Paeds · ophthalmology
Paediatric eye examination and red-reflex assessment
Also known as Red-reflex test · Bruckner test · Leukocoria assessment · White pupil · Paediatric vision screening · Newborn eye examination · Photoscreening
Foundation topic on the paediatric eye examination and red-reflex assessment: how to perform and interpret the red-reflex (Bruckner) test at the bedside in a dim room at about 30 to 45 centimetres, the normal symmetric orange-red reflex and the four abnormal patterns (dull or absent from a media opacity, white or leukocoria, asymmetric from anisometropia or strabismus, and the darker normal variant of a pigmented fundus), the age-adapted vision assessment from newborn fixation through preferential-looking, LEA and HOTV symbols to Snellen acuity, the differential diagnosis of leukocoria led by retinoblastoma and congenital cataract, the joint AAP, AAO and AAPOS policy that the red reflex be checked at every well-child visit from the newborn period, the role of instrument-based photoscreening for preverbal children, and the non-negotiable rule that every abnormal red reflex needs urgent ophthalmology referral.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A baby is born with eyes that are structurally almost complete but functionally unfinished, and the first years of life are when the visual system either wires itself correctly or learns to see badly. The job of the clinician at every well-child visit is to confirm that light is entering clearly, that the two eyes are seeing roughly equally, and that nothing dangerous is growing or sitting in the visual axis. The red-reflex test does all three of these things in about ten seconds, which is why it sits at the centre of the paediatric eye examination. [4] [1]
The red reflex is the orange-red glow you see in a child's pupil when you shine a direct ophthalmoscope at it from a distance in a dim room. It is not the reflection off the surface of the eye — it is light that has passed through the clear cornea, the aqueous, the lens and the vitreous, bounced off the retina and the blood-rich choroid behind it, and travelled back out through the same clear media. Because the light has to make that round trip, the reflex tests the clarity of the whole visual axis at once. A clear reflex says the pathway is open; a changed reflex says something along the pathway is blocking, scattering or replacing the light. [4] [3]
Performed properly, the test is done on both eyes together so the two reflexes can be compared side by side. This simultaneous comparison is the Bruckner test, and it is the part that catches asymmetry from anisometropia or strabismus — one reflex looks subtly darker than the other because that eye is out of focus or turned. The comparison is the point, which is why examining one eye at a time defeats half the test. [4] [3]
The red-reflex test is a screening test, not a diagnostic one. It tells you that the visual axis is probably clear, or that it is probably not, but it does not name the lesion. An abnormal result is therefore an indication for urgent ophthalmology referral, where a dilated fundus examination, ultrasound and, in an uncooperative child, an examination under anaesthesia will make the diagnosis. Holding that distinction — screening finding, not diagnosis — protects both the child (who gets referred) and the family (whom you do not wrongly label). [4] [6]
Classification
Think of a red-reflex result in terms of what it tells you about the visual axis, because that is what decides the next step. A normal symmetric glow means the pathway is clear. A dull or absent glow means something is blocking the light. A white glow means something pale has replaced the red reflection. An asymmetric glow means one eye is out of focus or turned. Those four patterns are the whole game. [4] [3]
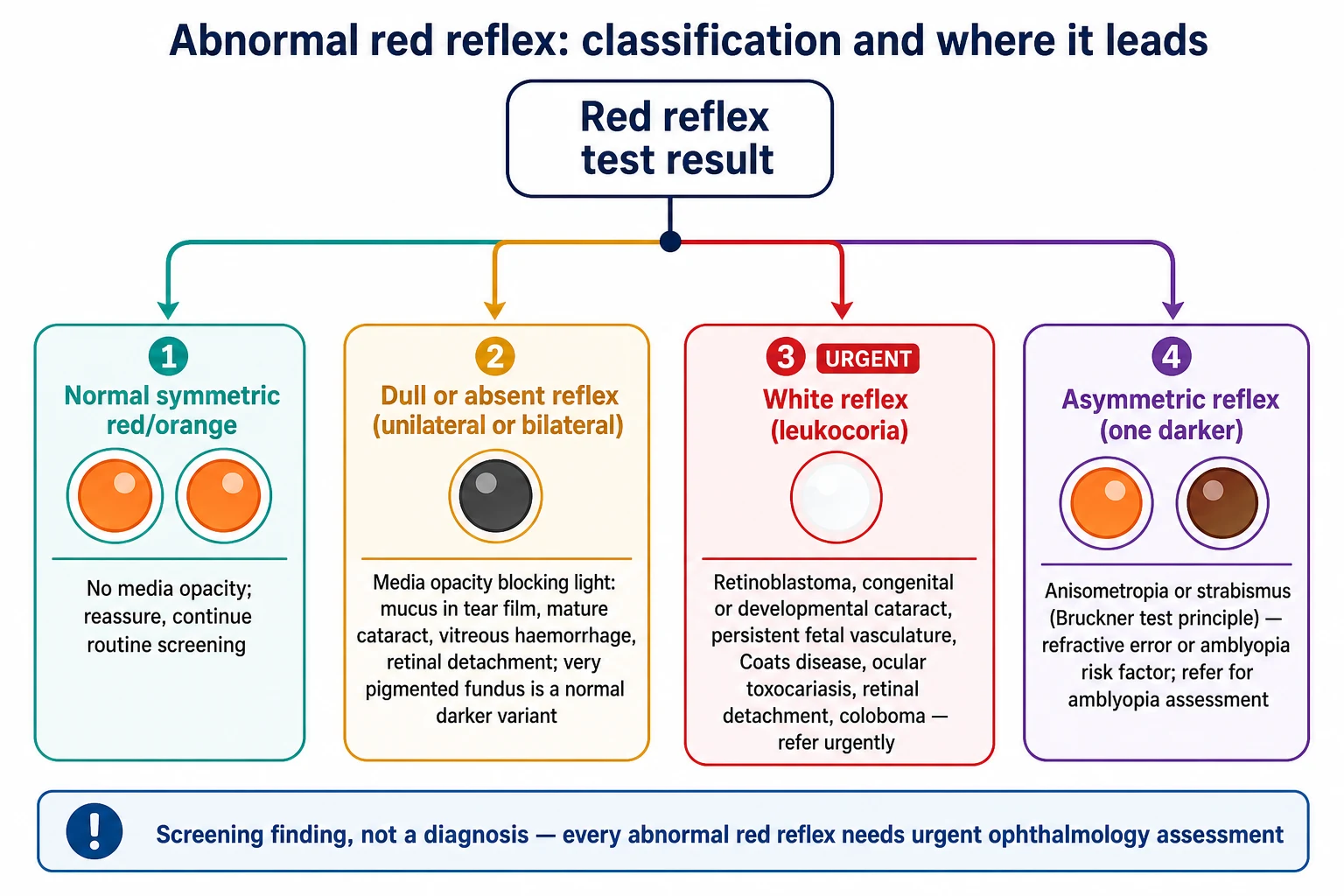
The normal reflex is a symmetric orange-red or reddish glow of equal brightness, colour and size in both pupils. It is present from the newborn period, though newborns with their small pupils and frequent lid closure can make it technically demanding. When you see it, document it and move on. [1] [4]
The dull or absent reflex is a darkening or loss of the glow, either in one eye or both. The mechanism is a media opacity absorbing or scattering the light on the way in or the way out — a mature cataract, a vitreous haemorrhage, inflammatory debris, or a retinal detachment sitting in the axis. Remember the one normal cause of a darker reflex: a heavily pigmented fundus, common in children of Asian, African or First Nations heritage, gives a darker, duskier but still present reflex, and it is symmetric. Compare the two eyes before you call it abnormal. [4] [3]
The white reflex — leukocoria, literally white pupil — is the finding that drives this whole topic. A pale lesion sits in the visual axis and reflects light back white, yellow-white or pink instead of letting it reach the choroid. The colour and pattern hint at the cause: a chalky white mass in retinoblastoma, a white lens in cataract, a fibrovascular stalk in persistent fetal vasculature, a yellow exudative detachment in Coats disease. A white reflex is an abnormal screening result, full stop, and it needs urgent ophthalmology referral. [3] [6]
The asymmetric reflex is the subtle one and the easiest to miss. One pupil glows back clearly red while the other is darker, because that eye is out of focus (anisometropia) or turned (strabismus). Either way it is an amblyopia risk factor, and the child needs ophthalmology referral for a refractive and motility assessment. This is the Bruckner principle in action: equal, symmetric, equally bright reflexes argue against a significant refractive asymmetry or a manifest squint. [4] [10]
Epidemiology & Risk Factors
The red-reflex test earns its place in every well-child visit because the conditions it catches are individually uncommon but collectively important, and several of them are time-critical. The joint policy of the American Academy of Pediatrics, the American Academy of Ophthalmology and the American Association for Pediatric Ophthalmology and Strabismus is that the test be performed at every well-child visit from the newborn period onward. [7] [4]
In the newborn, the test is cheap, fast and repeatable, and systematic review evidence supports its use as a screening tool. Sun and Ma reported the sensitivity and specificity of the red-reflex test in newborn eye screening, and the test performs well enough as a screen that it is a routine part of the newborn and discharge examination in most jurisdictions. A quality-improvement project in a level III neonatal intensive care unit showed that focused effort measurably increases the proportion of infants who are actually screened, which matters because premature and low-birth-weight infants carry extra eye risk. [1] [2] [5]
Among the causes of an abnormal reflex, two dominate the stakes. Retinoblastoma is the most common primary intraocular malignancy of childhood, and although it is rare it is the diagnosis that must never be missed because it can be fatal if it extends beyond the eye. Congenital or developmental cataract is among the most common causes of treatable leukocoria and a leading preventable cause of childhood blindness through amblyopia, because a dense infantile cataract must be operated on within weeks to preserve vision. [6] [11]
The amblyopia risk factors — significant refractive error, strabismus, a media opacity or an asymmetric reflex — are common, and most are invisible without screening. The reason early screening matters so much is the sensitive period: the visual cortex wires itself in the first few years of life, and if one eye sends a blurred image during that window, the brain learns to suppress it, producing amblyopia that becomes progressively harder to reverse. Eibschitz-Tsimhoni and colleagues showed that early screening for amblyogenic risk factors lowers both the prevalence and the severity of amblyopia, which is the evidence base for screening preverbal children before acuity can be tested. [9] [11]
Several factors raise the chance of a serious abnormality and should lower your threshold for careful testing and referral: a family history of retinoblastoma, congenital cataract or inherited eye disease; prematurity and low birth weight (retinopathy of prematurity); parental consanguinity; a syndrome such as Down, neurofibromatosis or tuberous sclerosis; and a parental report of an abnormal photograph or a child who does not seem to see well. None of these replaces the test, but each makes a borderline finding more worrying. [6] [3]
Pathophysiology
To use the red reflex well, picture the round trip the light makes. The ophthalmoscope beam enters the pupil and travels through the cornea, the aqueous humour in the anterior chamber, the lens, and the vitreous gel to reach the retina. It reflects off the retina and, more importantly, off the choroid — the densely vascular layer just behind the retina, rich in melanin and blood. That choroidal reflection is what gives the reflex its orange-red colour. The light then travels back out through the same clear media and reaches your eye. Clear media in, clear media out, red reflection in the middle: that is the normal reflex. [4] [3]
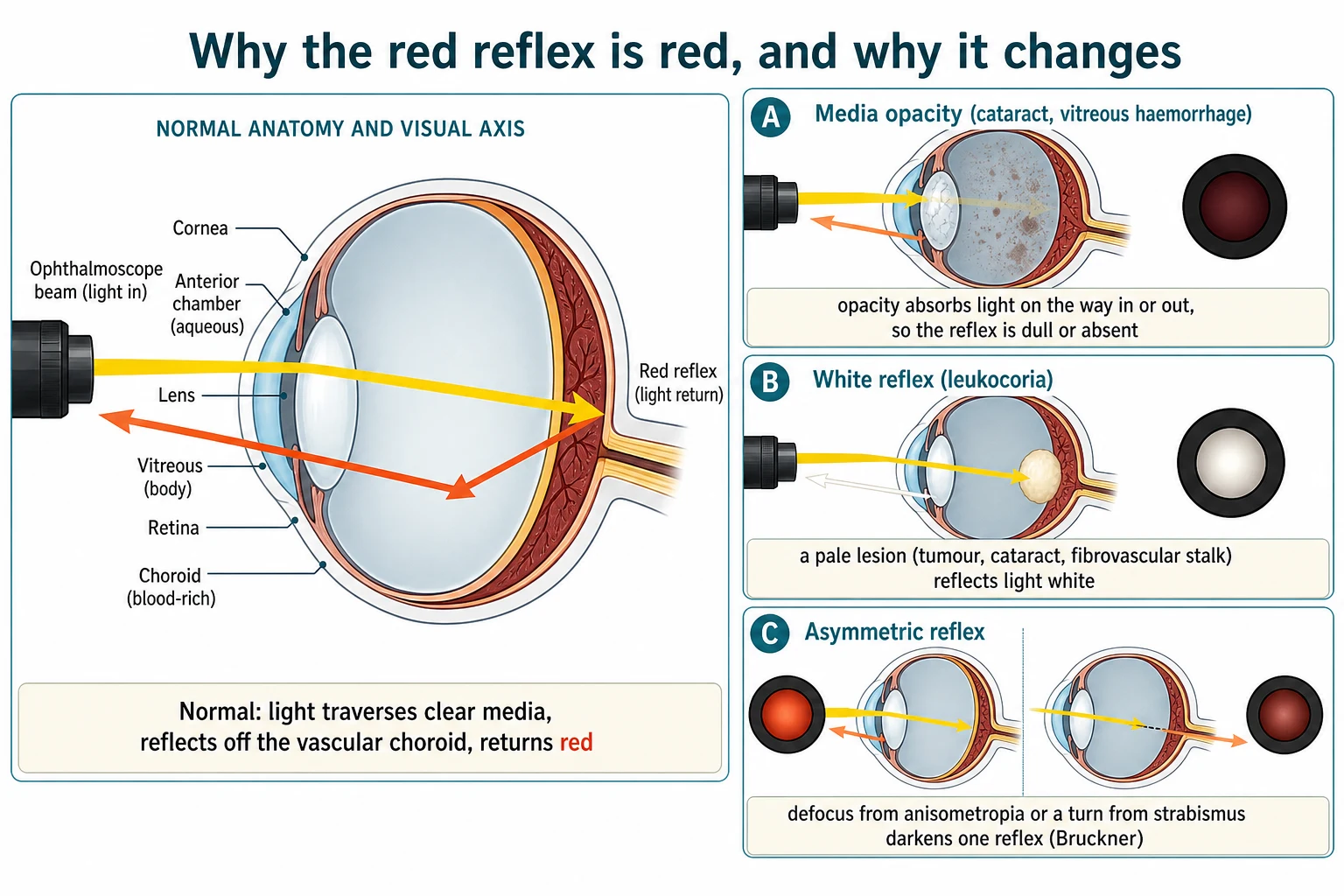
An opacity anywhere along that round trip blocks or scatters the light, which is why a dull or absent reflex localises to a media problem. A cataract in the lens, blood or inflammatory debris in the vitreous, or a detached retina sitting in the axis all absorb or scatter the beam on the way in or the way out. The denser and more central the opacity, the more of the reflex is lost, until a mature cataract can give a completely dark pupil. This is also why a little mucus in the tear film can cause a transient false abnormality that clears on blinking — a reason to repeat a surprising result. [4] [3]
A white reflex has a different mechanism. Instead of the light reaching the choroid and coming back red, a pale lesion in the axis reflects it back white. In retinoblastoma a chalky white tumour mass sits in the retina and reflects the flash; in congenital cataract the white lens itself scatters light; in persistent fetal vasculature a fibrovascular stalk and a retrolental mass block and reflect; in Coats disease a yellow exudative retinal detachment fills the axis. The common thread is a pale structure intercepting the light before it reaches the choroid. The exact colour and pattern are the ophthalmologist's clue to the cause, but for you the colour is simply white, and white is leukocoria. [6] [3]
The asymmetric reflex follows yet another mechanism, and it is the one that makes the Bruckner test work. When one eye is out of focus (anisometropia) or turned (strabismus), less of the returning light is captured, so that eye's reflex looks darker. If both eyes were equally defocused the reflexes would be equally dim, which is why the test depends on comparison: the eye that is more out of focus, or turned, is the darker one. A symmetric, equally bright reflex therefore argues against a significant refractive difference or a manifest squint, and an asymmetric one points you straight to an amblyopia risk factor. [4] [10]
Finally, remember that the colour of the reflex is partly a property of the fundus behind it. A heavily pigmented fundus absorbs more of the returning light, so children of Asian, African or First Nations heritage often have a darker, duskier reflex that is entirely normal — as long as it is symmetric. This is the single most common reason a junior clinician calls a normal reflex abnormal, and the fix is always the same: compare the two eyes. [4] [3]
Clinical Presentation
The normal red reflex is a symmetric orange-red or reddish glow of equal brightness, colour and size in both pupils, present from birth. When you see it, you document it and reassure the family. The abnormal reflex, by contrast, announces itself in one of three ways, and each has a typical story around it. [4] [1]
The first is the routine find: you are doing a well-child check and the reflex is not right. It may be white, dull, absent or asymmetric, and it has come as a surprise to everyone including the parents. This is why the test exists — to catch the silent lesion before anyone notices it. The story is unremarkable; the finding is not. [3] [4]
The second is the flash photograph: a parent has taken a photo with flash and one pupil has come back white instead of red. This is a real and important presentation, and it must be taken seriously even if your bedside reflex looks subtle, because a small or eccentric lesion may show in a flash that the bedside test barely detects. The caveat is that a single red-eye appearance from a normal photograph is common and benign; it is the asymmetric white pupil — one eye white, the other red — that warrants a careful repeat and referral if there is any doubt. [4] [6]
The third is the presenting symptom of poor vision or a squint: the child is not fixing and following, has a new head turn or squint, or the parents feel the child does not see well, and the red reflex is abnormal on testing. A new strabismus with leukocoria is a classic retinoblastoma presentation — the tumour destroys central vision and the eye drifts — which is why any new squint deserves a red-reflex check, and any leukocoria with a squint needs same-day referral. [6] [11]
Age shapes the likely cause. A newborn or young infant with a dense white reflex points to a congenital cataract or persistent fetal vasculature, both of which are time-critical for amblyopia. A toddler with a new white pupil points to retinoblastoma, whose incidence peaks in the first two to three years of life. A preschool child failing vision screening usually has a refractive error or amblyopia risk factor, found through an asymmetric reflex or an instrument-based screen. An older child is less likely to have retinoblastoma but can still develop an inflammatory, traumatic or structural cause — and a new leukocoria at any age still needs urgent referral. [6] [3]
Differential Diagnosis
When the reflex is abnormal, build the differential around the pattern you saw, and lead with the two diagnoses that threaten sight or life. For a white reflex the priority order is retinoblastoma and congenital or developmental cataract, then the vascular and structural causes, then the infectious and inflammatory ones, then the benign mimics. [3] [6]
Retinoblastoma is the malignancy that must never be missed. It arises from the developing retina, usually presents in the first two to three years of life, and classically gives a chalky white or pink-white reflex, sometimes with a squint. It can be bilateral in heritable cases, and a family history raises the stakes. Beyond the eye it is life-threatening, which is why a white reflex in a toddler is referred the same day, not next week. [6]
Congenital or developmental cataract is among the most common treatable causes of leukocoria and the most time-critical for amblyopia. A dense infantile cataract gives a white or grey pupillary reflex and, if not operated on within weeks, causes irreversible suppression of that eye. Unilateral dense cataracts are the most amblyopiagenic because the brain suppresses the blurrier eye completely. [11] [4]
The vascular and structural causes form the next layer. Persistent fetal vasculature (formerly persistent hyperplastic primary vitreous) leaves a fibrovascular stalk and a retrolental mass, typically unilateral and microphthalmic, present from birth. Coats disease is a retinal telangiectasia that leaks lipid exudate and produces a yellow exudative retinal detachment, usually in a young boy. A retinal detachment — from retinopathy of prematurity, trauma, or a shaken-impact injury — can sit in the axis and reflect white. A retinal or choroidal coloboma is a structural gap that can appear as a white or pale reflex. [3] [4]
The infectious and inflammatory causes include ocular toxocariasis (visceral larva migrans from the dog or cat roundworm, producing a granuloma or tractional detachment in a child with soil exposure), intermediate or posterior uveitis with inflammatory debris, and endophthalmitis in a red, painful eye. These are less common but belong in the differential of a child with an opaque media and a relevant history. [3] [4]
The benign and inherited causes should be known so they are not over-investigated: a retinal astrocytic hamartoma in tuberous sclerosis, myelinated nerve fibres near the disc, retinal dysplasia and Norrie disease, and a large optic disc anomaly. These still need ophthalmology confirmation, but they temper the prognosis. [3] [6]
Before accepting any of these, exclude the technical and physiological false causes, which are the real reason a normal child is referred. Mucus or a tear-film deposit, a small or eccentric pupil, poor technique (a lit room, too small a spot, wrong distance), high myopia, and a normally dark but symmetric pigmented-fundus reflex can all mimic an abnormality. Correcting the technique and repeating the test resolves most of these; the residual doubt is referred. [4] [3]
For an asymmetric but non-white reflex, the differential is narrower and points away from a mass: anisometropia (a difference in refractive error between the eyes) and strabismus. Both are amblyopia risk factors, and both need an ophthalmology referral for a refraction and a motility assessment rather than for an urgent mass workup. [10] [4]
Clinical & Bedside Assessment
The red-reflex test only works if it is done right, and doing it right means controlling four things: the room, the instrument, the distance, and the comparison. Get those four right and the reflex is reliable; get one wrong and you generate a false abnormal or, worse, miss a real one. [4] [1]
Darken the room. The reflex is best seen against a dark background, so turn the lights down or move to a dim corner. A brightly lit room washes out the glow and makes a subtle asymmetry invisible. Set the instrument. Use a direct ophthalmoscope on the largest, brightest spot at zero or low magnification — you want a broad beam that lights both pupils at once, not a pinpoint that examines one. Set the distance. Stand about an arm's length away, roughly 30 to 45 centimetres, close enough that both pupils fall within the beam. Compare both eyes together. Shine the beam at both pupils simultaneously and judge the colour, brightness and size of the two reflexes side by side — this simultaneous comparison is the Bruckner test, and it is what catches asymmetry. [4] [3]
Then repeat the test at a couple of distances and gaze positions, because some lesions are only visible off-axis or at a particular distance, and document the finding for each eye separately — "normal symmetric red reflex, both eyes" or "white reflex right, normal left". A finding that is not documented is a finding that did not happen, and a finding that was checked in a lit room with a tiny beam is a finding that cannot be trusted. [4] [1]
The red reflex is one part of a small set of bedside assessments that together screen the paediatric eye, and the others change with age. The vision assessment is age-adapted by what the child can do. In the newborn and young infant, test fixation and following: by two to three months an infant should fix on a face or a light and follow it to the midline and beyond, and a failure to do so is a red flag for poor vision. In the preverbal child, use preferential-looking acuity cards (such as Teller cards), which exploit an infant's preference for a striped pattern over a blank field to estimate acuity, and observe for steady, maintained fixation in each eye. [11] [4]
From about three years of age, when most children can match or name symbols, test monocular distance acuity with matching optotypes such as HOTV letters or LEA symbols, and add a test of stereopsis (binocular depth perception) such as Randot or Titmus, because reduced stereopsis is a sensitive marker of strabismus or amblyopia. From school age, use a Snellen or LogMAR chart for distance acuity, and consider colour-vision testing. At every age, also do the external inspection (ptosis, proptosis, an abnormal head posture, a red or discharging eye, a cloudy cornea which in an infant suggests congenital glaucoma, and an abnormal pupil), the pupil assessment for symmetry and reactivity, and the motility assessment with the corneal light reflex (Hirschberg) and, in a cooperative child, the cover-uncover and alternate-cover tests. [11] [4]
Synthesise what you find into a single problem representation, because that is how you communicate the urgency. "An eight-week-old with a dense white reflex on the right" tells the ophthalmologist everything they need to triage; "a three-year-old with an unequal red reflex and a right esotropia" points to an amblyopia risk factor. State the single next action out loud — for any abnormal reflex that action is urgent ophthalmology referral — and you have done your job as the screener. [4] [3]
Investigations
The red-reflex test is itself the screening investigation, and an abnormal result is an indication for urgent referral, not for a battery of primary-care tests. There is no blood test, no swab and no imaging in the community that changes the management of a white reflex, and ordering them only delays the referral that matters. [4] [6]
What ophthalmology will do, and what you should recognise but not order yourself, is a fuller workup. A dilated fundus examination is the core step, and in an uncooperative infant or toddler it becomes an examination under anaesthesia, where the ophthalmologist can dilate, inspect the whole retina, and take measurements. For a suspected intraocular mass, a B-scan ultrasound characterises the lesion and looks for the intralesional calcification that is classic for retinoblastoma; an orbital magnetic resonance image defines the mass and assesses optic-nerve and extraocular extension that change staging and treatment. [6] [3]
One adjunct that the generalist should understand is instrument-based screening — photoscreening and handheld autorefraction. Devices such as the Spot or Plusoptix screener capture an image of the eyes and estimate refractive error, pupil size and media clarity, flagging amblyopia risk factors in seconds. Because the child only needs to look at the device, it extends screening to the preverbal child who cannot yet do an acuity chart, and its performance against the AAPOS referral criteria has been validated. It does not replace the red reflex or the acuity test, but it fills the gap between them for one- to three-year-olds. [7] [8] [10]
The investigations that are not appropriate as first steps matter as much as the ones that are. Do not prescribe topical antibiotics, steroids or dilating drops before specialist assessment, because they do not change the underlying cause and may obscure the examination. Do not order blood tests or a swab in lieu of referral. And do not reassure the family on the basis of a normal-looking phone photograph when a careful bedside test was not done — a normal photograph does not exclude a small lesion, and the reassurance closes the referral loop prematurely. [4] [6]
Management — Resuscitation
There is one non-negotiable rule in this topic, and it is worth stating first because everything else flows from it. A white reflex, an absent reflex, or a clearly asymmetric reflex is an abnormal screening result that must be referred for urgent ophthalmology assessment. Retinoblastoma is a life-threatening malignancy, and a dense congenital cataract causes irreversible amblyopia within weeks to months, so the cost of waiting is measured in sight and in life. [6] [11]
Before the child leaves your room, do three things. First, do not apply anything to the eye — no ointment, no drops, no oral medication, no home remedy — because none of these changes the underlying cause and several obscure the specialist examination. Second, document the finding precisely, for each eye, including the pattern you saw and the conditions under which you tested. Third, arrange the referral at the right urgency: same-day for a suspected serious lesion such as a white reflex in an infant or toddler, and prompt ophthalmology referral for an asymmetric reflex or a refractive concern. [4] [3]
Then safety-net the family. Explain the urgency in plain language without using alarming diagnostic labels — "the test shows something that needs an eye specialist to look at today" rather than "this could be a tumour". Tell them exactly when and where to be seen, what would bring them back sooner, and that the specialist will dilate the pupil and examine the back of the eye. A family who understands why the review is urgent is a family who keeps the appointment. [4] [6]
Recognise the contexts that need the highest urgency and a same-day conversation: any white reflex in an infant or toddler (retinoblastoma or dense cataract); a new strabismus with an abnormal reflex; a child with poor fixation and a leukocoria; and a traumatic or suspected non-accidental injury with a media opacity. In each of these the lesion is either sight-threatening, life-threatening, or a safeguarding concern, and the right place for the child is the eye service that day. [6] [3]
Management — Definitive & Stepwise
Once the immediate triage decision is made, the stepwise management follows the result of the test. The red reflex sorts children into two streams, and the stream decides everything that happens next. [4] [3]
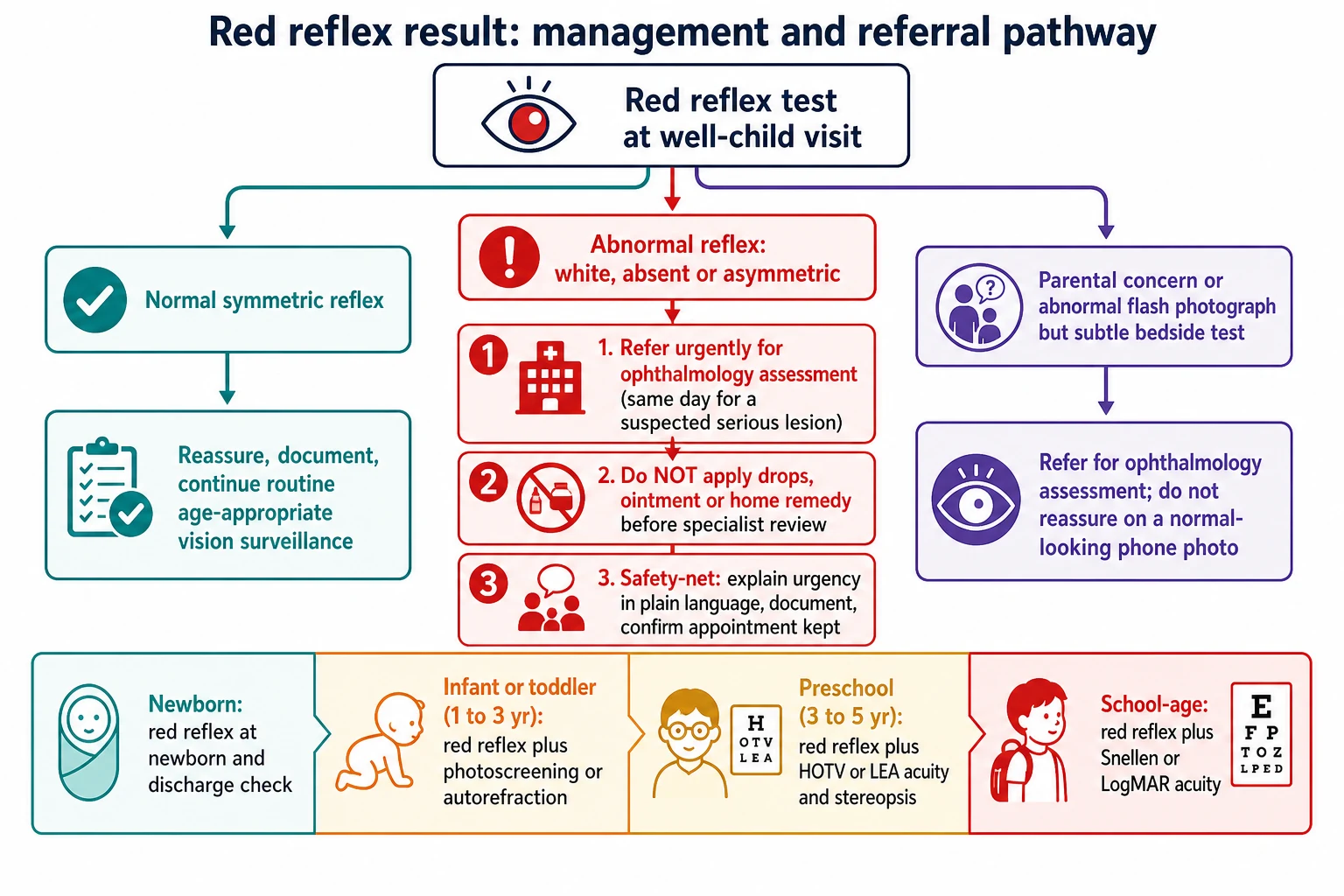
For a normal reflex, reassure the family, document the finding, and continue routine age-appropriate vision surveillance and screening at each well-child visit. That is the whole management, and it is the commonest outcome by far. The reassurance is genuine, but it is paired with the commitment to repeat the test next time, because a child who is normal today can develop a lesion tomorrow. [4] [1]
For an abnormal reflex, the management is referral, and the definitive treatment belongs to the underlying cause in the sibling topic leaves. Retinoblastoma is managed with chemoreduction, laser, cryotherapy, plaque brachytherapy or enucleation depending on size and spread. A dense congenital cataract is operated on within weeks, followed by optical correction and amblyopia therapy. Coats disease is treated with laser or cryotherapy to the leaking telangiectatic vessels. Persistent fetal vasculature may need surgery for its complications. Refractive error and amblyopia are managed with glasses and patching or atropine penalisation. Your job stops at the referral; theirs begins there. [6] [11]
The screening pathway itself is a stepwise, age-banded program, and knowing the bands is examinable. The red reflex is done at every visit from the newborn check. Instrument-based screening — photoscreening or autorefraction — is offered from about one to three years of age to catch amblyopia risk factors in the preverbal child, as endorsed by the American Academy of Ophthalmology and AAPOS. Formal visual-acuity testing begins from about three to four years, once the child can match or name symbols, using HOTV or LEA and a stereopsis test, with the AAPOS age-specific referral thresholds applied to the result. [7] [10] [9]
The follow-up principle closes the loop. Children who pass screening continue routine surveillance. Children who are referred are followed by ophthalmology for their specific lesion. And any child with a previously normal reflex who develops a new white reflex or a new squint is re-referred urgently — a normal result last visit does not protect against a lesion this visit, which is exactly why the test is repeated every time. [4] [6]
Specific Subtypes & Scenarios
The red reflex changes shape with the child in front of you, and the scenario decides which screening test to add alongside it. Hold the test constant — dim room, big bright spot, arm's length, both eyes together — and vary the adjunct by age and setting. [4] [1]
The newborn and neonatal intensive care infant is the first test of life. Perform the red reflex as part of the newborn and discharge examination, document it for each eye, and recognise that the premature and low-birth-weight infant carries extra risk — retinopathy of prematurity, refractive error and strabismus all cluster in this group, and they require retinal screening to a separate protocol that runs alongside the red reflex. A quality-improvement approach in the neonatal unit measurably raises the proportion of infants correctly screened, which is the practical lesson: screening rates rise when someone owns them. [5] [2]
The preverbal child, roughly one to three years, is the group the traditional acuity chart cannot reach, because the child cannot match or name symbols. Here the red reflex at every visit is paired with instrument-based photoscreening or autorefraction, which flags amblyopia risk factors from a single captured image. This is how refractive error, asymmetric focus and early media opacity are caught in the toddler years, before amblyopia consolidates. [7] [8]
The preschool child, roughly three to five years, can finally do a real acuity test. Add monocular distance acuity with HOTV or LEA symbols and a stereopsis test such as Randot, and apply the AAPOS age-specific referral thresholds — a child whose acuity falls below the age threshold, or who shows a two-line difference between eyes, or who fails stereopsis, is referred. This is the age band where vision screening programs deliver their biggest amblyopia dividend, and where screening coverage still varies widely. [12] [10]
The school-age child and adolescent is screened with the red reflex plus a Snellen or LogMAR chart, colour-vision testing, and an eye to new refractive error, convergence insufficiency or a new strabismus. A new leukocoria is less likely to be retinoblastoma at this age, but it still needs urgent referral — inflammatory, traumatic and structural causes do not respect age bands. [11] [3]
The flash-photograph presentation deserves its own paragraph because it arrives so often. A parent shows you a photo in which one pupil is white. Take it seriously. Repeat the red reflex carefully in a dim room at a couple of angles, compare the two eyes, and refer if there is any doubt — a single abnormal photograph warrants a formal test rather than reassurance, because a normal-looking phone photo does not exclude a small lesion. [4] [6]
The uncooperative child is the scenario that tempts you to record a reflex you did not properly see. Do not. A reflex that could not be obtained is an incomplete examination, and the right answer is an ophthalmology assessment or an examination under anaesthesia, not a guessed "probably normal". Recording a normal reflex you did not confirm is exactly how a serious lesion is missed. [4] [3]
Complications & Pitfalls
The complications of getting the red reflex wrong are the complications of the diseases it screens for, and they are severe. Missing a retinoblastoma can cost a child their eye and their life if the tumour extends beyond the globe. Missing a dense congenital cataract can cost a child permanent vision in that eye through irreversible amblyopia. These are not abstract risks — they are the reason the test exists. [6] [11]
The technical pitfalls are the ones you control, and they cause both false positives and false negatives. Examining in a lit room, using too small or too dim a spot, standing too close or too far, examining one eye at a time instead of both together, and failing to compare the two reflexes all degrade the test. The fix is the four-step discipline: dark room, big bright spot, arm's length, both eyes at once. [4] [3]
The false-negative pitfalls are the dangerous ones, because a reassuring normal reflex can hide a real lesion. A small or peripheral tumour may not reach the axis. A lesion visible only in certain gaze positions may be missed head-on. A heavily pigmented fundus gives a normally darker reflex that can mask asymmetry. Mucus or a tear-film deposit can temporarily dull a reflex that is truly normal. And a single normal reflex does not exclude a small retinoblastoma — so any parental concern or abnormal photograph is referred even when the bedside test looks normal. [6] [4]
The false-positive pitfalls waste referrals and anxiety but are preferable to the alternative. High myopia, a small or eccentric pupil, and artefact from the examination technique can all cause an apparent abnormality that resolves on correct technique. The disciplined response is to correct the technique, repeat the test, and refer the residual doubt rather than dismissing it. [4] [3]
The communication pitfall is using a diagnostic label before the specialist has made the diagnosis. Telling a family their child may have a tumour or cancer on the basis of a screening reflex causes avoidable distress and is not yours to say. The correct framing is an abnormal screening finding that needs urgent specialist review — accurate, urgent, and honest without presuming the diagnosis. [4] [6]
The systems pitfall is the one that defeats a good test at the population level: failing to document the finding, failing to close the referral loop, or reassuring on a normal-looking photograph when a careful bedside test was not done. A red reflex that was performed but not documented, or a referral that was suggested but never confirmed, is how a serious lesion slips through. Own the documentation, own the referral, and confirm the appointment was kept. [5] [4]
Prognosis & Disposition
The prognosis of an abnormal red reflex is the prognosis of its underlying cause, and the single variable that moves it most is the speed of referral. Caught early, retinoblastoma has a high survival rate with modern focal and systemic treatment; caught late, after extraocular spread, it can be fatal. Operated early and paired with amblyopia therapy, a congenital cataract can leave a child with useful vision; operated late, it leaves irreversible amblyopia. The reflex itself does not change the prognosis — the timing of your response does. [6] [11]
The disposition rule is simple and applies to every result. An abnormal red reflex is referred for urgent ophthalmology assessment. A normal reflex continues routine surveillance. And in every case, the primary clinician documents the finding and confirms that the appointment, if one was made, was kept. Closing the loop is part of the disposition, not an afterthought. [4] [3]
The long-term outcome of the amblyopia risk factors the test catches is improved by early detection and treatment during the sensitive period, and this is the evidence base for screening. Eibschitz-Tsimhoni and colleagues demonstrated that early screening for amblyogenic risk factors lowers the prevalence and severity of amblyopia, which is why a screening program that reaches preverbal children — through the red reflex and instrument-based screening — delivers a measurable visual dividend across a population. [9] [12]
One disposition deserves emphasis because it is counterintuitive. A child with a normal bedside reflex but a parental concern or an abnormal photograph is still referred for urgent ophthalmology assessment, because a normal-looking bedside test does not fully exclude a serious lesion. The disposition is driven by the whole picture — the history, the photograph, the parental concern — not by a single normal reflex in a lit room. [4] [6]
Special Populations
In Australia and Aotearoa New Zealand, the red-reflex test is part of the newborn and well-child checks, but access to timely ophthalmology is uneven. A child in a remote or First Nations community may be screened competently in primary care and then wait weeks for an eye service that a city child reaches the same day. For the clinician in a rural or remote setting, the test must be done and documented to a high standard, and the referral closed through telehealth, outreach or retrieval pathways — because delay compounds existing inequity. Closing the loop matters most where the loop is longest. [5] [4]
Several populations need more than the routine reflex because their baseline risk is higher. Preterm and low-birth-weight infants are at risk of retinopathy of prematurity and of refractive error and strabismus, and require retinal screening to a separate protocol alongside ongoing vision surveillance. Children with a family history of retinoblastoma or congenital cataract need earlier and more frequent screening, and genetic referral where indicated, because heritable retinoblastoma can be bilateral and early. [6] [2]
Children with developmental disability or neurodiversity may not cooperate with an acuity chart, and poor cooperation must never be recorded as a normal reflex. Instrument-based screening or an examination under anaesthesia may be the only reliable way to assess these children, and the threshold for specialist referral is lower when the bedside assessment is incomplete. [7] [4]
Children with syndromes carry a higher eye burden. Down syndrome brings cataract, refractive error and strabismus; neurofibromatosis brings optic pathway glioma; tuberous sclerosis brings retinal astrocytic hamartomas. Each warrants proactive, scheduled eye examination rather than reactive screening. [3] [6]
Migrant, refugee and asylum-seeking families, and children entering out-of-home care, may have missed routine screening along the way. A red-reflex and vision assessment at first contact closes that gap, and is part of basic health surveillance for a child whose screening history is unknown. [4] [1]
Evidence, Guidelines & Regional Differences
The evidence and guideline base for this topic is unusually consolidated, because three major bodies speak with one voice on the central point. The American Academy of Pediatrics, the American Academy of Ophthalmology and the American Association for Pediatric Ophthalmology and Strabismus jointly recommend that the red-reflex test be performed at every well-child visit from the newborn period onward. That single recommendation is the backbone of practice, and the systematic review of newborn red-reflex screening, together with the reported sensitivity and specificity of the test, supports it. [7] [1] [2]
The AAPOS and American Academy of Ophthalmology vision-screening age thresholds are the other examinable pillar. Instrument-based screening — photoscreening or autorefraction — is endorsed from about one to three years of age, because it reaches the preverbal child. Formal visual-acuity testing begins from about three to four years, applying the AAPOS age-specific referral thresholds. The clinical accuracy of those referral criteria, and of the Spot device for amblyopia risk factors, has been validated, which is the evidence that instrument-based screening is reliable enough to deploy at scale. [7] [10] [8]
| Region | Red reflex | Preschool instrument-based screening | School-entry acuity |
|---|---|---|---|
| United States | Every well-child visit from newborn (AAP, AAO, AAPOS); USPSTF endorses screening at 3 years and older | Photoscreening or autorefraction from about 1 to 3 years | Visual acuity (Snellen or LogMAR) from about 3 to 4 years |
| United Kingdom | Newborn and infant red reflex; part of child health surveillance | Variable; orthoptic-led screening in some areas | Orthoptic vision screening at school entry, around 4 to 5 years |
| Australia and Aotearoa New Zealand | Newborn and well-child checks (part of routine child health surveillance) | Variable by state and jurisdiction | Preschool or school-entry screening, variable by state |
| Canada | Newborn and well-baby red reflex (RCPSC guidance) | Photoscreening increasingly used in younger preverbal children | Visual acuity screening at preschool or school entry |
The regional differences are real and operational. In the United States, vision screening is endorsed by the AAP, AAPOS and AAO and recommended by the US Preventive Services Task Force for children aged three years and older, with a strong instrument-based pathway for younger children. In the United Kingdom, the NHS offers orthoptic vision screening at school entry, around four to five years, alongside the newborn and infant red-reflex check. In Australia and Aotearoa New Zealand, red-reflex testing is part of the newborn and well-child checks, but preschool vision screening varies by state and jurisdiction, which creates exactly the access gap that matters for Indigenous and remote children. [7] [11]
The genuine controversy is that the red reflex is operator-dependent and imperfect. It has false negatives — small or peripheral lesions, and the masking effect of a pigmented fundus — and false positives from technique, pigmentation and myopia. This is precisely why it is a screening test rather than a diagnostic one, and why any abnormal or doubtful result is referred rather than dismissed. The imperfection is not an argument against the test; it is an argument for doing it well and for erring on the side of referral when in doubt. [4] [3]
The strongest evidence for screening itself is outcome-based. Early vision screening lowers the prevalence and severity of amblyopia, which is the practical justification for reaching preverbal children with photoscreening when traditional acuity testing is not yet possible. The point of the whole apparatus — the red reflex at every visit, the instrument-based screen in the toddler, the acuity chart at preschool — is to find the amblyopia risk factor and the dangerous lesion while there is still time to change the outcome. [9] [12]
Exam Pearls
The red reflex is checked at every well-child visit from the newborn examination onward, under the joint policy of the AAP, AAO and AAPOS. It is not a one-off newborn test; it is a every-visit test, and a normal result last visit does not protect against a lesion this visit. [7] [4]
Do the test the right way: dim room, largest bright spot, about 30 to 45 centimetres, both pupils together. The simultaneous comparison is the Bruckner test, and it is what catches the asymmetric reflex of anisometropia and strabismus. Examining one eye at a time defeats half the test. [4] [3]
The four abnormal reflex patterns
For the differential of leukocoria, hold the order: retinoblastoma and congenital cataract first, then persistent fetal vasculature, Coats disease, ocular toxocariasis, retinal detachment and coloboma. The order is the examinable point because it is the urgency order. [6] [3]
A dense infantile cataract must be operated on within weeks to avoid irreversible amblyopia, because the sensitive period closes in the first months and years of life. This timing is why a white reflex in a newborn is a same-day conversation, not a next-month appointment. [11] [4]
Instrument-based photoscreening extends screening to the preverbal child (about one to three years); formal acuity testing begins at about three to four years. Know the bands, because they are a favourite written question. [7] [10]
Take a parent's report of a white pupil in a flash photograph seriously, and repeat the red reflex carefully in a dim room — a normal-looking phone photo does not exclude disease. And frame the finding to families as an abnormal screening result needing urgent review, never as a diagnosis, and apply no drops or ointment before specialist assessment. [4] [6]
References
- [1]Taksande A; Jameel PZ Red reflex test screening for neonates: A systematic review and meta analysis. Indian J Ophthalmol, 2021.PMID 34304165
- [2]Sun M; Ma A Sensitivity and Specificity of Red Reflex Test in Newborn Eye Screening. J Pediatr, 2016.PMID 27640356
- [3]Lin SY; Yen KG Abnormal Red Reflex: Etiologies in a Pediatric Ophthalmology Population. Clin Pediatr (Phila), 2020.PMID 32503396
- [4]McLaughlin C; Levin AV The red reflex. Pediatr Emerg Care, 2006.PMID 16481935
- [5]Sakaria RP; Davidson JM Improving Red Reflex Screening in a Level III NICU Through a Quality Improvement-based Approach. Hosp Pediatr, 2022.PMID 36321385
- [6]Aerts I; Lumbroso-Le Rouic L Retinoblastoma. Orphanet J Rare Dis, 2006.PMID 16934146
- [7]Oatts JT; Collins ME Instrument-Based Screening for the Detection of Amblyopia and Amblyopia Risk Factors: A Report by the American Academy of Ophthalmology. Ophthalmology, 2025.PMID 40864029
- [8]Garry GA; Donahue SP Validation of Spot screening device for amblyopia risk factors. J AAPOS, 2014.PMID 25266832
- [9]Eibschitz-Tsimhoni M; Friedman T Early screening for amblyogenic risk factors lowers the prevalence and severity of amblyopia. J AAPOS, 2000.PMID 10951293
- [10]Silbert DI; Matta NS Clinical accuracy of the AAPOS pediatric vision screening referral criteria. J AAPOS, 2012.PMID 22824492
- [11]McConaghy JR; McGuirk R Amblyopia: Detection and Treatment. Am Fam Physician, 2019.PMID 31845774
- [12]Hunter SC; He J The UCI EyeMobile Preschool Vision Screening Program: Refractive Error and Amblyopia Results from the 2019-2020 School Year. Clin Ophthalmol, 2022.PMID 36573233