Paeds · ophthalmology
Preseptal and orbital cellulitis
Also known as Preseptal cellulitis · Periorbital cellulitis · Orbital cellulitis · Postseptal cellulitis · Subperiosteal abscess of the orbit · Chandler classification of orbital complications
Fellowship topic on preseptal and orbital cellulitis in children: the orbital septum as the dividing line between a mild preseptal infection and a sight-threatening postseptal one; the Chandler five-stage classification of orbital complications of sinusitis from inflammatory oedema through orbital cellulitis, subperiosteal abscess and orbital abscess to cavernous sinus thrombosis; the sinogenic pathophysiology through the thin lamina papyracea and the valveless venous drainage; the Staphylococcus aureus, Streptococcus pyogenes, S. pneumoniae and Streptococcus anginosus microbiology; the clinical signs that separate the well child with preseptal swelling from the sick child with proptosis, ophthalmoplegia and visual loss; the role of contrast CT and the medical-versus-surgical decision for subperiosteal abscess including the age-based Garcia-Harris criteria; stepwise oral and intravenous antibiotic management; the intracranial and visual complications; and ANZ, UK and North American guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old brought to the emergency department with a swollen, red eye. Yesterday it was a mildly puffy lid after a small scratch; today the whole lid is tense and erythematous, but the eye itself looks normal, the child can move it in every direction without pain, the vision is fine, and the child is playful and afebrile. This is the common, benign end of the spectrum — preseptal cellulitis — and it will settle with oral antibiotics and safety-net advice. Now picture a different four-year-old, brought in the same evening with a swollen, red eye that protrudes, cannot look to the side, hurts when it tries, and is accompanied by fever and a listless child. This is the dangerous end — orbital cellulitis — and it will not settle without a hospital, an intravenous line and a scan. Recognising which child is which, and acting fast on the second, is the whole skill. [1] [3]
Periorbital infection is divided by the orbital septum, a fibrous sheet continuous with the periosteum of the orbital rim that forms the anterior boundary of the orbit. Preseptal (periorbital) cellulitis is infection of the eyelid and periorbital soft tissues anterior to this septum; it is common, usually mild, and most often follows a local skin breach, conjunctivitis or trauma. Orbital (postseptal) cellulitis is infection posterior to the septum, involving the orbital fat, extraocular muscles and neurovascular structures; it is uncommon but sight- and life-threatening, and it most often spreads from adjacent paranasal sinusitis. [2] [4]
The clinician's task is layered. The first layer is triage — separating the well child with anterior lid swelling from the sick child whose infection has crossed the septum, using the orbital signs that examiners test every time. The second layer is investigation — deciding when contrast CT is needed and reading it for a subperiosteal or orbital collection. The third layer is treatment — oral antibiotics for uncomplicated preseptal disease, intravenous antibiotics for orbital disease, and a surgical decision for the abscess that will not resolve or that threatens vision. [5] [11]
Classification
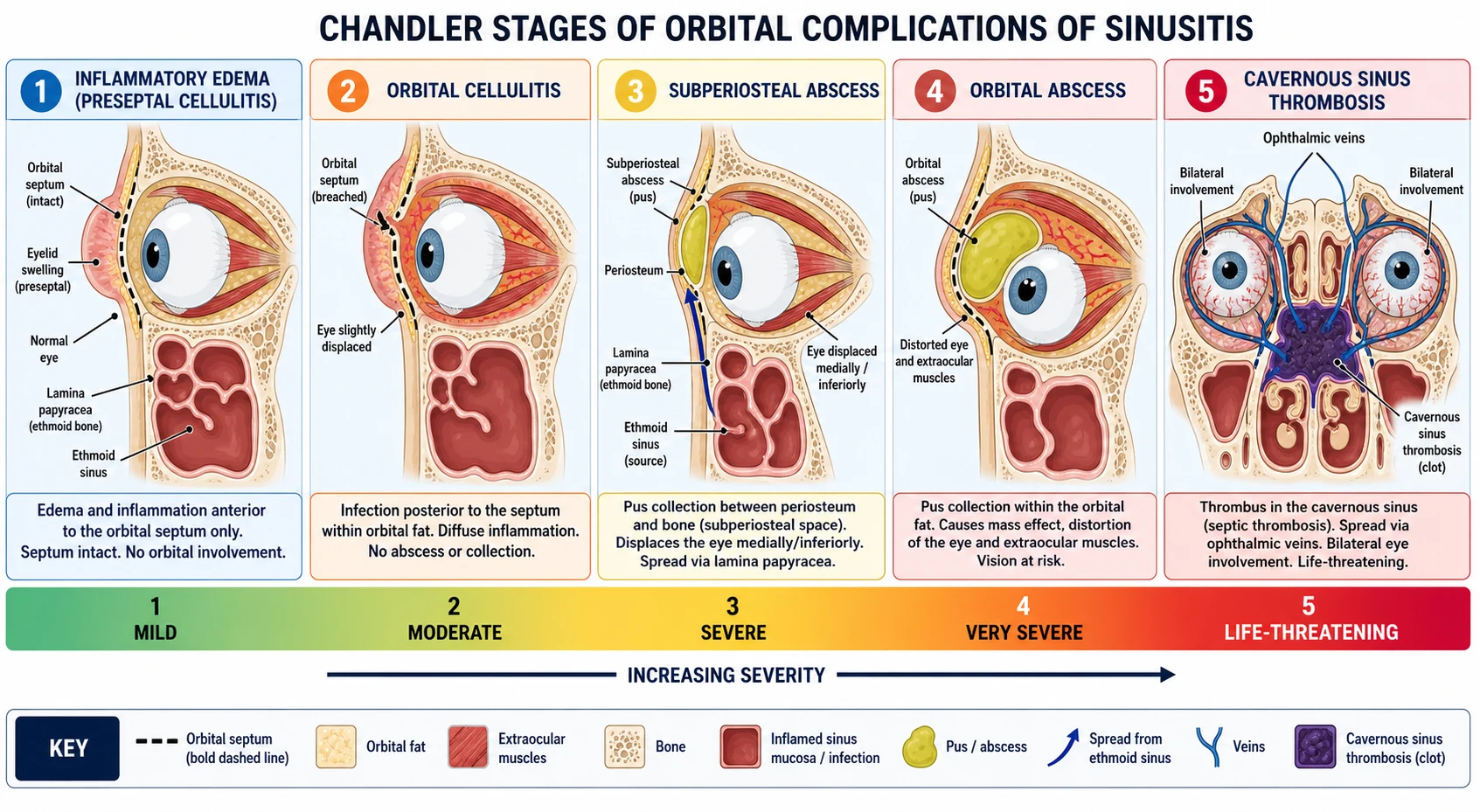
The Chandler classification, introduced in 1970 and still the universal teaching framework, frames the orbital complications of sinusitis as a five-stage progression of increasing severity. It is a clinical and radiological continuum, not a rigid ladder, and a child may present at any stage; but knowing the stages organises the assessment and the urgency. [2] [4]
Chandler stage 1 — inflammatory oedema is the earliest manifestation: eyelid swelling from impaired venous drainage of the orbit, with infection still confined to the sinus and the orbital septum intact. This corresponds to preseptal cellulitis in most modern usage. Stage 2 — orbital cellulitis is the infiltration of orbital fat and soft tissues by oedema and inflammatory cells posterior to the septum, without a discrete abscess. Stage 3 — subperiosteal abscess is a collection of pus between the orbital periosteum and the adjacent orbital wall, most often the medial wall from ethmoid disease, that displaces the orbital contents. [2]
Stage 4 — orbital abscess is a collection of pus within the orbital fat itself, distorting the globe, extraocular muscles and optic nerve, and carrying the highest risk of permanent visual loss. Stage 5 — cavernous sinus thrombosis is the thrombosis of the cavernous sinus via the valveless ophthalmic venous drainage, producing bilateral orbital signs, cranial nerve palsies and systemic toxicity — the end of the progression and the one most likely to kill. [4] [2]
Epidemiology & Risk Factors
Orbital cellulitis is predominantly a disease of young children, reflecting the early development of the ethmoid sinuses — the only paranasal sinuses present at birth — and the frequency of viral upper-respiratory infection and sinusitis in this age group. The median age at presentation is in the mid-primary-school years, and the incidence falls through adolescence. Preseptal cellulitis is far commoner than orbital cellulitis across all ages, and the two diseases have distinct demographic and aetiological profiles that the 262-case retrospective review helped define. [1] [3]
The single most important risk factor for orbital cellulitis is paranasal sinusitis, present in the great majority of cases, with ethmoiditis the dominant source because the lamina papyracea is thin, dehiscent and allows direct spread. Other risk factors include local trauma or surgery, dacryocystitis, dental infection, an immunocompromised state, and any cause of impaired local or systemic defence. Preseptal cellulitis more often follows a superficial skin breach — an insect bite, an abrasion, a chalazion or conjunctivitis. The 10-year review of hospitalised children confirmed that sinusitis underlies most orbital disease and that preseptal and orbital infections are epidemiologically and clinically distinct. [5] [9]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline frames periorbital and orbital cellulitis as a high-priority presentation requiring early distinction of preseptal from orbital disease, prompt intravenous antibiotics for the latter, and coordinated care between paediatrics, ophthalmology and ear-nose-and-throat surgery. The Australian Therapeutic Guidelines set the empiric antibiotic choices, with regional variation in methicillin-resistant Staphylococcus aureus prevalence guiding the addition of vancomycin or clindamycin where appropriate. Access to paediatric ophthalmology and ENT services shapes the retrieval and telehealth pathways for rural and remote children. [5]
The microbiology has shifted with immunisation and antimicrobial pressure. Haemophilus influenzae type b, once a feared cause of invasive periorbital disease in young children, is now rare in immunised populations. Staphylococcus aureus and Streptococcus pyogenes are the leading organisms in both preseptal and orbital disease, with Streptococcus pneumoniae and the Streptococcus anginosus group important in sinogenic orbital cellulitis and subperiosteal abscess. Anaerobes contribute when dental disease or chronic sinusitis is the source, and community-acquired MRSA is a consideration where locally prevalent. [1] [4]
Pathophysiology
Why does a child with a common cold develop a sight-threatening orbital infection? The answer lies in the anatomy of the orbit and its relationship to the sinuses, and in the valveless venous drainage that connects the orbit to the cavernous sinus. The ethmoid sinuses are present at birth and sit immediately medial to the orbit, separated only by the lamina papyracea, a paper-thin and often dehiscent bony wall. Ethmoid sinusitis — itself usually a complication of viral upper-respiratory infection — can erode or spread through this barrier directly into the orbit, which is why ethmoiditis is the dominant sinogenic source of orbital cellulitis in children. [1] [4]
Once infection crosses the lamina papyracea it enters the orbital space posterior to the septum, provoking oedema and inflammatory infiltration of the orbital fat — Chandler stage 2, orbital cellulitis. The inflamed, swollen tissues raise intraorbital pressure, restrict the extraocular muscles and compress the venous and lymphatic drainage, producing proptosis, chemosis and limitation of eye movement. If pus collects between the periosteum and the orbital wall it forms a subperiosteal abscess (stage 3); if it collects within the orbital fat it forms an orbital abscess (stage 4). Each step raises intraorbital pressure further and brings the optic nerve closer to irreversible ischaemic injury. [2] [8]
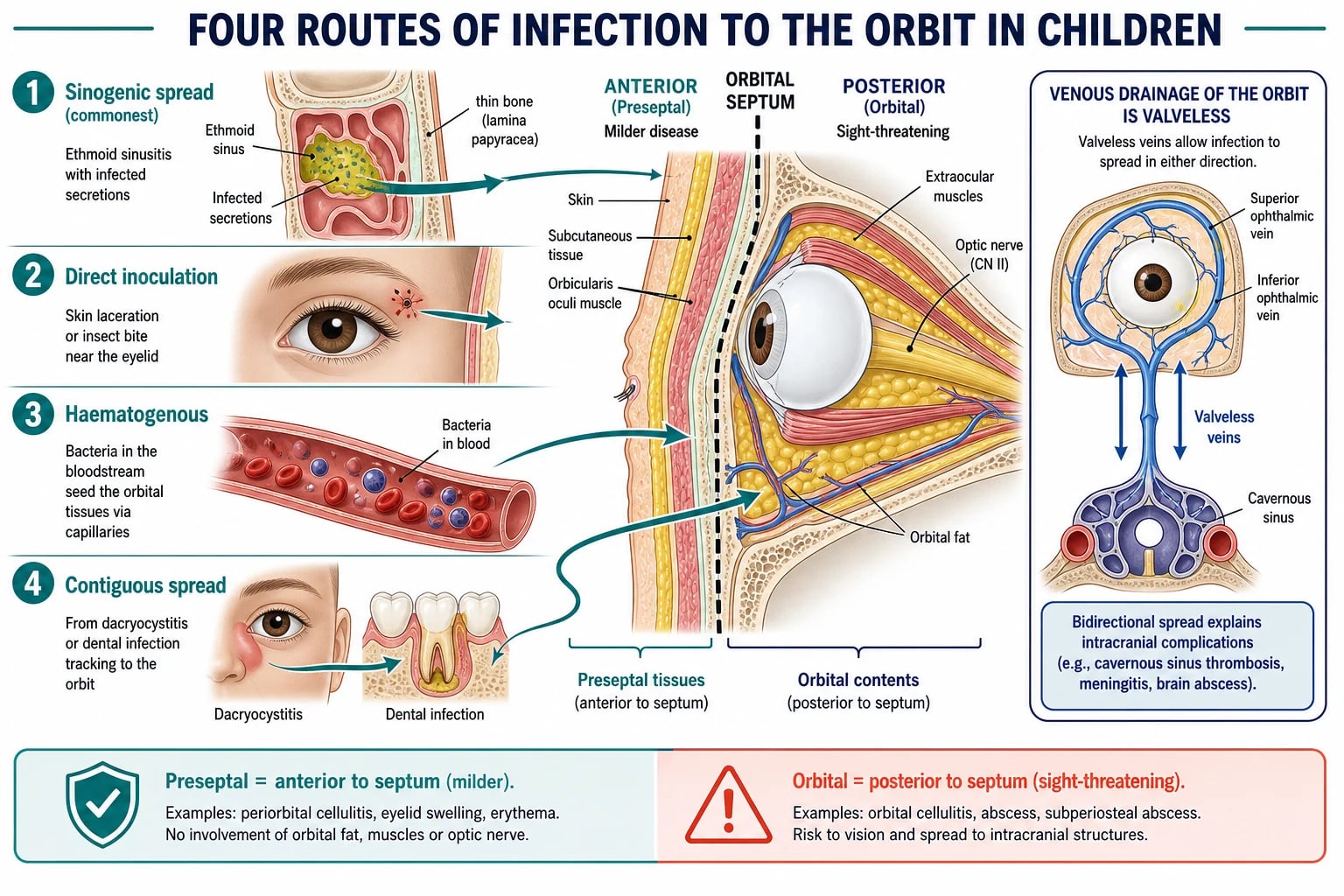
The valveless ophthalmic veins are the key to the most dangerous complication. The superior and inferior ophthalmic veins drain the orbit into the cavernous sinus, and because they have no valves, infection can track in either direction — from the orbit into the cavernous sinus, causing septic cavernous sinus thrombosis (stage 5), or from the face into the orbit. This is why infection of the skin of the upper face and nose in the so-called danger triangle can, in principle, spread to the orbit and the cavernous sinus, and why bilateral orbital signs with cranial nerve palsies are the hallmark of cavernous sinus thrombosis. [4]
Preseptal cellulitis follows a different and less dangerous course. Infection enters the eyelid and periorbital soft tissues anterior to the septum through a local breach — an insect bite, an abrasion, a chalazion, or a skin lesion — or spreads from adjacent conjunctivitis or dacryocystitis. Because the septum is intact, the infection cannot reach the orbital contents, and the eye remains structurally undisturbed: no proptosis, no ophthalmoplegia, no visual compromise. The distinction between the intact-septum and breached-septum states is the entire clinical and prognostic difference between the two diseases. [3] [9]
Clinical Presentation
The child with preseptal cellulitis presents with unilateral eyelid swelling and erythema, often preceded by a recognisable portal of entry — an insect bite, a scratch, a chalazion or conjunctivitis. The swelling is confined to the lid and periorbital skin, the underlying eye is white and quiet, and there is no proptosis, no chemosis of the conjunctiva, no limitation of eye movement, no pain on movement, and no visual disturbance. The child is typically afebrile and well, though low-grade fever may accompany more extensive lid involvement. Regional lymphadenopathy may be present. [3] [9]
The child with orbital cellulitis presents quite differently, and the difference is in the orbital signs. Unilateral lid swelling and erythema are accompanied by proptosis (forward displacement of the globe), chemosis (conjunctival oedema), limitation of eye movement (ophthalmoplegia), and pain on eye movement. The child is typically febrile and systemically unwell, with a recent or concurrent upper-respiratory infection. Decreased visual acuity, impaired colour vision and a relative afferent pupillary defect indicate optic nerve compromise and are the signs that demand immediate escalation. The ten-year review of hospitalised children confirmed that the presence of these orbital signs reliably separates orbital from preseptal disease. [1] [5]
A child with a subperiosteal abscess may have the orbital signs of cellulitis plus a globe displaced in a direction determined by the abscess site — medially and inferiorly displaced for a medial-wall abscess from ethmoid disease, or downward for a superior-wall collection. A child with cavernous sinus thrombosis presents with bilateral orbital signs, cranial nerve palsies (especially III, IV, V and VI), headache, meningism and progressive systemic deterioration. These advanced presentations are emergencies of the highest order. [4] [10]
Differential Diagnosis
The differential of the swollen red eye in a child turns on whether the orbital signs are present and on the tempo of the illness. For the child without proptosis or ophthalmoplegia, allergic eyelid oedema is painless, bilateral and itchy, and settles with antihistamines. Insect bites and contact dermatitis produce localised swelling without systemic features. Viral conjunctivitis causes redness and discharge but not the tense lid induration of cellulitis. A chalazion or hordeolum produces a localised lid lump. [3] [9]
[9]For the child with orbital signs, the dangerous differentials must be excluded. Orbital cellulitis is the commonest cause of proptosis with inflammation in a febrile child, but idiopathic orbital inflammation (orbital pseudotumour), rhabdomyosarcoma of the orbit, retinoblastoma with orbital extension, leukaemic infiltration, and orbital foreign body with infection can all mimic it. A subperiosteal abscess and orbital abscess are stages within the cellulitis spectrum rather than separate differentials, but they must be sought on imaging. Dacryocystitis produces swelling medial to the inner canthus with epiphora, and periorbital erysipelas produces a sharply demarcated raised rash. [4] [5]
The critical error is to dismiss orbital cellulitis as preseptal disease. A child with any orbital sign — proptosis, limitation of movement, pain on movement, visual change or an abnormal pupil — has postseptal disease, and the failure to recognise this, to image and to admit is the error that costs vision and lives. The threshold to assess for the orbital signs, and to image if any are present, must be deliberately low. [1] [8]
Clinical & Bedside Assessment
The assessment of the child with periorbital swelling is a structured search for the orbital signs, because their presence or absence determines the entire management pathway. Begin with the history: onset and progression of swelling, any preceding upper-respiratory infection, any portal of entry such as trauma or insect bite, any pain in or behind the eye, any fever or systemic upset, and the immunisation history — particularly Hib vaccination in a young child. [1] [3]
The examination must include a full orbital assessment, which is where the decision is made. Look for lid swelling and erythema (present in both preseptal and orbital disease), then systematically test for the orbital signs: proptosis (assess from above and the side, comparing the two eyes), eye movement in all directions of gaze and any pain or limitation, visual acuity (age-appropriate method, comparing to the other eye), colour vision (a sensitive indicator of optic nerve function), pupil reactions including a relative afferent pupillary defect, and fundoscopy for optic disc swelling. Examine the nose and oropharynx for sinusitis, the teeth for dental infection, and the skin for portals of entry. [4] [1]
The orbital signs — PROVe
Assess the systemic state directly. Fever, tachycardia, hypotension, lethargy and signs of meningism signal invasive disease, sepsis or intracranial extension. In the very young child, who cannot reliably cooperate with visual acuity or eye-movement testing, the threshold to treat as orbital disease and to image is lower, because the signs may be harder to elicit and the consequences of missing orbital involvement more severe. A child who is systemically unwell with a swollen eye is assumed to have orbital cellulitis until imaging proves otherwise. [4] [11]
Investigations
Investigation is driven by the clinical assessment. The well child with preseptal cellulitis, normal eye movements and normal vision needs no imaging and no blood tests — the diagnosis is clinical, and oral antibiotics are started empirically. Blood cultures and inflammatory markers are not routinely needed for uncomplicated preseptal disease, though they may guide management in the systemically unwell child. [3] [9]
The child with any orbital sign requires contrast-enhanced computed tomography of the orbits and paranasal sinuses. The indications for CT are proptosis, limitation of eye movement, pain on eye movement, decreased visual acuity or a relative afferent pupillary defect; systemic toxicity; no improvement or deterioration after 24 to 48 hours of intravenous antibiotics; and any suspicion of a subperiosteal or orbital abscess or intracranial extension. CT identifies the sinus source, defines a subperiosteal or orbital abscess and its extent, and reveals intracranial complications such as epidural or subdural empyema. The role of CT in managing orbital complications was established by the ethmoiditis series that defined the imaging-based approach to subperiosteal abscess. [6] [1]
At the Royal Children's Hospital Melbourne and in Australian and New Zealand paediatric practice, the guideline is to obtain contrast CT of the orbits and sinuses when orbital signs are present, when the child fails to improve on intravenous antibiotics at 24 to 48 hours, or when intracranial extension is suspected. Magnetic resonance imaging is reserved for suspected intracranial or cavernous sinus involvement where CT is equivocal, because it better defines soft-tissue and vascular complications. MRI should not delay intravenous antibiotics or surgical intervention in the deteriorating child. [5]
Microbiological investigation is opportunistic rather than routine. Blood cultures are obtained in the systemically unwell child before antibiotics but are often negative. Pus from a surgically drained abscess should always be sent for Gram stain, culture and susceptibility testing to guide de-escalation, and the Streptococcus anginosus group and Staphylococcus aureus are the organisms most often isolated from subperiosteal abscesses. In the child who does not respond to empiric therapy, culture results direct the switch to a targeted agent. [1] [8]
Management — Resuscitation
Resuscitation belongs to the child with orbital cellulitis and systemic compromise. The red flags are a child with proptosis, ophthalmoplegia or visual impairment who is febrile and toxic; a child with a rapidly progressive orbital abscess threatening the optic nerve; and a child with bilateral orbital signs, cranial nerve palsies or meningism suggesting cavernous sinus thrombosis or intracranial extension. Any of these warrants urgent assessment, intravenous access and senior paediatric, ophthalmology and ENT review. [4] [1]
The immediate priorities are to secure the airway and circulation if the child is shocked, to obtain intravenous access, to take blood cultures, and to start broad-spectrum intravenous antibiotics without delay. Do not wait for imaging or culture results in the deteriorating child — the empiric regimen must cover Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae and the Streptococcus anginosus group, with anaerobic cover if dental or chronic sinus disease is suspected and MRSA cover if locally prevalent or the child has risk factors. [8] [11]
Assess and document the vision at presentation and serially thereafter, because deterioration in visual acuity, colour vision or the pupillary reaction is the trigger for urgent surgical decompression. Escalate to intensive care for the child with cavernous sinus thrombosis, intracranial extension, or septic shock. Separate resuscitation from definitive therapy in your mind: the well child with preseptal cellulitis needs oral antibiotics and review, while the sick child with orbital cellulitis needs the hospital, the intravenous line, the scan and the multidisciplinary team. [4] [5]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to whether the septum has been crossed. Preseptal cellulitis in a well child takes oral antibiotics in the community; orbital cellulitis takes admission and intravenous antibiotics with urgent ophthalmology and ENT referral; and a subperiosteal or orbital abscess takes surgical drainage when medical therapy fails or vision is threatened. The art is to recognise the stage, to choose the right intensity, and to reassess relentlessly. [8] [11]
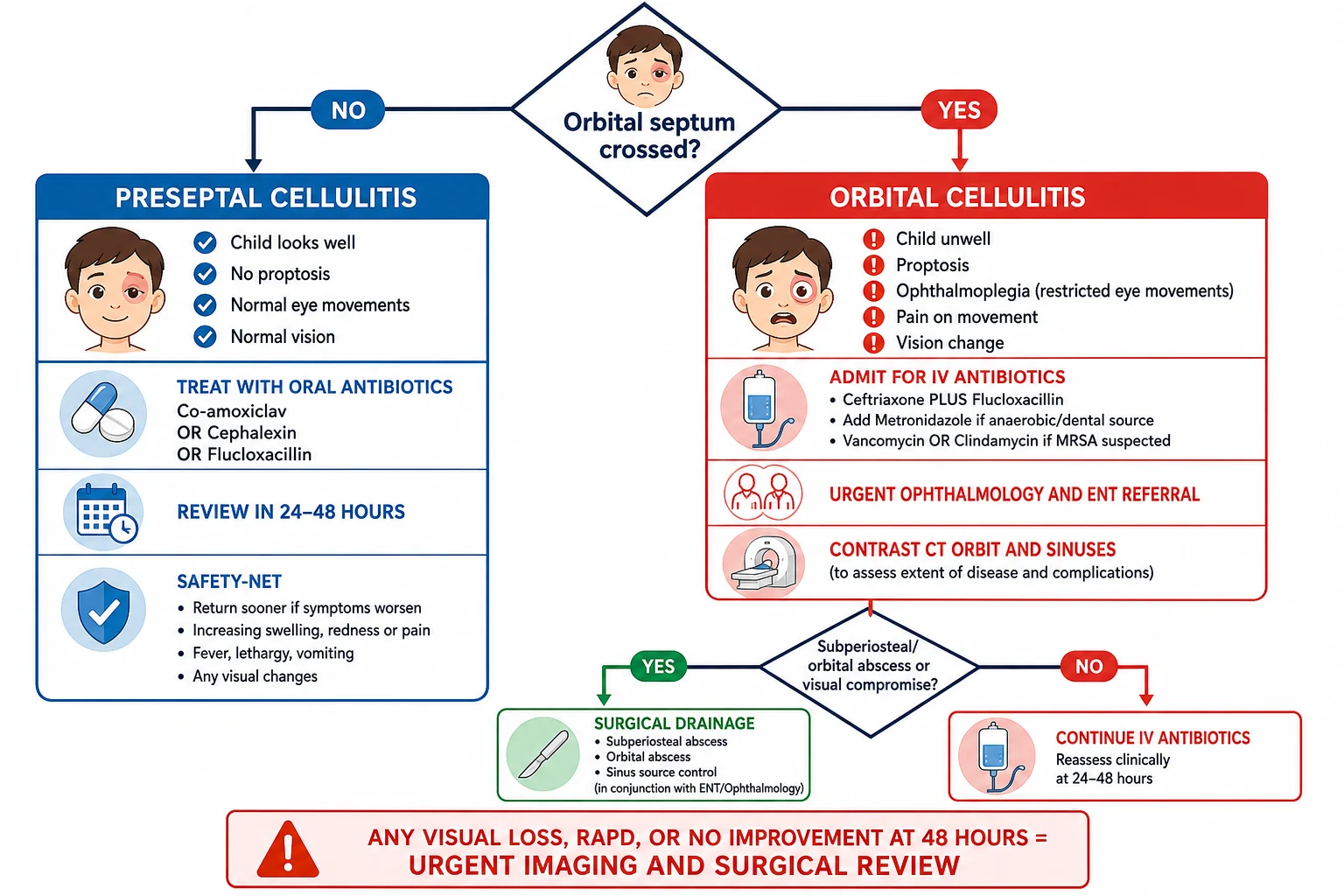
For preseptal cellulitis in a well child, oral antibiotics covering Staphylococcus aureus and streptococci are first-line. A common choice is co-amoxiclav (amoxicillin with clavulanate) orally — for example, child one to five years given five millilitres of the 250/62 suspension twice daily, or weight-based dosing for younger infants — or cephalexin 25 mg per kilogram (maximum 500 mg) twice daily or flucloxacillin (child one to five years 125 mg four times daily). Give an oral course of five to seven days, advise the family on hygiene and warm compresses, and review at 24 to 48 hours with a clear safety-net to return if orbital signs develop. [3] [9]
Preseptal and orbital cellulitis antibiotic pathway (BNFc / eTG / RCH — confirm locally)
For orbital cellulitis, admit and start intravenous antibiotics immediately after blood cultures. The standard empiric regimen combines ceftriaxone 50 mg per kilogram (maximum 2 g) once daily intravenously with flucloxacillin 25 to 50 mg per kilogram (maximum 2 g) every six hours intravenously, providing cover for the streptococci and staphylococci that dominate paediatric orbital disease. Add metronidazole 7.5 mg per kilogram (maximum 400 mg) every eight hours intravenously when anaerobic organisms are plausible — dental origin, chronic sinusitis, or a large abscess. Add vancomycin (15 mg per kilogram every six hours with monitoring) or clindamycin (10 mg per kilogram every eight hours) when MRSA is suspected or locally prevalent, or when the child is critically ill. [8] [11]
The stepwise periorbital-cellulitis pathway
Assess the orbital signs: if there is proptosis, ophthalmoplegia, pain on movement, visual change or an abnormal pupil, this is orbital cellulitis — admit for intravenous antibiotics.
Preseptal cellulitis in a well child: oral co-amoxiclav or cephalexin or flucloxacillin for five to seven days, with review at 24 to 48 hours and a clear safety-net for orbital signs.
Orbital cellulitis: admit, take blood cultures, start intravenous ceftriaxone plus flucloxacillin, add metronidazole for anaerobic or dental concern and vancomycin or clindamycin for suspected MRSA.
Obtain contrast CT of the orbits and sinuses when orbital signs are present or the child fails to improve at 24 to 48 hours.
Refer urgently to ophthalmology and ENT for combined assessment of the need for surgical drainage.
Surgical drainage for a subperiosteal or orbital abscess that is large, non-medial, fails medical therapy at 48 hours, or causes any visual compromise.
Reassess vision and orbital signs serially; deteriorating vision is the trigger for urgent surgical decompression.
Transition to oral antibiotics on clinical improvement and complete a total course guided by severity and culture results, with follow-up to confirm resolution.
The medical versus surgical decision for subperiosteal abscess is guided by the age-based criteria that the medical-management series established and that subsequent series refined. A child with a medial subperiosteal abscess, age under nine years, and normal vision may be given a trial of intravenous antibiotics with close monitoring, because the abscess in this group is often streptococcal or S. anginosus and may resolve without surgery. Surgical drainage is indicated for any visual compromise, for a non-medial abscess, for a large abscess, for failure to improve after 48 hours of intravenous antibiotics, for intracranial extension, and generally for age nine years or older. Superior subperiosteal abscesses warrant a particularly low threshold for surgery because of their association with the frontal sinus and intracranial spread. [7] [10]
Specific Subtypes & Scenarios
A well child with preseptal cellulitis. This is the bread-and-butter case. Confirm the absence of orbital signs, identify the portal of entry, and give oral antibiotics for five to seven days with review at 24 to 48 hours. Advise warm compresses and hygiene, and give a clear safety-net for spreading redness, fever, pain on eye movement or any visual change. Most cases settle promptly. [3] [9]
A febrile child with orbital cellulitis. This is the admission case. Recognise the orbital signs, take blood cultures, start intravenous ceftriaxone plus flucloxacillin, obtain contrast CT of the orbits and sinuses, and refer urgently to ophthalmology and ENT. Document vision at presentation and reassess it serially. Most children improve within 24 to 48 hours of intravenous therapy; failure to improve is the trigger to look for an abscess. [1] [5]
A child with a subperiosteal abscess. The CT shows a medial-wall collection in a young child with normal vision — give a trial of intravenous antibiotics with close monitoring, because many resolve. The CT shows a large, non-medial or superior collection, or the child has visual compromise or is nine years or older — proceed to surgical drainage. The medical-versus-surgical series established that age, abscess site and visual status drive the decision, and the superior- abscess series reinforced the low surgical threshold for non-medial disease. [7] [10]
A child with an orbital abscess and visual compromise. This is the sight-threatening emergency. Any decrease in visual acuity, colour vision or a relative afferent pupillary defect in a child with orbital cellulitis demands urgent surgical decompression alongside intravenous antibiotics, because optic nerve ischaemia from raised intraorbital pressure becomes irreversible within hours. The priority is drainage to relieve the pressure, not further imaging. [4] [8]
A child with cavernous sinus thrombosis. This is the life-threatening extreme. Bilateral orbital signs, cranial nerve palsies, headache, meningism and progressive systemic deterioration indicate septic thrombosis of the cavernous sinus. Admit to intensive care, give broad-spectrum intravenous antibiotics including MRSA and anaerobic cover, and involve neurology, ophthalmology, ENT and infectious diseases. The mortality remains substantial despite modern treatment. [4]
A child with intracranial extension. Orbital cellulitis can spread to produce an epidural or subdural empyema, a brain abscess, or meningitis. A child with severe headache, neck stiffness, altered conscious state or seizures needs urgent imaging of the brain and intracranial structures, neurosurgical involvement and prolonged intravenous antibiotics. The management patterns series confirmed that intracranial complications, though uncommon, carry the highest morbidity in paediatric complicated sinusitis. [11] [4]
A very young or unvaccinated child. Infants and young children with periorbital cellulitis and systemic upset warrant particular vigilance. In an unvaccinated child, Haemophilus influenzae type b must be considered as a cause of invasive disease, including meningitis and bacteraemia. The threshold to admit, to image and to use a third-generation cephalosporin is lower in the very young, because the signs may be harder to elicit and the consequences of missing invasive disease are severe. [1] [5]
Complications & Pitfalls
The most feared complications are visual loss and intracranial extension. Optic neuropathy from raised intraorbital pressure or direct infection of the optic nerve is the pathway to permanent visual loss, and it is preventable only by prompt recognition and surgical decompression when vision is threatened. Cavernous sinus thrombosis produces bilateral orbital signs, cranial nerve palsies and systemic toxicity. Intracranial complications include epidural and subdural empyema, brain abscess and meningitis, and they carry the highest morbidity in the complicated-sinusitis series. [4] [11]
The cardinal pitfall is mistaking orbital cellulitis for preseptal disease. A child with proptosis, ophthalmoplegia, pain on movement or visual change has postseptal infection, and treating them with oral antibiotics and outpatient review — as one might appropriately do for preseptal cellulitis — allows the infection to progress to abscess, optic neuropathy and intracranial extension. The single most important habit is to examine for the orbital signs in every child with a swollen eye, and to assume orbital disease when any is present or when the child is systemically unwell. [1] [3]
A second pitfall is delaying imaging. The child with orbital signs needs contrast CT without waiting to see whether 48 hours of intravenous antibiotics will resolve them, because an abscess may be present from the outset and may compromise the optic nerve while you wait. Imaging when the orbital signs are present, and again if the child fails to improve, is the discipline that catches the collection in time. [6] [8]
A third pitfall is inadequate empiric antibiotic cover. The regimen must cover Staphylococcus aureus and the streptococci at a minimum, with anaerobic cover for dental or chronic sinus disease and MRSA cover where indicated. A beta-lactam alone may miss MRSA in a high-prevalence region, and the omission of anaerobic cover in a dental-origin abscess may leave a reservoir of infection. Knowing the local microbiology and the source of the infection is part of the prescription. [8] [11]
A fourth pitfall is applying the medical-management trial too broadly. The criteria for a trial of intravenous antibiotics in subperiosteal abscess — young child, medial abscess, normal vision — are narrow, and expanding them to a non-medial, large or superior abscess, or to a child with any visual compromise, risks catastrophic delay in surgical drainage. The surgical threshold is deliberately low outside the narrow medical-trial group. [7] [10]
Prognosis & Disposition
Most preseptal cellulitis resolves completely with five to seven days of oral antibiotics, and the outlook is excellent. Orbital cellulitis in a child who is promptly admitted and treated with intravenous antibiotics has a good prognosis in the majority, with full recovery of vision and resolution of the infection. The morbidity and mortality rise sharply when the presentation is delayed, when an abscess is missed or undertreated, or when intracranial extension or cavernous sinus thrombosis occurs. [1] [5]
Disposition follows the stage. Admit the child with any orbital sign for intravenous antibiotics, imaging and multidisciplinary review. Manage the well child with preseptal cellulitis in the community with oral antibiotics and a 24- to 48-hour review, provided a clear safety-net is given and the family can return. The threshold for admitting the very young, the systemically unwell and the child who cannot be reliably examined is deliberately low. [3] [9]
At discharge from hospital, transition to oral antibiotics to complete a total course guided by the severity and the culture results, confirm resolution of the orbital signs and the vision, and arrange ophthalmology follow-up. Address any underlying sinus disease or dental source that predisposes to recurrence, and give the family a clear safety-net for spreading redness, fever, pain on eye movement or visual change. Recurrence is uncommon but reflects uncontrolled sinus or dental disease and warrants ENT reassessment. [5] [11]
Special Populations
Neonates and infants are at higher risk of invasive disease and may not show the orbital signs reliably. The threshold to admit, to image and to treat with intravenous antibiotics is lower, because the thin orbital bones, the immature immune response and the difficulty of examining vision combine to make under-diagnosis dangerous. A febrile infant with periorbital swelling is assumed to have orbital disease until proven otherwise. [1] [5]
Immunocompromised children are at risk of severe, persistent and atypical infection. The organism may be unusual, the disease more invasive, and the response to standard therapy slower. Early imaging, broad empiric cover and a lower surgical threshold are appropriate when these children present with orbital cellulitis. [4] [11]
Unvaccinated children may be exposed to Haemophilus influenzae type b, which in the prevaccine era was a feared cause of invasive periorbital disease, bacteraemia and meningitis in young children. In an unvaccinated child with periorbital cellulitis and systemic upset, consider Hib and cover it with a third-generation cephalosporin while awaiting cultures. [1]
Aboriginal and Torres Strait Islander, Maori and Pasifika children, and refugee, asylum-seeking and migrant families may carry a higher burden of respiratory infection and sinusitis and may face barriers to timely assessment. Ensure culturally safe, equitable care delivered with the family, use trained interpreters, and arrange early retrieval and telehealth support for rural and remote children so that distance does not delay the recognition and treatment of orbital cellulitis. [5]
Evidence, Guidelines & Regional Differences
The clinical evidence base for paediatric orbital cellulitis is built on large retrospective case series and institutional reviews rather than randomised trials, reflecting the nature of the disease. The series of orbital cellulitis in children defined the epidemiology, the microbiology and the clinical course, while the 262-case review of preseptal and postseptal infections established that the two are distinct diseases with different sources and severities. The 10-year review of hospitalised children confirmed sinusitis as the dominant source of orbital disease and the reliability of the orbital signs in distinguishing it from preseptal infection. [1] [3] [5]
Medical treatment of pediatric subperiosteal orbital abscess secondary to sinusitis
Population: Children with subperiosteal orbital abscess secondary to sinusitis, assessed for outcomes with intravenous antibiotic therapy as an alternative to immediate surgical drainage.
Key finding
Selected children with subperiosteal abscess — particularly young children with medial abscesses and preserved vision — could be managed successfully with intravenous antibiotics and close observation, establishing the medical-management approach that the age-based criteria later formalised.
Practice change
A trial of intravenous antibiotics is reasonable for a medial subperiosteal abscess in a young child with normal vision, provided vision is monitored closely and the threshold for surgical drainage is preserved for failure or for high-risk features.
The medical-versus-surgical evidence was advanced by the series comparing medical treatment with surgical management, which showed that age, abscess site and visual status predict the success of medical therapy and guide the surgical decision. The characteristics of superior orbital subperiosteal abscesses were defined by the series that identified their association with the frontal sinus and intracranial spread, reinforcing the low surgical threshold for non-medial and superior collections. The management-patterns study of paediatric complicated sinusitis consolidated the contemporary approach across institutions. [8] [10] [11]
Management patterns in pediatric complicated sinusitis
Population: Children with complicated sinusitis including orbital and intracranial complications, reviewed for management patterns, surgical rates and outcomes across a contemporary paediatric otolaryngology service.
Key finding
The majority of children with orbital complications were managed with intravenous antibiotics, with surgical intervention reserved for abscess, visual compromise or failure of medical therapy; intracranial complications, though uncommon, carried the highest morbidity.
Practice change
The stepwise approach — intravenous antibiotics first, surgery for the abscess or the deteriorating child — is supported by contemporary practice, with the threshold for surgery driven by abscess characteristics and visual status.
The regional policy structure is consistent in principle and varies in detail. In the UK, NICE antimicrobial-prescribing guidance and the Royal College of Paediatrics and Child Health guidance set the empiric antibiotic choices and the imaging indications. In Australia and New Zealand, the Royal Children's Hospital Melbourne clinical practice guideline and the Therapeutic Guidelines set the local pathway, with ceftriaxone plus flucloxacillin as the standard empiric regimen and MRSA cover added where prevalent. In North America, the American Academy of Ophthalmology Preferred Practice Pattern and the American Academy of Pediatrics guidance set the management framework. In Canada, the Canadian Paediatric Society guidance mirrors this approach. The controversies — the optimal duration of therapy, the precise surgical threshold, the role of steroids, and the place of MRSA-active agents — are resolved by the same principle in every region: recognise the orbital signs, image promptly, treat with broad intravenous antibiotics, and drain the abscess that fails or threatens vision. [5] [11]
Exam Pearls
- The orbital septum is the dividing line: anterior infection is preseptal (mild, community-managed); posterior infection is orbital (sight- and life-threatening, admitted). [3]
- The Chandler classification of orbital complications of sinusitis is five stages: 1 inflammatory oedema (preseptal), 2 orbital cellulitis, 3 subperiosteal abscess, 4 orbital abscess, 5 cavernous sinus thrombosis. [2]
- The five orbital signs that mean the septum is crossed are proptosis, ophthalmoplegia, pain on eye movement, decreased visual acuity and a relative afferent pupillary defect — any one mandates admission and CT. [1]
- Sinusitis, especially ethmoiditis through the thin lamina papyracea, is the commonest source of orbital cellulitis in children. [1] [4]
- The organisms are Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae and the Streptococcus anginosus group, with anaerobes in dental or chronic sinus disease. [4]
- Preseptal cellulitis in a well child takes oral antibiotics (co-amoxiclav, cephalexin or flucloxacillin) for five to seven days. [3] [9]
- Orbital cellulitis takes intravenous ceftriaxone plus flucloxacillin, with metronidazole for anaerobic or dental concern and vancomycin or clindamycin for suspected MRSA. [8]
- Contrast CT of the orbits and sinuses is indicated for any orbital sign, for systemic toxicity, or for failure to improve at 24 to 48 hours. [6]
- A medial subperiosteal abscess in a child under nine with normal vision may be given a trial of intravenous antibiotics; surgery is indicated for non-medial or large abscess, visual compromise, failure at 48 hours, or age nine or older. [7] [10]
- The feared complications are optic neuropathy and visual loss, cavernous sinus thrombosis, and intracranial extension (epidural empyema, brain abscess, meningitis). [4] [11]
- Valveless ophthalmic veins connect the orbit to the cavernous sinus, explaining the risk of cavernous sinus thrombosis and bilateral signs. [4]
References
- [1]Nageswaran S; Woods CR; Benjamin DK Jr; Givner LB; et al Orbital cellulitis in children. Pediatr Infect Dis J, 2006.PMID 16874168
- [2]Sobol SE; Marchand J; Tewfik TL; Manoukian JJ; et al Orbital complications of sinusitis in children. J Otolaryngol, 2002.PMID 12121013
- [3]Botting AM; McIntosh D; Mahadevan M Paediatric pre- and post-septal peri-orbital infections are different diseases. A retrospective review of 262 cases. Int J Pediatr Otorhinolaryngol, 2008.PMID 18191234
- [4]Chaudhry IA; Al-Rashed W; Arat YO The hot orbit: orbital cellulitis. Middle East Afr J Ophthalmol, 2012.PMID 22346113
- [5]Georgakopoulos CD; Eliopoulou MI; Stasinos S; Exarchou A; et al Periorbital and orbital cellulitis: a 10-year review of hospitalized children. Eur J Ophthalmol, 2010.PMID 20544674
- [6]Gutowski WM; Mulbury PE; Hengerer AS; Kido DK The role of C.T. scans in managing the orbital complications of ethmoiditis. Int J Pediatr Otorhinolaryngol, 1988.PMID 3397230
- [7]Greenberg MF; Pollard ZF Medical treatment of pediatric subperiosteal orbital abscess secondary to sinusitis. J AAPOS, 1998.PMID 10532723
- [8]Yang M; Quah BL; Seah LL; Looi A Orbital cellulitis in children—medical treatment versus surgical management. Orbit, 2009.PMID 19839897
- [9]Chaudhry IA; Shamsi FA; Elzaridi E; Al-Rashed W; et al Inpatient preseptal cellulitis: experience from a tertiary eye care centre. Br J Ophthalmol, 2008.PMID 18697809
- [10]Quintanilla-Dieck L; Chinnadurai S; Goudy SL; Virgin FW Characteristics of superior orbital subperiosteal abscesses in children. Laryngoscope, 2017.PMID 27291943
- [11]McDermott SM; Onwuka A; Elmaraghy C; Walz PC Management patterns in pediatric complicated sinusitis. Otolaryngol Head Neck Surg, 2020.PMID 32396416