Paeds · neurology-neurodisability-and-neuromuscular
Sleep disorders with neurological disease
Also known as Paediatric sleep disorders · Sleep disturbance in neurodisability · Sleep-disordered breathing in cerebral palsy · Narcolepsy in childhood · Restless legs syndrome in children · Parasomnias in children
Fellowship guide to sleep disorders with neurological disease: the four-cluster framework of dyssomnias, sleep-disordered breathing, parasomnias, and sleep-related movement disorders, the bidirectional mechanism linking sleep to seizures, cognition, behaviour, and tone, the high-yield case-finding history and validated questionnaires, the targeted investigation pathway from polysomnography to the multiple sleep latency test and cerebrospinal fluid orexin, the stepped management built on sleep hygiene and behavioural therapy with melatonin, iron, airway support, and ventilation, and the evidence base for melatonin in autism and intravenous ferric carboxymaltose in restless legs syndrome.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old with severe cerebral palsy who is brought in because he sleeps poorly, snores loudly, and has become harder to manage by day, and whose parents assume the restlessness is just part of his condition. That child carries the whole teaching point of paediatric sleep in neurology: the sleep problem is real, it is caused by the hypotonic airway of his cerebral palsy, and treating it will improve not only his nights but also his daytime tone, his seizures, and his family's exhausted quality of life. The clinician who grasps this treats the sleep and the neurology as one, rather than dismissing the nights as an unchangeable feature of the diagnosis. [7] [8]
A sleep disorder, in this context, is any disturbance of sleep onset, maintenance, architecture, or breathing that is either caused by the underlying neurological disease or so closely entwined with it that the two must be managed together. The definition matters because it directs the clinician away from two common errors, attributing all sleep disturbance to behaviour and prescribing a sedative, and attributing it all to the neurological disease and giving up. Most sleep disturbance in children with neurological disease has a specific, treatable driver, whether that driver is an obstructed airway, an iron-deficient restless leg, an overconsolidated epilepsy, or a disrupted circadian rhythm. [10]
The unifying mechanism, and the idea that earns the most marks at viva, is that the relationship is bidirectional. The brain generates and gates sleep through the hypothalamic orexin neurons, the suprachiasmatic circadian pacemaker, and the brainstem REM-atonia circuit, and neurological disease attacks these systems. In the other direction, fragmented and hypoxic sleep feeds back to lower the seizure threshold, impair learning and memory consolidation, magnify the behavioural dysregulation of autism and attention-deficit or hyperactivity disorder, and increase spasticity. Treating sleep is therefore not a comfort measure but a direct treatment of the neurological condition. [1] [9]
Classification
Classifying a child's sleep disorder answers one question: which sleep system has failed, the one that governs how much sleep the child gets, the one that keeps the airway and breathing drive working, the one that separates the sleep states cleanly, or the one that suppresses movement in sleep. The answer places the child in one of four clusters, and each cluster carries a distinct presentation, investigation, and treatment, which is why the classification is worth memorising rather than dismissed as taxonomy. [10]
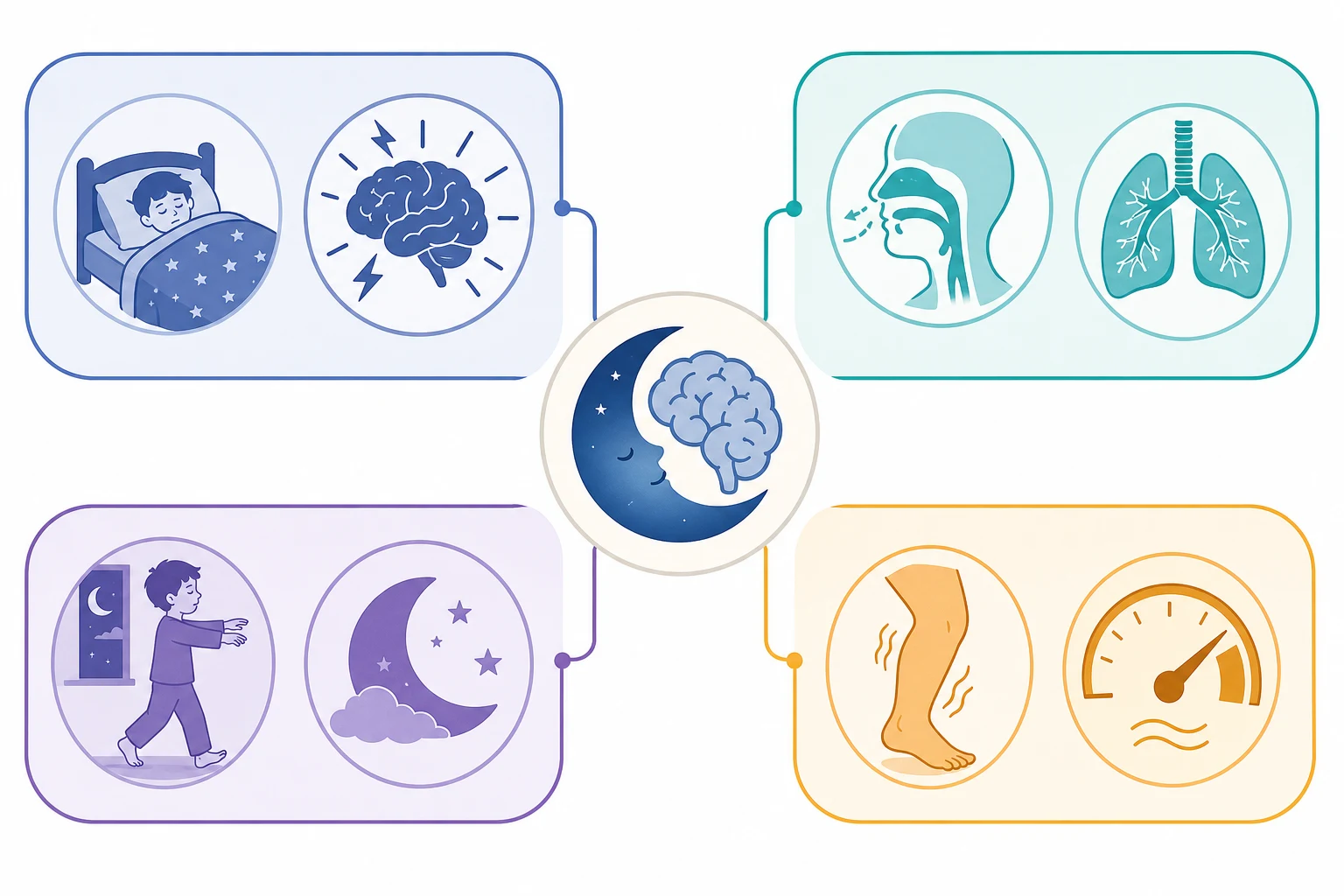
The dyssomnias are the disorders in which the child cannot get enough sleep, or cannot stay awake when they need to. Narcolepsy type 1, the loss of orexin neurons, is the prototypical dyssomnia of neurology, presenting with irresistible daytime sleep and cataplexy. Idiopathic hypersomnia shares the daytime sleepiness without cataplexy. Chronic insomnia of the neurodevelopmental disorders, the bedtime resistance and night-waking of autism and attention-deficit or hyperactivity disorder, is the commonest dyssomnia in practice and the one most amenable to behavioural therapy. [1] [9]
Dyssomnias
not enough sleep
- Narcolepsy type 1: orexin loss, cataplexy, daytime sleep
- Idiopathic hypersomnia: sleepiness without cataplexy
- Chronic insomnia of autism and ADHD
- Circadian phase delay of adolescence
- Investigate with multiple sleep latency test
Sleep-disordered breathing
airway or drive fails
- Obstructive sleep apnoea of cerebral palsy and Down syndrome
- Central apnoea of brainstem malformation
- Nocturnal hypoventilation of neuromuscular disease
- Driven by hypotonia, adenotonsillar hypertrophy, scoliosis
- Investigate with polysomnography and oximetry
Parasomnias
state transition misfires
- Disorders of arousal: sleepwalking, sleep terrors
- Confusional arousals in the first third of the night
- REM parasomnias and nightmare disorder
- Often amplified by fragmented slow-wave sleep
- Distinguish from nocturnal frontal lobe epilepsy
Sleep-related movement disorders
motor programmes intrude
- Restless legs syndrome: urge to move, relieved by movement
- Periodic limb movement disorder: repetitive leg jerks in sleep
- Driven by iron deficiency, low ferritin
- Responds to oral or intravenous iron
- Periodic limb movement index quantifies on polysomnography
The distinction that most often changes management is between the sleep-related breathing disorders and the rest, because a child with cerebral palsy and obstructive sleep apnoea needs airway and ventilatory support rather than a melatonin tablet, and missing the distinction allows a treatable cause of pulmonary hypertension and neurocognitive decline to persist. The other high-yield distinction is between a parasomnia and nocturnal frontal lobe epilepsy, because the two look similar to a frightened parent but are managed very differently, and the discriminator, stereotyped brief events against variable long events, determines whether the child gets an electroencephalogram or a safety plan. [10] [7]
Epidemiology & Risk Factors
Sleep disturbance is the rule, not the exception, in children with neurological disease, and stating its prevalence to a family is itself therapeutic, because it reframes a private struggle as a recognised and treatable problem. The meta-analysis by Wang and colleagues found sleep disorders in roughly 40 to 80 per cent of children and adolescents with autism spectrum disorder. This is far above the 25 to 40 per cent of typically developing children. It means that a sleep problem is the expected finding, not the exception, in an autism clinic. [9]
Children with epilepsy carry two to three times the rate of sleep disturbance of children without epilepsy, driven by the bidirectional link between sleep and seizures, by nocturnal seizures that fragment sleep, and by antiseizure medicines that alter sleep architecture. Children with cerebral palsy have a high prevalence of sleep-disordered breathing that rises with the severity of motor impairment, so that a child at Gross Motor Function Classification System level four or five, with oromotor dysfunction and scoliosis, is the child most likely to desaturate and hypoventilate at night. [7] [8]
The numbers that anchor your viva
The risk factors divide into those that are fixed and those that are modifiable, and the modifiable ones are where the clinician intervenes. The fixed drivers are the underlying neurological disease itself, its severity, and the genetic predisposition, such as the strong link of narcolepsy to the HLA-DQB1 star 06 colon 02 allele. The modifiable drivers are iron deficiency for restless legs syndrome, adenotonsillar hypertrophy and hypotonia for obstructive sleep apnoea, and unstructured routines, late screen exposure, and caffeine for behavioural insomnia, and addressing these three often resolves the disorder before any drug or device is needed. [5] [7]
Pathophysiology
To understand why a neurological disease disturbs sleep, and why disturbed sleep in turn worsens the disease, it helps to picture the brain as a small set of connected clocks and switches that build the state of sleep and hold it stable through the night. Three systems do most of the work, and each can fail in a recognisable way. The hypothalamic orexin neurons stabilise wakefulness, the suprachiasmatic nucleus times sleep to the light-dark cycle, and the brainstem and subcortical circuits produce the muscle atonia of REM sleep and the slow oscillation of non-REM sleep. [1]
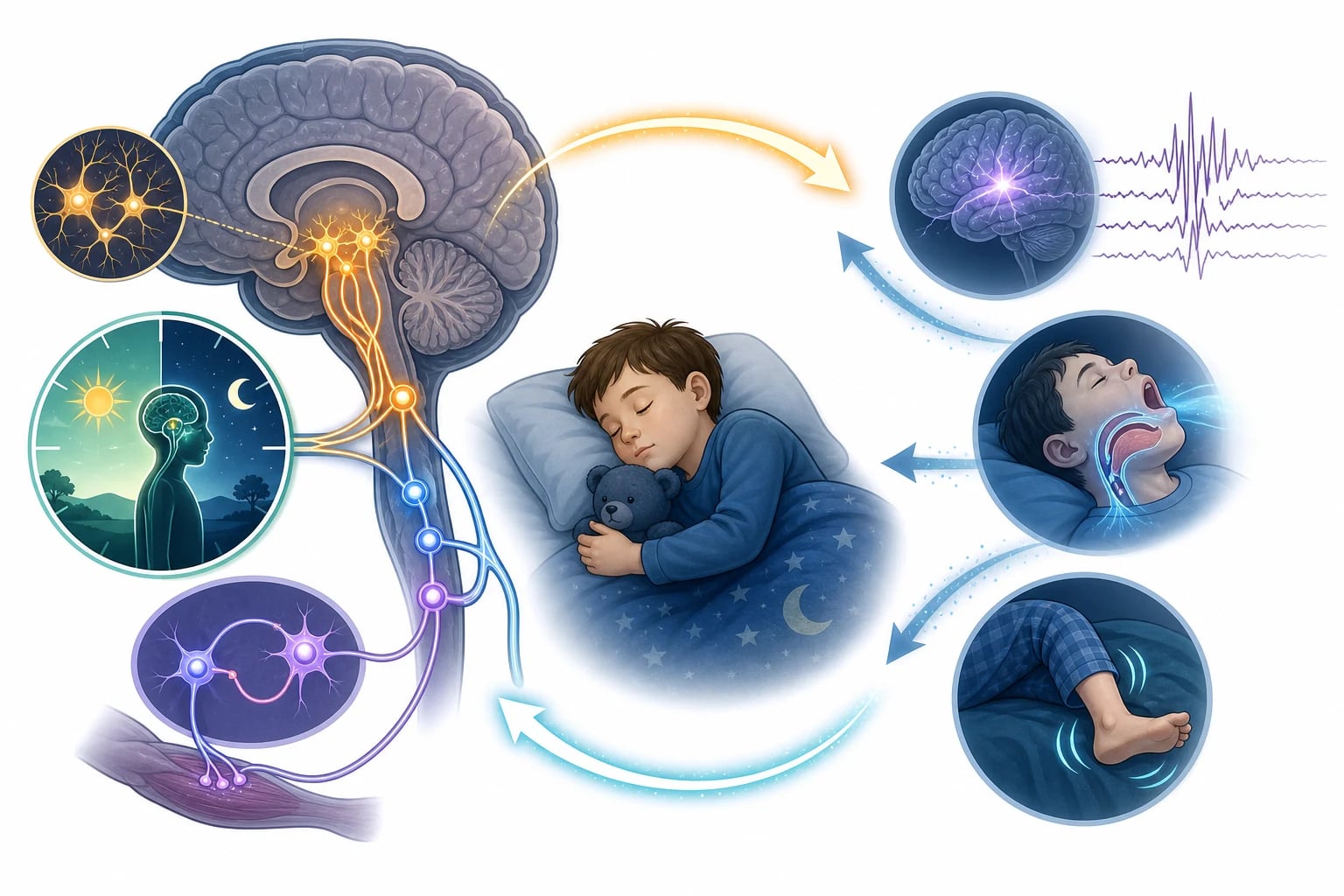
When the orexin neurons are lost, as in narcolepsy type 1, the brain can no longer hold a stable wake state. The child is overcome by irresistible sleep in the day. The brain can also no longer gate REM sleep to the night. REM phenomena intrude into wakefulness as cataplexy, the sudden emotion-triggered loss of muscle tone with preserved consciousness, and as sleep paralysis and vivid hypnagogic hallucinations. The loss is measurable, because cerebrospinal fluid orexin falls below 110 picograms per millilitre, and it is now directly treatable, because orexin receptor 2 agonists replace the missing signal. [1] [12]
[1] [12]The other half of the mechanism is the feedback loop, and it is the half that matters most for the neurodisability clinic. Fragmented and hypoxic sleep lowers the seizure threshold, so the child with poorly controlled epilepsy sleeps worse and seizes more in a vicious cycle. It impairs the synaptic consolidation that turns the day's learning into memory, so the child with autism who sleeps poorly falls further behind. It magnifies behavioural dysregulation, so the inattentive or hyperactive child becomes more so. And it increases spasticity and daytime tone, so the child with cerebral palsy becomes stiffer. Treating the sleep, by whichever route fits the cluster, breaks each of these loops and is a direct treatment of the neurological condition. [9] [7]
Clinical Presentation
The presentation depends on which sleep system has failed, and because families rarely volunteer the detail, the clinician must ask explicitly. The hypersomnolent child is the narcolepsy presentation. This is a previously well school-aged child with months of irresistible daytime sleep, falling asleep in class or at the table. There is often a sudden loss of muscle tone triggered by laughter or surprise, the cataplexy that confirms narcolepsy type 1. Sometimes there are frightening vivid hallucinations at sleep onset and a brief inability to move on waking. [1]
The snoring child is the sleep-disordered breathing presentation, and in a child with cerebral palsy, Down syndrome, or neuromuscular disease the snoring, restless sleep, mouth-breathing, witnessed pauses, morning headache, and daytime fatigue or behavioural dysregulation point to obstructive sleep apnoea or nocturnal hypoventilation. The restless child is the restless legs presentation, describing an urge to move the legs in the evenings that is relieved by movement, with bedtime resistance, and often a family history of the same. The parasomnia child has confusional arousals, sleepwalking, or sleep terrors in the first third of the night, with no memory of the event, and the child with sleep-related epilepsy has stereotyped nocturnal events that may occur several times a night. [5] [7]
| Night-time picture | What it implies | Act |
|---|
The red flags that demand urgent escalation, rather than routine outpatient review, are three. The first is cataplexy, which makes narcolepsy type 1 likely and changes the investigation pathway. The second is severe symptomatic nocturnal hypoventilation with morning headache or daytime hypercapnic sleepiness, which risks progression to respiratory failure. The third is any nocturnal event that might be a nocturnal frontal lobe seizure rather than a parasomnia, because the two are managed so differently. The family that films the event on a smartphone gives the clinician the single most useful piece of evidence, and asking for that video is part of the assessment. [1] [7]
Differential Diagnosis
The differential turns on one question: is this a primary sleep disorder, or is the sleep disturbance secondary to the neurological disease, a medication, or a mimic? The answer changes the management entirely, because a primary disorder is treated in its own right while a secondary one is treated by addressing the cause. Behavioural insomnia of childhood and circadian phase delay can look like hypersomnia or chronic insomnia but reflect unstructured routines and late screen exposure rather than neurological disease, and they respond to behavioural measures rather than to a drug. [9]
Sleep-disordered breathing from adenotonsillar hypertrophy mimics restless legs syndrome through fragmented sleep and bedtime resistance, so it must be excluded before attributing restless legs, and the discriminator is that restless legs has the characteristic urge-to-move relieved by movement and a low ferritin, while obstruction has snoring and witnessed pauses. Nocturnal frontal lobe epilepsy is the great mimic of the disorders of arousal, and it is the mimic that matters most because missing it leaves epilepsy untreated. The discriminator examiners reward is that seizures are stereotyped and brief and may occur in any sleep stage, while parasomnias are variable and long and confined to slow-wave sleep in the first third of the night. [10]
Primary sleep disorder
- Narcolepsy, restless legs, idiopathic hypersomnia
- Disorder-specific investigation and treatment
- Cataplexy is pathognomonic for narcolepsy type 1
- Low ferritin supports restless legs
- Not explained by the neurological disease alone
Secondary to the disease
- Obstructive sleep apnoea of cerebral palsy hypotonia
- Nocturnal hypoventilation of neuromuscular disease
- Insomnia of autism and intellectual disability
- Sleep fragmentation from nocturnal seizures
- Treat the driver, not the symptom
Medication effect
- Stimulants fragment sleep and delay onset
- Antipsychotics and antidepressants alter sleep architecture
- Sedating antiseizure medicines disrupt cycles
- Corticosteroids cause insomnia
- Review the drug list before adding a sedative
Mimic
- Behavioural insomnia from unstructured routines
- Circadian phase delay from late screen exposure
- Nocturnal frontal lobe epilepsy mimics parasomnia
- Depression and anxiety as insomnia and early waking
- Pain, reflux, and constipation disrupting sleep
The obstructive sleep apnoea of hypotonia in cerebral palsy differs from the central apnoea of a brainstem malformation in a way that changes management. Obstructive events have paradoxical respiratory effort as the child tries to breathe against a closed airway. Central events show no effort at all as the respiratory drive fails. The first is treated by opening the airway, with adenotonsillectomy or continuous positive airway pressure, while the second is treated by supporting the drive, with bilevel or volume-assured ventilation. Polysomnography distinguishes the two and prevents the error of treating a drive failure as an obstruction or vice versa. [7] [11]
Clinical & Bedside Assessment
Assessment rests on a structured sleep history, a validated questionnaire, and a focused examination, and the single most useful tool is the two-week sleep diary, because it converts a vague parental concern into an objective pattern of onset, waking, and duration. Ask separately about each phase of the night, bedtime resistance and sleep latency, night wakings and their triggers, total sleep duration, morning waking and morning mood, and daytime sleepiness, and ask specifically about snoring and witnessed pauses, abnormal movements or behaviours in sleep, and any impact on daytime function, behaviour, and seizures. [9] [10]
The validated questionnaires do the screening work that a busy clinic cannot do from open questions alone. The Sleep Disturbance Scale for Children and the Pediatric Sleep Questionnaire screen for the common disorders. These include the disorders of initiating and maintaining sleep, the sleep-related breathing disorders, the disorders of arousal, and the sleep-related movement disorders. They also track the response to treatment over time, so a clinician can see whether the iron or the melatonin is working. [9]
The examination targets the drivers of each cluster rather than being a general screen. Look at growth and adenotonsillar size for obstructive sleep apnoea, because a large child with big tonsils and a hypotonic airway is the one who obstructs. Map the oromotor function and the tone distribution for cerebral palsy, because the child with severe oromotor weakness and a Gross Motor Function Classification System level four or five is the one who hypoventilates. Assess muscle bulk and strength for neuromuscular disease, and build a developmental and behavioural profile for autism and attention-deficit or hyperactivity disorder, because the behavioural phenotype shapes which behavioural therapy will work. [7] [8]
Cataplexy deserves a separate sentence because it is pathognomonic and often missed. It is the sudden, bilateral loss of muscle tone triggered by strong emotion, usually laughter, with consciousness preserved, and its presence in a sleepy child makes narcolepsy type 1 so likely that it removes the need for a diagnostic lumbar puncture in many cases, because the cerebrospinal fluid orexin will be low. Asking the family to film the episodes and to describe exactly what happens when the child laughs hard is how the clinician catches it. [1]
Investigations
Investigation is targeted, not blanket, and the choice of test follows the suspected disorder, because a polysomnogram performed for the wrong reason wastes a scarce resource and answers the wrong question. Polysomnography, the multichannel overnight study scored by the American Academy of Sleep Medicine rules, is the gold standard for sleep-disordered breathing, for periodic limb movement disorder, and for the parasomnias. It quantifies the apnoea-hypopnoea index, the number of obstructive and central events per hour, the periodic limb movement index, and the architecture of sleep, and it is the test that turns a suspicion into a number that can be tracked. [11]
The thresholds that decide the test
For narcolepsy, the multiple sleep latency test is the key investigation, performed the day after an overnight polysomnogram that excludes other causes of sleepiness. A mean sleep latency of eight minutes or less with two or more sleep-onset REM periods confirms a central disorder of hypersomnolence, and when cataplexy is present this is narcolepsy type 1. When the cataplexy is absent or the picture is ambiguous, cerebrospinal fluid orexin below 110 picograms per millilitre is the definitive biomarker that distinguishes narcolepsy type 1 from type 2 and from idiopathic hypersomnia. [1]
For the technology-dependent child with neuromuscular disease or severe cerebral palsy, overnight pulse oximetry with capnography screens for nocturnal hypoventilation and guides the threshold for non-invasive ventilation, because a rising carbon dioxide through the night, with intermittent desaturation, is the pattern that precedes daytime respiratory failure. For restless legs syndrome, a serum ferritin below 50 micrograms per litre supports the diagnosis and predicts response to iron. For the ambiguous nocturnal event, video-electroencephalography, ideally performed in the sleep laboratory, distinguishes nocturnal frontal lobe epilepsy from a parasomnia. For the circadian rhythm disorders, where polysomnography is not warranted, actigraphy over one to two weeks objectifies the shifted sleep phase that the diary describes. [5] [7] [4]
Management — Resuscitation
Sleep disorders are rarely a resuscitation emergency, but two situations carry acute harm and demand urgent action rather than a routine outpatient appointment. The first is severe symptomatic nocturnal hypoventilation in a child with neuromuscular disease or severe cerebral palsy, who presents with morning headache, daytime sleepiness, morning confusion, or the signs of cor pulmonale. This child needs urgent respiratory and sleep review for non-invasive ventilation, because untreated chronic hypoventilation progresses steadily to daytime respiratory failure and is a preventable cause of death in neuromuscular disease. [7]
[7]The second urgent situation is the child whose sleep is being destroyed by frequent nocturnal seizures or by a status event, in whom the sleep disturbance is a symptom of uncontrolled epilepsy. Here the immediate task is epilepsy optimisation alongside the sleep assessment, because no sleep plan will work while nocturnal seizures fragment the night every hour, and the sleep service and the epilepsy service must act in parallel. [10]
The immediate tasks in the non-emergency clinic, the ones that make a difference at the first visit, are three. Make the child safe overnight by putting safety measures in place for a sleepwalker. Identify and treat the modifiable drivers such as iron deficiency and adenotonsillar hypertrophy. Remove sleep-destroying medications where possible. It is worth stating plainly that stimulants, antipsychotics, and several antiseizure medicines all disturb sleep architecture, so a careful medication review is part of the resuscitation of the exhausted child, because adding a sedative on top of a sleep-destroying drug is a common and avoidable error. [9]
Management — Definitive & Stepwise
Definitive management is stepped and built on three layers, and the order matters because each layer depends on the one beneath it. The foundation for every child is sleep hygiene and behavioural therapy, a consistent bedtime routine, a regular rise time, removal of screens and caffeine from the evening, and, for the behavioural insomnia of the neurodevelopmental disorders, graduated extinction and sleep scheduling. This layer alone resolves a large fraction of chronic insomnia, which is why it must never be skipped in favour of a drug, and why a family asked to start melatonin must first have the routine in place. [9] [10]
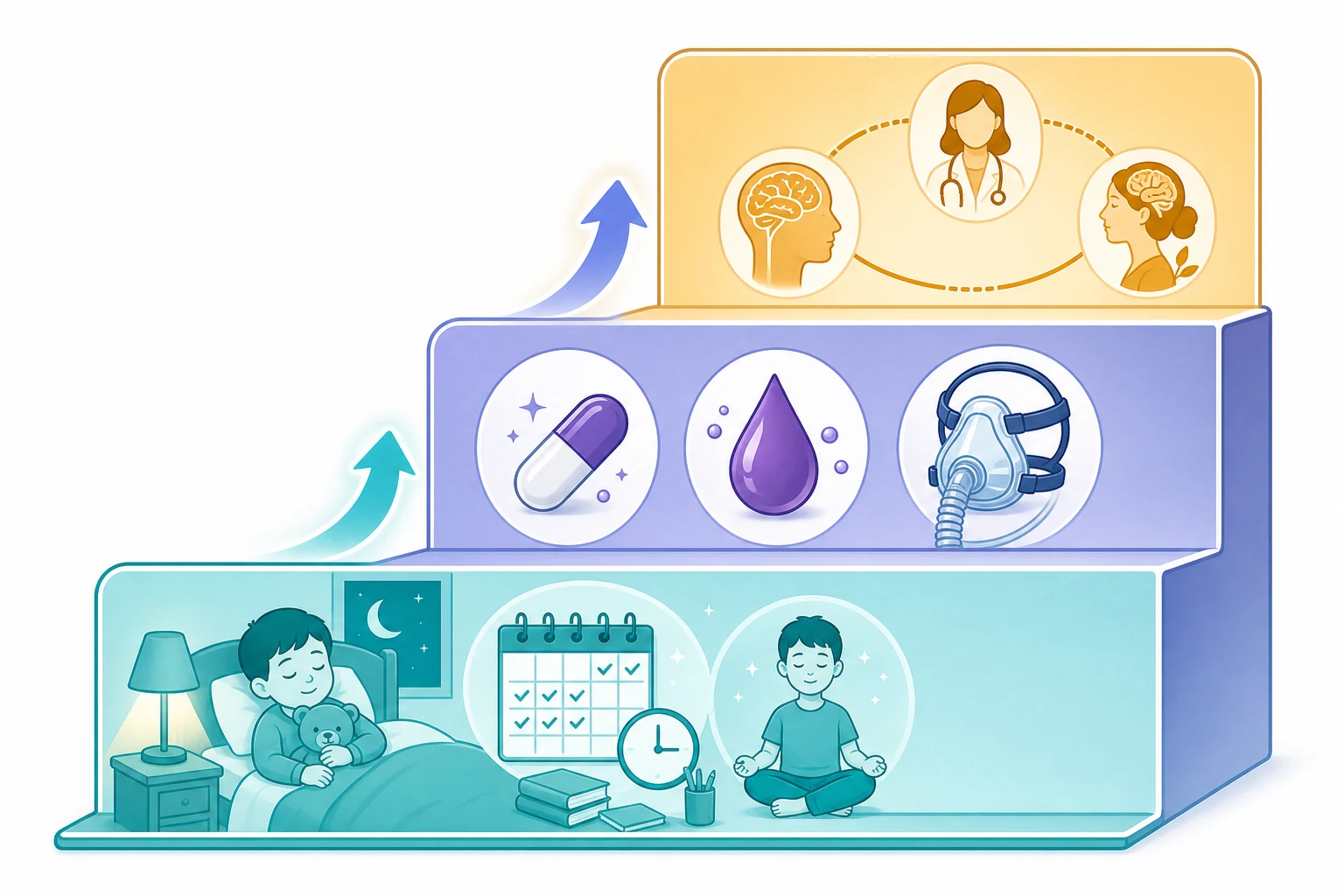
The second layer adds the targeted treatment that fits the cluster. Prolonged-release melatonin is the second-line agent for chronic sleep-onset insomnia of autism after behavioural measures have been optimised, and the Gringras trial established it as effective and safe, shortening sleep latency and lengthening total sleep, with the long-term Maras extension confirming sustained benefit. Iron supplementation, oral first then intravenous, treats restless legs syndrome with low ferritin, and the DelRosso trial established intravenous ferric carboxymaltose as effective when oral iron fails or is not tolerated. Adenotonsillectomy or continuous positive airway pressure treats obstructive sleep apnoea of cerebral palsy, and non-invasive ventilation treats the nocturnal hypoventilation of neuromuscular disease. [2] [3] [5]
The stepped ladder in one glance
Foundation for every child: consistent bedtime routine, regular rise time, no screens or caffeine in the evening, and behavioural therapy such as graduated extinction for behavioural insomnia
Targeted treatment by cluster: prolonged-release melatonin for insomnia of autism, iron for restless legs with low ferritin, adenotonsillectomy or CPAP for obstructive sleep apnoea, and non-invasive ventilation for nocturnal hypoventilation
Specialist pharmacotherapy for the refractory few: wake-promoting agents and sodium oxybate for narcolepsy, orexin receptor 2 agonists for narcolepsy type 1, and scheduled awakenings with safety measures for dangerous parasomnias
Parallel optimisation of the neurological condition: control the seizures, treat the reflux and constipation, manage the tone, and review the drug list for sleep-destroying medicines
The third layer is specialist pharmacotherapy for the disorders that do not respond to the first two layers. Narcolepsy type 1 is managed with scheduled naps, wake-promoting agents, and sodium oxybate for cataplexy, and the orexin receptor 2 agonists now offer a mechanism-targeted option that replaces the missing orexin signal directly. The dangerous parasomnias, in which a sleepwalking child is at risk of injury, are managed by safety measures such as alarms and window locks, by scheduled anticipated waking at the usual event time, and by treating any trigger such as obstructive sleep apnoea that fragments slow-wave sleep and amplifies the parasomnia. [1] [12]
Throughout the ladder, the comorbid neurological condition must be optimised in parallel, because uncontrolled epilepsy, untreated gastro-oesophageal reflux, constipation, and pain will defeat any sleep plan, and a child whose nights are broken by seizures or reflux will not settle however perfect the routine. The practical test of a good sleep plan is that it treats the sleep and the neurology together, and it is reviewed against the sleep diary and the validated questionnaire at every visit so that the clinician can see whether each layer is working. [9] [10]
Specific Subtypes & Scenarios
Each subtype carries a distinct decision, and the fellowship candidate is expected to handle each on its own. Narcolepsy type 1, the orexin-deficient syndrome with cataplexy and low cerebrospinal fluid orexin, is managed with scheduled naps, wake-promoting agents, and sodium oxybate for cataplexy, with the orexin receptor 2 agonists now an emerging targeted therapy that addresses the missing neurotransmitter directly. The diagnosis is confirmed by a multiple sleep latency test showing a mean sleep latency of eight minutes or less with two or more sleep-onset REM periods, and early diagnosis protects education and mental health. [1] [12]
Restless legs syndrome in children is the disorder most often missed, because the child cannot always describe the urge to move and presents instead with bedtime resistance and unsettled sleep. It is supported by a ferritin below 50 micrograms per litre and a family history, it responds to iron, and the DelRosso trial established intravenous ferric carboxymaltose as effective for refractory disease, so a child who fails oral iron or cannot tolerate it has a proven parenteral option. The periodic limb movement disorder that often accompanies it is now recognised as a distinct and treatable cause of daytime dysregulation and cognitive fatigue. [5] [6]
Narcolepsy type 1
- Orexin loss, cataplexy, daytime sleep
- MSLT: latency 8 min or less, 2 or more SOREMPs
- Orexin below 110 pg per mL confirms
- Naps, wake-promoting agents, sodium oxybate
- Orexin receptor 2 agonists are emerging
Restless legs syndrome
- Urge to move legs in the evening, relieved by movement
- Ferritin below 50 micrograms per litre
- Oral iron first, then intravenous ferric carboxymaltose
- Often a family history
- Periodic limb movement disorder travels with it
OSA of cerebral palsy
- Hypotonic airway collapse, snoring, desaturation
- Adenotonsillectomy in selected children
- CPAP or bilevel for severe disease
- Weigh postoperative airway risk in the hypotonic child
- Lifelong monitoring as the child grows
Insomnia of autism
- Bedtime resistance and night-waking
- Behavioural therapy first, always
- Prolonged-release melatonin second line
- Trial-proven and safe long term
- Often improves with age
Sleep-disordered breathing in cerebral palsy is driven by the hypotonic collapse of the upper airway and by the central and obstructive events that follow, and the Vanhaverbeke and Al-Iede studies quantify its high burden and frame it as one of the highest-yield treatable complications of neurodisability. It is treated by adenotonsillectomy in carefully selected children, weighing the postoperative airway risk in the hypotonic child, and by continuous positive airway pressure or bilevel support in severe disease, and it requires lifelong monitoring as the child grows and after any surgery. [7] [8]
The disorders of arousal, sleepwalking and sleep terrors, are the commonest parasomnias of childhood. They are managed by reassurance, by safety measures to prevent injury, and by scheduled awakenings shortly before the usual event time. The triggers must also be treated, because obstructive sleep apnoea fragments slow-wave sleep and amplifies the parasomnia. A child whose sleepwalking worsens may simply need the obstruction treated. The insomnia of autism is the commonest scenario of all and is the one most responsive to a combination of behavioural therapy and prolonged-release melatonin, and it is where the stepped ladder most reliably delivers. [2] [10]
Complications & Pitfalls
The complications flow from two sources, untreated sleep disturbance and the mistreatment of it, and the clinician who understands both avoids the harms on either side. Untreated obstructive sleep apnoea of cerebral palsy causes pulmonary hypertension and cor pulmonale, growth failure, and neurocognitive decline, and untreated nocturnal hypoventilation of neuromuscular disease progresses to daytime respiratory failure, which is why case-finding with oximetry and capnography is a safety practice, not a research exercise. [7] [8]
The cognitive and behavioural toll of chronic sleep deprivation is large and reversible, and missing it is the commonest oversight in the neurodisability clinic. Each of these children is being failed if the sleep is not asked about. The child with autism whose untreated insomnia is driving his behavioural dysregulation, the child with epilepsy whose fragmented sleep is lowering his seizure threshold, and the child with attention-deficit or hyperactivity disorder whose restless legs are exhausting him. The treatment of the sleep is often the most effective lever the clinician has. [9]
[1] [5] [7]The avoidable pitfalls cluster around the same theme, treating the symptom without identifying the driver. Prescribing a sedative for a child whose restlessness is iron-deficient restless legs makes the movements worse. Prescribing melatonin for a child whose insomnia is an unstructured routine sets up a dependence on a drug that cannot work without the routine. Attributing all of a child's sleep trouble to his neurological diagnosis closes off the treatable drivers that sit beneath it. The discipline of asking which sleep system has failed, and which driver is responsible, prevents each of these errors. [9] [10]
Prognosis & Disposition
Prognosis is favourable when the disorder is recognised and treated, and poor when it is missed, which is why case-finding is the main work of the neurodisability clinic and not an optional extra. Chronic insomnia of autism responds well to behavioural therapy combined with melatonin and improves with age for many children, so the family that is told the prognosis is good and given a clear stepped plan is the family that returns with a sleeping child. Narcolepsy is lifelong but highly treatable, and early diagnosis protects education, mental health, and driving in later life. [2] [1]
Restless legs syndrome often responds to iron and improves, and the periodic limb movement disorder that travels with it is increasingly recognised as a treatable cause of daytime dysregulation. Sleep-disordered breathing of cerebral palsy responds to airway and ventilatory support but requires lifelong monitoring, because the airway changes as the child grows and after any surgery, and a child who is well-supported at one age may desaturate again at the next. The prognosis for quality of life hinges on recognising these disorders early and treating the driver rather than the symptom. [7] [5]
Disposition is shared care, and naming the roles prevents the child falling between services. The primary paediatrician case-finds and coordinates, using a sleep history and a validated questionnaire at every neurodisability and epilepsy review. The neurodisability or epilepsy team optimises the underlying condition, because the seizures, tone, and behaviour must be controlled for any sleep plan to work. The paediatric sleep service performs the polysomnography and the multiple sleep latency test and supervises the ventilation and the specialist pharmacotherapy, and telehealth links the rural and remote family to the specialist centre so that distance is not a barrier to diagnosis and treatment. [10] [11]
Special Populations
Children with severe neurodisability and technology dependence are the population in whom sleep disorders carry the most risk and yield the most from treatment, because hypotonia, scoliosis, and oromotor dysfunction conspire to produce a nocturnal hypoventilation that is invisible without oximetry and capnography. These children need scheduled respiratory and sleep monitoring, early and proactive non-invasive ventilation when the carbon dioxide rises overnight, and a coordinated plan that treats the airway, the ventilation, the seizures, and the tone together, because each of these feeds the others. [7] [8]
Children with autism and intellectual disability struggle to report the inner experience of their sleep disorder, the urge of restless legs or the paralysis of narcolepsy, so the clinician must rely on structured observation, on validated questionnaires, and on the family's filmed account, and must treat a low ferritin empirically when the picture fits. The behavioural insomnia of autism responds well to behavioural therapy and to melatonin, but only when the routine is built first, and the family needs sustained support to hold the routine through the inevitable setbacks. [2] [9]
The adolescent in transition needs an explicit handover of the sleep plan to adult sleep and neurology services. Untreated sleep disturbance is a major driver of disengagement from care in young adult life. A young person with narcolepsy or a ventilated neuromuscular disease who loses their sleep service at transition is a young person at avoidable risk. Building the transition early, with a written summary of the diagnosis, the investigations, the treatments, and the monitoring plan, is the practice that protects continuity. [1] [7]
Evidence, Guidelines & Regional Differences
The evidence is converging on clear principles, though several questions remain live and the fellowship candidate is expected to hold both the settled and the contested. The randomised trial by Gringras and colleagues established prolonged-release melatonin as effective and safe for the insomnia of autism spectrum disorder, and the long-term extension by Maras confirmed sustained benefit, which underpins melatonin as the second-line agent after behavioural therapy and gives the clinician a firm evidence base to quote to a family. [2] [3]
The DelRosso intravenous ferric carboxymaltose trial established parenteral iron as effective for refractory paediatric restless legs syndrome. The Ferri consensus now reframes paediatric periodic limb movement disorder as a distinct childhood category. The clinician therefore has both a treatment and a framework for a disorder that was until recently under-recognised. The Vanhaverbeke and Al-Iede studies quantify the high burden of sleep-disordered breathing in cerebral palsy and frame it as a treatable neurodisability complication, and the American Academy of Sleep Medicine scoring rules standardise the paediatric polysomnogram so that the apnoea-hypopnoea index and the periodic limb movement index can be compared across centres and over time. [5] [6] [7] [11]
Gringras 2017 — prolonged-release melatonin in autism insomnia
Randomised double-blind placebo-controlled trial
Population: Children with autism spectrum disorder and chronic sleep-onset insomnia
Key finding
Prolonged-release melatonin significantly shortened sleep latency and lengthened total sleep time compared with placebo, with a favourable safety profile
Practice change
Establishes melatonin as the evidence-based second-line therapy for insomnia of autism after behavioural measures have been optimised
The live controversies are three, and a candidate who names them shows depth. The first is the role of the orexin receptor 2 agonists, now entering practice for narcolepsy type 1 after the Dauvilliers trial and offering the first mechanism-targeted therapy for an orexin-deficient disease. The second is the boundary between nocturnal frontal lobe epilepsy and the parasomnias, sharpened by video-electroencephalography, which has shown that many events labelled parasomnias are in fact seizures and vice versa. The third is the equity question, how to deliver polysomnography and specialist sleep care to the rural, remote, and low-income families who need them most and can reach them least, and telehealth and community oximetry are the emerging answers. [12] [10]
Exam Pearls
The high-yield facts are these, and each rewards a candidate who can state it cleanly. Sleep and the brain are bidirectional, so disordered sleep worsens seizures, cognition, behaviour, and tone, and must always be asked about in a neurodisability or epilepsy clinic, because treating it is a direct treatment of the neurological condition. The four-cluster classification, dyssomnias, sleep-disordered breathing, parasomnias, and sleep-related movement disorders, is the framework that directs the investigation and the treatment, and it is worth memorising. [10]
Narcolepsy type 1 is the loss of orexin neurons, it presents with cataplexy, and a multiple sleep latency test shows a mean sleep latency of eight minutes or less with two or more sleep-onset REM periods, with cerebrospinal fluid orexin below 110 picograms per millilitre the definitive test. Restless legs syndrome in children is supported by a ferritin below 50 micrograms per litre and responds to iron, with intravenous ferric carboxymaltose proven for refractory disease. The great mimic of the disorders of arousal is nocturnal frontal lobe epilepsy, and the discriminator is that seizures are stereotyped and brief while parasomnias are variable, long, and confined to slow-wave sleep in the first third of the night. [1] [5]
SLEEP
Melatonin, after behavioural therapy, is the second-line agent for chronic insomnia of autism and is trial-proven and safe long term. The apnoea-hypopnoea index and the periodic limb movement index are the two numbers that quantify breathing and movement disorders on polysomnography, and a paediatric apnoea-hypopnoea index of one or more per hour is abnormal, a lower threshold than the adult. The modifiable risk factors are iron deficiency, adenotonsillar hypertrophy, and unstructured routines, and treating these three often resolves the disorder before any drug or device is needed. The prognosis is favourable when the disorder is recognised and treated, and the main work of the clinic is case-finding. [2] [11]
References
- [1]Scammell TE Narcolepsy. N Engl J Med, 2015.PMID 26716917
- [2]Gringras P, Nir T, Breddy J, et al Efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry, 2017.PMID 29096777
- [3]Maras A, Schroder CM, Malow BA, et al Long-term efficacy and safety of pediatric prolonged-release melatonin for insomnia in children with autism spectrum disorder. J Child Adolesc Psychopharmacol, 2018.PMID 30132686
- [4]DelRosso LM, Picchietti DL, Sharon D, et al Periodic limb movement disorder in children: a systematic review. Sleep Med Rev, 2024.PMID 38652932
- [5]DelRosso LM, Ferri R, Chen ML, et al Clinical efficacy and safety of intravenous ferric carboxymaltose treatment of pediatric restless legs syndrome and periodic limb movement disorder. Sleep Med, 2021.PMID 34562823
- [6]Ferri R, Picchietti DL, Sharon D, et al Rethinking pediatric periodic limb movement disorder: a clinical review of pediatric PLMD and consensus criteria for an updated pediatric diagnostic category. Sleep Med, 2025.PMID 40203610
- [7]Vanhaverbeke K, Selcuk M, Ersu R, et al Sleep-disordered breathing in children with neurodisabilities. Eur Respir Rev, 2026.PMID 42128483
- [8]Al-Iede M, Al-Ani A, Libdeh AA, et al Sleep-disordered breathing in children with cerebral palsy compared to non-neurological controls: a prospective study. Neurol Int, 2026.PMID 41893051
- [9]Wang H, Yu L, Hu S, et al Prevalence and associated factors of sleep disorders in children and adolescents with autism spectrum disorder: a meta-analysis and systematic review. BMC Psychiatry, 2026.PMID 42192550
- [10]Nunes ML, El Halal CDS Sleep disorders in children and adolescents with neurodevelopmental and neurological disorders: what evidence do we have with the use of non-pharmacological interventions? Front Sleep, 2026.PMID 41929654
- [11]Berry RB, Brooks R, Gamaldo C, et al AASM Scoring Manual updates for 2017 (version 2.4). J Clin Sleep Med, 2017.PMID 28416048
- [12]Dauvilliers Y, Mignot E, Del Rio Villegas R, et al Oral orexin receptor 2 agonist in narcolepsy type 1. N Engl J Med, 2023.PMID 37494485