Paeds · neurology-neurodisability-and-neuromuscular
Status epilepticus
Also known as Convulsive status epilepticus · Prolonged seizure · Refractory status epilepticus · Non-convulsive status epilepticus · Established status epilepticus
Fellowship guide to status epilepticus in children. Covers the ILAE operational definition with the t1 and t2 time points, the classification into early, established, and refractory phases, the time-dependent pharmacodynamic shift of GABA-A receptor internalisation and glutamate receptor recruitment that erodes benzodiazepine efficacy, the APLS stepwise pathway from first-line benzodiazepines through second-line levetiracetam or fosphenytoin to refractory rapid sequence intubation and continuous infusion, the ConSEPT, EcLiPSE, and ESETT trials comparing levetiracetam with phenytoin across the age range, the reversible causes including hypoglycaemia and electrolyte disturbance, the role of continuous EEG after paralysis, and new-onset refractory status epilepticus.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who has been convulsing for more than five minutes is in status epilepticus, and the job is to stop the seizure with drugs, not to stand and watch. Status epilepticus is a continuous seizure, or a run of seizures without recovery in between, that lasts long enough to threaten the brain. The International League Against Epilepsy gave the condition an operational definition that turns the bedside clock into a trigger for action, and every fellow should be able to recite it. [1]
The ILAE definition rests on two time points. The first, called t1, is the duration beyond which the seizure is unlikely to stop on its own, set at five minutes for a convulsive seizure. The second, called t2, is the duration beyond which the seizure can begin to injure neurons, set at thirty minutes for a convulsive seizure. The window between t1 and t2 is the period in which treatment must work, because once a seizure crosses t2 the risk of lasting harm climbs steeply. [1]
Three facts make this topic central to the paediatric exam. The diagnosis is a clock, and five minutes of convulsion is the trigger to treat. The treatment is stepwise and time-critical, moving from benzodiazepine to second-line agent to anaesthetic infusion as the seizure persists. And the determinant of outcome is the speed and adequacy of early treatment, because the longer a seizure runs the harder it becomes to stop. Abend and Loddenkemper set out the principles that govern paediatric status epilepticus management. [8]
Classification
The ILAE classifies status epilepticus along two practical axes, and both matter at the bedside. The first axis is the seizure type, separating convulsive from non-convulsive status, because a convulsion demands immediate visible action while a non-convulsive state demands suspicion and an EEG. The second axis is time, separating the early, established, and refractory phases, because each phase carries its own drug ladder. [1]
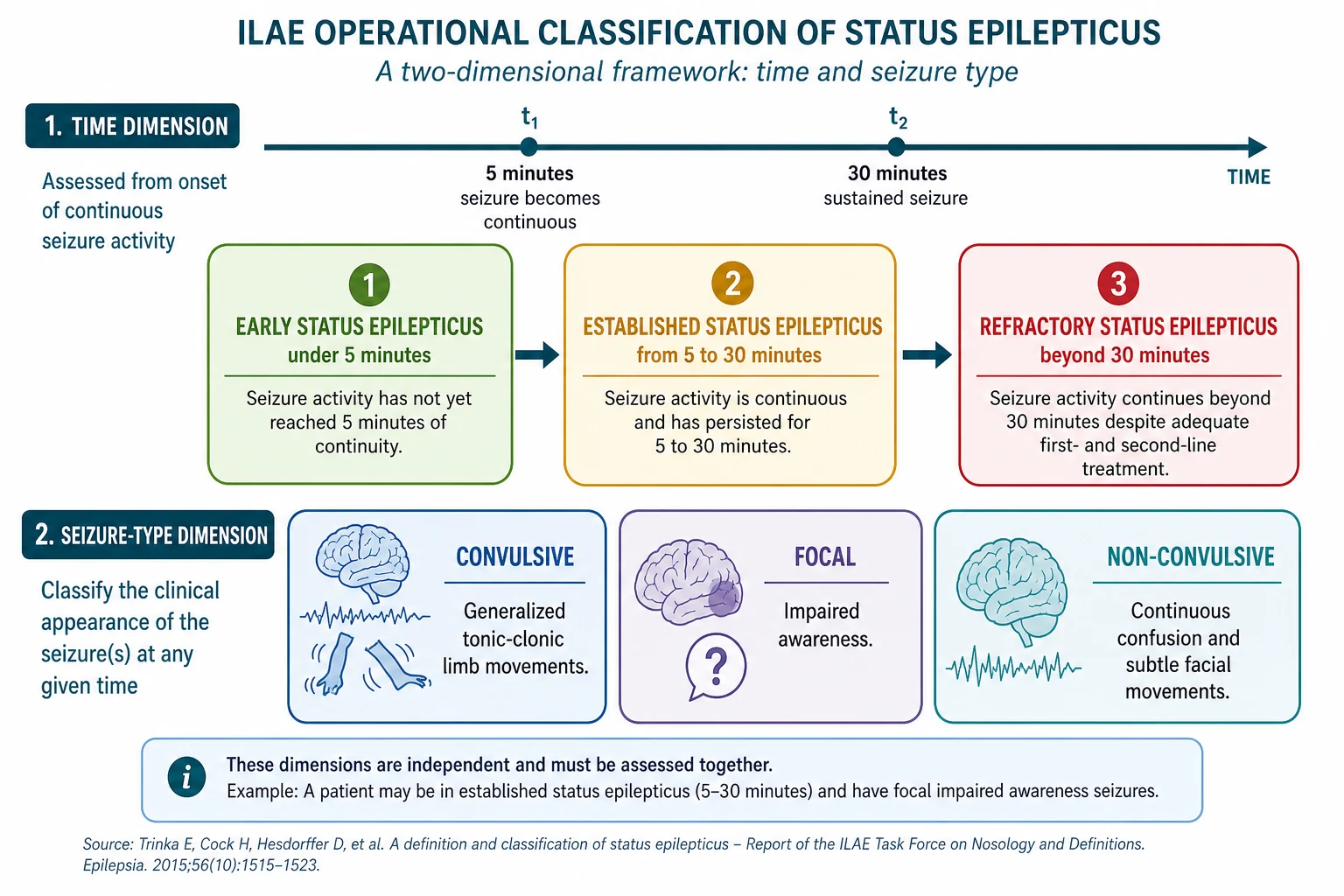
Convulsive status epilepticus is the form that brings the child to the emergency department, with overt tonic-clonic movements that are hard to miss. The convulsive form is the one that carries the acute cardiorespiratory risk, because the sustained muscle activity generates acidosis, hyperthermia, and airway compromise. Most exam scenarios and most of the trial evidence address the convulsive form. [8]
Non-convulsive status epilepticus is the hidden form, presenting as continuous confusion, subtle twitching of a limb or the face, or failure to recover after a convulsion has been controlled. It is suspected whenever a child fails to return to baseline within an hour of a seizure, and it is confirmed only by EEG. The non-convulsive form is common in intensive care, where a paralysed and sedated child can still be seizing in the brain, which is why continuous EEG monitoring is mandatory after intubation. [11]
The time axis divides the course into three phases. Early status epilepticus runs from seizure onset to the t1 threshold of about five minutes, and it is the window in which a benzodiazepine works best. Established status epilepticus sits between five and thirty minutes, when a second-line agent is added. Refractory status epilepticus is ongoing seizure beyond thirty minutes or despite adequate first and second-line therapy, and it is the threshold for anaesthetic escalation. [2]
Epidemiology & Risk Factors
Status epilepticus is the commonest neurological emergency of childhood, and most cases occur in children who are already known to have epilepsy. Roughly half of all episodes happen in a child with a prior diagnosis of epilepsy, and the other half present as the first seizure in a child who has never fitted before. About a quarter of children who present with a first unprovoked seizure do so in status epilepticus. [8]
The age distribution follows the shape of childhood epilepsy itself, with peaks in the first two years of life and again in early school age. The very young child is over-represented because febrile seizures, metabolic derangement, and central infection cluster in infancy. Mortality in paediatric status epilepticus is low in modern series, around one to two percent in resource-rich settings, but morbidity in the form of subsequent epilepsy, cognitive impairment, and a risk of recurrence is real. [8]
The dominant risk factors divide into the known and the acute. A child with poorly controlled epilepsy, especially one on a subtherapeutic antiseizure medication or with recent non-adherence, is at high risk. The acute triggers are the reversible causes that drive any provoked seizure, and they are fever and infection, metabolic disturbance such as hypoglycaemia or hyponatraemia, a rapid drop in antiseizure drug levels, head trauma, and toxin or drug withdrawal. Babl and colleagues showed that in Australia and New Zealand the commonest deviation from guideline care was under-dosing of the first-line benzodiazepine. [9]
Pathophysiology
A seizure starts as an imbalance between excitation and inhibition in the cortex, and status epilepticus is what happens when the normal self-limiting brake fails. The excitatory drive, carried by glutamate acting on NMDA and AMPA receptors, runs unchecked, while the inhibitory brake, carried by GABA acting on GABA-A receptors, fails to reset the circuit. The question the fellow must answer is why a seizure that benzodiazepines stop at five minutes becomes impossible to stop at thirty. [12]
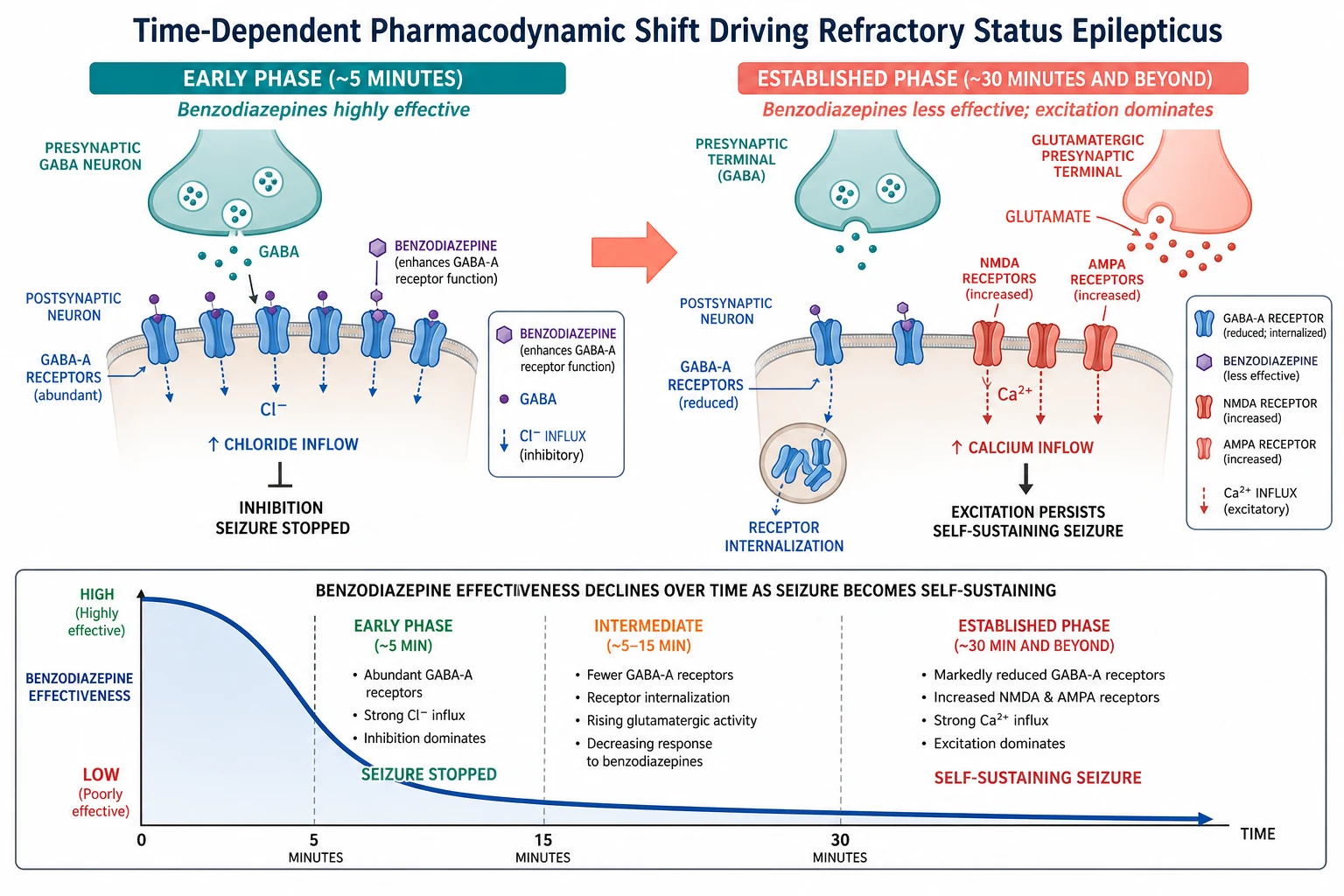
The answer is a time-dependent trafficking of receptors at the synapse. As the seizure runs, the GABA-A receptors on the neuronal surface are internalised into the cell, so fewer of them remain available to be boosted by a benzodiazepine. At the same time, the excitatory NMDA and AMPA receptors are recruited from inside the cell to the surface, increasing the calcium inflow that drives the seizure. The net effect is a synapse that is progressively harder to inhibit and progressively easier to excite. [12]
The clinical consequence is the steep decline in benzodiazepine efficacy with time. A full dose of lorazepam given at five minutes is highly effective, but the same dose given at thirty minutes works far less well, because the GABA-A receptors it needs to act on have been pulled inside the neuron. This is the mechanistic reason the first dose must be full, weight-based, and on time, and it is the reason that a child who arrives late needs a second-line agent, not a third benzodiazepine. [12]
A second consequence is the systemic and metabolic stress of a sustained convulsion. The continuous muscle activity produces a rising lactate, hyperthermia, rhabdomyolysis, and a metabolic acidosis, while the sympathetic surge drives tachycardia and hypertension that later give way to hypotension. The airway is compromised, the oxygen saturation falls, and the risk of hypoxic brain injury adds to the direct excitotoxic injury of the seizure itself. [8]
Clinical Presentation
The presentation of convulsive status epilepticus is unmistakable, a child in continuous tonic-clonic activity with no recovery between the jerks. The eyes may be deviated, the breathing is irregular and noisy, and the child is unresponsive. Cyanosis, foaming at the mouth, and incontinence are common. The convulsion may be generalized from the start or it may evolve from a focal onset, and the distinction matters for the cause search even though the immediate treatment is the same. [8]
How status epilepticus presents across the age spectrum
A febrile infant aged six months to five years with a convulsion lasting over five minutes, the commonest first presentation
A school-age child with known epilepsy who has a breakthrough seizure that fails to self-terminate, often with an intercurrent illness or a missed dose
An adolescent with a first generalized convulsion in status that turns out to be drug or toxin related
An intensive care patient who is paralysed and sedated but fails to wake, harbouring non-convulsive status that only the EEG reveals
A young infant with recurrent refractory convulsions that raise pyridoxine or pyridoxal-phosphate dependency until excluded
Two subtleties are deliberately examined. The first is the child who has stopped convulsing but has not recovered, which is the signature of transition into non-convulsive status. The rule is that a child who has not returned to a normal conscious state within thirty to sixty minutes of a convulsion needs an EEG, because the seizure may have continued in the brain after the movements stopped. The second is the child in subtle status, with continuous confusion, aphasia, or small twitching of a hand or the corner of the mouth, which is easily mistaken for a postictal state or a psychiatric presentation. [11]
The history taken in parallel with treatment focuses on the duration and the trigger. The exact time the seizure began is the most important historical fact, because it places the child in the early, established, or refractory phase. A fever points to a febrile or infectious cause, a recent illness or missed dose points to a breakthrough in a known epileptic, and a history of metabolic disease, toxin exposure, or head trauma directs the cause search. [9]
Differential Diagnosis
Not everything that shakes is a seizure, and not every prolonged spell is status epilepticus. The task at the bedside is to separate the true convulsive emergency from its mimics, because the treatment diverges sharply. The discriminator is the combination of the rhythm, the responsiveness, and the recovery, confirmed where doubt exists by an EEG. [8]
Convulsive status epilepticus
emergency, treat now
- Continuous rhythmic tonic-clonic jerking with no recovery
- Unresponsive throughout, abnormal breathing and colour
- Driven by epilepsy, fever, metabolic or infectious cause
- Treat stepwise with benzodiazepine then second-line agent
Febrile seizure (simple)
common, self-limiting
- Generalised convulsion under fifteen minutes with fever in a child six months to five years
- Recovers fully and quickly to baseline
- No focal features, no recurrence within twenty-four hours
- Child neurologically normal between episodes
Breath-holding / reflex anoxic spell
brief, self-limiting
- Triggered by pain, fright or minor head bump
- Brief loss of tone and colour, sometimes brief stiffening or jerking
- Rapid spontaneous recovery to normal
- Typical age six months to five years, with a clear precipitant
Pseudoseizure / dissociative spell
non-epileptic
- Variable asynchronous movements, eyes forced closed, resisting eye opening
- Responsiveness fluctuates, no postictal confusion
- Normal oxygen saturation and no metabolic acidosis
- EEG during the spell shows no ictal discharge
The febrile seizure is the commonest mimic in the young child, and a simple febrile seizure stops within fifteen minutes and the child recovers. A febrile convulsion that lasts over fifteen minutes is a complex febrile seizure and is managed as febrile status epilepticus, with the same drug ladder. The distinction matters because the child with a simple febrile seizure does not need antiseizure drugs, while the child in febrile status does. [8]
A breath-holding or reflex anoxic spell can produce a brief convulsive appearance, but it is triggered, brief, and recovers rapidly. A pseudoseizure or dissociative spell produces asynchronous, variable movements with preserved responsiveness and a normal EEG, and it is recognised by the inconsistent pattern and the absence of the metabolic and autonomic signs of a true seizure. The rule is that status epilepticus is treated first when there is genuine doubt, and the mimic is excluded by the EEG and the recovery afterwards. [8]
Clinical & Bedside Assessment
The bedside assessment of a convulsing child is a structured emergency that runs in parallel with the first drug dose, not after it. You call for help, you start the clock, you assess the airway and breathing, you give high-flow oxygen, and you check the blood glucose, all while the benzodiazepine is being drawn up. The assessment takes seconds, because the treatment is time-critical. [2]
The airway and breathing come first. The child is placed in the lateral position, high-flow oxygen is applied, and the airway is maintained with a jaw thrust and suction as needed. The oxygen saturation and the heart rate are monitored continuously, because hypoxia and bradycardia are the immediate threats. The blood glucose is checked at the bedside without delay, because a hypoglycaemic seizure will not stop until the glucose is corrected. [8]
The drug dose depends on an accurate weight, which is obtained by weighing the child, asking the parent, or using a length-based tape such as the Broselow when weighing is impossible. Every dose in the status ladder is weight-based, and an under-dose is the commonest reason a seizure persists. The intravenous route is preferred, and the buccal or intramuscular route is used when intravenous access cannot be secured quickly. [9]
Investigations
The investigation of status epilepticus runs in parallel with treatment, and the only test that gates the first drug is the bedside glucose. A capillary blood glucose is checked at once in every child, because hypoglycaemia is a rapidly reversible cause of seizure that no anticonvulsant will fix. If the glucose is low, two millilitres per kilogram of ten percent dextrose is given intravenously, and the cause is pursued. [8]
First-line benzodiazepine in convulsive status epilepticus
Dose
Lorazepam 0.1 mg per kg intravenously, maximum 4 mg per dose, repeated once after five minutes if still seizing
Blood is sent for a venous gas, electrolytes including sodium, calcium and magnesium, glucose, a full blood count, and a blood culture if infection is suspected. A low sodium, a low calcium, or a low magnesium each can sustain a seizure, and each is corrected as it is found. A toxicology screen is sent when ingestion is possible, because several toxins and drug withdrawals provoke refractory seizures. Antiseizure drug levels are checked in a child with known epilepsy to detect a subtherapeutic level. [8]
An EEG is the definitive investigation for non-convulsive and refractory status, and it is mandatory after a child is intubated and paralysed for refractory seizures. Once the patient is paralysed, the clinical signs of seizure disappear, but the brain can continue to seize, so the EEG is the only way to know whether the treatment is working. A lumbar puncture is performed after the seizure is controlled and the coagulation and platelets are checked, whenever a central nervous system infection is in the differential. Neuroimaging, with a computed tomography acutely and magnetic resonance imaging later, is performed once the child is stable to look for a structural cause. [11]
Management — Resuscitation
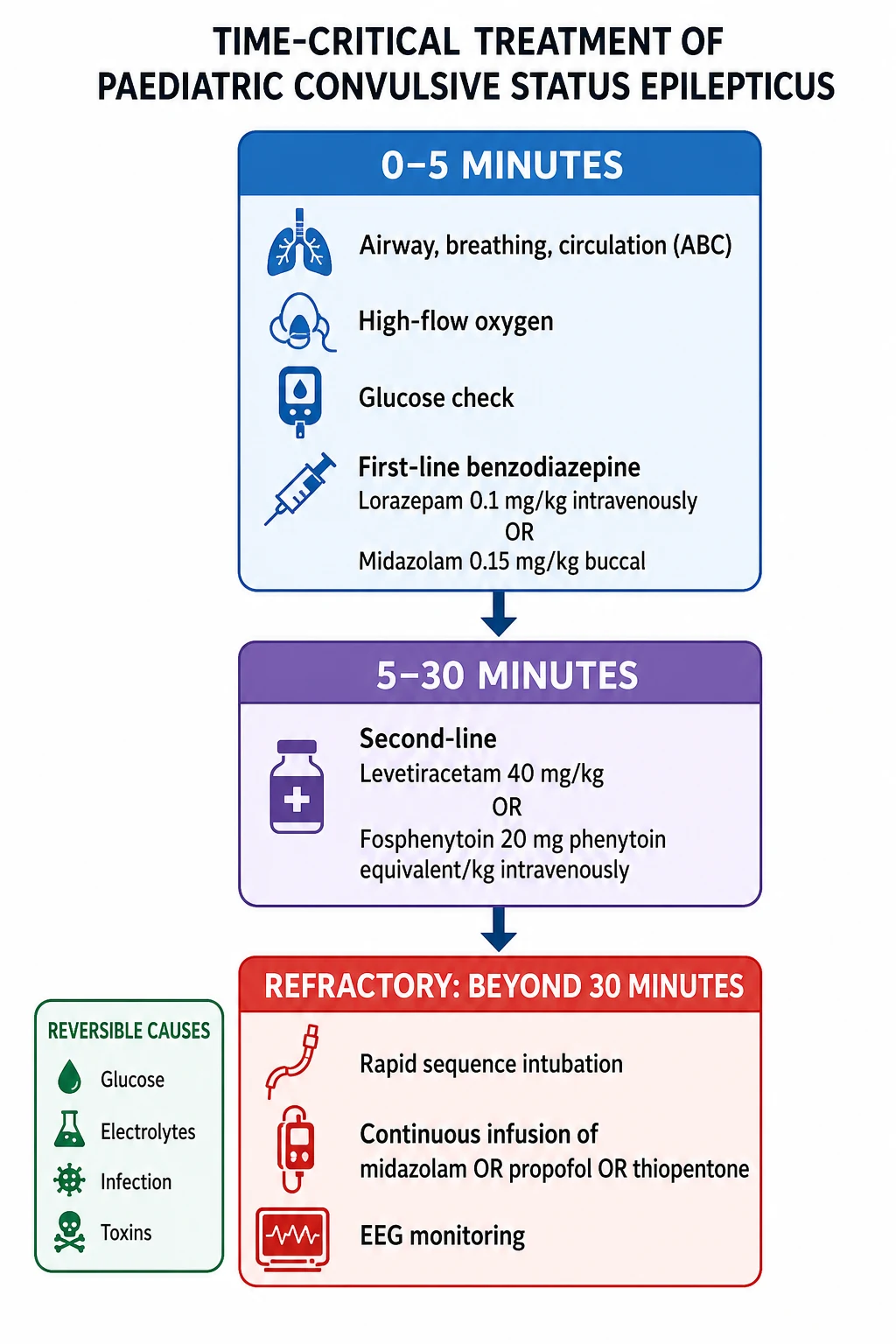
The resuscitation of a child in convulsive status epilepticus follows the APLS stepwise pathway, and the guiding principle is that the right drug, at the right dose, at the right time, stops the seizure. The pathway moves through three phases that mirror the ILAE time axis, and each phase has its own drug. The first move, before any anticonvulsant, is to secure the airway, give oxygen, check the glucose, and call for help. [2]
In the first five minutes the child receives a benzodiazepine. The preferred agent is lorazepam at 0.1 mg per kg intravenously, to a maximum of 4 mg per dose, because it is effective, long-acting, and carries a lower risk of respiratory depression than diazepam. If intravenous access cannot be secured, midazolam 0.15 mg per kg is given by the buccal route, or intramuscular midazolam is used in the prehospital setting. The dose is repeated once after five minutes if the seizure persists, and no more than two doses of benzodiazepine are given before the ladder moves on. [2]
The reversible causes are sought and treated at the same time as the drugs are given. Hypoglycaemia is corrected with two millilitres per kg of ten percent dextrose. Electrolyte disturbances, including hyponatraemia, hypocalcaemia, and hypomagnesaemia, are corrected as identified. Fever and a suspected central infection prompt a blood culture and, once stable, a lumbar puncture, with empirical antibiotics and aciclovir. In the young infant with refractory seizures of unknown cause, intravenous pyridoxine is given empirically, because pyridoxine-dependent seizures will not respond to any anticonvulsant until the vitamin is given. [8]
Management — Definitive & Stepwise
If the seizure persists beyond five to ten minutes despite two adequate benzodiazepine doses, the child has established status epilepticus and receives a second-line agent. The two principal options are levetiracetam and fosphenytoin, and either is acceptable. Levetiracetam is given at 40 mg per kg intravenously, to a maximum of 4.5 g, over five minutes. Fosphenytoin is given at 20 mg phenytoin-equivalent per kg intravenously, to a maximum of 1500 mg phenytoin-equivalent, infused over ten minutes. [4]
[2]The choice between levetiracetam and fosphenytoin is supported by three landmark trials. The Established Status Epilepticus Treatment Trial, ESETT, randomised children and adults with established status to levetiracetam, fosphenytoin, or valproate, and found that all three stopped the seizure in just over half of patients, with no significant difference between them. The paediatric subgroup analysis confirmed that the efficacy held across the age range, including in young children. Kapur and colleagues reported that levetiracetam and fosphenytoin were equally effective and equally safe. [4][7]
The two dedicated paediatric trials, ConSEPT and EcLiPSE, tested levetiracetam against phenytoin as second-line therapy in children and found no difference in seizure cessation between the two. Dalziel and colleagues reported the ConSEPT trial across Australia and New Zealand, and Lyttle and colleagues reported the EcLiPSE trial in the United Kingdom, and their shared finding was that levetiracetam was at least as effective as phenytoin with a more favourable safety profile, which is why it has become the preferred second-line agent in many paediatric pathways. [5][6]
Second-line agent in established status epilepticus
Dose
Levetiracetam 40 mg per kg intravenously, maximum 4.5 g, over five minutes
If the seizure persists beyond thirty minutes or despite adequate first and second-line therapy, the child has refractory status epilepticus, and the pathway calls for rapid sequence intubation and a continuous anaesthetic infusion. The airway is secured, the child is ventilated, and an infusion is started. The options are a midazolam infusion, a propofol infusion, or a thiopentone infusion, each titrated to burst suppression on the EEG. Once the child is intubated and paralysed, continuous EEG monitoring is mandatory, because the clinical signs of seizure disappear and only the EEG reveals whether the brain is still seizing. [2]
The stepwise pathway for paediatric convulsive status epilepticus
Zero to five minutes: secure airway, high-flow oxygen, check glucose, give lorazepam 0.1 mg per kg IV or buccal midazolam 0.15 mg per kg, repeat once after five minutes
Five to thirty minutes: give levetiracetam 40 mg per kg IV or fosphenytoin 20 mg PE per kg IV as second-line therapy
Beyond thirty minutes or refractory: rapid sequence intubation, start a continuous midazolam or propofol or thiopentone infusion titrated to burst suppression
Continuous EEG monitoring throughout the anaesthetic phase to confirm seizure control
Treat the reversible cause in parallel: glucose, electrolytes, infection, toxins, pyridoxine in the young infant
A subtlety in the refractory phase is the role of paralysis. A neuromuscular blocker is sometimes given to facilitate intubation and ventilation, and it stops the visible convulsion, but it does not stop the brain from seizing. The danger is that the child looks controlled while the cortical seizure runs unchecked, so the EEG is the only reliable guide to whether the treatment is working, and an anaesthetic infusion is titrated to electrical, not clinical, control. [11]
Specific Subtypes & Scenarios
Febrile status epilepticus is the commonest scenario in the young child, presenting as a convulsion lasting over fifteen minutes with fever in a child aged six months to five years. It is managed on the same drug ladder as any convulsive status, and the fever and the infection are investigated and treated. Most children recover fully, and the episode is followed by a discussion of the risk of recurrence and of subsequent epilepsy. [8]
Convulsive status in a child with known epilepsy is the second scenario, and it usually reflects an intercurrent illness, a missed dose, or a subtherapeutic drug level. The seizure is controlled on the standard ladder, the antiseizure drug level is checked, and the maintenance therapy is reviewed and optimised. The episode is a signal to revisit the epilepsy diagnosis and the adherence, and to consider whether the child needs a rescue benzodiazepine plan for future episodes. [9]
New-onset refractory status epilepticus, known as NORSE, is the third and most challenging scenario. It presents as refractory status in a previously well child or adult with no prior epilepsy and no clear acute cause, and it often proves to have an autoimmune or cryptogenic basis. Sculier and Gaspard described the spectrum and the prolonged intensive care course, the extensive cause search that includes autoimmune and infectious panels, the empirical immunotherapy that is often tried, and the guarded but heterogeneous prognosis. [11]
The young infant with refractory seizures is the fourth scenario, and it raises the metabolic and vitamin-responsive causes that are unique to early life. Pyridoxine-dependent seizures and pyridoxal-phosphate-dependent seizures present as intractable status in the neonatal or early infantile period, and they respond only to the vitamin. The diagnostic and therapeutic move is to give intravenous pyridoxine empirically while the metabolic workup proceeds, because no anticonvulsant will control the seizure until the dependency is treated. [8]
Complications & Pitfalls
Hypoxic and excitotoxic brain injury is the feared complication, and it is the reason every minute counts. The sustained seizure consumes oxygen and glucose, the airway is compromised, and the direct glutamate-mediated excitotoxicity injures neurons, with the hippocampus especially vulnerable. The risk of lasting cognitive and motor impairment rises with the duration of status and with the presence of hypoxia and hypotension. [8]
Systemic complications accompany the sustained convulsion. The continuous muscle activity produces a rising lactate and a metabolic acidosis, hyperthermia, rhabdomyolysis with the risk of acute kidney injury, and aspiration pneumonitis. The treatment-related complications are also real, chiefly respiratory depression from the benzodiazepines and the anaesthetic infusions, and the hypotension that accompanies the anaesthetic agents in the refractory phase. [8]
The classic pitfalls are temporal, dosing, and diagnostic. The first is delay in giving the first benzodiazepine, which lets the seizure cross into the refractory zone where the drugs work less well. The second is under-dosing the benzodiazepine out of caution, which fails to control the seizure and adds the very respiratory depression the cautious dose was meant to avoid. The third is forgetting the reversible cause, treating the seizure but missing the hypoglycaemia or the hyponatraemia that is sustaining it. [9]
A subtler pitfall is assuming the seizure has stopped after paralysis. The child who is intubated and paralysed looks controlled, but the cortical seizure can continue, and the only way to know is the EEG. Uppal and colleagues showed in their systematic review that deviation from the guideline pathway, including failure to escalate and failure to monitor, is associated with worse outcomes. [10]
Prognosis & Disposition
The prognosis of paediatric status epilepticus is, in the main, favourable, with mortality around one to two percent in modern resource-rich series. Most children recover from the acute episode without lasting sequelae, and the dominant determinants of the outcome are the underlying cause, the duration of the seizure, and the presence of hypoxia or hypotension. A short, rapidly controlled febrile status in a previously well child carries an excellent prognosis, while a prolonged refractory status with an infectious or metabolic cause carries a more guarded one. [8]
The risk of a further episode of status is real, with about one in six children having a recurrence, and the child with a prior neurological abnormality or an established epilepsy is at higher risk. The risk of subsequent epilepsy after a first presentation in status is elevated compared with a first brief seizure, reflecting the shared substrate of the cause. The cognitive outcome is driven by the underlying aetiology and by any hypoxic injury incurred during the episode. [8]
Disposition is to a paediatric ward for a child who has recovered quickly with a clear and treated cause, and to a paediatric intensive care unit for any child who required a second-line agent, who was intubated, or who has not returned to baseline. Every child is followed up in a paediatric neurology clinic to review the epilepsy diagnosis, to optimise the maintenance therapy if epilepsy is confirmed, and to provide a rescue benzodiazepine plan and family education for future episodes. [9]
Special Populations
The child with a neurodisability or established epilepsy is the population at highest baseline risk. A child with cerebral palsy, a structural brain lesion, or a genetic epilepsy syndrome is more likely to present in status and to have a refractory course, and the family often has a rescue benzodiazepine plan already in place. The management is the same drug ladder, with extra attention to the airway in the child with baseline tone and swallowing abnormality, and with early escalation given the higher refractory risk. [8]
The Aboriginal and Torres Strait Islander child and the child from a remote setting is the second population, and the one for whom the access to care shapes the outcome. The longer time to treatment in remote settings, the higher burden of infectious triggers, and the distance to a paediatric intensive care unit all conspire to lengthen the seizure duration, which is why retrieval pathways and the family rescue plan are central. The culturally appropriate communication and the engagement with the family are part of the acute and the follow-up care. [9]
The young infant is the third population, and the one for whom the cause search is most urgent. A refractory seizure in the first months of life raises the metabolic and vitamin-responsive epilepsies, the inborn errors of metabolism, and the central nervous system infection, and the workup is broader and faster than in the older child. Intravenous pyridoxine is given empirically when the cause is obscure, and the metabolic and genetic investigations are sent early. [8]
The child from a refugee or migrant family is the fourth population, and the one for whom the communication and the continuity are the challenges. The language barrier can hide the duration of the seizure and the past history, an interpreter is engaged early, and the cause search includes the infections and the nutritional deficiencies that are more common in this group. The family is connected to the local neurology service and to a rescue plan before discharge. [9]
Evidence, Guidelines & Regional Differences
The evidence base for the second-line agent was transformed by three trials that asked the same question and reached the same answer. The Established Status Epilepticus Treatment Trial, reported by Kapur and colleagues, randomised children and adults to levetiracetam, fosphenytoin, or valproate, and found that all three stopped the seizure in just over half of patients with no significant difference between them. Chamberlain and colleagues confirmed in the age-group analysis that the efficacy held across the age range, including in children under six. [4][7]
The two paediatric trials addressed the same comparison directly. Dalziel and colleagues reported the ConSEPT trial, conducted across Australia and New Zealand, and Lyttle and colleagues reported the EcLiPSE trial in the United Kingdom, and both compared levetiracetam with phenytoin as second-line therapy in children. Neither trial found a difference in seizure cessation, and their shared finding that levetiracetam is at least as effective as phenytoin with a more favourable safety profile underpins its place as the preferred second-line agent in modern paediatric pathways. [5][6]
ESETT 2019
NEJM, all ages
- Levetiracetam, fosphenytoin, and valproate equally effective
- Each stopped about half of established seizures
- No difference in safety across the three agents
- Age subgroup analysis confirmed efficacy in children
ConSEPT 2019
Lancet, Australia and NZ
- Levetiracetam versus phenytoin in children
- No difference in seizure cessation
- Levetiracetam favoured for safety profile
- Supported levetiracetam as preferred second-line
EcLiPSE 2019
Lancet, United Kingdom
- Levetiracetam versus phenytoin in children
- No difference in the primary outcome
- Stood with ConSEPT in the pooled evidence
- Confirmed equivalence and safety of levetiracetam
The guideline evidence is anchored by the American Epilepsy Society guideline, reported by Glauser and colleagues, which gives a level A recommendation to the early benzodiazepine and a level B to the second-line agent, and which frames the stepwise pathway that the trials later tested. The systematic review by Uppal and colleagues showed that deviation from the guideline pathway, chiefly the under-dosing of the first benzodiazepine and the failure to escalate, is associated with worse outcomes, which is why adherence to the ladder is itself an outcome measure. [2][10]
The regional differences centre on the preferred second-line agent and the dose. The Australian and New Zealand pathway, informed by ConSEPT, uses levetiracetam 40 mg per kg as the default second-line agent, while the North American pathway, informed by ESETT, accepts levetiracetam at up to 60 mg per kg or fosphenytoin. The shared foundation is the APLS stepwise framework of benzodiazepine first, second-line agent next, and anaesthetic infusion for the refractory case, with the reversible causes sought throughout. Babl and colleagues documented that the practice in Australia and New Zealand has converged on this framework, with the residual weakness being the consistency of the first benzodiazepine dose. [9]
Exam Pearls
The status epilepticus ladder to the minute
References
- [1]Trinka E, Cock H, Hesdorffer D, et al A definition and classification of status epilepticus--Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia, 2015.PMID 26336950
- [2]Glauser T, Shinnar S, Gloss D, et al Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr, 2016.PMID 26900382
- [3]Silbergleit R, Lowenstein D, Durkalski V, et al RAMPART (Rapid Anticonvulsant Medication Prior to Arrival Trial): a double-blind randomized clinical trial of the efficacy of intramuscular midazolam versus intravenous lorazepam in the prehospital treatment of status epilepticus by paramedics. Epilepsia, 2011.PMID 21967361
- [4]Kapur J, Elm J, Chamberlain JM, et al Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. N Engl J Med, 2019.PMID 31774955
- [5]Dalziel SR, Borland ML, Furyk J, et al Levetiracetam versus phenytoin for second-line treatment of convulsive status epilepticus in children (ConSEPT): an open-label, multicentre, randomised controlled trial. Lancet, 2019.PMID 31005386
- [6]Lyttle MD, Rainford NEA, Gamble C, et al Levetiracetam versus phenytoin for second-line treatment of paediatric convulsive status epilepticus (EcLiPSE): a multicentre, open-label, randomised trial. Lancet, 2019.PMID 31005385
- [7]Chamberlain JM, Kapur J, Shinnar S, et al Efficacy of levetiracetam, fosphenytoin, and valproate for established status epilepticus by age group (ESETT): a double-blind, responsive-adaptive, randomised controlled trial. Lancet, 2020.PMID 32203691
- [8]Abend NS, Loddenkemper T Pediatric status epilepticus management. Curr Opin Pediatr, 2014.PMID 25304961
- [9]Babl FE, Sheriff N, Borland M, et al Emergency management of paediatric status epilepticus in Australia and New Zealand: practice patterns in the context of clinical practice guidelines. J Paediatr Child Health, 2009.PMID 19686314
- [10]Uppal P, Cardamone M, Lawson JA Outcomes of deviation from treatment guidelines in status epilepticus: A systematic review. Seizure, 2018.PMID 29705433
- [11]Sculier C, Gaspard N New onset refractory status epilepticus (NORSE). Seizure, 2019.PMID 30482654
- [12]Kienitz R, Kay L, Beuchat I, et al Benzodiazepines in the Management of Seizures and Status Epilepticus: A Review of Routes of Delivery, Pharmacokinetics, Efficacy, and Tolerability. CNS Drugs, 2022.PMID 35971024