Paeds · neurology-neurodisability-and-neuromuscular
Spasticity, dystonia and tone management
Also known as Hypertonicity management · Spasticity management · Dystonia management · Tone management in cerebral palsy · Botulinum toxin therapy · Intrathecal baclofen therapy · Selective dorsal rhizotomy · Upper motor neuron syndrome
Fellowship guide to spasticity, dystonia and tone management in children, centred on cerebral palsy. Covers the Sanger classification of hypertonia into velocity-dependent spasticity and action-induced dystonia with the mixed picture common in cerebral palsy, the goal-directed principle that tone is treated only when it limits function comfort or care, the Modified Tardieu and Modified Ashworth scales and the Gross Motor Function Classification System from GMFCS I to V, the four core modalities of focal botulinum toxin type A with its non-interchangeable products and twelve-week re-injection interval, oral baclofen as a GABA-B agonist that must not be stopped abruptly, intrathecal baclofen with a screening bolus and the medical-emergency withdrawal syndrome, selective dorsal rhizotomy for the ambulant spastic diplegic child, the dystonia pathway from trihexyphenidyl to GPi deep brain stimulation, and the multidisciplinary prevention of contracture hip subluxation scoliosis and pain.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child whose arm draws up and whose hand clenches when they reach for a toy, or whose legs stiffen and scissor the moment they try to stand, is showing you hypertonia, and the paediatric job is to decide whether that tone is worth treating and how. Hypertonia is the abnormally increased resistance to an externally imposed movement about a joint, and in a child it is almost always an upper motor neuron sign. Cerebral palsy is the commonest cause, but the same tone problems follow spinal cord injury, traumatic brain injury, and a handful of metabolic and genetic disorders, and the principles of management carry across them all. [1][2]
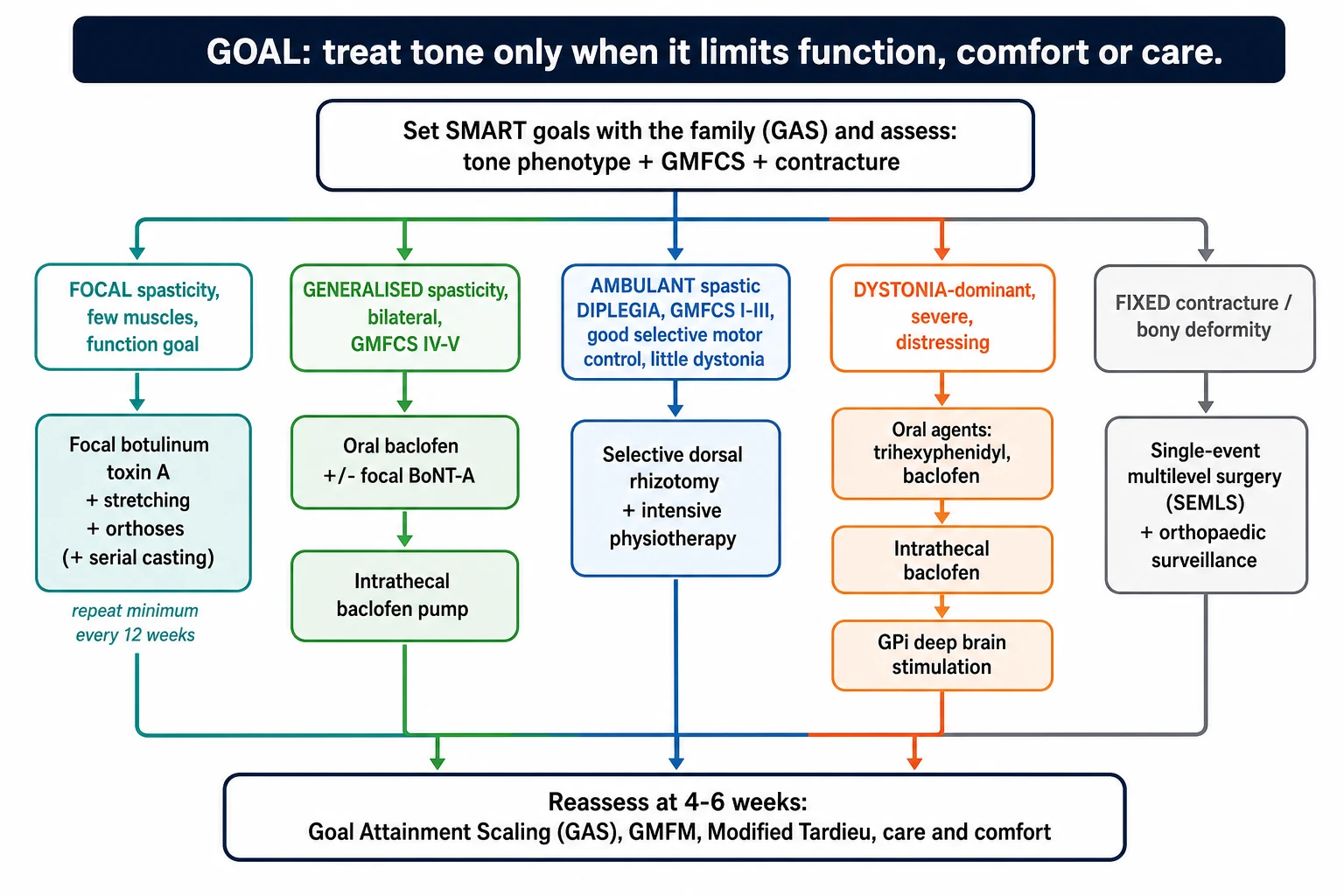
The single idea that governs the whole topic is that tone is treated only when it limits function, comfort, care or participation. A stiff leg that lets a child stand and transfer is an asset, not a target; a stiff adductor that defeats nappy changing and hygiene is a target. The fellowship candidate who reaches for this principle first, and matches the modality to the goal, will answer every tone question well. [1]
Four modalities carry the workload: focal botulinum toxin type A for the few troublesome muscles, oral baclofen for generalised spasticity, intrathecal baclofen for the severe generalised or dystonic child, and selective dorsal rhizotomy for the ambulant spastic diplegic child. The two phenotypes of spasticity and dystonia decide which one fits, and the Gross Motor Function Classification System decides how ambitious the functional goal can be. [3][6]
Classification
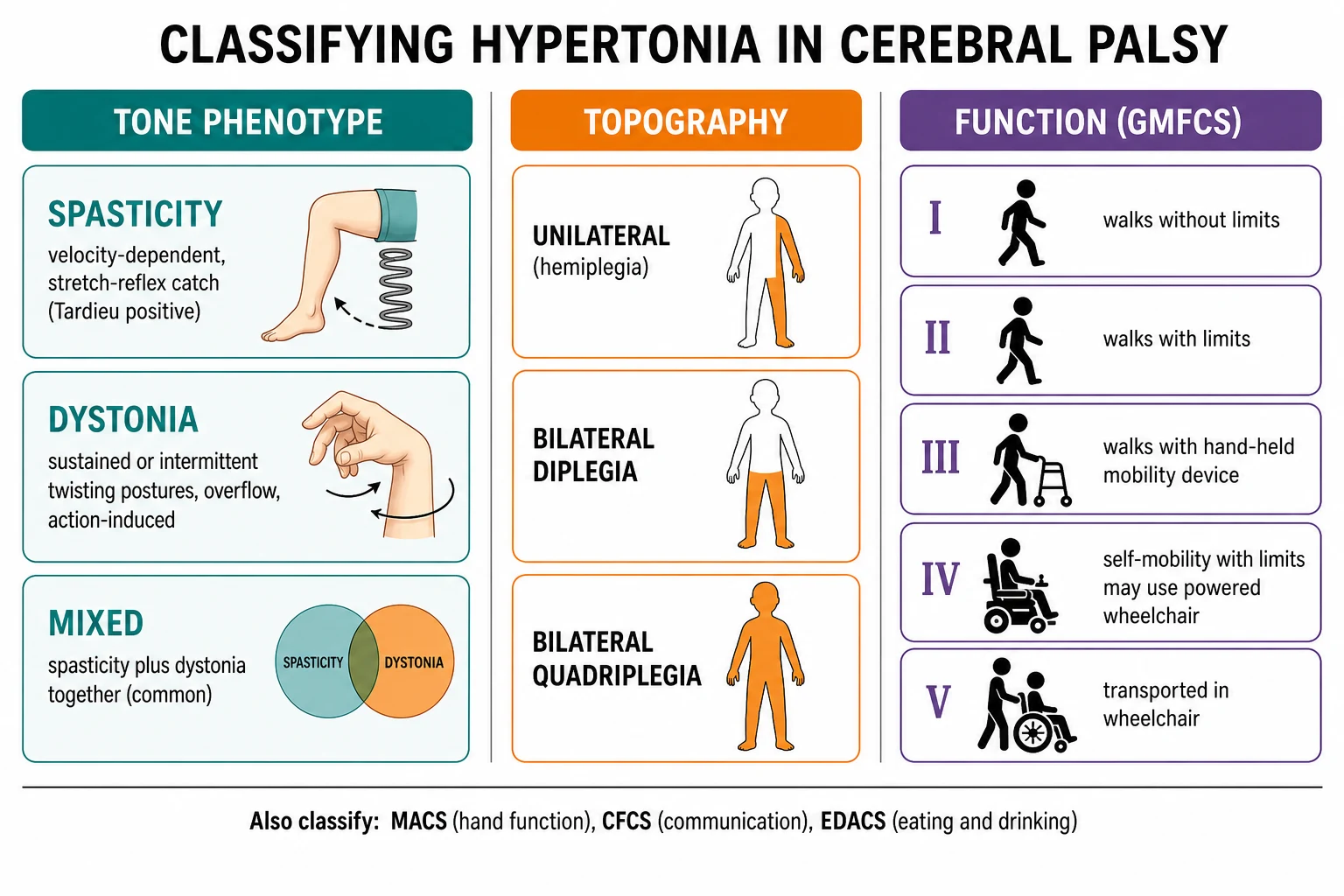
Sort the high tone first, because the phenotype drives the therapy. The Sanger framework, now the international standard for the paediatric motor examination, splits hypertonia into three patterns. Spasticity is velocity-dependent, so resistance rises the faster you move the joint and you feel a catch, then a release. Dystonia is action-induced and overflow-driven, so the twisting postures and co-contraction appear when the child tries to move or is aroused, and they vanish in sleep. Rigidity, which is rare in cerebral palsy, is constant through the range and independent of speed. Most children with cerebral palsy show a mixed spastic-dystonic picture, and the examiner will test whether you can tell the dominant one. [1][11]
Spasticity is then sorted by topography, because the pattern predicts the treatment and the orthopaedic risk. Unilateral spastic cerebral palsy, the old hemiplegia, affects one side and is the commonest form in term children. Bilateral spastic cerebral palsy splits into diplegia, where the legs dominate and walking is the central problem, and quadriplegia or tetraplegia, where all four limbs and often the trunk and oropharynx are involved. Diplegia is the prime candidate for selective dorsal rhizotomy; quadriplegia is the prime candidate for intrathecal baclofen. [2][3]
The functional axis that frames every conversation is the Gross Motor Function Classification System, which runs from level I, an independent community ambulator, to level V, a child transported in a wheelchair who cannot sit or stand without help. The GMFCS is stable over years and predicts walking, and it sets how ambitious the tone goal can be and which modality fits. A child at GMFCS I to III is an orthoses, botulinum toxin and selective dorsal rhizotomy candidate; a child at GMFCS IV to V is an oral and intrathecal baclofen and care-and-comfort candidate. [3]
Epidemiology & Risk Factors
Cerebral palsy is the backdrop to almost every paediatric tone question, with a prevalence of around two per thousand live births that has been stable for a generation in high-income countries. Prematurity is the dominant risk factor: the extreme preterm infant is forty times more likely to develop cerebral palsy than the term infant, and the white-matter injury of periventricular leukomalacia gives the classic spastic diplegia. Term children more often show unilateral spastic cerebral palsy from a middle cerebral artery territory stroke or dyskinetic cerebral palsy from acute near-total asphyxia or kernicterus. [2]
The tone burden is huge in this population. Roughly four in five children with cerebral palsy have spasticity, around one in ten have a dyskinetic or dystonic-dominant picture, and the mixed spastic-dystonic child is common. Hip displacement tracks with severity: by school age a substantial minority of non-ambulant children have a hip that has migrated beyond thirty percent, and the surveillance hip radiograph is built into the routine care of every child with cerebral palsy. [2][11]
The risk of an adverse tone outcome climbs with three things: greater motor severity, the presence of dystonia alongside the spasticity, and loss of access to a coordinated team. The Aboriginal and Torres Strait Islander child and the child from a remote setting carries a higher prevalence of cerebral palsy and worse secondary musculoskeletal outcomes, because distance and inequity delay the physiotherapy, the orthoses and the surveillance. [2]
Pathophysiology
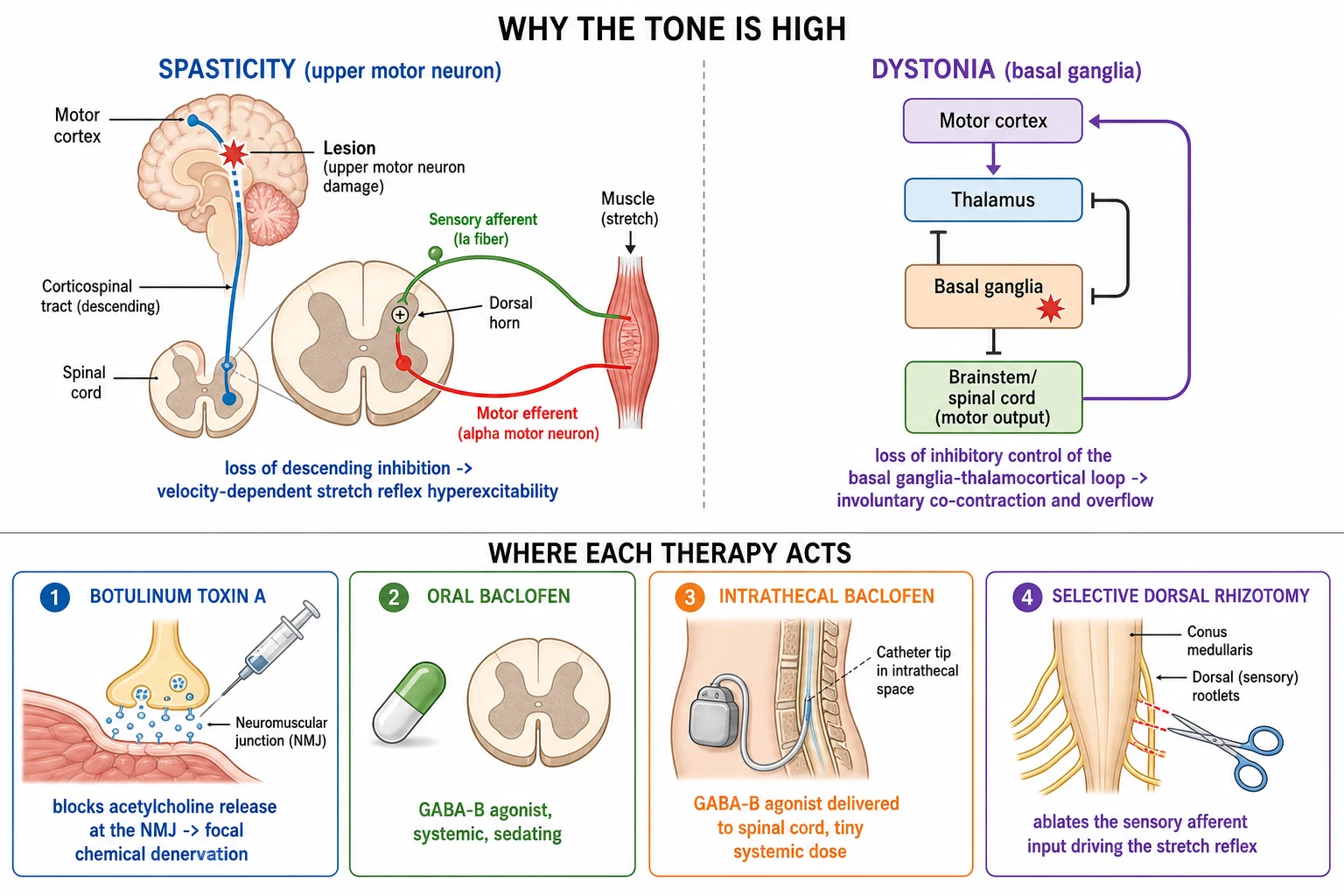
The tone is high because an upper motor neuron lesion has removed the braking system on the lower motor neuron. A normal corticospinal tract sends a steady stream of inhibition down to the spinal cord that holds the stretch reflex in check. When that tract is damaged in the developing brain, the inhibition is lost, the gamma motor neurons become overactive, and the monosynaptic stretch reflex fires too easily and too strongly. The clinical result is spasticity: the faster you stretch the muscle, the harder it resists, because the stretch reflex is velocity-dependent. [1]
Dystonia has a different origin in a different place. It comes from injury to the basal ganglia and the thalamus, the deep grey-matter structures that gate and shape the motor program. When their inhibitory control of the basal ganglia-thalamocortical loop is lost, the muscles co-contract and the overflow appears, so the child twists into a posture the moment they try a voluntary movement. Sleep switches dystonia off, which is a useful bedside discriminator from fixed contracture. [11]
Each therapy attacks this physiology at a different point, and knowing the point tells you the use and the side effect. Botulinum toxin acts at the neuromuscular junction, blocking acetylcholine release to produce a focal chemical denervation, so it suits a few overactive muscles but does nothing for the central driver. Baclofen is a gamma-aminobutyric acid type B agonist that binds receptors in the dorsal horn of the spinal cord to damp the reflex arc, so it suits generalised spasticity but is sedating when given by mouth. Intrathecal baclofen delivers the same drug straight onto the spinal cord in microgram doses, buying the effect without the systemic sedation. Selective dorsal rhizotomy goes one step further and cuts the sensory afferent rootlets that feed the overactive stretch reflex, ablating the driver in the legs for good. [1][8]
Clinical Presentation
The presentation is the cerebral palsy picture, and the tone is one feature of it, so take the whole child. The spastic child shows the flexed elbow and pronated forearm, the clenched fist with the thumb in palm, the scissoring adducted thighs, the equinus or tip-toe gait, and the brisk reflexes and clonus. The dystonic child shows the twisting, overflow and action-driven postures that vanish in sleep, with the grimacing, the arching and the involuntary movements that defeat function and care. The mixed child shows both, and the examiner wants to know which is dominant and which is the rate-limiting problem. [1][11]
Ask the family what the tone stops the child doing. The goals fall into four buckets: function, like a reach or a step that the stiffness defeats; care and hygiene, like nappy changing defeated by adductor spasticity, or dressing defeated by a flexed elbow; comfort and pain, like the muscle spasms that wake the child at night or the hip that aches as it subluxes; and participation and appearance, like the cosmetic and social burden of an asymmetrical gait or posture. The goal the family names is the one you treat, and a stiff limb that does none of these is left alone. [2]
Look for the secondary damage the tone has already caused, because it changes the plan. Run a hip radiograph in the non-ambulant child, look for scoliosis and joint contracture on examination, and feel for the painful hip. A child who comes in with a fixed equinus contracture is no longer a pure botulinum toxin candidate, because the toxin softens dynamic tone but cannot lengthen a fixed tendon, and the orthopaedic surgeon joins the team. [5]
Differential Diagnosis
The first cut is not what causes the tone but what kind of tone it is, because spasticity, dystonia and rigidity behave differently. Spasticity is velocity-dependent with a catch. Dystonia is action and overflow driven and sleep-relieved. Rigidity is constant and speed-independent, the lead-pipe or cogwheel feel of an extrapyramidal disorder, and it is uncommon in cerebral palsy. A child whose high tone does not fit the velocity-dependent pattern should make you question the diagnosis rather than reach for a toxin. [1]
The second cut is the cause of the upper motor neuron lesion, because cerebral palsy is a clinical label, not a final diagnosis, and treatable mimics hide behind it. A progressive neurological disorder must be excluded in any child whose tone is worsening or whose skills are being lost: think of a metabolic leukodystrophy, a hereditary spastic paraplegia, a dopa-responsive dystonia that responds dramatically to low-dose levodopa, or a spinal cord lesion with a mixed upper and lower motor neuron picture. Loss of skill, regression, or a changing examination is a red flag that the label cerebral palsy is wrong. [2]
The third cut separates the dynamic tone from the fixed deformity, because only the first answers to medical tone therapy. Dynamic tone, the catch that gives way to sustained stretch, softens with botulinum toxin and baclofen. A fixed contracture, the immovable endpoint of months of unopposed pull, does not, and it needs casting or surgery. The Modified Tardieu Scale is built to tell them apart, by comparing the angle of catch at a fast velocity with the passive range at a slow velocity. [1][5]
Clinical & Bedside Assessment
Begin with the airway, breathing and swallow in any child with severe cerebral palsy, because the oropharyngeal tone and the aspiration risk are the immediate threats and they sit beside the tone problem. Then move to the focused motor examination. Lay the child flat and roll each joint through its range at a slow velocity for the passive range of movement, then at a fast velocity for the angle of catch, and the gap between the two is the dynamic tone that a toxin can soften. Record the spasticity grade, the deep tendon reflexes, the clonus, and the selective motor control, because selective control is the single best predictor of who will walk and who will benefit from a rhizotomy. [3][5]
Quantify the tone with a validated tool rather than a vague impression, because the gate and the family both want a number. The Modified Tardieu Scale measures the angle of muscle reaction at a specified velocity, and it is the preferred tool for children because it separates dynamic tone from fixed contracture. The Modified Ashworth Scale grades resistance to passive movement on an ordinal scale from zero to four, and it is simpler but cruder and less sensitive to change. Pair the tone measure with a functional measure like the Gross Motor Function Measure or a goal measure like Goal Attainment Scaling, so the reassessment at four to six weeks can show whether the injection met the goal the family set. [1][2]
Examine the hips, the spine and the skin, because the complications of unmanaged tone live there. Palpate the hips for pain and limited abduction, order the migration percentage on a radiograph in the non-ambulant child, look for the emerging scoliosis and pelvic obliquity, and check the skin under the orthoses and the seating for pressure. A sudden change in tone, pain or mood between injections should prompt a hip radiograph before a repeat injection, because a subluxing hip presents as worsening tone and distress. [2]
Investigations
There is no blood test and no scan for spasticity, and the diagnosis is made on the clinical examination and the tone phenotype. Magnetic resonance imaging of the brain confirms the lesion underlying the cerebral palsy and helps exclude a progressive disorder, and it is recommended once in the work-up of every child with cerebral palsy, but it does not grade the tone or decide the therapy. The therapy is decided at the bedside with the Tardieu angle and the GMFCS, and with the goals the family names. [2][1]
The investigation that runs through the whole of childhood is the surveillance hip radiograph, because the spastic hip subluxes silently and the window to prevent a dislocation closes in the early school years. A non-ambulant child, GMFCS IV or V, has a hip radiograph yearly from around eighteen months to seven years, and an ambulant child at lower risk is screened less often. The migration percentage is the number that triggers referral: above thirty percent the hip is at risk, and above fifty percent the orthopaedic surgeon is involved for reconstruction. [2]
Run the checks the chosen therapy demands. Before intrathecal baclofen, screen the child for a ventriculoperitoneal shunt, scoliosis and swallow safety, and arrange the intrathecal test dose under observation. Before selective dorsal rhizotomy, document the gait analysis, the selective motor control, the MRI of the spine and the orthopaedic status of the hips and the tendon lengths, because the candidate selection is where the surgery succeeds or fails. Before each botulinum toxin cycle, confirm the goals and the muscles and re-check the hip if the tone has changed. [6][8]
Management — Resuscitation
The only tone emergency is the loss of an intrathecal baclofen pump, and it is a true resuscitation, so learn it cold. Abrupt withdrawal of intrathecal baclofen, from pump failure, catheter fracture, or an empty reservoir, drives rebound spasticity, high fever, rigidity, seizures, rhabdomyolysis and progression to multi-organ failure and death. Restore the infusion as soon as possible, give enteral baclofen at high dose, add a benzodiazepine such as diazepam or lorazepam for the rigidity and seizures, cool the fever, and admit to a high-dependency or intensive care setting. Do not wait for confirmation of the cause; treat on suspicion. [8][9]
The mirror image is intrathecal baclofen overdose, from a programming error or a refill mishap, which presents as hypotonia, drowsiness, respiratory depression and coma. Stop or reduce the infusion, support the airway and breathing, and arrange urgent pump interrogation and reprogramming by the implanting service. There is no antidote; the management is supportive while the drug clears, and severe cases may need cerebrospinal fluid drainage. [8]
The third acute problem is the painful muscle spasm or the dystonic storm, often triggered by infection, constipation, pain or a displaced fracture in a child who cannot say where it hurts. Treat the trigger first, because a dystonic storm in a child with cerebral palsy is as often a UTI or a fractured femur as it is a tone problem, and add a rescue dose of an oral agent such as diazepam or a bolus of intrathecal baclofen once the source is addressed. [9][11]
Management — Definitive & Stepwise
Definitive care is goal-directed and stepwise, and the step you choose is set by the goal, the phenotype and the GMFCS. Start with the non-pharmacological foundation that underpins every modality: a daily stretching and positioning program, orthoses such as an ankle-foot orthosis to hold range and shape growth, serial casting to gain length, and the seating and standing equipment that prevents contracture in the non-ambulant child. No drug or operation works without this layer, and it runs throughout childhood. [2][5]
Set the goal
Name with the family whether tone limits function, care and hygiene, comfort, or participation. Treat only the rate-limiting tone.
Phenotype and classify
Separate spasticity from dystonia, confirm dynamic rather than fixed tone with the Modified Tardieu Scale, and state the GMFCS level.
Foundation for all
Daily stretching, positioning, orthoses, serial casting and equipment. No drug works without this layer.
Focal spasticity
Focal botulinum toxin type A into the few overactive muscles, with a minimum twelve-week re-injection interval.
Generalised spasticity
Oral baclofen, then intrathecal baclofen for the severe generalised or dystonic GMFCS IV to V child.
Ambulant diplegia
Selective dorsal rhizotomy for the GMFCS I to III spastic diplegic child with good selective control and minimal dystonia.
Reassess and escalate
Re-measure at four to six weeks with Goal Attainment Scaling; add orthopaedic single-event multilevel surgery for fixed deformity.
Botulinum toxin type A is the workhorse for focal spasticity and the modality most fellowship questions probe. Injected into the overactive muscle, it blocks acetylcholine at the neuromuscular junction to give a focal, reversible chemical denervation, with onset in two to seven days, a peak effect around four weeks, and a duration of twelve to sixteen weeks. The three products, onabotulinumtoxinA, abobotulinumtoxinA and incobotulinumtoxinA, are not interchangeable, and their units must never be converted between brands. The total per-session onabotulinumtoxinA dose is individualised to the child, commonly up to around fifteen to twenty units per kilogram with a per-child ceiling near four hundred units, and the minimum re-injection interval is twelve weeks to limit neutralising antibody formation. [1][4][5]
Botulinum toxin type A (onabotulinumtoxinA)
Oral baclofen is the first-line drug for generalised spasticity, a gamma-aminobutyric acid type B agonist that damps the spinal reflex arc. It is sedating and only modestly effective, but it is cheap, familiar and useful as a systemic adjunct, especially when the spasticity is diffuse and the child is not a focal-injection candidate. Start low and titrate over weeks, because the adverse effects of sedation, hypotonia and constipation are dose-related, and never stop it abruptly, because sudden withdrawal causes seizures, rebound spasticity and hallucinations. [1][2]
Oral baclofen
Intrathecal baclofen is the escalation for the severe generalised spastic or the dystonic child whose tone defeats oral therapy and care. A continuous infusion through an implanted pump delivers microgram doses straight onto the spinal cord, buying a baclofen effect without the systemic sedation, and it improves care, comfort and function in the GMFCS IV and V child. The pathway begins with a screening bolus, typically twenty-five to one hundred micrograms, to confirm a responder before the pump is implanted, and the maintenance infusion is then titrated individually, with many children needing one hundred to one thousand micrograms per day. The price is a device, with the catheter and pump complications, the infection risk, and the withdrawal-and-overdose emergencies described above. [8][9][10]
Selective dorsal rhizotomy is the operation for the ambulant spastic diplegic child, and its evidence is the cleanest in paediatric tone care. The surgeon identifies the dorsal sensory rootlets from L2 to S1 and cuts a proportion of them, often around twenty-five to sixty-seven percent, to remove the afferent input that drives the spasticity in the legs. The ideal candidate is the child at GMFCS II or III with spastic diplegia, good selective motor control, minimal dystonia, no major orthopaedic deformity and a motivated family, and the operation is followed by an intensive period of physiotherapy and strengthening. The McLaughlin meta-analysis of three randomised trials showed that selective dorsal rhizotomy with therapy outperformed therapy alone for spastic diplegia in the younger child, and the long-term data confirm a durable reduction in spasticity and in the need for later orthopaedic surgery, though loss of spasticity is not the same as a gain in function and the child needs ongoing strengthening. [6][7]
[1] [6]Specific Subtypes & Scenarios
The ambulant spastic diplegic child at GMFCS II or III is the selective dorsal rhizotomy candidate, and the counselling turns on the evidence and the commitment. The operation gives a durable reduction in leg spasticity and reduces the later need for orthopaedic surgery, and the McLaughlin meta-analysis supports it over therapy alone in the younger child, but it does not buy a new GMFCS level by itself. The family must commit to months of intensive postoperative physiotherapy and strengthening, because the loss of spasticity unmasks underlying weakness, and a child who stops strengthening can lose ground. Pick the motivated family with the well-selected child, and the gain is real and lasting. [6][7]
The non-ambulant child at GMFCS IV or V is the intrathecal baclofen and the care-and-comfort candidate, and the goals are comfort, ease of care, pain relief and prevention of deformity rather than walking. Intrathecal baclofen improves care and comfort, eases dressing and hygiene, and may reduce pain, and it has a place in the dystonic child where oral therapy fails. The hip and spine surveillance runs in parallel, because the spastic hip subluxes silently and the scoliosis progresses with growth, and the orthopaedic surgeon is part of the team from the start. [8][10]
The dystonia-dominant child follows its own pathway, because botulinum toxin and selective dorsal rhizotomy are built for spasticity and disappoint in pure dystonia. Start with the oral agents: trihexyphenidyl, an anticholinergic, is first-line in many centres, with the caveat that the Cochrane evidence for it in cerebral palsy dystonia is limited and the anticholinergic burden of dry mouth, constipation, urinary retention and blurred vision is real and dose-related; oral baclofen and clonazepam are alternatives. The severe generalised dystonic child who fails oral therapy moves to intrathecal baclofen or to globus pallidus internus deep brain stimulation, which can give dramatic relief in selected dystonic cerebral palsy. [11][12]
Matching the modality to the child
Complications & Pitfalls
The musculoskeletal complications are the price of unmanaged tone, and they are the reason surveillance never stops. The spastic adductor and psoas pull the hip out of joint, the spastic hamstrings and hip flexors tilt the pelvis and curve the spine into scoliosis, and the unopposed pull across each joint freezes it into a fixed contracture. Each is preventable with early physiotherapy, orthoses, botulinum toxin and, in the right child, surgery, and each is harder to fix once established. The dislocated hip in particular causes pain, blocks care and seating, and is much harder to reconstruct than to prevent. [2][5]
The treatment complications are the ones the fellowship examiner tests. Botulinum toxin spreads to neighbouring muscles to cause unwanted weakness, and rare cases of generalised weakness follow high total doses; repeat injections at too short an interval risk neutralising antibodies that abolish the response. Oral baclofen sedates and causes tolerance, and abrupt withdrawal seizures are the trap. Intrathecal baclofen brings catheter fracture, pump malfunction, infection and the life-threatening withdrawal syndrome. Selective dorsal rhizotomy unmasks weakness, can leave the legs hypotonic, and very rarely causes bowel and bladder disturbance from rootlet section. [4][8]
The classic pitfalls are clinical. Treating high tone because it is there, rather than because it limits function, comfort or care, over-medicalises a child and buys side effects for no gain. Failing to exclude a progressive disorder before labelling the child cerebral palsy. Missing a subluxing hip that presents as worsening tone or distress between injections. Sending a child for selective dorsal rhizotomy who has dominant dystonia, where the operation fails. And the commonest error at the bedside: confusing a fixed contracture, which needs surgery, with dynamic spasticity, which answers to toxin and baclofen. [1][7]
Prognosis & Disposition
The prognosis of the tone itself, well managed, is good: spasticity softens with botulinum toxin and baclofen, the ambulant diplegic child gains from a rhizotomy, and the severe generalised child is made comfortable and cared-for with intrathecal baclofen. The prognosis of the function is set by the GMFCS, which is stable over years and predicts walking with a reliability that frames every conversation: a child at GMFCS I walks without limits, a child at GMFCS II walks with limits, and a child at GMFCS V is transported in a wheelchair throughout life. [3]
The long-term threats to quality of life are the musculoskeletal complications and the pain, and both are the business of the multidisciplinary team. Hip surveillance catches the subluxing hip, the orthotist and the physiotherapist hold the range, the orthopaedic surgeon reconstructs the deformity, and the rehabilitation engineer shapes the seating and the standing frame. Pain is common and under-recognised in cerebral palsy, and the dystonic storm and the muscle spasm are treated as seriously as the tone itself. [2]
Disposition is community-led and lifelong. The child is managed in the paediatric rehabilitation clinic with the team, the botulinum toxin cycles run every three to six months, the intrathecal baclofen pump is refilled every few months, and the hip and spine surveillance continues to skeletal maturity. The transition to adult rehabilitation care in the late teenage years is planned early, because the tone, the deformity and the pain do not end at eighteen and the adult service must inherit a coordinated plan. [2]
Special Populations
The Aboriginal and Torres Strait Islander child and the child from a remote or regional setting carries a higher burden of cerebral palsy and worse secondary musculoskeletal outcomes, because distance delays the physiotherapy, the orthoses and the hip surveillance. The threshold to retrieve, to fund travel for the botulinum toxin clinic and the orthopaedic review, and to support the family locally is low, and telehealth links the remote child to the multidisciplinary team. Equity of access to the funded therapies is a real issue the paediatrician advocates for. [2]
The child from a migrant or refugee family needs an interpreter at every visit, goal setting in language, and a clear explanation of the one-in-four recurrence risk where cerebral palsy has a genetic component and of the options for prenatal diagnosis. The technology-dependent child with an intrathecal baclofen pump, a gastrostomy or long-term ventilation needs a coordinated emergency plan, a pump card for the family to carry, and a clear local pathway for the withdrawal syndrome, because the remote hospital may never have seen one. [8]
The adolescent in transition faces the loss of the paediatric team and the burden of an adult body with cerebral palsy, where pain, fatigue and musculoskeletal deterioration often worsen. The tone management continues, but the goals shift toward independence, participation, reproductive and sexual health, and mental health, and the plan must be handed to the adult rehabilitation service with the full record of the pump, the injections and the surgery. [2]
Evidence, Guidelines & Regional Differences
The evidence base and the care framework rest on the American Academy of Neurology practice parameter on the pharmacologic treatment of spasticity in cerebral palsy, the NICE guideline on cerebral palsy in under twenty-five-year-olds, and the international consensus statements on botulinum toxin for the upper and lower limb. The selective dorsal rhizotomy evidence rests on the McLaughlin meta-analysis of three randomised trials and the Tedroff systematic review of the long-term effects, and the intrathecal baclofen evidence rests on the Albright landmark papers and the Eek study in dyskinetic cerebral palsy. The dystonia drug evidence is thinner, with the Cochrane review of trihexyphenidyl showing limited data despite widespread use. [1][2][7][12]
In Australia and Aotearoa New Zealand, hip surveillance follows the Australian Hip Surveillance Guidelines, with a standardised radiograph protocol and migration-percentage thresholds that drive orthopaedic referral, and the cerebral palsy registers track prevalence and outcomes. Selective dorsal rhizotomy is funded in dedicated centres for the well-selected ambulant diplegic child, and intrathecal baclofen is delivered through the rehabilitation services. Botulinum toxin is the commonest funded focal treatment.
Exam Pearls
Lead with the goal-directed principle every time: treat the tone only when it limits function, comfort, care or participation. Separate the velocity-dependent spasticity from the action-induced dystonia with the Modified Tardieu Scale, because the phenotype drives the drug, and state the GMFCS level, because it frames the goal and the modality. [1][3]
The four high-yield facts the examiner wants are these. First, the botulinum toxin products are not interchangeable, and the minimum re-injection interval is twelve weeks to avoid neutralising antibodies. Second, oral baclofen must never be stopped abruptly, because withdrawal causes seizures. Third, intrathecal baclofen withdrawal is a medical emergency with rebound rigidity, fever and rhabdomyolysis, restored by enteral baclofen, a benzodiazepine and infusion restoration. Fourth, selective dorsal rhizotomy is for the ambulant spastic diplegic child, not the dystonia-dominant or the most severe child, and it is supported by the McLaughlin meta-analysis of three randomised trials. [1][6][8]
The discriminating bedside skills are the angle of catch on the Modified Tardieu Scale for dynamic versus fixed tone, the GMFCS level for the functional frame, and the migration percentage on the surveillance hip radiograph for the orthopaedic threshold. The common traps are treating tone that does not limit anything, missing a progressive disorder behind the cerebral palsy label, and sending a dystonia-dominant child for a rhizotomy. Hold the goal, the phenotype and the GMFCS together, and the tone question answers itself. [2][3][6]
References
- [1]Delgado MR, Hirtz D, Aisen M, et al, Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society Practice parameter: pharmacologic treatment of spasticity in children and adolescents with cerebral palsy (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology, 2010.PMID 20101040
- [2]Shaunak M, Perkins L, Bandaranayake T, et al Cerebral palsy in under 25 s: assessment and management (NICE Guideline NG62). Arch Dis Child Educ Pract Ed, 2018.PMID 29056589
- [3]Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol, 1997.PMID 9183258
- [4]Fehlings D, Rang M, Glazier J, et al Botulinum toxin assessment, intervention and follow-up for paediatric upper limb hypertonicity: international consensus statement. Eur J Neurol, 2010.PMID 20633178
- [5]Molenaers G, Fagard K, Van Campenhout A, Desloovere K Botulinum toxin A treatment of the lower extremities in children with cerebral palsy. J Child Orthop, 2013.PMID 24432099
- [6]McLaughlin J, Bjornson K, Temkin N, et al Selective dorsal rhizotomy: meta-analysis of three randomized controlled trials. Dev Med Child Neurol, 2002.PMID 11811645
- [7]Tedroff K, Bjerke I, Akerström F, Tedroff L Long-term effects of selective dorsal rhizotomy in children with cerebral palsy: a systematic review. Dev Med Child Neurol, 2020.PMID 31342516
- [8]Albright AL, Cervi A, Singletary J Intrathecal baclofen for spasticity in cerebral palsy. JAMA, 1991.PMID 1999883
- [9]Albright AL, Barry MJ, Fasick P, Barron W, Shultz B Infusion of intrathecal baclofen for generalized dystonia in cerebral palsy. J Neurosurg, 1998.PMID 9420075
- [10]Eek MN, Olsson K, Lindblad LE, et al Intrathecal baclofen in dyskinetic cerebral palsy: effects on function and activity. Dev Med Child Neurol, 2018.PMID 29148568
- [11]Monbaliu E, Himmelmann K, Lin JP, et al Clinical patterns of dystonia and choreoathetosis in participants with dyskinetic cerebral palsy. Dev Med Child Neurol, 2016.PMID 26173923
- [12]Harvey AR, Gibson N, Berrington S, McMahon C Trihexyphenidyl for dystonia in cerebral palsy. Cochrane Database Syst Rev, 2018.PMID 29763510