Paeds · ophthalmology
Ocular trauma and chemical injury
Also known as Chemical eye injury · Ocular chemical burn · Open globe injury · Globe rupture · Traumatic hyphema · Birmingham Eye Trauma Terminology · Ocular Trauma Score · Dua classification of ocular surface burns
Fellowship topic on paediatric ocular trauma and chemical injury: the two time-critical first-contact emergencies — chemical injury, irrigated first before examination, and suspected open globe, shielded and not pressed; the Birmingham Eye Trauma Terminology (BETT) separating closed globe (contusion, lamellar laceration, superficial foreign body) from open globe (rupture from blunt force, or laceration — penetrating versus perforating — with retained intraocular foreign body); the Ocular Trauma Score and its raw-score components; the alkali-versus-acid pathophysiology of liquefactive versus coagulative necrosis with hydrofluoric acid as the exception; the Dua classification graded by clock hours of limbal ischaemia and the Roper-Hall grades; the immediate irrigation protocol continued until pH 7.0 to 7.2; the recognise-shield-refer pathway for open globe; traumatic hyphaema and the place of aminocaproic acid; retained intraocular foreign body and sympathetic ophthalmia; and ANZ, UK and North American guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a seven-year-old who runs in from the kitchen clutching his eye after a dishwasher tablet burst, and a ten-year-old hit in the eye by a dart. Both are screaming, both eyes are firmly shut, and in both cases the temptation is to prise the lids apart and examine. That instinct is right for one and dangerous for the other — and telling them apart is the whole skill of paediatric ocular trauma. For the chemical splash, the first thing you do is irrigate, because every minute of retained alkali destroys limbal stem cells. For the dart, the first thing you do is shield, because pressing a full-thickness wound extrudes the contents of the eye. Everything else — the classification, the score, the surgery — follows from getting those two first moves right. [5] [8]
Ocular trauma means any mechanical, chemical or physical injury to the eye and its adnexa. In children it is common, it is frequently preventable, and it remains a leading cause of non-congenital unilateral blindness because the developing visual system is unforgiving: a scarred cornea, a deprived retina or a neglected injury all seed amblyopia as well as structural damage. [8] [10] The clinical task is layered. The first layer is first aid — irrigate the chemical injury, shield the open globe. The second layer is recognition — naming the injury in the standardised BETT language so that it is communicated the same way to the ophthalmologist. The third layer is prognosis and definitive care — the Ocular Trauma Score, the chemical-burn grade, and the surgical and follow-up pathway. [1] [3]
Classification
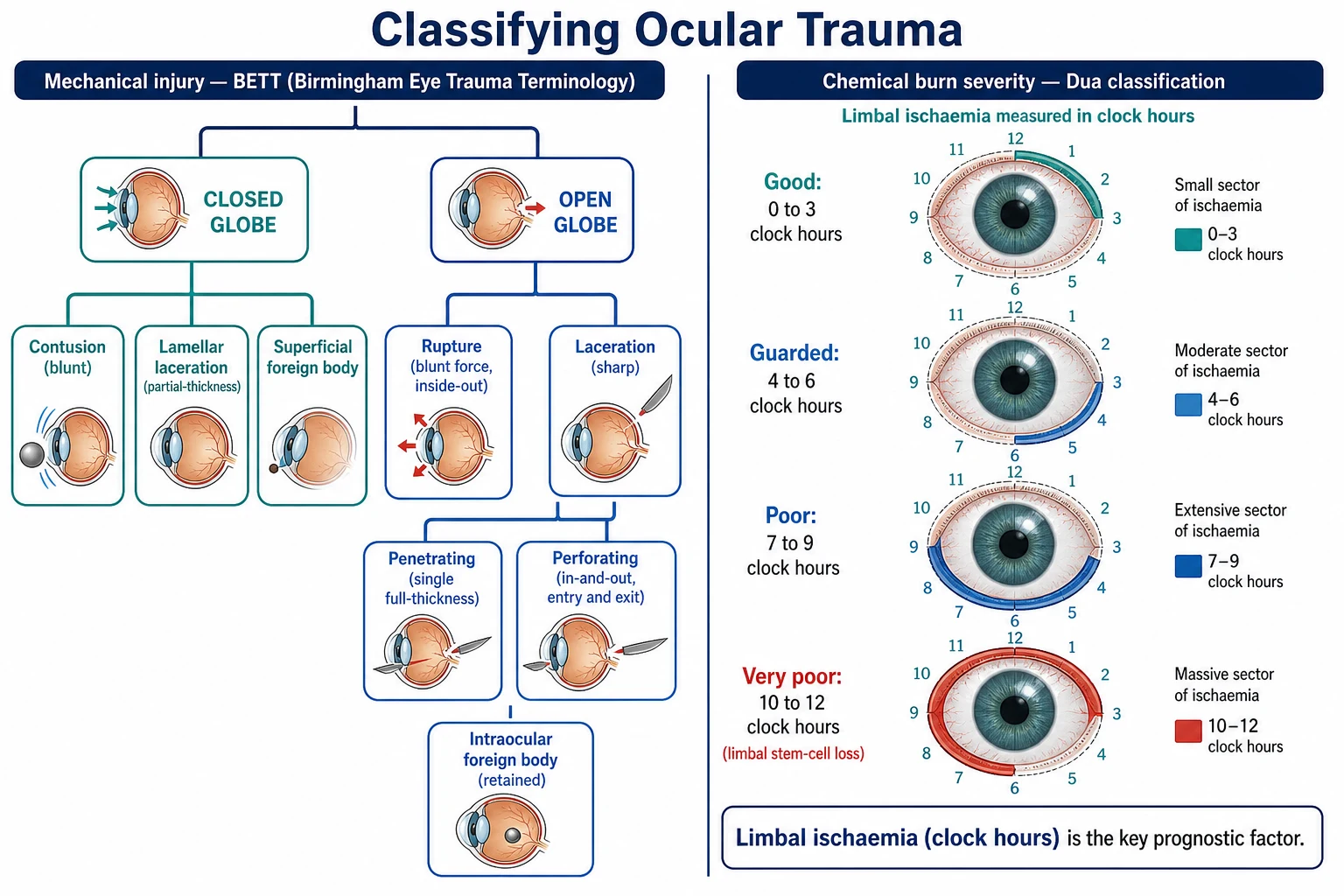
Mechanical eye injuries are named with the Birmingham Eye Trauma Terminology, introduced so that a wound described in one centre means the same thing in another. The first split is whether the wall of the globe is intact. A closed-globe injury leaves the corneoscleral wall whole: a contusion from a blunt blow, a lamellar laceration that is only partial-thickness, or a superficial foreign body sitting on the surface. An open-globe injury is a full-thickness wound of the wall. It is either a rupture, when blunt force bursts the globe from the inside out at its weakest point (the limbus, behind an extraocular muscle insertion, or an old surgical wound), or a laceration, when a sharp object cuts through. [1] [2]
Within laceration, the depth and number of wounds matter. A penetrating injury is a single full-thickness wound — an entrance only. A perforating injury has both an entrance and an exit, so a projectile has passed right through the globe. A retained intraocular foreign body is itself an open-globe injury and carries a particular risk of endophthalmitis. The distinction is not academic: a perforating injury and an intraocular foreign body each subtract points from the Ocular Trauma Score, and each changes the surgical plan. [1] [3]
The Ocular Trauma Classification Group added a zone system to the open-globe laceration — zone 1 confined to the cornea and limbus, zone 2 involving the sclera up to 5 mm posterior to the limbus, and zone 3 posterior to that — because the zone predicts which structures are threatened and how hard the repair will be. [2] Chemical burns are classified separately, by severity rather than mechanism, in the Dua and Roper-Hall systems described below. The Hoskin terminology survey confirmed that BETT remains the working language clinicians actually use at the slit lamp and in the trauma bay. [9]
Epidemiology & Risk Factors
Ocular trauma is common in childhood and over-represented in boys and adolescents, with peaks from projectiles, toys, sport, tools and fireworks. The nationwide study of toy-related ocular injuries in children presenting to United States emergency departments reinforced how often everyday play objects — darts, pellet and Nerf guns, projectiles and pressurised toys — produce serious eye injuries, and how much of this is preventable with eye protection. [10] Sport, do-it-yourself tools, fireworks and assault account for much of the remainder, and rural and remote children may present late after agricultural or mechanical injury. [8]
Chemical injuries are dominated by household and workplace alkalis — bleach, ammonia, drain cleaners, dishwasher and laundry tablets, cement, plaster and fertiliser — because these sit within a child's reach at home. Alkali injuries carry the worst prognosis because alkali penetrates and destroys the limbal stem cells that resurface the cornea, so the same splash from a drain cleaner can blind where an equivalent acid would not. [5] [12] Acid injuries more often follow battery fluid or industrial acids, and thermal and ultraviolet injuries (welder's flash, sunlamp burns) form a smaller group with their own pattern of superficial epithelial injury. [11]
The single biggest risk factor for a poor outcome is delay — delay to irrigation in a chemical injury, delay to recognition and shielding in an open globe, and delay to ophthalmology in either. A second risk factor is the absence of eye protection during high-risk play and work. A third, specific to children, is non-accidental injury: an inconsistent history, a pre-mobile infant, or retinal hemorrhages without a plausible mechanism must raise safeguarding concern and trigger the abusive-head-trauma pathway rather than being accepted at face value. [8]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline frames eye injury as a time-critical presentation in which immediate irrigation of a chemical injury and prompt recognition and shielding of an open globe come before anything else, with coordinated care between paediatrics, ophthalmology and retrieval. Rural and remote children depend on telehealth-guided first aid and early retrieval so that distance does not add to the delay that decides outcome. Eye-protection and household-chemical-safety counselling is part of routine child safety anticipatory guidance. [8]
Pathophysiology
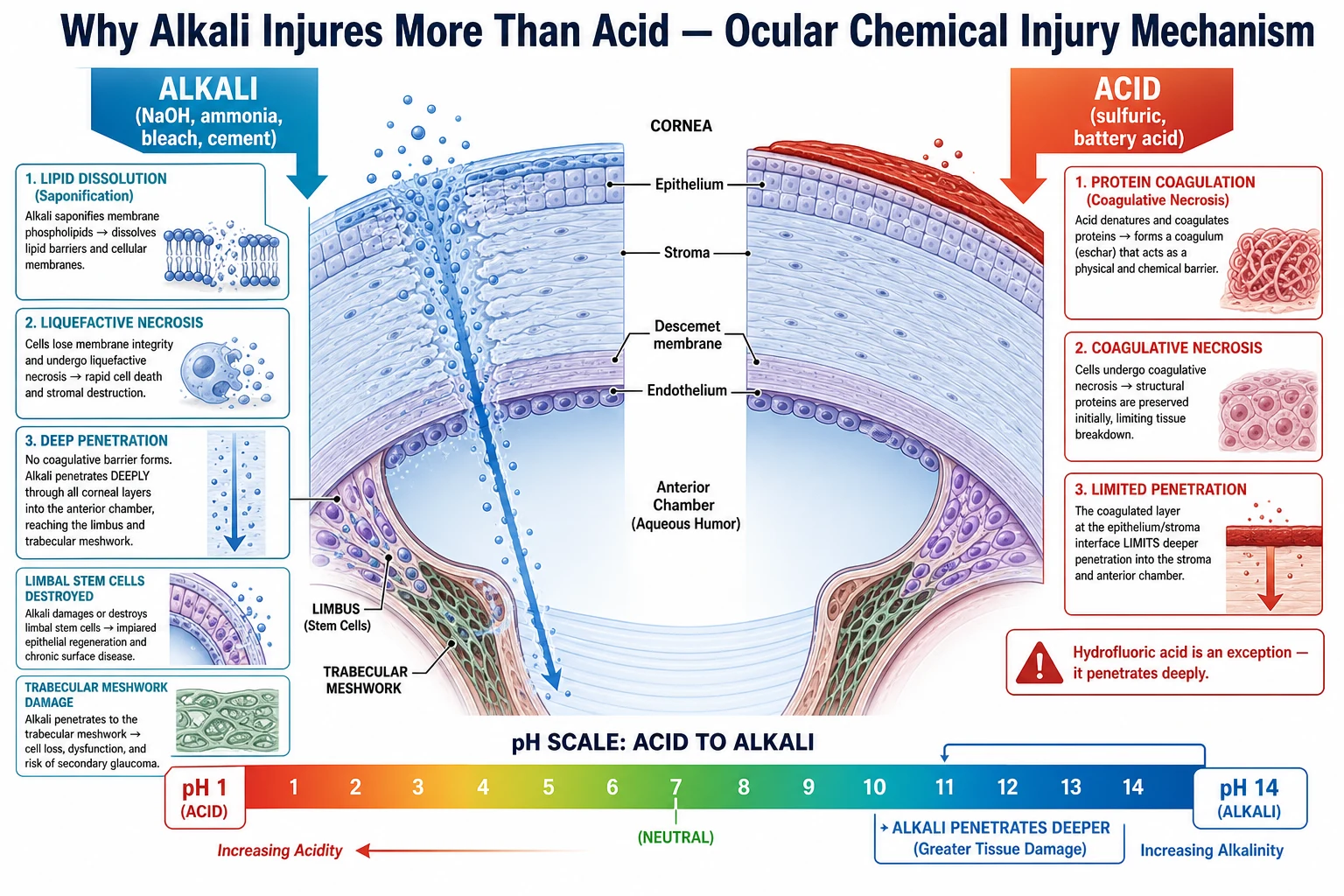
Why does a drain cleaner blind where a lemon-juice splash would not? The answer is in how alkali and acid interact with tissue, and it is the reason the irrigation must start immediately. Alkali — sodium hydroxide, ammonia, bleach, cement — saponifies the lipid membranes of cells, dissolving the barriers that hold tissue together. The result is liquefactive necrosis: the tissue melts, and the alkali keeps moving, penetrating through the corneal stroma into the anterior chamber, where it reaches and destroys the limbal stem cells and damages the trabecular meshwork. [5] [12]
Acid behaves differently. It coagulates surface proteins, producing coagulative necrosis and a tough coagulum — an eschar — that acts as a physical and chemical barrier and limits how deep the acid can go. This is why most acid injuries stay comparatively superficial. The exception is hydrofluoric acid, used in industry and rust removers: its fluoride ion penetrates deeply and chelates calcium, so it injures like an alkali and must be managed with the same urgency. [5] [11] The clinical consequence is that the time to irrigation matters most for alkali, because every minute it sits in the eye it is liquefying tissue and killing stem cells that cannot easily be replaced.
Mechanical trauma follows a different logic. A blunt blow — a ball, a fist, a projectile — momentarily raises the intraocular pressure and can burst the globe from the inside out, a rupture, typically where the wall is thinnest. A sharp object — a dart, a wire, glass — cuts through the wall directly, a laceration. Either way, once the wall is breached the intraocular contents are exposed: the uvea or vitreous can prolapse, the anterior chamber can shallow or flatten, blood can fill it as a hyphema, the globe can soften with hypotony, and the door is open to infection (endophthalmitis) and to the rare immune disaster of sympathetic ophthalmia. Even a closed-globe contusion can shear iris vessels to cause hyphema, batter the retina into commotio retinae, or tear the angle and trabecular meshwork and set up later glaucoma. [1] [7]
Clinical Presentation
The child with a chemical injury presents after a known or suspected splash, with eye pain, blepharospasm, watering, light sensitivity and blurred vision. The lids may be swollen shut and the child uncooperative, but the history usually makes the diagnosis — and the history must trigger irrigation before the formal examination, not after. Once irrigation is under way, the eye shows conjunctival injection and chemosis, epithelial defects that stain with fluorescein, and, in severe alkali injury, a pale, blanched limbus indicating ischaemia of the stem-cell bearing tissue. The paler the limbus, the worse the prognosis, which is exactly what the Dua grade measures. [4] [11]
The child with an open globe presents after blunt or sharp trauma with severe eye pain and reduced vision, and the signs are distinctive. A teardrop or peaked pupil points toward the wound — the peak is iris or uvea plugging the defect. The anterior chamber is shallow or flat, there may be a hyphema, and dark prolapsed uveal tissue or vitreous may sit at the wound. A 360-degree subconjunctival hemorrhage with chemosis can hide an underlying scleral laceration, and the eye is often soft with hypotony. Any of these after trauma is an open globe until proven otherwise. [1] [2]
A closed-globe contusion may present with hyphema alone — a layered blood level in the anterior chamber visible to the naked eye (gross hyphema) or only as red cells on slit-lamp examination (microscopic hyphema) — with traumatic iritis, a dilated or torn pupil, or commotio retinae. Traumatic hyphema has its own tempo: the rebleed classically occurs on day two to five as the original clot retracts, and a rebleed is larger, raises the intraocular pressure, and carries the worst prognosis. [7] [6] Atypical presentations are common in children: the pre-verbal child who cannot localise pain, the stoic older child who minimises the injury, and the small self-sealing wound whose only clue is an abnormally shaped pupil.
Differential Diagnosis
The differential of the red, painful eye after trauma turns on whether the wall of the globe is intact. The dangerous diagnosis is the open globe, and it must be excluded before the eye is pressed, probed or patched. A corneal abrasion causes pain, watering and a fluorescein-staining defect but preserves a normal pupil, a formed chamber and a firm globe. A superficial or intraorbital foreign body causes a foreign-body sensation and watering; an intraorbital foreign body may sit behind the globe with little surface sign and is found on imaging. [2] [8]
[8]When the mechanism is unclear, non-traumatic hyphema must be considered — juvenile xanthogranuloma, a bleeding disorder, a posterior segment tumour such as retinoblastoma, or self-induced eye-rubbing — because treating these as trauma misses the underlying disease. A chemical injury is usually evident from the history, but a thermal or ultraviolet injury (welder's flash) can mimic it with severe epithelial shedding and pain that peaks hours after exposure. The cardinal error in all of these is twofold: pressing a suspected open globe to examine it, and delaying irrigation in a chemical injury to complete an assessment first. Both errors convert a salvageable eye into a lost one. [5] [1]
Clinical & Bedside Assessment
The assessment is shaped by the suspected injury, because what you are allowed to do to the eye depends on it. Begin with the history: the mechanism (blunt versus sharp, chemical versus mechanical), the exact agent or object, whether eye protection was worn, the time since injury and any first aid already given, the vision before and after, past ocular history (including prior surgery that weakens the globe), and the immunisation and tetanus history. In a chemical injury this history is gathered while irrigation is running. [8] [11]
For a chemical injury, irrigation comes first; once it is established, record the visual acuity in each eye separately with an age-appropriate method, examine the lids, evert the upper lid to find retained particulate matter (a fleck of cement plastered to the tarsal conjunctiva will keep re-injuring until removed), and assess the cornea and limbus for the extent of ischaemia. A drop of topical anaesthetic and fluorescein makes this tolerable. The pH is checked with indicator paper after the first irrigation and again after a five-to-ten-minute pause, and irrigation continues until the reading is neutral. [5] [12]
Open globe — never do these
For a suspected open globe, examine gently and without pressure. Record the vision if the child can give it. Look for the teardrop pupil and assess the anterior chamber depth and pupillary shape, look for prolapsed tissue, and note a 360-degree subconjunctival hemorrhage that may overlie a hidden scleral laceration. Do not pry the lids open forcibly — if the lids are too swollen to open gently, stop and image, because forcing them can express intraocular contents. Examine the whole child for associated facial, orbital and intracranial injury, and have a low threshold for examination under sedation or anaesthesia once the globe is protected, because a frightened or pre-verbal child cannot cooperate. When the history is inconsistent, consider non-accidental injury. [2] [8]
Investigations
Ocular trauma is a clinical diagnosis at first contact, and the most important bedside test during resuscitation is the tear-film pH in a chemical injury — measured with indicator paper only after irrigation has begun, and used to judge when irrigation can stop. In a suspected open globe, no pressure is applied to the globe, which rules out applanation tonometry until the globe is repaired or protected; the diagnosis is made on the signs already described. [5] [1]
Computed tomography of the orbits and brain is the imaging of choice when an open globe, an intraocular or intraorbital foreign body, an orbital fracture, or intracranial injury is suspected. CT locates a retained foreign body, defines a fracture, and reveals associated brain injury. Magnetic resonance imaging must be avoided when a metallic foreign body is possible, because the magnet can move it and cause further injury. B-scan ultrasonography helps when the view is obscured by hyphema or corneal opacity, but only once open globe has been excluded or the globe is protected, because the probe presses on the eye. [2] [8]
In traumatic hyphema, a sickle cell test is warranted in at-risk children because sickled red cells block the trabecular meshwork, so even a small hyphema can spike the intraocular pressure and threaten the optic nerve — and it lowers the threshold for surgical evacuation. A coagulation screen is worth checking when the hyphema is disproportionate to the mechanism, suggesting an underlying bleeding tendency. Blood cultures are not routine unless endophthalmitis is suspected. [7] [6]
Management — Resuscitation
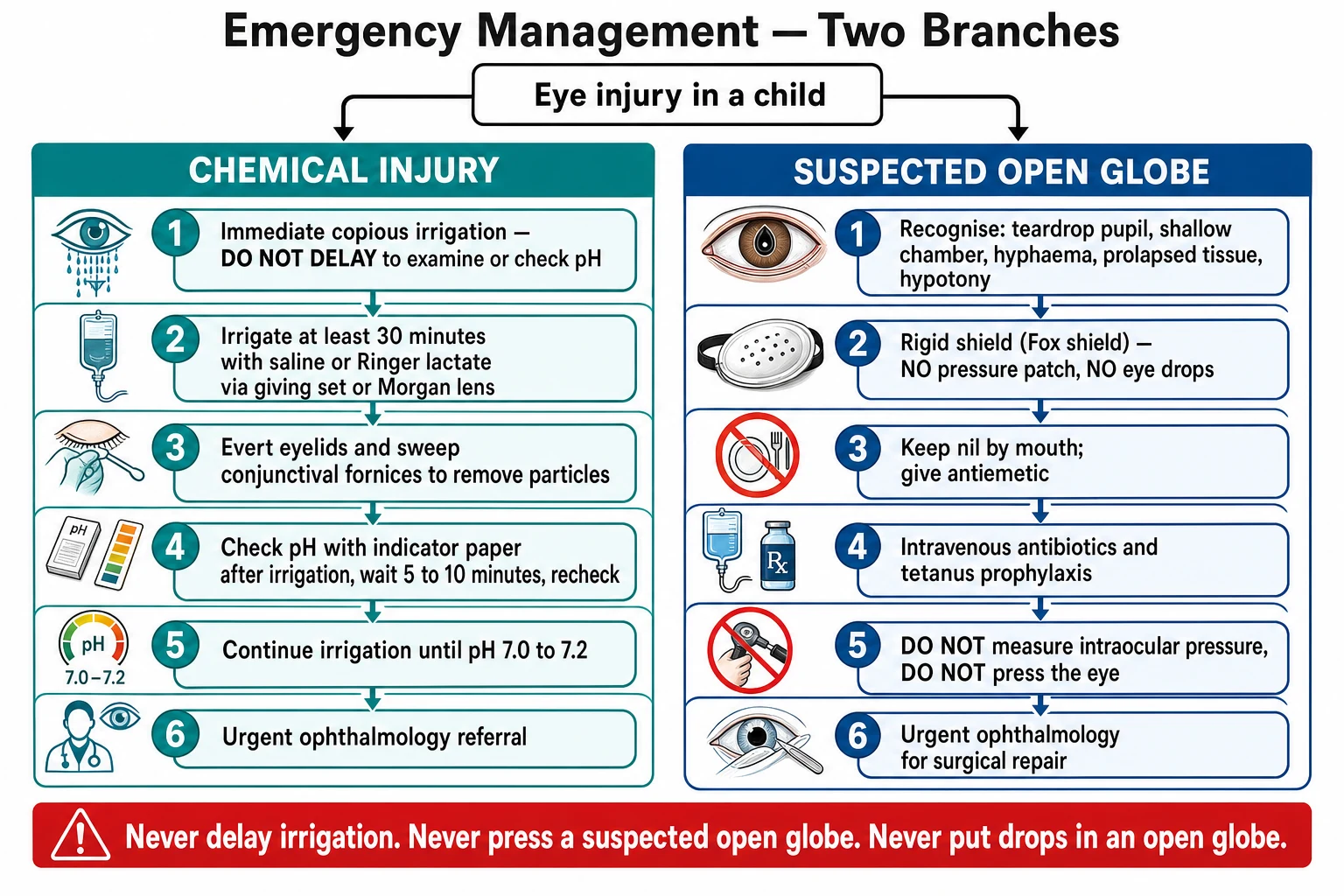
Resuscitation in ocular trauma is the two first-contact pillars, executed in the correct order. For a chemical injury, the resuscitation is the irrigation: begin copious irrigation with saline or Ringer lactate immediately, before examination and before a pH check. Instil a drop of topical anaesthetic to make irrigation tolerable, irrigate for at least 30 minutes, evert the lids and sweep the conjunctival fornices, and remove particulate matter with a moist cotton swab or fine forceps — a fleck of cement or tablet left in the fornix will keep releasing alkali. After the first irrigation, check the pH with indicator paper, wait five to ten minutes, recheck, and continue until the pH is 7.0 to 7.2. If only tap water is available at the scene, use it copiously — the volume and speed matter more than the fluid. [5] [11]
For a suspected open globe, resuscitation is protection and preparation for surgery. Place a rigid Fox shield over the eye — large enough to cover the orbit and lids, taped or bandaged so that it does not touch or press the globe. Keep the child nil by mouth and give an antiemetic, because vomiting raises venous pressure and can extrude intraocular contents. Give intravenous antibiotics with anti-endophthalmitis cover (covering Gram-positive and Gram-negative organisms — for example vancomycin plus ceftazidime, or a systemic fluoroquinolone, per local protocol) and tetanus prophylaxis. Provide analgesia and a calm environment, and escalate to paediatric intensive care for associated brain or facial injury. [1] [8]
The discipline of resuscitation is to separate the two injuries and not mix them up. A chemical injury that is shielded but not irrigated keeps burning; an open globe that is irrigated under pressure, prodded or patched can be destroyed. When the two coexist — for example, an alkali splash onto a globe already lacerated — irrigate gently without pressure, shield, and refer. The well child with a simple corneal abrasion and no open-globe sign is managed more conservatively, but only after open globe has been deliberately excluded. [8] [11]
Management — Definitive & Stepwise
Definitive management follows the resuscitation and is matched to the injury. A chemical injury, once irrigated to a neutral pH, is graded for severity and referred for ocular-surface care. An open globe is shielded, given antibiotics and tetanus, and repaired surgically. A closed-globe contusion and hyphema is managed medically with ophthalmology input. A retained intraocular foreign body is localised and removed vitreoretinally. The art is to match the intensity to the injury and to reassess relentlessly, because the complications are time-sensitive. [8] [3]
For a chemical injury after irrigation, grade the severity with the Dua classification (clock hours of limbal ischaemia) and the Roper-Hall grade. Give topical antibiotics to prevent infection, a cycloplegic for comfort and to prevent synechiae, and intraocular-pressure-lowering agents when the pressure rises from trabecular meshwork damage. Severe limbal ischaemia — more than about six clock hours — predicts limbal stem-cell deficiency and corneal scarring, and warrants urgent ophthalmology for amniotic-membrane transplantation and, later, limbal-stem-cell transplantation or keratoprosthesis in the worst cases. [4] [12]
The two-branch ocular-trauma pathway
Chemical splash: start copious irrigation with saline or Ringer lactate immediately, before examination and before a pH check.
Irrigate for at least 30 minutes, evert the lids, sweep the fornices and remove particulate matter, then check the pH and continue until it reads 7.0 to 7.2.
Grade the chemical burn by clock hours of limbal ischaemia (Dua) and refer urgently to ophthalmology for ocular-surface care; consider amniotic-membrane or limbal-stem-cell strategies for severe ischaemia.
Suspected open globe: apply a rigid Fox shield with no pressure, keep the child nil by mouth, give an antiemetic, intravenous antibiotics and tetanus prophylaxis.
Do not press the eye, do not apply drops, do not measure intraocular pressure; obtain CT of the orbits and brain to confirm the injury, locate any foreign body and assess associated injury.
Refer urgently to ophthalmology for surgical repair, with vitrectomy as indicated for a posterior injury or intraocular foreign body.
Manage traumatic hyphema with activity restriction, head elevation, daily review for rebleeding and intraocular pressure, and sickle cell screening in at-risk children.
Arrange amblyopia and vision surveillance at discharge, because the developing visual system is unforgiving of deprivation.
For an open globe, the priorities after shielding are intravenous antibiotics with anti-endophthalmitis cover, tetanus prophylaxis, and urgent surgical repair by ophthalmology — primary closure of the wound, restoration of the globe, and vitrectomy as indicated for a posterior injury, retinal detachment, or a non-metallic intraocular foreign body. A metallic foreign body may need magnet or vitreoretinal removal depending on size and site. Systemic corticosteroids may be used postoperatively at ophthalmology discretion to reduce inflammation and the risk of sympathetic ophthalmia. [2] [8]
For traumatic hyphema, management is conservative in most children: restrict activity, elevate the head, avoid antiplatelet agents, control any intraocular-pressure rise medically, and review daily for rebleeding and pressure. The Cochrane review of medical interventions for traumatic hyphema found no clear benefit of aminocaproic acid or systemic steroids on visual outcome, so these are not routine; the review and the controversies analysis both stress that the evidence for pharmacological prophylaxis is weak. [6] [7] Surgical evacuation of the blood is reserved for complications — corneal blood staining, uncontrolled glaucoma, a large clot that risks staining, or a persistently raised pressure in sickle-cell disease, in which a smaller hyphema can still blind. [7]
Specific Subtypes & Scenarios
An alkali splash from a household cleaner. This is the prototypical chemical emergency. Begin irrigation at the scene and continue it through to the emergency department, remove particulate matter from the fornices, irrigate to a neutral pH, grade the limbal ischaemia, and refer urgently. The outcome tracks the delay to irrigation and the clock hours of ischaemia more than anything else, so the first responder who irrigates immediately has done more for vision than the surgeon who repairs the late scarring. [5] [12]
A suspected open globe from a sharp object or a blunt blow. Recognise the teardrop pupil, shallow chamber, hyphema or prolapsed tissue, shield without pressure, keep the child nil by mouth with an antiemetic, give intravenous antibiotics and tetanus, and refer for surgical repair. The single rule is never to press, never to apply drops, and never to run a tonometer over a globe that may be open. [1] [2]
Traumatic hyphema. Restrict activity, elevate the head, avoid aspirin and non-steroidal anti-inflammatory drugs, and review daily for the day-two-to-five rebleed and for intraocular pressure. Screen for sickle cell in at-risk children, because sickled cells block the trabecular meshwork and lower the threshold for surgery. The Cochrane review confirms no clear benefit of aminocaproic acid, so pharmacological prophylaxis is not routine. [6] [7]
A retained intraocular foreign body. Localise it with CT, give intravenous antibiotics and tetanus, and arrange vitreoretinal removal. Stay alert for endophthalmitis, which can destroy the eye within days — worsening pain, falling vision and increasing inflammation after a penetrating injury demand urgent ophthalmology and intravitreal antibiotics. [2] [8]
Sympathetic ophthalmia. This is the rare bilateral granulomatous panuveitis that follows a penetrating injury, appearing anywhere from days to years later with a peak around three months, when the uninjured 'sympathising' eye inflames alongside the injured 'exciting' eye. It is treated with systemic immunosuppression. Enucleation of a blind, severely injured exciting eye within 14 days of the injury may prevent it, which is one reason a hopelessly injured eye is sometimes removed rather than repaired. [1] [8]
Non-accidental injury. When the history of an ocular injury is inconsistent, when the child is pre-mobile, or when retinal hemorrhages appear without a plausible mechanism, consider non-accidental injury and trigger the abusive-head-trauma and safeguarding pathway. Ocular findings — particularly extensive, multilayered retinal hemorrhages — can be the presenting sign of inflicted brain injury, and accepting an implausible story delays protection. [8]
Complications & Pitfalls
The complications of ocular trauma are visual and structural, and in a child they include the hidden harm of amblyopia. Chemical injury scars the cornea, destroys limbal stem cells (limbal stem-cell deficiency), raises the intraocular pressure through trabecular meshwork damage, causes cataract, and can culminate in a blind, painful eye. Open-globe injury risks endophthalmitis, retinal detachment, choroidal hemorrhage, proliferative vitreoretinopathy, phthisis bulbi, and sympathetic ophthalmia. Hyphema can rebleed, stain the cornea, and spike the pressure to ischaemic optic-nerve levels. Across all of these, the developing visual system adds amblyopia as a time-dependent complication that must be actively surveyed and treated. [5] [7]
The cardinal pitfall is delaying irrigation in a chemical injury to complete an assessment first. The history of a splash is enough to irrigate; the slit-lamp and the pH come after the first 30 minutes. A second pitfall is pressing a suspected open globe — to examine it, to apply a pressure patch, to instil drops, or to measure the intraocular pressure — each of which can extrude intraocular contents. A third is missing a small or self-sealing wound, especially a scleral laceration hidden behind a 360-degree subconjunctival hemorrhage, or a tiny intraocular foreign body whose only early sign is an abnormal pupil. A fourth is forgetting the whole child: the blow that ruptured a globe may also have fractured an orbit or injured a brain. [1] [8]
A fifth pitfall, specific to children, is neglecting amblyopia and the other eye. A structurally repaired eye in a young child still needs vision and amblyopia follow-up, because deprivation in the first years of life wires in permanent visual loss even when the anatomy is restored. And a sixth is missing non-accidental injury by accepting an implausible history for an injury in a pre-mobile infant. Each of these is preventable, and each is examined. [8]
Prognosis & Disposition
Prognosis after a chemical injury is determined by the extent of limbal ischaemia in clock hours (the Dua grade), the depth of penetration, and the time to irrigation. Delayed irrigation and severe limbal ischaemia — more than about six clock hours — predict limbal stem-cell deficiency, corneal scarring and poor vision, even with later reconstruction. [4] [12] Prognosis after an open-globe injury is captured by the Ocular Trauma Score, which combines the presenting acuity with subtractions for rupture, perforating injury, endophthalmitis, retinal detachment and an afferent pupillary defect; the worse the raw score, the worse the predicted final vision. [3]
The Ocular Trauma Score is built as follows. The presenting visual acuity sets the starting raw score — no light perception 60, light perception or hand motions 70, 1/200 to 19/200 (around counting fingers) 80, 6/60 to 6/15 (20/200 to 20/50) 90, and 6/12 (20/40) or better 100. Points are then subtracted for a rupture (minus 23), endophthalmitis (minus 17), perforating injury (minus 14), retinal detachment (minus 11), and an afferent pupillary defect (minus 10). The raw score maps to one of five categories: 0 to 44 category 1 (worst), 45 to 65 category 2, 66 to 80 category 3, 81 to 91 category 4, and 92 to 100 category 5 (best). A child in category 1 has a high chance of no light perception; a child in category 5 usually keeps useful vision. [3]
Ocular Trauma Score — the raw-score arithmetic
high
Disposition follows the injury. All chemical injuries and suspected open globes are referred urgently to ophthalmology. Hyphema is managed with ophthalmology input and daily review, and the child is admitted for surgical repair, severe injury, an unreliable family or social circumstance, or when associated brain or facial injury needs inpatient care. At discharge, arrange amblyopia and vision surveillance, ocular-surface and intraocular-pressure follow-up for chemical injury, and retina and amblyopia follow-up after open-globe repair, with a clear safety-net for pain, visual loss or rebleeding. [8]
Special Populations
Pre-verbal and frightened children cannot cooperate with a detailed eye examination and may not localise pain. Examine gently, use a topical anaesthetic, and keep a low threshold for examination under sedation or anaesthesia — but only once an open globe has been excluded or the globe is protected with a shield, because sedation is not a reason to press a possibly open eye. [8]
Children with sickle cell disease or trait are at particular risk from even a small hyphema. Sickled red cells block the trabecular meshwork, so the intraocular pressure climbs steeply and threatens the optic nerve with ischaemia; the threshold for surgical evacuation is lower, and standard pressure-lowering choices must avoid agents that worsen sickling. Screen for sickle cell in at-risk children with hyphema and keep the pressure low. [7]
Aboriginal and Torres Strait Islander, Maori and Pasifika children, and refugee, asylum-seeking and migrant families may carry a higher burden of injury and may face barriers to timely assessment. Ensure culturally safe, equitable care delivered with the family, use trained interpreters, and arrange early retrieval and telehealth-guided first aid for rural and remote children so that distance does not add to the delay that decides outcome. [8]
Children with a single seeing eye or an existing visual impairment have higher stakes from further injury, because losing the fellow eye means blindness. Protect and prioritise these children, lower the threshold for surgical exploration, and reinforce eye protection counsel at every visit, because prevention matters most when the reserve is gone. [8]
Evidence, Guidelines & Regional Differences
The evidence base for ocular trauma rests on landmark classification papers and large case series rather than randomised trials, because the ethics of withholding treatment are clear. The Kuhn Birmingham Eye Trauma Terminology paper standardised the language of eye injury into closed and open globe, and the Pieramici Ocular Trauma Classification Group added the zone system for open-globe laceration; the Hoskin terminology survey confirmed that BETT remains the working language clinicians use at the slit lamp and in the trauma bay. [1] [2] [9]
The Ocular Trauma Score (OTS)
Population: A large series of eye injuries, used to derive and validate a prognostic score for final visual outcome from the presenting clinical features.
Key finding
A small set of variables — the presenting visual acuity plus the presence of rupture, endophthalmitis, perforating injury, retinal detachment and an afferent pupillary defect — predicted the final vision with useful accuracy, giving five prognostic categories from best to worst.
Practice change
The OTS lets the clinician give a family an honest early prognosis and triage the urgency of repair and follow-up, anchored to reproducible clinical features rather than impression.
For chemical injury, the Dua classification reframed prognosis around clock hours of limbal ischaemia rather than corneal haze, because the limbus holds the stem cells; Wagoner's review set out the alkali-versus-acid pathophysiology and the irrigation-first principle that still drives management; and the current-perspectives review consolidates modern ocular-surface reconstruction. [4] [5] [12] For hyphema, the Gharaibeh Cochrane review found no clear benefit of aminocaproic acid or systemic steroids on visual outcome or rebleeding, and the Bansal review set out the residual controversies — the place of pharmacological prophylaxis, the surgical thresholds, and the special danger of sickle-cell disease. [6] [7] The Salvin review frames the systematic paediatric approach, and the Ashourizadeh nationwide study quantifies toy-related injury and underwrites eye-protection counselling. [8] [10]
Medical interventions for traumatic hyphema
Population: Randomised trials of pharmacological interventions — systemic aminocaproic acid, tranexamic acid and corticosteroids — in people with traumatic hyphema.
Key finding
The evidence for a benefit of aminocaproic acid or systemic steroids on visual outcome, rebleeding or complications was of low certainty and did not clearly support routine use.
Practice change
Most children with traumatic hyphema are managed without pharmacological prophylaxis; activity restriction, head elevation, daily review for rebleeding and pressure, and sickle-cell screening remain the backbone, with surgery reserved for complications.
The regional policy structure is consistent in principle and varies in detail. In the UK, NICE guidance and Royal College of Paediatrics and Child Health pathways set the first-aid and referral expectations. In Australia and New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline frames eye injury as a time-critical presentation with irrigation-first for chemicals and shield-don't-press for open globe. In North America, the American Academy of Ophthalmology EyeWiki and Preferred Practice Patterns set the management framework, and the American Academy of Pediatrics reinforces injury-prevention counselling. The controversies — aminocaproic acid in hyphema, early versus late surgery, amniotic-membrane and stem-cell strategies, and primary enucleation to prevent sympathetic ophthalmia — are resolved everywhere by the same principle: irrigate chemical injuries first, shield open globes, and refer early. [11] [8]
Exam Pearls
- A chemical eye injury is irrigated first — before examination and before checking the pH — with saline or Ringer lactate for at least 30 minutes, continued until the pH is 7.0 to 7.2. [5]
- Alkali causes liquefactive necrosis and penetrates deeply; acid causes coagulative necrosis and a barrier that limits penetration; hydrofluoric acid is the exception that penetrates. [5]
- The Dua classification grades chemical burns by clock hours of limbal ischaemia, the key prognostic factor: 0 to 3 good, 4 to 6 guarded, 7 to 9 poor, 10 to 12 very poor. [4]
- BETT separates closed globe (wall intact: contusion, lamellar laceration, superficial foreign body) from open globe (full-thickness defect); within open globe, rupture is blunt and inside-out, laceration is sharp, penetrating is an entrance only and perforating is in-and-out, with retained intraocular foreign body its own open-globe injury. [1]
- The open-globe signs are a teardrop pupil, shallow or flat anterior chamber, hyphema, prolapsed uveal tissue or vitreous, 360-degree subconjunctival hemorrhage and a soft eye with hypotony. [2]
- A suspected open globe is protected with a rigid Fox shield and no pressure; keep the child nil by mouth with an antiemetic, give intravenous antibiotics and tetanus, and refer urgently for surgery — never press, never apply drops, never measure intraocular pressure. [1]
- The Ocular Trauma Score starts from presenting acuity (NPL 60, LP/HM 70, 1/200 to 19/200 (CF) 80, 6/60 to 6/15 90, 6/12 or better 100) and subtracts for rupture 23, endophthalmitis 17, perforating injury 14, retinal detachment 11, afferent pupillary defect 10. [3]
- Traumatic hyphema rebleeds on day two to five; screen for sickle cell in at-risk children; aminocaproic acid has no clear benefit (Cochrane). [6] [7]
- Sympathetic ophthalmia is a rare bilateral granulomatous panuveitis after penetrating injury; enucleation of a blind injured eye within 14 days may prevent it. [1]
- Never forget amblyopia: a repaired young eye still needs vision and amblyopia follow-up, because the developing visual system is unforgiving of deprivation. [8]
References
- [1]Kuhn F; Morris R; Witherspoon CD; Heimann K; Jeffers JB; Treister G A standardized classification of ocular trauma. Graefes Arch Clin Exp Ophthalmol, 1996.PMID 8738707
- [2]Pieramici DJ; Sternberg P Jr; Aaberg TM Sr; Bridges WZ Jr; Capone A Jr; Cardillo JA A system for classifying mechanical injuries of the eye (globe). The Ocular Trauma Classification Group. Am J Ophthalmol, 1997.PMID 9535627
- [3]Kuhn F; Maisiak R; Mann L; Mester V; Morris R; Witherspoon CD The Ocular Trauma Score (OTS). Ophthalmol Clin North Am, 2002.PMID 12229231
- [4]Dua HS; King AJ; Joseph A A new classification of ocular surface burns. Br J Ophthalmol, 2001.PMID 11673310
- [5]Wagoner MD Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol, 1997.PMID 9104767
- [6]Gharaibeh A; Savage HI; Scherer RW; Goldberg MF; Lindsley K Medical interventions for traumatic hyphema. Cochrane Database Syst Rev, 2019.PMID 30640411
- [7]Bansal S; Gunasekeran DV; Ang B; Lee J; Khandelwal R; Sullivan P Controversies in the pathophysiology and management of hyphema. Surv Ophthalmol, 2016.PMID 26632664
- [8]Salvin JH Systematic approach to pediatric ocular trauma. Curr Opin Ophthalmol, 2007.PMID 17700228
- [9]Hoskin AK; Fliotsos MJ; Rousselot A; Ng SMS; Justin GA; Blanch R Globe and Adnexal Trauma Terminology Survey. JAMA Ophthalmol, 2022.PMID 35862061
- [10]Ashourizadeh H; Grinspan N; Lu ES; Armstrong GW A nationwide retrospective study of toy-related ocular injuries in children presenting to emergency departments in the United States. J AAPOS, 2026.PMID 42431578
- [11]Patek GC; Bates A; Gurnani B Ocular Burns. StatPearls, 2026.PMID 29083604
- [12]Rajarajan M; Bhambhani Chavda V; Murugesan V; Agarwal S Chemical Injuries Classification and Management - Current Perspectives. Semin Ophthalmol, 2026.PMID 40709370