Paeds · neurology-neurodisability-and-neuromuscular
Paediatric stroke and cerebral sinovenous thrombosis
Also known as Childhood arterial ischaemic stroke · Cerebral sinovenous thrombosis · Paediatric cerebrovascular disease · Childhood stroke · Venous sinus thrombosis in children
Fellowship guide to paediatric stroke and cerebral sinovenous thrombosis. Covers the classification of childhood cerebrovascular disease into arterial ischaemic stroke, cerebral sinovenous thrombosis, and haemorrhagic stroke, the epidemiology with arteriopathy as the dominant cause and recurrence driver, the pathophysiology of arterial occlusion versus venous outflow obstruction, the clinical presentation of sudden focal deficit in the older child and seizures in the infant, the urgent MRI and MRA and MRV imaging pathway, the acute management of supportive care with antithrombotic therapy for ischaemic stroke and anticoagulation for sinovenous thrombosis, the Thrombolysis in Pediatric Stroke trial and why thrombolysis is not routine in children, the focal cerebral arteriopathy and Moyamoya subtypes, secondary prevention with aspirin, and the rehabilitation and recurrence follow-up.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who develops a sudden focal neurological deficit is having a stroke until proven otherwise, and the job is to start the clock and get vascular imaging, not to attribute the deficit to a migraine or a minor fall. Paediatric stroke is broadly defined as a cerebrovascular event occurring between twenty-eight days of age and eighteen years, and it divides into three forms. Arterial ischaemic stroke is an infarction of brain tissue from occlusion of a cerebral artery. Cerebral sinovenous thrombosis is thrombosis of the dural sinuses or cerebral veins, which raises venous pressure and can produce a haemorrhagic venous infarct. Haemorrhagic stroke is non-traumatic intracranial bleeding. Neonatal stroke, which occurs between twenty-eight weeks of gestation and twenty-eight days of life, is a separate entity with its own presentation and management. [2]
The incidence of childhood arterial ischaemic stroke is about two per one hundred thousand children per year, and the incidence of cerebral sinovenous thrombosis is about 0.67 per one hundred thousand children per year. Together these are not rare in a busy paediatric service, and the dominant problem at the bedside is delay. Children present later than adults because the deficit is attributed to a postictal state, a migraine, or a limp, and the window for acute intervention narrows or closes. Lehman and colleagues identified delayed recognition as the single biggest barrier to improving paediatric acute stroke care, which is why every fellow should treat sudden focal deficit as a stroke alert. [10]
Three principles run through this topic and structure the exam answer. The diagnosis is clinical and time-critical, and sudden focal deficit in a child triggers the stroke pathway. The management is supportive care plus antithrombotic therapy for arterial ischaemic stroke and anticoagulation for cerebral sinovenous thrombosis, with thrombolysis reserved for trial contexts. And the long game is secondary prevention, because arteriopathy drives recurrence and rehabilitation shapes outcome. The American Heart Association Scientific Statement by Ferriero and colleagues sets the standard that governs paediatric stroke management across the age range. [2]
Classification
Paediatric stroke divides along a vascular axis, and the division matters because each form carries its own cause, its own imaging, and its own treatment. Arterial ischaemic stroke is an arterial occlusion producing a pale infarct, cerebral sinovenous thrombosis is a venous occlusion producing a congested and often haemorrhagic infarct, and haemorrhagic stroke is a non-traumatic bleed into the brain parenchyma or subarachnoid space. The fellow should be able to draw this division at the bedside, because it directs the vascular imaging and the drug choice. [2]
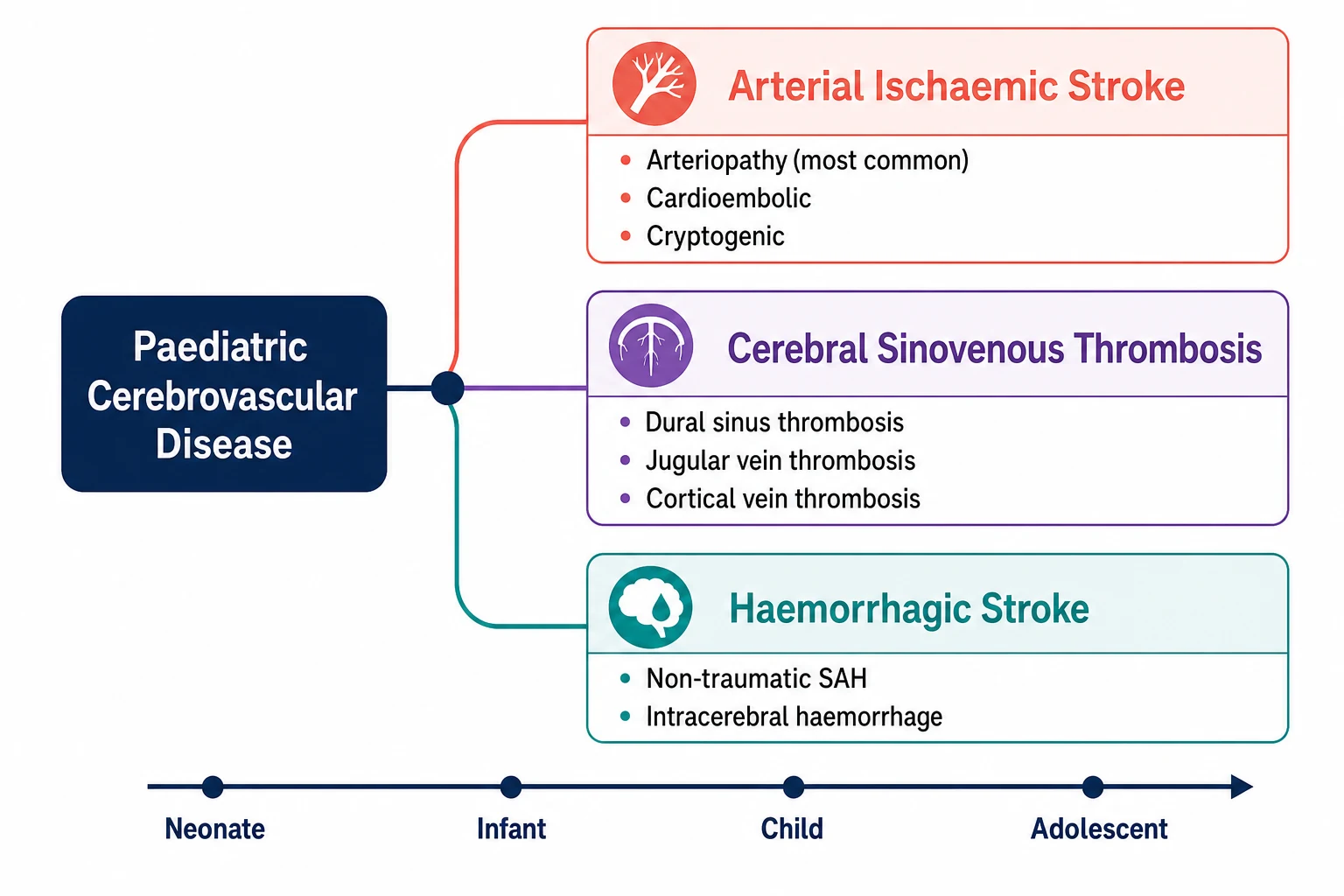
Arterial ischaemic stroke splits further by cause, and the cause search is the heart of the paediatric workup because arteriopathy is both the commonest cause and the strongest predictor of recurrence. The commonest arteriopathies are focal cerebral arteriopathy of childhood, Moyamoya disease and syndrome, post-varicella arteriopathy, and arterial dissection. Cardioembolic stroke accounts for a substantial minority and is driven by congenital heart disease, valve disease, and patent foramen ovale. Cryptogenic stroke remains the label when no cause is found despite a full workup. The CASCADE criteria were developed to standardise arteriopathy classification, and Bernard and colleagues showed that inter-rater reliability is a challenge even among experts, which is why serial imaging is part of every arteriopathy workup. [11][2]
Cerebral sinovenous thrombosis classifies by the site of the thrombus and by whether a venous infarct is present. The thrombus can sit in the superior sagittal sinus, the transverse sinus, the sigmoid sinus, the straight sinus, the jugular vein, or a cortical vein, and the superior sagittal and transverse sinuses are the commonest sites in children. The infarct, when it develops, is typically haemorrhagic because venous outflow obstruction ruptures the thin-walled cortical veins under back-pressure, and this is the key fact that explains why anticoagulation is given even when there is bleeding. [1][9]
Epidemiology & Risk Factors
Childhood arterial ischaemic stroke occurs at a rate of about two per one hundred thousand children per year, and perinatal stroke, which is not covered in detail here, is far more common at about one in four thousand live births. Boys are affected slightly more often than girls, and Black children have higher rates in some series, reflecting both sickle cell disease burden and access factors. About half of childhood arterial ischaemic strokes are attributable to arteriopathy, and the arteriopathy group is the group that recurs. [2]
The risk factors for arterial ischaemic stroke in children differ sharply from those in adults, because atherosclerosis is essentially absent. Arteriopathy is the dominant risk factor, and within that group focal cerebral arteriopathy of childhood, Moyamoya, dissection, and post-varicella arteriopathy are the main entities. Cardiac disease is the second pillar, including complex congenital heart disease, valve replacements, endocarditis, and patent foramen ovale. Infection is a frequent trigger, including bacterial meningitis, varicella, and upper respiratory and gastrointestinal infections that precede arteriopathy. Sickle cell disease carries a stroke risk several hundred times that of the general population. Prothrombotic conditions, head and neck trauma, and drugs such as oral contraceptives in adolescents complete the list. [2][6]
Cerebral sinovenous thrombosis has its own risk factor profile, and the fellow should be able to list them because several are directly treatable. Dehydration is the commonest systemic precipitant, especially in infants with poor oral intake and in those with fever. Head and neck infection, particularly otitis media and mastoiditis spreading to the adjacent dural sinuses, is the classic local cause. Iron deficiency anaemia is an important and treatable trigger, especially in toddlers. Nephrotic syndrome, prothrombotic conditions, head trauma, and the perinatal period round out the list. deVeber and colleagues established the modern understanding of paediatric cerebral sinovenous thrombosis in their landmark New England Journal of Medicine series, which set the incidence, the risk factor profile, and the outcomes that still guide practice. [1][9]
Pathophysiology
Arterial ischaemic stroke begins with an arterial occlusion, and in children the occlusion is most often driven by an arteriopathy rather than by an atherosclerotic plaque. Focal cerebral arteriopathy of childhood is a dynamic, unilateral narrowing of the terminal internal carotid and proximal middle cerebral artery that evolves over days to weeks, and Fullerton and colleagues showed that its severity and its trajectory can be scored and tracked. Moyamoya disease and syndrome produce progressive bilateral stenosis of the supraclinoid internal carotid arteries with a fragile network of collateral vessels that is prone to both ischaemic and haemorrhagic events. Arterial dissection, whether spontaneous or traumatic, tears the vessel wall and narrows the lumen or seeds a thrombus. [7][2]
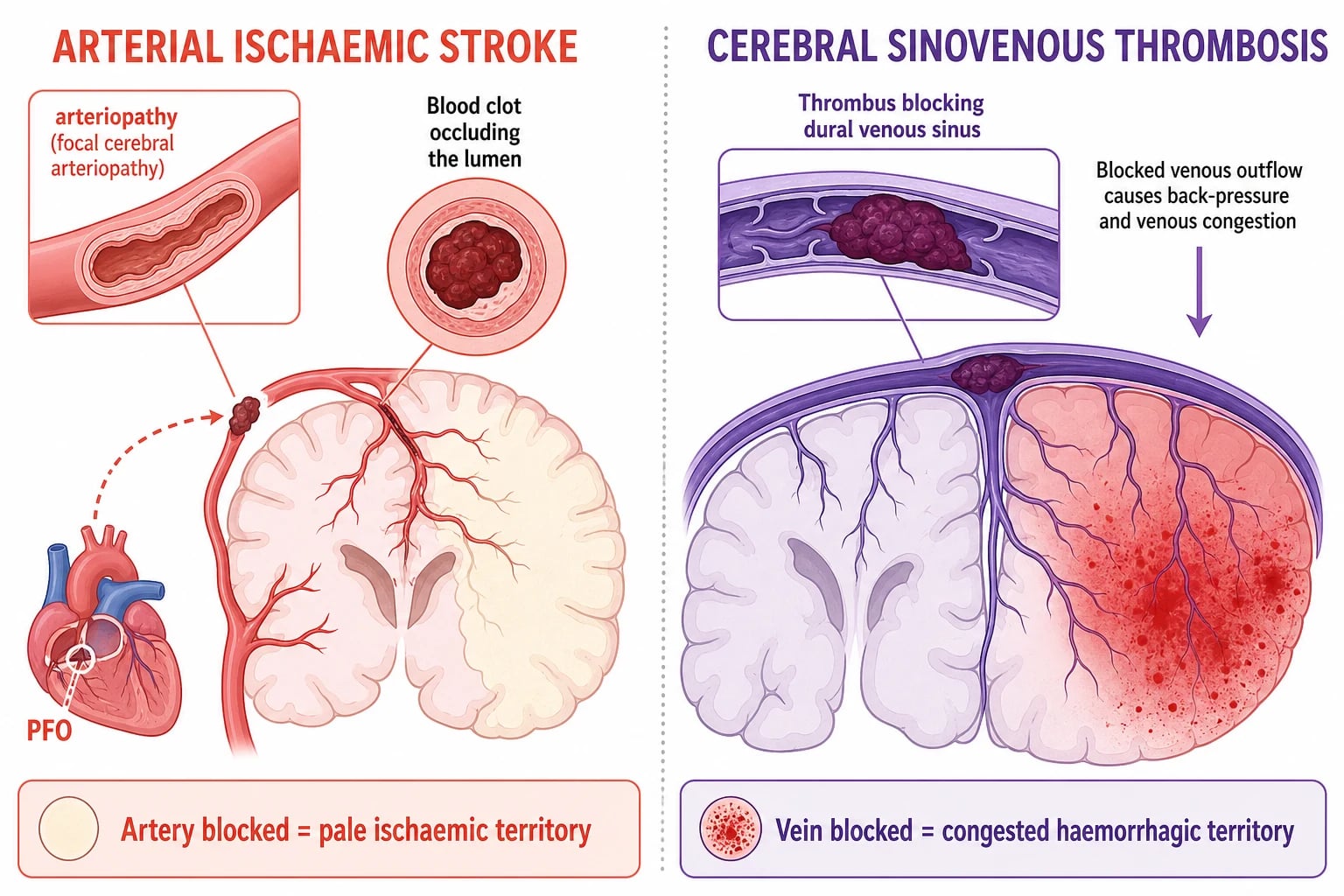
Once the artery is occluded, the downstream territory loses its blood supply and the neurons in the core die within minutes. The penumbra, the tissue at risk around the core, is salvageable if perfusion is restored, and this is the rationale for all acute stroke therapy. The energy failure triggers glutamate release, calcium influx, and excitotoxic cell death, and the infarct recruits inflammation and oedema over the following hours to days. In cardioembolic stroke the clot travels from the heart, commonly through a patent foramen ovale, and lodges in a medium-sized cerebral artery producing a sudden and often large deficit. [2]
Cerebral sinovenous thrombosis follows a different mechanical logic. The thrombus obstructs the venous outflow, the pressure rises in the upstream cortical veins and the sinus, and the brain cannot drain. The rising venous pressure produces congestion, oedema, and, when the thin-walled cortical veins rupture, a haemorrhagic venous infarct. The haemorrhage is a consequence of the obstruction, not an independent event, and removing the obstruction with anticoagulation addresses the root cause even though bleeding is already present. This is the mechanistic reason the guidelines recommend anticoagulation for cerebral sinovenous thrombosis in the face of haemorrhagic infarction. Raised intracranial pressure can follow if the thrombosis is extensive, and seizures are common because the cortex is irritated by the congested blood. [9][1]
Clinical Presentation
Arterial ischaemic stroke in the older child presents with a sudden focal neurological deficit that mirrors the affected vascular territory. Hemiparesis is the commonest sign, often with facial involvement, and the child may have slurred speech, aphasia, visual field loss, or ataxia depending on the territory. The onset is typically abrupt, and the deficit is maximal at onset, which distinguishes it from the progressive course of a tumour or a demyelinating lesion. The time of onset, or more precisely the time the child was last seen well, is the single most important historical fact because it gates any acute intervention. [3]
How paediatric stroke presents across the age spectrum
An infant who presents with new seizures, lethargy, or a hand preference, because the focal deficit is hard to elicit and seizures dominate the picture
A preschool child with sudden hemiparesis or facial droop after a minor viral illness, the classic focal cerebral arteriopathy presentation
A school-age child with sudden weakness and slurred speech during exercise or dehydration, raising Moyamoya or dissection
An adolescent on the oral contraceptive pill with an acute focal deficit, raising cardioembolic or prothrombotic causes
A child with sickle cell disease and acute neurological symptoms, treated as a stroke until exchange transfusion lowers the haemoglobin S fraction
Two subtleties are deliberately examined. The first is that seizures at the onset of a childhood stroke are far more common than in adult stroke, and the postictal state, known as Todd paresis, is the commonest mimic. The rule is that a focal deficit persisting beyond an hour after a seizure is a stroke until imaging proves otherwise, because the postictal deficit usually resolves within minutes to a few hours. The second is that the very young child cannot report a focal deficit, so the presentation is dominated by seizures, altered consciousness, or a change in tone or movement that the parent notices as a hand preference or a limp. [10]
Cerebral sinovenous thrombosis presents differently because the venous system is diffusely affected. The hallmarks are headache, vomiting, and papilloedema from raised intracranial pressure, often with seizures, altered consciousness, or a focal deficit. In infants the open fontanelle and the non-specific presentation mean that seizures, lethargy, and feeding difficulty are the commonest signs, and the diagnosis is easily missed. In the older child a headache that is progressive, worse on lying flat, or accompanied by vomiting and visual symptoms raises the diagnosis, and a sixth nerve palsy from raised pressure is a classic sign. Mandel-Shorer and colleagues emphasised that the index of suspicion must be high, because the presentation overlaps with common conditions such as viral illness and tension headache. [9][8]
Differential Diagnosis
The differential of a sudden focal neurological deficit in a child separates the true cerebrovascular event from its mimics, and the separation rests on the history, the tempo, and the imaging. The commonest mimic is the postictal Todd paresis after a seizure, which resolves within hours. Migraine with aura can produce a focal deficit that spreads over minutes, which distinguishes it from the abrupt onset of a stroke. Hypoglycaemia and electrolyte disturbance can produce focal signs, and the bedside glucose gates the workup in every case. [3]
Arterial ischaemic stroke
emergency, image now
- Sudden maximal focal deficit in a vascular territory
- Often preceded by arteriopathy, cardiac disease, or infection
- Confirmed by restricted diffusion on MRI
- Treated with antithrombotic therapy and supportive care
Postictal Todd paresis
resolves in hours
- Follows a witnessed or unwitnessed seizure
- Focal weakness that resolves within minutes to hours
- Normal MRI diffusion, no vascular occlusion on MRA
- Observe and treat the underlying seizure disorder
Migraine with aura
spreads over minutes
- Positive visual or sensory symptoms that march over minutes
- Often a personal or family history of migraine
- Normal MRI between episodes
- Treat with analgesia and antiemetic, confirm resolution
Cerebral sinovenous thrombosis
headache and raised pressure
- Headache, vomiting, papilloedema, seizures, altered awareness
- Venous infarct is often haemorrhagic
- Confirmed by absent flow on MRV
- Treated with anticoagulation even if haemorrhage present
Brain tumour, demyelination such as acute disseminated encephalomyelitis, and CNS infection such as cerebritis or abscess can all produce a focal deficit, and each is distinguished by its tempo and its imaging. A tumour produces a progressive deficit over days to weeks, demyelination often follows an infection and produces a multifocal deficit, and infection is accompanied by fever and systemic signs. Functional or conversion disorder can mimic stroke, especially in adolescents, but the pattern is inconsistent with a vascular territory and the imaging is normal. When genuine doubt exists the child is treated as a stroke and the mimic is excluded by the imaging and the evolution. [3][10]
Clinical & Bedside Assessment
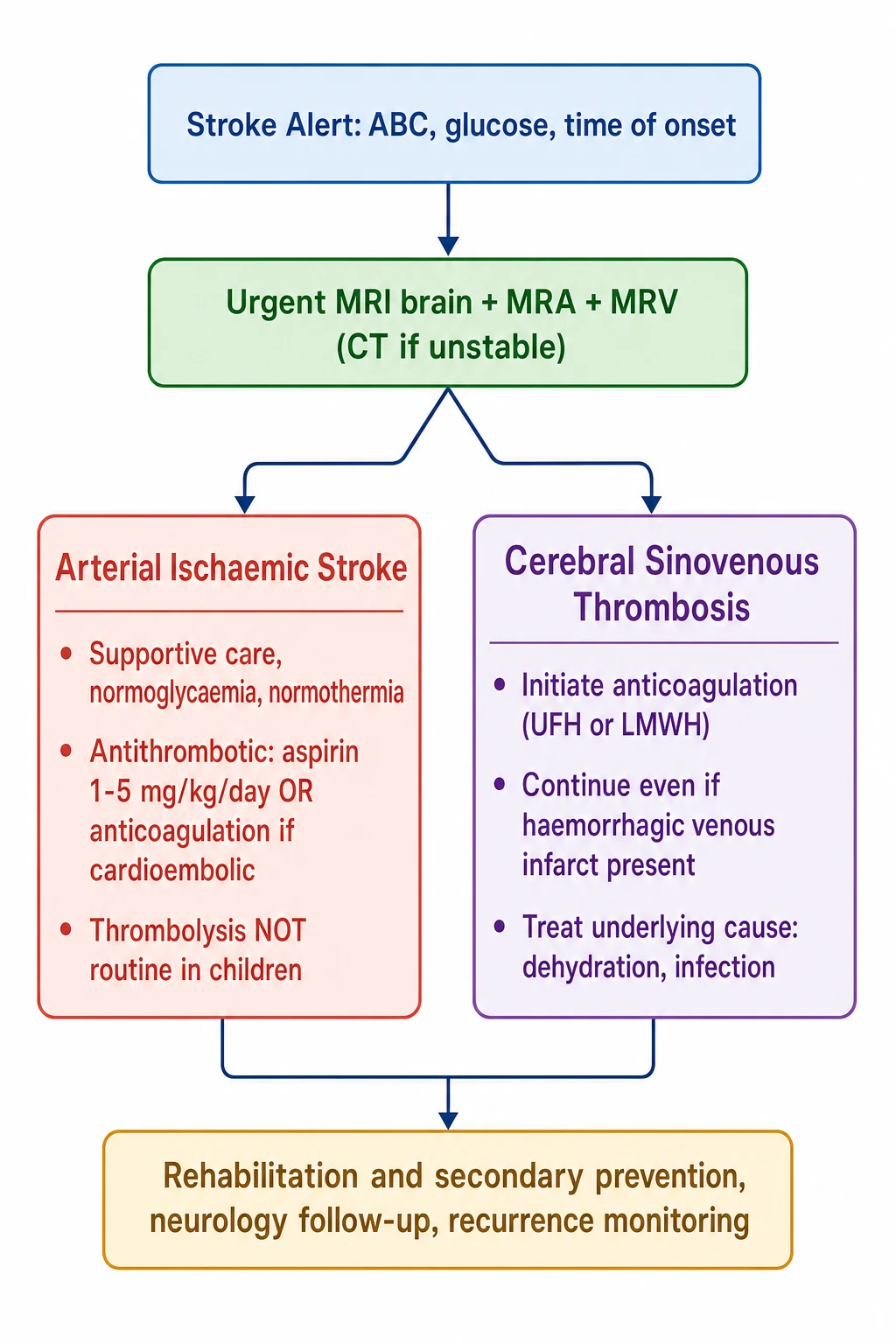
The bedside assessment of a child with a suspected stroke is a structured emergency that runs in parallel with the imaging request, not after it. The first move is to assess and support the airway, breathing, and circulation, then to check the bedside glucose, then to establish the time of onset or last seen well, and then to activate the stroke alert pathway. The clock starts at the last known well time, and the team must move toward vascular imaging without delay, because the window for any acute intervention is narrow. [3]
The focused neurological examination localises the deficit to a vascular territory and assesses the severity. Hemiparesis with facial involvement points to the middle cerebral artery territory, a visual field cut points to the posterior cerebral artery, and ataxia and vertigo point to the posterior circulation. The child with suspected cerebral sinovenous thrombosis needs a fundoscopy for papilloedema, because the raised intracranial pressure is the clue that separates venous disease from arterial. The general examination seeks the cause, including a cardiac murmur, a skin lesion suggesting a neurocutaneous syndrome, signs of head and neck infection, and evidence of trauma. [3][9]
The history taken in parallel focuses on the risk factors. A recent varicella infection, a minor head or neck trauma, an episode of dehydration, a known congenital heart disease, a sickle cell diagnosis, and a family history of early stroke or thrombosis each direct the cause search. The medication history includes the oral contraceptive pill in adolescents and any prothrombotic or cardiac medication. The developmental history matters because a child with a pre-existing hemiparesis from a perinatal stroke may present with a recurrence or a transient worsening that is mistaken for a new event. [3][2]
Investigations
The investigation of paediatric stroke rests on urgent vascular imaging, and the standard is magnetic resonance imaging of the brain with diffusion-weighted imaging, magnetic resonance angiography, and magnetic resonance venography. Diffusion-weighted imaging reveals the acute infarct within minutes of onset, which computed tomography cannot do reliably in the first hours. Magnetic resonance angiography shows the arterial tree and identifies the arteriopathy, and magnetic resonance venography shows the venous sinuses and identifies the thrombosis. A computed tomography is the fallback when the child is unstable or the MRI is unavailable, and it can exclude a large haemorrhage quickly, but it cannot replace the MRI for the acute ischaemic infarct or the vascular detail. [3]
The cause search follows the imaging and is tailored to the stroke type. An echocardiogram and an electrocardiogram are sent in every case to seek a cardioembolic source, including a patent foramen ovale, a valve lesion, and a clot in the cardiac chambers. A thrombophilia screen, including protein C, protein S, antithrombin, factor V Leiden, prothrombin gene mutation, and antiphospholipid antibodies, is sent when a prothrombotic cause is suspected, though the interpretation in the acute phase is difficult because the levels are deranged by the stroke itself. A sickle cell screen and a haemoglobin electrophoresis are sent in at-risk populations, and iron studies are sent in the child with cerebral sinovenous thrombosis because iron deficiency anaemia is a treatable trigger. [2]
Antithrombotic therapy for childhood arterial ischaemic stroke
Dose
Aspirin 1 to 5 mg per kg per day orally for secondary prevention in most cases
Serial imaging is part of every arteriopathy workup, because focal cerebral arteriopathy is dynamic and the arterial narrowing evolves over days to weeks. The first scan shows the stroke and the initial arterial appearance, and a repeat scan at one to two weeks and again at three to six months tracks the arteriopathy and guides the duration of secondary prevention. Lumbar puncture is performed when CNS infection is suspected, and it is deferred until the intracranial pressure is assessed. Electroencephalography is performed when seizures are suspected, because the child with cerebral sinovenous thrombosis often has both clinical and subclinical seizures that affect the outcome. [7][8]
Management — Resuscitation
The resuscitation of a child with an acute stroke follows the stroke alert pathway, and the guiding principle is to protect the penumbra by maintaining perfusion, oxygenation, and metabolic stability while the imaging and the cause search proceed. The airway, breathing, and circulation are assessed and supported first. Hypoxia is corrected with supplemental oxygen, and hypotension is treated with fluids to maintain cerebral perfusion. The bedside glucose is checked and corrected, because both hypoglycaemia and hyperglycaemia worsen the infarct. [2]
Normothermia is maintained, because fever in the acute phase extends the infarct, and antipyretics are given for any elevation. Seizures are treated with standard anticonvulsants, because seizure activity increases the metabolic demand of the already ischaemic brain. The child is kept nil by mouth until the swallow is assessed, because dysphagia is common after a stroke and aspiration pneumonia is a preventable complication. The paediatric neurology and rehabilitation teams are involved early, and the child is managed in a setting with neuroimaging and paediatric intensive care access. [2][3]
The child with sickle cell disease and an acute neurological deficit is a special case that demands immediate action. The stroke is assumed until proven otherwise, and the urgent exchange transfusion is started to lower the haemoglobin S fraction below thirty percent, because the sickled red cells occlude the cerebral arteries and the cerebral vasculopathy progresses if the fraction is not reduced. The imaging confirms the infarct, and the transfusion is the treatment, and both proceed in parallel rather than in sequence. [2]
Management — Definitive & Stepwise
The definitive management of arterial ischaemic stroke rests on antithrombotic therapy and supportive care, and the choice between antiplatelet and anticoagulant therapy depends on the cause. For most non-cardioembolic strokes, aspirin at 1 to 5 mg per kg per day is the standard secondary prevention, and it is started once the haemorrhage is excluded by imaging. For cardioembolic stroke, arterial dissection, and documented prothrombotic conditions, anticoagulation with low-molecular-weight heparin is preferred, and the duration depends on the cause and the reversibility of the risk factor. Darteyre and colleagues set out the secondary prevention framework, emphasising that the cause search guides the drug choice and the duration. [12][2]
[2]Intravenous thrombolysis with alteplase is not routinely recommended for paediatric arterial ischaemic stroke, and this is one of the most testable points in the topic. The Thrombolysis in Pediatric Stroke trial, known as TIPS, was the first prospective study of intravenous alteplase in children, and Amlie-Lefond and colleagues designed it to test the safety and pharmacokinetics of the standard adult dose of 0.9 mg per kg. The trial showed that children achieved lower systemic alteplase levels than adults at the same dose, suggesting that the paediatric dose may need to be higher, but the trial was closed early due to slow enrollment and could not establish efficacy or safety. The American Heart Association concludes that routine intravenous thrombolysis is not recommended for children outside a clinical trial, and this distinguishes paediatric stroke management sharply from adult practice. [5][4]
Endovascular thrombectomy is an emerging option in adults with large vessel occlusion, but the evidence in children is limited and it is not yet standard care. Bernard and colleagues described the emergence of the primary paediatric stroke center and the infrastructure needed to deliver acute stroke care to children, including the stroke alert pathway, the rapid imaging access, and the paediatric neurology and neurointerventional expertise. The current standard for most children remains supportive care with antithrombotic therapy, with thrombectomy reserved for selected cases in specialised centres under trial or registry conditions. [6]
The definitive management of cerebral sinovenous thrombosis is anticoagulation, and the approach differs from arterial ischaemic stroke. Unfractionated heparin or low-molecular-weight heparin is initiated once the diagnosis is confirmed, and the choice between the two depends on the clinical context. Unfractionated heparin is preferred when rapid reversal may be needed, such as before a neurosurgical procedure, and it is given as a loading bolus of 75 units per kg followed by a maintenance infusion titrated to the anti-Xa level. Low-molecular-weight heparin is preferred for most other cases for its predictable pharmacokinetics and its lower monitoring burden, and enoxaparin is given at 1 mg per kg subcutaneously every twelve hours in children over two months and at 1.5 mg per kg every twelve hours in infants under two months. Anticoagulation is continued for three to six months, and the underlying cause is treated in parallel. [9][2]
Specific Subtypes & Scenarios
Focal cerebral arteriopathy of childhood is the commonest arteriopathy and the one most likely to appear in the exam. It presents as a unilateral stenosis of the terminal internal carotid and proximal middle cerebral artery in a previously well child, often after a minor viral illness, and it produces a hemiparetic stroke in the middle cerebral artery territory. Fullerton and colleagues showed that the arteriopathy is dynamic, worsening over the first days to weeks, and that a severity score predicts the outcome. The arteriopathy may partly resolve over months, and the management is antithrombotic therapy with close serial imaging, and some centres add corticosteroids because an inflammatory component is suspected. [7]
Moyamoya disease and syndrome present with both ischaemic and haemorrhagic strokes, and the ischaemic events are often precipitated by hyperventilation, dehydration, or exercise, because the collateral vessels cannot increase flow to meet demand. The management combines medical prevention with aspirin and surgical revascularisation, which builds a new collateral supply to the compromised territory. The distinction between Moyamoya disease, which is idiopathic, and Moyamoya syndrome, which is secondary to conditions such as sickle cell disease or Down syndrome, matters for the counselling and the associated workup. [2]
Post-varicella arteriopathy is a specific and common entity in children, presenting as a stroke in the months after chickenpox. The virus infects the arterial wall and produces a unilateral arteriopathy in the terminal internal carotid, and the management is antithrombotic therapy, though the role of antiviral and anti-inflammatory treatment is debated. Sickle cell disease carries the highest stroke risk of any paediatric condition, and the stroke is often ischaemic from the vasculopathy, though haemorrhagic strokes also occur. Primary prevention with annual transcranial Doppler screening and chronic transfusion for the high-risk child, and secondary prevention with chronic transfusion to maintain the haemoglobin S below thirty percent, are the cornerstones. [2][12]
Cerebral sinovenous thrombosis associated with head and neck infection is the classic scenario, and the child with mastoiditis and a transverse or sigmoid sinus thrombosis is a common exam case. The management combines anticoagulation with the treatment of the infection, including antibiotics and the surgical drainage of the mastoid when indicated. Neonatal cerebral sinovenous thrombosis is a separate entity that presents with seizures and encephalopathy in the newborn, and Mineyko and colleagues showed that seizures and outcomes at one year differ between neonatal and childhood thrombosis, with neonates carrying a higher seizure burden. [8][9]
Complications & Pitfalls
Seizures are the commonest acute complication of paediatric stroke, and they occur both at onset and in the days that follow, because the ischaemic or congested cortex is irritable. Acute symptomatic seizures are treated with standard anticonvulsants, and the child is monitored for non-convulsive seizures, especially in the intensive care setting. Recurrent stroke is the feared long-term complication, occurring in fifteen to twenty-five percent of children, and arteriopathy is the strongest predictor. The recurrence risk drives the secondary prevention strategy and the serial imaging. [2]
Motor and cognitive impairment are the dominant long-term sequelae, and about half to two-thirds of children have some residual deficit after an arterial ischaemic stroke. The deficit ranges from a mild hemiparesis that allows independent walking to a dense hemiplegia that confines the child to a wheelchair. Cognitive and behavioural effects are common and often emerge as the child grows and the demands increase, and epilepsy develops in a substantial minority. The outcome is determined by the stroke size, the territory, the underlying cause, and the age at onset, with the very young and the very large strokes carrying the poorer prognosis. [2][10]
The classic pitfalls are diagnostic and therapeutic. The diagnostic pitfall is delay, attributing the sudden deficit to a migraine, a postictal state, or a minor fall, and missing the window for imaging and intervention. The second is failing to obtain vascular imaging, because the arteriopathy is invisible on a plain MRI and the recurrence risk cannot be assessed without it. The therapeutic pitfall in cerebral sinovenous thrombosis is withholding anticoagulation when haemorrhagic infarction is present, out of a mistaken fear of worsening the bleed. The therapeutic pitfall in arterial ischaemic stroke is overusing thrombolysis, applying the adult protocol to a child without the paediatric evidence to support it. [10][9]
Prognosis & Disposition
The prognosis of childhood arterial ischaemic stroke is guarded, with about half to two-thirds of children left with a residual motor or cognitive deficit, and the outcome driven by the stroke size, the territory, the cause, and the age. Mortality is low in modern series at two to five percent. The recurrence risk of fifteen to twenty-five percent is the dominant long-term concern, and arteriopathy is the strongest predictor of a second event, which is why the secondary prevention and the serial imaging continue for months to years. A child with a small stroke from a transient arteriopathy that resolves carries a better outlook than a child with a large stroke from progressive Moyamoya. [2]
Cerebral sinovenous thrombosis carries a better prognosis, with about eighty percent of children surviving without deficit or with only a mild deficit, and mortality between two and four percent in modern series. Mineyko and colleagues showed that seizures in the acute phase are the main predictor of a worse neurological outcome at one year, and that the neonatal thrombosis group carries a higher seizure burden than the childhood group. The recurrence rate is low when the underlying cause is treated, and the anticoagulation is typically continued for three to six months. [8]
Disposition is to the paediatric ward or the paediatric intensive care unit for the acute phase, depending on the stroke size, the level of consciousness, and the need for ventilation or seizure control. Rehabilitation begins in the acute setting and continues into the community, with physiotherapy, occupational therapy, speech therapy, and neuropsychology forming the multidisciplinary team. Every child is followed up in a paediatric neurology clinic to monitor the arteriopathy, to titrate the secondary prevention, and to address the developmental and educational needs that emerge over time. [2][3]
Special Populations
The child with sickle cell disease is the population at the highest baseline stroke risk, and the stroke risk is several hundred times that of the general population. The stroke is driven by a progressive cerebral vasculopathy, and the primary prevention rests on annual transcranial Doppler screening from the age of two years, with chronic transfusion initiated when the velocities are elevated. The child who presents with an acute stroke receives an urgent exchange transfusion to lower the haemoglobin S fraction below thirty percent, and the secondary prevention continues with chronic transfusion and iron chelation. [2]
The child with congenital heart disease is the second population, and the cardioembolic stroke is the dominant mechanism. The risk comes from the structural lesion itself, from the surgical correction, and from the catheter and the device procedures. The management combines anticoagulation for the cardioembolic stroke with the optimisation of the cardiac function, and the secondary prevention is tailored to the cardiac lesion and the procedure history. The child on the oral contraceptive pill or with a documented prothrombotic condition is a related population, and the management addresses the modifiable risk factor alongside the antithrombotic therapy. [2][12]
The Aboriginal and Torres Strait Islander child and the child from a remote setting is the third population, and the one for whom the access to care shapes the outcome. The longer time to presentation, the higher burden of infection and rheumatic heart disease, and the distance to a paediatric stroke centre all conspire to delay the diagnosis and narrow the intervention window. Retrieval pathways and the culturally appropriate communication are part of the acute care, and the engagement with the family and the local health service is part of the follow-up. [3]
The child from a refugee or migrant family is the fourth population, and the one for whom the communication and the continuity are the challenges. The language barrier can hide the onset time and the past history, an interpreter is engaged early, and the cause search includes the infections, the nutritional deficiencies such as iron deficiency anaemia, and the congenital conditions that may not have been screened in the country of origin. The family is connected to the local neurology service and to the rehabilitation and educational support before discharge. [10]
Evidence, Guidelines & Regional Differences
The guideline evidence is anchored by the American Heart Association Scientific Statement reported by Ferriero and colleagues, which covers the diagnosis and the management of stroke in neonates and children and sets the standard for the stroke alert pathway, the imaging, and the antithrombotic therapy. The Australian Clinical Consensus Guideline reported by Medley and colleagues addresses the diagnosis and the acute management of childhood stroke in the Australian and New Zealand context, and it converges with the American statement on the core principles of urgent imaging, supportive care, and antithrombotic therapy. [2][3]
AHA/ASA 2019
Scientific Statement
- Urgent MRI with MRA and MRV as the imaging standard
- Antithrombotic therapy with aspirin for most arterial ischaemic strokes
- Routine intravenous thrombolysis not recommended outside a trial
- Anticoagulation for cerebral sinovenous thrombosis even with haemorrhage
Australian Guideline 2019
Clinical Consensus
- Stroke alert pathway and rapid imaging access
- Supportive care with normoglycaemia, normothermia, normoxia
- Aspirin 1 to 5 mg per kg per day for secondary prevention
- Rehabilitation and structured neurology follow-up
TIPS Trial
Thrombolysis in children
- First prospective trial of intravenous alteplase in children
- Children achieved lower alteplase levels than adults at 0.9 mg per kg
- Closed early due to slow enrollment, could not establish efficacy
- Intracranial haemorrhage risk after tPA is low in children
The thrombolysis evidence rests on the Thrombolysis in Pediatric Stroke trial, reported by Amlie-Lefond and colleagues, which was the first prospective study of intravenous alteplase in children. The trial showed that children achieved lower systemic alteplase levels than adults at the standard 0.9 mg per kg dose, suggesting a need for a higher paediatric dose, but it was closed early due to slow enrollment and could not establish efficacy. Amlie-Lefond and colleagues subsequently showed that the risk of intracranial haemorrhage following intravenous alteplase for acute stroke is low in children, which keeps the door open for future trials but does not change the current recommendation against routine use. [5][4]
The arteriopathy evidence rests on the work of Fullerton and colleagues on focal cerebral arteriopathy, which provided the severity score and the natural history, and on the CASCADE criteria of Bernard and colleagues, which standardised the arteriopathy classification despite the acknowledged inter-rater challenges. The cerebral sinovenous thrombosis evidence rests on the landmark New England Journal of Medicine series of deVeber and colleagues, which set the incidence and the outcomes, and on the practical management framework of Mandel-Shorer and colleagues. The regional differences are small and centre on the thrombolysis policy, which varies between centres that participate in trials and those that do not, and on the anticoagulation duration for cerebral sinovenous thrombosis, which ranges from three to six months depending on the cause and the local protocol. [7][11][1][9]
Exam Pearls
The childhood stroke workup to the minute
References
- [1]deVeber G, Andrew M, Adams C, et al Cerebral sinovenous thrombosis in children. N Engl J Med, 2001.PMID 11496852
- [2]Ferriero DM, Fullerton HJ, Bernard TJ, et al Management of Stroke in Neonates and Children: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke, 2019.PMID 30686119
- [3]Medley TL, Miteff F, Andrews I, et al Australian Clinical Consensus Guideline: The diagnosis and acute management of childhood stroke. Int J Stroke, 2019.PMID 30284961
- [4]Amlie-Lefond C, Chan AK, Kirton A, et al Risk of Intracranial Hemorrhage Following Intravenous tPA (Tissue-Type Plasminogen Activator) for Acute Stroke Is Low in Children. Stroke, 2020.PMID 31842706
- [5]Amlie-Lefond C, deVeber G, Chan AK, et al Thrombolysis in acute childhood stroke: design and challenges of the thrombolysis in pediatric stroke clinical trial. Neuroepidemiology, 2009.PMID 19223687
- [6]Bernard TJ, Rivkin MJ, Scholz K, et al Emergence of the primary pediatric stroke center: impact of the thrombolysis in pediatric stroke trial. Stroke, 2014.PMID 24916908
- [7]Fullerton HJ, Elkind MS, Barkovich AJ, et al Focal Cerebral Arteriopathy of Childhood: Novel Severity Score and Natural History. Stroke, 2018.PMID 30355212
- [8]Mineyko A, Kirton A, Ng D, et al Seizures and Outcome One Year After Neonatal and Childhood Cerebral Sinovenous Thrombosis. Pediatr Neurol, 2020.PMID 31882182
- [9]Mandel-Shorer N, Jordan LC, Kossoff EH, et al Cerebral Sinovenous Thrombosis in Infants and Children: A Practical Approach to Management. Semin Pediatr Neurol, 2022.PMID 36456034
- [10]Lehman LL, Gitelman DK, Bebbington MW, et al What Will Improve Pediatric Acute Stroke Care? Stroke, 2019.PMID 30661501
- [11]Bernard TJ, Manco-Johnson ML, Lo W, et al Inter-Rater Reliability of the CASCADE Criteria: Challenges in Classifying Arteriopathies. Stroke, 2016.PMID 27633024
- [12]Darteyre S, Chabrier S, Heidemann-Bouvier B, et al Secondary Prevention of Childhood Arterial Ischemic Stroke. J Child Neurol, 2017.PMID 28128037