Paeds · neurology-neurodisability-and-neuromuscular
Neurological examination across childhood
Also known as Paediatric neurology examination · Infant neurological assessment · Hammersmith Infant Neurological Examination · General Movements Assessment · Floppy infant examination · Paediatric tone and reflex assessment
A fellowship approach to the neurological examination from the newborn to the adolescent: hold a single constant framework — mental state, cranial nerves, motor, sensory, cerebellar and gait, and development — while adapting the technique to age and cooperation; read tone, reflexes, posture and movement through the lens of corticospinal maturation; use the Hammersmith Infant Neurological Examination and General Movements Assessment to detect cerebral palsy early; and separate the benign and transient from the red-flag findings that demand urgent imaging.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The mark goes to the candidate who treats the examination as a developmental act, not a checklist applied once. The newborn brain is unfinished, and its examination reflects that: tone is flexor-biased, reflexes are mediated lower in the neuraxis, and signs we would call upper motor neuron in an adult are normal. Over the first two years the corticospinal tracts myelinate, voluntary control replaces reflex-driven movement, and the examination migrates toward the adult pattern. Reading a finding without this developmental lens is the commonest error in paediatric neurology — it labels the normal as abnormal, and far worse, can reassure when a finding has appeared that should alarm. [1] [2]
Overview & Definition
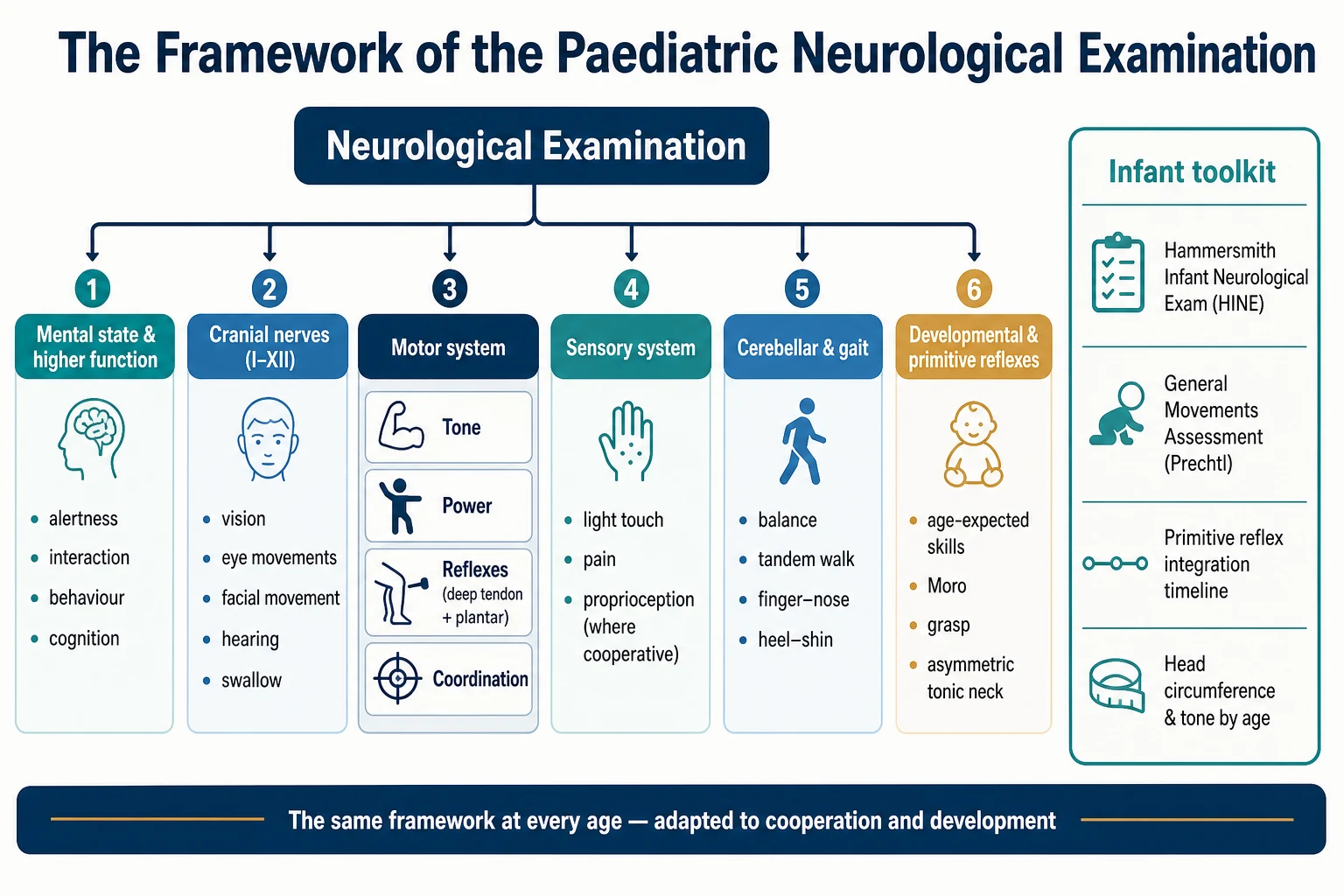
The paediatric neurological examination is a structured bedside assessment of a child's nervous system, performed to detect abnormality, to localise it within the neuraxis, and to track it over time. It is built on the same six-part framework used in adult neurology — mental state and higher function, the cranial nerves, the motor system, the sensory system, cerebellar and gait function, and development — but it is performed differently at every age, because the child's cooperation, their motor repertoire, and the maturity of their central nervous system all change month by month. [1]
What makes the paediatric examination distinctive is that the normal is a moving target. A term newborn lies flexed and tight, the hands clenched, the knees flexed, a brisk Moro snapping the arms open. Six months later that same child lies loose and open, reaches and rolls, and the primitive reflexes that dominated the newborn have integrated away. Two years on, the child walks and talks, and an upgoing plantar response — utterly normal in infancy — would now signal an upper motor neuron lesion. The clinician who can hold two questions at once — is this finding abnormal? and is it abnormal for this age? — has mastered the heart of the discipline. [2] [3]
The examination is also the single most reliable developmental surveillance tool in paediatrics, performed at every routine contact from the newborn check onward. Cerebral palsy affects roughly two per thousand live births, and the neurological examination — combined with the standardised infant tools — is how it is detected early enough for intervention to change the developing brain. A small, silent minority of findings are red flags: the head crossing centiles, the loss of a skill, the asymmetry that signals a focal lesion. The examination exists to catch these, and to distinguish them from the large benign majority. [8] [9]
Classification
The classification that earns marks is the classification of tone, because tone is the finding most often misread and the one that points most directly to a diagnosis. The Task Force on Childhood Motor Disorders defined hypertonia as abnormally increased resistance to externally imposed movement about a joint, and divided it into three patterns by the behaviour of that resistance during examination. Spasticity is velocity-dependent — the resistance increases the faster you stretch the muscle, producing the characteristic catch. Dystonia is a movement or posture produced by involuntary co-contraction of agonist and antagonist muscles, often triggered by attempted movement or emotion. Rigidity is resistance that is continuous throughout the range and independent of both velocity and movement. [6]
The opposite finding — hypotonia — is low resistance to passive movement, and it carries its own classification by where the problem lies. A central cause (brain) produces a floppy child who is also socially unengaged or delayed, often with the other stigmata of cerebral involvement. A peripheral cause (anterior horn cell, peripheral nerve, neuromuscular junction, or muscle) produces a floppy child whose weakness is proportional, whose reflexes are reduced or absent, and whose brain — when you can test it — is intact. The distribution and the reflex pattern separate these at the bedside long before the creatine kinase and the genetic panel arrive. [10] [12]
Epidemiology & Risk Factors
The examination is performed on every child, but its yield is concentrated in a high-risk minority. Roughly two in every thousand live births will develop cerebral palsy, and the rate is far higher — closer to one in ten — among very preterm and extremely low-birthweight infants. Global developmental delay is found in one to three per cent of children, and the neurological examination is the first and cheapest screen for both. The prevalence of these conditions is why the examination is built into every well-child contact, not reserved for the symptomatic. [8] [9]
The strongest risk factors for an abnormal neurological examination are the company the child keeps. Prematurity and very low birthweight, neonatal encephalopathy and therapeutic hypothermia, a complicated neonatal intensive care course, intrauterine growth restriction, congenital brain malformations, chromosomal syndromes, and a family history of neurodegenerative or neuromuscular disease all raise the yield and lower the threshold for a formal standardised assessment. In the older child, new-onset abnormality after a febrile illness, trauma, or a period of regression changes the picture entirely and points toward an acquired or progressive process. [4] [11]
Equity matters here as much as anywhere in paediatrics. In remote and Indigenous communities, and in migrant and refugee families, the gap between the appearance of an abnormal finding and access to a specialist assessment can stretch into years, and the developing brain does not wait. A low threshold to perform and document a careful examination, to use the standardised infant tools, and to refer early is the equity response that closes that gap. [9]
Pathophysiology
The reason the examination changes with age is that the central nervous system changes with age, and the most important driver is the maturation of the corticospinal tract. At birth, the corticospinal tracts that carry voluntary motor commands from the cortex to the spinal cord are incompletely myelinated. The lower, reflex-mediated pathways therefore dominate the newborn's motor behaviour — the Moro, the grasp, the stepping — and the clinical signs of an upper motor neuron lesion, which depend on an intact mature corticospinal tract, are not yet meaningful. [2] [3]
Over the first two years, myelination proceeds caudally from the cortex, voluntary motor control takes over from reflex-driven movement, and the primitive reflexes are gradually inhibited by the maturing cortex. This is why the plantar response — the Babinski — is extensor (upgoing) in the normal infant and becomes flexor (downgoing) as the corticospinal tract matures, usually by twelve to twenty-four months. An extensor plantar is not a sign in an infant; it is the absence of a sign, because the inhibitory pathway that would flex the toe has not yet come online. [2]
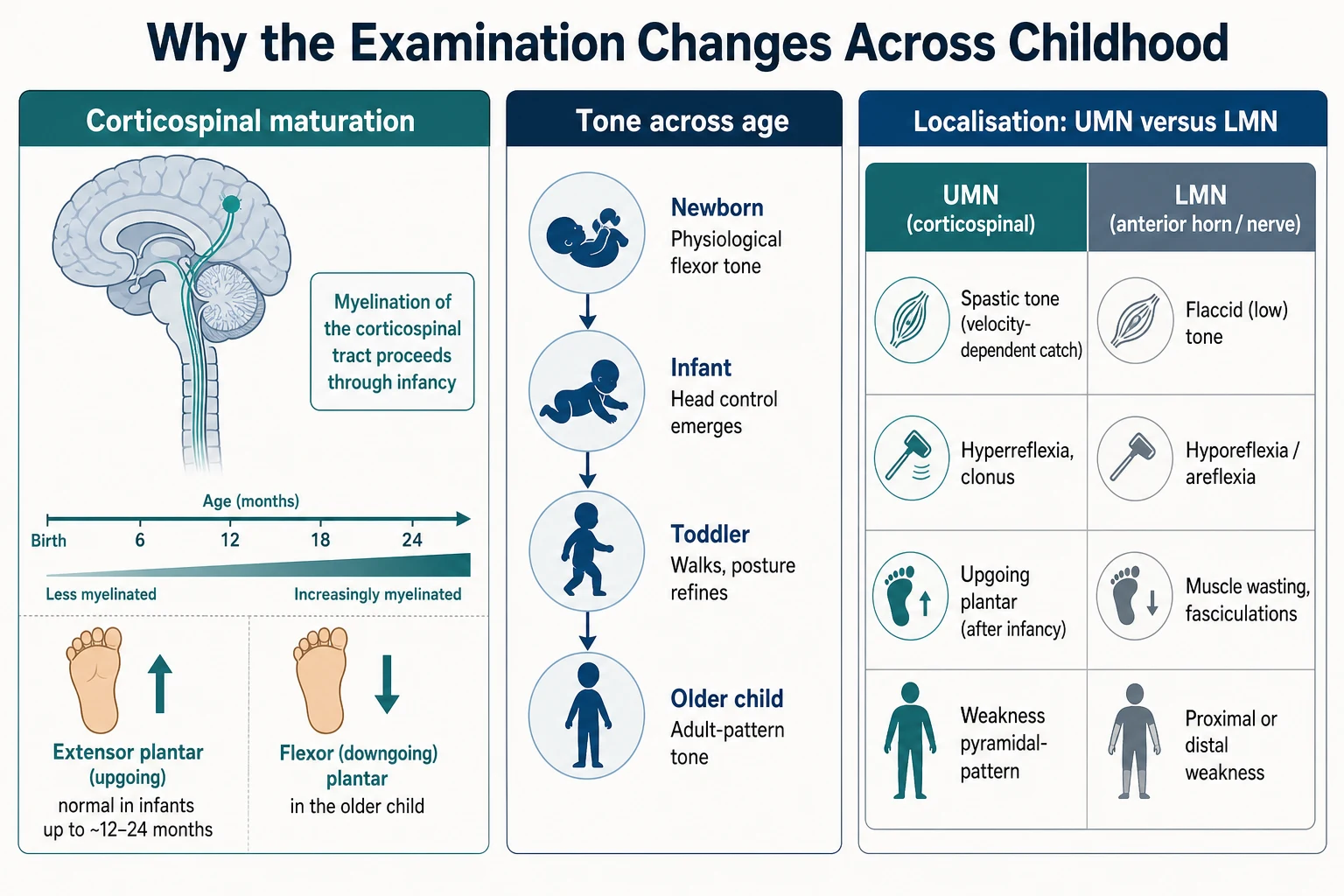
The pathophysiology of abnormal tone follows from the level of the lesion. An upper motor neuron lesion interrupts the descending inhibitory corticospinal tract and releases the lower motor neuron from inhibition, producing spasticity (the velocity-dependent catch of released stretch reflexes), hyperreflexia, clonus, and eventually an upgoing plantar. A lower motor neuron lesion destroys the final common pathway itself, producing flaccid weakness, hyporeflexia or areflexia, and muscle wasting with fasciculations. The distribution of these signs localises the lesion within the neuraxis — the central skill of the examination. [6]
Clinical Presentation
The findings you are looking for fall into two families: the normal-but-different findings of immaturity, and the genuinely abnormal findings that point to disease. The normal newborn carries physiological flexor tone from the curled intrauterine posture, lies with the limbs flexed, has a full range of primitive reflexes, and may show a few beats of ankle clonus and an extensor plantar. Head lag is marked but present; the infant cannot yet hold the head steady when pulled to sit. Over the first months the tone opens out, head control emerges, the primitive reflexes integrate, and fidgety movements appear in the general movement repertoire. [1] [2]
The abnormal findings announce themselves in characteristic ways. Increased tone in an infant appears as tightness on passive movement, a scissoring of the legs on vertical suspension, fist closure past six months, or delayed motor milestones, and it points toward cerebral palsy when the history carries risk. Decreased tone appears as the floppy infant — the rag-doll posture, the head lag that does not improve, the slip-through on vertical suspension — and the task is to separate central from peripheral. Asymmetry — a hand not used, a leg dragged, a smile that does not move both sides — points to a focal lesion. [10] [6]
Why scissoring of the legs on vertical suspension signals increased tone
Hold the infant under the axillae and lift vertically. A normal infant adducts and partly supports the legs; an infant with adductor hypertonia crosses the legs in scissoring, often with extension and the feet pointing down. The finding reflects released adductor tone from an immature but overactive corticospinal influence, and in a high-risk infant it is one of the earliest bedside clues to emerging cerebral palsy. It is not specific on its own — it must be read with the tone, the reflexes, and the developmental history. [6] [8]
In the older cooperative child the presentation shifts toward the adult pattern: a hemiparesis shown by a pyramidal-pattern weakness (arm flexors and leg extensors preferentially affected), a cerebellar ataxia shown by an wide-based staggering gait and intention tremor, a peripheral neuropathy shown by distal weakness and areflexia, or a neuromuscular junction disorder shown by fatigable ptosis and ophthalmoplegia. Each of these is read against the framework, and each points to a specific locus in the neuraxis. [12]
Differential Diagnosis
The differential is organised by the dominant finding. For the floppy infant, the causes run from the brain downward through the neuraxis: a central cause such as hypoxic-ischaemic encephalopathy, chromosomal syndrome or benign congenital hypotonia; a spinal cord cause such as birth trauma; an anterior horn cell cause such as spinal muscular atrophy; a peripheral nerve cause; a neuromuscular junction cause such as transient or congenital myasthenia or infant botulism; and a muscle cause such as a congenital myopathy or muscular dystrophy. The reflex pattern and the social engagement separate these at the bedside. [10] [11]
For the child with increased tone, the task is to distinguish a static process (cerebral palsy) from a progressive one (a metabolic or neurodegenerative disorder, a treatable dystonia such as dopa-responsive dystonia, or a spinal cord lesion masquerading as spasticity). The discriminating questions are whether the tone is worsening or changing in pattern, whether skills are being lost, and whether the upper motor neuron signs are accompanied by progression in cognition, vision, or seizures. A static picture in a high-risk infant with a non-progressive history favours cerebral palsy; a changing picture demands investigation for a treatable or progressive cause. [8] [6]
The mimics that must not be missed are few but serious. Infant botulism presents with descending flaccid weakness, a weak cry, poor feeding and constipation, often after honey exposure. Spinal muscular atrophy presents with severe symmetric proximal weakness, areflexia, and tongue fasciculations in an alert infant — a floppy baby who never moves. Acute disseminated encephalomyelitis or a spinal cord lesion can present as acute weakness with a sensory level. Each of these changes both the urgency and the investigation pathway. [11] [12]
Clinical & Bedside Assessment
The examination begins the moment you observe the child, before you touch them. Watch the posture at rest, the quality and symmetry of spontaneous movement, the level of interaction and alertness, and the cry. A floppy infant lies in a frog-leg posture with the limbs abducted and externally rotated; a hypertonic infant lies stiff with clenched fists and extended legs; a child with a hemiparesis avoids one hand or drags one leg. Observation tells you more than half of what the examination will yield, and it is the only window when the child will not cooperate with formal testing. [1] [3]
Tone is assessed by passive movement through the full range, moving each joint slowly and then quickly to feel for the velocity-dependent catch of spasticity. In the infant, add the traction response (pull to sit and watch the head and the limbs), the ventral suspension (the infant held prone should flex the limbs and hold the head near the horizontal), and the vertical and horizontal suspension manoeuvres. Each manoeuvre probes a different combination of tone, strength and postural control, and together they build a picture no single test can. [2] [10]
INFANT
Power is tested by functional observation in the infant — does the child move all four limbs against gravity, is the movement symmetric, is the child seen to reach and grasp — and by formal grading in the older cooperative child, using the Medical Research Council scale from zero (no contraction) to five (normal power). Reflexes are elicited with a reflex hammer across the biceps, triceps, brachioradialis, knee and ankle, and graded on the standard zero-to-four-plus scale: zero is absent, one-plus is hypoactive, two-plus is normal, three-plus is brisk without clonus, and four-plus is brisk with clonus. Always compare side to side. [6]
The plantar response is elicited by stroking the lateral border of the sole from the heel toward the ball and across the base of the toes, and the response of the great toe is read against age — extensor (upgoing) is normal in infancy and abnormal after the corticospinal tract matures. Coordination in the older child is tested with finger-to-nose, rapid alternating movement, heel-to-shin and tandem gait. Gait is the single most informative test in the ambulant child: observe the base, the symmetry, the arm swing, the ability to walk on heels, toes, and tandem, and whether the child can hop. A subtle hemiparesis or cerebellar lesion often declares itself only on gait. [3]
The cranial nerves are tested by the age-appropriate window: visual attention and fixing and following in the infant; formal visual acuity, eye movements, facial movement, hearing and swallow in the older child. Head circumference is measured at the widest occipitofrontal point and plotted — crossing centiles upward or downward is one of the most powerful single signs in paediatric neurology. The fontanelle is palpated for fullness and bulging. In the high-risk infant, the two standardised tools are added: the General Movements Assessment, observing the quality of the spontaneous movement repertoire, and the Hammersmith Infant Neurological Examination, a scored standardised assessment of tone, reflexes, posture and movement. [1] [4]
Investigations
Most neurological examinations need no investigation — the history and the bedside findings make the diagnosis and direct the disposition. Imaging is reserved for findings that suggest a structural lesion or raised intracranial pressure. Cranial ultrasound is the first-line modality in the newborn with an open fontanelle, screening for intraventricular haemorrhage, periventricular leukomalacia and ventriculomegaly. Computed tomography is reserved for the acute emergency when a rapid screen for haemorrhage, mass effect or fracture is needed and magnetic resonance imaging is not immediately available. Magnetic resonance imaging is the modality of choice for defining structural lesions, the brain malformations, the white matter injury of prematurity, and the stroke — and it is part of the early cerebral palsy diagnostic bundle. [8] [3]
The standardised infant tools function as investigations in their own right because they quantify risk. The General Movements Assessment is most informative at the fidgety age, around nine to twenty weeks post-term, when the normal repertoire is characterised by continuous, variable, low-amplitude movements of the neck, trunk and limbs. Absent or abnormal fidgety movements at this age are among the strongest single predictors of cerebral palsy, and they predict it months before a classic motor examination can. The Hammersmith Infant Neurological Examination yields a global optimality score; a low score in a high-risk infant, particularly one that fails to improve over serial assessments, raises the probability of an adverse outcome substantially. [4] [5]
For the floppy or weak child, the targeted investigations follow the neuraxis. Creatine kinase screens for a myopathy or muscular dystrophy; electromyography and nerve conduction studies localise the lesion to the anterior horn cell, the peripheral nerve, the neuromuscular junction, or the muscle; and genetic testing — now increasingly a rapid exome or genome — makes the specific molecular diagnosis in a large and growing share of cases. A lumbar puncture is considered when infection or inflammation is in play, but it is never performed before assessing for raised intracranial pressure, and the clinical meningeal signs are an unreliable guide in young infants. [11] [12]
Management — Resuscitation
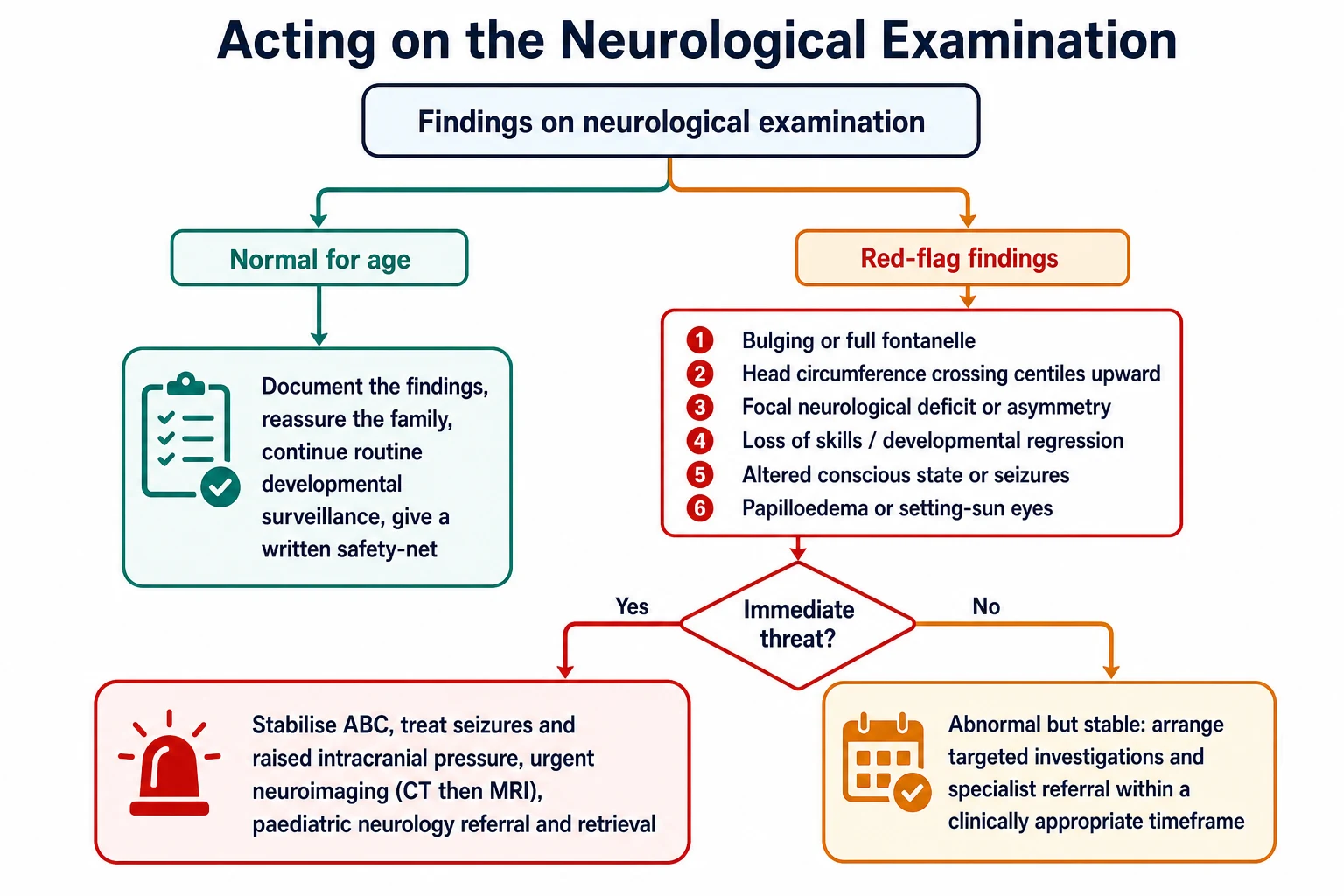
The neurological examination occasionally identifies a child in immediate danger, and the first action is always to secure the airway, breathing and circulation. The child with raised intracranial pressure — a full or bulging fontanelle, a rapidly enlarging head, setting-sun eyes, an altered conscious state, or a new focal deficit — is managed by nursing head midline and elevated to around thirty degrees, maintaining normoxia, normocapnia and a normal blood pressure to preserve cerebral perfusion, correcting hypoglycaemia and electrolyte disturbance, treating seizures promptly, and arranging urgent neuroimaging and neurosurgical and intensive care involvement. [8]
The child with an acute, progressive weakness — particularly with bulbar or respiratory involvement, as in a neuromuscular junction disorder or an acute spinal cord lesion — is managed by monitoring the respiratory rate, the work of breathing and the forced vital capacity where measurable, protecting the airway, and involving the intensive care and neurology teams early. The objective is to anticipate respiratory failure before it arrives, because a child who is still ventilating adequately can decompensate over hours. [12]
Management — Definitive & Stepwise
Once the immediate threats are excluded, the disposition follows the certainty and the severity of the finding. A finding that is clearly normal for age, in a thriving child with a reassuring history and no red flags, is documented, explained to the family, and followed with routine developmental surveillance and a written safety-net for the features that should prompt return. Over-investigation of the normal — a reflexive magnetic resonance imaging for every mildly delayed infant — adds anxiety and cost without changing outcome, and is itself a failure of good examination. [8]
A finding that is abnormal but stable, and not immediately dangerous, is referred to paediatric neurology or developmental services within a clinically appropriate timeframe, with targeted investigation arranged in parallel where the phenotype is clear — a creatine kinase for suspected muscle disease, an early magnetic resonance imaging for suspected cerebral palsy. The international clinical practice guideline for children at high risk of cerebral palsy recommends combining the General Movements Assessment, the Hammersmith Infant Neurological Examination and magnetic resonance imaging to make an early, accurate diagnosis before the corrected age of six months, because early intervention in this window can shape the developing motor system. [8] [9]
In Australia and Aotearoa New Zealand, the early-detection pathway is built around standardised infant tools delivered through the neonatal follow-up and developmental surveillance services, with referral to paediatric rehabilitation and the National Disability Insurance Scheme for confirmed cerebral palsy. The culturally safe assessment of Maori, Aboriginal and Torres Strait Islander children, and the equity of access to early intervention for remote families, are explicit quality measures — the goal is that the gap between an abnormal finding and a supported family is measured in weeks, not years. [9]
For the child with confirmed cerebral palsy, the examination is completed by assigning a Gross Motor Function Classification System level, a five-level ordinal scale that describes the child's usual gross motor ability and predicts the motor trajectory. Level one describes a child who walks without limitation; level two walks with limitations; level three walks with a handheld mobility device; level four has self-mobility with limitations and may use powered mobility; and level five is transported in a wheelchair, with severe limitation even of basic voluntary movement. The level anchors the prognosis, the rehabilitation goals, and the equipment plan, and it is re-stated at intervals as the child grows. [7]
Specific Subtypes & Scenarios
The newborn examination is its own discipline, formalised by the Dubowitz and the Hammersmith Neonatal Neurological Examination. It weighs posture and tone, primitive reflexes, spontaneous movement, and signs of central depression, and it is the earliest window on the brain after a complicated pregnancy or neonatal course. Serial examinations in the neonatal intensive care unit track the recovery from neonatal encephalopathy and the emergence of any fixed deficit. [1]
The infant at the fidgety age is the highest-yield single assessment in paediatric neurology, because this is the window in which the General Movements Assessment predicts cerebral palsy earliest. Absent or abnormal fidgety movements at corrected age nine to twenty weeks, combined with a low Hammersmith score and an abnormal magnetic resonance imaging, allow an early accurate diagnosis of cerebral palsy, and international guidelines now endorse intervention from this window. The candidate who can describe how to perform and read the General Movements Assessment will separate themselves at viva. [4] [8]
The floppy infant is the classic short case and the classic trap. Approach it by asking three questions in order: is the hypotonia central or peripheral? If peripheral, where in the lower motor unit does the lesion lie? And is the process static, improving, or progressive? A central cause keeps the reflexes and the social engagement; a peripheral cause loses the reflexes in proportion to the weakness but keeps the engagement. Spinal muscular atrophy is the can't-miss peripheral cause — severe symmetric proximal weakness, areflexia, and tongue fasciculations in an alert infant. [10] [11]
The older child with possible neuromuscular disease presents with a progressive pattern — a waddling Gowers gait, a calf pseudohypertrophy, a fatigable ptosis, a foot drop — and the examination localises the lesion before the investigations confirm it. The adolescent with a possible progressive disorder is read for regression, for a changing gait or handwriting, and for the cognitive and psychiatric features that can precede the motor signs of a neurodegenerative disease by months. [12]
The examination must also be adapted to the child with a disability, neurodiversity, or limited cooperation. Break the examination into short segments, observe movement in play, use the parent as the examiner's hands, and accept a staged assessment over several visits rather than forcing a single uncooperative encounter. A careful, patient examination of an anxious or autistic child yields more than a brisk one that traumatises and informs nobody. [9]
Complications & Pitfalls
The commonest pitfall is reading a finding without the developmental lens — calling a normal extensor plantar abnormal in a two-month-old, or a few beats of clonus sinister in a newborn. The corollary is the reverse error: reassuring when a finding that should have appeared has not, or when one has appeared that should alarm. The defence against both is to know the age-stratified normal, to document the trajectory, and to re-examine over time rather than rely on a single snapshot. [2]
The technique errors are the classic viva fare. A reflex is elicited poorly by striking the tendon obliquely or through a tense muscle; the plantar response is spoiled by stroking across the sole rather than along its lateral border, or by withdrawing the foot. Tone is misread when the infant is crying, cold, or resisting, and the catch of spasticity is missed when the limb is moved too slowly to bring it out. Each of these turns a real finding into a false negative or a false positive, and each is corrected only by deliberate, practised technique. [6]
The most dangerous pitfall is to mistake regression for delay. Delay is slow acquisition of skills that are still being gained; regression is the loss of skills once held. The former warrants surveillance and routine referral; the latter is an emergency that demands urgent investigation for a neurodegenerative, metabolic, structural, or severe epileptic process. The history must ask the trajectory explicitly, because the family will rarely volunteer it and the examination alone cannot always tell the difference. [12] [11]
Prognosis & Disposition
The prognosis of an abnormal neurological finding depends on its cause, its severity, and — crucially — its trajectory. The standardised infant tools carry their own prognostic weight: absent fidgety movements at the fidgety age are highly predictive of cerebral palsy, and a low Hammersmith optimality score that fails to improve over serial assessments predicts an adverse motor outcome. In the older child, the Gross Motor Function Classification System level, once assigned and stable, predicts the motor trajectory with remarkable consistency and anchors the rehabilitation plan. [4] [7]
The disposition is shared between the paediatric medical home and specialist services. The general paediatrician performs and documents the examination at every well-child contact, refers to neurology or developmental services for abnormal findings, and retains the coordination of care — the surveillance of growth and development, the immunisations, the schooling, and the family support. The specialist confirms the diagnosis, directs the investigation pathway, and shares the long-term management of the confirmed condition. [9]
Special Populations
The preterm and neonatal intensive care graduate is examined at corrected age until the second birthday, because comparing a preterm infant to their chronological age over-calls abnormality for two years. These infants carry the highest yield of abnormal findings, and they are the population in whom the standardised infant tools earn their place — the early detection of cerebral palsy is built around them. [3] [5]
The child with disability, neurodiversity, or limited cooperation is examined with patience and adaptation, as described above. The technology-dependent child with a neurodisability is examined regularly for the secondary complications of immobility — contractures, hip displacement, scoliosis, and respiratory compromise — and the examination is as much about preventing these as about detecting new disease. [9]
In Indigenous and remote communities, and in migrant and refugee families, the examination is the front line of equity. The distance from a finding to a specialist should not be the determinant of outcome, and the clinician's threshold to examine carefully, to use the standardised tools, and to refer early is the practical expression of that principle. [9]
Evidence, Guidelines & Regional Differences
The international clinical practice guideline for the early, accurate diagnosis of cerebral palsy, and its companion on early intervention for children aged zero to two years at high risk, established the integrated pathway: combine the General Movements Assessment, the Hammersmith Infant Neurological Examination, and magnetic resonance imaging to diagnose cerebral palsy early, and begin intervention in the window of greatest neuroplasticity. These guidelines changed the standard of care from a watch-and-wait approach to an active early-detection model. [8] [9]
The Task Force on Childhood Motor Disorders definitions of hypertonia, spasticity, dystonia and rigidity gave the field a shared, operational vocabulary, and they remain the reference standard for classifying tone abnormalities at the bedside. A recent systematic review and meta-analysis confirmed the prognostic value of the Hammersmith Infant Neurological Examination global scores for neurodevelopmental outcomes after two years, strengthening the case for their routine use in high-risk follow-up. [6] [5]
Where the evidence remains weak is in the grey zone: borderline findings in the late preterm infant, the role of early magnetic resonance imaging in the well term newborn, the optimal interval for surveillance after a normal but high-risk examination, and the interpretation of transient asymmetries that resolve. In these cases the honest answer is surveillance, documentation, and a low threshold to re-examine — and the courage to say that certainty is not yet available. [12]
Exam Pearls
The named signs worth holding are few but reward marks. The setting-sun sign — the eyes driven downward so the sclera shows above the iris — is raised intracranial pressure or hydrocephalus in an infant. The scarf sign — how far the hand crosses the chest when the arm is pulled across — grades tone in the infant. The frog-leg posture is severe hypotonia. The clasp-knife phenomenon is spasticity releasing after initial resistance, and the lead-pipe resistance is rigidity. The Gowers sign is proximal muscle weakness, the child climbing up the legs to stand. [6] [10]
The single most examinable discrimination is the central-versus-peripheral split in the floppy infant, because it localises the lesion at the bedside and directs the entire investigation pathway. The second is the timing of the early cerebral palsy detection — know the fidgety age, know that absent fidgety movements predict cerebral palsy, and know that international guidelines endorse early intervention from that window. Hold these two, and the rest of the examination falls into place around them. [4] [8]
References
- [1]Dubowitz L, Ricciw D, Mercuri E. The Dubowitz neurological examination of the full-term newborn Ment Retard Dev Disabil Res Rev, 2005.PMID 15856443
- [2]Guzzetta A, Haataja L, Cowan F, et al. Neurological examination in healthy term infants aged 3-10 weeks Biol Neonate, 2005.PMID 15627727
- [3]Ricci D, Cowan F, Pane M, et al. Neurological examination at 6 to 9 months in infants with cystic periventricular leukomalacia Neuropediatrics, 2006.PMID 17177152
- [4]Prechtl HF, Einspieler C, Cioni G, et al. An early marker for neurological deficits after perinatal brain lesions Lancet, 1997.PMID 9149699
- [5]Kuo TJ, Chen HC, Wang YH, et al. Hammersmith Infant Neurological Examination global scores for predicting neurodevelopmental outcomes after 2 years of age: a systematic review and meta-analysis Dev Med Child Neurol, 2026.PMID 42375103
- [6]Sanger TD, Delgado MR, Gaebler-Spira D, et al. Classification and definition of disorders causing hypertonia in childhood Pediatrics, 2003.PMID 12509602
- [7]Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy Dev Med Child Neurol, 1997.PMID 9183258
- [8]Novak I, Morgan C, Adde L, et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment JAMA Pediatr, 2017.PMID 28715518
- [9]Morgan C, Fetters L, Adde L, et al. Early Intervention for Children Aged 0 to 2 Years With or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews JAMA Pediatr, 2021.PMID 33999106
- [10]Peredo DE, Hannibal MC. The floppy infant: evaluation of hypotonia Pediatr Rev, 2009.PMID 19726697
- [11]Prasad AN, Prasad C. Genetic evaluation of the floppy infant Semin Fetal Neonatal Med, 2011.PMID 21131247
- [12]Cicala G, Mercuri E. The floppy infant revisited: from bedside to genome Dev Med Child Neurol, 2026.PMID 41495003