Paeds · ophthalmology
Ophthalmia neonatorum
Also known as Neonatal conjunctivitis · Ophthalmia neonatorum · Gonococcal ophthalmia neonatorum · Chlamydial ophthalmia neonatorum · Inclusion conjunctivitis of the newborn · Sticky eye of the newborn
Fellowship topic on ophthalmia neonatorum — conjunctivitis arising in the first 28 days of life. Covers the chemical, gonococcal, chlamydial and herpes simplex causes with their onset windows and discharge characters; the epithelial-invasive and intracellular pathophysiology that explains corneal perforation, chlamydial pneumonia and neonatal HSV dissemination; the swab and PCR work-up; the cause-specific systemic treatment of single-dose ceftriaxone for gonorrhoea, oral erythromycin for 14 days for chlamydia and intravenous aciclovir for HSV; birth ocular prophylaxis and maternal sexually-transmitted-infection screening; and ANZ, UK, US and Canadian guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A midwife calls you to the postnatal ward about a three-day-old boy whose right eye has been weeping thick yellow discharge since the morning, the lids now so swollen he cannot open them. Half an hour later a general-practitioner referral arrives: a ten-day-old with bloodstained mucopurulent discharge and a curious, repetitive cough. Both are ophthalmia neonatorum, but the first is a sight-threatening emergency and the second is a systemic infection in disguise. The fellowship skill is to read the day of life and the discharge and act on the cause, because the difference between them is measured in hours of corneal viability. [1] [12]
Ophthalmia neonatorum is any conjunctivitis — conjunctival inflammation with discharge — arising in the first 28 days of life. The name is old but the problem is current: worldwide it remains one of the commonest neonatal infections, and in settings without antenatal screening and birth prophylaxis it is still a leading preventable cause of childhood blindness. The conjunctiva of the newborn is immature, its tear film and immune defences underdeveloped, so organisms picked up during vaginal delivery invade readily and, for gonorrhoea, with devastating speed. [1] [2]
What makes the topic examinable is that the causes behave so differently. Gonorrhoea invades the conjunctival epithelium and can erode through the cornea within hours; chlamydia is an obligate intracellular organism that seeds the nasopharynx and descends to the lung; herpes simplex replicates in surface epithelium, forms a dendritic ulcer and may signal disseminated disease; and chemical conjunctivitis is simply the irritant effect of prophylactic drops. The clinical tool that separates them is the onset window and the character of the discharge, and it drives both the investigation panel and the systemic treatment — which is why a neonatal red eye is investigated and treated far more aggressively than conjunctivitis in an older child. [1] [3]
Classification
Picture the four causes laid out along a timeline of the first month of life, because that timeline is the whole point of the classification. The day the discharge begins, more than any single test, points to the organism. [1]
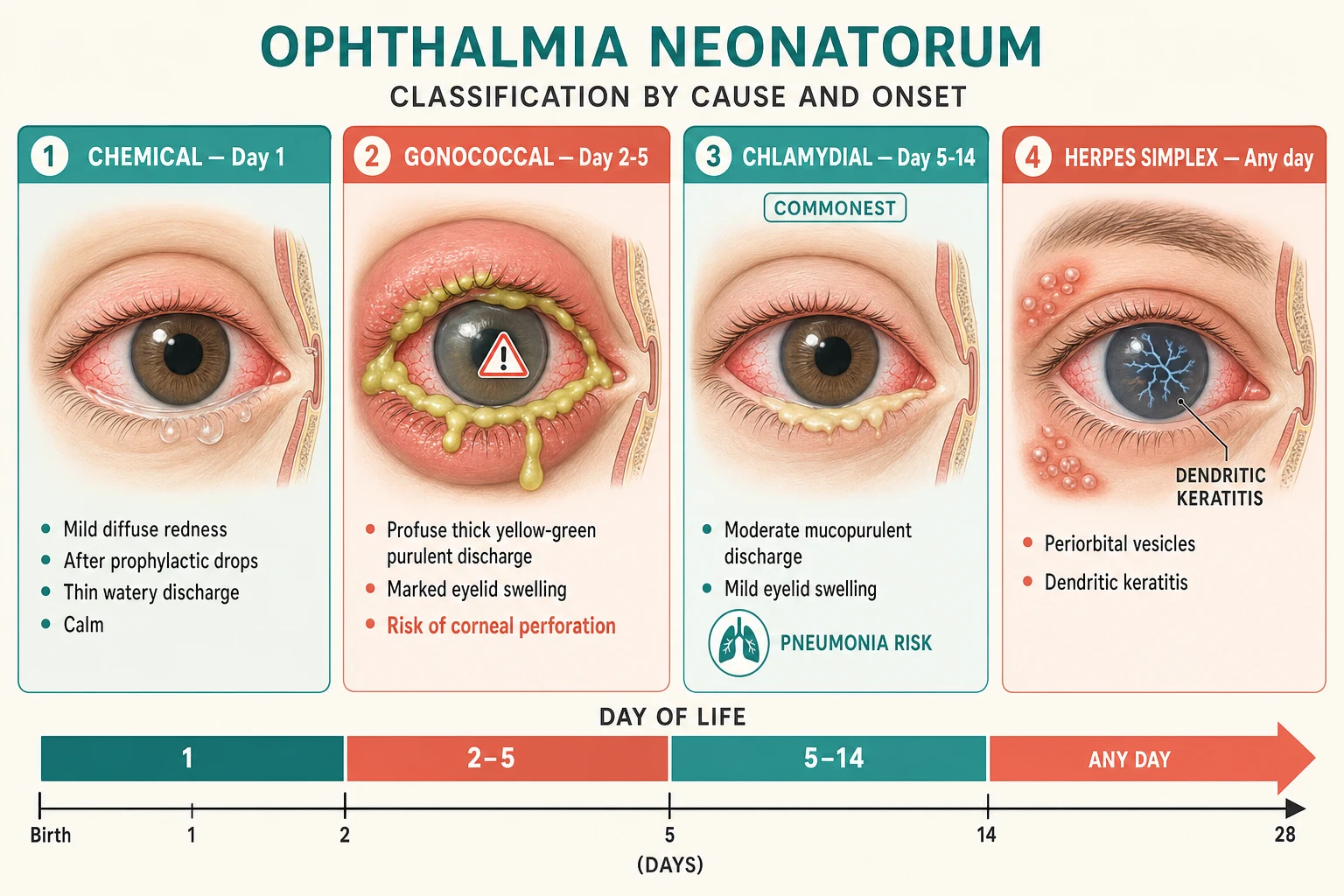
Ophthalmia neonatorum classified by cause and onset window
The classification does more than label — it triages. A discharge beginning in the first day after prophylactic drops is chemical and needs only observation, while one beginning on day two to five with profuse pus and lid oedema is gonococcal until proven otherwise and needs an emergency response. The chemical, gonococcal, chlamydial and herpes simplex windows are the spine of every history, examination and management decision that follows. [1]
Epidemiology & Risk Factors
Globally, ophthalmia neonatorum remains one of the commonest infections of the newborn, and its burden tracks the reach of antenatal screening and birth prophylaxis. A 2025 systematic review and meta-analysis confirmed high prevalence in regions without universal prophylaxis and a steep fall wherever it is practised. Where screening and prophylaxis are in place, chlamydia is the leading cause and gonorrhoea — though rarer — is the most sight-threatening. [2]
The core risk factor is maternal cervical infection acquired during vaginal delivery, amplified by absent or inadequate antenatal sexually-transmitted-infection screening, prolonged rupture of membranes and untreated maternal gonococcal or chlamydial carriage. A mother with undiagnosed gonorrhoea transmits the organism to around a third to half of exposed neonates, and many of those develop eye disease; the parallel figures for chlamydia are comparable. Caesarean delivery before membrane rupture substantially reduces but does not abolish the risk. [1] [3]
Two facts shape prevention. First, routine ocular prophylaxis at birth markedly reduces gonococcal ophthalmia but does not prevent chlamydial disease — so chlamydia dominates wherever prophylaxis alone is relied upon. Second, 2.5% povidone-iodine is a low-cost, effective prophylactic agent studied in resource-limited settings and now recommended by several authorities as an alternative to antibiotic ointment. The disproportionate burden falls on communities with limited antenatal screening, and the systemic spread of the causative organisms — chlamydial pneumonia, neonatal HSV dissemination — is amplified in the newborn. [3] [9] [10]
Pathophysiology
Why does gonorrhoea perforate the cornea while chlamydia causes pneumonia? The answer lies in how each organism grows, and it is the reason chlamydia and herpes simplex demand systemic rather than topical treatment. [6]
The neonatal conjunctiva is immature: its tear film is thin, lysozyme and secretory IgA are low, and the epithelial barrier is still developing. Organisms acquired during passage through an infected birth canal therefore meet a weakly defended surface and invade easily. This shared vulnerability is why a single exposure can produce disease so rapidly, and why prophylaxis at birth matters more than treating the established infection. [1]
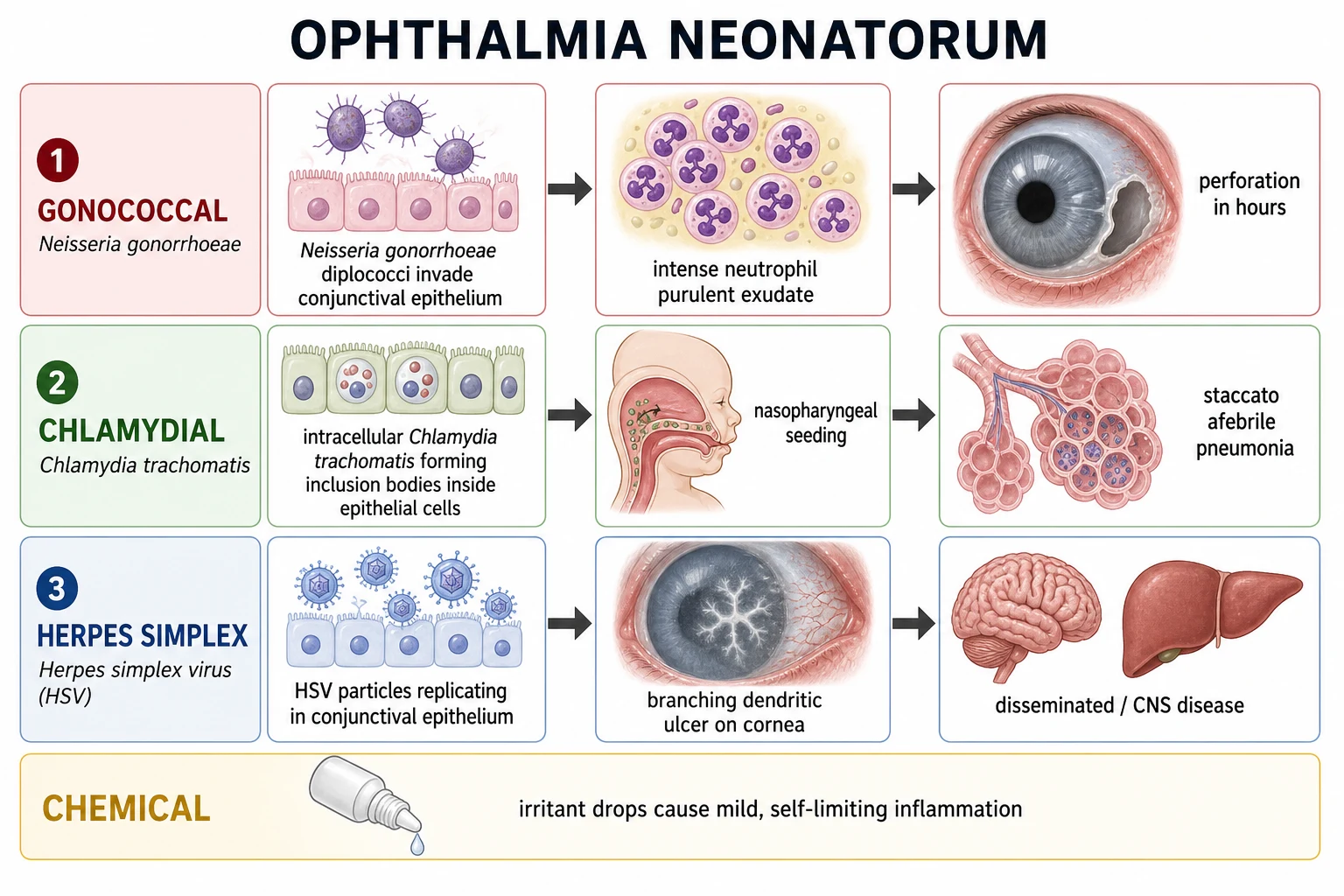
Gonococcal disease is the archetype of epithelial invasion. Neisseria gonorrhoeae attaches to and multiplies within the conjunctival epithelium, provoking an intense neutrophil-rich purulent reaction. The proteases and toxins released, together with the sheer mass of pus, can erode through the corneal epithelium and stroma and perforate the globe within hours if untreated — which is why gonococcal ophthalmia is measured against the clock, not the clinic day. [1] [11]
Chlamydial disease is the archetype of intracellular infection. Chlamydia trachomatis is an obligate intracellular organism that replicates inside conjunctival epithelial cells, forming inclusion bodies, and it cannot be reached by topical drops once intracellular. More importantly, it seeds the nasopharynx and can descend the airway to cause a distinctive afebrile, staccato pneumonia at four to twelve weeks of age. This is the single most important reason chlamydia is treated systemically: topical therapy clears the eye but leaves the organism in the chest. [6] [5]
Herpes simplex disease is the archetype of viral epithelial spread. HSV replicates in the conjunctival and corneal epithelium, producing the branching dendritic ulcer of HSV keratitis, and in the neonate an isolated eye finding may be the first sign of skin-eye-mouth, central-nervous-system or disseminated disease. Chemical conjunctivitis is simply the irritant effect of silver nitrate or antibiotic prophylactic drops — self-limiting, resolving within days without treatment. [7] [8]
Clinical Presentation
Read the eye the way the timeline tells you to — the day of life and the discharge do most of the diagnostic work, and the systemic signs do the rest. [1]
Chemical conjunctivitis announces itself in the first 24 hours, almost always after prophylactic ocular drops have been instilled at birth. It is a mild bilateral conjunctival injection with mild watery or mucoid discharge, no lid oedema to speak of, and it settles by around day five without treatment. The history of prophylaxis is the clue; if the timing or the severity do not fit, suspect an infective cause and swab. [1] [3]
Gonococcal ophthalmia neonatorum is sudden and dramatic, beginning on day two to five. The discharge is profuse, thick and hyperacute purulent — it literally reaccumulates minutes after wiping — with marked bilateral eyelid oedema and chemosis and a tense red eye. The danger is rapid corneal ulceration, seen as a grey infiltrate or crater, progressing to perforation and endophthalmitis. This is the cause you treat before the culture grows. [1] [12]
Chlamydial ophthalmia neonatorum comes on more insidiously at day five to fourteen. The discharge is mucopurulent, the lids are swollen, and a papillary reaction is seen on everting the lids; it is often bilateral and may be frankly haemorrhagic, which is a characteristic chlamydial sign. Ask specifically about a staccato cough — the same afebrile, repetitive cough of chlamydial pneumonia — because the eye may precede the chest by days or weeks. [6] [5]
Herpes simplex ophthalmia neonatorum can appear on any day, often in the first two weeks. Look for vesicles on the periocular skin or lid margin, a watery discharge, and — on fluorescein staining with a blue light — the branching dendritic corneal ulcer. Crucially, screen for systemic HSV: lethargy, poor feeding, temperature instability, seizures or vesicles elsewhere may mean the eye is the visible tip of central-nervous-system or disseminated disease. [7] [8]
Differential Diagnosis
Build the differential the way you built the classification — by onset window and discharge character — then strip out the non-infective mimics. [1]
The first mimic is congenital nasolacrimal duct obstruction, the classic "sticky eye" of infancy. The eye is white and quiet, there is no conjunctival injection, and the discharge is clear or mucoid reflux from a blocked duct that returns on pressure over the lacrimal sac — completely unlike the injected, purulent picture of infective ophthalmia neonatorum. The distinction matters: a blocked duct is managed conservatively, while infected discharge needs swabs and often systemic therapy. [1]
The second group is traumatic or mechanical. A corneal abrasion is fluorescein-positive in a distinct epithelial defect, often after instrumentation or a fingernail; a foreign body may be visible on the tarsal conjunctiva or cornea; and birth trauma can produce a subconjunctival haemorrhage that is alarming but benign. None of these have the profuse purulent discharge and lid oedema of gonococcal disease, but fluorescein staining is mandatory to separate a sterile abrasion from an infective keratitis. [1]
The practical pivot is this: use the day of life, the discharge type, the presence of vesicles or a staccato cough, and the maternal risk history to separate the chemical and self-limiting from the sight-threatening and systemic. When the discharge is profuse and purulent with lid oedema, do not entertain a blocked duct — act for gonococcus. [1] [12]
Clinical & Bedside Assessment
Start with the mother before the baby, because the perinatal history often holds the cause. Take a focused maternal and perinatal history: her sexually-transmitted-infection screening and its results, the mode of delivery, the duration of rupture of membranes, the type of ocular prophylaxis given at birth, and any maternal symptoms of cervical infection. A mother with untreated or incompletely treated gonorrhoea or chlamydia is the highest-risk scenario, and her results guide your empiric therapy. [3]
On examination, document the day of life and the exact timing of onset, the character and volume of the discharge (watery, mucoid, mucopurulent or profuse purulent), the presence and degree of lid oedema and chemosis, any periocular vesicles, and the infant's systemic wellbeing — feeding, temperature and respiratory signs. Evert the lids to look for papillae or a hidden foreign body. The combination of day three, profuse pus and tense lid oedema should make you act for gonorrhoea on the spot. [1] [12]
Perform fluorescein staining with a blue light at every neonatal red eye. It reveals a corneal defect, ulcer or the dendritic pattern of HSV keratitis that you will miss with the naked eye, and it is the single bedside test that distinguishes a surface abrasion from an infective keratitis. Assess the red reflex and corneal clarity to exclude a separate sight-threatening problem, and examine the chest for the crackles and tachypnoea of evolving chlamydial pneumonia. [1] [7]
Then order the laboratory panel. Send conjunctival swabs for Gram stain and culture on chocolate and Thayer-Martin media for Neisseria gonorrhoeae, nucleic-acid-amplification testing for both Chlamydia trachomatis and Neisseria gonorrhoeae, and HSV PCR from conjunctival and throat swabs. Arrange maternal and partner sexually-transmitted-infection screening in parallel — the eye infection is a sentinel for untreated maternal disease, and the public-health response is part of the treatment. [3] [5]
Investigations
Any neonatal conjunctivitis beyond mild chemical irritation warrants swabs, because the cause is rarely certain clinically and the treatment is cause-specific and often systemic. [1]
For bacterial and gonococcal work-up, send Gram stain and culture including chocolate and Thayer-Martin media for Neisseria gonorrhoeae; the Gram stain may show gram-negative intracellular diplococci within neutrophils, allowing you to act before culture matures. Pair this with nucleic-acid-amplification testing for both Chlamydia trachomatis and Neisseria gonorrhoeae, which is more sensitive than culture for chlamydia and increasingly the diagnostic standard. [1] [5]
For herpes simplex, send HSV PCR from conjunctival and throat swabs. When systemic HSV is suspected — and any neonatal eye HSV should prompt that suspicion — add cerebrospinal-fluid PCR and liver-function tests, because isolated eye disease may be the first sign of central-nervous-system or disseminated infection. The eye finding is never managed in isolation in neonatal HSV. [7] [8]
For the cornea and the chest, use fluorescein staining at the bedside for ulceration and dendritic keratitis, and assess the infant systemically for the crackles, tachypnoea and staccato cough of chlamydial pneumonia. A chest radiograph showing diffuse interstitial infiltrates in a well, afebrile infant with an eye discharge clinches chlamydial pneumonitis and confirms that systemic therapy was the right call. [6] [5]
[3] [7]Management — Resuscitation
Gonococcal ophthalmia neonatorum is a sight-threatening emergency that can perforate the cornea within hours, so the resuscitation mindset is "act, then confirm". Admit the infant, take swabs, begin frequent saline eye irrigation to reduce the protease load on the cornea, and start systemic therapy without waiting for culture. [1] [11]
Treat confirmed or suspected gonococcal disease with a single dose of ceftriaxone 25 to 50 mg per kilogram intravenously or intramuscularly, not exceeding 250 mg, with frequent saline irrigation and urgent ophthalmology review. For the jaundiced or premature neonate, or one receiving calcium-containing intravenous fluids, use cefotaxime instead — ceftriaxone displaces bilirubin and forms calcium-ceftriaxone precipitates. Reserve a longer (7-day) course for disseminated gonococcal infection. [1] [4]
Treat suspected neonatal HSV eye disease as possible disseminated or central-nervous-system disease: give intravenous aciclovir with a topical antiviral under ophthalmology and infectious-diseases guidance, and evaluate the cerebrospinal fluid and systemic organs. Do not be reassured by a quiet-looking eye — the keratitis and the dissemination are treated in parallel. [7] [8]
The key principle is to separate resuscitation from definitive care. The chemical and mild bacterial forms need swabs and observation, whereas the cornea-threatening and systemic forms need immediate admission, irrigation and systemic therapy. The decision is made on the day of life and the discharge, not on the culture plate. [1] [3]
Management — Definitive & Stepwise
Once the cause is named, treatment is cause-specific and systemic — topical drops alone must never be the whole answer for gonococcal, chlamydial or HSV disease. [1]
Cause-specific systemic treatment of ophthalmia neonatorum
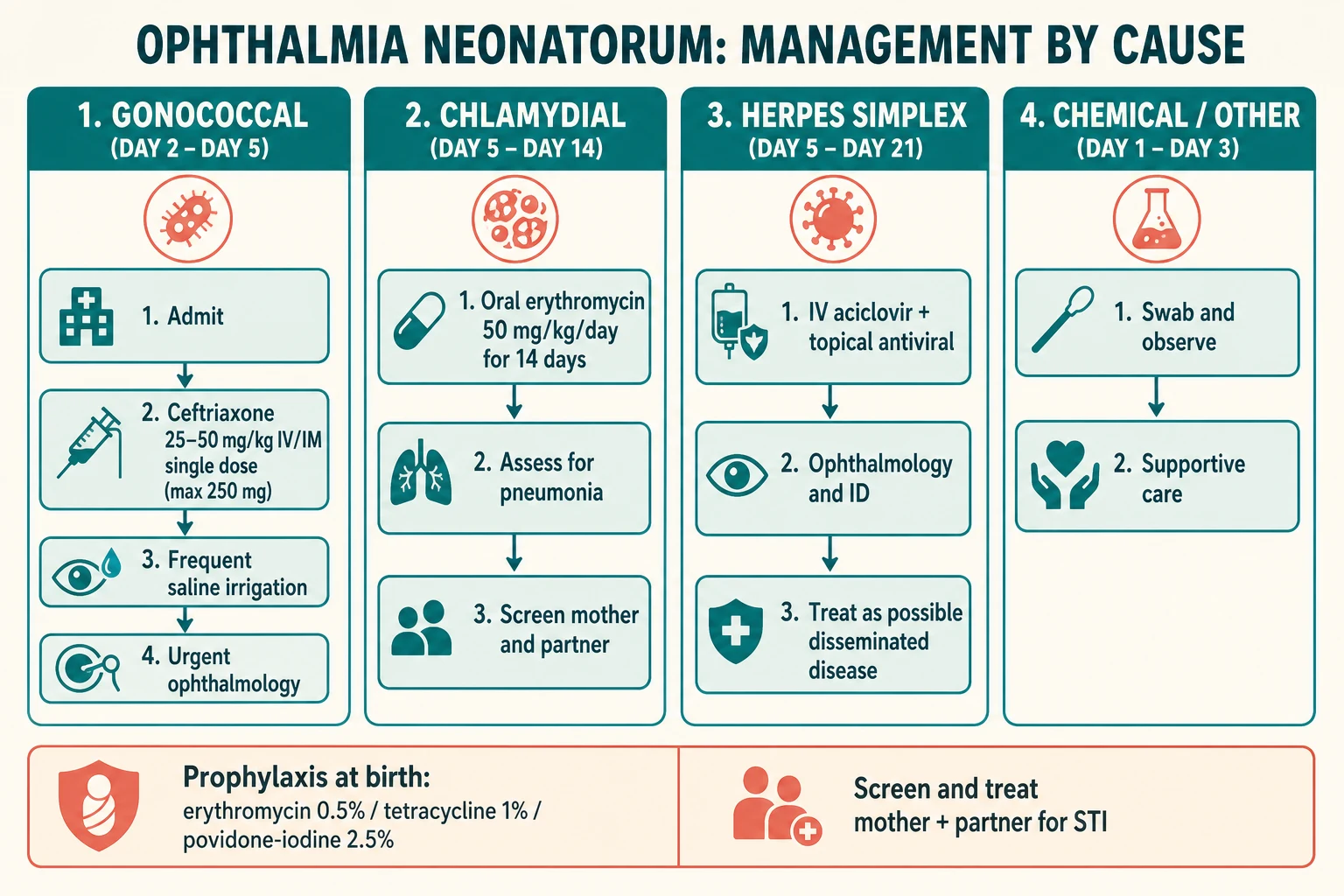
Gonococcal — single-dose ceftriaxone 25 to 50 mg/kg IV/IM (max 250 mg) or cefotaxime if jaundiced or premature, frequent saline irrigation, urgent ophthalmology, and maternal and partner treatment
Chlamydial — oral erythromycin 50 mg/kg/day in four divided doses for 14 days, assess for pneumonia, and screen and treat the mother and partner
Herpes simplex — intravenous aciclovir with topical antiviral, full systemic evaluation for CNS and disseminated disease, ophthalmology and infectious diseases
Chemical and other mild bacterial — supportive care, lid hygiene, observation and swabs; treat only confirmed symptomatic bacterial disease
For chlamydial ophthalmia neonatorum, give oral erythromycin 50 mg per kilogram per day in four divided doses for 14 days. A systematic review and meta-analysis confirmed high clinical and microbiological cure at this dose, though recurrence is appreciable and a repeat course is sometimes needed; azithromycin is a studied but less-established alternative. Erythromycin remains standard precisely because the systemic route eradicates nasopharyngeal carriage and prevents the pneumonia — a result topical drops cannot achieve. Counsel parents about the small association with infantile hypertrophic pyloric stenosis. [5] [6]
For gonococcal disease, give single-dose ceftriaxone (or cefotaxime) with frequent saline irrigation and urgent ophthalmology review, and arrange maternal and partner treatment. Rising gonococcal resistance threatens cephalosporin reliability, which is why current guidance is monitored closely and alternative agents remain under study — but cephalosporins remain first-line today. [11] [1]
For HSV disease, give intravenous aciclovir with a topical antiviral such as trifluridine or aciclovir ophthalmic ointment and a full systemic evaluation, and never apply topical steroid to a dendritic ulcer. For chemical and other mild bacterial causes, give supportive care, lid hygiene and observation with swabs, reserving topical antibiotics for confirmed symptomatic bacterial disease. [7] [8]
Erythromycin (chlamydial ophthalmia neonatorum)
Dose
50 mg/kg/day orally in 4 divided doses
Ceftriaxone (gonococcal ophthalmia neonatorum)
Dose
25 to 50 mg/kg IV or IM as a single dose (maximum 250 mg)
Specific Subtypes & Scenarios
The four scenarios below are the ones examiners reach for, because each forces a different decision under time pressure. [1]
Chemical conjunctivitis after prophylaxis is recognised by onset in the first 24 hours, a mild watery or mucoid discharge, and settling by around day five. Management is reassurance, observation and swabs only if any doubt exists about the timing or severity — the chief error is assuming chemical and missing an early gonococcal presentation. [1] [3]
A two-day-old with profuse purulent discharge and lid oedema is gonococcal ophthalmia neonatorum until proven otherwise. Admit, swab for Gram stain and culture, begin frequent saline irrigation, give single-dose ceftriaxone, request urgent ophthalmology review, and screen the mother and her partner. Do not wait for the culture to start treatment — the cornea may not survive the delay. [1] [12]
A ten-day-old with mucopurulent discharge and a staccato cough is chlamydial ophthalmia neonatorum with evolving pneumonia. Treat with oral erythromycin for 14 days, examine the chest and consider a radiograph, and screen and treat the mother and her partner. The eye will improve, but the point of the systemic course is the lung the topical drop could never reach. [6] [5]
A neonate with periocular vesicles and a dendritic ulcer is HSV keratoconjunctivitis. Give intravenous aciclovir with a topical antiviral, evaluate the cerebrospinal fluid and systemic organs for central-nervous-system and disseminated disease, and involve ophthalmology and infectious diseases. Never apply topical steroid until HSV is excluded. [7] [8]
Complications & Pitfalls
The cardinal pitfall is treating neonatal conjunctivitis with topical drops alone, which clears the eye in chlamydial and gonococcal disease but fails to eradicate nasopharyngeal carriage and systemic spread. The eye looks better; the pneumonia develops anyway. [6]
The sight-threatening complication is corneal ulceration and perforation from delayed gonococcal therapy — a grey infiltrate that cavitates into a full-thickness defect, endophthalmitis and permanent visual loss. This is the cost of waiting for culture instead of treating on suspicion, and it is why gonococcal ophthalmia is an emergency. [1] [11]
The systemic complications are chlamydial pneumonia — the afebrile, staccato-cough pneumonitis of four to twelve weeks of age — and neonatal HSV dissemination or central-nervous-system disease, both of which topical eye therapy cannot prevent. Missing HSV by attributing a red eye to simple conjunctivitis, when vesicles or a dendritic ulcer signal sight- and life-threatening systemic disease, is a recurrent and avoidable error. [6] [7]
Avoid ceftriaxone in the jaundiced or premature neonate or one on calcium-containing intravenous fluids, because of calcium-ceftriaxone precipitation and bilirubin displacement — use cefotaxime instead. Counsel parents on the small association between erythromycin and infantile hypertrophic pyloric stenosis, so that projectile vomiting in the following weeks is recognised and investigated. [1] [5]
Prognosis & Disposition
With prompt cause-specific systemic therapy the prognosis is excellent for chlamydial and gonococcal disease — but it is conditional on speed. Delayed gonococcal therapy causes permanent corneal scarring and visual loss, and untreated neonatal HSV carries significant mortality and long-term neurodevelopmental morbidity. [1] [7]
Discharge the well infant with chemical or treated chlamydial disease on completion of therapy, with a clear safety-net for fever, lethargy, poor feeding, worsening discharge or new respiratory signs. The parents must know that a chlamydial eye can recur and that a cough developing in the weeks ahead is the same organism — not a new infection. [6] [5]
Admit the neonate with gonococcal or suspected HSV disease for intravenous therapy, irrigation, ophthalmology review and systemic evaluation. Reinforce that recurrence of chlamydial disease after one erythromycin course is appreciable and may require a repeat course, and that the durable interventions are maternal screening, treatment and neonatal prophylaxis — not a stronger eye drop. [3] [7]
Special Populations
Neonates born to mothers with untreated or incompletely treated gonorrhoea or chlamydia carry the highest risk; ensure maternal screening results are available and treat the mother and her partner, because reinfection undoes the infant's cure. [3]
Premature and jaundiced neonates, and those receiving calcium-containing intravenous fluids, require cefotaxime rather than ceftriaxone because of calcium-ceftriaxone precipitation and bilirubin displacement. The premature infant's immature blood-brain barrier and reduced albumin binding make bilirubin displacement a genuine concern, not a theoretical one. [1]
Aboriginal and Torres Strait Islander, Maori, Pasifika, refugee, asylum-seeking and migrant families carry a disproportionate burden in settings of limited antenatal screening. Provide culturally safe care, trained interpreters, and treat the household and partner — the eye infection is a marker of untreated maternal infection and broader access gaps, not an isolated event. [3] [2]
Infants in resource-limited settings benefit from povidone-iodine 2.5% ocular prophylaxis at birth, a low-cost, effective alternative to antibiotic ointment that can be integrated into maternal and newborn care where the cost and cold-chain of erythromycin ointment are prohibitive. [9] [10]
Evidence, Guidelines & Regional Differences
The named regional guidance for treatment and prophylaxis is the CDC 2021 Sexually Transmitted Infections Treatment Guidelines, the AAP Red Book, the Canadian Paediatric Society statement, NICE CKS, and the USPSTF reaffirmation on ocular prophylaxis. In ANZ, the Royal Children's Hospital and eTG guidance is the practical reference. [3] [4]
The chlamydial treatment evidence is now strong: a systematic review and meta-analysis confirmed that oral erythromycin 50 mg per kilogram per day for 14 days achieves high clinical and microbiological cure in chlamydial ophthalmia neonatorum, with azithromycin a studied but less-established alternative and recurrence after a single course remaining appreciable. [5] [6]
There is an evolving controversy over the gonococcal regimen. Current guidance favours a single dose of ceftriaxone 25 to 50 mg per kilogram (maximum 250 mg) for gonococcal ophthalmia, while some older and international references describe once-daily dosing for up to 7 days, with a 7-day course reserved for disseminated disease. Rising gonococcal resistance threatens cephalosporin reliability, and alternative agents remain under active study — cephalosporins are first-line today, but the field is watched closely. [1] [11]
The prophylaxis controversy is clearer. Antibiotic ointment prevents gonococcal but not chlamydial ophthalmia, silver nitrate is obsolete because of chemical conjunctivis and limited chlamydial cover, povidone-iodine 2.5% is a low-cost effective alternative, and universal prophylaxis remains recommended while maternal screening is the deeper intervention. The USPSTF reaffirms grade B prophylaxis against gonococcal ophthalmia neonatorum; no prophylactic agent prevents chlamydia, which is why screening and treating the mother is the cornerstone. [3] [9] [10]
[3] [4]Exam Pearls
Ophthalmia neonatorum is conjunctivitis in the first 28 days, and the onset windows are the whole exam: chemical day 1, gonococcal day 2 to 5, chlamydial day 5 to 14 and HSV any day. [1]
Gonococcal ophthalmia is the sight-threatening emergency — profuse purulent discharge and lid oedema with corneal perforation within hours — treated with single-dose ceftriaxone 25 to 50 mg per kilogram (maximum 250 mg) or cefotaxime, plus saline irrigation and urgent ophthalmology. Chlamydial ophthalmia is the commonest cause and needs oral erythromycin 50 mg per kilogram per day for 14 days systemically, because topical therapy does not prevent the staccato afebrile pneumonia. [5] [11]
HSV ophthalmia needs intravenous aciclovir and topical antiviral, with evaluation for central-nervous-system and disseminated disease; never give topical steroid for a dendritic ulcer. Prophylaxis at birth — erythromycin or tetracycline ointment, or 2.5% povidone-iodine in resource-limited settings — prevents gonococcal but not chlamydial disease, so always screen and treat the mother and her partner. [7] [9]
References
- [1]Castro Ochoa KJ; Gurnani B Ophthalmia Neonatorum. StatPearls, 2026.PMID 31855399
- [2]Asiamah R; Owusu G; Amoako PT; et al Epidemiology of ophthalmia neonatorum: a systematic review and meta-analysis. BMC Pediatr, 2025.PMID 39810179
- [3]Moore DL; MacDonald NE; Canadian Paediatric Society Preventing ophthalmia neonatorum. Paediatr Child Health, 2015.PMID 25838784
- [4]Curry SJ; Krist AH; Owens DK; et al Ocular Prophylaxis for Gonococcal Ophthalmia Neonatorum: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA, 2019.PMID 30694327
- [5]Zikic A; Schunemann H; Wi T; et al Treatment of Neonatal Chlamydial Conjunctivitis: A Systematic Review and Meta-analysis. J Pediatric Infect Dis Soc, 2018.PMID 30007329
- [6]Zar HJ Neonatal chlamydial infections: prevention and treatment. Paediatr Drugs, 2005.PMID 15871630
- [7]Pinninti SG; Kimberlin DW Neonatal herpes simplex virus infections. Semin Perinatol, 2018.PMID 29544668
- [8]James SH; Kimberlin DW Neonatal herpes simplex virus infection: epidemiology and treatment. Clin Perinatol, 2015.PMID 25677996
- [9]Isenberg SJ; Apt L; Yoshimori R; et al Povidone-iodine for ophthalmia neonatorum prophylaxis. Am J Ophthalmol, 1994.PMID 7977595
- [10]Smith-Norowitz TA; Ukaegbu C; Kohlhoff S; Hammerschlag MR Neonatal prophylaxis with antibiotic containing ointments does not reduce incidence of chlamydial conjunctivitis in newborns. BMC Infect Dis, 2021.PMID 33731049
- [11]Belagal P Current alternative therapies for treating drug-resistant Neisseria gonorrhoeae causing ophthalmia neonatorum. Future Microbiol, 2024.PMID 38512111
- [12]Tan AK Ophthalmia Neonatorum. N Engl J Med, 2019.PMID 30625059