Paeds · ophthalmology
Congenital cataract and glaucoma
Also known as Infantile cataract · Congenital cataract · Primary congenital glaucoma · Buphthalmos · Aphakic glaucoma · Childhood glaucoma · Leukocoria
Fellowship topic on congenital cataract and glaucoma: why a lens opacity or a raised intraocular pressure in the first weeks of life is an emergency for the developing visual system. Covers deprivation amblyopia and the critical-period surgical window for dense unilateral cataract (by about 6 weeks) and bilateral cataract (by 6 to 10 weeks); the Childhood Glaucoma Research Network classification of paediatric glaucoma into primary congenital glaucoma (PCG), glaucoma with non-acquired ocular anomalies (Peters, aniridia, Axenfeld-Rieger), glaucoma with non-acquired systemic syndromes (Sturge-Weber, NF1), and acquired secondary glaucoma including glaucoma following cataract surgery; the classic PCG triad of epiphora, photophobia and blepharospasm with buphthalmos and Haab striae; the red-reflex (Brückner) test and the leukocoria differential including retinoblastoma; examination under anaesthesia with intraocular pressure, corneal diameter and disc cupping; the Infant Aphakia Treatment Study evidence on aphakia versus primary intraocular lens; the surgical ladder for PCG (goniotomy, 360-degree trabeculotomy, trabeculectomy with mitomycin C, drainage device, cycloablation); the drugs to avoid in the infant eye including brimonidine; and lifelong glaucoma surveillance after cataract surgery.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A baby is born with a visual system that is wired only in rough draft. Over the first months and years of life the brain refines that wiring, keeping the connections that carry a sharp, matching picture from each eye and pruning the ones that do not. Anything that blurs the picture during this critical and sensitive period — a cataract, or the corneal oedema and optic-nerve damage of glaucoma — permanently weakens the pathway from that eye. That permanent weakness is amblyopia, and it is the reason these two conditions are time-critical and the reason a general paediatric clinician sits at the front door of both of them. Most cases are found, or missed, at the red-reflex examination. [11]
This topic covers both diseases together because they share that single clock, because glaucoma is itself the commonest serious complication of cataract surgery, and because an examiner who asks about one will follow with the other. The cataract half is about recognising an abnormal red reflex and operating before amblyopia is locked in; the glaucoma half is about recognising the tearing, light-averse infant and re-establishing aqueous outflow before the globe is damaged. [3]
Overview & Definition
A cataract is any opacity of the crystalline lens. In an adult it dims vision slowly over years; in an infant it blocks the picture the brain needs to finish wiring the eye, so the harm accrues in weeks. A congenital cataract is present at birth or recognised in the first months, and an infantile cataract appears within the first year; the distinction matters less than the density and the timing, because both demand urgent decisions about surgery. [1]
Glaucoma in a child means sustained damage to the optic nerve from raised intraocular pressure (IOP), and in infancy the pressure does something it never does in an adult: because the infant sclera is elastic, the eye enlarges under pressure. That enlarged, tearing, light-hating eye is buphthalmos ("ox eye"), and it is the hallmark of primary congenital glaucoma (PCG), the commonest glaucoma of infancy, caused by maldevelopment of the anterior-chamber angle. [2]
Two definitions carry the whole topic. Deprivation amblyopia is the permanent cortical blindness that follows when a sharp image is withheld from an immature eye — the engine of urgency in cataract. And aphakic glaucoma (more precisely, glaucoma following cataract surgery) is the delayed, often silent rise in pressure that can blind a child who did well from their cataract operation — the reason every postoperative cataract child is a glaucoma patient for life. [3]
Classification
Both diseases sort cleanly, and examiners reward a candidate who can hold the two trees at once. The figure below lays them side by side; the two blocks of text explain how each is built. [9]
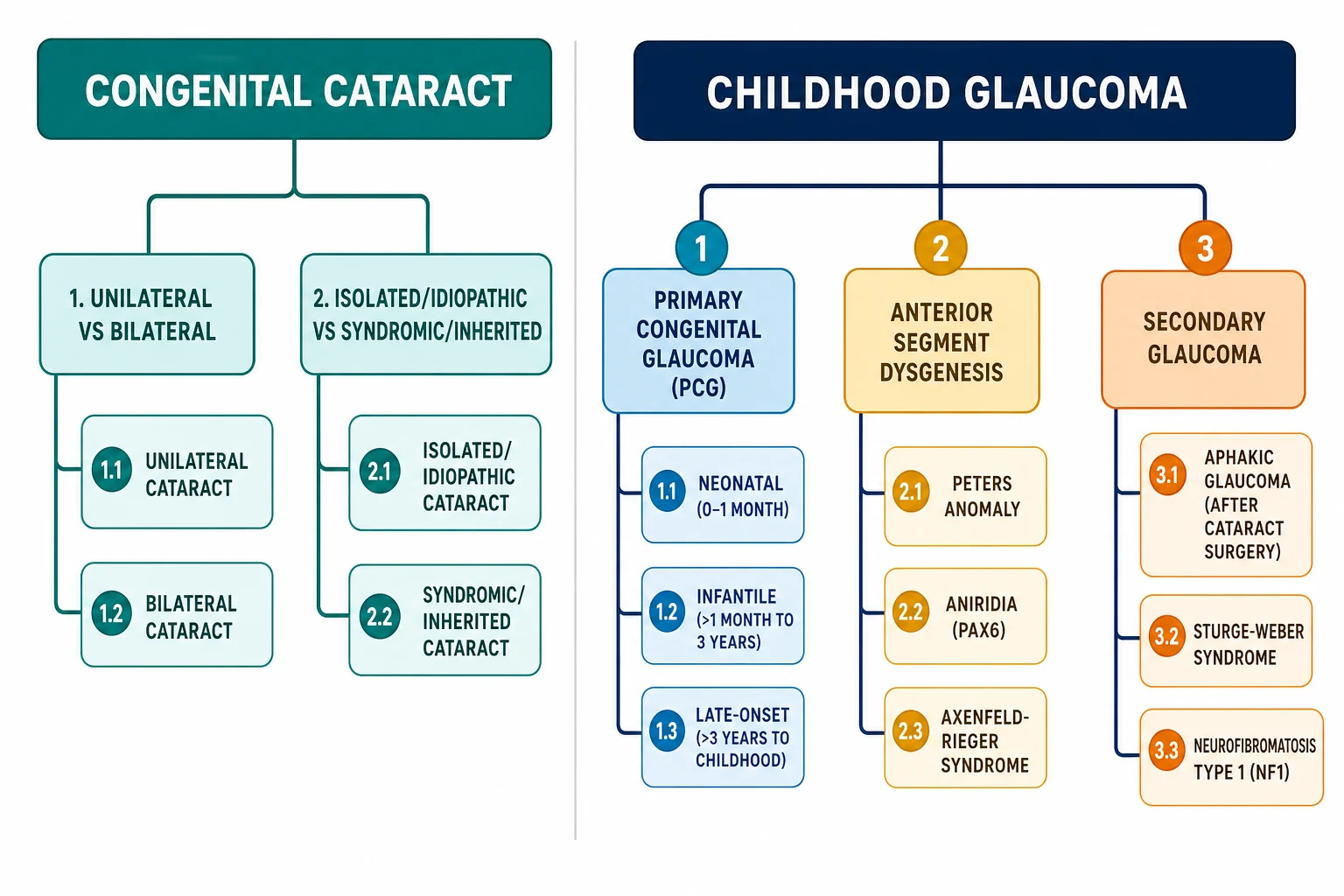
Congenital cataract is described along three axes at once. The first is laterality: a unilateral cataract is usually isolated, sporadic and idiopathic, and because the other eye sees well it is easily missed; a bilateral cataract is far more often hereditary or part of a systemic syndrome. The second is morphology, which points to a cause — a dense central nuclear cataract is typically present at birth and the most amblyogenic; a lamellar cataract sits between the nucleus and cortex and may be inherited; a posterior polar cataract lies on the visual axis and is stubbornly amblyogenic; anterior polar and sutural opacities are often small and watched. The third is aetiology: about one-third of bilateral cases are autosomal dominant crystallin-opathy, and the rest divide among metabolic disease (galactosaemia), intrauterine infection (congenital rubella), chromosomal syndromes (Down syndrome) and recognised syndromes (Lowe, Alport). [1]
Childhood glaucoma uses the Childhood Glaucoma Research Network (CGRN) / 9th-consensus framework, which sorts cases by whether the angle maldevelopment is isolated or accompanied by other ocular or systemic anomalies. [9]
The single most important row for a general paediatric trainee is the last one: glaucoma following cataract surgery. It is common, it is silent, and it can take a child who saw well after lensectomy and quietly erode that vision years later. [3]
Epidemiology & Risk Factors
Congenital and infantile cataract is uncommon but not rare. Population studies put the birth prevalence at roughly 3 to 4 per 10,000 live births in high-income settings, with bilateral disease in about half; the Danish nationwide series of more than a thousand cases remains the benchmark for how these cases split between hereditary, metabolic, infectious and idiopathic causes, with roughly one in ten of all cases attributable to a recognised systemic or syndromic process and the largest single group still idiopathic. [1]
Primary congenital glaucoma is rarer, with a birth prevalence around 1 in 10,000 to 1 in 18,000 in outbred populations but markedly higher — up to 1 in 2,500 — where consanguinity is common, reflecting its autosomal-recessive genetics. It accounts for the majority of childhood glaucoma seen in infancy, and it is the diagnosis behind most cases of buphthalmos in a baby. [2]
The risk factors that matter most are the ones you can act on, and they cluster around timing. For aphakic glaucoma, the dominant risk is age at cataract surgery — operating in the first weeks of life, particularly before about 9 months, carries a far higher glaucoma rate than operating later, because the immature angle is more vulnerable to inflammation and structural change. Other independent risks are microcornea, primary intraocular lens implantation in infancy, posterior capsule plaque, postoperative visual-axis opacification and nuclear morphology. [3]
The systematic synthesis of these risks changed practice. The individual-patient-data meta-analysis of glaucoma after infantile cataract surgery confirmed that a child operated very young is a child who must be watched for pressure for years — a finding the Infant Aphakia Treatment Study and the IoLunder2 cohort then sharpened, as the next sections describe. [4]
Pathophysiology
The mechanism of permanent harm is different in the two diseases, and both depend on the immaturity of the eye and brain. The figure on the next screen shows them side by side. [2]
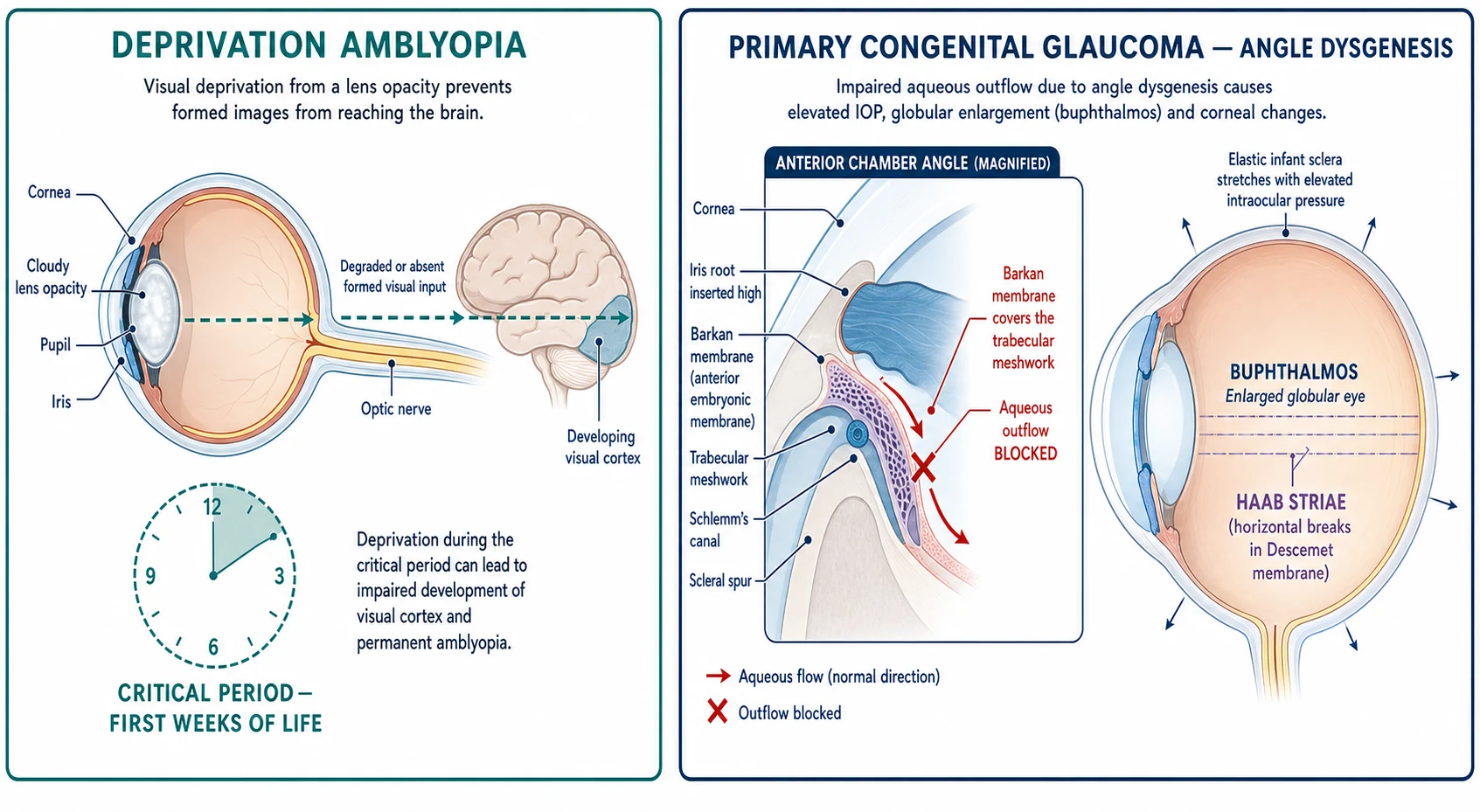
Deprivation amblyopia is the core concept of the cataract half. The visual cortex is not born equal to its task; it requires a equally sharp, well-aligned image from each eye during a critical period — most intense in the first 6 to 8 weeks for unilateral deprivation, and a broader sensitive period that runs to about 7 to 9 years. A dense cataract that occupies the visual axis denies the cortex that sharp input, so the cortical cells dedicated to that eye never develop normal receptive fields, and the connection is permanently weakened. The consequence is asymmetric: a unilateral cataract is devastating because the better eye wins the cortical competition and suppresses the deprived one, so even a small unilateral opacity is dangerous; a bilateral dense cataract is less competitive but still amblyopic, and delays vision so that sensory nystagmus appears around 2 to 3 months if both eyes are still opaque. This is the entire biological justification for operating within weeks, not months. [7]
Primary congenital glaucoma is a developmental failure of the angle, not a disease of the adult outflow apparatus wearing thin. The trabecular meshwork and Schlemm canal fail to complete their separation from the overlying mesenchyme, leaving a high, flat iris insertion and an abnormal, membrane-like tissue (the traditional Barkan membrane) over the meshwork that resists aqueous outflow. Aqueous is produced continuously by the ciliary body, so the resistance drives intraocular pressure up, and that pressure then does two things an adult eye cannot do. First, because the infant sclera and cornea are still elastic, the whole globe enlarges into buphthalmos, and the cornea stretches so that breaks open in Descemet membrane — Haab striae — which then heal as ridges and, with the oedema they cause, cloud the cornea and add a second source of amblyopia. Second, the pressure crushes the optic-nerve axons, producing the cupping and field loss of adult glaucoma but doing so in a cortically immature eye, so the loss is compounded by amblyopia. [2]
Glaucoma following cataract surgery has a more mechanical and inflammatory pathophysiology. Removing the lens in infancy alters the angle architecture, leaves the eye exposed to postoperative inflammation and retained lens material, and — when a primary intraocular lens is implanted — sets up a new anatomical relationship between iris, capsule and angle that promotes synechiae. The immature angle of a very young infant is least able to tolerate this, which is exactly why early surgery is the dominant risk factor. [3]
Clinical Presentation
A congenital cataract announces itself in one of four ways, and only one of them is glamorous. The leukocoria — a white pupil seen by a parent in a photograph taken with flash, or found by a clinician — is the classic and the most feared, because the same white reflex is produced by retinoblastoma. Far more often the discovery is an abnormal or absent red reflex at a routine newborn or infant check, which is why that test exists. A unilateral cataract may instead declare itself as a strabismus, because the eye with the cataract drifts once it stops seeing; and a bilateral dense cataract eventually produces a searching, sensory nystagmus by 2 to 3 months as the cortex, starved of any fixation target, begins its oscillating search. The trap is the small, unilateral posterior polar cataract that produces neither leukocoria nor obvious strabismus and is only caught by a red reflex done properly. [1]
Primary congenital glaucoma has its own unmistakable signature, the triad of epiphora, photophobia and blepharospasm. The baby has a watery eye (epiphora), squeezes it shut against light (photophobia with blepharospasm), and is brought in for what is often misdiagnosed as conjunctivitis or a blocked tear duct. The signs that distinguish it from those mimics are on the eye itself: the cornea is cloudy or oedematous, often with visible Haab striae; the eye is enlarged (buphthalmos) compared with its fellow; and over time the cornea becomes more hazy and the optic disc cups. Because the presentation overlaps so easily with trivial causes, any infant with persistent tearing plus light sensitivity must have the cornea and the disc looked at, not just the tear duct. [2]
The atypical presentations are the ones that cost vision. A late-onset PCG may declare itself only in a toddler or school-age child with myopia or visual blur and no buphthalmos, because the sclera has stiffened past the age of easy stretching. A child with Sturge-Weber may present with seizures and a facial port-wine stain in the ophthalmic division of the trigeminal nerve, with the glaucoma found only when the eye is examined. And the child with aniridia presents with nystagmus and poor vision from foveal hypoplasia, with the glaucoma arriving years later as the angle progressively closes. [9]
Differential Diagnosis
The leukocoria differential is one of the highest-yield lists in paediatric ophthalmology, because it is the gateway to retinoblastoma. The list must be held in order of danger, and the feature that distinguishes each must be named. [12]
The principle is to work outward from the lens. An opacity in the lens is a cataract; an opacity behind a clear lens is retinoblastoma until imaging proves otherwise; a small eye with a retrolental mass is persistent fetal vasculature; a clear media with an elevated, exudative retina is Coats disease or a detachment. The red reflex and a careful penlight view of the lens position this decision, but the definitive distinction of a retrolental lesion is made by the ophthalmologist with ultrasound under anaesthesia. [12]
For the tearing infant, the differential turns on whether the cornea is clear. Nasolacrimal duct obstruction gives a mucopurulent, reflux-positive watery eye with a clear cornea and a comfortable child. Conjunctivitis is bilateral or crusted, without corneal clouding or enlargement. Corneal abrasion or foreign body is acutely painful with fluorescein uptake. Primary congenital glaucoma is the diagnosis that is missed when any of these is assumed instead: it alone combines tearing with a cloudy, enlarged cornea and photophobia. [2]
A cloudy cornea at birth raises a separate, narrower list. Birth trauma from forceps produces vertical Descemet breaks (distinct from the horizontal Haab striae of glaucoma). Peters anomaly presents with a central corneal opacity and iridocorneal adhesion, often with a cataract. Metabolic clouding (the corneal haze of mucopolysaccharidoses or the storage of cystinosis) and congenital hereditary endothelial dystrophy round out the newborn differential, and each is separated by the presence or absence of raised pressure and of enlargement. [2]
Clinical & Bedside Assessment
The red-reflex test is the single highest-yield examination a general paediatric clinician performs, and it is done badly as often as it is done well. Perform it in a dimmed room, with a direct ophthalmoscope held about half a metre (an arm's length) from the child, the large light spot selected, and the focussing ring set to roughly 0 to +2 dioptres so the light beam is collimated. Shine it at both eyes at once and compare; then close each eye in turn. A normal reflex is an even orange-red glow filling both pupils symmetrically. Abnormality is anything that interrupts, darkens, whitens or makes asymmetric that glow — a cataract may show a dark pupillary void, a retinoblastoma a white reflex, and anisometropia or strabismus an unequal brightness. This same test, comparing both pupils, is the Brückner method, and an abnormal Brückner reflex is a reason to refer regardless of how well the child appears to see. [11]
For the suspected glaucoma infant, the bedside assessment adds three signs. Measure or at least compare the corneal diameters: a horizontal corneal diameter greater than about 11 mm in a newborn or 12 mm in an infant is abnormal, and frank buphthalmos reaches 13 to 15 mm. Look at the corneal surface for the stromal haze of oedema and, in the right light, the curvilinear ridges of Haab striae. And look at the optic disc with a direct ophthalmoscope through a dilated pupil if you can — asymmetry of cupping, or a cup-to-disc ratio above 0.3 in an infant, is suspicious. The full examination, including a true tonometry and gonioscopy, is done by the ophthalmologist under anaesthesia. [2]
The general paediatric and dysmorphology examination is where the syndromic cataract or glaucoma is found. Listen for a heart murmur and look at the hearing and the growth in a child with bilateral cataract, because congenital rubella affects all three; look for cataract with hypotonia and failure to thrive in a boy, raising Lowe syndrome; check for a port-wine stain in the ophthalmic distribution, café-au-lait macules and axillary freckling (NF1), midface hypoplasia and skeletal anomalies; and examine the parents, because a hereditary cataract may be visible in a parent who never knew they had one. [1]
Investigations
The diagnosis of congenital cataract is clinical — a lens opacity seen on penlight and red-reflex examination — and the role of investigation is to find the cause and to plan surgery, not to confirm the cataract. For a bilateral cataract, the systemic work-up looks for the treatable and the inherited: galactosaemia (a red-cell galactose-1-phosphate uridyltransferase assay, and urine reducing substances), serum calcium and glucose, TORCH serology (especially rubella), a karyotype if Down syndrome is suspected, and targeted genetic testing for the syndromes suggested by the examination (OCRL for Lowe, COL4A for Alport). For a unilateral cataract the yield of systemic testing is low, and the emphasis is on urgent ophthalmology and exclusion of retinoblastoma. [1]
The diagnosis of childhood glaucoma is also clinical, but it is locked down at an examination under anaesthesia (EUA), because a baby cannot cooperate with tonometry, gonioscopy and funduscopy. At the EUA the ophthalmologist measures four things: intraocular pressure (using rebound tonometry, an iCare or a Perkins applanation, recognising that anaesthesia and crying both distort the reading, so the first, calmest measurement is the one to trust); corneal diameter; refraction (the axial elongation of buphthalmos produces myopia and astigmatism); and the optic disc for cupping. Gonioscopy defines the angle anomaly. The diagnosis is made from the constellation — a raised pressure, an enlarged or oedematous cornea, Haab striae and cupping — not from any single number. [2]
Genetic testing now sits inside the work-up of both diseases and has become more useful as panels have grown. CYP1B1 sequencing is indicated in familial or consanguineous primary congenital glaucoma; PAX6 in aniridia; FOXC1 or PITX2 in Axenfeld-Rieger; and the crystallin and developmental genes in hereditary cataract. A confirmed molecular diagnosis informs counselling, recurrence risk and — for some cataracts and angle anomalies — prognosis, and it is increasingly expected at fellowship level. [9]
Management — Resuscitation
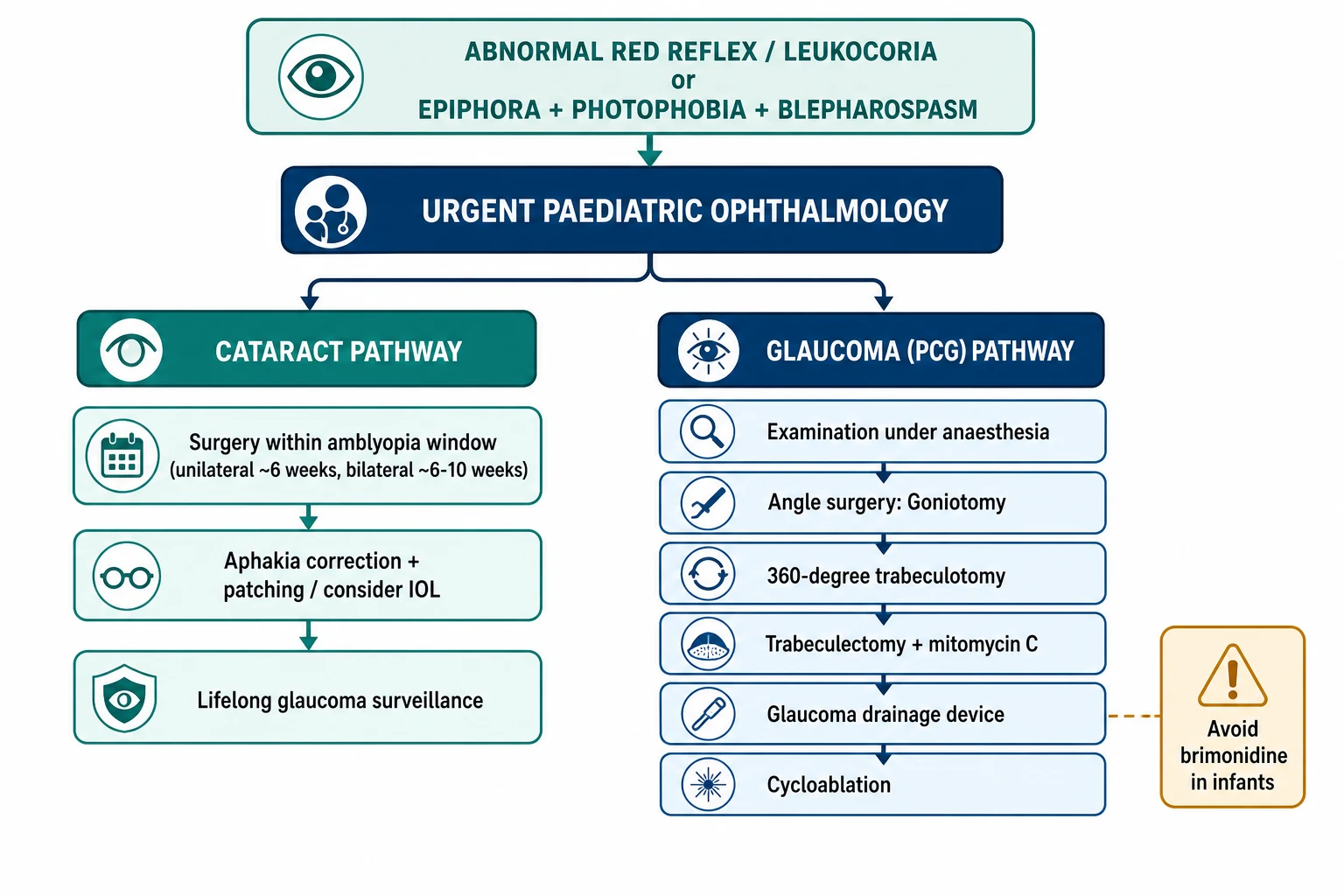
There is no resuscitative "bundle" of fluids or drugs for these diseases, but there is a time-critical first action that does the same job: the moment an abnormal red reflex, leukocoria or the glaucoma triad is found, the child is referred urgently to paediatric ophthalmology. For leukocoria or an absent white reflex the referral is same-day or within days, because retinoblastoma cannot be excluded by the generalist; for a confirmed dense congenital cataract the clock is the amblyopia clock and the surgeon is booked within days to weeks; for suspected primary congenital glaucoma the child is seen within days, because every week of raised pressure stretches and scars the cornea and cups the disc further. [11]
While the surgical date is being set, two things protect the cataract eye. First, confirm the cataract is dense and axial rather than a small, off-axis opacity that may be watched — the surgeon decides this. Second, in a unilateral cataract begin planning the amblyopia strategy: once the lens is out the eye will be left aphakic or pseudophakic and will need optical correction and patching of the good eye, so set family expectations early that the operation is the start of treatment, not the end. For the glaucoma infant, a short course of topical pressure-lowering drops may be started by the ophthalmologist to clear corneal oedema before surgery, but definitive treatment is surgical and not delayed for medical control. [10]
Management — Definitive & Stepwise
The definitive management of the two diseases is surgical, and both have stepped ladders. The figure on the next screen is the map of both pathways. [10]
Congenital cataract: the surgical window and the aphakia question
The operation is a lensectomy with anterior vitrectomy, and the non-negotiable variable is the timing. A dense unilateral congenital cataract is operated by about 6 weeks of age (ideally within the first 4 to 6 weeks), because the unilateral critical period is brutal and brief; a dense bilateral cataract is operated within about 6 to 10 weeks, operating the second eye within a week or two of the first so the eyes compete on equal terms. These windows are not arbitrary delays — they balance the steeply rising risk of deprivation amblyopia against the higher rate of aphakic glaucoma that comes with operating a very young eye. [7]
The Infant Aphakia Treatment Study (IATS) answered the question that follows: in a unilateral infantile cataract, should the surgeon leave the child aphakic and correct with a contact lens, or place a primary intraocular lens (IOL)? At 4.5 years the two groups had no difference in visual acuity, but the primary-IOL group had substantially more reoperations and more glaucoma. The practical conclusion, now standard teaching, is that for an infant operated in the first months of life the eye is usually left aphakic and corrected with a contact lens (or spectacles for bilateral aphakia), with a secondary IOL considered later in childhood; primary IOL is reserved for older infants and children where the glaucoma calculus is more favourable. The IATS long-term data, and the IoLunder2 cohort, also make clear that younger age at surgery independently predicts glaucoma. [5] [6]
After surgery the management is an amblyopia programme: full-time optical correction of the aphakic or pseudophakic eye, and occlusion (patching) of the better eye — proportionate to the severity (from a couple of hours a day to most of the waking day for a dense unilateral case) — continued through the sensitive period. The family must understand that compliance with patching, far more than the elegance of the surgery, decides the final acuity. [10]
Primary congenital glaucoma: the angle-surgery ladder
Unlike adult glaucoma, PCG is not managed primarily with drops — medical therapy is a temporising or adjunctive bridge, because the defect is structural and only surgery restores outflow. The first-line operation is angle surgery, and the choice between the two classic techniques turns on whether the ophthalmologist can see the angle: [8]
- Goniotomy opens the meshwork from within using a gonio lens and a blade, but it requires a clear cornea to visualise the angle.
- Trabeculotomy ab externo is used when the cornea is too cloudy for goniotomy: the surgeon localises Schlemm canal from outside and tears the meshwork open with a probe. [2]
Both have now been overtaken for many surgeons by 360-degree (circumferential) trabeculotomy using an illuminated microcatheter threaded all the way around Schlemm canal, which opens the meshwork for its full circumference in one pass; a 2026 systematic review and meta-analysis confirmed higher success for the circumferential technique than for traditional, sectoral angle surgery, and it is increasingly the primary operation of choice in centres with the equipment. [8]
Surgical ladder for primary congenital glaucoma (escalation when pressure is uncontrolled)
Angle surgery — goniotomy (clear cornea) or trabeculotomy ab externo (cloudy cornea); 360-degree circumferential trabeculotomy where available
Repeat angle surgery or combined trabeculotomy-trabeculectomy, particularly in severe or presenting-with-cloudy-cornea disease
Trabeculectomy with mitomycin C — used when angle surgery fails, with bleb-related risks and a higher failure rate in children than adults
Glaucoma drainage device (Ahmed, Baerveldt or PAUL implant) — for refractory cases or eyes with unfavourable conjunctiva
Cyclodestructive procedures (transscleral or endoscopic cyclophotocoagulation) — reserved for refractory disease or eyes with limited visual potential
The drugs that buy time (and the one to avoid)
Topical and oral pressure-lowering agents are used as a bridge to surgery and as adjuncts when pressure is not fully controlled. A topical beta-blocker such as timolol 0.25% once or twice daily is the usual first agent, used with caution in asthma and heart block (even topical timolol can cause bronchospasm or bradycardia in an infant). A topical carbonic anhydrase inhibitor such as dorzolamide is additive, and an oral one — acetazolamide 10 to 15 mg/kg/day in divided doses — is a useful short-term adjunct. Prostaglandin analogues (latanoprost) are less effective in childhood glaucoma than in adult open-angle disease but are tried. [2]
Postoperative care and the shared surveillance duty
After either operation the child enters lifelong surveillance. The postoperative guidance from a survey of paediatric ophthalmologists sets the pattern: cataract children are reviewed for visual-axis clarity, refraction and intraocular pressure at every visit, because aphakic glaucoma can declare itself months to years later and is often asymptomatic; glaucoma children are reviewed for pressure control, corneal clarity, disc cupping and refractive change (the axial myopia of buphthalmos must be corrected to prevent amblyopia). Both groups need their amblyopia therapy and refraction updated as they grow. [10]
Specific Subtypes & Scenarios
Aphakic glaucoma is the subtype that binds the two halves of the topic, and the one a general paediatrician must understand because they will share the child's care. It develops in a substantial minority of children operated for infantile cataract — the rate rises with the length of follow-up and clusters in those operated very young, with microcornea, or with a primary IOL. The mechanism is a mix of angle inflammation, retained lens material and the anatomical shift of surgery. Because it is silent, the only safeguard is scheduled pressure checks and disc review indefinitely. [4]
Glaucoma in Sturge-Weber syndrome is congenital or develops in infancy in the ipsilateral eye to the facial port-wine stain (and is often accompanied by a diffuse choroidal haemangioma, which raises the risk of effusion after surgery). Aniridia (PAX6) brings foveal hypoplasia, nystagmus and glaucoma in about half to three-quarters over time as the angle closes; sporadic aniridia demands a renal ultrasound to screen for Wilms tumour, because a contiguous deletion can include WT1 (the WAGR constellation of Wilms tumour, aniridia, genitourinary anomalies and range of developmental delay). Peters anomaly presents with a central corneal opacity and iridocorneal adhesion, often with a cataract, and is surgically demanding. Neurofibromatosis type 1 is better known for optic-pathway glioma and Lisch nodules but carries a smaller glaucoma risk. [9]
A traumatic cataract in the older child follows its own clock: the lens may swell and rupture after a blunt or penetrating injury, and a rosette opacity appears. The cataract is removed once the eye is quiet and any comorbid retinal or zonular injury is defined, and the operated eye is then patched aggressively — traumatic cataract in a previously sighted older child often does better than congenital cataract precisely because the visual system was mature at the moment of injury. [1]
Complications & Pitfalls
The complications of infantile cataract surgery are the reason it is never a "quick fix": posterior capsule opacification (now largely prevented by primary posterior capsulotomy and anterior vitrectomy in infants), visual-axis opacification, amblyopia if patching fails, strabismus, and — above all — glaucoma, which is the leading cause of late visual loss after a successful cataract operation. The classic errors at the front door are the dangerous ones: missing a retinoblastoma hiding behind an apparent "cataract," attributing a tearing infant to a blocked tear duct instead of PCG, and delaying surgery past the amblyopia window because the family "wanted to wait." [12]
The complications of childhood glaucoma surgery follow from operating on a small, inflamed, elastic eye: hypotony and its sequelae (choroidal effusion, suprachoroidal haemorrhage, phthisis), endophthalmitis, tube exposure or migration after a drainage device, bleb-related infection and leak after mitomycin trabeculectomy, and the anaesthetic risk of repeated examinations under anaesthesia in an infant. The pitfall on the medical side is reaching for brimonidine, and the pitfall on the surgical side is treating a refractory infant angle as if it were adult glaucoma — the drugs and the incisional options are genuinely different. [8]
Prognosis & Disposition
The prognosis of congenital cataract is decided by four variables, in roughly this order: laterality (bilateral generally better than unilateral, because the eyes compete on equal terms and there is no suppression), density and axial position of the opacity, timing of surgery relative to the critical period, and — most modifiable and most decisive — compliance with patching and optical correction. A dense unilateral cataract operated late and patched poorly leaves a near-blind, strabismic eye; the same cataract operated within weeks and patched faithfully can reach useful acuity. The Infant Aphakia Treatment Study and its successors show that even in the best hands, unilateral infantile cataract usually achieves moderate rather than normal acuity, which sets honest expectations for the family. [7]
The prognosis of primary congenital glaucoma after successful angle surgery is broadly good for pressure control — modern circumferential trabeculotomy achieves control in the great majority — but the visual outcome is limited by the corneal scarring, astigmatism and amblyopia the disease caused before surgery, and by the myopia of the enlarged eye. Children who present early, with clear corneas and intact discs, do best; those who present late, with dense corneal oedema and cupped discs, are left with visually significant eyes. [8]
Every child who has had either operation is followed indefinitely by paediatric ophthalmology. The general paediatric role in disposition is to hold the long view: keep the surveillance appointments, support patching and glasses adherence, watch development and education for the impact of reduced vision, and coordinate the multidisciplinary needs of syndromic children. [10]
Special Populations
In consanguineous families, primary congenital glaucoma may recur through autosomal-recessive CYP1B1 variants, and a second affected child is a real possibility; genetic counselling and targeted CYP1B1 testing inform recurrence risk and prenatal or preimplantation options. The same applies to the autosomal-dominant crystallin cataracts, where an affected parent may be detected only on slit-lamp examination. [9]
The syndromic cataract child needs more than an eye operation. Galactosaemia demands a galactose-free diet and metabolic follow-up; the cataract itself may even regress in early galactosaemia if the diet is started promptly. Congenital rubella combines cataract with sensorineural deafness and cardiac disease and needs audiology, cardiology and developmental input. Lowe syndrome (oculocerebral dystrophy) adds renal tubular dysfunction, intellectual disability and seizures. Down syndrome and other chromosomal diagnoses bring their own surveillance schedules. The paediatrician is the coordinator of this wider care, not just the referrer. [1]
In rural and remote settings, and for migrant and refugee families, the abnormal red reflex or the tearing, light-averse infant may present late, when buphthalmos is established or the cataract dense. The safety-net is a structured red-reflex check at every newborn and early-infancy contact, low-threshold teleophthalmology with image review by a paediatric ophthalmologist, and a clear, fast referral pathway so that distance does not become the reason a child sees light instead of faces. [11]
Evidence, Guidelines & Regional Differences
The modern practice of both diseases rests on a small set of landmark studies, and a fellowship candidate should know what each changed. The Infant Aphakia Treatment Study (IATS) randomised infants with unilateral congenital cataract to contact-lens aphakia versus primary IOL and showed equal acuity but more complications with an IOL, settling the aphakia-first approach for infants. Its long-term follow-up, with IoLunder2 (the British cohort of cataract surgery in the first two years), established the incidence and risk factors of glaucoma following infantile surgery, and the individual-patient-data meta-analysis by Mataftsi and colleagues quantified the pooled risk across studies. On the glaucoma side, the recent meta-analysis of circumferential versus traditional trabeculotomy is the evidence behind the move to 360-degree angle surgery. [5] [6] [4] [8]
In Australia and New Zealand, red-reflex testing is embedded in the personal health record checks performed at the newborn examination and at each scheduled well-child contact, with same-day or rapid paediatric ophthalmology referral for an abnormal reflex and a clear state-based retrieval pathway for children in remote areas. Paediatric ophthalmology is centralised in the major children's hospitals, so the general paediatrician's job is a confident, early referral rather than local management. [11]
Two genuine controversies remain. The first is the place of primary IOL in very young infants — the IATS data have tilted practice toward aphakia-and-contact-lens, but surgeon preference and family circumstances still drive variation. The second is the choice of incisional operation for refractory PCG — trabeculectomy with mitomycin C versus a drainage device versus repeat angle surgery — with growing use of tubes in younger children as device outcomes improve. Neither is settled, and both are fair game in a long-case discussion. [10]
Exam Pearls
SEE
A few facts candidates invert under pressure. The critical period for unilateral deprivation is the first 6 to 8 weeks (not months), whereas the broader sensitive period runs to about 7 to 9 years — the two are not interchangeable. Buphthalmos occurs only in infancy, because the sclera stiffens with age; an older child with raised pressure does not get a big eye, they get a cupped disc and field loss instead. The red reflex is abnormal when it is dark, white, or asymmetric, and an asymmetric reflex can be the only sign of anisometropia or a small cataract. And remember the units that catch candidates: intraocular pressure in mmHg, corneal diameter in mm — and the normal infant numbers are lower and smaller than people guess. [11] [12]
References
- [1]Haargaard B; Wohlfahrt J; Fledelius HC; Rosenberg T; Melbye M A nationwide Danish study of 1027 cases of congenital/infantile cataracts: etiological and clinical classifications. Ophthalmology, 2004.PMID 15582089
- [2]Biglan AW Glaucoma in children: are we making progress? J AAPOS, 2006.PMID 16527674
- [3]Rabiah PK Frequency and predictors of glaucoma after pediatric cataract surgery. Am J Ophthalmol, 2004.PMID 14700641
- [4]Mataftsi A; Haidich AB; Kokkali S; et al Postoperative glaucoma following infantile cataract surgery: an individual patient data meta-analysis. JAMA Ophthalmol, 2014.PMID 24921712
- [5]Freedman SF; Lynn MJ; Beck AD; et al Glaucoma-Related Adverse Events in the First 5 Years After Unilateral Cataract Removal in the Infant Aphakia Treatment Study. JAMA Ophthalmol, 2015.PMID 25996491
- [6]Solebo AL; Rahi JS; British Congenital Cataract Interest Group Glaucoma following cataract surgery in the first 2 years of life: frequency, risk factors and outcomes from IoLunder2. Br J Ophthalmol, 2020.PMID 31586948
- [7]Repka MX; Sutherland DR; Hatt SR; et al Effects of Age at Surgery and Laterality of Cataract on Visual Acuity 5 Years after Surgery in Infants Left Aphakic. Ophthalmology, 2025.PMID 40582417
- [8]Abbas J; Haider F; Arooj H; et al Comparison of 360-Degree Trabeculotomy Versus Traditional Angle Surgery in Primary Congenital Glaucoma: A Systematic Review and Meta-Analysis. J Glaucoma, 2026.PMID 41875194
- [9]Thau A; Lloyd M; Freedman S; et al New classification system for pediatric glaucoma: implications for clinical care and a research registry. Curr Opin Ophthalmol, 2018.PMID 30096087
- [10]Ngo AM; Kraus CL Postoperative guidelines following pediatric cataract and glaucoma surgeries: a survey of preferred surgeon instructions. J AAPOS, 2025.PMID 39863265
- [11]Toli A; Perente A; Labiris G Evaluation of the red reflex: An overview for the pediatrician. World J Methodol, 2021.PMID 34631483
- [12]Anderson J Don't Miss This! Red Flags in the Pediatric Eye Examination: Abnormal Red Reflex. J Binocul Vis Ocul Motil, 2019.PMID 31329054