Paeds · neurology-neurodisability-and-neuromuscular
Pain, feeding and respiratory care in severe neurodisability
Also known as Supportive care in severe neurodisability · Cerebral palsy respiratory and nutritional care · Pain in non-verbal children · Gastrostomy feeding in neurodisability · Sialorrhoea and secretion management
Fellowship guide to the three threats that dominate the life of a child with severe neurodisability: persistent pain, feeding failure, and respiratory compromise. Covers the population at GMFCS level four or five with severe cerebral palsy and neurodegenerative conditions, pain assessment in non-verbal children using the revised FLACC the Paediatric Pain Profile and the Non-communicating Children's Pain Checklist with a search for treatable sources such as hip dislocation reflux constipation and fracture, the stepwise analgesic and gabapentinoid approach, oromotor dysfunction and the eating and drinking ability classification with videofluoroscopic swallow assessment and the role of gastrostomy and reflux management, and the respiratory pathway of weak cough and sialorrhoea and aspiration and sleep-disordered breathing leading to recurrent chest infection and respiratory failure with secretion control airway clearance glycopyrrolate and non-invasive ventilation, built on the American Academy of Pediatrics pain clinical report and the Australia New Zealand cerebral palsy respiratory consensus statement.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who cannot walk, cannot speak, and cannot swallow safely, and who arches with distress that no one can localise, is the everyday reality of severe neurodisability, and the three threats that decide this child's life are pain, feeding, and breathing. Severe neurodisability means a severe disorder of the developing brain or nervous system that limits motor, cognitive, and communicative function, most often severe cerebral palsy at Gross Motor Function Classification System level four or five, but also neurodegenerative conditions, severe acquired brain injury, and severe genetic and metabolic encephalopathies. The paediatrician's job is not to cure the underlying disorder but to protect comfort, nutrition, and breathing, because those three domains drive almost every admission, every complication, and the length and quality of the child's life. [1][10]
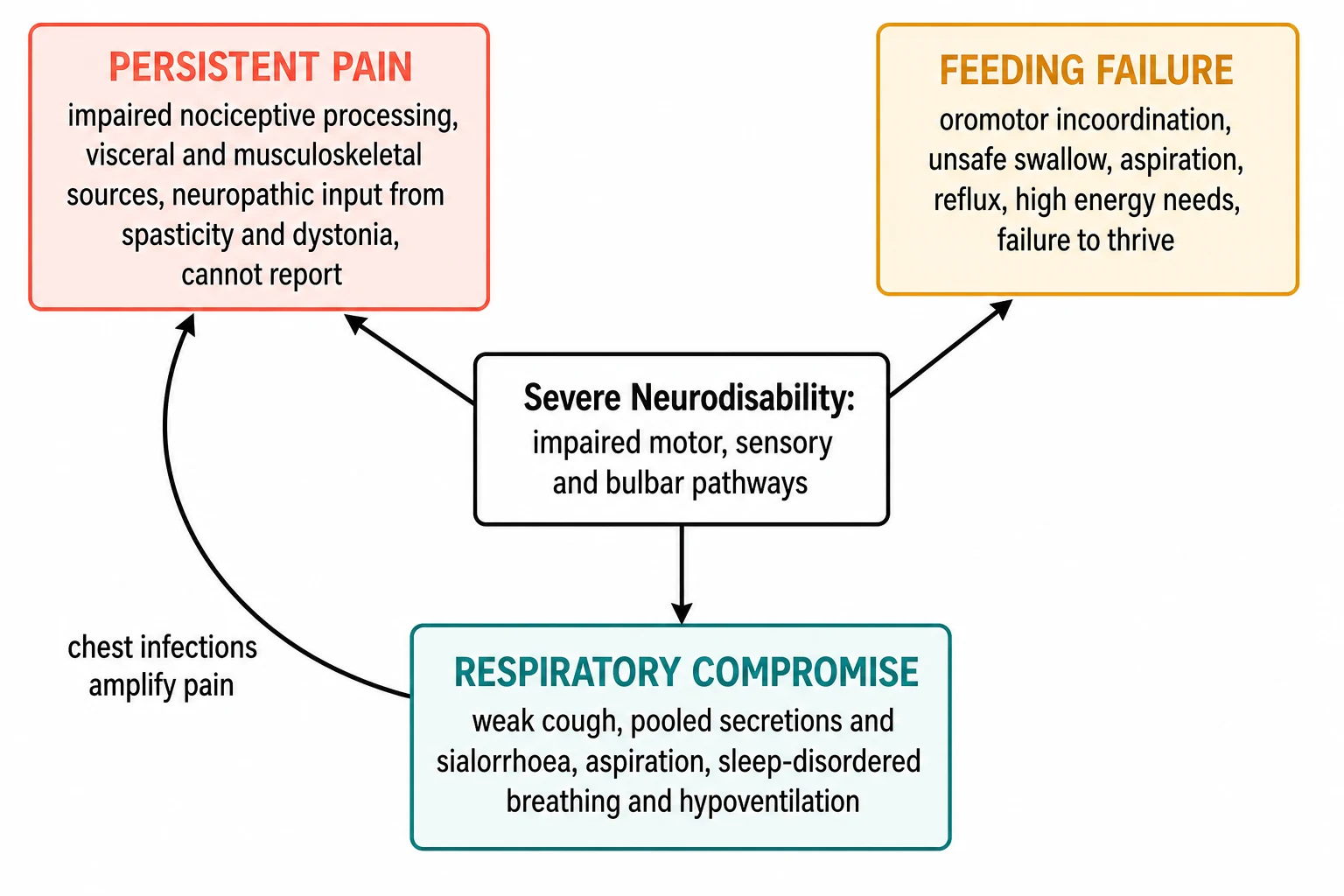
The framing idea for the exam is that pain, feeding, and breathing are not three separate problems but one interconnected care challenge. A child with oromotor weakness aspirates, the aspiration seeds chest infections, the chest infection is painful, the pain drives dystonia and worsens feeding, and the cycle accelerates. Break the cycle by treating all three together, and the child lives longer and more comfortably. Treat only one and the others pull it back down. The clinician who holds this interconnected picture will manage these children well, and the examiner rewards the candidate who says it aloud. [1]
The single most common mistake is to treat these children as static and untreatable. They are neither. Persistent pain is found in a large proportion of children with severe neurologic impairment, and most of it goes unrecognised because the child cannot report it. Respiratory illness is the leading cause of hospital admission and of death in severe cerebral palsy. Malnutrition and feeding failure are nearly universal in the most severe group. Every one of these is treatable, and treatment changes outcomes, which is why this topic sits at the heart of general paediatric practice and of the fellowship exam. [2][10]
Classification
Severity is the first thing to establish, because the child at GMFCS level five who is tube-fed and ventilated overnight has a different risk profile from the child at level three who walks with a frame and eats by mouth. The Gross Motor Function Classification System, or GMFCS, sorts cerebral palsy into five levels, and levels four and five define the population whose pain, feeding, and breathing this topic addresses: level four means the child walks short distances with a walker but mostly uses a wheelchair, and level five means the child is transported in a wheelchair and has severe limits on head and trunk control. [10]
Two further classification systems complete the bedside picture, and the candidate who names them shows fellowship depth. The Eating and Drinking Ability Classification System, or EDACS, grades oromotor function from level one, eats and drinks safely and efficiently, to level five, unable to eat or drink safely, and it predicts aspiration risk and the need for gastrostomy. The Communication Function Classification System grades how a child communicates, which matters because a non-verbal child cannot report pain and needs an observational pain tool. Reading GMFCS, EDACS, and communication level together tells the clinician how vulnerable the child is across all three domains. [8]
The three care domains themselves are then classified by their dominant problem, and this drives the assessment. Pain is sorted into nociceptive pain from a defined source such as hip, gut, or bone, and neuropathic or centrally mediated pain that is harder to localise and harder to treat. Feeding failure is sorted into unsafe swallow with aspiration, inadequate intake with failure to thrive, and reflux with vomiting and discomfort. Respiratory compromise is sorted into secretion load and sialorrhoea, recurrent aspiration pneumonia, and sleep-disordered breathing with hypoventilation. Holding these categories lets the clinician choose the right tool for each. [1][10]
Epidemiology & Risk Factors
Pain, feeding difficulty, and respiratory illness are not occasional complications of severe neurodisability but the expected baseline, and the clinician who treats them as such finds them early. Persistent pain is reported by parents in a large proportion of children with severe neurologic impairment, with musculoskeletal, gastrointestinal, and dystonia-related sources dominating, and most episodes are undertreated because the child cannot say where it hurts. [1][2]
Feeding difficulty and malnutrition track the motor severity. Children at GMFCS level four and five are the group most likely to need enteral feeding, and oromotor dysfunction affects most children in this group, with unsafe swallow and aspiration the key risks. Failure to thrive is common before gastrostomy, and weight and nutrition often improve after a feeding tube is placed, which is part of the evidence that feeding failure is treatable rather than inevitable. [8][9]
Respiratory disease is the dominant cause of hospital admission and the leading cause of death in severe cerebral palsy. The risk rises with the severity of motor impairment, with poor cough and secretion clearance, with oromotor dysfunction and aspiration, with scoliosis restricting lung capacity, and with gastro-oesophageal reflux. Each of these is a modifiable risk factor, which is the central message of the respiratory consensus statement and the reason prevention works. [10]
Pathophysiology
The mechanism that links all three domains is the loss of motor, sensory, and bulbar control that follows severe damage to the developing brain. The upper motor neuron injury causes spasticity and dystonia, the bulbar pathways fail so the swallow and cough are weak, and the sensory and cognitive pathways are impaired so the child cannot report where pain is. These three losses converge on comfort, nutrition, and breathing, and they explain why the three problems travel together. [1]
Pain in this population is neuropathic and centrally mediated as often as it is nociceptive, and that distinction changes treatment. Spasticity and dystonia generate sustained muscle contraction that is painful in itself and that drives musculoskeletal deformity, hip dislocation, and scoliosis, all of which add nociceptive pain on top. Visceral pain from reflux, constipation, and urinary tract problems is common and easily missed. The impaired ability to report and to self-regulate means pain persists, and persistent pain rewires the central nervous system so that the child becomes more, not less, sensitive over time. [2][1]
Feeding failure follows the loss of coordinated oromotor function. The muscles of the tongue, palate, and pharynx contract out of sequence, so the food bolus is not propelled safely and instead enters the airway. The cough that should clear it is weak, and the laryngeal protective reflex is blunted, so aspiration is silent and chronic. Reflux is common because the low muscle tone and the lying posture defeat the lower oesophageal sphincter, and reflux adds both discomfort and further aspiration. The combination of unsafe swallow, weak cough, and reflux is the engine of recurrent pneumonia. [9][8]
Respiratory compromise is the end result of that engine plus the mechanics of a small, distorted chest. Weak respiratory muscles give a poor cough that cannot clear secretions, the pooled saliva and sialorrhoea are aspirated, the spine curves into scoliosis that restricts lung growth and capacity, and the weak airway dilator muscles collapse the upper airway at night. The result is atelectasis, recurrent infection, and sleep-disordered breathing that progresses from obstructive apnoea to nocturnal hypoventilation, and untreated hypoventilation leads to respiratory failure and death. [10][11]
Clinical Presentation
The presentation is rarely a clear symptom, because the child cannot give one, so the clinician reads behaviour and function instead. The cardinal clue in pain is a change from baseline: new or worsening distress, arching, crying, grimacing, sleep disturbance, irritability, reduced interaction, or a sudden increase in tone and dystonia. Any of these in a non-verbal child with severe neurodisability is pain or a treatable medical problem until proven otherwise, and the clinician must resist the trap of calling it baseline behaviour. [1][2]
Feeding difficulty shows itself at the meal and on the growth chart. The child tires after a short time of feeding, coughs, chokes, gags, or pool secretions, takes a long time to eat, or refuses food. The clothes no longer fit, the weight falls across the centiles, and the child is failing to thrive. Wet or noisy breathing during or after meals, a recurrent cough, and chest infections that cluster around mealtimes all point to aspiration. The parent is usually the first to know, and the clinician must listen to the report that feeding has become a struggle. [8]
Respiratory compromise shows itself in the pattern of breathing and the pattern of illness. The child breathes fast, works hard, has a weak and ineffective cough, and is wet or rattly with secretions and sialorrhoea. Recurrent chest infections, each followed by incomplete recovery, repeated hospital admissions, and a slow decline in baseline function are the trajectory of chronic aspiration and declining reserve. Overnight, snoring, pauses, restless sleep, morning headache, and daytime sleepiness point to sleep-disordered breathing, and the finding that matters most is that the child is slowly worsening over months. [10][11]
Differential Diagnosis
The differential for a deteriorating or distressed non-verbal child is the list of treatable sources, and the discipline is to search it systematically rather than to assume the distress is neurological. The structured approach is to work head to toe and by system, and the candidate who can recite this list under viva pressure shows the thinking that keeps these children safe. [1]
SOURCES
The musculoskeletal sources are the most missed and the most rewarding to find. Hip subluxation and dislocation, pathological or occult fracture, scoliosis, and severe contractures cause sustained pain that the child cannot localise. The hip is the classic site in non-ambulant children, where the adduction and internal rotation posture and the lack of weight-bearing drive progressive displacement, and a sudden spike in distress often turns out to be a hip that has dislocated or an undiagnosed fracture from minimal trauma or osteoporosis. [1]
The gastrointestinal sources dominate the day-to-day burden. Gastro-oesophageal reflux, oesophagitis, constipation with faecal impaction, gallstones, peptic ulcer, and dental caries or abscess are all common and all treatable. Constipation is nearly universal in this group and a frequent cause of distress that is missed until it is asked about and examined for. The genitourinary sources are urinary tract infection, renal stones, and in the menstruating girl, dysmenorrhoea. The neurological sources are dystonia, muscle spasm, and neuropathic pain. The respiratory sources are pneumonia, atelectasis, and pleuritic pain from aspiration. The discipline is to keep searching until a source is found, because assuming there is none is the error. [1][2]
Clinical & Bedside Assessment
The bedside assessment has three jobs: to find the source of any acute change, to measure pain with a validated tool, and to grade function across the three domains. Begin with the airway and breathing, because respiratory failure is the immediate danger, and remember that in neuromuscular respiratory compromise the carbon dioxide rises before the oxygen falls, so a normal saturation does not exclude ventilatory failure. [10]
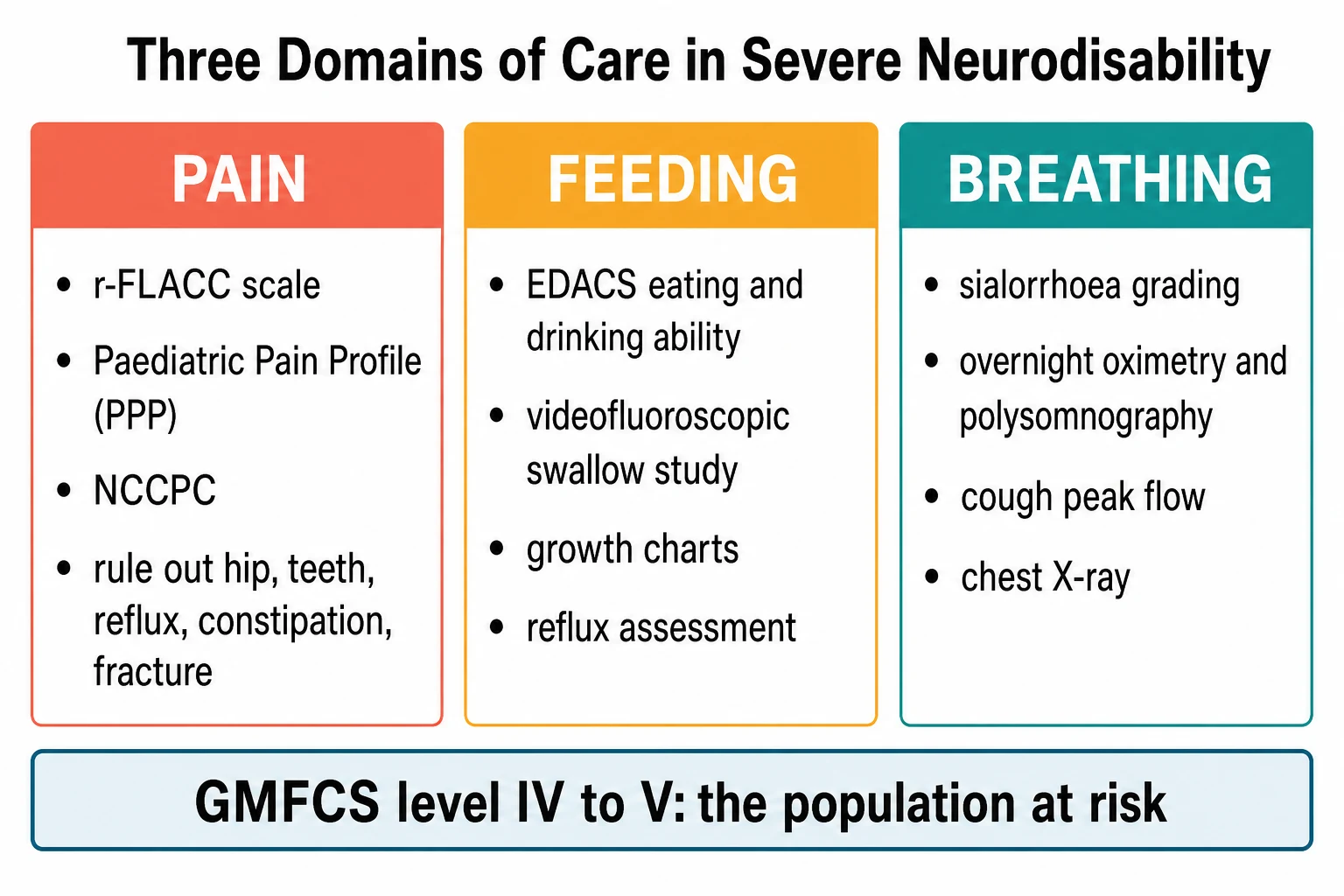
Pain assessment in a non-verbal child must use an observational tool, because the child cannot self-report and the clinician's guess is unreliable. The revised FLACC, or r-FLACC, adds a cognitive-impairment section to the face, legs, activity, cry, and consolability scale and is validated for children with cognitive impairment. The Non-communicating Children's Pain Checklist records behaviours across vocal, social, facial, activity, body and limbs, and physiological domains. The Paediatric Pain Profile is a longer, validated tool built specifically for children with severe neurological disability. Choose one, use it consistently, and treat to a comfort goal. [3][4][5]
The focused examination then searches the differential. Examine the hips for the adducted posture and limited, painful rotation that suggests dislocation, the spine for scoliosis, the mouth for dental caries and ulceration, the abdomen for constipation and impaction, and the skin for pressure injury and ingrown toenails. Observe a meal for coughing, choking, pooling, and fatigue, and time how long it takes. Grade the oromotor function with EDACS and the communication with the communication classification, and weigh and measure the child to plot growth. The clinician who does all of this at the bedside finds the treatable sources that a scan would miss. [1][8]
Investigations
The investigations are chosen to confirm a source the assessment has pointed to, not as a blanket screen. For pain, request the test that matches the suspected source: a hip X-ray for the irritable non-ambulant child, a full blood count and CRP for infection, urinalysis for urinary tract infection, an abdominal X-ray for severe constipation, and dental review for the mouth. Blood tests for calcium, phosphate, and vitamin D assess the bone health that underlies fracture risk. [1]
For feeding, the key investigation is the instrumental swallow assessment, most often a videofluoroscopic swallow study, which directly visualises aspiration during swallowing of different textures and guides the decision between texture modification and tube feeding. Growth is tracked on cerebral palsy-specific growth charts, and reflux is assessed clinically and with pH or impedance studies when the diagnosis is unclear. Nutritional assessment by a dietitian measures intake, energy needs, and micronutrient status. [8][9]
For breathing, the respiratory workup defines the reserve and the mechanism of failure. A chest X-ray shows consolidation, atelectasis, and scoliosis, and overnight oximetry and polysomnography quantify sleep-disordered breathing and hypoventilation. Spirometry or cough peak flow, where the child can cooperate or where equipment allows, measures the strength of the cough that clears secretions. Sialorrhoea is graded with a drooling scale such as the Thomas-Stonell and Greenberg scale to follow the response to treatment. The set of tests maps onto the respiratory consensus framework and drives the management plan. [10][11]
Management — Resuscitation
Resuscitation addresses the immediate threat while the assessment runs in parallel, and in this population the immediate threat is usually respiratory. A child presenting in respiratory failure from aspiration pneumonia or a chest infection needs oxygen, airway clearance, and often ventilatory support, and the clinician must support the breathing on the effort, the cough, and the carbon dioxide rather than the oxygen saturation alone. Involve paediatric intensive care early, because these children tire and deteriorate quickly. [10]
For the acute pain crisis, give analgesia promptly rather than waiting for the full workup, because untreated pain in a child who cannot report it is both cruel and clinically harmful, and the analgesia itself helps the examination by settling the distress enough to localise a source. Start with paracetamol for mild to moderate pain and step up as needed, and use an opioid for severe pain, titrated and monitored for sedation and respiratory depression. [1]
The airway is threatened by secretions and sialorrhoea in the acute chest illness, so suction, position, and chest physiotherapy are part of resuscitation, not afterthoughts. For the child who aspirates during the acute illness, stop oral feeding and protect the airway while the swallow is reassessed, and use the enteral feeding route that is already in place or place a nasogastric tube for the interim. The resuscitation phase ends when the breathing and the pain are controlled and the child is stable enough for the definitive plan. [10]
Management — Definitive & Stepwise
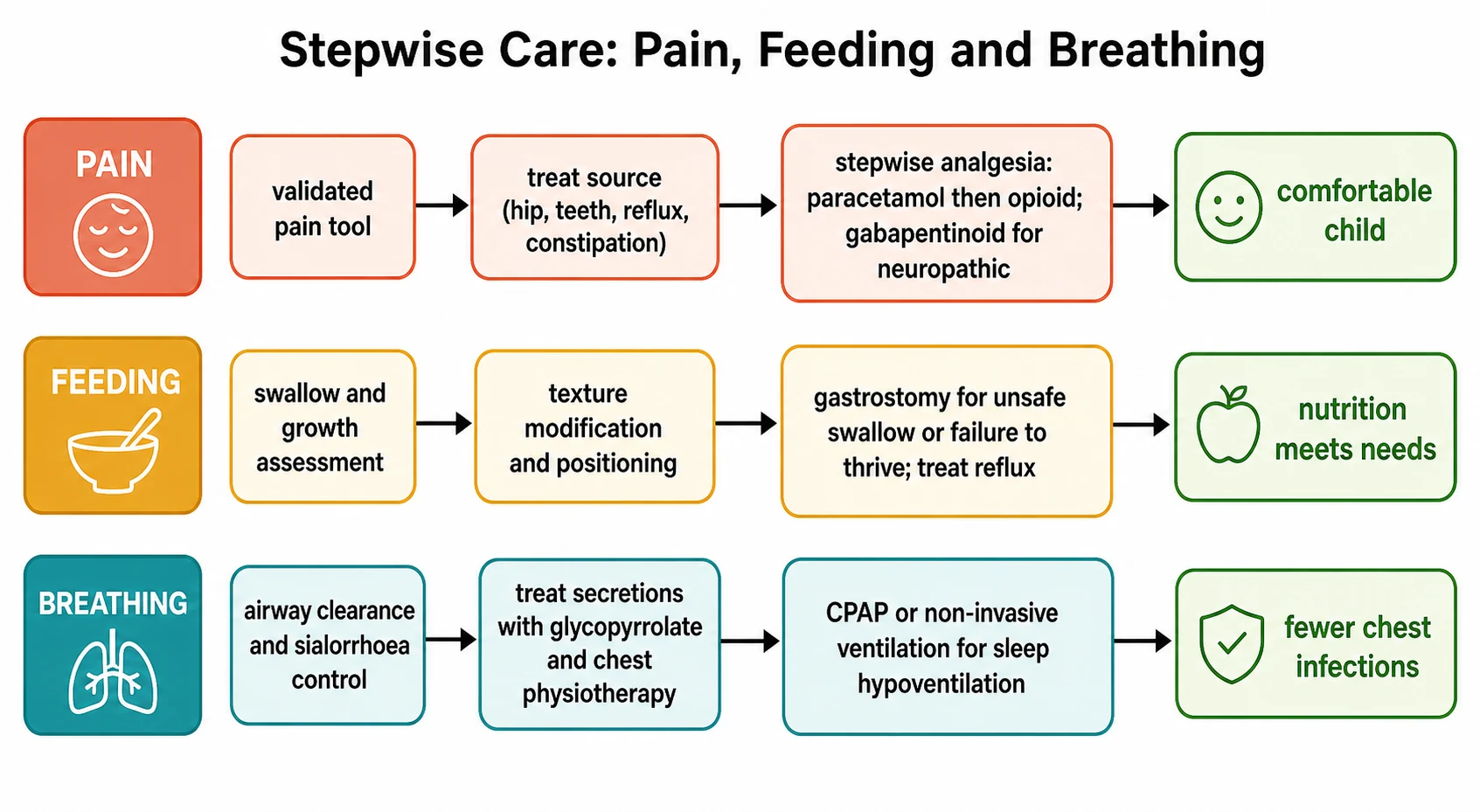
The definitive management runs along the three domains in parallel, and the guiding principle is that each domain has a stepwise path from assessment through intervention to a comfort, nutrition, or breathing goal. The clinician who treats all three together breaks the cycle that drives deterioration. [1][10]
Pain management begins with finding and treating the source, which is the single most important step and the one most often skipped. For nociceptive pain, use the stepwise analgesic ladder: paracetamol at age-appropriate weight-based dosing first, then a non-steroidal anti-inflammatory for musculoskeletal and inflammatory pain, then an opioid for severe pain, titrated to a comfort goal with an observational tool. For neuropathic or centrally mediated pain, which is common and poorly responsive to opioids, a gabapentinoid such as gabapentin or pregabalin is first-line, started low and titrated; the retrospective evidence in non-verbal children with severe neurological impairment supports gabapentin for recurrent pain. Spasticity and dystonia that drive pain are treated with antispasticity medication, botulinum toxin, or intrathecal baclofen as appropriate. [1][6]
Feeding management follows the swallow assessment and the growth data. For the child with an unsafe swallow or failure to thrive despite oral feeding and modification, enteral feeding via a gastrostomy is the definitive step, and the prospective evidence shows it improves weight and nutrition and eases the burden of feeding for the family. Treat coexisting reflux, because a gastrostomy does not eliminate aspiration risk and may unmask or worsen reflux, so medical anti-reflux therapy or, in selected cases, an anti-reflux procedure is considered alongside the feeding tube. The decision for gastrostomy is shared with the family and the feeding team, and it is framed as a step that improves nutrition and reduces aspiration, not as a failure of oral feeding. [8][9]
Respiratory management is built on the consensus framework and runs from prevention to support. Airway clearance with chest physiotherapy and a cough-assist device improves secretion clearance in the weak cough. Sialorrhoea is treated stepwise with posture and oromotor therapy first, then an antisialogogue such as glycopyrrolate, then botulinum toxin injection into the salivary glands for refractory cases, with surgery reserved for the few who fail all else. Recurrent chest infection is reduced by airway clearance, immunisation including the annual influenza and pneumococcal vaccines, and, in selected children with frequent infective exacerbations, prophylactic azithromycin. For sleep-disordered breathing and hypoventilation, overnight polysomnography guides the use of continuous positive airway pressure for obstruction or non-invasive ventilation for hypoventilation, and a small group progresses to tracheostomy and long-term ventilation. [10][11][12]
[1] [10]Specific Subtypes & Scenarios
The child who presents with a sudden change in behaviour or tone is the most common scenario and the highest-stakes one, because the default assumption must be pain with a treatable source. Run the head-to-toe and system search, use an observational pain tool, give analgesia, and re-examine. Hip dislocation and occult fracture are the classic finds in the non-ambulant child, constipation and reflux in the gut, and dental abscess in the mouth, and finding and treating the source is the whole game. [1][2]
The failing-to-thrive child with a difficult feed needs an instrumental swallow study and a nutritional assessment, and the decision turns on whether the swallow is unsafe, the intake is inadequate, or both. Gastrostomy is offered when the swallow is unsafe or when oral feeding cannot meet needs despite modification, and the conversation with the family covers the benefits for nutrition and aspiration, the residual reflux risk, and the care of the tube. The child who aspirates silently needs the feeding pathway and the respiratory pathway together, because aspiration is where feeding failure becomes respiratory illness. [8][9]
The child with recurrent chest infections needs the full respiratory prevention bundle and a search for the mechanism. The contributory factors are weak cough and poor airway clearance, sialorrhoea and aspiration of saliva, aspiration from an unsafe swallow or reflux, scoliosis, and sleep-disordered breathing. Address each in turn: airway clearance and cough-assist, antisialogogue or botulinum toxin for sialorrhoea, gastrostomy and reflux control for swallowing aspiration, and non-invasive ventilation for nocturnal hypoventilation. The child with daytime respiratory failure or cor pulmonale from chronic hypoventilation needs long-term ventilation and a paediatric intensive care and home-ventilation service. [10][11]
Complications & Pitfalls
The life-threatening complications follow the three domains. The respiratory complications are recurrent pneumonia, atelectasis, cor pulmonale from chronic hypoxaemia, and death from respiratory failure, which remains the leading cause of mortality in severe cerebral palsy. The feeding complications are aspiration pneumonia from an unsafe swallow, malnutrition and micronutrient deficiency, and the residual aspiration risk that persists after a gastrostomy because the tube does not stop the aspiration of saliva and reflux. The pain complications are sustained distress, sleep disruption, worsening dystonia and spasticity, and central sensitisation that makes future pain harder to treat. [9][10]
The classic pitfalls are the ones that cause harm. The first is to attribute a change in behaviour or tone to the underlying disorder and to miss a treatable source of pain, which is the single most common error. The second is to treat the oxygen saturation rather than the carbon dioxide in neuromuscular respiratory failure, because the saturation reads normal until late. The third is to assume a gastrostomy eliminates aspiration, when the aspiration of saliva and reflux persists and the respiratory benefit is partial. The fourth is to undertreat neuropathic pain with opioids when a gabapentinoid is what the pain needs, and the fifth is to delay polysomnography in a child with overnight desaturation and to give oxygen instead of ventilatory support for hypoventilation. [1][11]
Prognosis & Disposition
The prognosis in severe neurodisability is set by the underlying condition, but it is shaped to a large degree by the quality of the multidisciplinary care, and the message for the family and for the exam is that this care changes outcomes. Respiratory illness is the leading cause of death, and a coordinated respiratory prevention bundle reduces admissions and infection frequency. Improved nutrition after gastrostomy improves weight, energy, and sometimes respiratory reserve. Recognised and treated pain improves comfort, sleep, and interaction. None of this cures the underlying disorder, and all of it improves the life the child has. [8][10]
The disposition depends on the acuity and the domain. A child in respiratory failure goes to paediatric intensive care for ventilatory support, and a child with a severe acute pneumonia goes to the ward for antibiotics, airway clearance, and oxygen with a low threshold for escalation. The stable child is managed in the multidisciplinary clinic with paediatric, dietetic, speech and language, physiotherapy, respiratory, orthopaedic, and palliative care input, and the technology-dependent child on home ventilation or overnight feeding needs a coordinated home-care package and a clear emergency and advance care plan. [10]
Special Populations
The Aboriginal and Torres Strait Islander child and the child from a remote setting often presents later and with more advanced disease, because of distance, access, and the variable availability of multidisciplinary services, and the clinician's threshold to investigate, treat, and retrieve must be low. Equity of access to gastrostomy, home ventilation, and funded therapies is a real issue that the paediatrician advocates for, and telehealth and outreach bring the multidisciplinary team to the child who cannot travel. [10]
The child from a refugee or migrant family needs an early interpreter, culturally safe communication about feeding tubes and ventilation, and an understanding of how the family perceives disability and medical technology, because the decisions about gastrostomy and home ventilation are deeply personal and culturally shaped. The technology-dependent child on long-term ventilation and overnight feeding needs a home-care package, respite, and a school plan, and the family needs support because the caregiving burden is immense and sustained. The young person in transition to adult services needs an early and structured handover to adult neurodisability and respiratory care, because the gaps at transition are where care and continuity are lost. [10]
Evidence, Guidelines & Regional Differences
The evidence and guideline backbone is shared across regions. The American Academy of Pediatrics clinical report on pain assessment and treatment in children with significant impairment of the central nervous system sets the framework for recognising and treating pain in this population, and the supporting reviews emphasise that pain is common, under-recognised, and treatable. [1][2]
The respiratory framework rests on the Australia and New Zealand consensus statement on the prevention and management of respiratory disease in young people with cerebral palsy, which sets out the modifiable risk factors and the prevention bundle, and on the evidence that respiratory illness is the leading cause of death and admission. The feeding evidence rests on the Cochrane review of gastrostomy versus oral feeding and the prospective longitudinal studies of gastrostomy outcomes, and the drooling evidence rests on the Cochrane review of interventions for drooling. The sleep-disordered breathing evidence is summarised in the current European Respiratory Review on sleep-disordered breathing in children with neurodisabilities. [7][8][10][11][12]
Regional practice differs in the operational details. The NICE guideline on cerebral palsy in under twenty-five-year-olds sets the United Kingdom standard for assessment and management across pain, feeding, and respiratory care. The AACPDM care pathways guide nutrition and drooling management in North America. Dosing of analgesics, gabapentinoids, and antisialogogues follows the BNF for Children in the United Kingdom and Australasia and local formularies elsewhere, and the candidate should name the local source rather than recite a dose from memory. [1][10]
Exam Pearls
Severe neurodisability at GMFCS level four or five is governed by three threats: pain, feeding, and breathing, and the paediatrician who treats all three together changes length and quality of life. Pain is common and under-recognised because the child cannot report it, so a change from baseline is pain or a treatable source until proven otherwise. Use an observational tool, the revised FLACC, the Non-communicating Children's Pain Checklist, or the Paediatric Pain Profile, and search the head-to-toe and system list: hip, fracture, dental, reflux, constipation, urinary tract, dystonia. Treat the source, and use stepwise analgesia with a gabapentinoid for neuropathic pain. [1][3]
Feeding failure shows itself at the meal and on the growth chart, and the instrumental swallow study is the key test. Gastrostomy for unsafe swallow or failure to thrive improves nutrition, but it does not eliminate aspiration, because the aspiration of saliva and reflux persists. Reflux must be treated alongside the tube. [8][9]
Respiratory illness is the leading cause of death, and the modifiable risk factors are secretions and sialorrhoea, aspiration, reflux, scoliosis, and sleep-disordered breathing. The prevention bundle is airway clearance and cough-assist, antisialogogues such as glycopyrrolate or botulinum toxin for sialorrhoea, immunisation, and non-invasive ventilation for nocturnal hypoventilation. Remember that the carbon dioxide rises before the oxygen falls in neuromuscular respiratory failure, so treat the breathing on the effort and the carbon dioxide, not the saturation alone. The evidence rests on the AAP pain report, the Australia and New Zealand cerebral palsy respiratory consensus, the Cochrane reviews of gastrostomy and drooling, and the European Respiratory Review on sleep-disordered breathing. [1][10][11]
References
- [1]Hauer J, Houtrow AJ, Section on Hospice and Palliative Medicine, Council on Children with Disabilities Pain Assessment and Treatment in Children With Significant Impairment of the Central Nervous System: A Review. Pediatrics, 2017.PMID 28562301
- [2]Hauer JM Pain in Children With Severe Neurologic Impairment: Undoing Assumptions. JAMA Pediatr, 2018.PMID 30128540
- [3]Malviya S, Voepel-Lewis T, Burke C, et al The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr Anaesth, 2006.PMID 16490089
- [4]Breau LM, Finley GA, McGrath PJ, Camfield CS Validation of the Non-communicating Children's Pain Checklist-Postoperative Version. Anesthesiology, 2002.PMID 11873023
- [5]Hunt A, Wisbeach A, Seers K, et al Development of the paediatric pain profile: role of video analysis and saliva cortisol in validating a tool to assess pain in children with severe neurological disability. J Pain Symptom Manage, 2007.PMID 17349497
- [6]Hauer JM, Solodiuk JC Gabapentin for management of recurrent pain in 22 nonverbal children with severe neurological impairment: a retrospective analysis. J Palliat Med, 2015.PMID 25658145
- [7]Gantasala S, Sullivan PB, Thomas AG Gastrostomy feeding versus oral feeding alone for children with cerebral palsy. Cochrane Database Syst Rev, 2013.PMID 23900969
- [8]Sullivan PB, Juszczak E, Bachlet AM, et al Gastrostomy tube feeding in children with cerebral palsy: a prospective, longitudinal study. Dev Med Child Neurol, 2005.PMID 15707230
- [9]Sullivan PB, Morrice JS, Vernon-Roberts A, et al Does gastrostomy tube feeding in children with cerebral palsy increase the risk of respiratory morbidity? Arch Dis Child, 2006.PMID 16446283
- [10]Gibson N, Blackmore AM, Chang AB, et al Prevention and management of respiratory disease in young people with cerebral palsy: consensus statement. Dev Med Child Neurol, 2021.PMID 32803795
- [11]Vanhaverbeke K, Selcuk M, Ersu R, et al Sleep-disordered breathing in children with neurodisabilities. Eur Respir Rev, 2026.PMID 42128483
- [12]Walshe M, Smith M, Pennington L Interventions for drooling in children with cerebral palsy. Cochrane Database Syst Rev, 2012.PMID 23152263