Paeds · neurology-neurodisability-and-neuromuscular
Tics and Tourette syndrome
Also known as Tourette disorder · Tourette syndrome · Chronic tic disorder · Provisional tic disorder · Persistent motor or vocal tic disorder · Childhood tic disorder
Fellowship guide to tics and Tourette syndrome: the DSM-5 spectrum from provisional to persistent tic disorder to Tourette disorder, the defining phenomenology of premonitory urge and suppressibility with waxing and waning, the cortico-striato-thalamo-cortical mechanism and the shared genetics with attention-deficit or hyperactivity disorder and obsessive-compulsive disorder, the high-yield comorbidity screen that drives most of the impairment, the stepped management built on Comprehensive Behavioural Intervention for Tics with alpha-2 agonists and antipsychotics, and the favourable prognosis that tics peak around 10 to 12 years and improve through adolescence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the seven-year-old boy whose teacher reports he cannot stop blinking, throat-clearing, and jerking his neck, whose parents notice these movements vanish when he plays a video game and surge when he is tired or anxious, and who is now being asked whether he needs a brain scan and a pill. That child carries the whole teaching point of paediatric tics: the diagnosis is clinical, the prognosis is reassuring, and the thing that most needs treating is usually not the movement at all but the attention-deficit, the anxiety, or the obsessive-compulsive symptom riding alongside it. The clinician who grasps this triage avoids two opposite errors, over-medicalising a benign fluctuating movement and missing the comorbidity that is silently harming the child. [2]
A tic is defined by four phenomenological features rather than by any single movement. It is sudden, rapid, recurrent, and non-rhythmic. It is briefly suppressible, so a child can hold it off for a short time. It is preceded by a premonitory urge, a mounting sensory tension that builds until the tic is performed. And performing the tic brings transient relief before the cycle restarts. Movements that lack the urge, the suppressibility, and the relief are usually not tics, and these four features are what separate a tic from a stereotypy, a myoclonic jerk, a choreiform movement, or a habitual mannerism. [2]
The tics themselves divide into motor and vocal, and each divides again into simple and complex. Simple motor tics involve one muscle group, such as eye-blinking, facial grimacing, shoulder-shrugging, or head-jerking, while complex motor tics are coordinated sequences such as jumping, touching, or copropraxia, an obscene gesture. Simple vocal tics are sounds such as sniffing, grunting, throat-clearing, or coughing, while complex vocal tics include words, echolalia repeating another's words, palilalia repeating one's own words, and coprolalia, the involuntary uttering of socially inappropriate words. The famous feature, coprolalia, is in fact uncommon and is never required to make the diagnosis. [2]
Classification
Classifying a child's tics answers two questions: how long have they been present, and do motor and vocal tics coexist. The answer places the child somewhere on the DSM-5 tic disorder spectrum, and that placement predicts prognosis and frames the conversation with the family. A child whose tics have lasted under a year is, by definition, still in the provisional phase, and most of these children will resolve. A child whose single-type tics have lasted over a year has a persistent tic disorder. A child with multiple motor tics plus at least one vocal tic over more than a year has Tourette disorder, the severe and persistent end of the spectrum. [2]
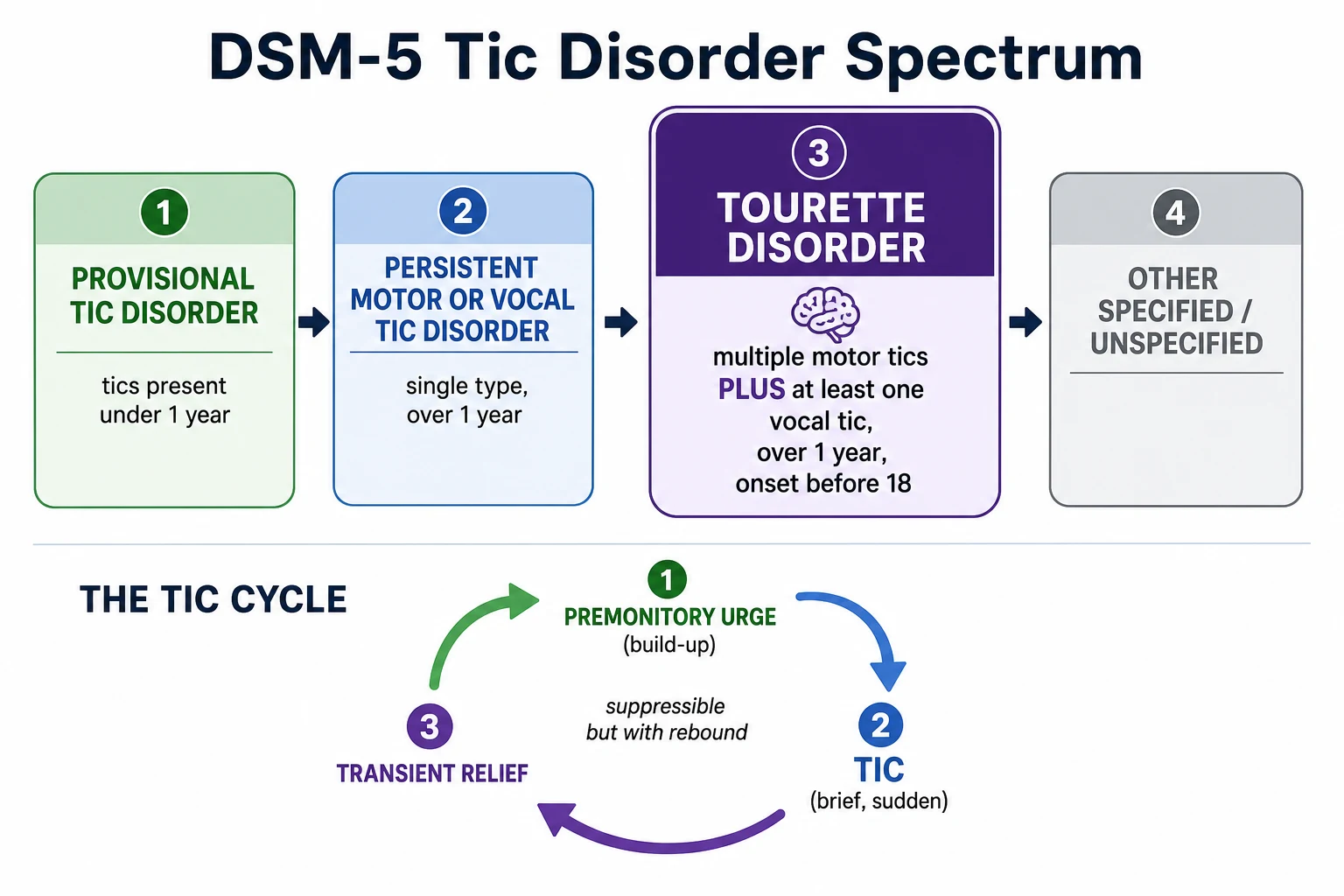
The duration rule matters because it changes the prognosis given to the family. Provisional tic disorder, tics for under one year, is the commonest presentation in young children and carries the highest chance of spontaneous resolution, so the message is watchful reassurance, not a diagnosis of Tourette. Persistent motor or vocal tic disorder, single-type tics for over one year, sits between provisional and Tourette in its course. Tourette disorder, motor plus vocal tics for over one year with onset before 18, is the diagnosis that predicts persistence, comorbidity, and the need for multidisciplinary care. [2]
Provisional tic disorder
DSM-5
- Motor and/or vocal tics present for under 1 year
- Onset before 18, not substance- or disease-caused
- Criteria never met for Tourette or persistent tic disorder
- Most resolve, so reassure and review
- The commonest presentation in young children
Persistent motor or vocal tic disorder
DSM-5
- Single type, either motor or vocal but not both
- Present for over 1 year
- Onset before 18, not substance- or disease-caused
- Intermediate course between provisional and Tourette
- Treat impairment when present
Tourette disorder
DSM-5
- Multiple motor tics plus at least one vocal tic
- Present for over 1 year since the first tic
- Onset before age 18, not substance- or disease-caused
- Motor and vocal tics need not occur at the same time
- The severe, persistent end of the spectrum
Other specified or unspecified
DSM-5
- Tics that do not fit the three main categories
- Onset after 18 is other specified, not Tourette
- Capture atypical or secondary patterns
- Demands review for a secondary cause
- Refer to paediatric neurology
A common misconception is that motor and vocal tics must be present at the same moment to diagnose Tourette disorder. They do not. DSM-5 requires only that both have been present at some time during the illness, and a child whose eye-blinking of last year has been replaced by throat-clearing this year still meets criteria if both have occurred over more than a year. The other rule worth stating plainly is that the diagnosis is never made by coprolalia. The involuntary swearing is striking, memorable, and uncommon, and the child with Tourette who never swears is the rule, not the exception. [2]
Epidemiology & Risk Factors
Tics are among the most common movement disorders of childhood, and recognising how common they are is itself therapeutic, because it lets the clinician reassure a frightened family. The Swedish school population study by Khalifa and von Knorring found Tourette syndrome in about one per cent of schoolchildren, with any tic disorder substantially more common when transient and provisional tics are included. Tics are two to four times more frequent in boys than in girls, and the typical age of onset is between four and six years, with peak severity reached around ten to twelve years. [7]
The single strongest risk factor is a family history. Tourette syndrome is highly heritable, and the condition clusters in families alongside attention-deficit or hyperactivity disorder and obsessive-compulsive disorder, reflecting a shared genetic liability that expresses as different symptoms in different relatives. A boy whose father had tics and whose mother has obsessive-compulsive traits is the kind of family history that sharpens the diagnosis before any tic is seen. Other influences on severity include male sex, perinatal and pregnancy complications, and psychosocial stress, but these modify severity rather than cause the disorder. [6] [12]
The numbers that anchor your viva
Most children improve over time, and saying so clearly is the foundation of the consultation. Tic severity peaks around ten to twelve years and then declines for the majority through late adolescence and early adulthood, with only a minority carrying severe tics into adult life. What persists more often than the tics is the obsessive-compulsive symptomatology, which can rise through adolescence even as the movements fade, which is why follow-up must keep asking about the comorbidities and not only about the tics. [11]
Pathophysiology
Tics arise not from a single broken nerve but from a dysregulation of the brain's motor-filtering circuits, and understanding the circuit explains both the movements and the drugs that calm them. The relevant anatomy is the cortico-striato-thalamo-cortical loop, a circuit that links the motor cortex, the striatum within the basal ganglia, and the thalamus, and that normally gates which motor programmes are released and which are suppressed. When this gating fails, unwanted motor programmes leak through as tics. [2]
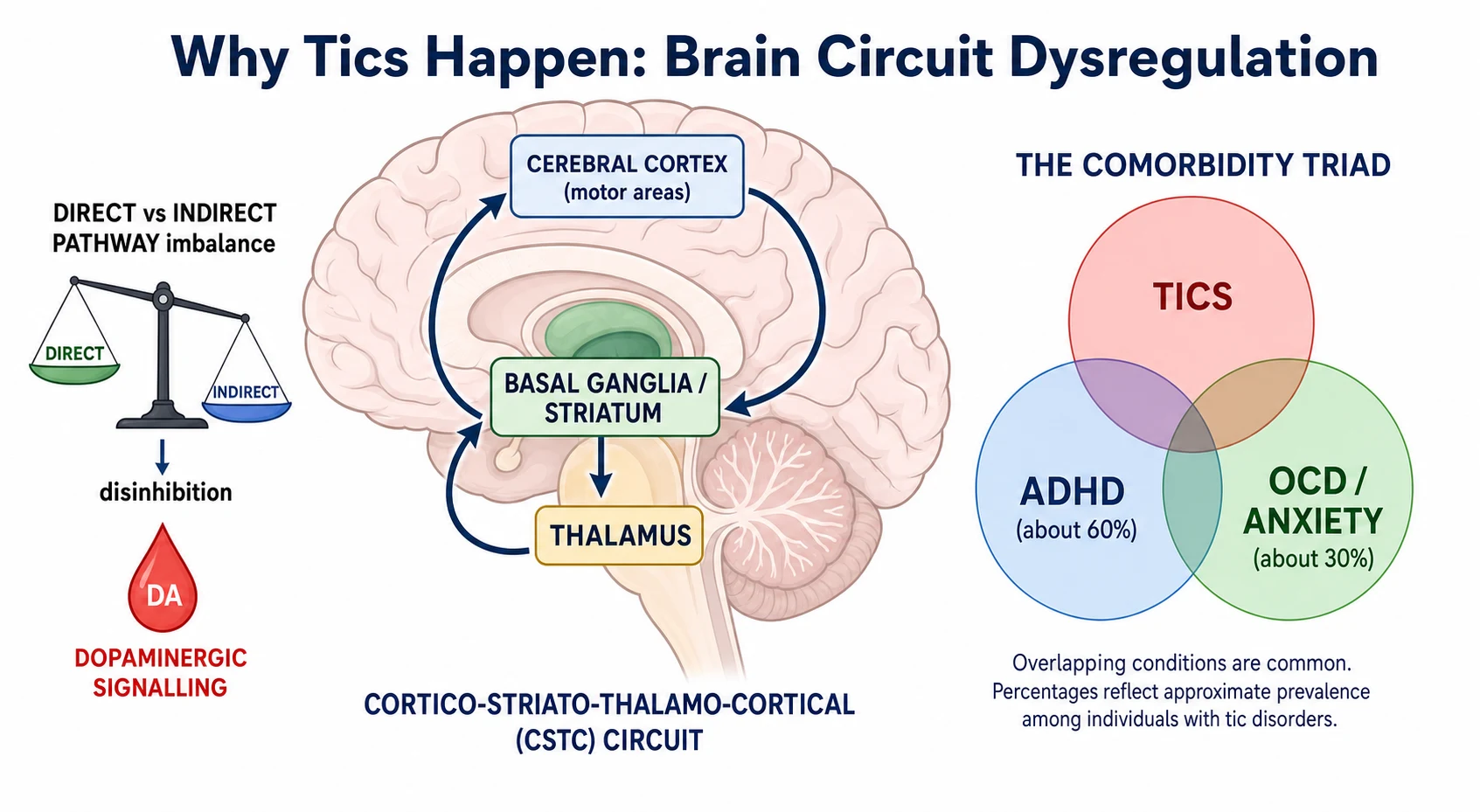
Within the basal ganglia the balance between the direct pathway, which promotes movement, and the indirect pathway, which suppresses movement, is tilted, producing a state of disinhibition in which tics break through. Dopamine is the neurotransmitter that dominates these circuits, which is why the most effective tic-suppressing drugs are those that block dopamine, the antipsychotics, and why the condition can be worsened by stimulant and dopaminergic drugs in susceptible individuals. The premonitory urge is thought to arise from the same sensitised sensorimotor circuitry, so the urge and the tic are two expressions of one dysregulation. [2] [3]
[6] [12]The high placebo response seen in adult tic trials and the strong benefit of behavioural therapy both point to a disorder in which top-down control can be trained, not only drugged. Comprehensive Behavioural Intervention for Tics works by teaching the child to detect the premonitory urge and to perform a competing movement that blocks the tic, and its effectiveness is itself evidence that the cortico-striato-thalamo-cortical circuit is modifiable by learning. This is why a behavioural therapy, not a drug, is first-line active treatment for impairing tics. [1] [4]
Clinical Presentation
The typical child is a school-aged boy whose parents or teachers notice blinking, facial grimacing, shoulder-shrugging, head-jerking, sniffing, grunting, or throat-clearing that comes and goes over weeks and months. The tics wax and wane in severity, so a good week does not rule out the diagnosis and a bad week does not mean deterioration. They also shift body location over time, so the blinking of last month becomes the shoulder-shrug of this month, and this roving quality is characteristic. The child is usually otherwise well and developing normally between episodes. [2]
The feature that most confirms a tic, and that examiners love, is the premonitory urge. Children old enough to describe it report a mounting sensation in the affected body part, a tightness, an itch, or a pressure that builds until the tic is performed and then dissipates, only to build again. Tics can be suppressed for a short time, for example in clinic or during a favoured activity, but suppression raises the inner tension and is followed by a rebound burst of tics once the suppressing context ends. This is why tics often vanish during focused absorption, such as sport or a video game, and return with fatigue, stress, anxiety, or excitement. [2]
| Clinical picture | What it implies | Act |
|---|
Coprolalia is the symptom families fear and examiners probe. The involuntary uttering of obscene or socially inappropriate words is real but uncommon, occurs in a minority of children with Tourette, and is never required for the diagnosis. When it does occur it is socially devastating, and the child is as distressed by it as the bystanders. Complex tics can also take the form of echolalia, repeating another person's words, palilalia, repeating one's own whispered words, copropraxia, an obscene gesture, or self-injurious behaviours such as slapping or hitting, and these complex and self-injurious forms are the tics that most often bring a child to specialist care. [2]
Differential Diagnosis
The first differential question is whether the movement is a tic at all, because several common childhood movements mimic tics and their management differs entirely. Stereotypies, seen in young children and in children with autism or developmental delay, are rhythmic, fixed, purposeful-appearing movements such as hand-flapping or body-rocking that lack the premonitory urge, the suppressibility, and the roving waxing-and-waning course of a tic. Myoclonus is a brief shock-like jerk without urge; chorea is a flowing, unpredictable, non-suppressible movement; dystonia is a sustained posturing; and tremor is rhythmic. Each of these lacks the defining phenomenology of a tic. [2]
The motor restlessness of attention-deficit or hyperactivity disorder is a particular trap. The child with attention-deficit or hyperactivity disorder is fidgety and constantly in motion, but this restlessness is not suppressible in the tic sense, is not preceded by an urge, and does not follow the waxing-and-waning course of tics. Because the two conditions coexist in about 60 per cent of children with Tourette, the clinician must distinguish the restless fidgeting from the discrete tics at the same consultation, and home video helps enormously. Functional or psychogenic tics form a further category, with a more variable, suggestible, and non-waxing course, often with an abrupt onset and atypical features, and they need a careful functional-neurological-disorder assessment. [6]
Primary tic or Tourette
- Premonitory urge, suppressible, rebound
- Waxes and wanes, shifts body location
- Onset before 18, normal examination
- Often with ADHD, OCD, or anxiety
- Clinical diagnosis, no scan needed
Stereotypy
- Rhythmic, fixed, purposeful-appearing
- Lacks urge and suppressibility
- Often in autism or developmental delay
- Hand-flapping, body-rocking
- Behavioural management in context
Other movement disorder
- Myoclonus, chorea, dystonia, tremor
- Each lacks the urge-and-relief cycle
- Chorea is flowing and non-suppressible
- Dystonia is sustained posturing
- Neurology review for atypical movements
Secondary or functional tic
- Drug-induced after stimulant or antipsychotic
- Fixed course or onset after 18
- Abrupt, suggestible, non-waxing for functional
- With focal deficit or regression
- Demands imaging and specialist review
The second and more dangerous question is whether the tics are secondary. Drug-induced tics can follow stimulants, antipsychotics, or dopamine agents, and a careful medication review is part of any new presentation. Tics arising from brain injury, infection, or rare neurodegenerative or genetic disease are suggested by atypical age of onset, a fixed rather than fluctuating course, accompanying neurological or systemic signs, and developmental regression. PANS or PANDAS, the abrupt dramatic onset of tics and obsessive-compulsive symptoms after streptococcal infection, is a recognised but controversial entity that sits between primary and secondary, and it is covered below. Any atypical feature shifts the consultation from reassurance to investigation. [8]
Clinical & Bedside Assessment
The diagnosis is made by history and by observation, and the single most useful tool is home video, because tics are routinely suppressed in the clinic and the child who sits still for the doctor is the child who tics at home. Ask the family to record short clips in the setting where the tics are worst, and review them with the parents. This converts an uncertain history into a confident diagnosis and avoids the temptation to investigate a child who has nothing to investigate. [2]
The history characterises the movements as motor or vocal and as simple or complex, and maps their course. Ask when the tics started, how often they occur, how long they last, and which body parts are involved now and in the past, to capture the roving waxing-and-waning quality. Ask about the premonitory urge, about suppressibility and rebound, and about the contexts that worsen and ease the tics, such as stress, fatigue, anxiety, and focused absorption. Record the family history of tics, attention-deficit or hyperactivity disorder, and obsessive-compulsive disorder. [2]
The deliberate comorbidity screen is the highest-yield part of the assessment, because the comorbidities cause most of the impairment. Ask explicitly about attention, activity level, impulsivity, and school performance for attention-deficit or hyperactivity disorder, about obsessions, compulsions, checking, and symmetry for obsessive-compulsive disorder, about worry, separation difficulty, and low mood for anxiety and depression, about rage attacks and self-injurious behaviour, and about learning and sleep. Each positive answer reshapes the management plan, because treating the comorbidity usually helps the child more than treating the tics. [6]
A general and neurological examination is performed at least once, with two aims. The first is to confirm that the child is otherwise developing and examining normally, which supports a primary tic disorder. The second is to exclude alternative causes, looking for dysmorphism, neurocutaneous stigmata, focal neurological signs, changes in tone or gait, and any regression. In a typical Tourette presentation the examination is entirely normal, and the purpose of examining is to exclude, not to confirm. Severity and impairment are then graded clinically, and a structured scale such as the Yale Global Tic Severity Scale can be used to quantify motor and vocal tic severity and impairment for tracking over time. [9]
Investigations
There is no blood test, no scan, and no electroencephalogram that diagnoses Tourette syndrome, and the diagnosis is made by applying the DSM-5 criteria to a typical history and a normal examination. Routine neuroimaging in a child with a classic history and a normal examination is not indicated, and over-investigation causes real harm through radiation exposure, incidental findings that generate anxiety, delays to the behavioural plan, and the medicalisation of a child whose tics are mild. The restraint to investigate is as important a clinical skill as the decision to treat. [2]
Targeted investigation is reserved for the atypical case. A recent streptococcal illness with abrupt onset of tics and obsessive-compulsive symptoms prompts an antistreptolysin O titre and specialist paediatric neurology or psychiatry involvement for suspected PANS or PANDAS. A drug or toxin exposure prompts a medication review. A fixed deficit, developmental regression, an abnormal examination, or a non-fluctuating course prompts magnetic resonance imaging to exclude a structural cause. Genetic or metabolic testing is reserved for children with regression, dysmorphism, or a neurodegenerative picture, and is directed by the clinical suspicion rather than requested as a screen. [8]
[9]Management — Resuscitation
Tics are not a medical emergency, and the first act of management is reassurance. Most children who present with tics have mild, fluctuating movements that will not damage the brain and that will improve with age, and for these children the correct management is psychoeducation, watchful waiting, and no drug. Explaining the natural history, that tics peak around ten to twelve years and improve for most through adolescence, and that the brain is not being harmed, is itself a powerful intervention that lifts anxiety from the whole family. [2]
The situation that does demand prompt attention at first presentation is not the tic but a comorbidity crisis. An acute flare of obsessive-compulsive disorder, a decompensation of attention-deficit or hyperactivity disorder with severe school failure, a self-injurious tic, a distressing rage attack, or a child made miserable by social stigma each needs an immediate response. Drawing blood, chasing a scan, or starting an antipsychotic for a mild tic reassures no one and exposes the child to harm, so the acute task is to listen for what is actually impairing the child and to target that first. [6]
Safety-netting closes the first encounter. The family is told that tics fluctuate, that a worsening week does not mean deterioration, and that certain features warrant earlier review, including self-injury, sudden marked worsening, new obsessive-compulsive or behavioural symptoms, and any regression or new neurological sign. The child is booked for follow-up to re-assess severity and comorbidity over time, because the trajectory of tics and the burden of the comorbidities are revealed over months, not in a single visit. [2]
Management — Definitive & Stepwise
Definitive management is stepped, and the step is chosen by the impairment the tics cause, not by their appearance. The 2019 American Academy of Neurology guideline and the 2022 European clinical guidelines converge on a single ladder that moves from the least to the most intensive intervention, always treating the comorbidities in parallel. The guiding principle is that treatment aims at function, at school attendance, friendships, and self-esteem, and never at the elimination of every tic, which is neither achievable nor desirable. [2] [5]
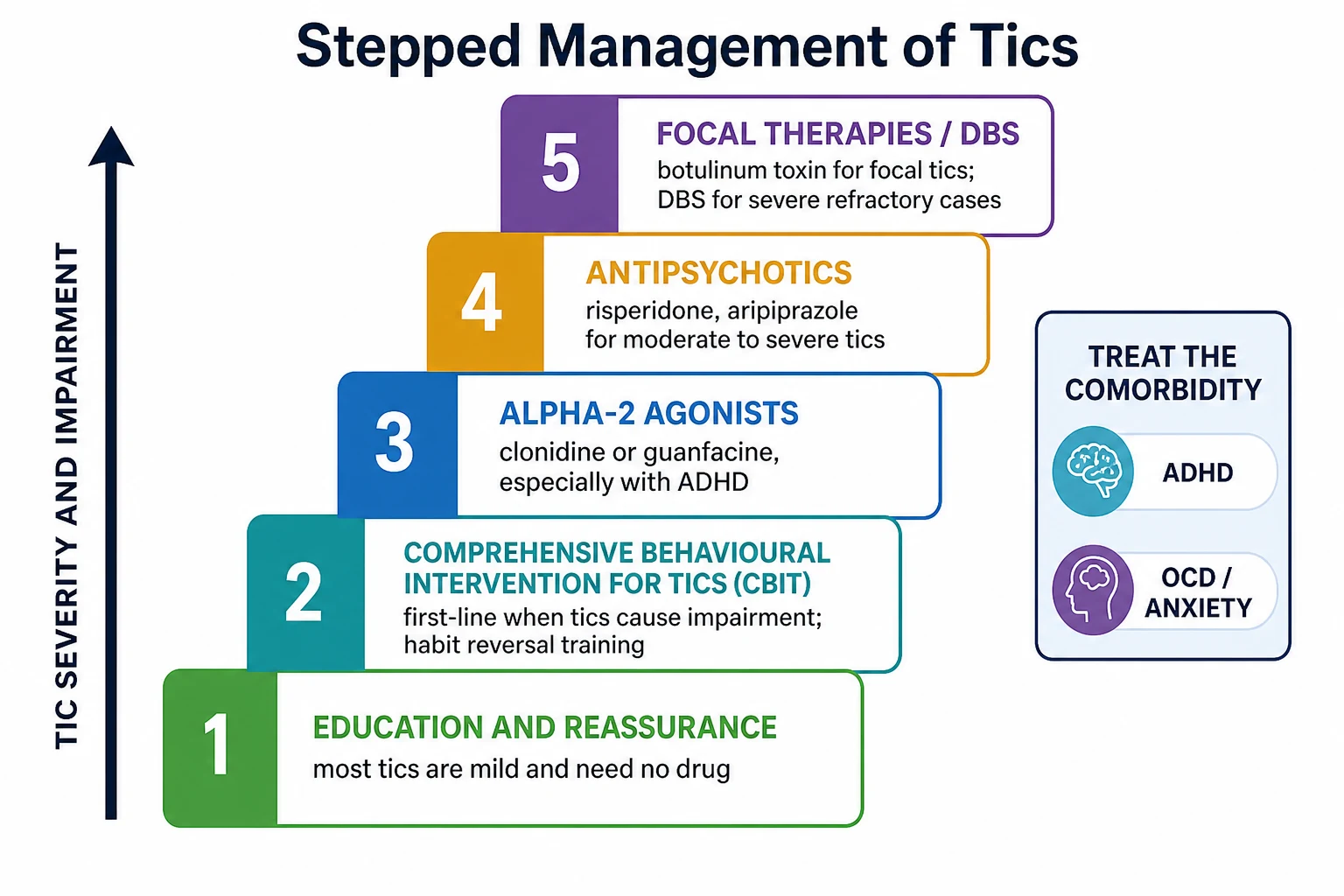
Step one is psychoeducation, reassurance, and watchful waiting, and for most children this is enough. Step two, when tics cause distress, pain, social stigma, or functional impairment, is Comprehensive Behavioural Intervention for Tics, or CBIT. CBIT is an eight-session structured therapy built on habit reversal training, which teaches the child to recognise the premonitory urge and to perform a competing response that is physically incompatible with the tic. The Piacentini randomised trial showed that CBIT significantly reduced tic severity compared with supportive therapy, and it is endorsed as first-line active treatment by both the American and European guidelines. [1] [4]
The stepped ladder for impairing tics
Psychoeducation, reassurance, and watchful waiting for mild tics
Comprehensive Behavioural Intervention for Tics when tics cause impairment
Alpha-2 agonists, clonidine or guanfacine, especially with comorbid ADHD
Antipsychotics, risperidone or aripiprazole, for moderate to severe tics with monitoring
Botulinum toxin for a focal disabling tic, or deep brain stimulation for severe refractory disease
Step three brings in pharmacotherapy, and the preferred first drugs are the alpha-2 agonists clonidine and guanfacine. These are chosen first because they have a safer profile than antipsychotics and because they also treat attention-deficit or hyperactivity disorder, which coexists in most children needing a drug. Clonidine is started low, around 25 to 50 micrograms a day and titrated to a usual range of about 50 to 200 micrograms per day in divided doses, and guanfacine extended-release is titrated from about 1 mg toward 1 to 4 mg per day, with blood-pressure and sedation monitoring throughout. The 2019 American Academy of Neurology guideline endorses the alpha-2 agonists as treatment options for tics. [2] [5]
Step four is the antipsychotics, the most effective tic-suppressing drugs, reserved for moderate to severe impairment because of their safety profile. Risperidone and aripiprazole are the most used, started low and titrated to effect, risperidone typically from about 0.25 mg toward 1 to 3 mg per day and aripiprazole from about 1 to 2 mg toward a target of a few milligrams per day, with weight, metabolic, and extrapyramidal monitoring. Haloperidol and pimozide are effective but now rarely first choice because of their adverse-effect burden and, for pimozide, QT prolongation. The European guideline endorses aripiprazole and risperidone as the recommended antipsychotics, with tiapride and clonidine for milder disease. [5]
Clonidine (alpha-2 agonist)
Dose
Start low, about 25 to 50 micrograms a day, titrated to a usual range of about 50 to 200 micrograms per day in divided doses
Step five addresses the focal or refractory case. Botulinum toxin injection into a single overactive muscle can reduce a focal, painful, or socially disabling tic such as a dystonic neck jerk, and the Marras randomised trial showed modest benefit for simple motor tics and for the premonitory urge in the injected muscle. Deep brain stimulation of thalamic or pallidal targets is reserved for a small number of adults and older adolescents with severe, refractory, disabling tics that have failed behavioural and pharmacological treatment, and it requires specialist multidisciplinary assessment. [10]
Aripiprazole (second-generation antipsychotic)
Dose
Started low, about 1 to 2 milligrams, titrated toward a target of a few milligrams per day by a specialist
The comorbidities are treated in parallel, because they usually cause more impairment than the tics. Attention-deficit or hyperactivity disorder is managed with behavioural strategies and, when needed, with stimulant or non-stimulant medication, and the modern evidence shows that stimulants do not routinely worsen tics, so effective attention-deficit or hyperactivity disorder treatment should not be withheld on that account. Obsessive-compulsive disorder is treated with cognitive behavioural therapy using exposure and response prevention, with a selective serotonin reuptake inhibitor for the obsessive-compulsive component. Anxiety, mood, rage, and learning difficulties are addressed with their own evidence-based interventions. [6]
Specific Subtypes & Scenarios
Provisional tic disorder, the commonest presentation in young children, is the scenario that most rewards restraint. The tics have been present for under a year, the prognosis for spontaneous resolution is good, and the correct management is reassurance, watchful waiting, and a review appointment rather than a diagnosis of Tourette. The family is told what to watch for and is spared the anxiety of a premature label, and the clinician re-assesses if the tics persist beyond a year or if comorbidities emerge. [2]
The child with Tourette and comorbid attention-deficit or hyperactivity disorder is the most common complex scenario and the one that most often needs a drug. Here the alpha-2 agonists are attractive because they can address both the tics and the attention-deficit or hyperactivity disorder, and careful stimulant use remains an option when attention-deficit or hyperactivity disorder is the dominant impairment, with the evidence now showing that stimulants do not routinely exacerbate tics. The child with Tourette and obsessive-compulsive disorder needs cognitive behavioural therapy with exposure and response prevention for the obsessive-compulsive component, with a selective serotonin reuptake inhibitor when the symptoms are moderate to severe, and the tics and the obsessive-compulsive disorder are tracked separately because their trajectories diverge. [6]
PANS, paediatric acute-onset neuropsychiatric syndrome, and its post-streptococcal subtype PANDAS, present with the abrupt, dramatic onset of obsessive-compulsive symptoms or severe food restriction together with concurrent tics, anxiety, behavioural regression, or deterioration in school performance, often following an infection. The PANS consensus criteria guide the clinical evaluation, and management involves paediatric neurology and psychiatry, treatment of the obsessive-compulsive and tic symptoms with behavioural and pharmacological means, and evaluation and treatment of any triggered infection. The role of immune-modulating treatments such as antibiotics, intravenous immunoglobulin, and plasma exchange remains debated, and these are reserved for specialist centres. [8]
Rage attacks, sudden explosive outbursts of anger that are disproportionate and often frightening to the family, and self-injurious tics such as slapping or head-banging, are the behavioural complications that most distress families and most often bring a child to urgent care. These are managed with behavioural strategies, with treatment of the comorbidities that drive them, and with pharmacotherapy directed at the tics and the mood where appropriate, and the family needs explicit safety advice and a clear plan for escalation. [6]
Complications & Pitfalls
The complications of Tourette syndrome are the disabilities caused by the tics and their comorbidities, not damage done to the brain by the tics themselves. Untreated comorbid attention-deficit or hyperactivity disorder erodes school achievement, untreated obsessive-compulsive disorder and anxiety erode daily function and wellbeing, and untreated learning difficulty leaves a child struggling without support. Self-injurious tics can cause real physical harm, coprolalic tics can isolate and stigmatise a child, and the social burden of visible tics can damage self-esteem and friendships, which is why the quality-of-life measures track the comorbidities far more closely than they track the tic count. [6]
[6]The avoidable pitfalls cluster around four errors. The first is diagnosing Tourette only when coprolalia appears, when it is uncommon and never required; the diagnosis rests on motor plus vocal tics over a year with onset before 18. The second is over-investigating a typical child with scans, bloods, and electroencephalograms that reassure no one and that stigmatise and delay. The third is prescribing an antipsychotic for mild tics that needed only reassurance, exposing the child to weight gain, metabolic risk, and extrapyramidal effects for no functional gain. The fourth is attributing a tic flare to a stimulant and withholding effective attention-deficit or hyperactivity disorder treatment, when the evidence shows stimulants do not routinely worsen tics and the untreated attention-deficit or hyperactivity disorder is doing more harm. [2]
Prognosis & Disposition
The prognosis of Tourette syndrome is favourable for the tics themselves, and communicating this clearly is part of the treatment. Tic severity peaks around ten to twelve years and then improves substantially for the majority of children through late adolescence and early adulthood, with only a minority carrying severe tics into adult life. The Bloch longitudinal cohort showed that tic severity falls through adolescence even as obsessive-compulsive symptom severity persists or rises, which is why follow-up must keep asking about the obsessive-compulsive component and not only about the movements. [11]
Disposition is matched to severity and comorbidity. Mild tics with no comorbidity are managed in primary care with psychoeducation, school support, and follow-up. Diagnostic uncertainty, moderate tics, or a suspected secondary cause prompts referral to paediatric neurology. Significant attention-deficit or hyperactivity disorder, obsessive-compulsive disorder, anxiety, learning difficulty, rage attacks, or self-injurious tics prompt multidisciplinary involvement with paediatric psychology and psychiatry, behavioural therapy services, and the school learning-support team. The family is counselled that tics fluctuate, that treatment targets impairment and function rather than tic elimination, and that the long-term outlook is good. [2]
The prognosis for quality of life hinges on the comorbidities, which is the single most useful sentence a clinician can offer a family at the first visit. A child whose tics fade but whose attention-deficit or hyperactivity disorder, obsessive-compulsive disorder, and anxiety are left untreated will not thrive, while a child whose tics persist but whose comorbidities are well managed can flourish. This is why the comorbidity screen is repeated at every visit and why the plan is built around function, not around the visible movements. [6]
Special Populations
Children with disability and neurodiversity, including autism spectrum disorder and intellectual disability, present a particular challenge because their repetitive movements blur the boundary between stereotypies and tics. The defining phenomenology, the premonitory urge and the suppressibility, may be hard for a child with limited communication to report, so behavioural signs and carer report take greater diagnostic weight. Behavioural management is adapted to the child's developmental level, and the comorbidities, which are frequent, demand coordinated multidisciplinary care. [6]
Adolescent boys approaching the age of peak tic severity face the greatest social and self-esteem burden, because visible and vocal tics collide with the developmental tasks of adolescence. This is the group that most benefits from Comprehensive Behavioural Intervention for Tics, from school accommodation, and from prompt treatment of the anxiety and obsessive-compulsive symptoms that so often emerge alongside. The clinician must also ask directly about mood, self-harm, and substance use, because the psychosocial burden is real. [11]
Children in out-of-home care and those facing psychosocial adversity may present with tic exacerbation driven by stress, because tics worsen with anxiety and psychosocial disruption. These children need a trauma-informed assessment that looks beyond the movements to the environment sustaining them, and the plan must address safety, stability, and schooling alongside the tics and their comorbidities. [6]
Evidence, Guidelines & Regional Differences
The international evidence has converged on clear principles. The diagnosis is clinical and built on DSM-5 criteria. The Piacentini randomised trial established Comprehensive Behavioural Intervention for Tics as effective, and the 2022 European psychological guideline and the 2019 American Academy of Neurology guideline both endorse it as first-line active treatment for impairing tics. The 2019 American Academy of Neurology guideline and the 2022 European pharmacological guideline endorse the alpha-2 agonists and the antipsychotics as pharmacological options, with the antipsychotics effective but requiring metabolic and extrapyramidal safety monitoring. [1] [2] [4] [5]
The controversies are live and examinable. Whether stimulants worsen tics was a long-standing concern that the modern evidence has largely refuted, so effective attention-deficit or hyperactivity disorder treatment is no longer withheld on tic grounds alone. The role of cannabis-based products for tics has been studied, and the American Academy of Neurology found insufficient evidence of benefit, so they are not recommended. PANS and PANDAS remain a focus of active debate: the abrupt post-streptococcal onset of tics and obsessive-compulsive symptoms is recognised, but the role of immune-modulating treatments such as antibiotics, intravenous immunoglobulin, and plasma exchange is contested and is reserved for specialist centres. [2] [3]
Piacentini 2010, JAMA
Population: 126 children aged 9 to 17 with Tourette or chronic tic disorder
Key finding
CBIT produced significantly greater reduction in tic severity than supportive therapy
Regional practice is concordant across Australia and New Zealand, the United Kingdom, North America, and Europe, because the guidelines agree. The Australian and New Zealand approach follows the Royal Children's Hospital Melbourne pathway, the American Academy of Neurology 2019 guideline, and the European clinical guidelines, all converging on a clinical diagnosis, a comorbidity-led assessment, a stepped plan beginning with reassurance and CBIT, and risk-stratified pharmacotherapy. The differences are practical rather than principled, principally in access to behavioural therapy and specialist services, which telehealth and primary-care-led plans aim to bridge. [2] [5]
Exam Pearls
Tourette disorder needs multiple motor tics plus at least one vocal tic, present for over a year, with onset before age 18, and coprolalia is neither required nor common, occurring in only a minority. The phenomenology that defines a tic is the premonitory urge, the suppressibility with rebound, and the waxing-and-waning, body-shifting course, and these features separate a tic from a stereotypy, a myoclonic jerk, a choreiform movement, and the restlessness of attention-deficit or hyperactivity disorder. The diagnosis is clinical, made on history and home video, and there is no scan or blood test for Tourette syndrome. [2]
The comorbidities are the question, because they drive the impairment and the management. About 60 per cent of children with Tourette have attention-deficit or hyperactivity disorder and about 30 per cent have obsessive-compulsive disorder, with anxiety, learning difficulty, rage attacks, and self-injurious behaviour also common. Treating these in parallel with the tics is the whole art of management, and missing them by focusing only on the movements is the cardinal error. [6]
[2] [5]Two final facts that examiners reward. Tics peak around 10 to 12 years and improve for most children through adolescence, so the prognosis for the movements is good, even though obsessive-compulsive symptoms may persist or rise. And stimulants do not routinely worsen tics, so effective attention-deficit or hyperactivity disorder treatment should not be withheld on tic grounds alone, a fact that corrects a long-standing and now outdated clinical fear. [11] [6]
TICS
References
- [1]Piacentini J, Woods DW, Scahill L, et al Behavior therapy for children with Tourette disorder: a randomized controlled trial. JAMA, 2010.PMID 20483969
- [2]Pringsheim T, Okun MS, Muller-Vahl K, et al Practice guideline recommendations summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology, 2019.PMID 31061208
- [3]Pringsheim T, Holler-Managan Y, Okun MS, et al Comprehensive systematic review summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology, 2019.PMID 31061209
- [4]Andren P, Jakubovski E, Murphy TL, et al European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part II: psychological interventions. Eur Child Adolesc Psychiatry, 2022.PMID 34313861
- [5]Roessner V, Eichele H, Stern JS, et al European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part III: pharmacological treatment. Eur Child Adolesc Psychiatry, 2022.PMID 34757514
- [6]Hirschtritt ME, Lee PC, Pauls DL, et al Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry, 2015.PMID 25671412
- [7]Khalifa N, von Knorring AL Prevalence of tic disorders and Tourette syndrome in a Swedish school population. Dev Med Child Neurol, 2003.PMID 12729145
- [8]Chang K, Frankovich J, Cooperstock M, et al Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): recommendations from the 2013 PANS Consensus Conference. J Child Adolesc Psychopharmacol, 2015.PMID 25325534
- [9]Leckman JF, Riddle MA, Hardin MT, et al The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry, 1989.PMID 2768151
- [10]Marras C, Andrews D, Sime E, Lang AE Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology, 2001.PMID 11245710
- [11]Bloch MH, Peterson BS, Scahill L, et al Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch Pediatr Adolesc Med, 2006.PMID 16389213
- [12]Hirschtritt ME, Darrow SM, Illmann C, et al Genetic and phenotypic overlap of specific obsessive-compulsive and attention-deficit or hyperactive subtypes with Tourette syndrome. Psychol Med, 2018.PMID 28651666