Paeds · neurology-neurodisability-and-neuromuscular
Spinal cord compression and transverse myelitis
Also known as Malignant spinal cord compression · Metastatic spinal cord compression · Acute transverse myelitis · Longitudinally extensive transverse myelitis · Epidural spinal cord compression · Spinal epidural abscess
A fellowship approach to the child with an acute or subacute spinal cord syndrome. The first act is to recognise that a new back pain with a neurological deficit is a cord emergency until an emergency whole-spine MRI proves otherwise, and to separate the two great threats to the cord - a structural compressive lesion (tumour, epidural abscess, disc, haematoma) that is a surgical emergency from an intrinsic inflammatory transverse myelitis (idiopathic, neuromyelitis optica spectrum disorder, myelin-oligodendrocyte-glycoprotein antibody-associated disease, multiple sclerosis, post-infectious) that is a medical emergency. Treat the compressive lesion with dexamethasone and surgical decompression within twenty-four to forty-eight hours, plus radiotherapy or antibiotics as indicated, and treat the inflammatory lesion with high-dose intravenous methylprednisolone escalating to intravenous immunoglobulin or plasma exchange. Ambulation at presentation is the single strongest predictor of outcome, so the emergency MRI is never delayed while workup tests return.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A previously well nine-year-old wakes in the night with thoracic back pain that will not settle, and by morning is dragging her left leg; her bladder will not empty. Across town, a four-year-old being treated for Ewing sarcoma refuses to walk, and a feverish teenager with an indwelling central line develops acute urinary retention and a band of numbness around the chest. In every one of these rooms the unifying question is the same - is the spinal cord being crushed from outside or inflamed from within, and is there still time to save it? The fellowship task is to convert that bedside alarm into one action - the emergency whole-spine MRI - and then into the matched treatment: dexamethasone and the operating theatre for a compressive lesion, high-dose methylprednisolone for an inflammatory one. [1] [7]
C · O · R · D
Overview & Definition
The clinician's first act is to recognise that an acute or subacute spinal cord syndrome is not one disease but two threats that share a presentation and diverge in treatment. The two threats are a structural compressive lesion, in which something outside the cord presses on it, and an intrinsic inflammatory lesion, in which the immune system attacks the cord substance itself. Both produce the same bedside picture - back pain, limb weakness, a sensory level, and bladder and bowel disturbance - and both can destroy the cord within hours to days. The single test that separates them is the emergency whole-spine MRI with gadolinium, which shows the mass or abscess outside the cord in the compressive case and a swollen, enhancing lesion within the cord in the inflammatory case. [1] [7]
Why does this fork matter at the bedside? Because the two threats need opposite treatments and the wrong treatment loses the cord. A compressive lesion is a surgical emergency: the mass must be removed or the cord decompressed within twenty-four to forty-eight hours, backed by dexamethasone to buy time and by radiotherapy or antibiotics matched to the cause. An inflammatory transverse myelitis is a medical emergency: the attack is calmed with high-dose corticosteroids, escalating to intravenous immunoglobulin or plasma exchange when steroids fail. Giving steroids alone to a child with an abscess or a tumour, or sending a child with transverse myelitis to the operating theatre, are the two errors the emergency MRI is designed to prevent. [1] [9]
What makes this group worth knowing in depth is that the modern antibody-led framework has transformed the inflammatory side of the fork. A transverse myelitis is no longer a single waste-basket diagnosis: it is now classified by its cause into idiopathic disease and the antibody-associated disorders - neuromyelitis optica spectrum disorder driven by aquaporin-4 IgG, myelin-oligodendrocyte-glycoprotein antibody-associated disease driven by MOG-IgG, and the spinal-cord attacks of multiple sclerosis - each with a different long-term treatment and a different prognosis. The general paediatrician's role is to secure the emergency MRI, begin the matched acute treatment, and hand over to neurosurgery or paediatric neurology with the cause already in flight. [3] [5]
Classification
The acute spinal cord syndromes are best classified by the single fork that the MRI resolves: is the lesion outside the cord, pressing on it, or inside the cord, inflaming it? The figure below lays out the two columns alongside the causes that fill each, with the emergency whole-spine MRI as the decision node that sits between them - because that one test is what a general paediatrician can act on at the first encounter, and it governs whether the child goes to the operating theatre or to a medical regimen. [1] [7]
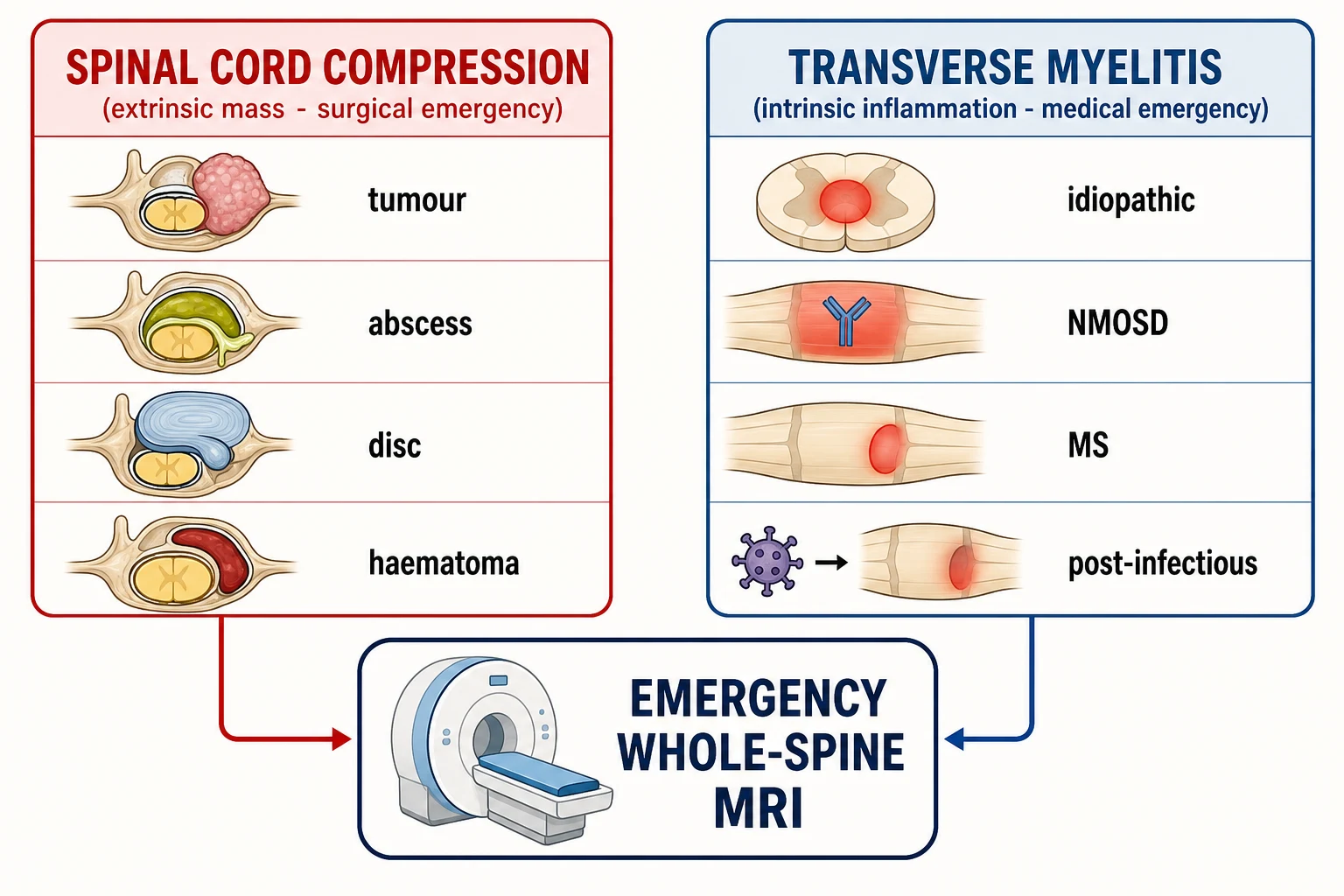
The compressive column is built around a structural lesion in the epidural or intradural extramedullary space. The commonest malignancy-related cause is an epidural tumour - in children, the primary paediatric cancers that metastasise or extend into the spinal canal: sarcomas (Ewing sarcoma, rhabdomyosarcoma), neuroblastoma, lymphoma (especially non-Hodgkin lymphoma and precursor B-cell lymphoblastic leukaemia), leukaemia (acute myeloid leukaemia forming a chloroma or granulocytic sarcoma), germ-cell tumours, and intradural intramedullary astrocytomas. A spinal epidural abscess is the infective compressive cause, dominated by Staphylococcus aureus and often arising from a contiguous discitis or vertebral osteomyelitis or by haematogenous spread. A traumatic or spontaneous epidural or intramedullary haematoma and an acute disc herniation complete the compressive column. [7] [10]
The inflammatory column is built around transverse myelitis, defined by the Transverse Myelitis Consortium Working Group 2002 criteria as an intrinsic inflammatory lesion of the cord that produces bilateral sensory, motor, or autonomic dysfunction with a clearly defined sensory level, excludes a compressive cause on imaging, demonstrates inflammation in the cord or the cerebrospinal fluid, and progresses to its worst point between four hours and twenty-one days from onset. Within it, the antibody-associated disorders are the named diseases: neuromyelitis optica spectrum disorder, driven by aquaporin-4 IgG and producing a longitudinally extensive lesion spanning three or more vertebral segments; myelin-oligodendrocyte-glycoprotein antibody-associated disease, driven by MOG-IgG and often producing an ADEM-like or concomitant-optic-neuritis phenotype in the young; and the spinal-cord attacks of multiple sclerosis, which are typically short, peripheral, and focal. Idiopathic acute transverse myelitis is the term reserved for the inflammatory cord lesion in which no cause is found. [1] [3]
The two columns at a glance - lesion site, defining test, first treatment, and urgency
- Spinal cord compression (extrinsic): a mass or collection outside the cord pressing on it. Defining test: emergency whole-spine MRI shows an extradural or extramedullary lesion displacing the cord. First treatment: dexamethasone plus surgical decompression within twenty-four to forty-eight hours, with radiotherapy for a radiosensitive tumour or intravenous antibiotics for an abscess. Urgency: surgical emergency; ambulation at presentation predicts outcome.
- Transverse myelitis (intrinsic): an inflammatory lesion within the cord substance. Defining test: MRI shows an intramedullary T2-hyperintense, often enhancing lesion with no compressive mass. First treatment: high-dose intravenous methylprednisolone 20 to 30 mg per kg per day to a maximum of 1 g per day for three to five days. Urgency: medical emergency; escalate to intravenous immunoglobulin or plasma exchange if steroid-refractory at forty-eight to seventy-two hours.
- Longitudinally extensive transverse myelitis: an intrinsic lesion spanning three or more vertebral segments, pointing to neuromyelitis optica spectrum disorder or myelin-oligodendrocyte-glycoprotein antibody-associated disease over multiple sclerosis. First treatment: methylprednisolone then early plasma exchange for the severe aquaporin-4-positive attack, and never a multiple-sclerosis drug before the antibody status is known. [1] [3]
Epidemiology & Risk Factors
Acute transverse myelitis is uncommon, with an estimated incidence of one to eight new cases per million persons per year across all ages and a substantial paediatric share, and in children the median age at onset is around seven to ten years with a mild female preponderance in some series. A preceding infection within the prior one to four weeks is reported in around half of paediatric cases - most often a non-specific viral upper-respiratory or gastrointestinal illness - and it is the post-infectious trigger that explains the temporal clustering after common childhood infections and, rarely, after vaccination. The general paediatrician meets transverse myelitis as an acute paraparesis in a previously well child, and the pre-test probability is raised by a recent illness, by a non-European ancestry, or by coexisting autoimmunity. [2] [3]
The epidemiology of the compressive side is shaped by the paediatric malignancies. In children, malignant spinal cord compression is far more often a primary paediatric cancer extending into the epidural space than an adult-style metastasis, and the commonest culprits are the small-round-blue-cell tumours and the sarcomas: Ewing sarcoma and other sarcomas, neuroblastoma in the younger child, non-Hodgkin lymphoma (the largest single histology in population-based series), and leukaemia presenting as a chloroma. The thoracic and thoracolumbar spine are most often involved because the canal is narrowest and the blood supply most tenuous there. A useful epidemiological point is that cord compression is the presenting feature of the malignancy in a substantial minority of children, so the first encounter may be in a child with no prior cancer diagnosis - which is why a high index of suspicion and an emergency MRI, not a cancer history, drive the workup. [10] [11]
The risk factors for a spinal epidural abscess reshape the pre-test probability and are worth holding as a cluster. Immunocompromise - from malignancy, chemotherapy, or a primary immune defect - diabetes, an indwelling vascular catheter, a recent spinal procedure or surgery, a skin or soft-tissue infection, and intravenous drug use all raise the prior probability of an abscess, and the commonest organism by a wide margin is Staphylococcus aureus, including methicillin-resistant strains. A fever with back pain and an elevated C-reactive protein in any of these hosts is an abscess until the MRI excludes it, because the abscess can compress and infarct the cord as fast as a tumour. [12]
The epidemiology at a glance
Pathophysiology
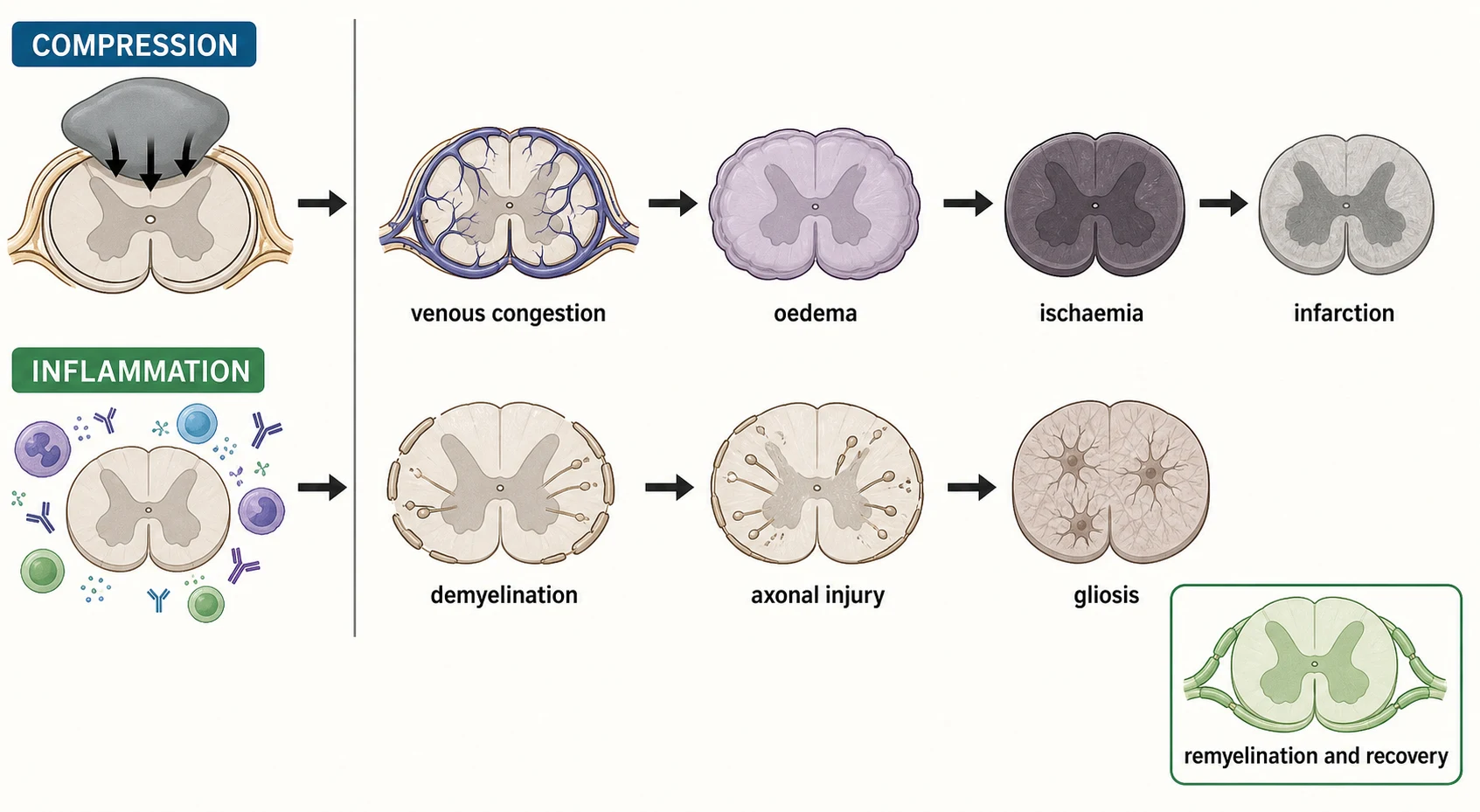
A compressive cord lesion is, at its core, a mechanical problem that converts through a vascular cascade into an irreversible one - and understanding the cascade is what makes the urgency rational rather than reflexive. An extradural mass first narrows the spinal canal and compresses the epidural venous plexus, producing venous congestion and cord oedema; at this stage the deficit is potentially reversible because the axons are intact. As the compression worsens, the arterial supply to the cord is compromised, and the cord becomes ischaemic; finally the cord infarcts, the axons die, and the deficit becomes permanent. The early oedematous phase is the salvageable window, and it is why a child who is still ambulatory - the cord is oedematous but not yet infarcted - can be rescued, while a child who is already paraplegic has often crossed into infarction. [7] [9]
The inflammatory side is a different cascade with the same endpoint. In transverse myelitis, an immune-mediated attack on the cord substance produces demyelination of the ascending and descending tracts, and in the more severe attacks it injures the underlying axons and leaves a gliotic scar. The mechanism of the attack is what separates the antibody-associated disorders, and it is why the antibody test governs the long-term treatment. In neuromyelitis optica spectrum disorder, aquaporin-4 IgG binds the water channel on astrocyte end-feet at the blood-cord barrier, recruiting complement and producing a longitudinally extensive, often necrotising lesion that is characteristically centred on the central cord and can leave a cavity. In myelin-oligodendrocyte-glycoprotein antibody-associated disease, MOG-IgG binds the myelin surface and produces a demyelinating lesion that often spares the axon, which explains the better recovery but the relapsing phenotype when the antibody persists. [3] [5]
Multiple sclerosis sits as a third biology in the inflammatory column. The spinal-cord attack of multiple sclerosis is T-cell- and B-cell-driven, producing the classic sharply demarcated demyelinated plaque that is typically short (one or two segments), peripheral, and focal rather than longitudinally extensive - a pattern that, combined with the periventricular brain lesions and the cerebrospinal-fluid oligoclonal bands, supports the diagnosis under the 2017 McDonald criteria. The paediatric disease is conspicuously more inflammatory than its adult counterpart, with more frequent spinal involvement and a higher relapse rate. Holding the lesion-length distinction in mind - longitudinally extensive points to NMOSD or MOGAD, short and focal points to MS - is one of the highest-yield reasoning steps in the topic. [3] [6]
Clinical Presentation
The presenting complaint is back pain with a neurological deficit, and the pattern of the deficit follows the cord segment involved. The classic sequence of a compressive lesion runs in a fixed and examinable order: back pain first, then radicular pain in a dermatomal band, then motor weakness progressing from distal to proximal and from one leg to both, then a sensory level, and finally sphincter disturbance with urinary retention and constipation. The pain of malignancy has a tell-tale quality - it is often nocturnal, waking the child from sleep, and is worse lying flat, which distinguishes it from mechanical back pain that eases at rest. Sphincter loss is a late and ominous sign, and its presence tells you the compression is far advanced. [7] [8]
Transverse myelitis presents with the same core features - bilateral leg weakness, a sensory level, sphincter disturbance, and back pain - but evolving over hours to days rather than weeks, and often after a recent infection. The weakness is typically ascending and symmetric at the onset, a sensory level is usually clearly definable on the trunk, and urinary retention is common. The bedside picture is clinically indistinguishable from a compressive cord syndrome, which is exactly why the two cannot be separated without the MRI - and why the rule that the MRI is never delayed for bloods or a lumbar puncture is absolute. A transverse myelitis that is part of neuromyelitis optica spectrum disorder may declare itself with the severe bilateral optic neuritis or the area-postrema syndrome of intractable hiccups and vomiting that complete the NMOSD core, and a MOGAD myelitis is often accompanied by optic neuritis in a child. [2] [3]
The young child presents atypically, and this is where the diagnosis is hardest and the MRI most important. An infant or toddler may refuse to walk, become irritable, hold the back or neck rigid (torticollis), or present with abdominal pain or acute urinary retention rather than a complaint the clinician can localise to the spine. A verbal young child may not describe a sensory level clearly, and the first objective sign may be a refusal to bear weight or an unexplained retention. The safeguard in the young is a low threshold to scan: a child who refuses to walk or who retains urine without an obvious explanation is imaged, not observed. [2] [10]
Differential Diagnosis
The first and most consequential differential is between a compressive and an inflammatory lesion, and it is settled by the MRI. But within each column a focused differential must be held in mind, because each compressive cause carries a different treatment and each inflammatory cause a different long-term drug. The compressive differential comprises the malignant epidural tumour, the epidural abscess, the disc herniation, and the epidural or intramedullary haematoma - and the MRI pattern, the tempo, and the host tell them apart. A mass with vertebral body destruction in a child with a known cancer is a malignancy; an epidural collection with discitis and vertebral body signal change and rim enhancement in a febrile host is an abscess; a focal posterior disc fragment in a teenager after trauma is a disc; and a biconvex epidural collection in a coagulopathic or recently-traumatised child is a haematoma. [7] [12]
The inflammatory differential is the antibody-associated family plus the systemic and post-infectious causes. Idiopathic acute transverse myelitis is the label reserved for the inflammatory cord lesion in which no cause is found; neuromyelitis optica spectrum disorder, myelin-oligodendrocyte-glycoprotein antibody-associated disease, and multiple sclerosis are the antibody-associated diseases; and systemic lupus erythematosus, sarcoidosis, and the post-infectious and para-infectious myelitides complete the medical list. The distinction matters because each carries a different long-term treatment - a multiple-sclerosis drug for MS, a NMOSD-specific drug for NMOSD, maintenance only if relapsing for MOGAD - and the cardinal avoidable harm is starting a multiple-sclerosis disease-modifying therapy before the aquaporin-4 and MOG antibody status is known. [3] [4]
A focused differential also includes the non-cord causes of acute paralysis, because the cord is not the only structure that fails acutely. Guillain-Barre syndrome produces an ascending, symmetric, flaccid paralysis with areflexia and no sensory level, and it is the great mimic that the bedside examination - the absent reflexes, the absence of a sensory level, and the peripheral pattern - is meant to separate from a cord lesion. Acute flaccid myelitis, driven by enteroviruses, produces an asymmetric flaccid weakness with a grey-matter lesion on MRI. A vascular event - an infarct of the anterior spinal artery, or an arteriovenous malformation - produces a sudden deficit, and a spinal-cord concussion or SCIWORA (spinal cord injury without radiographic abnormality, commoner in the young child due to ligamentous laxity) enters the traumatic differential. The point is not to memorise every mimic but to hold the discipline of the emergency MRI before committing to a label. [1] [2]
Clinical & Bedside Assessment
The single most informative bedside act is to establish the tempo, the focality, and the presence of a sensory level. Ask exactly when the child was last well, whether there was a preceding illness, how fast the deficit evolved, and whether there is back pain and what its quality is. A subacute or progressive course with nocturnal pain raises a malignancy; a febrile course in an at-risk host raises an abscess; an acute or post-infectious course raises an inflammatory transverse myelitis. The presence of a clearly defined sensory level on the trunk localises the lesion to the cord and is the bedside finding that converts a vague weakness into a cord emergency warranting the emergency MRI. [1] [7]
Three questions frame every assessment. First, is there back pain, and what is its quality - nocturnal and worse lying flat raises malignancy, and febrile with local spinal tenderness raises infection. Second, is there a motor deficit, and is it fitting a cord distribution (a paraparesis, possibly with a sensory level) or a peripheral distribution (an ascending flaccid areflexic weakness)? Third, is there sphincter involvement - acute urinary retention, a distended palpable bladder, faecal incontinence, or reduced anal tone - because sphincter loss is a late and ominous sign of an established cord lesion. A combination of motor, sensory, and autonomic deficit referable to one cord segment is the pattern that mandates the scan. [2] [8]
The examination is then directed and recorded with the cord level in mind. Assess ambulation first, because ambulation at presentation is the strongest predictor of outcome and the marker of disease progression; a child who was walking yesterday and is not today is progressing. Examine the motor power in the legs, the tone, and the reflexes: a flaccid paraparesis with absent reflexes and a distended bladder is spinal shock, the acute phase of a severe cord lesion before the upper-motor-neuron signs emerge; a hyperreflexic paraparesis with upgoing plantars is the evolved cord lesion. Map the sensory level on the trunk by testing pinprick and light touch from below upward, because the level localises the lesion to a vertebral segment. Check anal tone and perform a post-void bladder scan. The discriminating cord-level signs localise the lesion and justify the emergency MRI before any test is sent. [1] [7]
Investigations
The investigation strategy is built around one principle: the emergency whole-spine MRI with gadolinium is the single critical investigation and the rate-limiting step, and it is performed without waiting for bloods or a cerebrospinal-fluid analysis when a cord syndrome is suspected. The MRI is requested the moment a cord syndrome is suspected, performed as an emergency within hours, and read by a radiologist with the clinical question stated - is there a compressive lesion needing surgery? An extradural or extramedullary mass displacing the cord is a compressive lesion; an intramedullary T2-hyperintense, swollen, often-enhancing lesion is an inflammatory transverse myelitis; and the lesion length and pattern then point to the cause. [1] [7]
The compressive lesion patterns are distinct and examinable. A malignant epidural tumour shows a mass in the epidural space, often with vertebral body destruction or replacement and contrast enhancement, and frequently a paravertebral soft-tissue component extending through the neural foramen (classic for neuroblastoma and lymphoma). An epidural abscess shows a collection in the epidural space, often with high signal on T2, rim enhancement on post-contrast sequences, and adjacent discitis with vertebral body signal change. A disc herniation shows a focal posterior disc fragment indenting the cord or the thecal sac. A haematoma shows a biconvex epidural collection with signal that depends on its age. In the inflammatory column, a transverse myelitis shows an intramedullary lesion that is T2-hyperintense and swollen, often with patchy gadolinium enhancement, and a longitudinally extensive lesion spanning three or more vertebral segments raises neuromyelitis optica spectrum disorder and myelin-oligodendrocyte-glycoprotein antibody-associated disease over multiple sclerosis. [3] [12]
The parallel workup
- Recognise the cord syndrome - back pain plus a motor, sensory, or sphincter deficit, and the presence of a spinal sensory level.
- Emergency whole-spine MRI with gadolinium - the rate-limiting step; performed within hours and never delayed for bloods. State the clinical question: is there a compressive lesion?
- If a compressive lesion - start dexamethasone, refer to neurosurgery and oncology or infectious diseases in parallel, and plan decompression or drainage within twenty-four to forty-eight hours.
- If an inflammatory lesion - send the antibody panel (serum AQP4-IgG and MOG-IgG by live cell-based assay) and perform a lumbar puncture for cerebrospinal-fluid analysis (cell count, protein, glucose, oligoclonal bands on a paired serum sample, and an infective screen) only after a compressive lesion is excluded.
- Ancillary tests - full blood count and film, inflammatory markers, coagulation, a connective-tissue and infective screen, and vitamin B12 and copper to exclude the metabolic mimics. [1] [3]
The cerebrospinal fluid is examined only after a compressive lesion is excluded on the MRI, because performing a lumbar puncture below a complete cord block risks neurological deterioration, and because the inflammatory pattern is what the cerebrospinal fluid adds. A pleocytosis, an elevated protein, and oligoclonal bands unique to the cerebrospinal fluid (absent from a paired serum sample) support an inflammatory transverse myelitis and can, in the 2017 McDonald criteria, substitute for dissemination in time in the diagnosis of multiple sclerosis. The Transverse Myelitis Consortium 2002 criteria require demonstration of inflammation - a cerebrospinal-fluid pleocytosis, an elevated immunoglobulin-G index, or gadolinium enhancement on the MRI - and if none is present at the first evaluation, the MRI and the lumbar puncture are repeated two to seven days later. [1] [6]
Management — Resuscitation
When the cord syndrome presents as an acute paraparesis, a rapidly progressive deficit, or acute urinary retention, the response is resuscitation first and the diagnostic workup in parallel. Secure the airway, breathing, and circulation; provide analgesia; catheterise the bladder for retention and monitor the residual; attend to pressure areas and start venous thromboembolism prophylaxis in the immobile child; and move immediately to the emergency whole-spine MRI. The general paediatrician owns the first hours, with neurosurgery, oncology, infectious diseases, and paediatric neurology taking over as the cause firms. [7] [8]
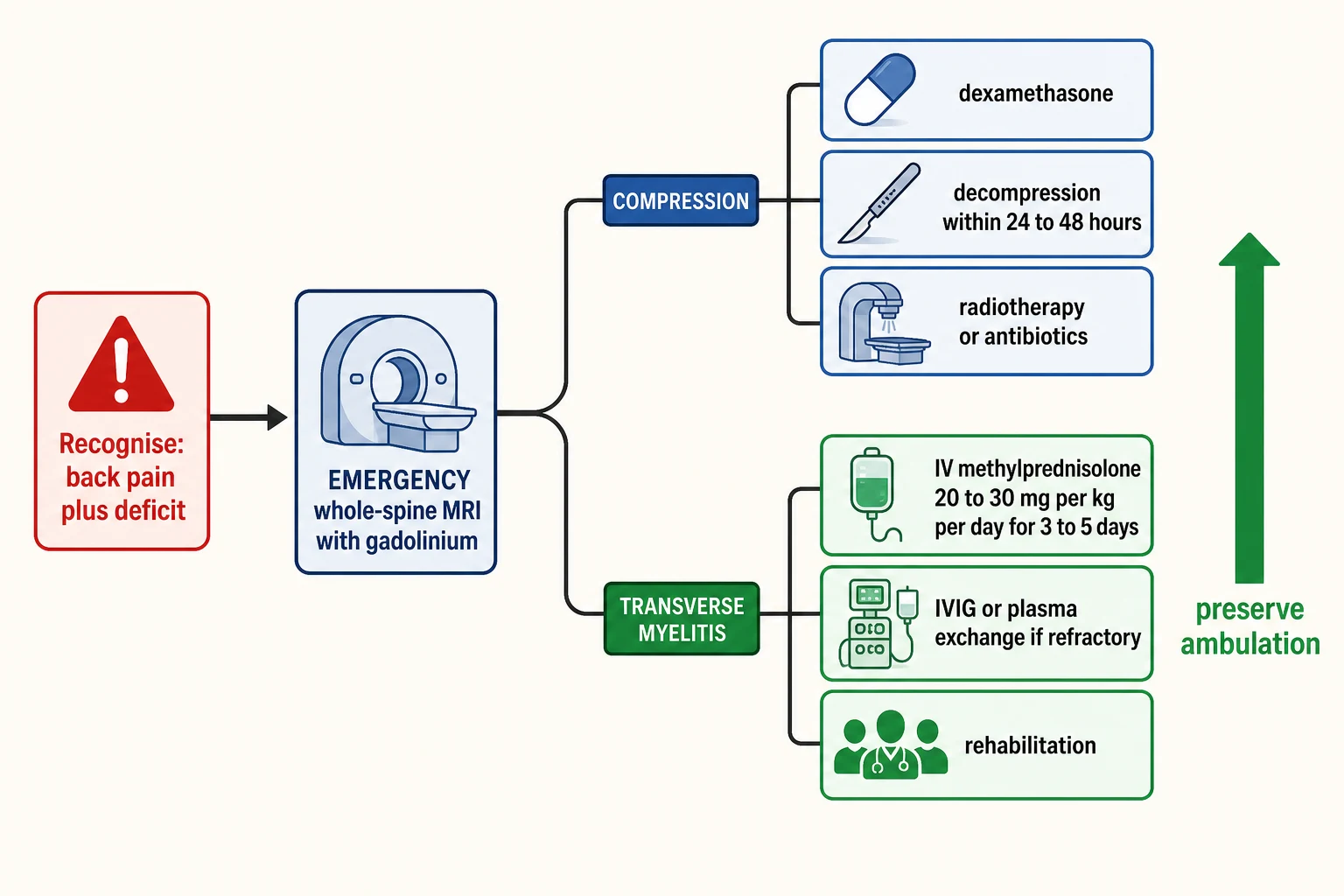
The corticosteroid is matched to the suspected cause and started before the final diagnosis is confirmed. For malignant spinal cord compression, dexamethasone is started immediately to reduce cord oedema and to preserve neurological function; the adult National Institute for Health and Care Excellence benchmark is a loading dose of 16 mg followed by 16 mg per day (in divided doses), continued until definitive treatment and then tapered, and in children the dose is weight-based and set by the local paediatric-oncology and neurosurgery protocol. For inflammatory transverse myelitis, the first-line acute therapy is high-dose intravenous methylprednisolone. The standard paediatric regimen is 20 to 30 mg per kg per day to a maximum of 1 g per day, given over three to five days, and it is begun as soon as infection is reasonably excluded, with the workup in parallel. [3] [8]
Acute corticosteroid regimens for the cord syndrome
Escalation is the rule for the severe or steroid-refractory inflammatory event. If the deficit has not improved after forty-eight to seventy-two hours of high-dose corticosteroids, the next step is intravenous immunoglobulin at a total dose of 2 g per kg (given over two to five days) or plasma exchange, typically five to seven exchanges of one to one-and-a-half plasma volumes on alternate days. Plasma exchange is favoured for the severe aquaporin-4-IgG-positive attack because it removes the pathogenic antibody directly. For the compressive lesion, the escalation is not more steroids but surgery - and the surgical decompression is timed within twenty-four to forty-eight hours of the loss of ambulation, because beyond that window the cord has often infarcted. [3] [9]
Management — Definitive & Stepwise
Definitive management means naming the cause on the MRI and matching the treatment to it, because the compressive and the inflammatory pathways diverge completely and the timing of each is unforgiving. The figure below lays out the staged emergency pathway from the recognition of the red flags, through the emergency whole-spine MRI decision node, to the matched compression pathway on one side and the matched inflammatory pathway on the other, converging on the single goal that frames the whole topic - the preservation of ambulation. [7] [9]
For the compressive lesion, definitive treatment is surgical decompression plus removal or drainage of the cause, with the adjuncts matched to the pathology. A malignant epidural tumour is decompressed and stabilised surgically where feasible, and a radiosensitive tumour (such as lymphoma, neuroblastoma, or germ-cell tumour) is treated with urgent radiotherapy or chemotherapy, sometimes as the primary modality when the tumour is exquisitely sensitive or when surgery is not feasible. An epidural abscess is drained surgically and treated with targeted intravenous antibiotics, typically for four to six weeks, guided by the culture (Staphylococcus aureus most often). The decompression is timed within twenty-four to forty-eight hours of the loss of ambulation, and ambulation at presentation is the strongest predictor of postoperative function. [7] [10]
For the inflammatory lesion, definitive treatment is the acute corticosteroid course followed by a maintenance strategy matched to the confirmed antibody cause. For idiopathic acute transverse myelitis that is monophasic, no maintenance therapy is required beyond the acute attack treatment and surveillance. For neuromyelitis optica spectrum disorder, the maintenance therapy is a NMOSD-specific drug and never a multiple-sclerosis drug - rituximab or another anti-CD20 agent, satralizumab (an interleukin-6 receptor blocker), a complement blocker (eculizumab, ravulizumab), mycophenolate mofetil, or azathioprine. For myelin-oligodendrocyte-glycoprotein antibody-associated disease, maintenance immunotherapy is reserved for the relapsing course. For multiple sclerosis, a high-efficacy disease-modifying therapy is started early. The safeguard across all three is the antibody result before any long-term drug. [3] [5]
Rehabilitation is begun early and runs alongside the medical and surgical therapy rather than after it. Physiotherapy for strength and mobility, occupational therapy for function, a bladder-and-bowel plan for the neurogenic bladder and bowel, pressure-area and thromboembolism prophylaxis, neuropathic-pain management, and psychological and educational support are part of management from the first week. The care plan is multidisciplinary and coordinated by the general paediatrician, with paediatric neurology, neurosurgery, oncology or infectious diseases, and rehabilitation sharing the long view. [2] [8]
Specific Subtypes & Scenarios
Malignant spinal cord compression is the subtype that defines the urgency of the topic, and every candidate must know its paediatric pattern. A child with a known malignancy - or, in a substantial minority, a child in whom the compression is the presenting feature of the cancer - develops back pain, then a progressive paraparesis, then a sensory level, then sphincter loss. The causative tumours are the paediatric primaries: sarcomas (Ewing sarcoma and rhabdomyosarcoma), neuroblastoma in the younger child, non-Hodgkin lymphoma, leukaemia presenting as a chloroma or granulocytic sarcoma, germ-cell tumours, and intradural astrocytomas. The management is dexamethasone started immediately, an emergency MRI, and surgical decompression plus radiotherapy or chemotherapy matched to the tumour type, timed within twenty-four to forty-eight hours of the neurological deficit. Population-based paediatric series confirm that the presenting neurological status is the dominant determinant of the long-term motor outcome and of survival. [10] [11]
A spinal epidural abscess is the infective compressive subtype and the one where the host clues drive the suspicion. The classic triad of back pain, fever, and a neurological deficit is present in only a minority of patients, which is why each component must be sought actively and the absence of one must not reassure. The risk factors are immunocompromise, diabetes, an indwelling vascular catheter, a recent spinal procedure or surgery, a skin or soft-tissue infection, and intravenous drug use, and Staphylococcus aureus is the predominant organism, including methicillin-resistant strains. The management is surgical drainage of the abscess plus intravenous antibiotics for four to six weeks, guided by the culture, and the decompression is timed on the same principle as the malignant lesion - within twenty-four to forty-eight hours of a neurological deficit. [12]
Longitudinally extensive transverse myelitis is the inflammatory subtype that the antibody panel resolves, and it is the one in which the wrong long-term drug harms. A lesion spanning three or more vertebral segments raises neuromyelitis optica spectrum disorder (aquaporin-4 IgG positive) and myelin-oligodendrocyte-glycoprotein antibody-associated disease (MOG-IgG positive) over multiple sclerosis, which is typically short and focal. The acute attack is treated with high-dose methylprednisolone, and plasma exchange is favoured early for the severe aquaporin-4-positive attack because it removes the pathogenic antibody directly. The cardinal safety point is unchanged from the wider demyelinating topic: a multiple-sclerosis disease-modifying therapy must never be started before the aquaporin-4 and MOG antibody status is known, because several of those drugs worsen NMOSD. [3] [4]
Traumatic paediatric spinal cord injury, including SCIWORA (spinal cord injury without radiographic abnormality), enters the acute-paralysis differential and is worth naming precisely. SCIWORA is commoner in the young child because the spinal ligaments are lax and the vertebral column can stretch and injure the cord without a fracture visible on plain radiographs or computed tomography; modern MRI now shows the cord lesion that was previously occult. A child with neck or back trauma and a neurological deficit is immobilised, imaged with an emergency MRI, and managed with the neurosurgical and spinal-injury team. The general paediatrician's role is to recognise the cord injury, immobilise the spine, and avoid the secondary injury that hypotension and hypoxia cause. [1] [2]
Complications & Pitfalls
The most consequential complication is irreversible neurological loss, and it is almost always the consequence of delay. A delayed emergency MRI, a delayed decompression, or a delayed steroid course allows the oedematous cord to progress to infarction in the compressive case and allows the inflammatory attack to injure axons in the myelitis case, and the result is a permanent paraparesis, a neurogenic bladder and bowel, and the lifelong burden of a cord lesion. The safeguard is the rule that the emergency MRI is never delayed for bloods or a lumbar puncture, and that the decompression is timed within twenty-four to forty-eight hours of the deficit. [7] [9]
A second and classic pitfall is attributing an acute paralysis to Guillain-Barre syndrome and sending the cerebrospinal fluid rather than the MRI. The two share an acute ascending weakness, but the cord lesion declares itself with a sensory level, with sphincter disturbance, and with an upper-motor-neuron or spinal-shock pattern that a peripheral neuropathy does not produce - and the test that separates them is the MRI, not the cerebrospinal fluid. A related pitfall is performing a lumbar puncture below a complete cord block, which risks neurological deterioration; the lumbar puncture is done only after the MRI has excluded a compressive lesion. [1] [2]
A third pitfall is over-reliance on a single antibody result or on adult dosing. A negative MOG-IgG in the acute phase does not exclude myelin-oligodendrocyte-glycoprotein antibody-associated disease if the assay is insensitive or the titre is low, and the assay must be a live cell-based assay to avoid false positives. Applying the adult dexamethasone dose to a child is a dosing error: the paediatric dose is weight-based and set by the local protocol. A fourth pitfall is underestimating the long-term complications - neuropathic pain, spasticity and contractures, neurogenic bladder and bowel, osteoporosis, and the psychological and educational burden - which are addressed by the multidisciplinary team from the first week, not deferred to rehabilitation after the acute event. [3] [5]
Prognosis & Disposition
Prognosis in a compressive cord lesion is determined above all by the neurological status at presentation, and this is the single most examinable prognostic fact in the topic. A child who is ambulatory at presentation is likely to remain ambulatory after treatment, while a child who presents paraplegic rarely recovers ambulation - which is why ambulation at presentation is the strongest predictor of both motor outcome and, in malignant compression, of survival. The interval from symptom onset to treatment, the tumour type and its radiosensitivity, and the completeness of the deficit at the time of decompression all modify the outcome, but the presenting motor status dominates. This fact is what makes the emergency MRI and the twenty-four-to-forty-eight-hour decompression window rational rather than arbitrary. [7] [10]
Prognosis in idiopathic acute transverse myelitis is more favourable than the compressive lesion but is far from uniformly good. Around one-third to a half of children recover well, a substantial minority are left with a residual motor or sphincter deficit, and a smaller group remain severely disabled. The predictors of a poorer outcome include the severity of the deficit at the nadir, the presence of spinal shock, sphincter involvement, and a longitudinally extensive lesion - the last of which should redirect the clinician to the antibody panel and to the more guarded prognosis of neuromyelitis optica spectrum disorder. The antibody-associated disorders carry their own prognosis: generally favourable attack-by-attack recovery but a relapsing course in myelin-oligodendrocyte-glycoprotein antibody-associated disease, severe attacks with poor recovery in neuromyelitis optica spectrum disorder, and a relapsing course in multiple sclerosis. [2] [3]
Disposition is structured around the tertiary paediatric neurology, neurosurgery, and oncology or infectious-diseases services, with the general paediatrician coordinating the multidisciplinary team and holding the whole child. The compressive lesion is managed by neurosurgery with oncology or infectious diseases; the inflammatory lesion is managed by paediatric neurology and neuroimmunology; and rehabilitation - physiotherapy, occupational therapy, a bladder-and-bowel plan, pressure-area and thromboembolism prophylaxis, neuropathic-pain management, and neuropsychological and educational support - is begun early and runs in parallel. A structured follow-up with serial MRI for the inflammatory lesions, an individualised education plan, and a transition plan to adult services for the chronic cases complete the disposition. [5] [8]
Special Populations
The approach differs across the age span and across the host. The young child and infant present atypically - a refusal to walk, irritability, torticollis, abdominal pain, or acute urinary retention rather than a complaint the clinician can localise - and this is where the diagnosis is hardest and the emergency MRI most important; a low threshold to scan, rather than to observe, is the safeguard. The adolescent presents more classically and, in the inflammatory column, may declare the relapsing course of multiple sclerosis or the severe attack of neuromyelitis optica spectrum disorder, in which the antibody status and the maintenance strategy dominate the long-term plan. [2] [6]
The child with a known malignancy, or who is immunocompromised, carries a higher prior probability of a malignant compression or an epidural abscess, and the consultation reframes the workup toward the compressive side of the fork. Early involvement of paediatric oncology and infectious diseases, a dexamethasone course, and an emergency MRI are the threshold actions. For the rural, remote, and disadvantaged child, equitable and timely access to an emergency whole-spine MRI, to neurosurgery, and to rehabilitation is a real challenge, concentrated as those services are in tertiary centres; the retrieval network and telehealth are the practical pathway, and the principle is to transfer the child and the imaging question together rather than to wait for a delayed local scan. [8] [10]
The technology-dependent and complex-chronic child, and the Indigenous and migrant-refugee child, need a culturally safe and coordinated pathway that addresses the lifelong burden of a cord lesion. A neurogenic bladder managed by clean intermittent catheterisation, a wheelchair and seating service, a home and school modification plan, and a structured transition to adult spinal-injury or neurology services are part of management, not afterthoughts. The general paediatrician holds the whole child and coordinates the team across the lifespan of the diagnosis. [5] [7]
Evidence, Guidelines & Regional Differences
The conceptual backbone of the topic is a set of diagnostic frameworks and management guidelines that let the clinician act before the confirmatory cause returns. The Transverse Myelitis Consortium Working Group 2002 criteria define idiopathic acute transverse myelitis on the bilateral signs, the clearly defined sensory level, the exclusion of a compressive cause on imaging, the demonstration of inflammation, and the progression to the nadir between four hours and twenty-one days. The IPND 2015 criteria confirm neuromyelitis optica spectrum disorder on the aquaporin-4 IgG status and the core clinical characteristics, and the MOGAD Panel 2023 criteria confirm myelin-oligodendrocyte-glycoprotein antibody-associated disease on a clinical event plus serum MOG-IgG by a cell-based assay. The 2017 McDonald criteria extend the multiple-sclerosis diagnosis to the spinal attacks of MS. [1] [6]
In Australia and Aotearoa New Zealand, paediatric neurology, neurosurgery, and oncology services and the live cell-based antibody assays are concentrated in tertiary paediatric centres, with regional and remote access via retrieval networks and telehealth. The National Institute for Health and Care Excellence metastatic spinal cord compression guideline (CG75), which anchors the dexamethasone 16 mg loading-then-maintenance regimen and the decompression window, is widely adopted in spirit, but the paediatric dexamethasone dose is weight-based and set by the local paediatric-oncology and neurosurgery protocol. Emergency whole-spine MRI access is available in tertiary centres and via retrieval, and funded access to the NMOSD-specific monoclonal antibodies is governed by national and jurisdictional programmes. State the local protocol and the local funded pathway rather than assuming a universal regimen, secure the MRI on the phenotype, and involve the tertiary team early. [8] [9]
The strength of the evidence varies across the topic. The evidence for high-dose corticosteroids as first-line acute therapy for transverse myelitis, and for the decompression window in malignant compression, is mature and consistent. The optimal dexamethasone regimen for malignant cord compression is still debated: the historical high-dose regimen (a 96 mg bolus followed by 96 mg per day, derived from older trials) has been compared with the moderate-dose regimen (the 16 mg loading and maintenance of the modern guidelines), and the latter is favoured for a better side-effect profile at comparable efficacy, but the paediatric dose remains weight-based and protocol-dependent. Where the evidence is weaker - the optimal maintenance strategy in relapsing myelin-oligodendrocyte-glycoprotein antibody-associated disease - the choice is individualised by relapse risk. [8] [9]
Exam Pearls
Remember the two principles that frame every consultation. First, secure the emergency whole-spine MRI the moment a cord syndrome is suspected, because the imaging - not the history and not the bloods - resolves the compression-versus-inflammation fork, and the fork decides whether the child goes to the operating theatre or to a medical regimen. Second, treat in parallel, not in sequence: dexamethasone and neurosurgical-oncological referral for the compressive lesion with the decompression timed within twenty-four to forty-eight hours, and high-dose methylprednisolone for the inflammatory lesion with escalation to intravenous immunoglobulin or plasma exchange when steroid-refractory. Ambulation at presentation is the single predictor of outcome, and the antibody status governs the long-term treatment of the inflammatory lesions - never start a multiple-sclerosis drug before the aquaporin-4 and MOG antibody results are known. [1] [9]
Self-test: a seven-year-old with nocturnal back pain and a dragging leg
A previously well seven-year-old wakes at night with thoracic back pain that is worse lying flat, and by the next morning is dragging her left leg and cannot pass urine. On examination she has a sensory level at T10, a flaccid left leg, and a distended bladder. What is the single most important next investigation, what is the most likely diagnosis if it shows an extradural mass with vertebral destruction, and what is the immediate treatment? [1] [7]
Answer: The single most important next investigation is an emergency whole-spine MRI with gadolinium, performed within hours and never delayed for bloods or a lumbar puncture. An extradural mass with vertebral body destruction in a previously well child makes a malignant spinal cord compression - in this age group commonly a sarcoma (Ewing sarcoma, rhabdomyosarcoma), a neuroblastoma, a lymphoma, or a leukaemic chloroma - the most likely diagnosis, and the immediate treatment is dexamethasone started at once (weight-based per the local paediatric-oncology and neurosurgery protocol, with the adult NICE benchmark of 16 mg loading then 16 mg per day), with neurosurgical and oncological referral in parallel and a plan for surgical decompression within twenty-four to forty-eight hours. Ambulation at presentation is the strongest predictor of her eventual motor outcome, which is why the MRI and the referral are not delayed. [7] [10]
References
- [1]Transverse Myelitis Consortium Working Group. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology, 2002.PMID 12236201
- [2]Pidcock FS, Krishnan C, Crawford TO, Salorio CF, Trovato M, Kerr DA, et al. Acute transverse myelitis in childhood: center-based analysis of 47 cases. Neurology, 2007.PMID 17470749
- [3]Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology, 2015.PMID 26092914
- [4]Banwell B, Bennett JL, Marignier R, Kim HJ, Brilot F, Flanagan EP, et al. Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria. Lancet Neurol, 2023.PMID 36706773
- [5]Marignier R, Hacohen Y, Cobo-Calvo A, Probstel AK, Aktas O, Alexopoulos H, et al. Myelin-oligodendrocyte glycoprotein antibody-associated disease. Lancet Neurol, 2021.PMID 34418402
- [6]Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol, 2018.PMID 29275977
- [7]Prasad D, Schiff D. Malignant spinal-cord compression. Lancet Oncol, 2005.PMID 15629272
- [8]Savage P, Sharkey R, Kua T, Foley M, Melcher H, Eaton N, et al. Malignant spinal cord compression: NICE guidance, improvements and challenges. QJM, 2014.PMID 24336849
- [9]Loblaw DA, Laperriere NJ. Emergency treatment of malignant extradural spinal cord compression: an evidence-based guideline. J Clin Oncol, 1998.PMID 9552073
- [10]Ertekin M, Temuroglu A, Aksoy GR, Karaborklu O, Caglar HD, Arslan M, et al. Spinal cord compression at initial presentation in pediatric oncology patients: neurological sequelae and survival outcomes. J Neurooncol, 2026.PMID 41826763
- [11]Riquelme A, Werner J, Zimmermann M, Borde J, Stahnke M, Rehe K, et al. Non-Hodgkin lymphoma presenting with spinal cord compression: A population-based analysis of the NHL-BFM study group. Pediatr Blood Cancer, 2024.PMID 38961598
- [12]Darouiche RO. Spinal epidural abscess. N Engl J Med, 2006.PMID 17093252