Paeds · ophthalmology
Refractive error in children
Also known as Myopia in children · Short-sightedness in children · Hyperopia in children · Long-sightedness in children · Astigmatism in children · Anisometropia · Refractive amblyopia · Myopia control
Fellowship topic on refractive error in children: the optical principle that refractive state is set by the balance between axial length and corneal and lenticular power, so that myopia focuses light in front of the retina, hyperopia behind it, and astigmatism at two focal lines; the classification of refractive errors into emmetropia, myopia (low, moderate and high), hyperopia, astigmatism (by axis) and anisometropia; the paediatric-specific point that uncorrected refractive error is the leading cause of preventable visual impairment in children and a major reversible cause of amblyopia, so that cycloplegic retinoscopy is the gold-standard refraction; the epidemiology of the global myopia epidemic and the risk factors of parental myopia, East Asian ethnicity, urban living, intense near work and limited outdoor time; the stepwise management of spectacle correction first, contact lenses and orthokeratology in older children, and low-dose atropine 0.01 to 0.05 percent for myopia control with outdoor time and reduced near work; the amblyopia risk-factor thresholds for hyperopia, astigmatism and anisometropia that drive prescribing and referral; and the red flags of reduced vision not improving with correction, a new squint or abnormal head posture, and a progressive rapid myopic shift.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The optical balance and what each error means
Overview & Definition
Picture a seven-year-old who squints at the board and holds books to her nose, a four-year-old whose preschool screening flags a "refer" result, and a teenager whose myopia has jumped a dioptre in a year and whose parents ask whether anything can be done. Each is refractive error, and each is solved faster once you remember that the eye is an optical instrument whose focal power and eyeball length must match. [1] [12]
A refractive error exists when the optical components of the eye fail to focus parallel rays of light precisely on the retina. The four common types are myopia (excess optical power or, far more commonly, excessive axial length, focusing light in front of the retina), hyperopia (insufficient power or a short globe, focusing light behind the retina), astigmatism (unequal curvature of the cornea or lens producing two focal lines) and anisometropia (a difference in refractive error between the two eyes). When the eye focuses light exactly on the retina it is emmetropic. [2] [8]
The clinician's task has three layers. The first is recognition — identifying the child who cannot see clearly, fails a vision screen, or has a squint, eye strain or school difficulty. The second is accurate measurement under cycloplegia and a decision about whether and how much to prescribe, weighted by amblyopia risk. The third is definitive care — spectacles, contact lenses, myopia-control treatment and amblyopia prevention — balanced against the red flags that point to pathology rather than simple optics. Refractive error is common and usually benign, but in a child it is never merely a pair of glasses: it is a time-sensitive question about visual development. [10] [11]
Classification
Classify refractive error by where the light focuses, because the focal point sets the lens sign and the management. Emmetropia focuses light on the retina. Myopia focuses it in front of the retina, corrected by a minus (concave) lens. Hyperopia focuses it behind the retina, corrected by a plus (convex) lens. Astigmatism produces two focal lines rather than a point, corrected by a cylinder lens oriented to the steepest meridian. Anisometropia is simply a clinically important difference between the two eyes, measured by the dioptre gap. [2] [9]
Myopia carries its own severity scale that matters for prognosis and for risk of sight-threatening complications. Low myopia is a spherical equivalent of minus 0.50 to under minus 3.00 dioptres, moderate myopia is minus 3.00 to under minus 6.00 dioptres, and high myopia is minus 6.00 dioptres or more, the range that raises the lifetime risk of myopic maculopathy, retinal detachment, glaucoma and cataract. This is the scale behind the modern drive for myopia control — slowing an eye toward high myopia is worth more than refracting it once it arrives there. [2] [1]
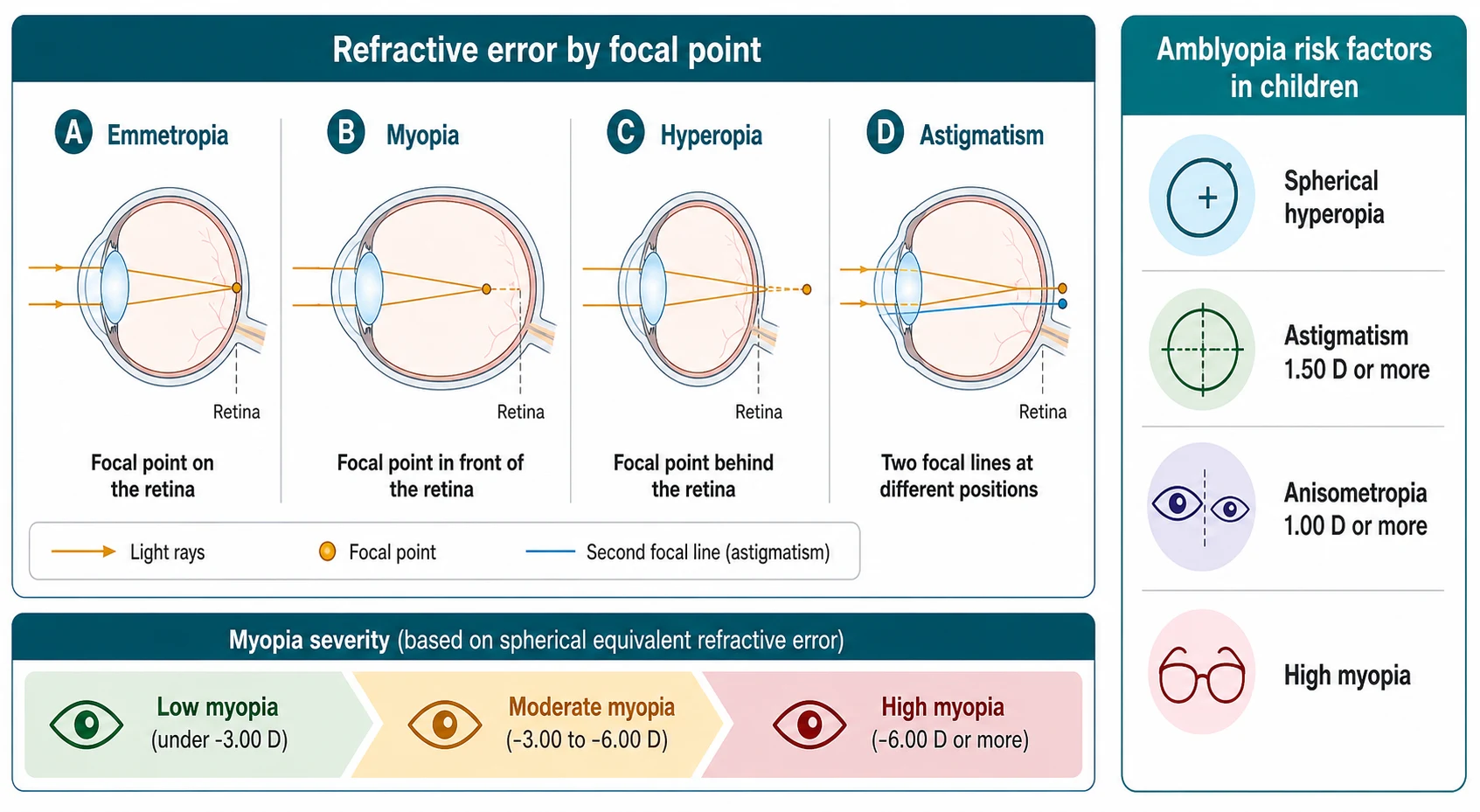
A second axis is by whether the error is amblyogenic in a young child. The widely used amblyopia risk-factor thresholds are significant hyperopia (typically a spherical equivalent of plus 3.00 dioptres or more), astigmatism of 1.50 dioptres or more, and anisometropia of around 1.00 dioptre or more between the eyes, alongside high myopia. These thresholds are the reason a refractive error in a four-year-old is managed differently from the same error in an adult: in the amblyopic age range you prescribe to protect visual development, not only to sharpen sight. [10] [9]
Epidemiology & Risk Factors
The dominant epidemiological story of modern childhood ophthalmology is the myopia epidemic. The global projection estimated that roughly half of the world's population — about five billion people — would be myopic by 2050, with nearly one billion in the high-myopia range, driven by East and South East Asia first but spreading globally. The rise is too fast to be genetic alone: it tracks urbanisation, intensive education, near work and the loss of outdoor time. For a paediatrician this means myopia is now a routine, escalating problem in every clinic, and prevention is a population as well as an individual concern. [1] [12]
The risk factors for childhood myopia are well mapped and clinically useful. The strongest are parental myopia (one parent roughly doubles and two parents roughly triples the risk), East and South East Asian ethnicity, urban residence, and a lifestyle of intense near work and limited outdoor time. The protective effect of outdoor time is the single most actionable point — around two hours a day of outdoor light appears to reduce incident myopia by raising retinal dopamine and slowing axial elongation, which is why it is now written into public-health guidance. [12] [1]
Hyperopia, astigmatism and anisometropia have their own epidemiology that matters for screening. Most infants are born physiologically hyperopic, and the eye grows toward emmetropia through childhood in emmetropisation. Astigmatism in early childhood is common and often resolves, but clinically significant astigmatism persists more often in some ethnic groups, as the Multi-ethnic Pediatric Eye Disease Study showed. Anisometropia, though individually uncommon, is disproportionately important because even a modest difference between the eyes is a powerful driver of amblyopia — the eye that sees the blurrier image is the one the brain suppresses. [8] [9]
In Australia and Aotearoa New Zealand, childhood vision screening is delivered through universal programmes — the preschool check and school-entry screening — with paediatric ophthalmology concentrated in major centres and accessed by rural, remote and Aboriginal and Torres Strait Islander and Māori families mainly through outreach or telehealth. This matters for refractive error because a child in a remote community who fails a screen may wait months to be refracted, and uncorrected refractive error remains an important and inequitable cause of preventable visual impairment in these populations. Building accurate screening and timely spectacle provision into primary care, with clear referral pathways, is part of delivering equitable eye care, not an afterthought. [11] [1]
Pathophysiology
Refractive state is set by a balance between two things: the axial length of the globe and the focusing power of the cornea and crystalline lens. Parallel light entering the eye is refracted mainly at the cornea and then fine-tuned by the lens, and clarity at the retina depends on those optical powers matching the eye's length. When the balance is exact the eye is emmetropic; when it is off, refractive error follows. This single balance explains every refractive error, and it explains why the eye can drift into myopia during the school years as the globe elongates faster than the optics weaken. [2] [3]
Myopia is overwhelmingly a problem of axial elongation: the globe grows too long, so the focused image falls in front of the retina. The elongation is driven by a mix of genetics and environment, with strong evidence that prolonged near work and a lack of outdoor retinal light exposure encourage axial growth, while diffuse outdoor light and reduced near demand slow it. Once an eye is longer, its optics no longer match its length, and the price of high myopia is structural — a stretched retina and sclera that raise the lifetime risk of maculopathy, retinal detachment, glaucoma and cataract. [1] [12]
Hyperopia is the opposite optical fault: the globe is too short, or the cornea and lens too weak, so light focuses behind the retina. The child compensates by accommodating — using the ciliary muscle to thicken the lens and bring the focus forward — which is why hyperopia is so easily hidden in an awake child and so easily revealed by cycloplegia. Sustained accommodation causes eye strain, headaches and, in some children, an accommodative (convergent) squint as convergence is linked to focusing effort. Astigmatism arises when the cornea (or lens) curves more steeply along one meridian than another, so the eye focuses light at two focal lines and vision is distorted at every distance. [8] [10]
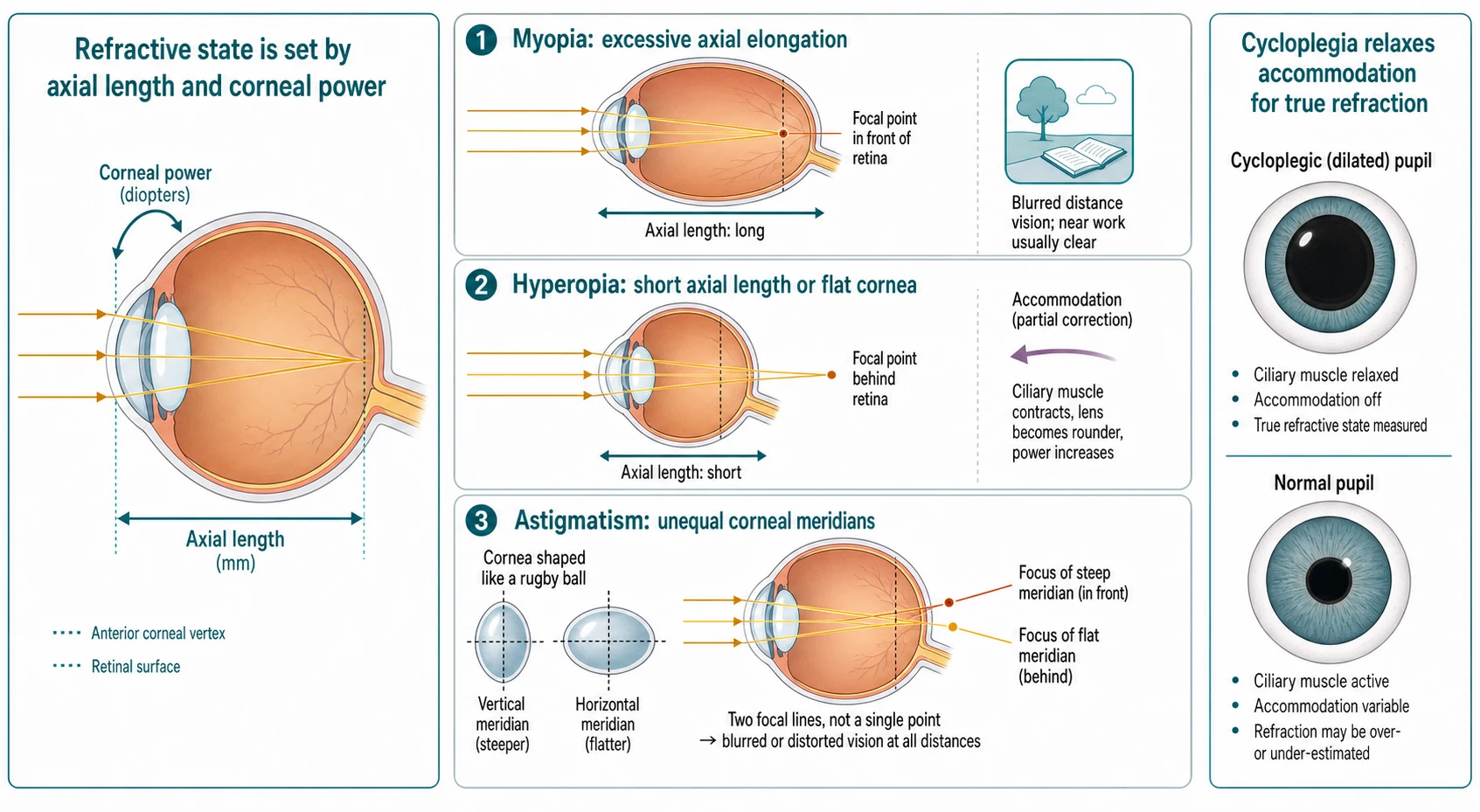
The reason cycloplegia matters so much in children is the strength of the accommodative reflex. A child can accommodate several dioptres, which means an awake, undilated refraction will overestimate myopia and, far more dangerously, underestimate or completely mask hyperopia — the child simply focuses through it. Cyclopentolate drops paralyse the ciliary muscle, abolish accommodation, and yield the true refractive state. This is why cycloplegic retinoscopy is the gold standard in young children, and why a non-cycloplegic refraction that reports no hyperopia in a squinting child is not to be trusted. [10] [12]
Clinical Presentation
Myopia declares itself as blurred distance vision with clear near vision, and the signs are often behavioural before they are measured: a child squints, sits close to the television or front of the classroom, holds a phone or book very close, rubs the eyes, or complains of distance blur, headaches or tired eyes after sustained near work. The onset is typically in the school years, with progression through the teenage growth spurt, and a family history of myopia is a strong clue. The error is usually bilateral and fairly symmetric; a large asymmetry should prompt the question of anisometropia and amblyopia. [1] [12]
Hyperopia presents more variably because the child accommodates through it. Some children are asymptomatic; others complain of eye strain, headaches, blurred vision or difficulty with near tasks, or are brought because of an accommodative convergent squint in which the effort to focus pulls the eyes inward. High hyperopia in an infant or toddler may present as poor visual attention or delayed visual behaviour. Astigmatism presents as distortion and blur at all distances, and in a young child often first surfaces as a failed vision screen or a squinting, head-tilting behaviour as the child seeks the least distorted view. [8] [10]
[10] [8]The presentation that must never be dismissed is reduced vision that does not improve with correction, a new squint or abnormal head posture, or a rapid myopic shift. These are the pointers away from simple refractive error toward amblyopia, motility disorder or pathology (including, rarely, a refractive change driven by systemic disease such as poorly controlled diabetes). A child whose acuity does not reach age-normal levels with pinhole or best correction needs cycloplegic refraction and ophthalmology assessment, not a new pair of glasses. [10] [12]
Differential Diagnosis
For a child with blurred distance vision, the first fork is between myopia and the conditions that mimic or accompany it. Myopia gives clear near and blurred distance vision that improves with a pinhole, but visual blur from any cause improves with a pinhole, so the pinhole is a refraction test, not a diagnosis. Always consider whether the reduced acuity is from uncorrected refractive error (which pinhole corrects) or from an organic or amblyopic cause (which it does not). A child whose vision fails to normalise with a pinhole or best correction needs dilated fundus examination and orthoptic assessment. [10] [2]
For a child who squints or has an abnormal head posture, the differential splits between refractive causes (high hyperopia driving an accommodative esotropia, or astigmatism driving a head tilt), motility causes such as incomitant strabismus or a cranial nerve palsy, and structural causes such as a media opacity or retinal problem. The red flag is a child whose squint is new, incomitant, or associated with reduced vision or neurological signs — that child is not a routine refractive case and needs urgent assessment. [10] [12]
[10] [2]For a child struggling at school, remember that refractive error is only one cause of learning difficulty — consider convergence insufficiency, accommodative dysfunction, attention and cognitive factors, and the rare mimics such as colour vision deficiency or a subtle retinal dystrophy. A failed vision screen should always be followed through to a definitive refraction rather than dismissed as inattention, because the only way to know whether vision is contributing is to measure it. [11] [10]
Clinical & Bedside Assessment
Begin with a focused history: the nature of the visual difficulty (distance, near or both), age of onset, squinting or abnormal head posture, headaches and eye strain, school performance, and the timing and result of any prior vision screening. Then widen the lens: a family history of myopia, squint or amblyopia, prematurity, syndromic diagnosis, and the lifestyle balance of near work and outdoor time. The history often names the error before you test — a book-to-nose school-age child with two myopic parents is almost certainly myopic. [1] [12]
Examine vision in an age-appropriate way, because the method is set by the child's developmental stage. In a preverbal infant or toddler use fixation behaviour and preferential-looking tests; in a preschool child use matching or picture acuity tests; in a school-age child use a Snellen or logMAR chart at distance, testing each eye separately with the other occluded. Check near vision, look for a squint with a cover test, examine eye movements, and inspect the red reflex and anterior segment. A pinhole retest of any reduced distance acuity tells you whether the deficit is refractive (improves) or organic and amblyopic (does not). [10] [11]
Apply the systemic and developmental lens. Refractive error is commoner and more severe in premature and low-birth-weight children, in certain syndromes (for example Down syndrome, Marfan syndrome with lens subluxation, Stickler syndrome with high myopia), and in children with neurodevelopmental disability who may not report blur. Lower the threshold to screen and refer these groups, and remember that an uncooperative or non-verbal child still needs an accurate assessment — instrument-based screening and cycloplegic retinoscopy can refact a child who cannot read a chart. [11] [10]
Investigations
The single most important investigation in paediatric refractive error is cycloplegic retinoscopy — the objective measurement of refractive state after abolishing accommodation with cyclopentolate (often combined with tropicamide or phenylephrine) drops. It is the gold standard because a child's accommodation hides hyperopia and distorts every other measurement, and because young and uncooperative children cannot give reliable subjective responses. Subjective refraction (asking the child which lens is clearer) refines the result in older cooperative children, but the cycloplegic objective measurement anchors the prescription. [10] [12]
Instrument-based vision screening (photoscreeners and autorefractors such as the Spot Vision Screener) has an expanding role, especially in preschool children who cannot do optotype testing. These devices estimate refractive error and detect amblyopia risk factors in seconds and are valuable for mass screening, but they are a screening tool, not a diagnostic refraction: a child flagged by photoscreening still needs cycloplegic refraction to confirm the error and decide the prescription. A "pass" on screening in a child with parental concern or symptoms does not exclude a refractive error. [11] [8]
For most children no further investigation is needed once the refractive error is measured, because the cause is optical. Reserve additional testing for the atypical or asymmetric case: a dilated fundus examination to exclude a retinal or macular cause of reduced vision; orthoptic assessment for a squint or motility disorder; and, in a child with a rapid myopic shift or systemic features, blood glucose testing to exclude a transient refractive change of poorly controlled diabetes. Over-investigation of a straightforward refractive error is a failure of clinical judgement — measure the optics, look at the retina, and refer when the picture does not fit simple error. [10] [12]
Management — Resuscitation
Resuscitation in paediatric refractive error is about recognising the few situations that cannot wait for a routine clinic while reassuring yourself that the great majority are managed electively. The red flags that demand prompt ophthalmology referral rather than a spectacle prescription are reduced vision that does not improve with correction (suspect amblyopia or pathology), a new or worsening squint or abnormal head posture (suspect a motility or refractive cause, or rarely a cranial nerve palsy), and a rapid or progressive myopic shift, especially in a young child, which may signal a pathological or systemic cause. [10] [12]
The other "cannot wait" group is the amblyopic-age child with an uncorrected amblyogenic error. Because the visual system develops through a sensitive period, a young child with significant hyperopia, astigmatism or anisometropia needs prompt cycloplegic refraction, prescription, and amblyopia treatment if amblyopia is already present. Delaying correction of an amblyogenic error in a three-year-old to "see if it settles" can cost the child permanent visual potential — this is the time-sensitive emergency of refractive error, even though it is never dramatic. [10] [9]
Keep resuscitation in proportion. Most children with refractive error are well, with myopia or mild hyperopia that will be managed with spectacles over months and years, and myopia control where appropriate. The danger lives in the non-improving vision, the new squint, the rapid shift, and the uncorrected amblyogenic error in a young child — each a reason to act promptly, but each a minority of the refractive problems you will see. [10] [1]
Management — Definitive & Stepwise
Definitive management runs as a cause-matched ladder that begins with the simplest and safest correction and reserves myopia-control treatment for the progressing child. The paediatric eye is growing and developing, so the art is to correct the error accurately, prescribe to protect amblyopia where it is a risk, and add myopia control to slow the drift toward high myopia — while never letting a non-refractive cause of reduced vision wait behind a pair of glasses. [10] [12]
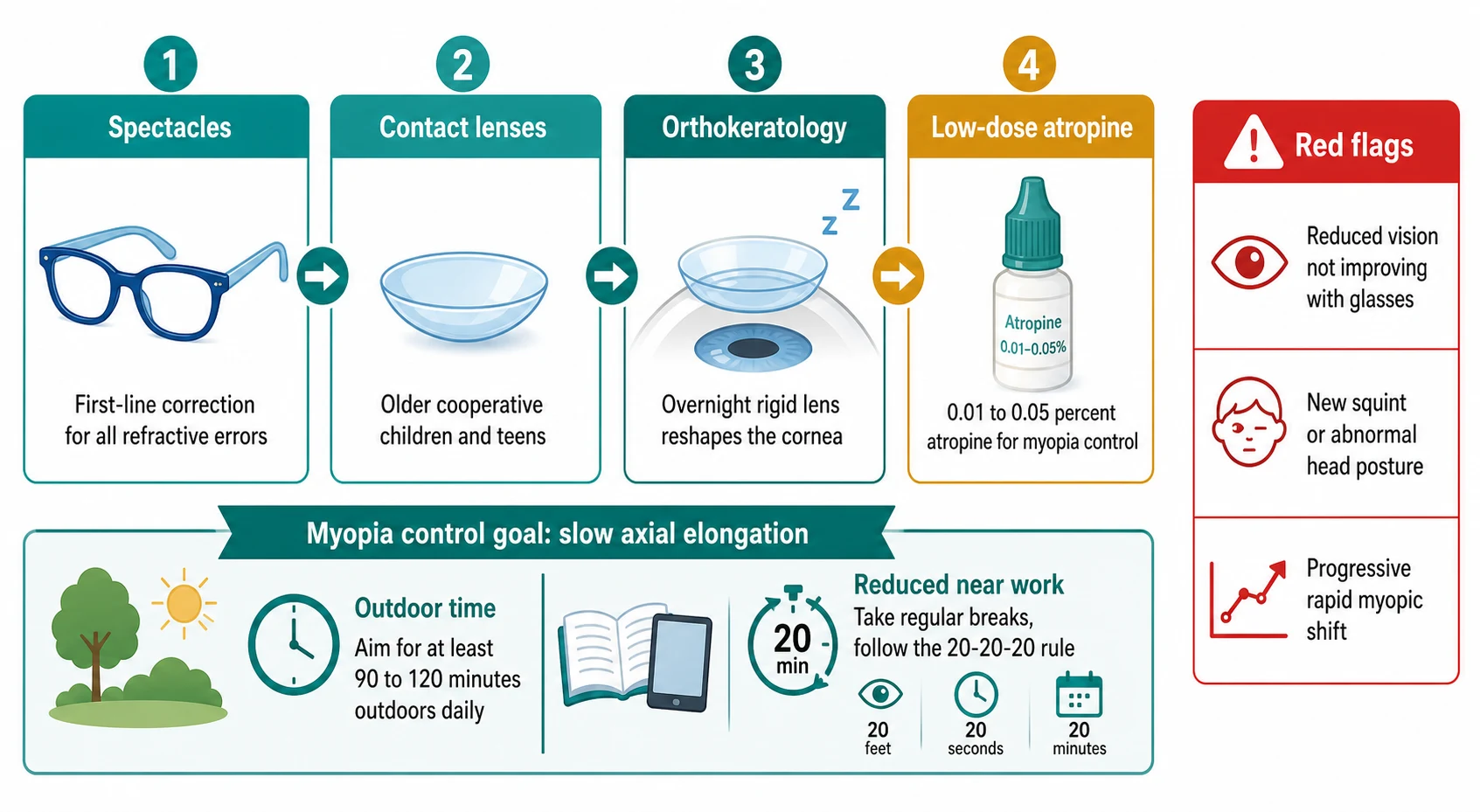
For every refractive error, spectacles are the first-line correction. Prescribe the full cycloplegic correction for significant hyperopia, astigmatism and anisometropia in amblyopic-age children, and a minus correction for myopia to give clear distance vision. Spectacles are safe, reversible, well tolerated once fitted, and the correct first step for almost every child. A young child needs a well-fitted, flexible frame and a strap, and the family needs clear advice that consistent wear is essential — both for vision and, where relevant, for amblyopia treatment. [10] [8]
For the progressing myopic child, myopia control is now part of standard care. The non-pharmacological foundation is increased outdoor time (around two hours a day) and reduced prolonged near work, which slow axial elongation. Pharmacological and optical options are then layered on. Low-dose atropine eye drops are the most widely used medical therapy: the LAMP trial established that among 0.05, 0.025 and 0.01 percent concentrations, 0.05 percent was the most effective over the first year, with the lower concentrations also effective, given as one drop at bedtime. [4] [6]
Childhood refractive error therapy ladder (confirm with local formulary such as BNF for Children)
Orthokeratology — wearing a rigid contact lens overnight to reshape the cornea and provide clear unaided vision by day — and peripheral-defocus soft contact lenses and spectacles also slow axial elongation and are options for older, cooperative children and teenagers. The network meta-analysis of myopia-control interventions ranked anti-muscarinic agents and orthokeratology among the more effective options, while low-dose atropine, orthokeratology and defocus-modifying lenses carry a favourable safety profile when appropriately supervised. The choice is individualised to the child's age, motivation, error and access to care. [3] [5]
The stepwise paediatric refractive error pathway
Recognise the child: a failed vision screen, distance or near blur, squinting, eye strain, a squint or abnormal head posture, or school difficulty; take a focused history including family history of myopia, squint and amblyopia.
Test vision in an age-appropriate way, each eye separately; recheck reduced distance acuity with a pinhole to separate refractive from non-refractive causes; examine the red reflex, anterior segment and cover test.
Measure under cycloplegia: cyclopentolate retinoscopy is the gold-standard refraction because a child's accommodation hides hyperopia; refine with subjective refraction in older cooperative children.
Prescribe spectacles to the cycloplegic correction — full hyperopic and astigmatic correction in amblyopic-age children, and minus correction for myopia to give clear distance vision; ensure consistent wear.
Protect visual development: correct amblyogenic errors promptly in young children and add occlusion or atropine penalisation if amblyopia is present.
For the progressing myopic child, add myopia control: outdoor time and reduced near work, plus low-dose atropine 0.01 to 0.05 percent, orthokeratology or peripheral-defocus lenses.
Red flags — refer urgently: reduced vision that does not improve with correction, a new squint or abnormal head posture, or a rapid progressive myopic shift.
Specific Subtypes & Scenarios
A school-age child with progressive myopia. Correct the distance refractive error with spectacles and start the conversation about myopia control. Begin with the foundation of increased outdoor time (around two hours a day) and reduced prolonged near work, then offer a control treatment appropriate to the child and family — low-dose atropine (0.05 percent most effective in LAMP, given one drop at bedtime), orthokeratology, or a peripheral-defocus lens. Set the expectation that myopia control aims to slow, not reverse, axial elongation, and that adherence over years is what matters. [4] [12]
A young child with significant hyperopia and an accommodative squint. This is the classic cycloplegia case. Refact under cyclopentolate to reveal the true plus error, prescribe the full hyperopic correction, and watch the accommodative convergent squint reduce or resolve as the accommodative effort falls. Monitor acuity for amblyopia and add occlusion if one eye lags. The squint that fails to improve with full hyperopic correction is not a purely accommodative problem and needs ophthalmology and orthoptic review. [10] [9]
A preschool child with astigmatism flagged by photoscreening. Confirm the magnitude and axis with cycloplegic retinoscopy, because the photoscreener is a screen, not a prescription. Prescribe a cylinder correction when the astigmatism is at or above the amblyogenic threshold (about 1.50 dioptres), to protect visual development and sharpen vision; observe lower amounts in a visually normal child. Re-examine to ensure acuity reaches age-normal levels with correction, and treat any amblyopia that has already developed. [8] [10]
A child with anisometropia. Even a modest difference between the two eyes is a powerful amblyopia driver, because the brain favours the clearer image and suppresses the other. Correct the more ametropic eye fully, ensure both eyes see clearly with correction, and assess for and treat amblyopia with occlusion or atropine penalisation. Because anisometropia can escape notice (the child functions with the good eye), it is a key reason to test each eye separately at every vision screen. [9] [10]
A high-risk child (premature, syndromic, or neurodevelopmental disability). These children have higher rates of refractive error and may not report blur, so screen early and lower the threshold for cycloplegic refraction. Children with Stickler syndrome carry high myopia and retinal detachment risk, children with Down syndrome have increased refractive error and accommodation lag, and children with neurodevelopmental disability may need instrument-based screening and an accurate cycloplegic refraction even when they cannot cooperate with a chart. [11] [10]
Complications & Pitfalls
The first pitfall is relying on a non-cycloplegic refraction in a child. A child's accommodation hides hyperopia and distorts every other measurement, so an undilated test that reports no hyperopia in a squinting child is unreliable and may miss the very error driving the problem. Cycloplegic retinoscopy is the gold standard in young children, and reaching for a prescription without it is how amblyogenic hyperopia is missed. [10] [9]
The second pitfall is missing amblyopia behind a refractive error. A child whose vision does not reach age-normal levels with best correction is not simply under-corrected — that child may have amblyopia or an organic cause, and needs cycloplegic refraction and ophthalmology assessment rather than a stronger prescription. Treating the optics without addressing amblyopia in the sensitive period squanders the window in which amblyopia is treatable. [10] [2]
The third pitfall is under-prescribing hyperopia in a young child for fear of over-correction. While clinicians rightly avoid over-minusing myopia, the equivalent fear of prescribing plus power leads to amblyogenic hyperopia going uncorrected. The principle is to prescribe to the cycloplegic measurement in amblyopic-age children, with cycloplegic guidance on how much plus to leave to accommodate comfortably — balancing protection of visual development against comfort. [10] [8]
The fourth pitfall is omitting myopia control or omitting its foundation. A progressing myopic child who is simply refracted each year drifts toward high myopia and its structural risks, and a family offered atropine without advice on outdoor time and near-work habits gets only half the intervention. Myopia control is now standard of care for the progressing child, built on outdoor time and reduced near work and layered with atropine, orthokeratology or defocus lenses. [4] [12]
The fifth pitfall is dismissing a rapid myopic shift as ordinary progression. A rapid or marked myopic change, especially in a young child, can be a transient refractive shift of systemic disease such as poorly controlled diabetes, or a sign of ocular pathology, and warrants blood glucose testing and ophthalmology review rather than a routine prescription. The defence is to ask whether the rate and age of the change fit ordinary school-age progression, and to investigate when they do not. [10] [12]
The sixth pitfall is ignoring inequity of access. A child in a rural, remote or disadvantaged community who fails a vision screen may wait months to be refracted, and uncorrected refractive error is a major and inequitable cause of preventable visual impairment. Delivering accurate screening, timely refraction and spectacle provision through primary care with clear referral pathways is part of the management, not a footnote. [11] [1]
Prognosis & Disposition
The disposition for most childhood refractive error is outpatient and primary-care led, with spectacles and review sufficient for the majority. Simple myopia is managed with correction and myopia control over the school years, with the expectation that progression continues through the teenage growth spurt before stabilising in early adulthood. Hyperopia, astigmatism and anisometropia that are corrected promptly in the amblyopic-age child have an excellent prognosis for visual development, provided amblyopia is treated in its sensitive window. [10] [1]
Myopia control changes the natural history for the progressing child. Low-dose atropine, orthokeratology and peripheral-defocus lenses slow axial elongation and reduce the proportion of children reaching high myopia, which in turn lowers the lifetime risk of myopic maculopathy, retinal detachment, glaucoma and cataract. The benefit is proportional to the axial elongation prevented, which is why starting control earlier in a fast progressor matters more than starting it once the error is already high. [4] [3]
The disposition hardens around the red flags. A child with reduced vision that does not improve with correction, a new squint or abnormal head posture, or a rapid myopic shift needs cycloplegic refraction and ophthalmology assessment to exclude amblyopia and pathology. At each review, re-measure acuity in each eye, re-confirm the prescription under cycloplegia where indicated, and reinforce consistent spectacle wear, outdoor time and the safety-netting around the red flags. [10] [12]
Special Populations
Infants and toddlers are physiologically hyperopic and undergo emmetropisation through early childhood, so refractive management here is about the exceptions — high or asymmetric error, a squint, or failure of fixation behaviour — which need cycloplegic refraction and correction to protect the developing visual system. The threshold to refer a preverbal child with suspected poor vision is low, and instrument-based screening helps where optotype testing is impossible. [10] [11]
School-age children and adolescents carry the bulk of myopia and its progression, driven by near work, screen use and limited outdoor time, and they bear the educational and social burden of uncorrected error. Address the lifestyle drivers, involve the child in decisions about myopia control, and frame outdoor time and reduced near work as treatment rather than lifestyle advice. For adolescents choosing contact lenses or orthokeratology, discuss hygiene and the small risk of microbial keratitis. [4] [12]
Premature and low-birth-weight children have higher rates of refractive error, strabismus and amblyopia, and need structured vision surveillance regardless of whether retinopathy of prematurity was present. Children with Down syndrome, Stickler syndrome, Marfan syndrome and neurodevelopmental disability carry increased and sometimes atypical refractive error (high myopia in Stickler, accommodation lag in Down syndrome) and may not report blur, so screen early and lower the threshold for cycloplegic refraction. [11] [10]
Children in rural, remote and disadvantaged communities, and Aboriginal and Torres Strait Islander and Māori children, face real inequity of access to refraction, spectacles and myopia control. Deliver as much as possible through accurate primary-care screening and clear referral pathways, and use outreach and telehealth so that distance and disadvantage are not the reason a child with an amblyogenic error waits past the sensitive period for correction. [11] [1]
Evidence, Guidelines & Regional Differences
The evidence base for childhood refractive error rests on a set of landmark epidemiological and clinical-trial references that frame the scale of the problem and the effectiveness of treatment. The Holden global projection established the scale of the myopia epidemic and the forecast that half the world would be myopic by 2050, while the IMI Defining and Classifying Myopia standards (Flitcroft) set the shared language of myopia, its severity bands and the threshold at minus 0.50 dioptres. These are the framing references for the topic. [1] [2]
Low-Concentration Atropine for Myopia Progression (LAMP) Study
Population: Children with myopia randomised to 0.05 percent, 0.025 percent or 0.01 percent atropine eye drops or placebo, one drop at bedtime, to compare efficacy and safety across low concentrations.
Key finding
Over one year, all three low concentrations reduced spherical equivalent and axial length progression compared with placebo, and 0.05 percent was the most effective of the low doses, with minimal side effects, establishing low-dose atropine — and 0.05 percent in particular — as an effective medical therapy for childhood myopia control.
Practice change
The LAMP trial underpins modern myopia-control prescribing, justifying low-dose atropine as a standard option for the progressing myopic child and favouring 0.05 percent where the lowest effective dose was once assumed to be 0.01 percent.
The myopia-control evidence is consolidated by the Huang network meta-analysis comparing sixteen interventions, which ranked anti-muscarinic agents and orthokeratology among the more effective options, and by the Bullimore review of the risks and benefits of myopia control, which set out the safety profile of low-dose atropine and optical treatments and rebutted the concern that under-correcting myopia slows progression. The Chua atropine-for-childhood-myopia trial is the original study that opened the field of pharmacological myopia control. [3] [5] [6]
The hyperopia, astigmatism and anisometropia evidence is grounded in the Holmes and Clarke Lancet review of amblyopia, which frames uncorrected refractive error as a major reversible cause of amblyopia, and in the epidemiological studies — the MEPEDS astigmatism prevalence (Fozailoff) and the Afsari anisometropia study — which establish how common these errors are in young children and how strongly anisometropia predicts amblyopia. The Vincent CLEAR orthokeratology review and the Nemeth European and IMI myopia management guidance frame the optical and guideline landscape. [10] [8] [9] [7] [12]
The regional policy structure is consistent in principle and varies in access. Vision screening schedules, cycloplegic refraction as the gold standard, spectacles as first-line correction, and low-dose atropine, orthokeratology and peripheral-defocus lenses for myopia control are endorsed across the AAO Pediatric Eye Evaluations Preferred Practice Pattern, European and Australasian guidance. The controversies are real: the optimal atropine concentration (0.01 versus 0.05 percent), the age at which to start myopia control, the role of peripheral-defocus spectacles versus atropine, and the threshold for prescribing hyperopia in an older child. The defence against each is the same — accurate cycloplegic refraction, correction matched to amblyopia risk, myopia control for the progressing child, and prompt referral for the red flags. [12] [4]
Exam Pearls
- Refractive state is set by the balance of axial length against corneal and lenticular power: myopia focuses light in front of the retina (excess axial length), hyperopia behind it (short globe), astigmatism at two focal lines (unequal corneal meridians). [2]
- Cycloplegic retinoscopy is the gold-standard refraction in children because a child's accommodation hides hyperopia and distorts every other measurement — never trust a non-cycloplegic "no hyperopia" in a squinting child. [10]
- Myopia severity: low minus 0.50 to under minus 3.00 D, moderate minus 3.00 to under minus 6.00 D, high minus 6.00 D or more; high myopia raises the lifetime risk of maculopathy, retinal detachment, glaucoma and cataract. [2]
- Amblyopia risk-factor thresholds: significant hyperopia (about plus 3.00 D or more), astigmatism about 1.50 D or more, anisometropia about 1.00 D or more — correct these promptly in young children. [10] [9]
- The LAMP trial showed 0.05 percent atropine is the most effective of the low doses (0.05, 0.025, 0.01 percent), one drop at bedtime, for myopia control — not the 0.01 percent once assumed lowest-effective. [4]
- Under-correction of myopia does NOT slow progression — it is not a myopia-control strategy; full distance correction is standard, with control added separately. [5]
- Outdoor time (about two hours a day) and reduced near work slow axial elongation and reduce incident myopia — the non-pharmacological foundation of myopia control. [12]
- Orthokeratology (overnight rigid lens) and peripheral-defocus lenses also slow axial elongation; options for older, cooperative children and teenagers, with attention to contact-lens hygiene and the small risk of microbial keratitis. [7]
- The pinhole distinguishes refractive (improves) from non-refractive (does not) reduced vision — but a pinhole never rules out amblyopia or pathology on its own. [10]
- Red flags for urgent referral: reduced vision not improving with correction, a new squint or abnormal head posture, and a rapid progressive myopic shift (consider, rarely, poorly controlled diabetes). [10] [12]
References
- [1]Holden BA; Fricke TR; Wilson DA; Jong M; et al Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology, 2016.PMID 26875007
- [2]Flitcroft DI; He M; Jonas JB; et al IMI - Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci, 2019.PMID 30817826
- [3]Huang J; Wen D; Wang Q; McAlinden C; et al Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology, 2016.PMID 26826749
- [4]Yam JC; Jiang Y; Tang SM; Law AKP; et al Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology, 2019.PMID 30514630
- [5]Bullimore MA; Ritchey ER; Shah S; Leveziel N; et al The Risks and Benefits of Myopia Control. Ophthalmology, 2021.PMID 33961969
- [6]Chua WH; Balakrishnan V; Chan YH; et al Atropine for the treatment of childhood myopia. Ophthalmology, 2006.PMID 16996612
- [7]Vincent SJ; Cho P; Chan KY; et al CLEAR - Orthokeratology. Cont Lens Anterior Eye, 2021.PMID 33775379
- [8]Fozailoff A; Tarczy-Hornoch K; Cotter S; et al Prevalence of astigmatism in 6- to 72-month-old African American and Hispanic children: the Multi-ethnic Pediatric Eye Disease Study. Ophthalmology, 2011.PMID 20888047
- [9]Afsari S; Rose KA; Gole GA; et al Prevalence of anisometropia and its association with refractive error and amblyopia in preschool children. Br J Ophthalmol, 2013.PMID 23613508
- [10]Holmes JM; Clarke MP Amblyopia. Lancet, 2006.PMID 16631913
- [11]Kapoor V; Magoon S; Kaur S; et al Community based vision screening in preschool children; performance of the Spot Vision Screener and optotype testing. Ophthalmic Epidemiol, 2022.PMID 34423736
- [12]Nemeth J; Tapaszto B; Aclimandos WA; et al Update and guidance on management of myopia. European Society of Ophthalmology in cooperation with International Myopia Institute. Eur J Ophthalmol, 2021.PMID 33673740