Paeds · ophthalmology
Ophthalmic manifestations of systemic disease
Also known as Eye signs of systemic disease · Uveitis in juvenile idiopathic arthritis · Diabetic retinopathy in children · Phakomatoses and the eye · Sickle cell retinopathy · Neurocutaneous ophthalmic signs · Ectopia lentis · Kayser-Fleischer ring · Xerophthalmia · Cherry-red spot
Fellowship guide to the ophthalmic manifestations of systemic disease in children. Covers the eye as the window to systemic disease, the sight-threatening uveitis of juvenile idiopathic arthritis and the ACR screening schedule, the microvascular retinopathy of type one diabetes, the proliferative sickle cell retinopathy, the neurocutaneous phakomatoses from the neurofibromatosis optic pathway glioma and the Lisch nodules through the tuberous sclerosis retinal hamartoma and the Sturge-Weber glaucoma and choroidal haemangioma, the congenital infections with the toxoplasmosis chorioretinitis, the vitamin A deficiency xerophthalmia, the Marfan ectopia lentis and the Wilson Kayser-Fleischer ring, the cherry-red spot of the storage disorders, and the red-flag recognition and the multidisciplinary referral.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old girl with the oligoarticular juvenile idiopathic arthritis runs into the clinic with a swollen knee and a smile, and she has no eye pain and no redness and no complaint about her vision. Behind that cheerful exterior, however, the low-grade inflammation of the anterior uvea may be scarring her eye in silence, depositing the band keratopathy on the cornea and the posterior synechiae across the pupil, and narrowing the angle toward the glaucoma. This is the central lesson of the ophthalmic manifestations of systemic disease: the eye declares the danger of a distant disease long before the child complains, and the paediatrician who screens the right child at the right interval saves the sight that the symptoms would have given away too late. The slit-lamp examination of the child with the juvenile arthritis is the prototype, and it sets the pattern for the whole topic. [1]
The eye shares its blood supply, its immune system, its connective tissue and its embryology with every other organ, and so the systemic diseases of childhood appear in the eye through several doors. The immune-mediated inflammation of the uvea follows the juvenile arthritis and the inflammatory bowel disease. The microvascular injury of the retinal capillary follows the diabetes and the sickle cell disease. The developmental tumour and the hamartoma follow the neurocutaneous phakomatoses. The congenital infection seeds the retina, the metabolic disorder deposits the substrate, the nutritional deficiency depletes the tissue, and the connective tissue disorder displaces the lens. The candidate who holds these mechanisms together is the candidate who can predict which systemic disease will appear in which part of the eye. [4][9]
The clinical weight of the topic rests on two pillars, and the examination rewards the candidate who holds both. The first is the screening of the asymptomatic child at risk, because the sight-threatening uveitis of the juvenile arthritis and the early retinopathy of the diabetes are silent, and the screening schedule is the only safeguard against the irreversible blindness. The second is the recognition of the red-flag sign in the child who is already known to carry a systemic disease, because the optic pathway glioma of the neurofibromatosis, the glaucoma of the Sturge-Weber and the xerophthalmia of the vitamin A deficiency declare themselves through the eye, and the same-day ophthalmology referral is the non-negotiable step. The fellow who can name the screening interval and the red flag carries the whole topic. [1][6]
Classification
The clinician who meets the child with a systemic disease and an eye finding organises the problem along two practical axes, and the examination rewards the candidate who can hold both. The first axis is the organ system that drives the disease, because the rheumatology, the endocrinology, the haematology, the neurocutaneous, the infectious and the metabolic diseases each carry a characteristic ocular signature. The second axis is the mechanism by which the disease reaches the eye, because the immune-mediated inflammation, the microvascular injury, the developmental tumour, the direct infection and the substrate deposition each produce a recognisable lesion in a recognisable part of the eye. The candidate who can move from the eye finding to the mechanism and the system reasons the topic rather than memorising the list. [1][4]
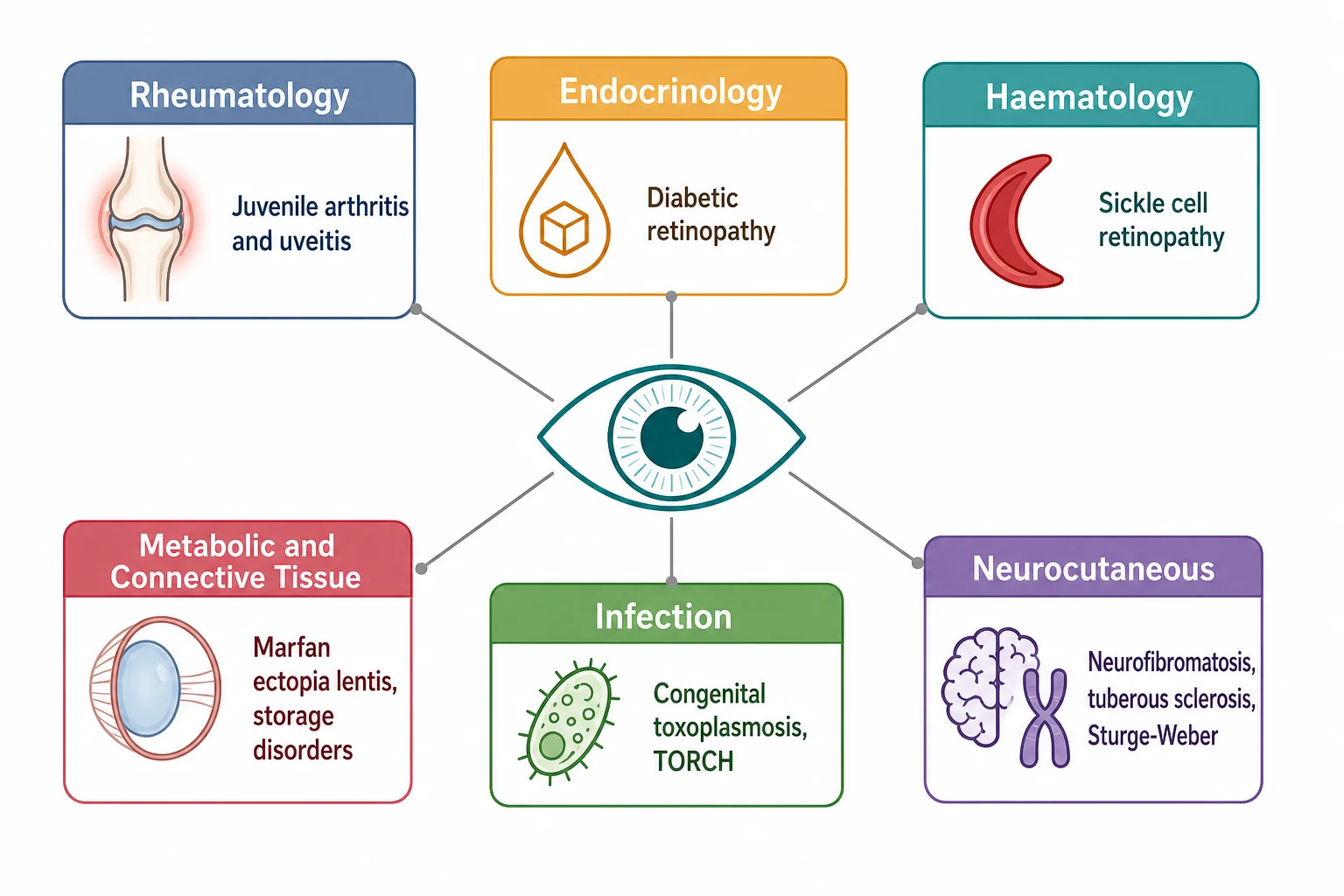
The rheumatology door opens onto the chronic anterior uveitis of the juvenile idiopathic arthritis, and it is the single most important ocular manifestation of any systemic disease in childhood, because it is common, it is silent and it is blinding. The endocrinology door opens onto the diabetic retinopathy of the type one diabetes, the cataract of the poorly controlled diabetes and the rare thyroid eye disease. The haematology door opens onto the proliferative retinopathy of the sickle cell disease, with the sea-fan neovascularisation and the risk of the vitreous haemorrhage and the retinal detachment. The neurocutaneous door opens onto the phakomatoses, with the optic pathway glioma and the Lisch nodules of the neurofibromatosis, the retinal hamartoma of the tuberous sclerosis and the glaucoma and the choroidal haemangioma of the Sturge-Weber. [1][7][4]
The infectious and the metabolic doors complete the picture, and the examination rewards the candidate who can name the lesion. The congenital infection seeds the retina with the pigmented chorioretinal scar of the toxoplasmosis and the salt-and-pepper retinopathy and the cataract of the congenital rubella. The metabolic door deposits the substrate in the cornea and the retina, with the Kayser-Fleischer ring of the Wilson disease at the limbus, the corneal clouding of the mucopolysaccharidoses, the cherry-red spot of the Tay-Sachs and the Niemann-Pick in the macula, and the superotemporal ectopia lentis of the Marfan syndrome. The nutritional door depletes the tissue, with the night blindness and the Bitot spots and the keratomalacia of the vitamin A deficiency that remains the leading cause of the preventable childhood blindness across the world. [3][8][9]
Rheumatology
immune-mediated
- Juvenile idiopathic arthritis chronic anterior uveitis
- Inflammatory bowel disease episcleritis and uveitis
- Slit-lamp screening every three months for the high-risk child
- Topical steroid, methotrexate, adalimumab
Endocrinology
microvascular
- Type one diabetes retinopathy
- Diabetic cataract in poor control
- Annual retinal screening from age eleven after two to five years
- Tight glycaemic control prevents the progression
Haematology
vasculopathy
- Sickle cell proliferative retinopathy
- Sea-fan neovascularisation and vitreous haemorrhage
- Annual dilated fundus exam from age ten
- Laser for the high-risk neovascularisation
Neurocutaneous
hamartoma
- Neurofibromatosis optic pathway glioma and Lisch nodules
- Tuberous sclerosis retinal hamartoma
- Sturge-Weber glaucoma and choroidal haemangioma
- Annual review and the urgent imaging
Epidemiology & Risk Factors
The epidemiology of the ophthalmic manifestations of systemic disease is the epidemiology of the underlying conditions, and the candidate who knows which child is at risk knows whom to screen. The juvenile idiopathic arthritis is the commonest rheumatological disease of childhood, and the chronic anterior uveitis develops in roughly one in six of the children with the disease, yet it carries no eye symptom in the majority. The risk concentrates in the child with the oligoarticular disease, the positive antinuclear antibody, the young age of onset under seven years and the short disease duration under four years, and the ACR guideline of twenty-nineteen builds the screening schedule around exactly these four risk factors. [1]
The type one diabetes is the commonest metabolic disease of childhood, and the diabetic retinopathy is the leading cause of the new-onset blindness in the working-age adult, because the retinopathy that begins in adolescence matures into the sight-threatening disease of the early adulthood. The risk rises with the duration of the diabetes and the quality of the glycaemic control, and the retinopathy is rare before five years of duration but rises steeply through the teenage years, which is why the screening begins at age eleven after two to five years of the disease. The sickle cell disease carries the proliferative retinopathy in roughly a third of the adolescents and the young adults, and the risk is higher in the HbSC and the HbS-beta-thalassaemia genotypes than in the HbSS disease, which is the counter-intuitive fact the boards probe. [2][7]
The neurocutaneous phakomatoses carry the ocular risk in proportion to their population frequency, and the neurofibromatosis type one is the commonest, at one in three thousand. The optic pathway glioma develops in roughly fifteen percent of the children with the neurofibromatosis, and it is the commonest central nervous system tumour of the disease, while the Lisch nodules of the iris accumulate with the age until they are present in nearly all the adults. The tuberous sclerosis carries the retinal hamartoma, and the Sturge-Weber syndrome carries the ipsilateral glaucoma and the diffuse choroidal haemangioma that threaten the sight of the eye on the side of the facial port-wine stain. The vitamin A deficiency drives the global burden of the childhood blindness, and it concentrates in the regions of the malnutrition, the malabsorption and the measles, where the xerophthalmia progresses to the corneal melting within the days. [4][3][6]
Pathophysiology
The pathophysiology of the ocular manifestations rests on the shared anatomy of the eye and the body, and the candidate who understands the four mechanisms reasons the whole topic. The first mechanism is the immune-mediated inflammation, in which the systemic autoimmunity recruits the lymphocytes and the cytokines into the uveal tract, and the chronic low-grade inflammation of the anterior chamber deposits the cells and the flare, the keratic precipitates and the posterior synechiae. The juvenile idiopathic arthritis drives this mechanism through the antinuclear-antibody-positive immune complex deposition, and the inflammatory bowel disease drives it through the shared mucosal and the ocular immunity. [1][10]
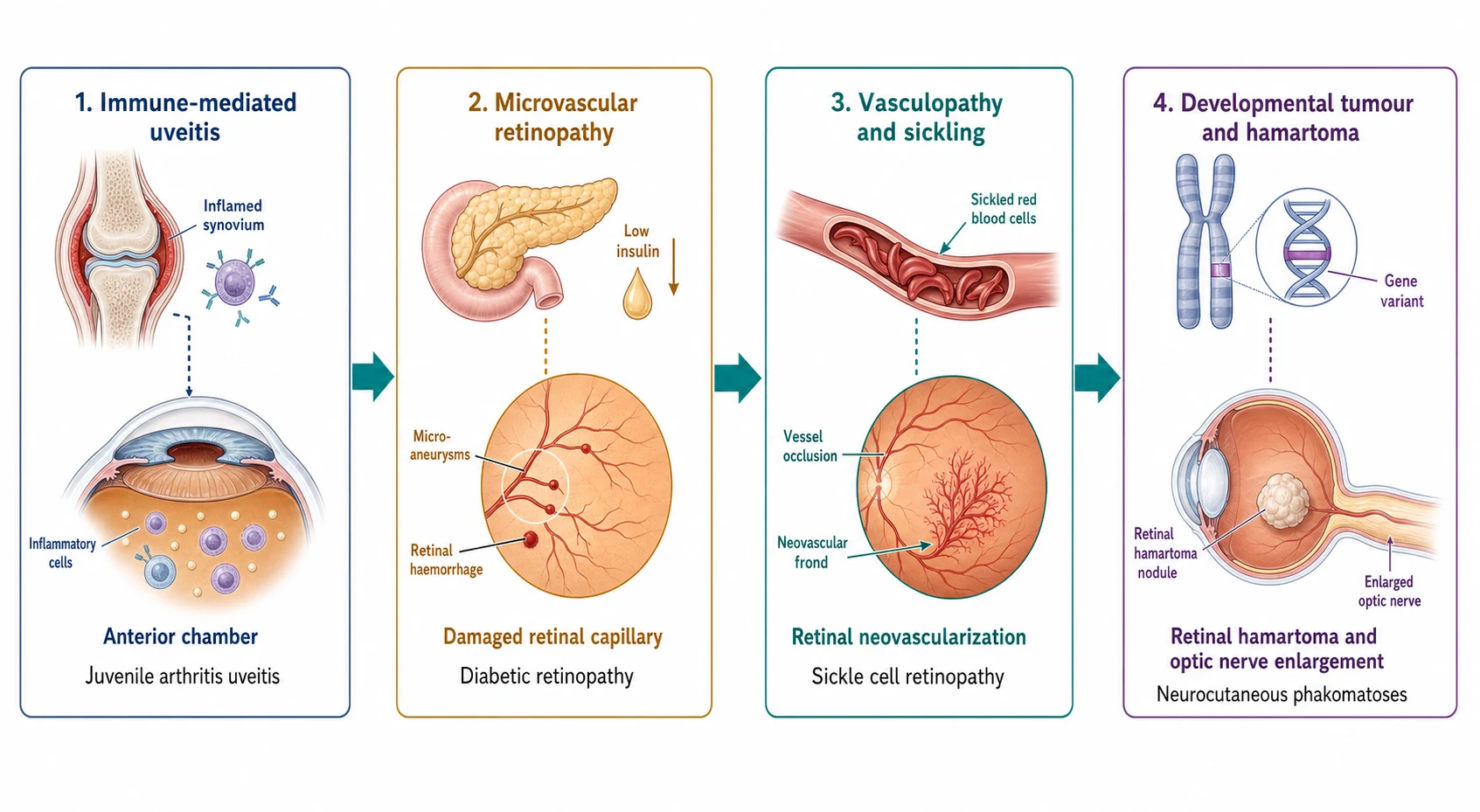
The second mechanism is the microvascular injury, and it dominates the diabetes and the sickle cell disease. The chronic hyperglycaemia of the diabetes damages the retinal pericyte through the polyol pathway and the advanced glycation, the capillary weakens and the microaneurysm forms, and the ischaemia drives the vascular endothelial growth factor that produces the neovascularisation of the proliferative retinopathy. The sickle haemoglobin polymerises in the low-oxygen sludge of the retinal periphery, the red cell sickles and adheres to the endothelium, the vessel occludes and the ischaemia drives the sea-fan neovascularisation that bleeds into the vitreous and pulls on the retina. The third mechanism is the developmental tumour and the hamartoma of the neurocutaneous syndromes, in which the germline mutation of the tumour suppressor or the growth pathway produces the optic pathway glioma of the neurofibromatosis, the retinal astrocytic hamartoma of the tuberous sclerosis and the choroidal and the leptomeningeal angioma of the Sturge-Weber. [2][7][5]
The fourth and the fifth mechanisms are the substrate deposition and the nutritional depletion, and they complete the picture. The metabolic storage disorders deposit the undegraded substrate in the tissue of the eye. The copper of the Wilson disease accumulates in the Descemet membrane at the limbus to form the Kayser-Fleischer ring. The glycosaminoglycan of the mucopolysaccharidoses clouds the corneal stroma, and the ganglioside of the Tay-Sachs and the sphingomyelin of the Niemann-Pick swell the ganglion cells around the macula and leave the cherry-red spot where the retina is thinnest. The connective tissue disorders displace the lens, and the fibrillin defect of the Marfan syndrome disrupts the zonular suspension and allows the lens to dislocate upward and outward. The vitamin A deficiency depletes the retinal photoreceptor and the conjunctival epithelium. The rod function fails first and the night blindness appears, the conjunctiva dries into the Bitot spot, and the cornea melts through the keratomalacia. The candidate who links the lesion to the mechanism carries the reasoning the boards reward. [3][9][8]
Clinical Presentation
The clinical presentation of the ocular manifestation depends on the disease and the part of the eye it attacks, and the examination probes the candidate who can name the sign and link it to the system. The chronic anterior uveitis of the juvenile arthritis presents with no symptom at all in the majority of the children, which is the single most important fact of the topic, because the silent inflammation scars the eye while the child plays. When the uveitis declares itself, it presents with the pain, the redness, the photophobia and the blurred vision of the acute flare, and the chronic complications of the band keratopathy, the cataract, the posterior synechiae and the glaucoma follow the untreated disease. [1]
The neurocutaneous signs are the ones the boards probe for the pattern recognition. The neurofibromatosis type one presents with the reduced visual acuity, the proptosis or the precocious puberty of the optic pathway glioma, with the Lisch nodules of the iris and the sphenoid wing dysplasia, and with the cafe-au-lait patches and the axillary freckling of the skin. The tuberous sclerosis presents with the retinal astrocytic hamartoma beside the epilepsy, the developmental delay and the ash-leaf macules and the adenoma sebaceum of the skin. The Sturge-Weber syndrome presents with the facial port-wine stain in the ophthalmic division of the trigeminal nerve, the ipsilateral leptomeningeal angioma with the seizures and the hemiparesis, and the glaucoma and the diffuse choroidal haemangioma of the eye on the side of the stain. [4][5][6]
The metabolic and the connective tissue signs present through the characteristic lesion. The Kayser-Fleischer ring of the Wilson disease is the brown-green copper deposit in the Descemet membrane at the limbus, and it accompanies the hepatitis and the movement disorder of the copper accumulation. The ectopia lentis of the Marfan syndrome is the superotemporal dislocation of the lens, and it accompanies the tall stature, the arachnodactyly and the aortic root dilatation. The cherry-red spot is the red macula surrounded by the pale swollen retina of the ganglioside storage, and it accompanies the developmental regression and the startle response of the Tay-Sachs. The night blindness and the Bitot spots and the corneal xerosis of the vitamin A deficiency present in the child with the malnutrition, the malabsorption or the recent measles, and the keratomalacia may follow within the days. [9][3][8]
Differential Diagnosis
The differential diagnosis of the ocular manifestation of systemic disease works by the lesion, and the candidate who can walk through the cause of a given finding demonstrates the breadth the examination rewards. The cause of the chronic anterior uveitis in the child is the juvenile idiopathic arthritis in the majority, but the differential includes the sarcoidosis, the Behcet disease, the HLA-B27-associated uveitis, the postinfectious uveitis and the tubulointerstitial nephritis with the uveitis. The cause of the chorioretinal scar is the congenital toxoplasmosis in the majority of the pigmented macular scar, but the differential includes the cytomegalovirus, the rubella and the lymphocytic choriomeningitis of the congenital infections. [1][8]
The cause of the retinal neovascularisation is the diabetic retinopathy and the sickle cell retinopathy in the child with the systemic disease. The differential includes the retinopathy of prematurity, the Coats disease, the familial exudative vitreoretinopathy and the Eales disease. The distinction rests on the history of the systemic disease and the pattern of the vascular change. The cause of the optic disc swelling is the raised intracranial pressure of the idiopathic intracranial hypertension, the optic pathway glioma of the neurofibromatosis, the papilloedema of the meningoencephalitis and the inflammation of the optic neuritis. The distinction rests on the acuity, the visual acuity and the imaging. The cause of the red eye is the uveitis in the child with the arthritis, the episcleritis in the child with the inflammatory bowel disease, and the conjunctivitis and the trauma in the child without the systemic disease. [7][4][10]
The cause of the lens dislocation is the Marfan syndrome with the superotemporal displacement, but the differential includes the homocystinuria with the inferonasal displacement, the Weill-Marchesani syndrome with the microspherophakia, the sulfite oxidase deficiency and the ectopia lentis et pupillae, and the direction of the dislocation is the high-yield discriminator the boards probe. The cause of the cherry-red spot is the Tay-Sachs and the Sandhoff of the gangliosidoses, but the differential includes the Niemann-Pick, the Gaucher, the sialidosis, the metachromatic leukodystrophy and the GM1 gangliosidosis. The candidate who can move from the lesion to the shortlist and back to the systemic disease reasons the differential the way the boards reward. [9]
Clinical & Bedside Assessment
The bedside assessment of the child with a systemic disease and a suspected ocular manifestation begins with the visual acuity, because the reduced acuity is the red flag that crosses every disease. The age-appropriate acuity is measured with the preferential looking in the preverbal child, the picture or the letter matching in the preschool child, and the Snellen or the logMAR chart in the school-age child, and any asymmetry or any fall from the baseline is investigated. The red reflex test in the dim room with the direct ophthalmoscope screens for the media opacity, the cataract and the retinoblastoma. The external examination seeks the port-wine stain of the Sturge-Weber, the cafe-au-lait patches of the neurofibromatosis and the ash-leaf macules of the tuberous sclerosis. [4][6]
The slit-lamp examination is the cornerstone of the screening of the chronic anterior uveitis, and it is the skill the boards reward the candidate who describes. The slit-lamp detects the cells and the flare of the anterior chamber inflammation, the keratic precipitates on the corneal endothelium, the posterior synechiae between the iris and the lens, the band keratopathy of the chronic disease and the cataract. The ACR guideline grades the uveitis by the number of the cells in the high-power field, from the inactive zero cells through the mild, the moderate and the severe, and the grade drives the treatment intensity. The intraocular pressure is measured, because the uveitis and the steroid both raise the pressure and the glaucoma is the complication. [1]
The dilated fundus examination completes the assessment, and it is performed by the ophthalmologist with the indirect ophthalmoscopy after the dilation of the pupil. The fundus examination seeks the microaneurysm and the haemorrhage of the diabetic retinopathy, the sea-fan neovascularisation of the sickle cell retinopathy, the pigmented scar of the congenital toxoplasmosis, the retinal hamartoma of the tuberous sclerosis and the swollen or the pale optic disc of the optic pathway glioma. The general examination is the third pillar, because the ocular finding is the window to the systemic disease: the joints for the arthritis, the skin for the neurocutaneous, the abdomen for the hepatosplenomegaly of the storage, the growth for the endocrine and the neurology for the Wilson and the phakomatoses. [7][5][9]
Investigations
The investigation of the ocular manifestation of systemic disease is built around the slit-lamp, the dilated fundus, the imaging and the laboratory, and the biopsy is rare. The slit-lamp biomicroscopy is the first-line investigation of the anterior uveitis, and it is repeated at the screening interval to detect the silent inflammation before it scars the eye. The optical coherence tomography measures the macular oedema of the uveitis and the retinopathy, and the fundus photography documents the retinopathy for the serial comparison. The fluorescein angiography maps the ischaemia and the leakage of the diabetic and the sickle retinopathy, and it guides the laser. [1][2]
The imaging of the optic pathway glioma of the neurofibromatosis is the magnetic resonance imaging of the orbits and the brain, and it defines the optic nerve, the chiasm and the hypothalamic tumour that threatens the vision and the endocrine axis. The magnetic resonance imaging also images the leptomeningeal angioma and the cortical calcification of the Sturge-Weber. The ultrasound of the eye images the choroidal haemangioma of the Sturge-Weber and the retinal detachment of the sickle cell disease. The laboratory investigation confirms the systemic disease: the antinuclear antibody for the juvenile arthritis uveitis risk, the haemoglobin electrophoresis for the sickle cell disease, the caeruloplasmin and the urinary copper for the Wilson disease, and the genetic testing for the Marfan and the phakomatoses. [4][6][9]
The serology and the molecular testing define the congenital infection, and the toxoplasma immunoglobulin and the polymerase chain reaction confirm the congenital toxoplasmosis that produced the chorioretinal scar. The vitamin A level confirms the deficiency behind the xerophthalmia, and the dietary and the malabsorption assessment defines the cause. The paediatrician orders the systemic investigations, while the ophthalmologist owns the slit-lamp, the dilated fundus and the ocular imaging, and the two work together in the multidisciplinary pathway. [8][3]
Management — Resuscitation
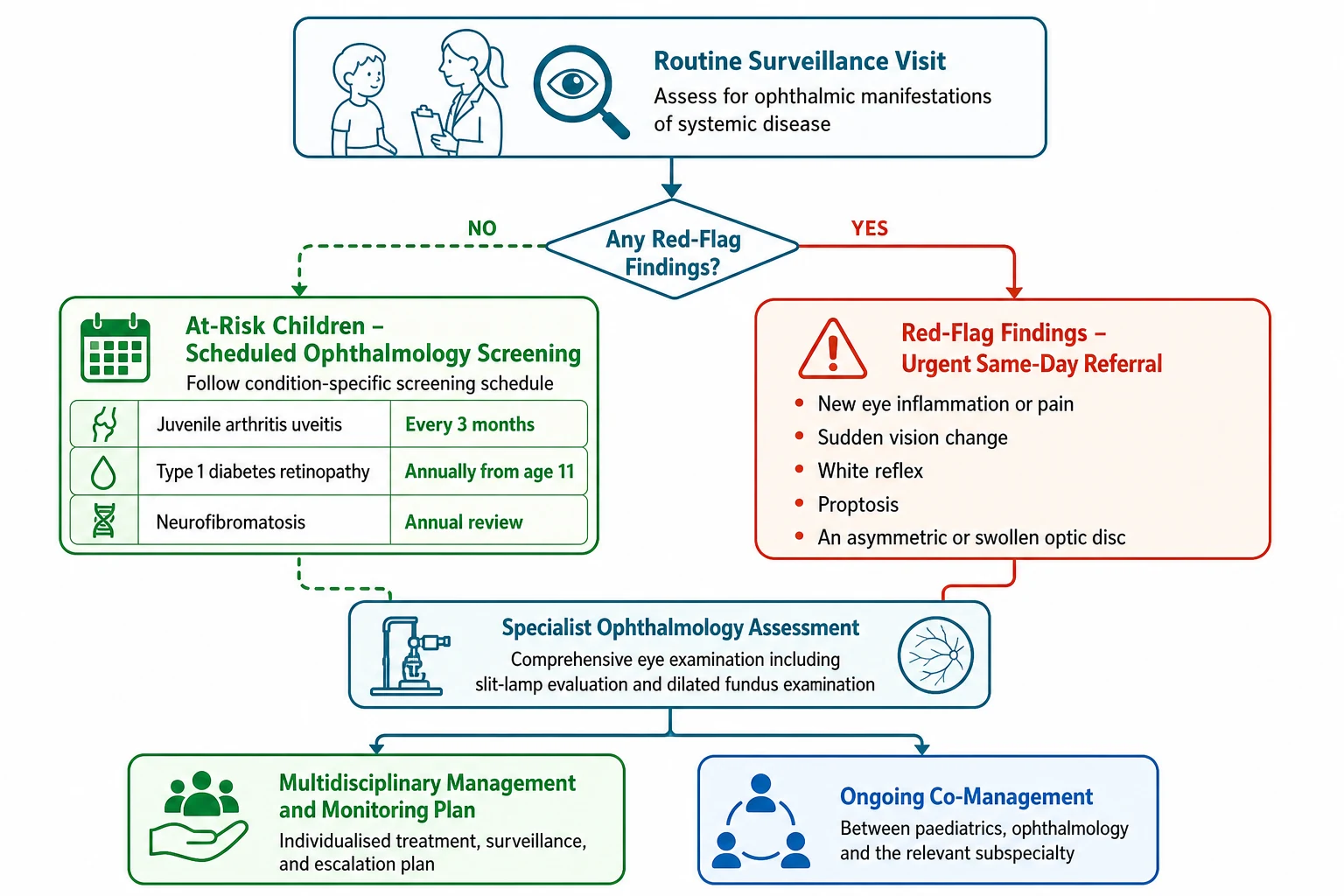
The resuscitation of the ocular manifestation of systemic disease is governed by the principle that the dangerous element is the delayed referral, and the management begins with the recognition of the red flag. The child with a known systemic disease who develops the sudden loss of vision, the new proptosis, the abnormal red reflex, the swollen optic disc or the painful red eye is referred the same day to the ophthalmology service. The optic pathway glioma, the acute uveitis, the retinal detachment and the keratomalacia all progress within the days. The child with the suspected raised intracranial pressure of the optic pathway glioma or the Sturge-Weber is imaged urgently and managed with the neurology and the neurosurgery. [4][6]
The child with the acute flare of the uveitis is managed with the topical corticosteroid and the cycloplegic to break the inflammation and to prevent the synechiae, and the ophthalmology is involved the same day. The child with the vitreous haemorrhage of the sickle cell retinopathy is managed with the rest, the elevation and the ophthalmology referral for the laser or the surgery. The child with the keratomalacia of the vitamin A deficiency is the emergency of the global child health, and the high-dose vitamin A is given immediately, because the cornea may perforate within the days. The child with the acute vision loss and the systemic disease is never reassured and sent home, because the delay costs the sight. [1][3][7]
The urgent pathway for the ocular red flag in the child with systemic disease
Recognise the red flag: the reduced vision, the proptosis, the abnormal red reflex, the swollen disc or the painful red eye
Any of these in a child with a known systemic disease is the emergency
Refer the child the same day to the ophthalmology service
Do not wait for the routine appointment, because the optic pathway glioma, the uveitis and the keratomalacia progress within the days
The ophthalmology service performs the slit-lamp, the dilated fundus and the urgent imaging
The magnetic resonance imaging defines the optic pathway glioma and the Sturge-Weber angioma
Initiate the disease-specific treatment
The topical steroid for the uveitis, the vitamin A for the xerophthalmia, the laser for the retinopathy, the imaging-guided pathway for the glioma
Coordinate the multidisciplinary care
The ophthalmology, the rheumatology, the endocrinology, the haematology, the neurology and the genetics as the disease demands
Management — Definitive & Stepwise
[1] [4]The definitive management begins with the screening of the asymptomatic child, and the prototype is the juvenile idiopathic arthritis uveitis schedule of the ACR guideline of twenty-nineteen. The high-risk child with the oligoarticular or the polyarticular rheumatoid-factor-negative disease, the positive antinuclear antibody, the onset under seven years and the duration under four years receives the slit-lamp screening every three months. As the risk factors fall away, the interval lengthens to every six months and then to every twelve months, and the screening continues for years after the arthritis remits, because the uveitis may flare in the quiet joint. The candidate who can recite the every-three-months interval for the high-risk child carries the single most testable fact of the topic. [1]
The treatment of the active chronic uveitis builds in the stepwise fashion the boards reward. The topical corticosteroid, the prednisolone acetate one percent, is the first line for the acute inflammation, and the cycloplegic prevents the posterior synechiae. The systemic treatment is added when the topical steroid fails to control the inflammation or when the steroid-induced glaucoma and cataract threaten the sight, and the ACR guideline strongly recommends the methotrexate as the first-line steroid-sparing agent. The biologic is added when the methotrexate fails, and the adalimumab, the anti-tumour-necrosis-factor monoclonal antibody, is the standard second-line, approved for the juvenile arthritis uveitis and proven to control the inflammation and to spare the steroid. [1]
Methotrexate for the chronic anterior uveitis of juvenile idiopathic arthritis
Dose
Ten to fifteen milligrams per square metre per dose once weekly in the child, up to a maximum of twenty-five to thirty milligrams per dose, titrated to the response and the tolerance, with the subcutaneous route preferred for the doses above the fifteen milligrams for the absorption
The screening and the management of the other systemic diseases follow the same principle of the asymptomatic screening and the red-flag referral. The diabetic retinopathy is screened with the annual dilated fundus examination or the retinal photography from age eleven after two to five years of the type one diabetes, with the earlier onset of the diabetes or the poor control prompting the earlier and the more frequent screening, and the tight glycaemic and blood-pressure control prevents the progression. The sickle cell retinopathy is screened with the annual dilated fundus examination from age ten, with the laser photocoagulation for the high-risk proliferative disease. The neurocutaneous phakomatoses receive the annual ophthalmology review, with the magnetic resonance imaging for the optic pathway glioma of the neurofibromatosis and the intraocular pressure for the glaucoma of the Sturge-Weber. [2][7][4]
The screening schedules across the systemic diseases
Specific Subtypes & Scenarios
The optic pathway glioma of the neurofibromatosis type one is the scenario the boards probe most directly, because it links the eye to the central nervous system and the endocrine axis. The optic pathway glioma is the low-grade pilocytic astrocytoma of the optic nerve, the chiasm and the hypothalamus, and it develops in roughly fifteen percent of the children with the neurofibromatosis. The presentation is the reduced vision, the proptosis, the precocious puberty or the new strabismus, and the surveillance magnetic resonance imaging is performed in the first years of life, because the glioma may grow silently before it compresses the visual pathway. Most of the gliomas are stable and observed, but the progressive or the sight-threatening glioma is treated with the chemotherapy, and the candidate who names the carboplatin and the vincristine demonstrates the depth the boards reward. [4]
The Sturge-Weber syndrome is the scenario of the port-wine stain and the glaucoma, and the ophthalmology is involved at the birth. The facial port-wine stain in the ophthalmic division of the trigeminal nerve carries the risk of the ipsilateral leptomeningeal angioma with the seizures and the hemiparesis, and the risk of the glaucoma and the diffuse choroidal haemangioma of the eye on the same side. The intraocular pressure is measured in the first weeks of life, because the congenital glaucoma of the Sturge-Weber presents with the buphthalmos, the corneal oedema and the tearing, and the early control preserves the vision. The choroidal haemangioma may cause the exudative retinal detachment later in the childhood, and the annual review continues through the adolescence. [6]
The high-risk child for the juvenile arthritis uveitis
The congenital toxoplasmosis is the scenario of the chorioretinal scar and the global child health, and it is the prototype of the congenital infection. The transplacental infection produces the triad of the chorioretinitis, the hydrocephalus and the intracranial calcification, and the pigmented chorioretinal scar sits in the macula and reduces the vision. The diagnosis rests on the maternal serology, the neonatal toxoplasma immunoglobulin and the polymerase chain reaction, and the treatment is the pyrimethamine, the sulfadiazine and the folinic acid in the first year of life. The child is monitored for the reactivation of the chorioretinitis through the childhood, because the parasite encysts in the retina and may reactivate years later. The vitamin A deficiency is the scenario of the global childhood blindness, and the night blindness is the earliest sign, the Bitot spot is the conjunctival sign, and the keratomalacia is the corneal melting that blinds within the days. [8][3]
Complications & Pitfalls
The complications of the ocular manifestations divide into the disease-related and the treatment-related, and the candidate who holds both together manages the child across the years. The disease-related complications are the blindness, the amblyopia, the cataract, the glaucoma and the retinal detachment. The chronic uveitis of the juvenile arthritis causes the band keratopathy, the cataract, the posterior synechiae and the secondary glaucoma, and the amblyopia follows the deprivation in the young child. The diabetic retinopathy progresses to the vitreous haemorrhage and the tractional retinal detachment, and the sickle retinopathy bleeds and detaches. The optic pathway glioma compresses the visual pathway and the hypothalamus, and the Sturge-Weber glaucoma blinds the eye. [1][4]
The treatment-related complications are the steroid toxicity and the late effects, and the late effects dominate the long-term management. The topical and the systemic corticosteroid of the uveitis cause the cataract and the glaucoma, and the methotrexate causes the myelosuppression and the hepatotoxicity. The laser of the retinopathy causes the visual field loss, and the surgery of the retinal detachment carries the risk of the proliferative vitreoretinopathy. The biologic of the uveitis carries the risk of the serious infection, and the cancer risk is monitored in the registries. The candidate who balances the control of the inflammation against the treatment toxicity reasons the management the way the boards reward. [1]
The classic diagnostic pitfalls are the ones the examiner probes, because they are the points where the sight is lost through the inattention. The asymptomatic child with the juvenile arthritis who is not screened for the uveitis loses the sight to the silent inflammation, because the slit-lamp is the only detection and the every-three-months schedule is the safeguard. The child with the neurofibromatosis whose reduced vision is attributed to the refractive error loses the sight to the unrecognised optic pathway glioma. The child with the Sturge-Weber whose glaucoma is missed in the newborn period loses the sight to the buphthalmos. The child with the malnutrition whose night blindness is dismissed loses the cornea to the keratomalacia. The candidate who names the screening schedule and the red flag avoids the pitfall. [1][6][3]
Prognosis & Disposition
The prognosis of the ocular manifestation of systemic disease depends on the disease, the timing of the detection and the quality of the treatment, and the prognosis is transformed by the screening. The juvenile arthritis uveitis carries a poor prognosis when it is detected late, because the silent inflammation scars the eye, but the screening and the early treatment preserve the vision in the majority of the children. The diabetic retinopathy carries the prognosis of the glycaemic control, because the tight control slows the progression and the laser prevents the blindness. The sickle retinopathy carries the prognosis of the genotype and the laser, and the optic pathway glioma carries the prognosis of the location and the growth. [1][2][7]
The disposition of the child is the co-management between the paediatrician and the ophthalmologist, because the systemic disease and the eye disease are managed together. The paediatrician owns the screening schedule and the systemic control, the ophthalmologist owns the slit-lamp and the dilated fundus and the ocular treatment, and the subspecialty owns the underlying disease. The child with the chronic uveitis is co-managed with the rheumatology, the child with the retinopathy with the endocrinology or the haematology, the child with the phakomatoses with the neurology and the genetics, and the child with the metabolic eye disease with the metabolic and the genetic services. The transition to the adult care is planned in the adolescence, because the ocular manifestations of the systemic disease persist into the adulthood. [4][9]
Special Populations
The indigenous and the remote populations carry the burden of the ocular manifestations of systemic disease, and the candidate who acknowledges the social determinants demonstrates the depth the boards reward. The trachoma and the vitamin A deficiency concentrate in the regions of the poverty and the remoteness, and the indigenous child with the malnutrition or the measles is at the risk of the xerophthalmia and the keratomalacia that the high-resource setting rarely sees. The sickle cell disease concentrates in the populations of the African and the Mediterranean ancestry, and the screening and the laser prevent the blindness that the untreated proliferative retinopathy causes. The access to the slit-lamp, the dilated fundus and the ophthalmology referral is the equity issue, because the remote child faces the delayed detection and the worse outcome. [3][7]
The child with the neurocutaneous or the metabolic syndrome is the patient in whom the lifelong surveillance transforms the outcome, because the ocular manifestations declare the disease and the complications across the years. The child with the neurofibromatosis receives the annual review for the optic pathway glioma through the childhood, and the child with the Marfan syndrome receives the annual ophthalmology review for the ectopia lentis and the retinal detachment alongside the cardiology review for the aortic root. The child with the complex chronic disease is the patient in whom the ophthalmology is one thread of the multidisciplinary care, and the candidate who coordinates the threads demonstrates the breadth the boards reward. [4][9]
The migrant and the refugee child and the child from the socioeconomic disadvantage face the barriers of the language, the cost and the access, and the screening schedules may be interrupted by the displacement. The telehealth and the outreach screening bring the slit-lamp and the retinal photography to the remote and the disadvantaged child, and the social work and the educational liaison support the family through the years of the surveillance. The candidate who links the ocular manifestation to the social determinant and the equity of the access reasons the special population the way the boards reward. [3][2]
Evidence, Guidelines & Regional Differences
The landmark evidence for the ophthalmic manifestations of systemic disease is the body of the guidelines and the trials that have refined the screening and the treatment. The ACR guideline of twenty-nineteen for the screening, the monitoring and the treatment of the juvenile idiopathic arthritis uveitis standardised the slit-lamp schedule around the four risk factors and established the methotrexate and the adalimumab as the stepwise treatment, and it is the evidence the boards reward the candidate who can cite. The International Society for Pediatric and Adolescent Diabetes and the national diabetes programmes refined the retinopathy screening from age eleven after two to five years of the disease, and the annual screening with the retinal photography transformed the early detection. [1][2]
The NHLBI guideline of twenty-fourteen for the sickle cell disease standardised the annual dilated fundus examination from age ten and the laser for the high-risk proliferative retinopathy, and it is the evidence that the boards reward the candidate who can cite. The International Tuberous Sclerosis Complex Criteria of twenty-twenty-one refined the diagnosis and the surveillance of the retinal hamartoma and the brain involvement. The Global Burden of Disease studies and the World Health Organization established the vitamin A deficiency as the leading cause of the preventable childhood blindness, and the high-dose vitamin A supplementation in the regions of the deficiency reduced the mortality and the blindness. [7][5][3]
The standard of care across the high-resource regions, including Australasia, the United Kingdom, the United States and Canada, is the protocol-based screening of the juvenile arthritis uveitis with the slit-lamp every three months for the high-risk child, the annual diabetic retinopathy screening from age eleven, and the annual neurocutaneous review. The ophthalmic manifestations of the sickle cell disease and the phakomatoses are co-managed with the haematology, the neurology and the genetics, and the metabolic eye disease with the metabolic and the genetic services. The regional differences concentrate in the access and the burden of the disease, with the vitamin A deficiency and the trachoma in the low-resource regions and the diabetic retinopathy rising in the regions of the rising childhood obesity and the type two diabetes.
[1][3]The controversies are the ones the candidate can discuss without pretending to resolve them. The optimal interval of the diabetic retinopathy screening, the role of the optical coherence tomography in the uveitis screening, the threshold for the laser in the sickle retinopathy, and the role of the screening magnetic resonance imaging in the neurofibromatosis are the open questions. The emerging treatments, including the sustained-release intraocular corticosteroid implants, the new biologics for the uveitis and the gene therapy for the inherited retinal and metabolic disease, are the directions the candidate may name. The precision medicine approaches, including the genotype-guided screening of the sickle retinopathy and the metabolic eye disease, are the future the boards reward the candidate who can anticipate. [1][7]
Exam Pearls
The high-yield facts for the examination are the ones the examiner probes and the candidate must carry without hesitation. The juvenile arthritis uveitis and the every-three-months slit-lamp for the high-risk child are the core, alongside the diabetic retinopathy screening from age eleven and the sickle retinopathy screening from age ten. The optic pathway glioma of the neurofibromatosis, the glaucoma of the Sturge-Weber, the Kayser-Fleischer ring of the Wilson, the ectopia lentis of the Marfan, the cherry-red spot of the storage disorders and the vitamin A deficiency as the leading preventable blindness complete the core. The candidate who carries the screening schedule and the red flag holds the whole topic. [1][3]
The direction of the lens dislocation is the high-yield discriminator the boards reward the candidate who knows: the Marfan syndrome dislocates the lens superotemporally, the upward and the outward, while the homocystinuria dislocates the lens inferonasally, the downward and the inward, and the Weill-Marchesani causes the microspherophakia. The location of the copper deposit is the discriminator of the Wilson disease: the Kayser-Fleischer ring sits in the Descemet membrane at the limbus, while the sunflower cataract sits in the anterior lens capsule. The candidate who pairs the sign with the lesion and the system carries the examination. [9]
References
- [1]Angeles-Han ST, Ringold S, Beukelman T, et al 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of Juvenile Idiopathic Arthritis-Associated Uveitis. Arthritis Care Res, 2019.PMID 31021540
- [2]Herskin CW, Olsen BS, Madsen M, et al Screening for retinopathy in children with type 1 diabetes in Denmark. Pediatr Diabetes, 2020.PMID 31618523
- [3]Singh V, West KP Jr Vitamin A deficiency and xerophthalmia among school-aged children in Southeastern Asia. Eur J Clin Nutr, 2004.PMID 15054414
- [4]Gutmann DH, Ferner RE, Listernick RH, et al Neurofibromatosis type 1. Nat Rev Dis Primers, 2017.PMID 28230061
- [5]Northrup H, Aronow ME, Bebin EM, et al Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations. Pediatr Neurol, 2021.PMID 34399110
- [6]Higueros E, Roe E, Granell E, et al Sturge-Weber Syndrome: A Review. Actas Dermo-Sifiliograficas, 2017.PMID 28126187
- [7]Yawn BP, Buchanan GR, Afenyi-Annan AN, et al Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA, 2014.PMID 25203083
- [8]Bollani L, Auriti C, Achille C, et al Congenital Toxoplasmosis: The State of the Art. Front Pediatr, 2022.PMID 35874584
- [9]Milewicz DM, Braverman AC, De Backer J, et al Marfan syndrome. Nat Rev Dis Primers, 2021.PMID 34475413
- [10]Rohani P, Abdollah Gorji F, Eshaghi M, et al Ocular Complications of Pediatric Inflammatory Bowel Disease: A Case Series From a Pediatric Tertiary Medical Center. Clin Pediatr, 2022.PMID 35152727