridor, the swallowing difficulty, and the apnoea of the Chiari II. The hips are examined for the dislocation and the feet for the deformity that accompany the paralysis, and the anal tone and the perineal sensation are checked for the sacral involvement. [1]
The child with an occult dysraphic state presents through the cutaneous stigmata over the spine, and the skin signs are the single most important clue to the closed defect. The high-risk stigmata are the hypertrichosis or the localised hair tuft, the subcutaneous lipoma, the dermal sinus tract, the haemangioma or the capillary stain, the skin tag or the pseudotail, and the deviation or the duplication of the gluteal cleft. The lower-risk stigmata are the simple sacral dimple that is less than 5 millimetres across and within 2.5 centimetres of the anal verge, which rarely tracks to the spinal canal. The rule is that any atypical midline back skin stigma prompts a spinal ultrasound in the infant with an open posterior acoustic window or a spinal magnetic resonance imaging in the older child. [8]
The older child or the adolescent with a tethered cord presents with the progressive deterioration that comes from the stretching of the cord with growth. The neurological signs are the progressive leg weakness, the loss of the ankle jerks, the muscle atrophy, and the foot deformity, most often a cavus or a club foot. The urological signs are the new or the worsening incontinence, the recurrent urinary tract infections, and the incomplete bladder emptying that reflect the neurogenic bladder. The orthopaedic signs are the progressive scoliosis and the leg length discrepancy. The presentation may be acute, after a growth spurt or a flexion injury, or it may be insidious over months or years, and the spinal magnetic resonance imaging that shows the low-lying conus and the thickened filum is the test that confirms it. [8]
Differential Diagnosis
The differential of a newborn with a midline back lesion is the heart of the exam question, because the management and the prognosis turn on whether the lesion is open or closed and on what is inside the sac. The task is to separate the myelomeningocele from the meningocele and the occult dysraphic states, and the discriminator is the combination of the clinical appearance of the lesion, the motor and the sensory level in the legs, and the spinal imaging. [1]
Myelomeningocele
open, neurosurgical emergency
- Open spinal lesion with the neural placode exposed in the cystic sac
- Motor and sensory level in the legs that corresponds to the lesion
- Near-universal Chiari II malformation and hydrocephalus
- Closure within 24 to 72 hours and a lifelong multidisciplinary burden
Meningocele
closed, better prognosis
- Sac of meninges and cerebrospinal fluid without neural tissue inside
- Skin may cover the sac or it may be open
- The cord and the roots are spared and the neurological exam is usually normal
- Surgical repair with a better neurological and urological outcome
Lipomyelomeningocele
closed, tethers the cord
- Skin-covered lesion with a lipoma that tethers the conus to the subcutaneous fat
- Normal at birth then progressive leg weakness and bladder dysfunction
- Cutaneous stigma of a subcutaneous lipoma over the lower back
- Surgical untethering to prevent or arrest the deterioration
Occult dysraphism (tethered cord)
closed, skin stigmata
- Skin-covered back with a hair tuft, a dermal sinus, or a deviated gluteal cleft
- Low-lying conus below L2 and a filum thicker than 2 millimetres on the magnetic resonance imaging
- Progressive leg weakness, foot deformity, scoliosis, and neurogenic bladder
- Untethering by filum section or cord release
The first distinction is between the open and the closed lesion. A myelomeningocele has an open defect with the neural placode visible in the sac, while a meningocele and the occult dysraphic states have the skin intact. The second distinction is between a sac that contains neural tissue and one that does not, because the meningocele carries a far better prognosis. The myelomeningocele has a motor and a sensory level in the legs, while the meningocele usually has a normal neurological exam. The third distinction is between the open lesion and the occult dysraphism, because the occult lesion is skin-covered and it declares through the skin stigmata and the tethered cord rather than through the neonatal sac. [1]
The second differential is the cause of the cutaneous stigmata, because not every midline back skin mark is a dysraphism. The simple sacral dimple that is small and close to the anus is a common and a benign finding that rarely tracks to the spinal canal. The deviated gluteal cleft, the hair tuft, the lipoma, the dermal sinus, and the haemangioma are the high-risk stigmata that demand imaging, and the rule is that the imaging is the spinal ultrasound in the young infant and the magnetic resonance imaging in the older child. The dermal sinus tract that opens onto the skin is a particular concern, because it is a route for the bacterial entry that produces the recurrent meningitis and the intraspinal abscess, and it demands imaging and the neurosurgical excision. [8]
The third differential is the cause of the progressive leg weakness and the neurogenic bladder in the older child, which includes the tethered cord, the spinal cord tumour, the transverse myelitis, and the hereditary neuropathy. The tethered cord is the one with the skin stigmata and the low-lying conus, and the magnetic resonance imaging distinguishes it from the tumour and the inflammation. The hereditary neuropathies, such as the Charcot-Marie-Tooth disease, produce a slowly progressive distal weakness and the foot deformity, and they are distinguished by the nerve conduction studies and the family history. [8]
Clinical & Bedside Assessment
The bedside assessment of a newborn with a myelomeningocele is a structured emergency that runs in parallel with the call to neurosurgery. The baby is handled in a latex-free environment from the first contact, because the latex sensitisation that complicates spina bifida begins with the early exposure. The lesion is inspected and covered with a sterile saline-soaked dressing to prevent drying and infection, and the baby is placed prone or in the lateral position to keep the pressure off the sac. The call to the neonatal and the neurosurgical teams is made at the outset, because the definitive treatment is the closure within 24 to 72 hours. [1]
The motor and the sensory level is the central bedside finding, because it predicts the ambulation potential and it maps the severity of the lesion. The motor level is the lowest spinal level with an intact muscle function, and it is tested by the systematic examination of each leg muscle group, from the hip flexors for L2 to the knee extensors for L3 to L4, the ankle dorsiflexors for L4 to L5, and the plantar flexors for S1 to S2. A lesion at or below L3 to S1 predicts a reasonable chance of community ambulation, while a lesion above L2 predicts a worse motor outcome and a dependence on the wheelchair. The sensory level is mapped by the pinprick and the light touch, and the sacral sensation and the anal tone are tested for the bowel and the bladder involvement. [1]
The head and the brainstem are examined next. The head circumference is measured and plotted, because the macrocephaly and the full fontanelle point to the hydrocephalus that complicates 80 to 90 percent of myelomeningoceles. The baby is watched for the stridor, the swallowing difficulty, the weak cry, and the apnoea of the Chiari II malformation, which are the signs of the brainstem compression that is the life-threatening presentation of the malformation. The hips are examined for the dislocation and the feet for the deformity that accompany the paralysis, and the spine is examined for the scoliosis and the kyphosis that may accompany the lesion. [7]
The bedside assessment of the child with an occult dysraphic state is the examination of the back skin and the neurological system. The midline back skin is inspected for the high-risk stigmata, which are the hair tuft, the lipoma, the dermal sinus, the haemangioma, the skin tag, and the deviated gluteal cleft. The legs are examined for the muscle weakness, the muscle atrophy, the reflex changes, and the foot deformity, and the gait is observed in the walking child. The bladder and the bowel function are assessed for the incontinence, the recurrent infections, and the constipation that reflect the neurogenic involvement, and the back is examined for the scoliosis and the spinal tenderness. [8]
Investigations
The investigation of the open defect begins prenatally and ends with the postnatal imaging of the brain and the spine. The maternal serum alpha-fetoprotein is the screening test, offered at 15 to 20 weeks, and a value above two and a half multiples of the median raises an open defect. The fetal ultrasound, performed at 18 to 20 weeks, confirms the spinal defect and looks for the cranial signs of the Chiari II malformation, which are the lemon sign of the bifrontal scalloping and the banana sign of the cerebellar compression, and the ventriculomegaly of the hydrocephalus. The amniocentesis, with the alpha-fetoprotein and the acetylcholinesterase in the amniotic fluid, is offered when the screening and the ultrasound are equivocal or when the family wants the karyotype. [2]
The postnatal imaging of the newborn with a myelomeningocele includes the cranial and the spinal studies that map the lesion and its complications. The cranial ultrasound or the magnetic resonance imaging of the brain shows the hydrocephalus and the Chiari II malformation, with the downward herniation of the cerebellar vermis and the brainstem through the foramen magnum. The spinal magnetic resonance imaging maps the level and the extent of the lesion, and it looks for the diastematomyelia, the lipoma, and the dermal sinus that may accompany it. The renal ultrasound and the urodynamic studies assess the neurogenic bladder, because the upper tract dilation and the bladder compliance predict the risk to the kidneys, and the baseline studies guide the clean intermittent catheterisation. [1]
The investigation of the occult dysraphic state is the spinal ultrasound in the young infant and the spinal magnetic resonance imaging in the older child. The spinal ultrasound is useful in the first three to six months while the posterior vertebral arches are not yet ossified, and it shows the position of the conus, the thickness of the filum, and any lipoma or sinus tract. The spinal magnetic resonance imaging is the definitive test, and it is the one ordered for the older infant and the child, and it shows the low-lying conus below L2, the thickened filum above 2 millimetres, the fatty filum, the lipomyelomeningocele, the diastematomyelia with its bony spur, and the dermal sinus tract. Klinge and colleagues set out the clinical criteria for the filum terminale resection in the occult tethered cord syndrome, anchoring the diagnosis in the imaging and the clinical deterioration. [8]
Management — Resuscitation
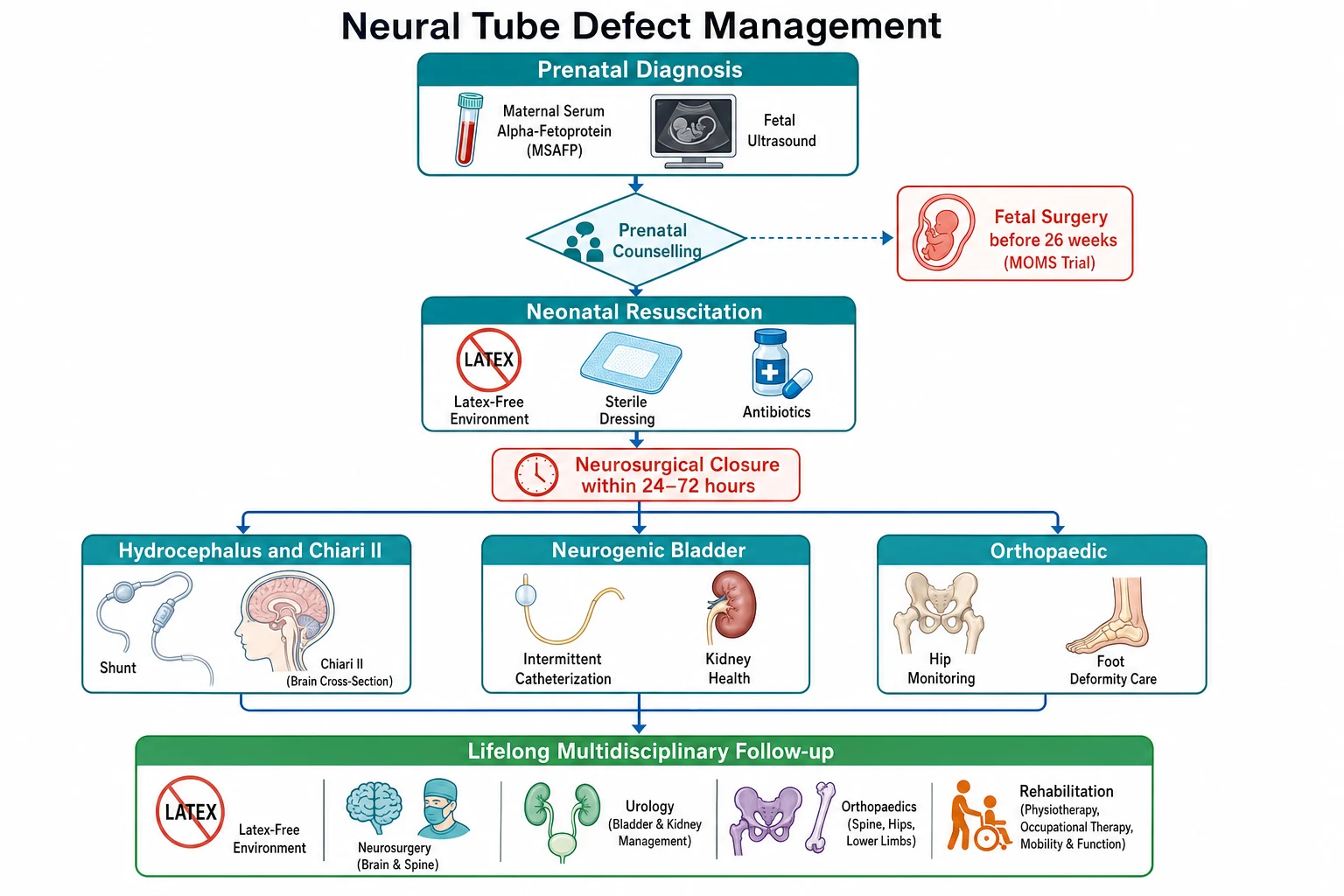
The resuscitation of the newborn with a myelomeningocele is the protection of the exposed neural tissue and the prevention of the infection while the neurosurgical closure is arranged. The baby is handled in a latex-free environment from birth, and the lesion is covered with a sterile saline-soaked dressing that is changed regularly to keep the placode moist and clean. The baby is placed prone or lateral to keep the pressure off the sac, and the broad-spectrum antibiotics that cover the skin flora, such as a first-generation cephalosporin, are started while awaiting the closure. The call to the neurosurgical team is made at the outset, because the closure within 24 to 72 hours prevents the infection and preserves the remaining neurological function. [1]
The airway and the breathing are assessed, because the Chiari II malformation may compress the brainstem and produce the stridor, the apnoea, and the respiratory distress that need the airway support. The baby with the brainstem compression is a neurosurgical emergency, and the decompression of the posterior fossa may be needed alongside the lesion closure and the shunt. The circulation is assessed and the intravenous access is secured, and the bedside glucose is checked, because the baby of the diabetic mother carries the additional risk of the hypoglycaemia. The head circumference is monitored for the rapid enlargement of the hydrocephalus, and the shunt is placed when the ventriculomegaly progresses, either at the time of the lesion closure or soon after. [7]
The latex-free environment is the resuscitation principle that prevents the sensitisation that complicates the life of the child with spina bifida. Every catheter, every glove, every dressing, and every piece of equipment from the first contact is latex-free, and the latex-free status is documented and flagged at every admission. The latex allergy that develops from the early and the repeated exposure can cause the anaphylaxis under anaesthesia, and the latex avoidance from birth prevents the sensitisation. Meneses and colleagues set out the latex allergy guidelines for the people with spina bifida. [10]
Management — Definitive & Stepwise
The definitive management of the myelomeningocele is the neurosurgical closure, the management of the hydrocephalus and the Chiari II, the urological protection of the kidneys, and the lifelong multidisciplinary follow-up. The closure of the lesion is performed within 24 to 72 hours of birth, and the surgeon frees the neural placode from the surrounding tissue, reconstructs the neural tube, closes the meninges, and brings the muscle and the skin over the defect. The timing matters, because the early closure prevents the infection and preserves the remaining neurological function. [1]
[1]The hydrocephalus is managed with the ventriculoperitoneal shunt or the endoscopic third ventriculostomy, and the shunt is placed when the ventriculomegaly progresses, either at the time of the lesion closure or soon after. The Chiari II malformation is managed expectantly when it is asymptomatic, and the posterior fossa decompression is reserved for the symptomatic baby with the stridor, the swallowing difficulty, the apnoea, or the arm weakness, because the decompression relieves the brainstem compression. The shunt malfunction must be excluded before the Chiari II symptoms are attributed to the malformation, because a shunt that does not drain can produce the same brainstem signs through the rising intracranial pressure. [7]
Periconceptional folic acid for the prevention of neural tube defects
Dose
400 to 800 micrograms daily for all women of reproductive age, and 4 milligrams daily for the high-risk woman with a previous affected pregnancy or diabetes
The Management of Myelomeningocele Study, reported by Adzick and colleagues, established the fetal surgery option. The randomised trial compared the prenatal repair before 26 weeks with the standard postnatal repair, and it showed that the prenatal repair reduced the need for the ventriculoperitoneal shunt from 82 percent to 40 percent, improved the composite score for the mental development and the motor function at 30 months, and doubled the chance of walking without orthoses from 21 percent to 42 percent. The benefits came with the risks of the preterm birth, with the mean gestational age at birth of 34 weeks against 37 weeks, and the uterine dehiscence, which is why the fetal surgery is offered only at the specialist centres and only to the selected families. [6]
The stepwise pathway for the newborn with a myelomeningocele
Use the latex-free environment from the first contact and cover the lesion with a sterile saline-soaked dressing
Call the neurosurgical team and arrange the closure within 24 to 72 hours
Image the brain for the hydrocephalus and the Chiari II and place the shunt when the ventriculomegaly progresses
Assess the neurogenic bladder with the renal ultrasound and the urodynamics and start the clean intermittent catheterisation
Manage the orthopaedic burden of the hip dislocation, the foot deformity, and the scoliosis
Start the lifelong multidisciplinary follow-up across neurosurgery, urology, orthopaedics, and rehabilitation in a latex-free environment
The neurogenic bladder is managed to protect the kidneys and to achieve the continence, and the EAU and ESPU guidelines, reported by Stein and colleagues, set out the standard. The clean intermittent catheterisation is the foundation, started early to ensure the complete bladder emptying and the low storage pressure, and the anticholinergic drugs, such as the oxybutynin, are added to relax the detrusor and to increase the bladder capacity. The upper tracts are monitored with the renal ultrasound and the urodynamic studies, because the high storage pressure and the vesicoureteric reflux threaten the kidneys, and the bladder management is intensified when the upper tract dilation appears. The continence surgery, the botox injections, and the augmentation are the later options for the child who fails the conservative management. [9]
Specific Subtypes & Scenarios
Myelomeningocele is the commonest and the most significant open neural tube defect, and it is the subtype that carries the heaviest multidisciplinary burden. The lesion sits in the lumbosacral region, the motor and the sensory level in the legs defines the ambulation potential, and the near-universal Chiari II malformation and the hydrocephalus complicate 80 to 90 percent of the cases. The management is the neonatal closure, the shunt for the hydrocephalus, the clean intermittent catheterisation for the neurogenic bladder, the orthopaedic management of the hips and the feet, and the lifelong follow-up in a latex-free environment. [1]
Anencephaly is the failure of the anterior neuropore, and it is the open cranial defect that is incompatible with life. The skull vault and the cerebral cortex do not form, and the exposed neural tissue is covered by a thin membrane. The condition is detected on the prenatal ultrasound and the alpha-fetoprotein, and the counselling is the confirmation that the baby will not survive beyond the hours or the days after birth. The management is the supportive care and the compassionate counselling, and the option of the organ donation is discussed with the families who wish it. [2]
The lipomyelomeningocele is the occult dysraphic state where a lipoma tethers the conus to the subcutaneous fat through a vertebral defect, and it is the subtype that is skin-covered and that declares through the progressive deterioration. The child may be normal at birth, and the lipoma is felt as a subcutaneous mass over the lower back, and the cord is tethered. The presentation is the progressive leg weakness, the foot deformity, the bladder and the bowel dysfunction, and the spinal magnetic resonance imaging confirms the low-lying conus and the lipoma. The management is the surgical untethering, which frees the cord from the lipoma and prevents the further deterioration. [8]
The diastematomyelia, or the split cord malformation, is the subtype where a bony or a fibrous spur splits the cord into two hemicords, and it is the subtype that presents with the cutaneous stigmata and the progressive asymmetry. The skin over the lesion often shows a hair tuft, and the legs show the progressive weakness and the reflex asymmetry, and the magnetic resonance imaging shows the two hemicords and the spur. The management is the surgical removal of the spur and the release of the cord, which prevents the further stretching and the deterioration. The dermal sinus tract is the subtype where an epithelial track runs from the skin to the spinal canal, and it is the subtype that risks the recurrent meningitis and the intraspinal abscess. The management is the imaging and the neurosurgical excision of the whole tract. [8]
The tethered cord syndrome is the clinical consequence of any occult dysraphic state, and it is the scenario that brings the older child and the adolescent to the clinic. The cord is anchored, the growth of the spine stretches it, and the ischaemic and the mechanical injury produces the progressive leg weakness, the foot deformity, the scoliosis, and the bladder and the bowel dysfunction. The magnetic resonance imaging shows the low-lying conus below L2 and the thickened filum above 2 millimetres, and the management is the untethering, which sections the filum or releases the lipoma and frees the cord. The untethering is performed when the diagnosis is made, because the deterioration that has occurred may not reverse, and the goal is to prevent the further loss. [8]
Complications & Pitfalls
The feared complications of the myelomeningocele are the shunt malfunction, the Chiari II brainstem compression, the renal failure from the neurogenic bladder, and the latex anaphylaxis. The shunt malfunction is the commonest shunt emergency in this group, and a child with a myelomeningocele and a shunt who presents with the headache, the vomiting, or the drowsiness has a shunt malfunction until proven otherwise. The Chiari II brainstem compression presents with the stridor, the swallowing difficulty, the apnoea, and the arm weakness, and it is the life-threatening presentation of the malformation that needs the urgent posterior fossa decompression once the shunt malfunction is excluded. [7]
The renal failure from the neurogenic bladder is the long-term complication that shortens the life, and it is the one that the clean intermittent catheterisation and the anticholinergics are designed to prevent. The high storage pressure and the vesicoureteric reflux damage the kidneys, and the upper tract dilation on the renal ultrasound is the sign that the bladder management needs the intensification. The latex anaphylaxis is the intraoperative complication that can kill, and the latex-free environment from birth prevents the sensitisation that produces it. The shunt infection and the repeated revisions scar the abdomen and the ventricle and make each successive operation harder, and the lifetime burden shapes the development and the schooling. [9]
The classic pitfalls are the prenatal, the diagnostic, and the preventive. The first prenatal pitfall is to miss the folate window, because the tube closes before the missed period and the supplement started after the positive test is too late. The second is to attribute the Chiari II symptoms to the malformation without excluding the shunt malfunction, because a shunt that does not drain produces the same brainstem signs through the rising pressure, and the shunt series and the head scan must come first. The third is to assume that a skin-covered back with a hair tuft or a lipoma is a cosmetic finding, because the cutaneous stigmata mark the occult dysraphism that needs the imaging and the untethering, and the child sent home without the scan returns later with the irreversible deterioration. [8]
A subtler pitfall is to under-treat the neurogenic bladder. The child with the myelomeningocele and the neurogenic bladder needs the clean intermittent catheterisation started early, because the high storage pressure damages the kidneys before the symptoms appear, and the upper tract dilation on the renal ultrasound is a late sign. The bladder management is driven by the urodynamics and the renal ultrasound, not by the symptoms, and the catheterisation and the anticholinergics are started before the kidneys are harmed. The continence is a later goal, and the renal protection is the earlier and the more important one. [9]
Prognosis & Disposition
The prognosis of the neural tube defect divides by the subtype and by the level of the lesion, and it is the open and the closed distinction that frames the outlook. Anencephaly is incompatible with life, and the prognosis is the survival of hours or days. The myelomeningocele carries a heavy but a treatable burden, and the prognosis for the survival is good with the modern management, with most children surviving into adulthood. The prognosis for the ambulation tracks the motor level, so a lesion at or below L3 predicts a reasonable chance of the community ambulation while a lesion above L2 predicts a dependence on the wheelchair. The prognosis for the continence tracks the urological management, and the clean intermittent catheterisation achieves the social continence in most children. [1]
The cognitive outcome is shaped by the shunt complications, the Chiari II, and any additional malformations, and most children with the myelomeningocele have an intelligence in the normal range, though the learning and the behavioural difficulties are common, and the shunt infection and the repeated revisions take a cognitive toll. The transition to the adult care is the challenge of the adolescence, because the shunt and the bladder and the skin do not stop needing the attention, and the young adult with the spina bifida needs the structured handover to the adult neurosurgical and the urological services. The life expectancy is reduced in the group with the severe shunt complications and the renal failure, and the modern management has improved it towards the near-normal for the well-managed child. [1]
Disposition after the neonatal closure is to the neonatal or the paediatric intensive care unit depending on the course, and the child is discharged with the multidisciplinary plan and the clear safety-net. The safety-net names the shunt malfunction and the Chiari II signs that demand the immediate return, which are the headache, the vomiting, the drowsiness, the stridor, and the change in the eyes or the conscious level. The family is taught the clean intermittent catheterisation, the latex-free status is documented and flagged, and the school and the carers receive the same plan. The follow-up is lifelong and multidisciplinary, and the transition to the adult care begins in the adolescence. [9]
Special Populations
The woman with a previous affected pregnancy is the population for whom the high-dose folate is prescribed, because the recurrence risk of 3 to 5 percent is ten times the background risk. The 4 milligram folic acid supplement is started at least one month before the conception and continued through the first trimester, and it is taken separately from the routine multivitamin to avoid the excess of the other vitamins. The prenatal counselling includes the maternal serum alpha-fetoprotein, the detailed fetal ultrasound, and the option of the amniocentesis, and the family is seen by the fetal medicine and the paediatric neurosurgery teams before the delivery. [3][5]
The woman with the diabetes or the anticonvulsant drugs is the population with the additional risk, because the diabetes and the folate antagonist drugs, particularly the valproate and the carbamazepine, each raise the neural tube defect risk. The woman with the diabetes needs the tight glycaemic control before and through the pregnancy, because the hyperglycaemia is teratogenic beyond the neural tube. The woman on the valproate or the carbamazepine needs the review of the medication and the high-dose folate, and the discussion of the alternative anticonvulsant where the epilepsy allows it. [2]
The child with the neurodisability or the technology dependence is the population whose shunt and bladder and skin need the lifelong attention, and the carer's observation of the irritability, the vomiting, or the change in the seizure pattern becomes the red flag for the shunt malfunction. The family knows the child's baseline better than any clinician, and the parental report that something is wrong is taken seriously and worked up. The latex-free status is documented at every admission, and the airway and the swallowing are watched for the Chiari II signs. [10]
The population without the food fortification is the group at the highest population risk, and the mandatory fortification of the flour with the folic acid is the public health measure that lowers the prevalence by a quarter to a half. The woman from the remote or the disadvantaged setting may not take the supplement and may not have the fortified food, and the culturally appropriate education and the engagement with the family and the community are part of the prevention. The woman from the migrant or the refugee family is connected to the interpreter and the local service, and the folate advice is given in the language and the format she understands. [2]
Evidence, Guidelines & Regional Differences
The modern evidence base for the prevention rests on the two landmark trials and the reaffirmation guideline. The Medical Research Council Vitamin Study, reported in 1991, showed that the 4 milligram folic acid supplement reduced the recurrence of the neural tube defects by about 72 percent in the women with a previous affected pregnancy, and it established the high-dose supplement for the high-risk group. The trial of Czeizel and Dudas, reported in 1992, showed that the periconceptional multivitamin with 0.8 milligrams of folic acid reduced the first occurrence of the neural tube defects, and it established the supplement for the general population. The United States Preventive Services Task Force reaffirmed the grade A recommendation in 2023 that all women planning a pregnancy take 400 to 800 micrograms daily. [3][4][5]
MRC Vitamin Study 1991
recurrence prevention
- 4 milligram folic acid supplement for the woman with a previous affected pregnancy
- Reduced the recurrence by about 72 percent
- Established the high-dose supplement for the high-risk group
- The foundation of the periconceptional prevention
Czeizel and Dudas 1992
first occurrence prevention
- Periconceptional multivitamin with 0.8 milligrams of folic acid
- Reduced the first occurrence of the neural tube defects
- Established the supplement for the general population
- Complemented the recurrence evidence with the primary prevention
MOMS Trial 2011
fetal surgery
- Randomised trial of the prenatal repair before 26 weeks
- Reduced the shunt need from 82 percent to 40 percent
- Improved the motor function and the ambulation
- Risk of the preterm birth and the uterine dehiscence
The evidence for the fetal surgery rests on the Management of Myelomeningocele Study, reported by Adzick and colleagues in 2011, and it changed the practice for the selected families. The trial showed that the prenatal repair before 26 weeks reduced the need for the shunt, improved the motor function, and doubled the chance of the independent walking, and the benefits came with the risks of the preterm birth and the uterine dehiscence. The fetal surgery is now offered at the specialist centres and only to the selected families, and the counselling is the honest presentation of the benefits and the risks. [6]
The urological evidence rests on the EAU and ESPU guidelines, reported by Stein and colleagues, which standardised the neurogenic bladder management. The clean intermittent catheterisation, the anticholinergics, the urodynamic studies, and the upper tract surveillance are the foundation, and the continence surgery, the botox, and the augmentation are the later options. The latex allergy evidence rests on the guidelines of Meneses and colleagues, which established the latex-free environment from birth as the standard of care for the child with the spina bifida. [9][10]
Regional practice differs in three areas. The mandatory fortification of the flour with the folic acid is the law in the United States, Canada, Australia, and New Zealand and many other countries, but it is not universal, and the regions without it carry the higher prevalence. The fetal surgery is offered only at the specialist centres, and the access varies by the region and the health system. The routine use of the spinal ultrasound in the young infant with the cutaneous stigmata, as a radiation-free alternative to the magnetic resonance imaging, varies by the centre, though the magnetic resonance imaging remains the definitive test. The shared foundation is the periconceptional folate, the prenatal screening, the neonatal closure, the neurogenic bladder management, and the lifelong multidisciplinary follow-up, which no region disputes. [2]
Exam Pearls
The cutaneous stigmata of occult spinal dysraphism
References
- [1]Copp AJ, Adzick NS, Chitty LS, et al Spina bifida. Nat Rev Dis Primers, 2015.PMID 27189655
- [2]Kancherla V Neural tube defects: a review of global prevalence, causes, and primary prevention. Childs Nerv Syst, 2023.PMID 36882610
- [3]MRC Vitamin Study Research Group Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet, 1991.PMID 1677062
- [4]Czeizel AE, Dudas I Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N Engl J Med, 1992.PMID 1307234
- [5]US Preventive Services Task Force, Barry MJ, Nicholson WK, et al Folic Acid Supplementation to Prevent Neural Tube Defects: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA, 2023.PMID 37526713
- [6]Adzick NS, Thom EA, Spong CY, et al A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med, 2011.PMID 21306277
- [7]Fons K, Jnah AJ Arnold-Chiari Malformation: Core Concepts. Neonatal Netw, 2021.PMID 34518383
- [8]Klinge PM, Leary OP, Allen PA, et al Clinical criteria for filum terminale resection in occult tethered cord syndrome. J Neurosurg Spine, 2024.PMID 38489815
- [9]Stein R, Bogaert G, Dogan HS, et al EAU/ESPU guidelines on the management of neurogenic bladder in children and adolescent part I diagnostics and conservative treatment. Neurourol Urodyn, 2020.PMID 31724222
- [10]Meneses V, Parenti S, Burns H, et al Latex allergy guidelines for people with spina bifida. J Pediatr Rehabil Med, 2020.PMID 33285646