Paeds · neurology-neurodisability-and-neuromuscular
Secondary headache and raised intracranial pressure
Also known as Secondary headache in a child · Raised intracranial pressure in childhood · Papilloedema and the dangerous headache · Idiopathic intracranial hypertension in children · Brain tumour headache · Pseudotumour cerebri syndrome
Fellowship guide to the child whose headache may be secondary: the central task is not to diagnose the headache but to exclude a dangerous cause, using a red-flag screen that separates the small minority with raised intracranial pressure from the large majority with a benign primary headache. The two syndromes that dominate the exam are idiopathic intracranial hypertension, defined by the Friedman 2013 revised criteria of papilloedema with normal neuroimaging and cerebrospinal fluid and an elevated opening pressure, and the brain tumour, whose HeadSmart symptom cluster of morning headache, vomiting and behavioural change is the key to early diagnosis. The single error that fails children is reassuring a progressive or morning headache with vomiting, because headache alone is a late and unreliable sign of a tumour.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
This page is built around the three questions a clinician actually answers, in order, when a child presents with headache. First, is this a primary headache that is safe to manage in the community, or does a red flag demand imaging? Second, if imaging is needed, what modality and what finding? Third, for the two raised-pressure syndromes that examiners test hardest, how is idiopathic intracranial hypertension confirmed and treated, and how is a brain tumour recognised early? The thread that runs through all three is papilloedema: the fundoscopic finding that converts a subjective complaint into an objective sign of raised pressure. [6]
Headache is one of the commonest reasons a child is brought to a clinician, and the great majority are primary headaches that need no scan. The danger lies in the small secondary minority, where the cost of reassurance is a delayed tumour diagnosis, permanent visual loss, or death from herniation. The sections that follow teach the screen, the mechanism, the work-up, and the management of the raised-pressure syndromes, and they link to the headache-and-migraine leaf for primary headache depth and to the hydrocephalus-and-shunt-emergencies leaf for the mechanical and shunt-dependent pathways. [2] [10]
Overview & Definition
A secondary headache is a headache caused by a separate, identifiable process acting on the pain-sensitive structures of the head. The process may be a growing tumour, obstructed cerebrospinal fluid, an infection, a bleed, a vascular lesion, or a drug. A primary headache, by contrast, is the condition itself: migraine, tension-type headache, and the trigeminal autonomic cephalalgias are disorders of headache generation rather than symptoms of something else. [3]
The clinical problem is one of proportion. Most children with headache have a primary headache or a viral illness, and scanning every child would do more harm than good. Yet the secondary causes, though uncommon, carry the full weight of missed serious disease. The red-flag screen exists to resolve this tension: it tells the clinician when a headache has crossed the line from safe to investigate. [4]
Within the secondary headaches, the raised-intracranial-pressure syndromes are the exam centrepiece because they are common enough to meet, dangerous enough to matter, and treatable if found early. Idiopathic intracranial hypertension produces headache and papilloedema without a mass. A brain tumour produces headache and vomiting through a mass or through obstructed cerebrospinal fluid. Both can threaten vision or life, and both are missed when the clinician reaches for a reassuring label before examining the fundi. [8]
Classification
The first classification decision separates a primary from a secondary headache. This is not a laboratory test but a structured judgement built from the history, the examination, and the red-flag screen. A child with a stable recurrent pattern consistent with migraine or tension-type headache, a normal examination including the fundi, a compatible family history, and no red flags is classified as primary and managed without imaging. [1]
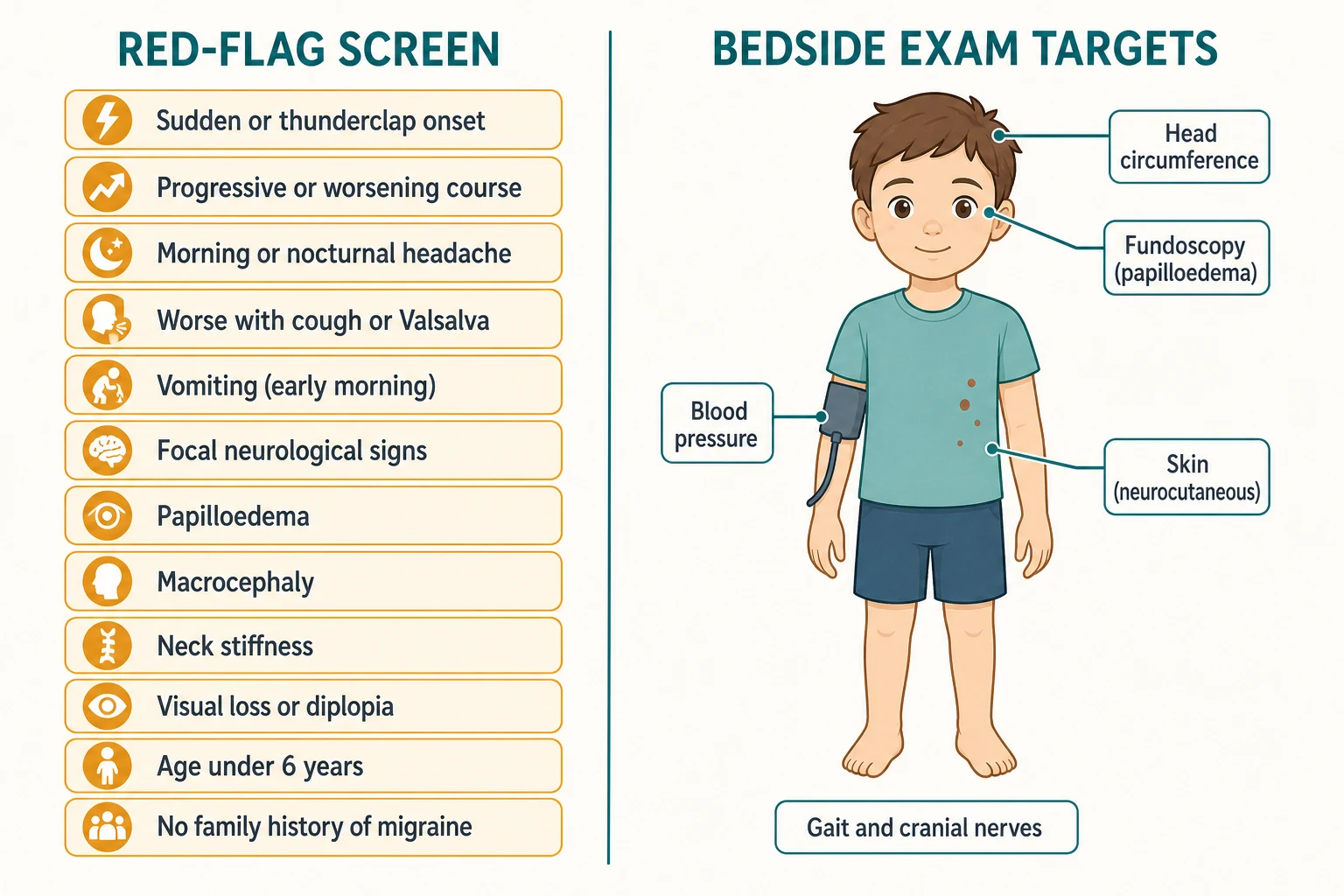
The red-flag screen is the operational classifier for the secondary headache. It is the paediatric adaptation of the framework used in adults, organised so that each flag points toward a dangerous mechanism. The flags are: a sudden or thunderclap onset, a progressive or accelerating course, a change from the child's usual pattern, a morning or nocturnal headache, worsening with cough or straining, vomiting especially in the early morning, a focal neurological sign, papilloedema, macrocephaly, neck stiffness, visual loss or diplopia, a first severe headache, age under six years, and the absence of a family history of migraine. [4]
The raised-intracranial-pressure headaches are then classified by mechanism. A space-occupying lesion, a tumour, an abscess, or a haematoma, adds volume inside the skull. Obstructive or communicating hydrocephalus adds cerebrospinal fluid. Idiopathic intracranial hypertension raises pressure without a mass. Secondary intracranial hypertension raises pressure through a defined cause such as a cerebral venous sinus thrombosis, meningitis, or a drug. Distinguishing the idiopathic from the secondary form changes the work-up and the prognosis, which is why magnetic resonance imaging with venography is part of the first investigation rather than an add-on. [7] [5]
Epidemiology & Risk Factors
Primary headaches account for the large majority of paediatric presentations, with migraine and tension-type headache dominating. By adolescence, migraine alone affects around one in ten children, and the burden rises through the school years. Secondary causes are far less common, but they are over-represented among the children who come to harm, which is why their rarity never justifies a lower index of suspicion. [2]
Idiopathic intracranial hypertension has a recognisable phenotype in the post-pubertal adolescent: female, obese, and complaining of daily headache with visual symptoms. The pre-pubertal child is a distinct phenotype, often male and not obese, and the absence of the classic phenotype must not close the mind to the diagnosis. Secondary intracranial hypertension shares the pressure rise but has a cause to find: cerebral venous sinus thrombosis, chronic otitis media or mastoiditis, recent head trauma, corticosteroid withdrawal, tetracycline-class antibiotics, isotretinoin and other retinoids, growth hormone therapy, and iron-deficiency anaemia. [8] [7]
Brain tumours are the commonest solid tumour of childhood and the second commonest childhood malignancy after leukaemia. The posterior fossa and midline tumours are the subtypes most likely to raise pressure, because they sit where cerebrospinal fluid flows: medulloblastoma, pilocytic astrocytoma, ependymoma, brainstem glioma, and craniopharyngioma. A clinician who knows where these tumours grow can predict how they present, which is why the symptom cluster maps so tightly onto the anatomy. [10]
Although individual red flags have a low positive predictive value in isolation, the yield rises steeply when flags cluster. The findings that carry the highest yield for intracranial pathology are an abnormal neurological examination and papilloedema, and a child with both is not a candidate for watchful waiting. [4]
Pathophysiology
The skull is a rigid box that holds three components: the brain, the blood, and the cerebrospinal fluid. The volume inside the box is fixed. When a tumour grows or cerebrospinal fluid is obstructed, the added volume is first absorbed by displacing fluid and venous blood, so the pressure barely moves. Once that compensation is exhausted, small further additions of volume produce large rises in pressure. This is the flat portion of the intracranial volume-pressure curve, and it explains why a child can look well one week and decompensate the next. [7]
The raised-pressure headache is generated by traction and displacement of the pain-sensitive structures inside the head. These are the dura at the skull base, the large venous sinuses, and the proximal arteries. The pattern follows directly from the mechanism: it is worse in the morning because lying flat overnight raises intracranial pressure; it is worse with coughing, straining, or bending because those manoeuvres further raise venous pressure; and it is accompanied by vomiting because of pressure on brainstem centres. [3]
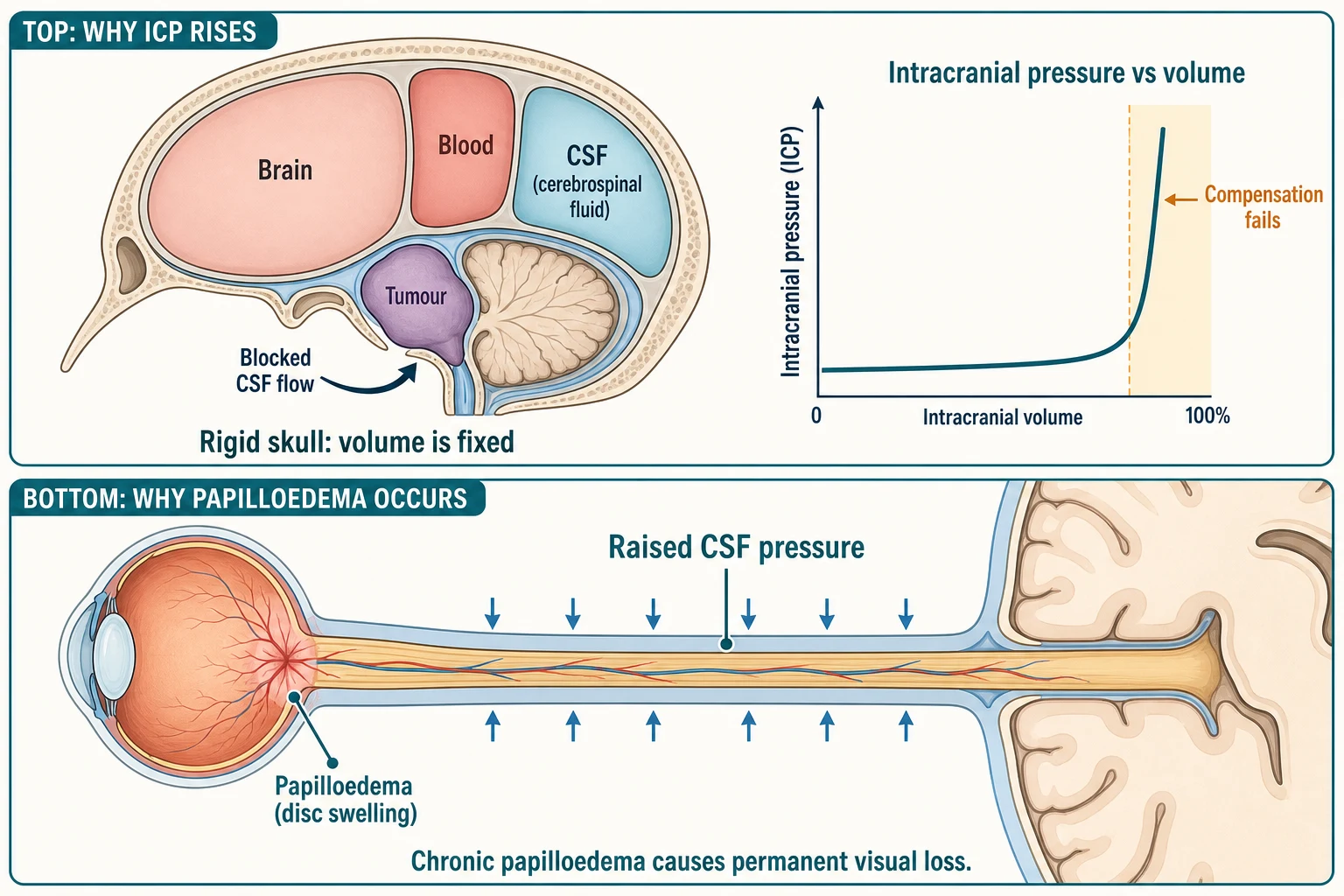
Idiopathic intracranial hypertension is a disorder of cerebrospinal-fluid balance, with impaired absorption at the arachnoid granulations and a contribution from cerebral venous hypertension. The raised pressure transmits along the optic nerve sheath and produces papilloedema, the swelling that threatens vision. The same pressure stretches the abducens nerve as a long, vulnerable false-localising sign, which is why a sixth-nerve palsy in this context does not point to a local lesion. [5] [6]
Papilloedema is optic-disc swelling caused by raised intracranial pressure transmitted along the optic nerve sheath. It is bilateral, though it may be asymmetric, and it evolves through stages from early swelling to chronic atrophy. The clinical importance is direct: chronic papilloedema causes secondary optic atrophy and permanent visual loss, and that visual loss is the main reason idiopathic intracranial hypertension is treated at all. [8]
Clinical Presentation
A child with a safe primary headache tells a consistent story. The episodes are stereotyped and recurrent, they last hours, they build through the day rather than on waking, and they improve with sleep or simple analgesia. There is a family history of migraine, the examination is normal, and the child is entirely well between episodes. That child needs a primary-headache plan, not a scan. [1]
The raised-pressure headache tells a different story, and the examiner listens for its shape. It is progressive rather than stable. It is often bi-frontal or occipital. It is present on waking and improves as the day goes on. It is made worse by coughing, straining, or bending forward. It is accompanied by nausea and vomiting, and the vomiting is classically in the early morning. Any one of these features demands attention; several together demand imaging. [3] [11]
The brain tumour rarely announces itself with headache alone. The HeadSmart guideline describes a symptom cluster, and the combination and its change over time matter more than any single feature. The cluster is: headache, vomiting, behavioural or school change, ataxia and abnormal gait, visual disturbance, growth and endocrine change, seizures, a motor or sensory deficit, cranial-nerve palsies, regression of milestones, and, in an infant, macrocephaly or a bulging fontanelle. Headache by itself is a late and unreliable sign, which is why waiting for a focal deficit before imaging costs time. [11] [10]
Idiopathic intracranial hypertension presents with a daily headache that may resemble a primary headache and so is easily dismissed. The features that mark it out are transient visual obscurations, a whooshing pulsatile tinnitus, and diplopia from a sixth-nerve palsy. The decisive finding is papilloedema on fundoscopy. Once papilloedema is seen, the question stops being whether to investigate and becomes how quickly. [8] [6]
Differential Diagnosis
The secondary causes to exclude form a short, learnable list. A space-occupying lesion, a tumour, an abscess, or a haematoma, heads it. Hydrocephalus and a malfunctioning shunt follow. Idiopathic and secondary intracranial hypertension come next. Intracranial infection, meningitis, encephalitis, and a brain abscess, must not be missed. Vascular causes include haemorrhage, an arteriovenous malformation, cerebral venous sinus thrombosis, and arterial dissection. Trauma and the post-concussive headache, hypertensive encephalopathy, and the refractory ocular, dental, and sinus causes complete the list. [3]
Secondary headache causes worth naming at viva
The hardest distinction is between idiopathic and secondary intracranial hypertension, because the two look alike until the cause is found. The work-up does the separating: magnetic resonance imaging with venography excludes a venous sinus thrombosis and a mass, the history excludes causative drugs, and the cerebrospinal fluid is normal in composition. A child with papilloedema and an identified trigger, a recent tetracycline, a known thrombosis, or otitis media, has secondary intracranial hypertension, and the trigger must be removed alongside the pressure control. [5] [7]
The raised-pressure headache must also be told apart from migraine, and the history does most of the work. Migraine is episodic, with photophobia, phonophobia, and a throbbing quality, is relieved by sleep, and runs in the family. The raised-pressure headache is progressive, positional, morning, and paired with vomiting and papilloedema. The danger is the child whose migraine label was applied years ago and never revisited as the pattern changed; a change in the pattern is itself a red flag. [2] [12]
A separate and common pitfall is the optic disc that looks swollen but is not. Optic disc drusen, tilted discs, and congenital disc anomalies can mimic papilloedema, and overcalling them drives unnecessary investigation and anxiety. This is why the diagnosis of raised pressure is confirmed with formal visual fields, optical coherence tomography, and ultimately a lumbar puncture, rather than on the fundoscopic view alone. [6]
Clinical & Bedside Assessment
Every child with a headache needs a documented general and neurological examination, and the examination is the part most often skimped. Measure the blood pressure to exclude hypertensive encephalopathy, the head circumference in the young to detect macrocephaly, and inspect the skin for the neurocutaneous stigmata of neurofibromatosis and tuberous sclerosis that predispose to tumours. Complete the cranial nerves, the motor and cerebellar systems, the gait, and the fundoscopy. [2] [1]
Fundoscopy is the single most important and the most often deferred part of the examination, because the fundoscopic finding of papilloedema converts a complaint into an objective sign. The practical difficulty is that a clear view of the disc is hard to obtain in an uncooperative child, and a poor view is not a negative result. When the view is poor or the suspicion is real, arrange dilated fundoscopy by ophthalmology or fundal photography rather than documenting the fundi as normal. [6]
The headache history is taken in the same structured way every time, and its shape is what matters. Ask about the onset, the frequency, and the duration. Ask about the quality, the location, and the severity. Ask specifically about the temporal pattern: is it progressive, is it morning or nocturnal, is it positional. Ask what aggravates it, coughing, straining, or bending, and what relieves it. Ask about the associated features, vomiting, visual change, and any neurological deficit. Ask about the impact on school and activity, the sleep, and, crucially, the change over time. [1] [11]
Investigations
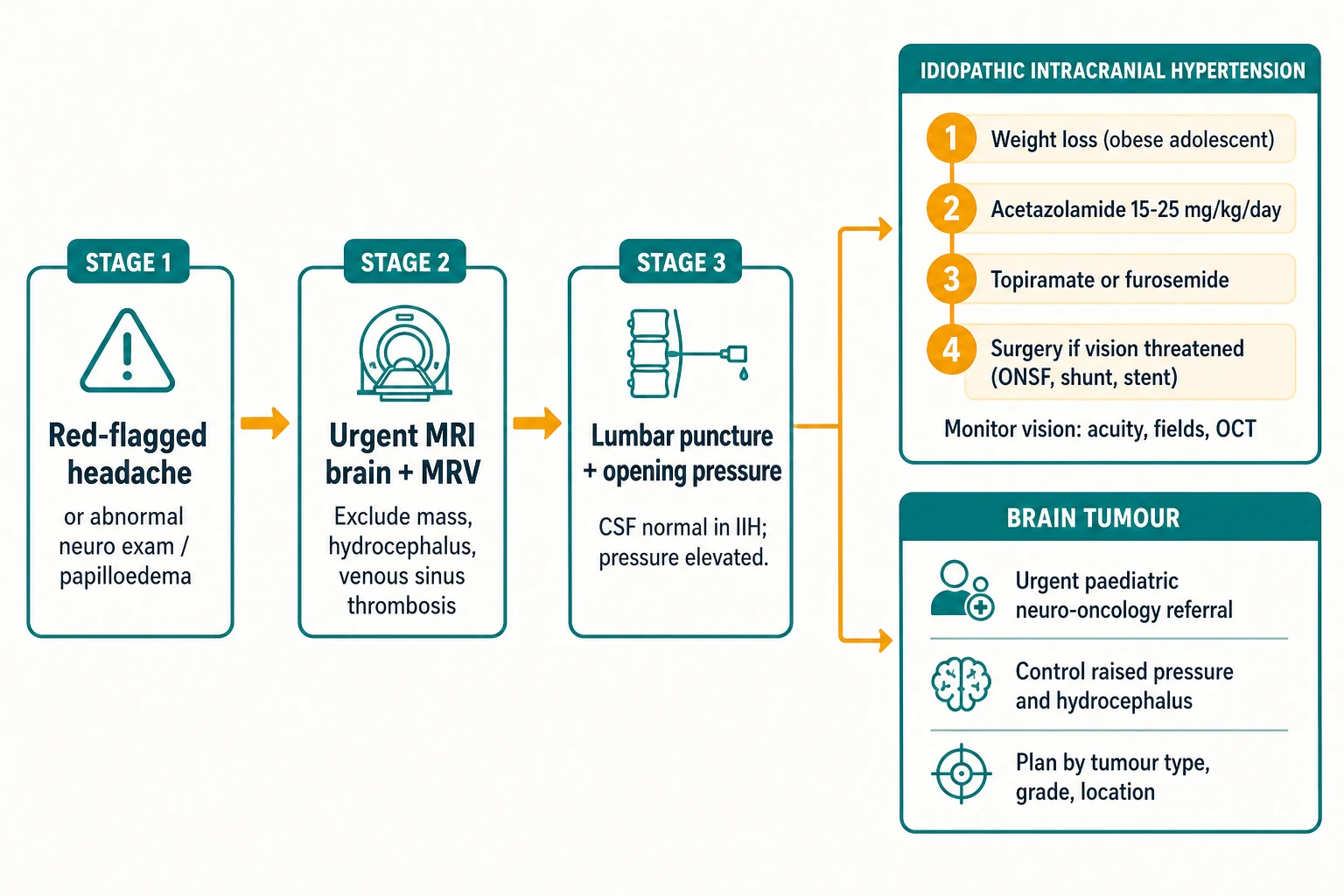
Neuroimaging is indicated for any headache with a red flag, and the modality matters. Magnetic resonance imaging is preferred for the elective evaluation of a suspected mass, hydrocephalus, or idiopathic intracranial hypertension. Magnetic resonance venography is added when intracranial hypertension is suspected, to exclude a venous sinus thrombosis. Computed tomography is reserved for the emergency setting or when magnetic resonance imaging is unavailable, because it is less sensitive for a posterior fossa tumour and it delivers radiation. [1] [5]
A child with suspected raised pressure or idiopathic intracranial hypertension needs a defined work-up once imaging has excluded a mass. The work-up is magnetic resonance imaging of the brain with venography, formal ophthalmology assessment of the visual acuity, the visual fields by perimetry, and the optic nerves by optical coherence tomography, and then a lumbar puncture with a measured opening pressure. The lumbar puncture is both diagnostic and therapeutic, and it is performed only after imaging has excluded a mass or obstructive hydrocephalus. [5] [6]
The cerebrospinal-fluid opening pressure is the measurement that confirms the diagnosis, and it is read with the child relaxed in the lateral decubitus position. The Friedman 2013 revised criteria require an elevated opening pressure, quoted as greater than 250 millimetres of cerebrospinal fluid in adults. The paediatric threshold is debated and is best interpreted in context, with several authorities citing a value in the region of greater than 250 millimetres in a relaxed child; sedation and body habitus shift the interpretation, so the number is never read in isolation. [5] [6]
The cerebrospinal-fluid composition is the other half of the criteria, and it must be normal. A raised cell count, a raised protein, or a low glucose redirects the diagnosis away from idiopathic intracranial hypertension and toward infection, inflammation, or malignancy. A child with papilloedema and an abnormal fluid does not have idiopathic intracranial hypertension, and the search turns to the cause the fluid has revealed. [5]
Management — Resuscitation
Most children with headache are stable and need assessment rather than resuscitation. A small minority present with the immediate threats of raised intracranial pressure, and recognising them is a time-critical skill. The threats are a falling conscious level, the signs of impending herniation, and airway compromise. The herniation signs are the Cushing triad of hypertension with bradycardia and irregular respiration, a dilated pupil, and posturing, and any one of them is an emergency. [3]
A child with a posterior fossa tumour and obstructive hydrocephalus can decompensate within hours, because the obstruction converts a compensated pressure into an uncontrolled one. The immediate management is to elevate the head of the bed, to control the airway and ventilation targeting a normal carbon dioxide, and to refer urgently to neurosurgery for an external ventricular drain or a shunt. The definitive relief of the obstruction is neurosurgical, and the medical measures only buy time. [11] [10]
Idiopathic intracranial hypertension is usually a subacute problem, but it has a fulminant form that is a neuro-ophthalmological emergency. Rapidly progressive visual loss, severe papilloedema, and a short history mark the fulminant variant, and the threat is permanent blindness within days. The management is urgent intervention to lower the pressure and protect vision, which may mean surgery on the same admission rather than a trial of medication. [8] [7]
Management — Definitive & Stepwise
The definitive management of idiopathic intracranial hypertension proceeds in steps, and the goal that governs every step is the preservation of vision. The first step is weight loss for the obese adolescent, because weight reduction lowers intracranial pressure and is the only measure that addresses a root driver. The second step is acetazolamide as the first-line drug, which reduces cerebrospinal-fluid production. The third step adds an alternative such as topiramate or furosemide, and the fourth step is surgery for progressive visual loss or refractory headache. [7] [8]
The paediatric acetazolamide dose is approximately 15 to 25 milligrams per kilogram per day in divided doses, with a maximum in the order of 1 to 4 grams per day. Acetazolamide causes a metabolic acidosis through its carbonic anhydrase inhibition, and that acidosis may be symptomatic and may carry a hypokalaemia. The practical consequence is that serum bicarbonate and potassium are monitored during treatment, and the dose is adjusted or electrolytes are replaced when the acidosis becomes marked. [9]
Vision is the single most important outcome in idiopathic intracranial hypertension, and the structure of follow-up reflects that. The child is monitored with serial visual acuity, visual fields, and optical coherence tomography, and any decline drives escalation up the ladder. A clinician who treats the headache but does not monitor the vision has missed the point of the treatment, because the headache is tolerable and the visual loss is not. [8] [6]
The surgical options are reserved for progressive visual loss despite medical therapy or for refractory headache. Optic nerve sheath fenestration protects the threatened optic nerve directly. Cerebrospinal-fluid shunting, usually a ventriculoperitoneal shunt, lowers the pressure overall. Venous sinus stenting is considered where venous sinus stenosis is demonstrated and thought to drive the pressure. The choice depends on the dominant problem, the vision or the headache, and the local neurosurgical and neuro-ophthalmological expertise. [7]
The definitive management of a brain tumour begins the moment the imaging is seen. The child is referred promptly to the paediatric neuro-oncology service, the raised pressure and any hydrocephalus are addressed first, and the oncological plan, surgery, chemotherapy, and radiotherapy, is determined by the tumour type, grade, and location. Early attention to the pressure and the cerebrospinal-fluid flow prevents the deterioration that turns a treatable tumour into an emergency, and early referral to a coordinated service shortens the diagnostic interval. [11] [10]
Specific Subtypes & Scenarios
The pre-pubertal child with idiopathic intracranial hypertension breaks the classic phenotype. The child is often male and not obese, the headache may be less prominent, and the diagnosis is more easily missed because the phenotype does not flag it. The work-up is the same: exclude a secondary cause with imaging and venography, confirm the pressure with a lumbar puncture, and treat to protect the vision. [8]
The adolescent girl with idiopathic intracranial hypertension fits the classic phenotype: obese, post-pubertal, with daily headache, papilloedema, and visual symptoms. Weight loss and acetazolamide are the first-line measures, and venous sinus stenosis may contribute to the pressure and become a target for stenting in selected cases. The partnership with ophthalmology for serial visual surveillance is the backbone of the long-term plan. [7] [8]
[2]A child with a ventriculoperitoneal shunt and a headache is a shunt malfunction or infection until proved otherwise, and this is one of the highest-stakes scenarios in paediatrics. The assessment distinguishes a shunt-related emergency from an intercurrent viral illness, and the work-up centres on shunt-series imaging, a head computed tomography, and urgent neurosurgical review. The detailed mechanical and shunt-dependent pathway is owned by the hydrocephalus-and-shunt-emergencies leaf, which the clinician reaches for rather than reconstructing here. [11]
Complications & Pitfalls
The harms of a missed secondary headache are the reason the topic exists. A delayed tumour diagnosis shortens survival and increases morbidity from raised pressure. Untreated papilloedema causes permanent visual loss. A posterior fossa lesion with obstructive hydrocephalus can herniate and kill. Behind each of these is a clinician who applied a reassuring label to a dangerous headache, and the medicolegal and human costs are the measure of the failure. [3] [10]
The single most common error is reassuring on a progressive or morning headache with vomiting in a young child. The error rests on the belief that headache alone is an early sign of a tumour; it is not, it is a late sign, and the absence of focal signs does not exclude one. The case-control evidence is blunt about this: the features that distinguish a brain neoplasm from a primary headache are morning headache, vomiting, visual symptoms, an abnormal examination, and the absence of a family history of migraine, and several together should override a normal early scan or a reassuring pattern. [12] [11]
The diagnostic pitfalls of idiopathic intracranial hypertension are four, and a candidate who names them at viva shows they have held the syndrome. The first is overcalling pseudopapilloedema, drusen and tilted discs, as papilloedema. The second is missing a venous sinus thrombosis by omitting the venography. The third is performing a lumbar puncture before excluding a mass. The fourth is under-treating because the visual threat was not monitored. Each error is preventable by following the criteria and the work-up in order. [6] [5]
The treatment pitfall is acetazolamide's metabolic acidosis. The acidosis is a direct effect of carbonic anhydrase inhibition, it may carry a hypokalaemia, and it can be symptomatic enough to limit the dose. The practical answer is to monitor the serum bicarbonate and potassium, to replace the electrolytes, and to adjust the dose, so that the drug that protects the vision is not abandoned for a preventable side effect. [9]
Prognosis & Disposition
The prognosis of a primary headache with a normal examination is excellent, and the task at the first consultation is diagnosis, safety-netting, and a primary-headache plan. A headache diary, a clear explanation, and a return precaution for any red flag are the tools that keep the child safe without exposing them to imaging they do not need. [1]
The prognosis of idiopathic intracranial hypertension is generally good for the headache, but it is dominated by the risk to vision. The risk of permanent visual loss is highest with fulminant disease, with severe papilloedema at presentation, and with poor adherence or loss to follow-up. The structure of care, the serial visual surveillance, exists precisely because the headache improves while the vision can silently decline. [8] [6]
The prognosis of a childhood brain tumour is determined by the tumour type, the grade, the extent of resection, and the molecular markers, and the details belong to the neuro-oncology leaf. What is within the general paediatrician's control is the diagnostic interval: a shorter interval reduces the morbidity from raised pressure and hydrocephalus, and early recognition of the symptom cluster is the single most effective intervention available before the child reaches the oncology service. [10]
The disposition is shared care. A low-risk primary headache returns to the general paediatrician or primary care with a headache diary and safety-netting. A confirmed or suspected secondary cause is referred urgently to paediatric neurology, neurosurgery, or neuro-oncology, with the raised pressure addressed first. Idiopathic intracranial hypertension is co-managed with ophthalmology for serial visual surveillance, and the general paediatrician often coordinates the weight-management, the adherence, and the long-term follow-up. [11] [8]
Special Populations
The infant and the very young child cannot give the headache history that an older child can, and the signs of raised pressure are different. The clinician looks for vomiting, irritability, lethargy, a bulging fontanelle, and an increasing head circumference, and the threshold for imaging is lower because the open sutures may mask the pressure. A macrocephalic, vomiting infant is imaged, not watched. [2]
The child with a ventriculoperitoneal shunt, established hydrocephalus, or a known tumour is a high-stakes special population. Any new or changed headache in these children is a complication of the underlying condition until excluded, and the work-up begins with shunt-series imaging and neurosurgical review. The general paediatrician's role is to treat the headache as a shunt or tumour emergency first and an intercurrent illness second. [11]
[2]Equity matters in a time-critical condition. Indigenous, Maori, and Pacific children, and children from migrant, refugee, and socioeconomically disadvantaged backgrounds, face real barriers to timely imaging and specialist review. A delayed scan in a child with a posterior fossa tumour is the same disease with a worse outcome, and equitable access to diagnosis and treatment is part of the standard of care, not an add-on. The HeadSmart lesson, that professional and public awareness shortens the diagnostic interval, applies across all the populations a service sees. [11] [10]
Evidence, Guidelines & Regional Differences
The evidence base for this topic is anchored by a small set of documents that a candidate should be able to name. The American Academy of Neurology 2002 practice parameter on the evaluation of recurrent headaches in children set the framework for the red-flag screen and the selective use of imaging. The Friedman 2013 revised diagnostic criteria for the pseudotumour cerebri syndrome remain the standard definition of idiopathic intracranial hypertension in adults and children. The Wilne 2007 systematic review and the 2010 HeadSmart guideline defined the brain tumour symptom cluster and drove the public-health campaign that shortened the diagnostic interval in the United Kingdom. [1] [5] [10] [11]
Australian and New Zealand practice follows the same red-flag framework. Magnetic resonance imaging is preferred for the elective work-up, venography is added when intracranial hypertension is suspected, and acetazolamide is the first-line medical therapy for idiopathic intracranial hypertension with surgery reserved for threatened vision. The regional neuro-ophthalmology and neurosurgery pathways are well established in the tertiary centres, and the general paediatrician's task is to recognise the red flag and refer early. [7] [8]
The persistent controversies are few but real, and naming them shows depth. The paediatric cerebrospinal-fluid opening-pressure threshold is debated, with several authorities citing a value in the region of greater than 250 millimetres in a relaxed child and acknowledging the effect of sedation and body habitus. The role of repeated lumbar puncture is contested. The contribution of venous sinus stenosis, and the place of stenting, continues to be refined in selected centres. The optimal imaging strategy for the genuinely low-risk headache is settled in favour of clinical follow-up over scanning. [5] [6]
The HeadSmart campaign in the United Kingdom demonstrated that raising professional and public awareness of the symptom cluster shortens the symptomatic interval to diagnosis of a childhood brain tumour. Comparable awareness strategies underpin the Australian and New Zealand approach, and the general paediatrician is the key node in that chain, because they are the first clinician the parent brings the child to. [11] [10]
Exam Pearls
The cardinal rule, and the one a candidate must say aloud, is that a progressive, morning, or vomiting headache in a young child is a brain tumour until imaging proves otherwise. The corollary is that headache alone is a late and unreliable sign, so the absence of a focal deficit does not make a progressive headache safe. These two sentences are the spine of the topic and the most common reason a fellowship candidate is failed on a headache viva. [12] [11]
The Friedman 2013 criteria for idiopathic intracranial hypertension are a viva staple and must be reproduced exactly: papilloedema with a normal neurological examination allowing a sixth-nerve palsy, normal magnetic resonance imaging of the brain and venography excluding a mass, hydrocephalus, and venous sinus thrombosis, normal cerebrospinal-fluid composition, and an elevated opening pressure, quoted as greater than 250 millimetres of cerebrospinal fluid in adults with the paediatric threshold debated. A candidate who omits the venography or the fluid composition has not given the criteria. [5] [6]
The high-yield management points close the topic. Acetazolamide at approximately 15 to 25 milligrams per kilogram per day, with bicarbonate and potassium monitoring. Weight loss for the obese adolescent. Serial visual surveillance as the chief outcome, because the vision can decline while the headache improves. Surgery, optic nerve sheath fenestration, shunt, or stent, for progressive visual loss. And for the brain tumour, urgent neuro-oncology referral with the raised pressure and hydrocephalus addressed first. [7] [9] [8]
References
- [1]Lewis DW; Ashwal S; Dahl G; et al Practice parameter: evaluation of children and adolescents with recurrent headaches: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society Neurology, 2002.PMID 12196640
- [2]Langdon R; DiSabella MT Pediatric Headache: An Overview Curr Probl Pediatr Adolesc Health Care, 2017.PMID 28366491
- [3]Yonker M Secondary Headaches in Children and Adolescents: What Not to Miss Curr Neurol Neurosci Rep, 2018.PMID 30058035
- [4]Park EG; Yoo IH The diagnostic values of red flags in pediatric patients with headache Brain Dev, 2022.PMID 35568652
- [5]Friedman DI; Liu GT; Digre KB Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children Neurology, 2013.PMID 23966248
- [6]Inger HE; Rogers DL; McGregor ML; et al Diagnostic criteria in pediatric intracranial hypertension J AAPOS, 2017.PMID 29081363
- [7]Raoof N; Hoffmann J Diagnosis and treatment of idiopathic intracranial hypertension Cephalalgia, 2021.PMID 33631966
- [8]Gaier ED; Heidary G Pediatric Idiopathic Intracranial Hypertension Semin Neurol, 2019.PMID 31847041
- [9]Bulkowstein Y; Nitzan-Luques A; Schnapp A; et al The manifestations of metabolic acidosis during acetazolamide treatment in a cohort of pediatric idiopathic intracranial hypertension Pediatr Nephrol, 2024.PMID 37480382
- [10]Wilne S; Collier J; Kennedy C; et al Presentation of childhood CNS tumours: a systematic review and meta-analysis Lancet Oncol, 2007.PMID 17644483
- [11]Wilne S; Koller K; Collier J; et al The diagnosis of brain tumours in children: a guideline to assist healthcare professionals in the assessment of children who may have a brain tumour Arch Dis Child, 2010.PMID 20371594
- [12]Sheridan DC; Waites B; Lezak B; et al Clinical Factors Associated With Pediatric Brain Neoplasms Versus Primary Headache: A Case-Control Analysis Pediatr Emerg Care, 2020.PMID 29135901