Paeds · ophthalmology
Papilloedema and optic nerve disorders
Also known as Optic disc swelling · Pseudopapilloedema · Idiopathic intracranial hypertension · Pseudotumour cerebri · Optic neuritis · Myelin oligodendrocyte glycoprotein antibody-associated disease · Frisén papilloedema grading · Optic nerve sheath fenestration
Fellowship guide to papilloedema and optic nerve disorders in children. Covers the swollen optic disc and the distinction of the true papilloedema from the pseudopapilloedema, the Frisén grading of zero through five, the raised intracranial pressure and the secondary causes, the idiopathic intracranial hypertension and the Friedman criteria with the opening pressure above two hundred and eighty millimetres of cerebrospinal fluid, the optic neuritis of the child with the pain on the eye movement and the relative afferent pupillary defect, the myelin oligodendrocyte glycoprotein antibody disease and the neuromyelitis optica spectrum disorder, the intravenous methylprednisolone, the acetazolamide and the optic nerve sheath fenestration, and the optic coherence tomography.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A school-age girl wakes with a throbbing headache and finds the world grey at the edges, and the optometrist photographs a swollen optic disc that neither parent can interpret. A boy with a cold develops pain behind one eye, loses the colour vision, and the doctor finds the disc swollen and the pupil slow. Both have met the optic nerve in distress, and the clinician who can tell the papilloedema of the raised intracranial pressure from the optic neuritis of the inflammation, and both from the harmless pseudopapilloedema of the buried drusen, is the clinician who protects the vision and the life. The swollen optic disc is the single most consequential sign in the paediatric neuro-ophthalmology, because behind it may sit a brain tumour, a clot in the venous sinus, or an inflammatory attack that will return. [1][2]
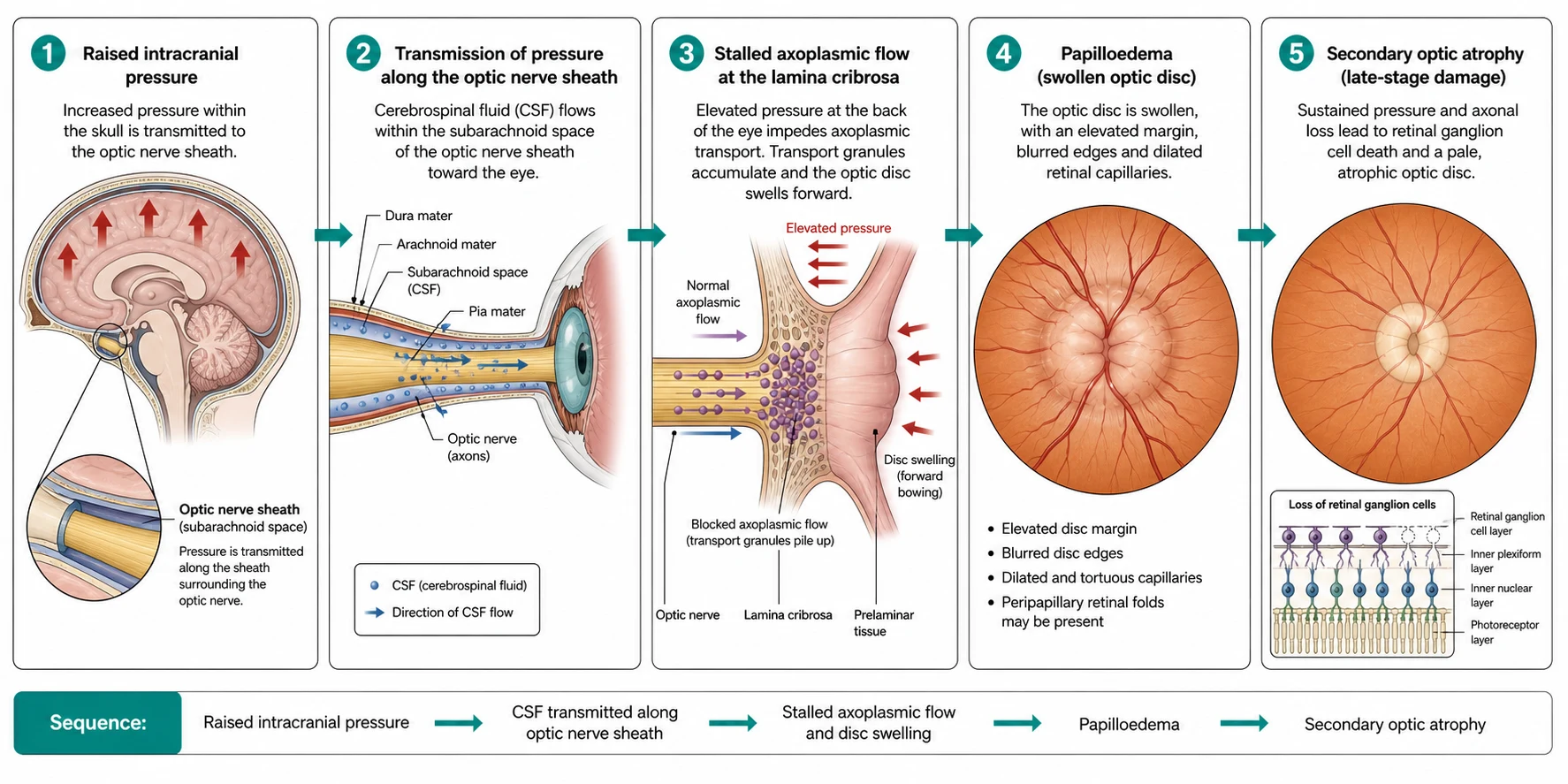
Papilloedema is the bilateral optic disc swelling that arises from the raised intracranial pressure, and it is a mechanical sign, not a disease. The pressure in the cranial compartment is transmitted along the optic nerve sheath to the prelaminar tissue, and the axoplasmic flow stalls and the disc swells. The clinician who sees the swollen disc and reasons backwards to the cause demonstrates the thinking the boards reward, because the papilloedema is the pointer to a long list of the intracranial problems, from the tumour and the hydrocephalus through the venous sinus thrombosis to the idiopathic intracranial hypertension. The optic neuritis, in contrast, is the inflammation of the optic nerve itself, and it produces the disc swelling from the local inflammation rather than from the raised pressure, and it carries the questions of the demyelination and the antibody. [1][9]
The clinical gravity of the topic rests on three skills the candidate must carry without hesitation. The first is the recognition that the bilateral disc swelling is the raised intracranial pressure until proven otherwise, and that the neuroimaging must precede the lumbar puncture. The second is the Friedman criteria for the pseudotumour cerebri syndrome, with the opening pressure above two hundred and eighty millimetres of cerebrospinal fluid in the child, the normal composition and the normal neuroimaging, because the idiopathic label is the diagnosis only after the secondary cause is excluded. The third is the swinging-flashlight test for the relative afferent pupillary defect, the single bedside sign that points to the optic nerve rather than the retina as the seat of the visual loss. [1][8]
Classification
The classification of the swollen optic disc rests on two axes, and the examination rewards the candidate who holds both clearly. The first is the cause of the swelling, the split between the papilloedema of the raised intracranial pressure, the optic neuritis and the optic neuropathy of the local inflammation or the ischaemia, and the pseudopapilloedema of the structural anomaly. The second is the severity of the papilloedema once it is confirmed, the Frisén grading of zero through five that drives the urgency and the surveillance. The candidate who walks the examiner from the cause to the severity, and from the bilateral to the unilateral, demonstrates the breadth the boards reward. [1][6]
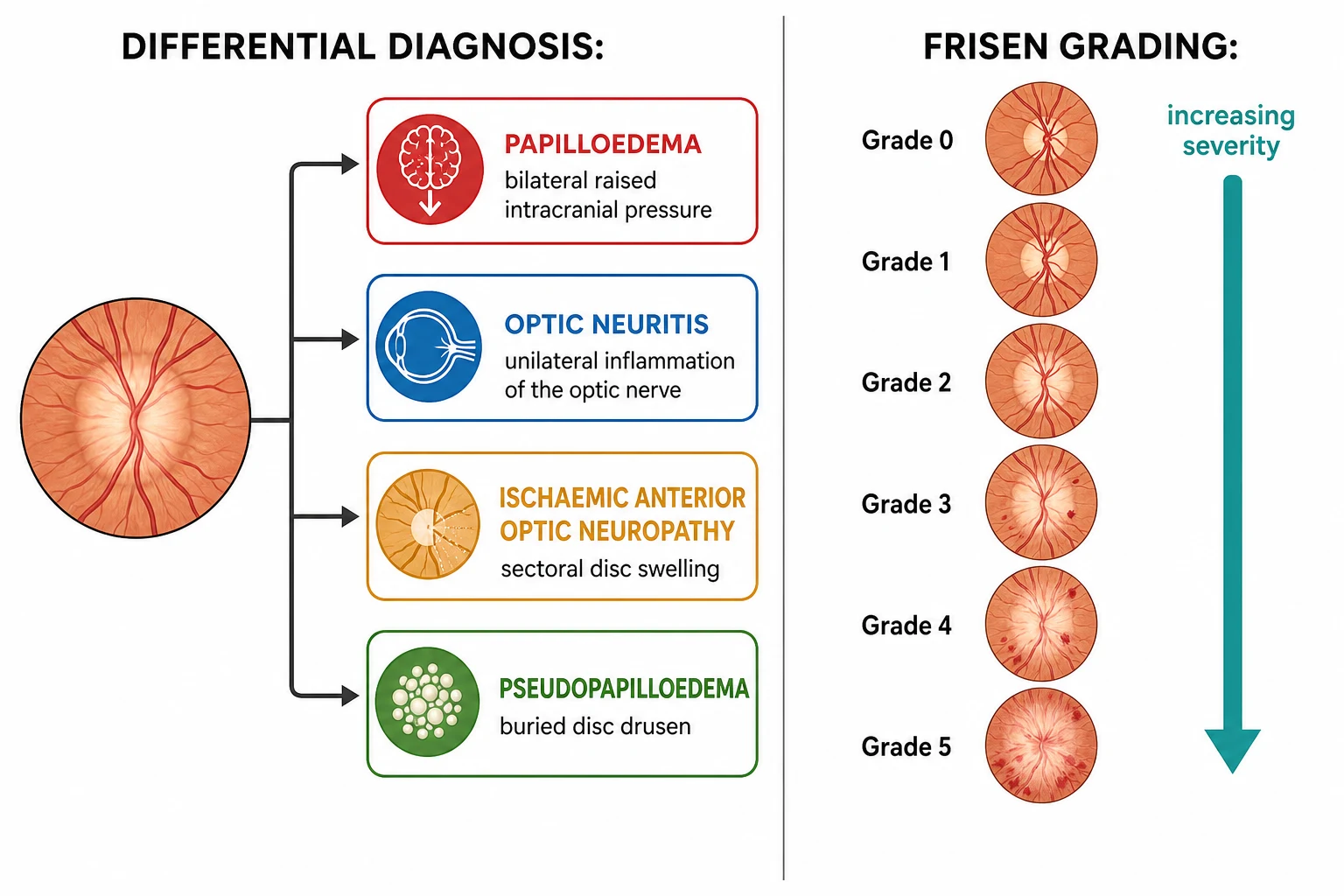
The Frisén grading scale is the standard for the severity of the papilloedema, and it runs from the grade zero of the normal disc to the grade five of the severe swelling. The grade zero is the flat disc with the normal vessels. The grade one is the C-shaped halo that surrounds the disc and spares the temporal margin, the earliest sign. The grade two is the complete halo that encircles the whole disc. The grade three is the elevation of the disc with the halo and the early deflection of the vessels at the disc margin. The grade four is the partial obscuration of the major vessels on the disc, and the grade five is the complete obscuration of all the vessels at the disc, the severe swelling that threatens the vision. The candidate who can name the five grades and the transition from the halo to the obscured vessel carries the scale without the hesitation. [1][3]
Papilloedema
raised pressure
- Bilateral by definition
- Disc swollen, vessels normal early
- Headache, vomiting, sixth-nerve palsy
- Neuroimaging before the lumbar puncture
Optic neuritis
inflammation
- Often unilateral, painful on eye movement
- Relative afferent pupillary defect
- Disc may swell (papillitis) or stay flat
- Antibody and MRI testing for the cause
Pseudopapilloedema
mimic
- Buried optic disc drusen, tilted disc
- No raised pressure, no vision loss
- Ultrasound and OCT settle the question
- Reassurance, no treatment required
AION
ischaemia
- Sudden painless visual loss in the older child
- Sectoral disc swelling, altitudinal defect
- Rare in children, seek the vasculitis
- Urgent referral, treat the cause
The distinction of the true papilloedema from the pseudopapilloedema is the fork that separates the urgent neuroimaging from the reassurance, and it is the one the boards probe most directly. The true papilloedema has the hyperaemic disc, the blurred margins, the absent spontaneous venous pulsations, the peripapillary haemorrhages and the exudates, while the pseudopapilloedema of the buried disc drusen has the normal disc colour, the distinct vessels and the absence of the haemorrhage. The spontaneous venous pulsation is the single most useful sign, because its presence at the disc implies the normal intracranial pressure and argues against the papilloedema, while its absence is suggestive but not diagnostic. The candidate who looks for the venous pulsation and the haemorrhage before reaching for the scanner demonstrates the bedside skill. [1][6]
Epidemiology & Risk Factors
The idiopathic intracranial hypertension, formerly the pseudotumour cerebri, has a bimodal distribution in the child, and the epidemiology that the boards reward is the split between the prepubertal and the pubertal child. In the prepubertal child, the boys and the girls are affected equally, the association with the obesity is weak, and the secondary cause is more often found. In the pubertal and the adolescent child, the girls dominate, the obesity is the strong risk factor, and the clinical picture resembles the adult disease. The incidence is rising with the rise of the childhood obesity, and the recent population-based studies confirm the burden in the older child. [2][4]
The optic neuritis of the child is less common than the optic neuritis of the adult, but it is the commonest acute optic neuropathy of the paediatric age, and it carries the different prognosis. The paediatric optic neuritis is more often bilateral than the adult, it is more often preceded by the infection or the vaccination, and it is more often associated with the acute disseminated encephalomyelitis. The recovery of the visual acuity is generally better in the child than in the adult, but the relapse and the long-term disability depend on the underlying antibody, and the myelin oligodendrocyte glycoprotein, the aquaporin-four and the multiple sclerosis define the three trajectories. [8][11]
The risk factors for the papilloedema are the risk factors for the raised intracranial pressure, and the candidate who lists them demonstrates the breadth. The space-occupying lesion, the hydrocephalus, the venous sinus thrombosis and the meningitis are the structural causes. The drugs are the common secondary trigger, and the tetracyclines, the vitamin A and the retinoids, the growth hormone and the withdrawal of the chronic corticosteroid are the recurring offenders. The systemic disease, including the lupus, the sarcoidosis and the chronic renal failure, and the sleep apnoea of the obese adolescent, complete the list. The candidate who links the drug history to the disc swelling is the candidate who does not miss the secondary cause. [2][3]
Pathophysiology
The pathophysiology of the papilloedema begins with the raised intracranial pressure and the optic nerve sheath, because the disc swelling is a mechanical consequence of the pressure. The optic nerve is the white-matter tract of the central nervous system, and it is wrapped in the meninges and bathed in the cerebrospinal fluid of the subarachnoid space that surrounds it. When the intracranial pressure rises, the pressure is transmitted along the subarachnoid space of the optic nerve sheath to the back of the eye, and the cerebrospinal fluid presses on the prelaminar tissue of the disc. The pressure stalls the axoplasmic flow, the slow transport of the proteins and the organelles along the retinal ganglion cell axons, and the dammed axoplasm swells the disc. [1][3]
The pathophysiology of the optic neuritis is the inflammation of the optic nerve, and it is the immune-mediated attack on the myelin rather than the mechanical pressure. The optic nerve is the myelinated tract, and the inflammatory attack strips the myelin sheath from the axons, slows the conduction, and blocks the signal from the retina to the brain. The pain on the eye movement is the sign of the inflammation of the meningeal sheath of the nerve, because the extra-ocular muscles pull on the inflamed nerve. The disc swelling of the papillitis is the local inflammation at the nerve head, and it distinguishes the paediatric optic neuritis from the more often retrobulbar adult form. The relative afferent pupillary defect is the sign of the asymmetrical input to the two eyes, and it is the single most reliable sign that the optic nerve rather than the retina carries the lesion. [8][9]
The antibody-mediated optic neuritis is the modern dimension of the topic, and it is the one that defines the prognosis. The myelin oligodendrocyte glycoprotein antibody disease is the commonest of the antibody-mediated forms in the child, and it presents with the bilateral optic neuritis, the disc swelling, the frequent association with the acute disseminated encephalomyelitis, and the generally favourable recovery of the visual acuity, though the relapse is common. The aquaporin-four antibody neuromyelitis optica spectrum disorder is the severe form, and it presents with the severe bilateral optic neuritis, the poor recovery, the longitudinally extensive transverse myelitis and the brainstem lesions. The multiple-sclerosis-associated optic neuritis sits between, with the unilateral attack, the recovery and the risk of the relapse and the long-term disability driven by the brain lesions on the magnetic resonance imaging. [8][9]
Clinical Presentation
The child with the papilloedema presents through several doors, and each carries its own clue. The headache is the commonest symptom, and it has the features of the raised-pressure headache, the throbbing character, the worsening in the morning, the worsening with the bending or the coughing, and the relief with the vomiting. The transient visual obscurations, the brief grey-outs of the vision on the change of posture, are the classic symptom of the papilloedema, and they reflect the transient ischaemia of the swollen disc. The diplopia from the sixth-nerve palsy is the false-localising sign of the raised pressure, because the long sixth nerve is stretched by the pressure. The pulsatile tinnitus and the photophobia complete the picture. [2][3]
The child with the optic neuritis presents with the different story, and the features point to the optic nerve rather than the pressure. The visual loss is the central symptom, and it comes on over the hours to the days, often with the pain on the eye movement that precedes or accompanies the visual loss. The dyschromatopsia, the loss of the colour vision, is out of proportion to the loss of the acuity, and the red looks washed out. The relative afferent pupillary defect is the sign in the affected eye, and the fundus may show the swollen disc of the papillitis or the normal disc of the retrobulbar neuritis. The bilateral involvement, the preceding infection and the associated neurological deficit point to the acute disseminated encephalomyelitis or the antibody-mediated disease. [8][11]
The infant and the young child present with the special challenge of the non-verbal visual loss, and the boards probe the recognition. The infant may present with the irritability, the vomiting, the failure to thrive, the developmental regression, the sunset sign of the downward gaze, or the head tilt. The bulging fontanelle and the increasing head circumference are the signs of the raised pressure in the infant with the open skull, and the papilloedema may be absent because the open sutures decompress the pressure. The young child may present with the behavioural change, the decline in the school performance or the squint, and the fundoscopy is the step that must not be missed. The candidate who examines the fundus of the child with the unexplained headache or the vomiting demonstrates the safety-critical habit. [2][5]
Acetazolamide for the idiopathic intracranial hypertension
Dose
Approximately fifteen to twenty-five milligrams per kilogram per day in the divided doses in the child, with the lower starting dose and the gradual titration, avoiding the rapid escalation, with the monitoring for the paraesthesia, the taste disturbance, the metabolic acidosis and the renal stones
Differential Diagnosis
The differential of the bilateral optic disc swelling is the one the boards probe most directly, and the task is to separate the papilloedema from the long list of the causes of the swollen disc. The papilloedema is the bilateral disc swelling of the raised intracranial pressure, and the cause is sought with the neuroimaging, the magnetic resonance venography and the lumbar puncture. The optic neuritis may produce the swollen disc of the papillitis, and it is distinguished by the painful visual loss and the relative afferent pupillary defect. The malignant hypertension produces the bilateral disc swelling, and the blood pressure settles the question. The uveitis and the posterior scleritis are the local inflammations that swell the disc, and the slit-lamp examination finds the cells. [1][6]
The pseudopapilloedema is the mimic that demands the confident recognition, and the buried optic disc drusen is the commonest of its causes. The drusen are the calcified deposits in the disc substance, and they raise the disc and blur the margin without the raised pressure, and they are more common in the white child and the small hyperopic disc. The tilted disc and the crowded disc of the high hyperopia are the structural anomalies that simulate the swelling, and the peripapillary myelinated nerve fibre is the white streak that mimics the swelling. The optical coherence tomography and the orbital ultrasound settle the question, because the drusen calcify and reflect the ultrasound and the OCT shows the buried reflectivity, while the true papilloedema shows the elevated nerve fibre layer. [6]
Idiopathic IIH
no cause found
- Obese pubertal girl, or the prepubertal child
- Normal MRI, normal MRV, normal CSF
- Opening pressure above 280 mm CSF
- Acetazolamide and the weight loss
Venous sinus thrombosis
secondary
- Dehydration, otitis, head infection
- MRV shows the absent venous flow
- Anticoagulation and the cause treatment
- Mimics the IIH on the fundus
Drug-induced
secondary
- Tetracyclines, vitamin A, retinoids
- Growth hormone, the steroid withdrawal
- Resolves with the drug cessation
- Take the careful drug history
Mass and hydrocephalus
structural
- MRI shows the tumour or the ventricles
- Urgent neurosurgery and oncology
- Papilloedema is the pointer
- Not the IIH, never label as idiomatic
The differential of the acute unilateral visual loss connects the optic neuritis to the general paediatric and the emergency assessment, and the principle is to hold the optic nerve high on the list. The optic neuritis is the commonest cause of the acute unilateral visual loss in the child with the painful eye and the relative afferent pupillary defect, but the trauma, the retrobulbar haemorrhage, the retinal detachment and the central retinal artery occlusion must be excluded. The functional or the non-organic visual loss is the mimic in the older child, and the normal pupil, the normal disc and the inconsistent fields point to the diagnosis. The candidate who performs the swinging-flashlight test on every child with the acute visual loss is the candidate who holds the optic nerve on the list. [8][9]
Clinical & Bedside Assessment
The bedside assessment of the child with the suspected disc swelling begins with the fundoscopy, and it is the single most important skill in the topic. The direct ophthalmoscope is used in the dim room, and the disc is assessed for the colour, the margin, the elevation, the vessels and the haemorrhages. The normal disc is the pink-yellow with the sharp margin, the spontaneous venous pulsations and the cup in the centre. The papilloedema is the hyperaemic disc with the blurred margin, the absent venous pulsations, the elevation, the dilated capillaries and the peripapillary haemorrhages and the exudates. The candidate who can describe the disc in the structured way, from the colour to the margin to the vessels, is the candidate who carries the fundoscopy. [1][6]
The visual assessment adds the quantification that the boards reward, and it is the part that the candidate must perform systematically. The visual acuity is measured with the age-appropriate tool, the Snellen or the logMAR for the school-age child, the picture or the letter-matching for the younger child, and the fixing-and-following for the infant. The colour vision is tested with the Ishihara plates, and the dyschromatopsia disproportionate to the acuity is the sign of the optic nerve. The visual fields are tested with the confrontation in the child and the formal perimetry in the older child, and the enlarged blind spot of the papilloedema and the central scotoma of the optic neuritis are the classic defects. The swinging-flashlight test for the relative afferent pupillary defect is the single most reliable sign of the optic nerve lesion, and it is performed by swinging the light between the two eyes and watching for the paradoxical dilation of the affected eye. [8][11]
The general examination adds the context that points to the cause, and the candidate who performs it demonstrates the breadth. The blood pressure is measured, because the malignant hypertension produces the bilateral disc swelling. The weight and the body mass index are measured, because the obesity is the risk factor for the idiopathic intracranial hypertension. The skin is examined for the café-au-lait patches of the neurofibromatosis and the ash-leaf macules of the tuberous sclerosis, because the phakomatoses produce the brain tumours that raise the pressure. The ears are examined for the otitis media, because the otitis is the cause of the venous sinus thrombosis. The drug history is taken in detail, because the tetracyclines and the vitamin A and the retinoids are the recurring offenders. [2][3]
Investigations
The investigation of the child with the suspected papilloedema is built around the neuroimaging, the lumbar puncture and the optical coherence tomography, and the order is non-negotiable. The magnetic resonance imaging of the brain is the first-line investigation, and it excludes the tumour, the hydrocephalus, the structural cause and the meningeal disease. The magnetic resonance venography is added to exclude the venous sinus thrombosis, because the plain magnetic resonance imaging may miss the clot in the venous sinus. The lumbar puncture follows the neuroimaging, and it measures the opening pressure in the lateral decubitus position with the child relaxed and the legs extended, and it analyses the cerebrospinal fluid for the cells, the protein and the glucose to exclude the meningitis and the inflammation. The opening pressure above two hundred and eighty millimetres of cerebrospinal fluid in the child is the threshold for the raised pressure. [1][5]
The optical coherence tomography is the modern tool that quantifies the disc swelling, and it is the standard for the surveillance of the papilloedema. The optical coherence tomography measures the retinal nerve fibre layer thickness, and the elevated thickness in the acute papilloedema falls as the swelling resolves, and the late thinning signals the axonal loss and the secondary optic atrophy. The orbital ultrasound is the tool that distinguishes the buried disc drusen from the true papilloedema, because the drusen calcify and reflect the ultrasound, while the true papilloedema does not. The fluorescein angiography may be used to confirm the leakage of the true papilloedema, and the American Academy of Ophthalmology has reviewed the imaging methods for the paediatric disc. [6][5]
The investigation of the optic neuritis is built around the magnetic resonance imaging and the antibody testing, and the candidate who orders both demonstrates the modern practice. The magnetic resonance imaging of the brain and the orbits with the gadolinium shows the inflamed optic nerve, the enhancement and the swelling, and the brain lesions that predict the multiple sclerosis. The antibody testing for the myelin oligodendrocyte glycoprotein and the aquaporin-four is performed on the blood, and the positive antibody defines the antibody-mediated disease and its prognosis. The cerebrospinal fluid may show the oligoclonal bands and the mild pleocytosis, and it adds the evidence for the demyelination. The visual evoked potentials show the delayed latency of the demyelinated nerve, and the optical coherence tomography shows the retinal nerve fibre layer changes. [7][8]
The urgent pathway for the child with the bilateral disc swelling
Recognise the bilateral disc swelling as the raised pressure until proven otherwise
Hyperaemic disc, blurred margin, absent venous pulsations, haemorrhages
Perform the urgent magnetic resonance imaging with the venography
Exclude the tumour, the hydrocephalus, the venous sinus thrombosis and the meningeal disease
Perform the lumbar puncture after the neuroimaging
Measure the opening pressure in the lateral decubitus, the child relaxed, the legs extended; above 280 mm is raised
Classify the cause and start the treatment
Idiopathic IIH versus the secondary; acetazolamide and the weight loss, or the targeted treatment of the cause
Management — Resuscitation
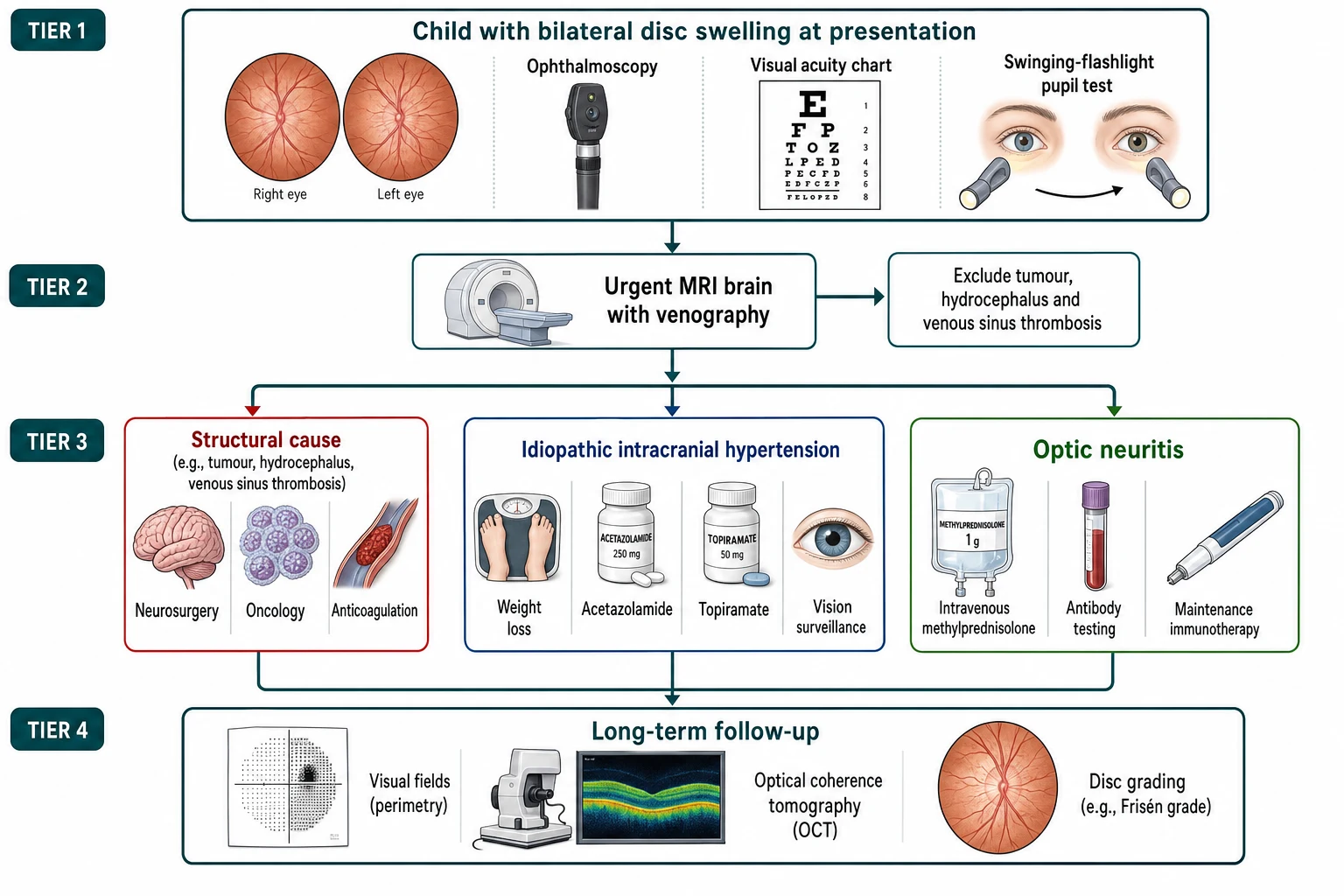
The resuscitation of the child with the papilloedema is governed by the principle that the dangerous element is the cause and the delay, and the management begins with the urgent neuroimaging. The child with the headache, the vomiting and the papilloedema has the raised intracranial pressure, and the first step is the magnetic resonance imaging with the venography to exclude the tumour, the hydrocephalus and the venous sinus thrombosis. The lumbar puncture follows the neuroimaging, never precedes it, because the blind lumbar puncture in the obstructed flow can cause the fatal herniation. The child with the falling conscious level, the bradycardia, the hypertension and the abnormal breathing of the Cushing triad is managed as the emergency, with the airway, the elevation of the head, the mannitol or the hypertonic saline, and the urgent neurosurgical transfer. [1][3]
The child with the optic neuritis is managed with the urgency of the acute visual loss, and the treatment begins with the intravenous corticosteroid. The intravenous methylprednisolone is the first-line treatment for the acute optic neuritis of the child, and it is given at twenty to thirty milligrams per kilogram per day to a maximum of one gram for three to five days, and the slower the treatment the poorer the recovery, because the untreated inflammation destroys the retinal ganglion cell axons. The plasma exchange is considered for the severe or the steroid-refractory optic neuritis, particularly the antibody-mediated disease, and the intravenous immunoglobulin has the role in the selected cases. The oral prednisolone alone is avoided, because the Optic Neuritis Treatment Trial showed the oral steroid did not improve the outcome and may increase the relapse. [8][9]
The child with the secondary intracranial hypertension is managed by the treatment of the cause, and the candidate who holds this principle demonstrates the safety-critical thinking. The venous sinus thrombosis is treated with the anticoagulation and the treatment of the precipitant, the dehydration or the otitis. The drug-induced intracranial hypertension resolves with the cessation of the offending drug, the tetracycline, the vitamin A or the retinoid. The meningitis and the encephalitis are treated with the targeted antimicrobial. The shunt malfunction and the tumour are managed by the neurosurgery. The idiopathic label is the diagnosis only after the secondary cause is excluded and treated. [2][3]
Management — Definitive & Stepwise
[1] [9]The definitive treatment of the idiopathic intracranial hypertension builds on the weight loss, the carbonic anhydrase inhibitor and the surveillance, and the surgery is reserved for the failing vision. The weight loss is the cornerstone of the management in the obese adolescent, and the modest weight reduction of the five to ten percent may resolve the papilloedema and the symptoms. The acetazolamide is the carbonic anhydrase inhibitor that reduces the cerebrospinal fluid production, and it is given at approximately fifteen to twenty-five milligrams per kilogram per day in the divided doses in the child, with the gradual titration and the monitoring for the paraesthesia, the taste disturbance and the metabolic acidosis. The topiramate is the alternative, and it offers the additional benefit of the weight loss and the migraine control, but it carries the cognitive and the weight-loss side effects. The surveillance of the vision is the non-negotiable part of the management, because the vision loss may occur without the warning symptom. [2][3]
The surgery is the treatment for the progressive vision loss despite the medical therapy, and it is the decision the boards probe for the reasoning. The optic nerve sheath fenestration is the ophthalmic procedure that opens the sheath of the optic nerve to decompress the nerve and protect the vision, and it is the procedure of the choice for the dominant or the asymmetric vision loss. The cerebrospinal fluid shunting, the ventriculoperitoneal or the lumboperitoneal shunt, is the neurosurgical procedure that diverts the cerebrospinal fluid and lowers the pressure, and it is the procedure of the choice for the headache and the generalised pressure. The venous sinus stenting is the interventional procedure for the selected case with the demonstrated venous stenosis and the pressure gradient, and it is the emerging option. The candidate who names the three surgical options and their indications demonstrates the breadth. [2][3]
The treatment journey of the paediatric intracranial hypertension
The definitive treatment of the optic neuritis builds on the acute corticosteroid and the antibody-directed long-term therapy, and the relapse defines the trajectory. The acute optic neuritis is treated with the intravenous methylprednisolone at twenty to thirty milligrams per kilogram per day to a maximum of one gram for three to five days, and the recovery of the visual acuity is generally good in the child. The myelin oligodendrocyte glycoprotein antibody disease is the relapsing form, and it may need the maintenance immunotherapy for the recurrent attacks, with the mycophenolate, the azathioprine or the rituximab in the selected cases. The aquaporin-four antibody neuromyelitis optica spectrum disorder is the severe form with the poor recovery, and it demands the early maintenance immunotherapy with the rituximab, the mycophenolate or the satralizumab to prevent the relapse and the disability. The multiple-sclerosis-associated optic neuritis is treated with the disease-modifying therapy when the multiple sclerosis is confirmed by the magnetic resonance imaging. [9][10]
Specific Subtypes & Scenarios
The idiopathic intracranial hypertension is the scenario that the boards probe most directly, and the candidate who holds the Friedman criteria carries it. The Friedman criteria require the papilloedema or the sixth-nerve palsy, the normal neurological examination except for the cranial-nerve palsy, the normal neuroimaging that excludes the mass, the hydrocephalus and the venous cause, the normal cerebrospinal fluid composition, and the elevated opening pressure above two hundred and eighty millimetres of cerebrospinal fluid in the child. The secondary intracranial hypertension is the syndrome that fulfils the criteria but has the identifiable cause, the venous sinus thrombosis, the drug, the infection or the systemic disease, and it is treated by the cause. The candidate who distinguishes the idiopathic from the secondary is the candidate who does not miss the treatable cause. [1][2]
The myelin oligodendrocyte glycoprotein antibody disease is the scenario that defines the modern optic neuritis, and it is the commonest antibody-mediated form in the child. The disease presents with the bilateral optic neuritis, the disc swelling, the frequent association with the acute disseminated encephalomyelitis in the younger child, and the generally favourable recovery of the visual acuity. The relapse is the rule, and the recurrent optic neuritis and the transverse myelitis are the features that demand the maintenance immunotherapy. The aquaporin-four antibody neuromyelitis optica spectrum disorder is the severe form, and it presents with the severe bilateral optic neuritis, the poor recovery, the longitudinally extensive transverse myelitis and the area-postrema syndrome of the hiccups, the nausea and the vomiting. The candidate who links the antibody to the prognosis demonstrates the depth. [9][10]
The Friedman criteria for the pseudotumour cerebri syndrome
The optic neuritis of the acute disseminated encephalomyelitis is the scenario that connects the optic nerve to the broader demyelination, and it is the commonest association in the younger child. The acute disseminated encephalomyelitis is the post-infectious demyelinating disease of the central nervous system, and it presents with the encephalopathy, the multifocal neurological deficit and the bilateral optic neuritis in the child under ten years. The magnetic resonance imaging shows the bilateral, the multifocal and the poorly demarcated lesions, and the recovery is generally complete with the corticosteroid. The multiphasic disseminated encephalomyelitis and the overlap with the myelin oligodendrocyte glycoprotein antibody disease are the nuances that the boards reward the candidate who can name. [7][8]
Complications & Pitfalls
The complications of the papilloedema divide into the disease-related and the treatment-related, and the candidate who holds both together manages the patient as well as the diagnosis. The disease-related complication is the vision loss, and it is the complication that drives the urgency. The chronic papilloedema produces the secondary optic atrophy, the loss of the retinal ganglion cell axons and the permanent vision loss, and the visual fields show the constriction, the enlargement of the blind spot and the nasal steps. The treatment-related complications are the acetazolamide toxicity, the paraesthesia, the taste disturbance, the metabolic acidosis and the renal stones, and the surgical complications of the optic nerve sheath fenestration and the shunt, the infection, the failure and the overdrainage. [2][3]
The complications of the optic neuritis are the vision loss and the relapse, and the antibody defines the trajectory. The vision loss of the acute attack is usually partial and recoverable in the child, but the severe attack of the aquaporin-four disease may leave the permanent blindness. The relapse is the feature of the antibody-mediated disease, and the recurrent optic neuritis of the myelin oligodendrocyte glycoprotein disease and the neuromyelitis optica spectrum disorder produce the cumulative damage and the disability. The multiple sclerosis is the long-term risk of the idiopathic optic neuritis with the brain lesions, and the disease-modifying therapy reduces the relapse and the disability. [9][10]
The classic diagnostic pitfalls are the ones the examiner probes, because they are the points where the diagnosis is missed or the harm is done. The disc swelling attributed to the benign drusen without the optical coherence tomography, the headache attributed to the migraine without the fundoscopy, the visual loss attributed to the functional without the swinging-flashlight test, and the lumbar puncture performed before the neuroimaging are the errors that change the outcome. The failure to measure the opening pressure, the failure to send the antibody testing on the optic neuritis, and the failure to surveil the vision of the intracranial hypertension are the mistakes that cost the sight. The candidate who names the pitfalls demonstrates the safety-critical awareness. [1][6]
Prognosis & Disposition
The prognosis of the papilloedema depends on the cause and the speed of the treatment, and the vision is the outcome that the boards probe. The idiopathic intracranial hypertension, treated early with the weight loss and the acetazolamide and the surveillance, carries the generally good prognosis, with the resolution of the papilloedema and the preservation of the vision in the majority. The vision loss occurs in the minority, and it is the complication that the surveillance is designed to catch, because the field loss may appear without the symptom. The secondary intracranial hypertension carries the prognosis of the cause, and the venous sinus thrombosis, the tumour and the meningitis demand the targeted treatment. [2][4]
The prognosis of the optic neuritis depends on the antibody and the brain lesions, and the candidate who links the antibody to the recovery demonstrates the modern reasoning. The myelin oligodendrocyte glycoprotein antibody optic neuritis carries the generally favourable recovery of the visual acuity, with the relapse the main concern. The aquaporin-four antibody optic neuritis carries the poor recovery and the severe cumulative disability, and it demands the early maintenance immunotherapy. The multiple-sclerosis-associated optic neuritis carries the risk of the relapse and the long-term disability driven by the brain lesions on the magnetic resonance imaging, and the disease-modifying therapy reduces the progression. The recent multicentre studies confirm the recovery and the relapse in the paediatric cohorts. [9][11]
The disposition of the child is the multidisciplinary team, because the diagnosis, the surveillance and the treatment demand the neurology, the ophthalmology and the neurosurgery. The child with the idiopathic intracranial hypertension is managed jointly by the neurology and the ophthalmology, with the regular review of the vision and the disc. The child with the optic neuritis is managed by the neurology and the ophthalmology, with the antibody testing and the magnetic resonance imaging at the diagnosis and the follow-up. The child with the structural cause is managed by the neurosurgery and the oncology. The family is counselled about the diagnosis, the surveillance and the prognosis, and the school and the social work are engaged for the support. [1][8]
Special Populations
The infant and the young child with the open skull is the patient in whom the papilloedema may be absent, and the candidate who holds this fact demonstrates the depth. The open sutures and the fontanelle of the infant allow the skull to expand and to decompress the raised pressure, and the papilloedema may not develop, while the bulging fontanelle, the increasing head circumference, the sunset sign and the developmental regression are the signs of the raised pressure in the infant. The optic nerve sheath fenestration and the shunt are the surgical options, and the surveillance of the vision is the challenge in the non-verbal child. The candidate who links the open skull to the absent papilloedema demonstrates the paediatric reasoning. [2][5]
The adolescent with the obesity and the IIH is the patient in whom the weight loss transforms the outcome, and the approach is shaped by the lifestyle and the multidisciplinary support. The obese adolescent girl is the classic phenotype of the idiopathic intracranial hypertension, and the weight loss of the five to ten percent may resolve the papilloedema, reduce the headache and spare the vision. The lifestyle intervention, the dietetic support, the exercise and the behavioural therapy are the foundation, and the bariatric surgery is the option for the severe obesity and the refractory disease. The mental health and the eating-disorder screening are the part of the care, because the weight loss is the long and the hard road. [2][4]
The socioeconomic disadvantage, the remoteness and the migrant or the refugee status affect the access to the ophthalmology, the neuroimaging and the specialist care, and the indigenous and the remote populations carry the later presentation and the worse outcome in the regions where the access is limited. The tele-ophthalmology and the regional outreach are the part of the equitable care, and the candidate who acknowledges the social determinants demonstrates the depth. The family from the remote area may face the prolonged separation during the treatment, and the social work, the educational liaison and the telehealth are part of the multidisciplinary care. [2][3]
Evidence, Guidelines & Regional Differences
The landmark evidence for the intracranial hypertension is the Friedman revised criteria and the body of the paediatric and the adult studies that have refined the diagnosis and the treatment. The Friedman criteria, published in the Neurology in twenty-thirteen, unified the pseudotumour cerebri syndrome and set the opening pressure above two hundred and eighty millimetres of cerebrospinal fluid in the child, and they are the criteria that every board rewards the candidate who can cite. The adult Idiopathic Intracranial Hypertension Treatment Trial established the role of the acetazolamide and the weight loss, and the paediatric literature has adapted the findings to the child, with the recent reviews by Aylward and Brun synthesising the evidence. [1][3]
The landmark evidence for the optic neuritis is the Optic Neuritis Treatment Trial and the modern antibody era, and the candidate who links the two demonstrates the evolution. The Optic Neuritis Treatment Trial, the adult study of the nineteen-nineties, established the intravenous methylprednisolone over the oral steroid and predicted the multiple-sclerosis risk from the brain lesions. The modern era has added the antibody testing, and the myelin oligodendrocyte glycoprotein and the aquaporin-four antibodies have redefined the prognosis and the treatment. The International Pediatric Multiple Sclerosis Study Group criteria of twenty-thirteen set the definitions for the paediatric demyelinating disease, and the recent multicentre studies of the visual outcomes have refined the prognosis. [7][9]
The standard of care across the high-resource regions, including Australasia, the United Kingdom, the United States and Canada, is the multidisciplinary management by the neurology, the ophthalmology and the neurosurgery, with the magnetic resonance imaging and the venography, the lumbar puncture and the optical coherence tomography. The acetazolamide and the weight loss are the standard for the idiopathic intracranial hypertension, and the intravenous methylprednisolone is the standard for the acute optic neuritis. The antibody testing for the myelin oligodendrocyte glycoprotein and the aquaporin-four is the standard for the optic neuritis, and the maintenance immunotherapy for the relapsing forms is the standard. The regional differences are concentrated in the access and the timing, with the rural and the remote populations carrying the later presentation.
[1][9]The controversies are the ones that the candidate can discuss without pretending to resolve them. The optimal duration of the acetazolamide and the threshold for the surgery in the paediatric intracranial hypertension, the role of the venous sinus stenting, the optimal maintenance immunotherapy for the myelin oligodendrocyte glycoprotein disease, and the role of the plasma exchange and the intravenous immunoglobulin for the severe optic neuritis are the open questions. The evidence is weakest in the rare antibody-negative optic neuritis and in the resource-limited setting, where the access to the antibody testing and the magnetic resonance imaging is limited. The candidate who names the controversies demonstrates the mature reasoning the boards reward. [3][10]
Exam Pearls
The high-yield facts for the examination are the ones that the examiner probes and that the candidate must carry without hesitation. The papilloedema as the bilateral disc swelling of the raised pressure, the Friedman criteria with the opening pressure above two hundred and eighty millimetres of cerebrospinal fluid, the Frisén grading, the neuroimaging before the lumbar puncture, and the acetazolamide at fifteen to twenty-five milligrams per kilogram per day are the core of the intracranial hypertension. The swinging-flashlight test and the relative afferent pupillary defect, the antibody testing and the intravenous methylprednisolone at twenty to thirty milligrams per kilogram per day to a maximum of one gram are the core of the optic neuritis. The pseudopapilloedema of the buried drusen and the optical coherence tomography complete the picture. [1][8]
The swinging-flashlight test is the single most testable skill in the topic, and the principle is simple and absolute. The light is swung between the two eyes in the dim room, holding for two to three seconds on each, and the normal pupil constricts to the light in either eye, while the affected eye with the optic nerve lesion dilates paradoxically when the light swings to it, because the reduced input is perceived as the dimming. The test is performed in every child with the acute visual loss, and the relative afferent pupillary defect is the sign that points to the optic nerve. The candidate who performs the test on every child with the visual loss, and who orders the neuroimaging before the lumbar puncture on every child with the disc swelling, is the candidate who carries the safety and the topic. [8][11]
References
- [1]Friedman DI, Liu GT, Digre KB Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology, 2013.PMID 23966248
- [2]Aylward SC, Way AL Pediatric Intracranial Hypertension: a Current Literature Review. Curr Pain Headache Rep, 2018.PMID 29441432
- [3]Brun BN, Aylward SC Pediatric Intracranial Hypertension: A Spotlight on Imaging, the Idiopathic Intracranial Hypertension Treatment Trial, and COVID-19 Associated Cases. Semin Pediatr Neurol, 2021.PMID 34749916
- [4]Botrous M, Surendran S, Sarossy A, et al Incidence of idiopathic intracranial hypertension (IIH) in adults and children: a 14-year population-based study. J Neurol, 2026.PMID 42287435
- [5]Çakmak M, Karagülle M, Kaya FS, et al Clinical and MRI Features in Pediatric Idiopathic Intracranial Hypertension: Focus on Optic Nerve ADC Values. Childs Nerv Syst, 2025.PMID 41307705
- [6]Chang MY, Binenbaum G, Heidary G, et al Imaging Methods for Differentiating Pediatric Papilledema from Pseudopapilledema: A Report by the American Academy of Ophthalmology. Ophthalmology, 2020.PMID 32386809
- [7]Krupp LB, Tardieu M, Amato MP, et al International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: revisions to the 2007 definitions. Mult Scler, 2013.PMID 23572237
- [8]Bonhomme GR, Waldman AT, Balcer LJ, et al Pediatric optic neuritis: brain MRI abnormalities and risk of multiple sclerosis. Neurology, 2009.PMID 19273821
- [9]Lana-Peixoto MA, Talim NC, Christo PP From the Optic Neuritis Treatment Trial to Antibody-Mediated Optic Neuritis: Four Decades of Progress and Unanswered Questions. Biomedicines, 2026.PMID 41751233
- [10]Sriram M, Shivarthi T, Anand V, et al Long-term visual outcomes and treatment-related prognostic variables in pediatric demyelinating optic neuritis: A 10-year retrospective cohort study. Mult Scler Relat Disord, 2026.PMID 42276020
- [11]Joo HJ, Song JR, Lim BC, et al Six-Month Visual Outcomes in Pediatric Optic Neuritis: A Multicenter Study From South Korea. J Neuroophthalmol, 2026.PMID 42212697