Paeds · ophthalmology
Conjunctivitis and red eye
Also known as Pink eye · Acute conjunctivitis · Bacterial conjunctivitis · Viral conjunctivitis · Adenoviral conjunctivitis · Allergic conjunctivitis · Ophthalmia neonatorum · Neonatal conjunctivitis · Red eye
Fellowship topic on conjunctivitis and the red eye in children: the bacterial, viral and allergic forms of conjunctivitis and ophthalmia neonatorum in the newborn; the adenoviral and IgE pathophysiology alongside the pyogenic bacterial response; the differential diagnosis of the red eye and the red-flag features that point away from simple conjunctivitis toward keratitis, iritis and trauma; a clinical diagnosis built on discharge type, laterality and the presence of pain and photophobia; stepwise management from supportive care and topical chloramphenicol to antihistamine-mast-cell-stabiliser drops and the neonatal chlamydia and gonococcal pathways; and ANZ, UK, US and Canadian guidance on school exclusion, neonatal prophylaxis and the moderate antibiotic benefit.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-year-old brought in with both eyes red and gritty for two days, the lashes stuck together in the morning with yellow crust, and a runny nose. The child is afebrile, playing between wiping the eyes, and the vision is normal when you coax a look at a toy. This is the everyday face of conjunctivitis in childhood — common, contagious in its infective forms, almost always benign, and the single commonest reason a child presents with a red eye. The skill is not in treating the conjunctivitis; it is in not missing the cause of a red eye that threatens sight. [1] [5]
Conjunctivitis is inflammation of the conjunctiva — the thin, transparent membrane lining the anterior sclera and the inner eyelids — caused most often by infection or allergy, and less often by irritants or trauma. It produces redness, discharge and discomfort, and it sits at the benign end of the red-eye spectrum. The dangerous end holds keratitis, iritis, acute angle-closure glaucoma, corneal abrasion and the retained foreign body, each of which asks a different question and needs a different response. The clinician's first task is therefore triage, not treatment: decide whether this is conjunctivitis at all, and only then decide which form it is. [5] [1]
The task has three layers. The first is recognition of the red-flag features — pain, photophobia, reduced vision, a foreign-body sensation, contact-lens use, trauma or a unilateral painful eye — that move the child out of the conjunctivitis basket and into urgent ophthalmology. The second is cause-matched management of the common, benign forms: supportive care and hygiene for viral disease, a short topical antibiotic course for severe or persistent bacterial disease, and antihistamine with mast-cell stabiliser for allergic disease. The third layer is the newborn, where the same red eye is ophthalmia neonatorum and the response is culture, systemic therapy and maternal screening rather than a topical cream. [1] [9]
Classification
Sort conjunctivitis by cause, because cause decides treatment: supportive care for virus, topical antibiotic for severe bacteria, antihistamine-mast-cell-stabiliser for allergy, and systemic antimicrobials for the neonatal causes. The common infective and allergic forms sit beside the neonatal-specific causes, which deserve their own place in the scheme. [1] [2]
Bacterial conjunctivitis is purulent or mucopurulent, often bilateral, with crusting of the lashes that is worst in the morning. The common organisms are Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis; in older children and adolescents S. aureus predominates, while in younger children H. influenzae (notably nontypeable strains) and S. pneumoniae are prominent. It is usually self-limiting and rarely sight-threatening in the immunocompetent child. [1] [2]
Viral conjunctivitis is watery and follicular, with a tender preauricular lymph node and often an accompanying upper-respiratory infection. Adenovirus causes most cases, and its syndromes include pharyngoconjunctival fever (types 3, 4 and 7, with fever and pharyngitis) and epidemic keratoconjunctivitis (types 8, 19 and 37, with corneal subepithelial infiltrates). Enterovirus and coxsackievirus cause the haemorrhagic form seen in acute haemorrhagic conjunctivitis. Herpes simplex virus is the dangerous exception — a dendritic ulcer on fluorescein staining that must never receive topical steroid. [6] [7]
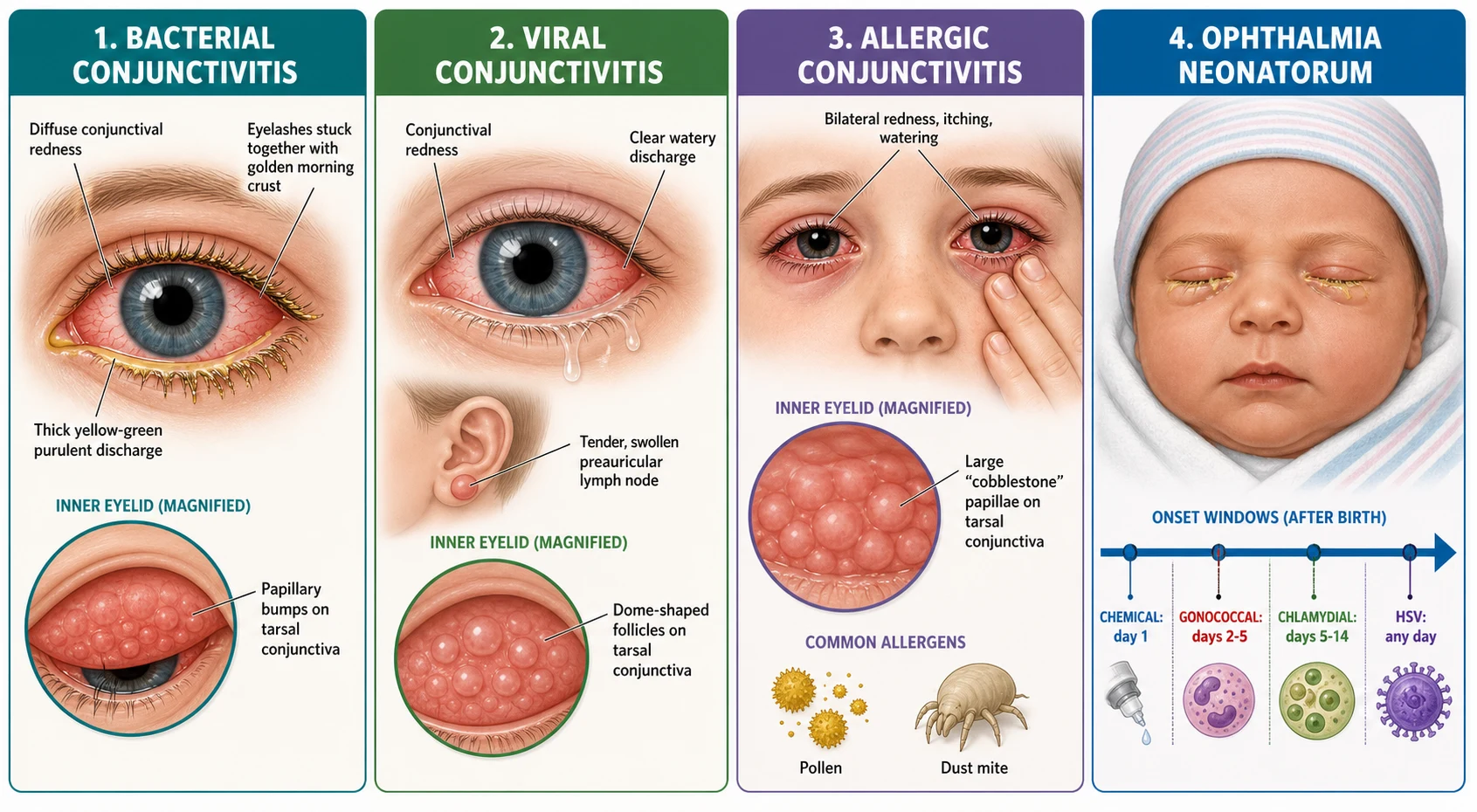
Allergic conjunctivitis is IgE-mediated, bilateral, and dominated by itching. Seasonal allergic conjunctivitis follows pollen exposure; perennial allergic conjunctivitis follows house-dust mite and animal dander; and the chronic, sight-threatening forms — vernal keratoconjunctivitis and atopic keratoconjunctivitis — produce cobblestone giant papillae and can scar. Allergic conjunctivitis travels with the atopic march, alongside eczema, asthma and allergic rhinitis. [8]
Ophthalmia neonatorum is conjunctivitis arising in the first 28 days of life, and it is classified by cause because each cause has its own onset window and systemic treatment. Chemical conjunctivitis follows prophylactic drops in the first 24 hours and settles by day five. Gonococcal (Neisseria gonorrhoeae) appears at day two to five with hyperacute, profuse purulent discharge and lid oedema and can perforate the cornea. Chlamydial (Chlamydia trachomatis) appears at day five to fourteen, is the commonest cause overall, and can progress to chlamydial pneumonia. Herpes simplex is rare but severe, with dendritic keratitis and systemic disease. [9] [10]
Epidemiology & Risk Factors
Conjunctivitis is the commonest eye complaint of childhood and a leading reason for primary-care and emergency presentations. The burden falls unevenly across the forms. Bacterial conjunctivitis is more common in children than adults and peaks in the preschool and early school years; viral conjunctivitis surges in outbreaks that sweep through schools and swimming pools; and allergic conjunctivitis affects up to a third of children with other atopic disease. [2] [8]
The risk factors follow the cause. Bacterial conjunctivitis spreads by direct contact and fomites, amplified by childcare attendance, crowding, poor hand hygiene and the natural tendency of children to rub their eyes. Viral adenoviral conjunctivitis is exceptionally contagious, transmitting on hands, towels, eye cosmetics and contaminated instruments, and it thrives in the close contact of classrooms and households. A recent upper-respiratory infection is the classic precursor of adenoviral pharyngoconjunctival fever. [6] [7]
Allergic conjunctivitis is driven by atopy. A personal or family history of eczema, asthma or allergic rhinitis, sensitisation to pollen, house-dust mite or animal dander, and the seasonal pattern of spring and summer exposure shape who develops it. The chronic forms — vernal keratoconjunctivitis, which predominates in young boys in hot, dry climates, and atopic keratoconjunctivitis — carry the additional risk of corneal scarring. [8]
In Australia and Aotearoa New Zealand, trachoma caused by Chlamydia trachomatis serovars A to C remains present in some remote Aboriginal and Torres Strait Islander communities, where crowding, limited water access and recurrent reinfection sustain transmission; the SAFE strategy (Surgery, Antibiotics, Facial cleanliness, Environmental improvement) frames the public-health response. Conjunctivitis in these settings is as much an environmental-health problem as a clinical one, and facial cleanliness and access to washing water are the durable interventions. [2]
Pathophysiology
Why does a red eye produce a yellow crust in one child, a torrent of clear water in another, and an itch that will not stop in a third? The answer lies in the mechanism each cause sets loose on the conjunctiva. The conjunctiva is a vascular mucous membrane, and anything that dilates its vessels, increases its permeability or recruits inflammatory cells produces the redness and discharge that define conjunctivitis. [1] [5]
In bacterial conjunctivitis, organisms colonise the conjunctival surface and multiply, provoking a neutrophil-rich acute inflammatory response. The vessels dilate, the permeability rises, and the exuded fluid and inflammatory cells produce the mucopurulent discharge that dries into the morning crust. The reaction is papillary — small, vascular elevations on the tarsal conjunctiva — and the discharge is the hallmark that separates it from the watery viral form. [1] [2]
In viral conjunctivitis the mechanism is different. Adenovirus replicates in the conjunctival epithelium and provokes a lymphocyte-rich response that produces follicles — dome-shaped collections of lymphoid tissue on the tarsal conjunctiva — together with the watery discharge and the tender preauricular lymph node that are the bedside signature of the viral form. In epidemic keratoconjunctivitis the virus reaches the cornea and produces subepithelial infiltrates that can blur vision for weeks after the acute redness settles. The danger exception is herpes simplex virus, which produces a branching dendritic ulcer on the corneal epithelium that fluorescein staining reveals. [6] [7]
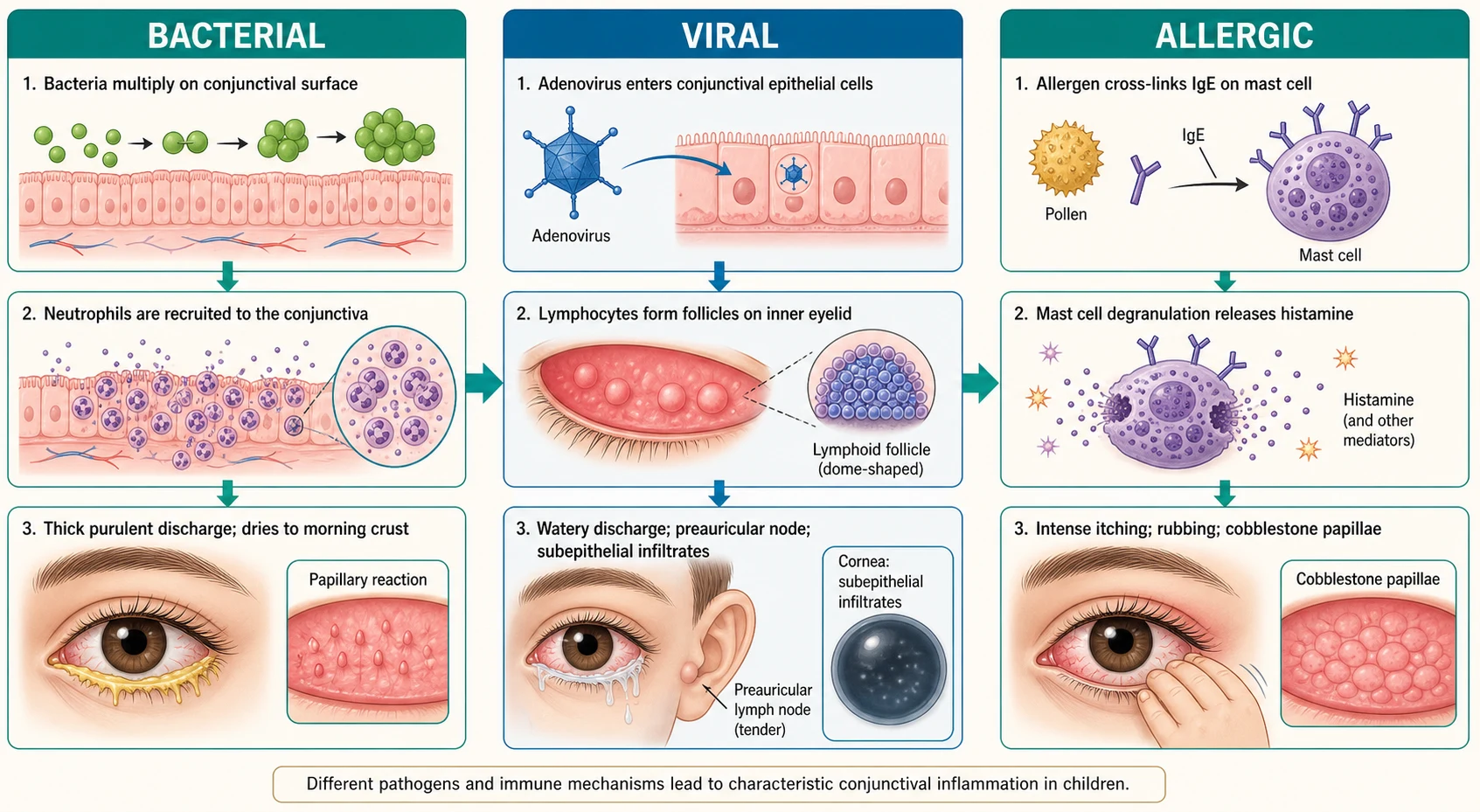
In allergic conjunctivitis the mechanism is immunological. Allergen cross-links IgE bound to mast cells in the conjunctival mucosa, triggering degranulation and the release of histamine, leukotrienes and prostaglandins. These mediators dilate vessels, increase permeability and stimulate the itch nerve fibres — and itching, rather than pain or discharge, is the symptom the child complains of. Repeated exposure in the chronic forms drives the formation of the giant, cobblestone papillae of vernal and atopic keratoconjunctivitis. The mast-cell stabiliser-antihistamine drop works at exactly this point, blocking both the trigger and the mediator. [8]
The neonatal mechanisms follow the organism. Neisseria gonorrhoeae invades the conjunctival epithelium and produces an intense, profuse, hyperacute purulent reaction that can erode and perforate the cornea within hours if untreated. Chlamydia trachomatis is an intracellular organism that infects the conjunctival epithelium and, in a substantial proportion of infants, ascends or seeds the respiratory tract to cause a distinctive afebrile, staccato chlamydial pneumonia weeks later — which is why systemic, not topical, treatment is required. Herpes simplex virus can produce keratitis and disseminated disease, and the chemical cause is simply the irritant effect of prophylactic silver nitrate or antibiotic drops, which is self-limiting. [9] [11]
Clinical Presentation
The common infective and allergic forms present with redness, discharge and discomfort, and the distinguishing features are the type of discharge, the laterality, the presence of itching, and the associated symptoms. The clinician's job is to read these features into a cause and, at the same time, to screen for the red-flag features that point elsewhere. [1] [5]
Bacterial conjunctivitis presents with redness and a purulent or mucopurulent discharge that accumulates overnight and glues the lashes together, so the parents describe the eye being stuck shut in the morning. It is often bilateral but can begin in one eye and spread. There is redness of the tarsal and bulbar conjunctiva, a papillary reaction on the lower tarsal conjunctiva, and usually little pain and no photophobia. The child is typically afebrile and well, and the vision is normal. [2] [1]
Viral conjunctivitis presents with a red, gritty, watery eye. The discharge is clear and scant rather than purulent, the tarsal conjunctiva shows follicles rather than papillae, and a palpable tender preauricular lymph node is the helpful sign that points to a viral cause. A recent or concurrent upper-respiratory infection with fever and pharyngitis suggests pharyngoconjunctival fever. Epidemic keratoconjunctivitis is more severe, with marked lid oedema, pseudomembrane formation and, later, visual blur from corneal infiltrates. The infection is highly contagious and the history often reveals a sick classmate or a sibling. [6] [7]
Allergic conjunctivitis presents with the cardinal symptom of itching, bilateral redness, watering and a stringy mucus discharge. The child rubs the eyes, may have swollen lids and is likely to have eczema, asthma or hayfever. The tarsal conjunctiva shows papillae, and in the chronic forms the giant cobblestone papillae of vernal keratoconjunctivitis are distinctive. The seasonal or exposure pattern — worse in spring, with pets, or after playing in grass — is the clue that separates allergy from infection. [8]
Differential Diagnosis
The differential of the red eye is the heart of this topic, because the dangerous causes masquerade as conjunctivitis and lose sight if treated as conjunctivitis. The structured approach separates the conjunctival causes from the corneal, intraocular and traumatic causes, and the red-flag features decide the direction. [5] [1]
Keratitis — inflammation or infection of the cornea — produces a red, painful eye with photophobia, watering and reduced vision, often with a foreign-body sensation. Bacterial keratitis is the feared complication of contact-lens wear, producing a corneal ulcer visible on fluorescein staining; herpes simplex keratitis produces the dendritic ulcer; and the photophobia and ciliary flush distinguish keratitis from conjunctivitis at the bedside. [5] [7]
Iritis (anterior uveitis) produces a painful red eye with photophobia, ciliary flush (a ring of redness concentrated around the cornea), a small or irregular pupil, and cells and flare in the anterior chamber on slit-lamp examination. In children, iritis is associated with juvenile idiopathic arthritis and needs urgent ophthalmology assessment, because delayed treatment blinds. Acute angle-closure glaucoma is rare in children but causes severe pain, a hazy cornea, a fixed mid-dilated pupil and nausea; it is an emergency. [5]
[5] [1]Corneal abrasion follows trauma — a fingernail, a toy, a foreign body — and presents with sudden pain, watering, redness and a foreign-body sensation, with the defect shown by fluorescein staining under a blue light. A retained foreign body persists as long as it remains, with the same pain and watering. Subconjunctival haemorrhage — a bright-red patch under the conjunctiva — usually follows trauma, coughing or vomiting and is benign unless bilateral or recurrent, when trauma or a bleeding disorder must be considered. [5]
For the newborn, the differential is the ophthalmia neonatorum causes by their onset window: chemical in the first day, gonococcal from day two to five, chlamydial from day five to fourteen, and herpes simplex throughout — each demanding culture-confirmed, cause-specific systemic treatment rather than a broad guess. A duct obstruction from congenital nasolacrimal duct obstruction mimics conjunctivitis with chronic watering without redness, and is distinguished by the clear, non-purulent nature of the tears once the infection settles. [9] [10]
Clinical & Bedside Assessment
The assessment begins with a focused history and a careful look at the eye, and the single most important step is to decide whether this is conjunctivitis or a dangerous red eye. Ask about the onset, the type of discharge, the laterality, itching, pain, photophobia and any change in vision. Ask about a recent cold, a sick contact, childcare attendance, contact-lens use, trauma, allergies and the atopic history, and — for the newborn — the day of life, maternal screening and the type of prophylaxis given at birth. [5] [2]
Examine both eyes, including the vision. In the cooperative child, check that vision is normal — can the child count fingers, read, or fix and follow a toy appropriate to age? Inspect the lids, the lashes and the discharge, evert the upper lid if a foreign body or papillary reaction is suspected, and look at the pattern of redness. Diffuse tarsal and bulbar redness fits conjunctivitis; a ring of redness concentrated around the cornea — ciliary flush — fits keratitis or iritis. Feel for a preauricular lymph node, which points to a viral cause. [1] [5]
The decisive examination is fluorescein staining with a blue light. A corneal defect — an abrasion, a dendritic ulcer, an ulcer — takes up the dye and glows green, separating the traumatic and infectious corneal causes from simple conjunctivitis. Check the pupil: a small, irregular or poorly reactive pupil, or a difference between the two eyes, points to iritis. A hazy cornea with a fixed mid-dilated pupil points to acute glaucoma. Any of these findings is a red flag for urgent referral. [5]
In the newborn, the assessment is structured by the ophthalmia neonatorum framework. Note the day of life and the onset, the character of the discharge (thin and scant, or profuse and purulent), the lid oedema, and any systemic signs. Take conjunctival swabs for Gram stain, culture and chlamydia testing, and send the mother for sexually-transmitted-infection screening if any neonatal conjunctivitis is confirmed, because the mother's infection is the source and her treatment is part of the management. [9] [10]
Investigations
Conjunctivitis is a clinical diagnosis, and routine investigations are not needed for the common, uncomplicated forms in the older child. The history and examination — the discharge type, the laterality, itching, the preauricular node and the absence of red flags — are enough to choose supportive care, a topical antibiotic or an antihistamine-mast-cell stabiliser. [1] [2]
Reserve conjunctival swabs for microbiology and culture for the situations where the result changes management: neonatal conjunctivitis, where Gram stain and culture for Neisseria gonorrhoeae and chlamydia testing are part of the work-up; hyperacute or severe purulent conjunctivitis in any age; conjunctivitis not responding to first-line treatment; the immunocompromised child; and the contact-lens wearer with a red eye, where corneal scraping for culture is an ophthalmology decision. Viral PCR is reserved for suspected herpes simplex or during outbreaks. [9] [10]
Fluorescein staining is the key bedside investigation for the red eye, and it should be performed whenever pain, photophobia, a foreign-body sensation, contact-lens use or trauma is in the history. It reveals corneal abrasions, dendritic ulcers and bacterial ulcers, and it is the test that separates conjunctivitis from the corneal causes that need referral. Slit-lamp examination by ophthalmology adds cells and flare for iritis and defines the corneal lesion for keratitis. [5]
Supportive tests are guided by the suspected complication or systemic cause. For suspected allergic conjunctivitis that is severe, recurrent or atypical, allergy testing helps define the triggers and guide avoidance. For chlamydial ophthalmia neonatorum, the infant is assessed for the staccato, afebrile pneumonia that may follow. For the iritis associated with juvenile idiopathic arthritis, the ophthalmology referral drives the systemic work-up. In every case, the investigation serves the cause, not the routine. [8] [11]
Management — Resuscitation
Resuscitation belongs to the sight-threatening and the newborn. The red flags that demand urgent assessment and ophthalmology referral are a unilateral painful red eye; photophobia; reduced vision; a foreign-body sensation; contact-lens use; trauma; ciliary flush; a corneal opacity or ulcer; an abnormal pupil; and, in the newborn, profuse hyperacute purulent discharge with lid oedema. None of these is conjunctivitis, and none is treated with a topical conjunctivitis drop. [5] [1]
For suspected bacterial keratitis in a contact-lens wearer, remove the lens, do not patch the eye, stop contact-lens use, and refer the same day to ophthalmology for corneal scraping and intensive topical antibiotic therapy. A delay in treating a corneal ulcer can cost the eye, and the temptation to treat a red, painful, lens-wearing eye as conjunctivitis is the classic and dangerous error. [5] [7]
For gonococcal ophthalmia neonatorum, the concern is corneal perforation within hours, so the response is immediate admission, culture, and systemic therapy. Herpes simplex ophthalmia neonatorum is treated with systemic aciclovir and topical antiviral under ophthalmology guidance, because it may signal disseminated or central-nervous-system disease. The principle is that a neonatal red eye is never managed in the community with topical drops alone. [9] [10]
Separate resuscitation from definitive treatment in your mind. The older child with simple bacterial, viral or allergic conjunctivitis is managed in the community with supportive care, hygiene and a cause-matched topical agent. The child with a red-flag red eye and the newborn with ophthalmia neonatorum need the hospital, ophthalmology and systemic therapy — and the skill is in recognising them at the first encounter. [1] [9]
Management — Definitive & Stepwise
Definitive management is a cause-matched pathway built on the clinical diagnosis and free of red flags. Viral conjunctivitis takes supportive care and hygiene; bacterial conjunctivitis takes a short topical antibiotic course for severe or persistent disease; allergic conjunctivitis takes avoidance, cold compresses and a topical antihistamine with mast-cell stabiliser; and ophthalmia neonatorum takes culture-confirmed, cause-specific systemic therapy. The art is matching the treatment to the cause and using antibiotics with stewardship discipline. [1] [2]
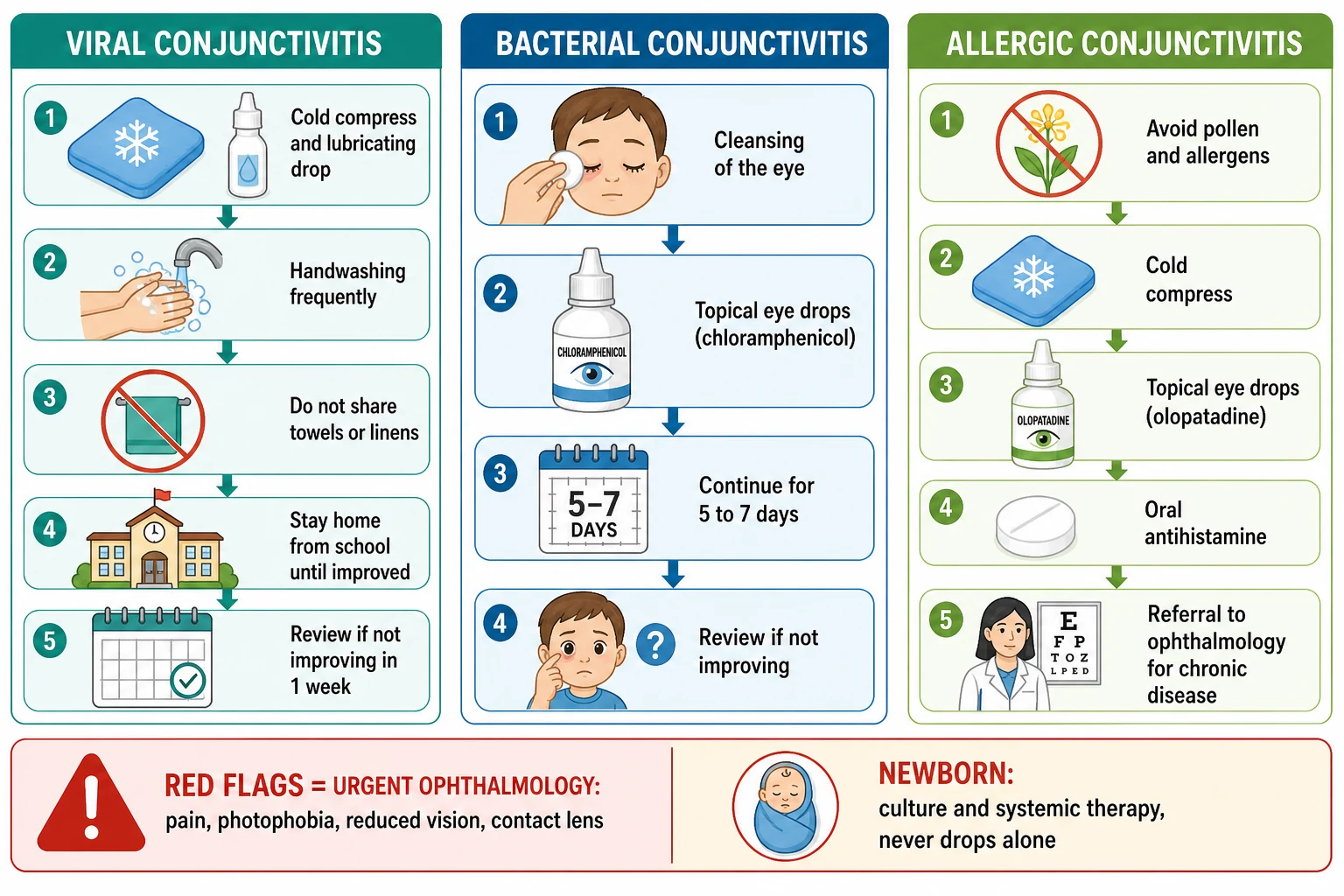
For viral conjunctivitis, supportive care is the treatment. Lubricating drops and cold compresses ease the discomfort, and the emphasis is on hygiene to limit spread: frequent hand washing, not sharing towels or pillows, avoiding eye rubbing, and staying away from school, childcare and swimming pools until the discharge has settled. The condition is self-limiting, resolving over one to two weeks, and topical antibiotics do not help a viral cause. Advise the family to return if pain, photophobia or reduced vision develops, because these are the red flags for keratitis or a secondary complication. [6] [2]
For bacterial conjunctivitis, the Cochrane review is the anchor. It found that topical antibiotics improve the early clinical cure rate — at days two to five, more people are cured with antibiotics than with placebo — but that this early benefit disappears by day six to ten, when most cases have resolved regardless of treatment. The practical consequence is that a short topical antibiotic course is reasonable for severe, persistent or socially-disruptive bacterial conjunctivitis, while many mild cases can be managed with cleansing and observation. [3] [4]
Bacterial conjunctivitis topical ladder (NICE CKS / BNFc — confirm locally)
For allergic conjunctivitis, management is layered. Start with allergen avoidance — reducing exposure to the identified trigger — and cold compresses for symptom relief. A topical antihistamine with mast-cell stabiliser such as olopatadine (one drop to the affected eye once or twice daily) addresses both the trigger and the mediator and is the mainstay. An oral antihistamine such as cetirizine helps the systemic atopic symptoms. The chronic, sight-threatening forms — vernal and atopic keratoconjunctivitis — need ophthalmology referral because they may require topical calcineurin inhibitors or, in selected cases under specialist supervision, topical steroid. [8]
The stepwise conjunctivitis and red-eye pathway
Triage first: screen for red flags — pain, photophobia, reduced vision, foreign-body sensation, contact-lens use, trauma, ciliary flush, corneal opacity, abnormal pupil. Any red flag is urgent ophthalmology, not conjunctivitis.
Read the cause from the discharge, laterality, itching and the preauricular node: watery and follicular is viral; purulent and crusted is bacterial; itchy and bilateral is allergic.
Viral conjunctivitis: supportive care, lubricants, cold compresses, strict hygiene and exclusion from school, childcare and pools until settled; review if not improving at one week.
Bacterial conjunctivitis: cleanse the discharge and give a five to seven day topical chloramphenicol course for severe or persistent disease; many mild cases resolve with cleansing alone.
Allergic conjunctivitis: allergen avoidance, cold compresses, a topical antihistamine with mast-cell stabiliser such as olopatadine, and an oral antihistamine for systemic atopic symptoms.
Ophthalmia neonatorum: culture, and treat the cause systemically — never topical drops alone — with maternal sexually-transmitted-infection screening.
Safety-net every child: return immediately with pain, photophobia, reduced vision, or in the newborn with fever, lethargy or profuse discharge.
Specific Subtypes & Scenarios
A preschool child with sticky, crusted eyes and a cold. This is classic viral conjunctivitis, with watery redness, follicles, a preauricular node and an accompanying upper-respiratory infection. The management is supportive care, lubricants and hygiene, with exclusion from school and swimming until the discharge settles. The family needs a clear safety-net for pain, photophobia or visual change, and reassurance that the natural course is one to two weeks. [6] [2]
A school-age child with itchy, watery eyes in spring. This is seasonal allergic conjunctivitis in an atopic child. Bilateral itching, watering and stringy mucus with a hayfever history make the diagnosis, and the management is allergen avoidance, cold compresses and a topical antihistamine with mast-cell stabiliser such as olopatadine, with an oral antihistamine for the systemic symptoms. Controlling the allergic rhinitis and eczema completes the atopic picture. [8]
An adolescent contact-lens wearer with a painful red eye. This is bacterial keratitis with a corneal ulcer until proven otherwise. Remove the lens, do not patch, stop lens use, and refer the same day for corneal scraping and intensive topical antibiotic therapy under ophthalmology. Treating this as conjunctivitis with a chloramphenicol drop is the error that blinds, and the contact lens is the clue that must never be missed. [5] [7]
A two-day-old with profuse purulent conjunctivitis and lid oedema. This is gonococcal ophthalmia neonatorum, which can perforate the cornea within hours. Admit, take conjunctival swabs for Gram stain and culture, and start systemic therapy — intramuscular or intravenous ceftriaxone (avoiding ceftriaxone in the jaundiced or calcium-infused neonate, when cefotaxime is the alternative) — with saline irrigation of the eye and urgent ophthalmology review. Screen and treat the mother and her partner for sexually-transmitted infection. [9] [10]
A ten-day-old with mucopurulent conjunctivitis and a staccato cough. This is chlamydial ophthalmia neonatorum, the commonest cause, and the cough signals evolving chlamydial pneumonia. The treatment is systemic oral erythromycin 50 mg per kilogram per day in four divided doses for 14 days — topical treatment is inadequate because it does not eradicate nasopharyngeal carriage or prevent pneumonia. Screen and treat the mother. A single course may need repeating, because the recurrence rate after one course is appreciable. [11] [9]
A child with recurrent, unilateral, sticky eyes but no redness. This is congenital nasolacrimal duct obstruction, which mimics chronic conjunctivitis with persistent watering and secondary mucoid discharge in an otherwise white, quiet eye. The management is conservative — lid hygiene and lacrimal sac massage — because most resolve spontaneously in the first year, with probing reserved for those that persist beyond 12 to 18 months. Recognising it prevents repeated, unnecessary antibiotic courses. [10] [2]
Complications & Pitfalls
The most important pitfall is treating a dangerous red eye as conjunctivitis. A contact-lens wearer with a corneal ulcer, a child with herpes simplex keratitis, an adolescent with iritis from juvenile idiopathic arthritis and a newborn with gonococcal ophthalmia neonatorum can each present with redness and discharge that superficially resembles conjunctivitis — and each loses sight if given a chloramphenicol drop and sent home. The defence is the red-flag screen at every encounter: pain, photophobia, reduced vision, a foreign-body sensation, contact-lens use, trauma, ciliary flush, a corneal opacity and an abnormal pupil. [5] [1]
The second pitfall is using topical antibiotics for every red eye. The Cochrane evidence shows topical antibiotics give only a modest early benefit that vanishes by day six to ten, so routine prescribing for viral and mild bacterial conjunctivitis drives resistance and cost without meaningful gain. The disciplined approach reserves topical antibiotics for severe, persistent or disruptive bacterial disease and explains the self-limiting course to the family. [3] [4]
The third pitfall is treating neonatal chlamydial conjunctivitis with topical drops alone. Topical erythromycin clears the eye but does not eradicate the nasopharyngeal carriage that causes the pneumonia, so the infant needs systemic oral erythromycin, and the family needs screening. The same principle applies to maternal gonococcal infection: the mother and her partner must be screened and treated, or the newborn is re-exposed. [11] [9]
A fourth pitfall is reaching for topical steroid. Steroids ease the redness of almost any red eye, but in herpes simplex keratitis they promote corneal melting and blindness, and in bacterial keratitis they worsen infection. Steroids in the red eye are an ophthalmology decision, made after fluorescein examination and slit-lamp assessment, never a primary-care reflex. [7] [5]
The fifth pitfall is the wrong school-advice frame. Viral conjunctivitis is highly contagious and the child should stay away from school, childcare and swimming pools until the discharge settles; but simple infective conjunctivitis in an older, well child generally does not require prolonged exclusion, and the unnecessary exclusion of well children disrupts families. Match the advice to the cause and the child's condition. [2] [6]
Prognosis & Disposition
Most bacterial and viral conjunctivitis resolves completely within one to two weeks without sequelae, and allergic conjunctivitis settles with allergen avoidance and topical treatment, flaring with re-exposure. The prognosis of conjunctivitis itself is excellent; the morbidity lies in contagion, in disruption to school and family, and in the chronic forms of allergic disease. The disposition follows the cause and the presence or absence of red flags. [1] [8]
Manage in the community the well, older child with simple conjunctivitis and no red flags — supportive care for viral disease, a short topical antibiotic course for severe bacterial disease, and antihistamine-mast-cell stabiliser for allergy — with a clear safety-net for return. Refer urgently to ophthalmology the child with any red-flag feature, and admit the newborn with ophthalmia neonatorum for culture and systemic therapy. The threshold for assessing and admitting the newborn, the contact-lens wearer and the immunocompromised child is deliberately low. [5] [9]
At discharge or review, confirm healing, complete any antibiotic or antihistamine course, give clear hygiene and exclusion advice, and provide the safety-net for pain, photophobia, reduced vision and — in the newborn — fever, lethargy or profuse discharge. Reinforce the underlying skin and allergy care, because controlling eczema and allergic rhinitis is what prevents the next flare of allergic conjunctivitis, and good hygiene is what limits the household spread of the viral forms. [2] [8]
Recurrence is common for the infective forms, which spread readily through households and classrooms, and for the allergic forms, which flare with each pollen season. Natural infection does not confer durable immunity to the respiratory adenoviruses or bacteria, and the atopic tendency is lifelong. The durable interventions are hygiene, allergen avoidance and — for ophthalmia neonatorum — maternal screening and neonatal prophylaxis, not repeated courses of topical antibiotic. [6] [9]
Special Populations
Newborns and young infants carry the highest risk of the sight-threatening and systemic forms. Ophthalmia neonatorum is a distinct entity with cause-specific systemic treatment, and a neonatal red eye is a culture-confirmed, systemically-treated, maternally-screened problem until proven otherwise — never a topical-drop problem. The onset window (chemical, gonococcal, chlamydial, herpes simplex) and the day of life organise the response. [9] [10]
Children with allergic disease — eczema, asthma and allergic rhinitis — are the allergic conjunctivitis population, and the chronic forms (vernal and atopic keratoconjunctivitis) can scar the cornea. Treat the conjunctivitis and the systemic atopy together, and refer the chronic forms early to ophthalmology. Controlling the eczema and rhinitis is what prevents the next flare, and the mast-cell stabiliser-antihistamine drop is the mainstay of the acute episode. [8]
Contact-lens wearers are the population at risk of bacterial keratitis, and a painful red eye in a lens wearer is a corneal ulcer until proven otherwise. Remove the lens, stop lens use, and refer the same day for scraping and intensive topical therapy. Hygiene in lens care, overnight removal and prompt attention to any discomfort are the preventive measures that the family and adolescent must understand. [5] [7]
Aboriginal and Torres Strait Islander, Maori and Pasifika children, and refugee, asylum-seeking and migrant families carry disproportionate burden in some settings. Trachoma persists in remote Australian communities where crowding and limited water access sustain it, and the SAFE strategy — Surgery, Antibiotics, Facial cleanliness, Environmental improvement — frames the integrated response. Ensure culturally safe care, use trained interpreters, treat the household and the environment alongside the child, and address the determinants — crowding, water and housing — that sustain endemic eye disease. [2]
Immunocompromised children are at risk of severe, persistent and atypical infection, and they warrant a lower threshold for culture, systemic therapy and ophthalmology referral. The organism may be unusual, the disease more invasive, and the response slower, so early specialist involvement is appropriate when these children present with a red eye that does not follow the benign course. [1] [10]
Evidence, Guidelines & Regional Differences
The treatment evidence for bacterial conjunctivitis is anchored by the Cochrane review of antibiotics versus placebo, updated in 2023 and summarised in 2024. It found that topical antibiotics improve the early clinical cure rate at days two to five compared with placebo, but that this benefit is no longer significant by day six to ten, when most cases have resolved. The implication is that a short topical antibiotic course is reasonable for severe, persistent or disruptive bacterial conjunctivitis, while mild cases can be observed — a stewardship-conscious stance that resists the reflex to prescribe for every red eye. [3] [4]
Cochrane review: antibiotics versus placebo for acute bacterial conjunctivitis
Population: Children and adults with acute bacterial conjunctivitis, randomised to topical antibiotics versus placebo across the included trials.
Key finding
Topical antibiotics improved the early clinical cure rate at days two to five relative to placebo, but the difference was no longer significant by day six to ten, when most cases had resolved regardless of treatment.
Practice change
Reserve topical antibiotics for severe, persistent or disruptive bacterial conjunctivitis; many mild cases resolve with cleansing and observation, and routine prescribing adds resistance and cost without durable benefit.
The diagnosis-and-treatment evidence is consolidated in the JAMA systematic review of conjunctivitis, which frames the cause-based approach and the red-eye differential, and the paediatric-specific review of conjunctivitis in children, which sets the clinical forms, the management and the exclusion advice for the paediatric population. The viral conjunctivitis literature, including the adenoviral keratoconjunctivitis review, frames the supportive-care stance and the contagiousness that drives exclusion. [1] [2]
The neonatal evidence and guidance converge on prevention and cause-specific systemic therapy. The Canadian Paediatric Society statement on preventing ophthalmia neonatorum, the StatPearls overview and the neonatal chlamydial infection review set the prophylaxis, the onset windows and the systemic treatment — erythromycin for chlamydia, ceftriaxone (or cefotaxime) for gonorrhoea, aciclovir for herpes simplex — alongside maternal screening and treatment. Neonatal prophylaxis at birth reduces gonococcal ophthalmia neonatorum, and the USPSTF continues to recommend it. [9] [10]
In Australia and New Zealand, the approach aligns with the Therapeutic Guidelines and the National Health and Medical Research Council guidance on neonatal prophylaxis, with topical antibiotic prophylaxis at birth and maternal sexually-transmitted-infection screening as standard. The remote-community trachoma response follows the SAFE strategy, integrating antibiotic treatment, facial cleanliness and environmental improvement. In the UK, NICE Clinical Knowledge Summaries set chloramphenicol first-line for severe bacterial conjunctivitis and the conservative, observation-acceptable stance for mild disease. In the US and Canada, the AAP and Canadian Paediatric Society guidance set neonatal prophylaxis and the school-exclusion and maternal-screening frame. [9] [2]
The controversies are active. The first is the persistent over-prescribing of topical antibiotics for a self-limiting condition, against the Cochrane evidence. The second is the choice of neonatal prophylactic agent — erythromycin and tetracycline remain effective, silver nitrate is obsolete, and povidone-iodine is a low-cost alternative studied in resource-limited settings. The third is the school-exclusion policy, where guidance has shifted toward not excluding well older children while maintaining exclusion for the highly contagious viral forms. The defence against each is the same: a red-flag screen, a cause-matched treatment, stewardship discipline, and a public-health lens for the newborn and the remote community. [3] [9]
Exam Pearls
- The three common forms are bacterial (purulent or mucopurulent discharge, crusted lashes, bilateral), viral (watery, follicular, preauricular node, adenovirus) and allergic (itching is cardinal, bilateral, cobblestone papillae, IgE-mediated). [1]
- The red-eye red flags that point away from conjunctivitis are pain, photophobia, reduced vision, foreign-body sensation, contact-lens use, trauma, ciliary flush, corneal opacity and an abnormal pupil — each is keratitis, iritis, glaucoma, abrasion or foreign body, and each needs fluorescein and urgent ophthalmology. [5]
- The Cochrane review found topical antibiotics give a modest early benefit that disappears by day 6 to 10; reserve them for severe, persistent or disruptive bacterial conjunctivitis, not every red eye. [3]
- First-line topical for severe bacterial conjunctivitis is chloramphenicol (0.5% drops or 1% ointment for 5 to 7 days); fusidic acid is the alternative. [4]
- Viral conjunctivitis is supportive care, hygiene and exclusion until settled; topical antibiotics do not help. Herpes simplex produces a dendritic ulcer — never give topical steroid. [6] [7]
- Allergic conjunctivitis is allergen avoidance, cold compresses and a topical antihistamine with mast-cell stabiliser such as olopatadine, with an oral antihistamine for systemic symptoms. [8]
- Ophthalmia neonatorum is conjunctivitis in the first 28 days: chemical (day 1, after prophylaxis), gonococcal (day 2 to 5, hyperacute, sight-threatening), chlamydial (day 5 to 14, commonest, may cause pneumonia) and herpes simplex. [9] [10]
- Gonococcal ophthalmia neonatorum is systemic therapy (ceftriaxone, or cefotaxime in the jaundiced neonate), saline irrigation and urgent ophthalmology; it can perforate the cornea within hours. [9]
- Chlamydial ophthalmia neonatorum is oral erythromycin 50 mg per kilogram per day in four divided doses for 14 days — never topical alone — because topical does not prevent the pneumonia. [11]
- A contact-lens wearer with a painful red eye is a corneal ulcer until proven otherwise — remove the lens, do not patch, refer same day. [5]
References
- [1]Azari AA; Barney NP Conjunctivitis: a systematic review of diagnosis and treatment. JAMA, 2013.PMID 24150468
- [2]Mahoney MJ; Bekibele R; Notermann SL; et al Pediatric Conjunctivitis: A Review of Clinical Manifestations, Diagnosis, and Management. Children (Basel), 2023.PMID 37238356
- [3]Chen YY; Liu SH; Nurmatov U; et al Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Database Syst Rev, 2023.PMID 36912752
- [4]Liu SH; Chen YY; Nurmatov U; et al Antibiotics Versus Placebo for Acute Bacterial Conjunctivitis: Findings From a Cochrane Systematic Review. Am J Ophthalmol, 2024.PMID 37482371
- [5]Cronau H; Kankanala RR; Mauger T Diagnosis and management of red eye in primary care. Am Fam Physician, 2010.PMID 20082509
- [6]Muto T; Imaizumi S; Kamoi K Viral Conjunctivitis. Viruses, 2023.PMID 36992385
- [7]Jhanji V; Chan TC; Li EY; Agarwal K; Vajpayee RB Adenoviral keratoconjunctivitis. Surv Ophthalmol, 2015.PMID 26077630
- [8]Vazirani J; Shukla S; Chhawchharia R; et al Allergic conjunctivitis in children: current understanding and future perspectives. Curr Opin Allergy Clin Immunol, 2020.PMID 32739978
- [9]Moore DL; MacDonald NE; Canadian Paediatric Society Preventing ophthalmia neonatorum. Paediatr Child Health, 2015.PMID 25838784
- [10]Castro Ochoa KJ; Gurnani B Ophthalmia Neonatorum. StatPearls, 2026.PMID 31855399
- [11]Zar HJ Neonatal chlamydial infections: prevention and treatment. Paediatr Drugs, 2005.PMID 15871630