Paeds · ophthalmology
Strabismus and ocular motility disorders
Also known as Squint · Misalignment of the visual axes · Esotropia · Exotropia · Childhood strabismus · Comitant and incomitant deviation · Cranial nerve palsy in children · Amblyopia and ocular misalignment
Fellowship topic on strabismus and ocular motility disorders in children: the definition of strabismus as a misalignment of the visual axes and the comitant-versus-incomitant fork that drives investigation; the cover-uncover and alternate-cover tests and the prism and Hirschberg methods for quantifying a deviation; the classification of horizontal deviations into infantile esotropia, accommodative esotropia (refractive and high accommodative convergence to accommodation ratio needing bifocals), acute acquired comitant esotropia as a red flag for intracranial disease, pseudoesotropia from epicanthal folds, and intermittent exotropia with its divergence-excess and convergence-insufficiency patterns; the incomitant disorders of cranial nerve three, four and six palsy, Duane retraction and Brown syndromes, restrictive disease from orbital fracture, and childhood myasthenia; the pathophysiology of suppression, anomalous retinal correspondence and amblyopia that follows childhood misalignment within the critical period of roughly the first seven years; the stepwise management of cycloplegic refraction then refractive correction then amblyopia therapy (occlusion or atropine penalisation) before any surgery, with prism, overminus lenses and botulinum toxin for selected deviations and recession or resection surgery timed to binocular potential; the red flags that demand neuroimaging and urgent referral; and the ANZ and international ophthalmology and primary-care guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Tropia, phoria, and the two cover tests
Overview & Definition
Picture a four-month-old brought in because the eyes have crossed since birth, a three-year-old who screws up one eye in bright sunlight, and a seven-year-old who has started seeing double. Each story is strabismus, yet the meaning of the turn could not be more different: the first is a developmental deviation to align and salvage binocular vision, the second is intermittent exotropia that may deteriorate, and the third is a red flag for a cranial nerve problem. The same sign — eyes not pointing together — opens three completely different clinical paths. [1] [6]
Strabismus is a misalignment of the visual axes, so the two foveas no longer look at the same object at the same time. We name it by direction — esotropia (inward), exotropia (outward), hypertropia (one eye up) and hypotropia (one eye down) — and we separate the manifest deviation, the tropia, from the latent one, the phoria, that only appears when fusion is broken. The other axis that matters most is whether the angle stays constant in every direction of gaze (comitant) or changes as the eyes move (incomitant), because that distinction routes the child toward either routine paediatric ophthalmology or urgent neurology. [1] [3]
The clinician's task runs in three layers. The first is detection and measurement: perform the cover test, quantify the angle, and decide comitant versus incomitant. The second is the management sequence: cycloplegic refraction, refractive correction, amblyopia therapy, then alignment through prism, overminus lenses, botulinum toxin or surgery. The third is vigilance — recognising that a sensory deviation may hide retinoblastoma or a cataract, and that acute or incomitant strabismus may hide a brain lesion. Strabismus is common and often benign, but it rewards a methodical, cover-test-led approach. [1] [12]
Classification
Classify strabismus along two practical axes that together set the plan. The first axis is comitant versus incomitant. A comitant deviation keeps the same angle in every direction of gaze and is the territory of the common childhood disorders: infantile esotropia, accommodative esotropia, intermittent exotropia and microtropia. An incomitant deviation changes with gaze direction and signals a paralytic cause (a cranial nerve palsy or myasthenia) or a restrictive cause (an orbital floor fracture, thyroid eye disease or a tight muscle in Brown syndrome). This one fork decides whether the child needs a refraction and glasses or a scan and a neurologist. [1] [3]
The second axis is direction and onset, which names the disorder. Esotropia splits into infantile (onset under six months, large angle), accommodative (onset around two to three years, hyperopia-driven), acute acquired comitant (a red flag in the older child) and pseudoesotropia (the epicanthal-fold illusion with a normal cover test). Exotropia is usually intermittent, controlled for near and breaking down for distance or in bright light. Vertical deviations point to a fourth nerve palsy, a superior oblique problem or dissociated vertical deviation. Naming the disorder this way points straight to its management. [3] [6]
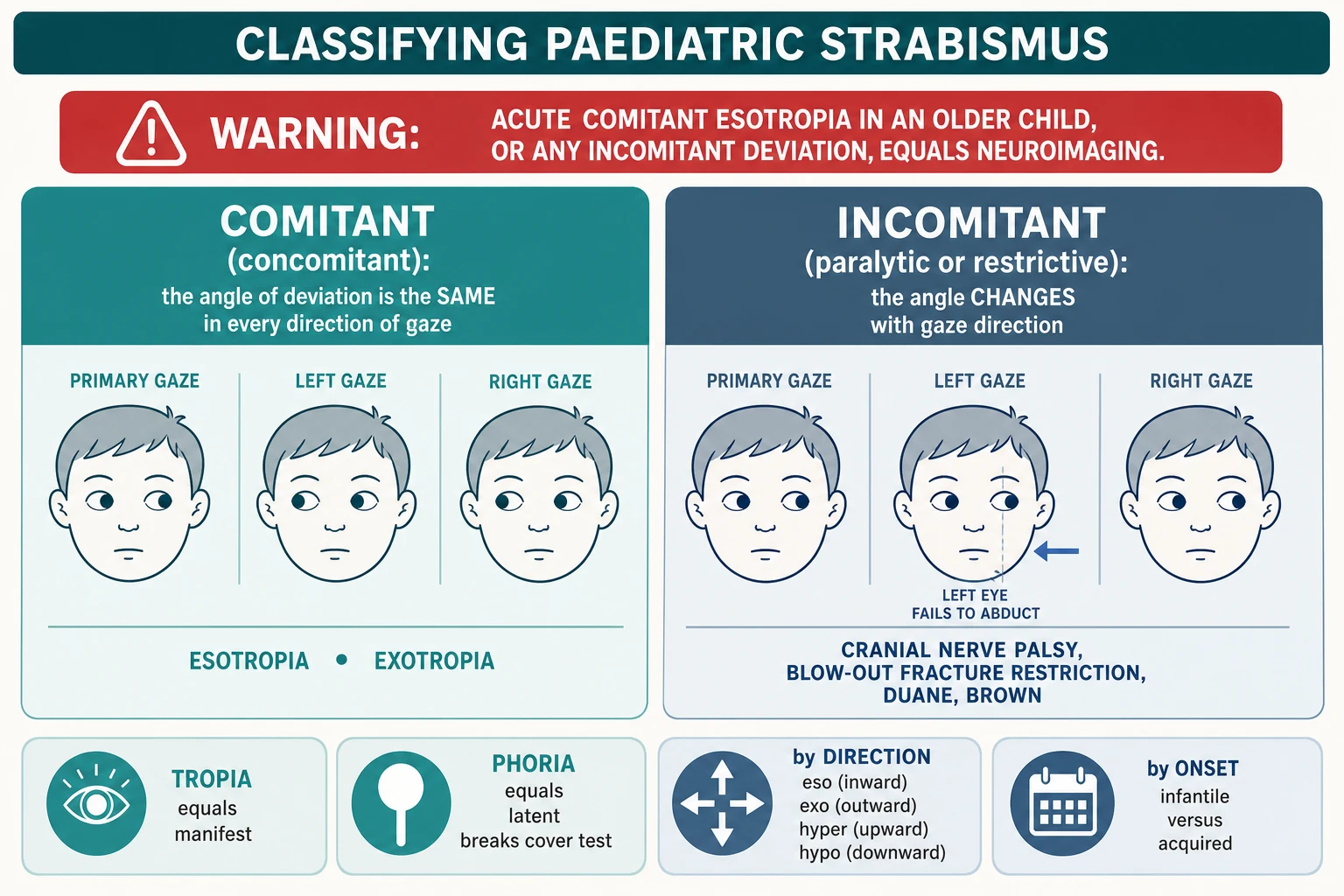
The incomitant disorders deserve their own grouping because they are the ones that threaten the brain. A third nerve palsy turns the eye down and out with ptosis and sometimes a dilated pupil. A fourth nerve palsy of the superior oblique produces a hypertropia worse on contralateral gaze and ipsilateral head tilt, so the child tilts the head away. A sixth nerve palsy of the lateral rectus produces an esotropia worse at distance and on attempted abduction, and it can be a non-localising sign of raised intracranial pressure. Duane retraction syndrome narrows the palpebral fissure and retracts the globe on adduction, and Brown syndrome limits elevation in adduction from a tight superior oblique tendon. [1] [3]
Finally, separate the primary deviation from the secondary. Most childhood strabismus is primary, a disorder of binocular fusion or motor alignment. A secondary or sensory deviation follows poor vision in one eye from any cause — cataract, retinopathy, retinoblastoma, optic nerve disease — so the worse-seeing eye drifts outward or inward. This is why every child with strabismus needs a dilated fundus examination: the deviation may be the first and only clue to sight-threatening or life-threatening disease. [2] [1]
Epidemiology & Risk Factors
Strabismus is one of the most common childhood eye problems, affecting roughly two to five per cent of children, with esotropia more frequent than exotropia in Western populations and exotropia relatively more common in East Asian children. The peak presentations map neatly onto the disorders: infantile esotropia appears in the first six months, accommodative esotropia around two to three years, and intermittent exotropia through the preschool and early school years. Knowing these age windows sharpens the differential before you even measure the angle. [1] [2]
Several risk factors recur across the disorders. Family history matters strongly — strabismus is highly heritable, and a parent or sibling with a childhood squint raises the child's risk. Significant hyperopia is the engine of accommodative esotropia, while anisometropia (a large difference in refractive error between the two eyes) is the engine of amblyopia. Prematurity, low birth weight, cerebral palsy, Down syndrome and other neurodevelopmental conditions all raise the risk of both comitant and incomitant strabismus. Any child with a developmental or genetic syndrome deserves a careful alignment and motility examination. [2] [3]
The most important epidemiological point is the link between strabismus and amblyopia. A constant unilateral deviation in a young child almost always produces amblyopia, because the developing visual cortex suppresses the image from the deviating eye to avoid double vision and confusion. This is the reason timing matters: the visual cortex is most plastic in the first seven years, and an uncorrected deviation in that window can lock in permanent vision loss that later treatment cannot fully reverse. Early detection and early treatment are the whole game. [11] [2]
In Australia and Aotearoa New Zealand, paediatric vision screening in the preschool years and primary-care surveillance are the main routes by which strabismus is detected, with paediatric ophthalmology concentrated in metropolitan centres. For rural and remote families — and disproportionately for Aboriginal and Torres Strait Islander children — distance to an ophthalmologist or orthoptist can delay diagnosis and amblyopia treatment into and beyond the critical period. Building the cover test into primary-care and child-health checks, with clear telehealth-supported referral pathways, is part of delivering equitable eye care, not a footnote to it. [12] [2]
Pathophysiology
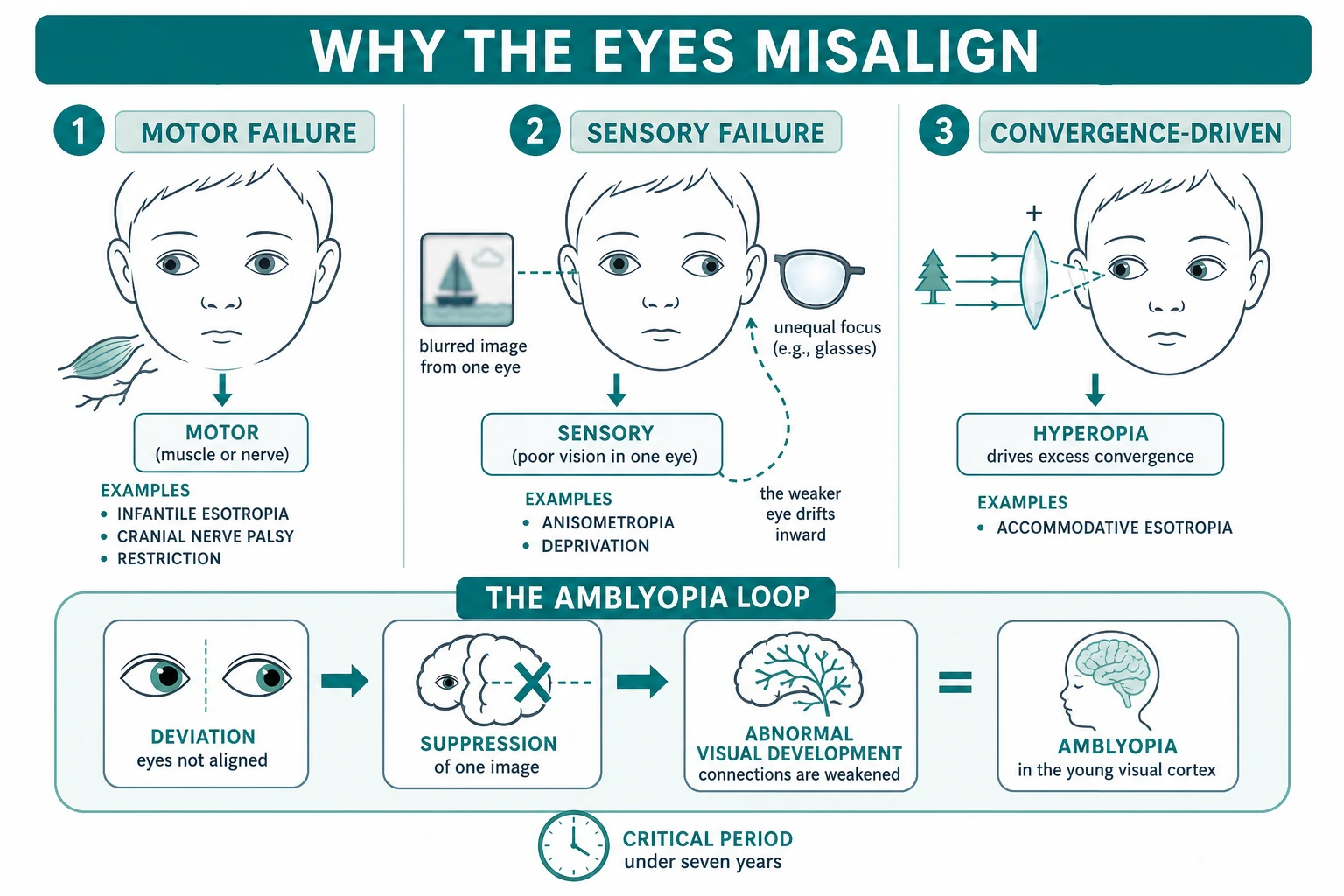
Strabismus arises when the motor system cannot hold the two eyes aligned, or when the sensory system loses the image that drives fusion. The motor failures are mechanical or neurological: an imbalance in the extraocular muscles, a cranial nerve palsy, or a restrictive tether. The sensory failures begin with poor vision in one eye — from anisometropia, deprivation or retinal disease — so the brain stops fusing and the affected eye drifts. The vergence failures sit in between: uncorrected hyperopia drives excess accommodative convergence, which is the mechanism of accommodative esotropia. [6] [1]
Accommodative esotropia shows the convergence mechanism at its clearest. To focus a near or hyperopic image the child accommodates, and accommodation is physiologically yoked to convergence through the accommodative convergence to accommodation, or AC to A, ratio. A hyperopic child over-accommodates to see clearly, which over-converges, and the eyes cross. Correct the hyperopia with glasses and the excess accommodation — and the esotropia — disappears. In the high AC to A subtype the near deviation exceeds the distance deviation, which is why a bifocal add is used for the near angle. [5] [6]
Infantile esotropia has a different mechanism — an early failure of binocular fusion in the developing visual system rather than a refractive or paralytic one — which is why surgery to align the eyes in infancy aims to give the cortical binocular cells a chance to wire up at all. Incomitant strabismus is mechanical or neurological: a sixth nerve palsy paralyses the lateral rectus, a third nerve palsy paralyses the medial, superior and inferior recti and the inferior oblique, and a fourth nerve palsy weakens the superior oblique. Restriction, as in an orbital floor fracture entrapping the inferior rectus, physically tethers the eye and produces a mechanical, positive forced-duction picture. [1] [3]
The consequence that ties everything together is amblyopia. When one eye deviates, the brain receives two different images, and to avoid diplopia and confusion it suppresses the image from the deviating eye and may develop anomalous retinal correspondence. Within the critical period — greatest in the first seven years and declining through the early teens — this suppression weakens the cortical connections from that eye and locks in poor acuity. This is the pathophysiological reason why a child with strabismus is not just a surgical problem but an amblyopia problem with a closing window. [11] [1]
Clinical Presentation
Infantile esotropia presents in the first six months with a large, constant inward turn, often at least thirty prism dioptres, and the infant typically cross-fixates, using the adducted contralateral eye to look to either side rather than abducting. Associated features are common and important: latent nystagmus, dissociated vertical deviation in which the covered eye drifts up, and inferior oblique overaction. The refraction is usually only mildly hyperopic, because infantile esotropia is not an accommodative problem. Parents describe an eye that has turned in since the first weeks of life. [4] [6]
Accommodative esotropia presents later, around two to three years, as an intermittent inward turn that becomes constant, often worse when the child is tired or focusing on near objects. The child is typically hyperopic, and the angle improves or resolves when the hyperopia is corrected with glasses. A parent may notice the turn fluctuating through the day. The high accommodative convergence to accommodation ratio subtype shows a much larger near than distance angle, and the child may hold things close or frown. Recognising the hyperopic, age-typical presentation names the disorder and its first treatment — glasses. [5] [6]
The incomitant presentations are the ones you must read as danger signs. A sixth nerve palsy shows a sudden esotropia worse at distance with an abduction deficit and double vision. A third nerve palsy shows the eye down and out with ptosis, and a dilated pupil marks a compressive cause that is an emergency. A fourth nerve palsy shows a head tilt to the opposite shoulder and a hypertropia worse on contralateral gaze. Duane retraction syndrome shows limited abduction or adduction with globe retraction and narrowing of the palpebral fissure on adduction. Brown syndrome shows limited elevation in adduction. Each points to a specific motor or neurological mechanism. [1] [3]
Differential Diagnosis
For an infant whose eyes appear to turn in, the first fork is pseudoesotropia versus true esotropia. Pseudoesotropia is the illusion of a convergent squint from broad, flat epicanthal folds and a wide, flat nasal bridge; the cover test is normal and the corneal light reflexes are symmetrical, which reassures the family that the child will grow out of the appearance as the bridge develops. A true esotropia shows a positive cover test. This is the commonest reason a baby is referred for a "squint," and the cover test resolves it in seconds. [12] [1]
[12] [4]For an older child with a new horizontal deviation, the critical distinction is acute acquired comitant esotropia from a decompensated refractive or fusion problem versus an incomitant deviation from a cranial nerve lesion. Acquired comitant esotropia that appears suddenly in a previously straight child, especially with no significant refractive error or with new neurological signs, is a recognised presentation of a posterior fossa or brainstem lesion and demands neuroimaging. The rule is simple: a new deviation in an older child is neurological until a thorough assessment proves otherwise. [6] [1]
For diplopia with an incomitant picture, run through the paralytic and restrictive causes. Myasthenia gravis causes variable ptosis and diplopia that fatigues through the day — a key clue is fluctuation and fatigability. Thyroid eye disease restricts the recti, especially the inferior rectus, and is rare but possible in older children. An orbital floor fracture from trauma entraps the inferior rectus and limits upgaze. Internuclear ophthalmoplegia points to a brainstem lesion. The variability of myasthenia and the gaze-dependent restriction of mechanical causes are the discriminators that separate them from a stable cranial nerve palsy. [1] [3]
Clinical & Bedside Assessment
Begin with a focused history: the age of onset, whether the turn is constant or intermittent, which eye, any closing of one eye in bright light, any head tilt or turn, and whether the parents have old photographs to date the deviation. Ask about double vision — its presence in a child signals an acquired or incomitant problem. Add the developmental and family history: prematurity, cerebral palsy or Down syndrome, and any family member with a childhood squint or amblyopia. A photograph that shows the turn has been present since infancy changes the differential completely from a turn that started last month. [1] [12]
The cover test is the core skill and is worth performing precisely. With the child fixing on a target, perform the cover-uncover test: cover the right eye and watch the left; if the left moves to take up fixation it had a tropia, and the direction of the movement names it (outward movement equals esotropia, inward equals exotropia, downward equals hypertropia). Then perform the alternate-cover test, switching the occluder rapidly between the eyes to break fusion; the eye just uncovered moves to refix, revealing the total deviation, which is always larger than the cover-uncover measurement. Test at distance and near, and in the cardinal positions of gaze to test comitance. [1] [2]
Quantify the angle with a prism when the child cooperates. Hold prisms of increasing power in front of one eye during the alternate-cover test until the refixation movement just disappears; the prism power is the deviation in prism dioptres. For the younger or uncooperative child, the Hirschberg test uses the corneal light reflex: each millimetre the reflex is off centre corresponds to roughly seven degrees or about fifteen prism dioptres, with the reflex at the pupillary margin suggesting about thirty prism dioptres. The Krimsky test refines this by placing prisms in front of the fixating eye to recentre the reflex in the deviating eye. [1] [12]
Widen the examination to a full ocular and neurological assessment. Check visual acuity in each eye with an age-appropriate method, because the difference that unmasks amblyopia is often subtle. Perform ocular motility in all six cardinal directions to detect an incomitant or restrictive pattern. Inspect the eyelids for ptosis, check the pupils for asymmetry, look for a head tilt or turn, and examine the fundus after dilation to exclude optic nerve disease, retinoblastoma or a cataract. Any incomitant deviation, new cranial nerve sign or papilloedema moves the child out of routine ophthalmology and into urgent imaging. [2] [3]
Investigations
Most childhood strabismus is a clinical diagnosis made at the bedside with the cover test and a refraction, and over-investigation of the common comitant deviations is itself a failure. The discipline is to investigate when it changes management: every child needs a cycloplegic refraction and a dilated fundus examination, and the child with an incomitant or acute acquired deviation needs neuroimaging. A routine blood panel or MRI is not part of assessing a straightforward infantile or accommodative esotropia. [1] [2]
Cycloplegic refraction is non-negotiable and is the single most important investigation in childhood strabismus. Cyclopentolate (often with tropicamide, and atropine for the most strongly accommodating or darkly pigmented eyes) paralyses accommodation so the full hyperopic or anisometropic error is revealed. This is what uncovers the hyperopia driving accommodative esotropia and the anisometropia driving amblyopia — errors that glasses can correct and that no surgery substitutes for. Skipping the cycloplegic refraction is the classic reason an accommodative esotropia is sent to surgery unnecessarily. [5] [2]
The dilated fundus examination excludes the sensory causes of a secondary deviation. A child whose eye drifts because it cannot see must have the cause of the poor vision found: a cataract, retinoblastoma, retinal or optic nerve disease. This is why a refraction alone is not enough — the fundus examination can be the step that finds a life-threatening tumour behind a benign-looking turn. In the right child, orthoptic measurements of stereoacuity and binocular function quantify the sensory consequences and guide surgical decisions. [2] [1]
For the incomitant or acute acquired deviation, neuroimaging is the investigation. An MRI of the brain and orbits (computed tomography if MRI is unavailable or in the acute trauma setting) looks for a posterior fossa or brainstem lesion, raised intracranial pressure, a cranial nerve lesion or an orbital fracture. A new sixth nerve palsy with papilloedema or a painful third nerve palsy with a dilated pupil is imaged immediately. In selected cases, ice-pack or edrophonium testing for myasthenia and neurophysiology clarify a fluctuating weakness. Imaging is reserved for the deviation that is not a straightforward childhood squint. [3] [1]
Management — Resuscitation
Resuscitation in strabismus means recognising the few deviations that cannot wait while reassuring yourself that the great majority are elective. The red-flag presentations are an acute comitant esotropia in an older child (possible intracranial lesion), any new incomitant deviation (cranial nerve palsy, raised intracranial pressure or compression), and a painful third nerve palsy with a dilated pupil (a possible compressive aneurysm that is an emergency). Each earns urgent neuroimaging and neurology or neurosurgery involvement rather than a routine ophthalmology appointment. [6] [1]
The other resuscitation layer is finding the sensory cause of a secondary deviation before assuming a benign squint. A child whose eye has drifted because it cannot see may have a cataract, retinoblastoma or an optic nerve lesion, and the deviation is the first clue. A dilated fundus examination at the first visit is the step that converts a "turned eye" into a timely diagnosis of sight-threatening or life-threatening disease. Missing a retinoblastoma behind a sensory exotropia is the catastrophic failure this examination exists to prevent. [2] [1]
Keep resuscitation in proportion. Most children with strabismus are well, with infantile or accommodative esotropia or intermittent exotropia that will be managed electively with refraction, glasses, amblyopia therapy and timed surgery. The danger lives in the acute, the incomitant and the sensory deviations — each a reason to escalate now, but each a small minority of the children you will see. The discipline is to perform the cover test, measure the angle, dilate and examine the fundus, and reserve imaging for the deviation that does not fit the common pattern. [1] [12]
Management — Definitive & Stepwise
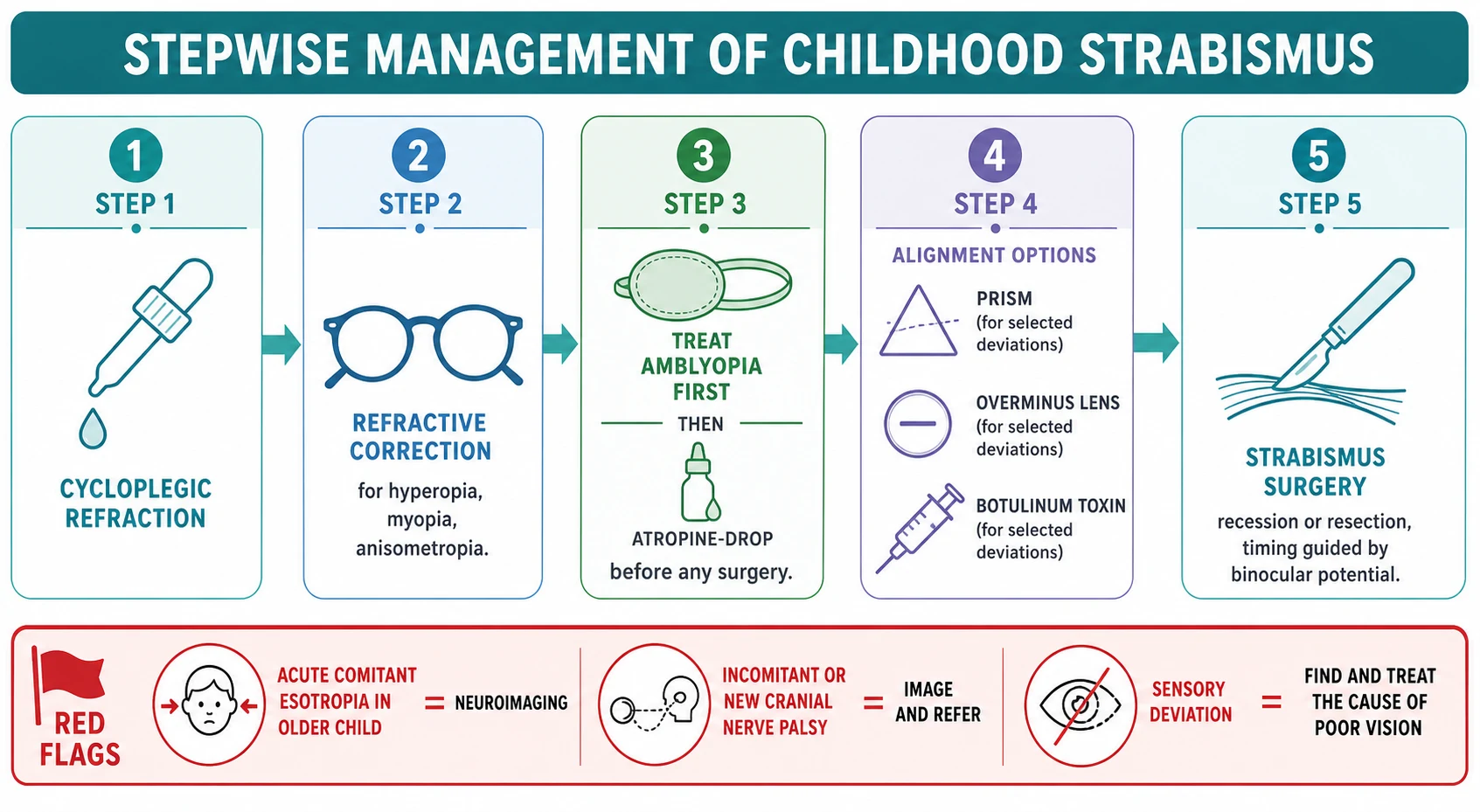
Definitive management follows a strict sequence that protects binocular vision: cycloplegic refraction first, then refractive correction, then amblyopia therapy, then alignment. The sequence is not optional, because operating on an eye that still suppresses will not give fusion, and giving glasses after surgery undoes the refraction-driven planning. The paediatric visual cortex is forgiving within its critical period but unforgiving after it, so the art is to move through the sequence in the right order and within the right window. [1] [11]
Refractive correction is the first treatment and is curative in many. Full hyperopic correction straightens a refractive accommodative esotropia, a result that can appear within weeks of wearing the glasses. Anisometropia is corrected to equalise the two retinal images and treat the amblyopia it causes. In the high accommodative convergence to accommodation ratio subtype, a bifocal add reduces the near angle. The point is that glasses are real treatment, not a holding measure, and many children never need surgery once the refractive error is corrected. [5] [2]
Amblyopia therapy comes next, before surgery, and runs as a choice between occlusion and pharmacologic penalisation. Occlusion patches the better-seeing eye for a set number of hours a day (from two hours for moderate amblyopia toward more for severe), and atropine penalisation uses atropine one per cent in the sound eye to blur its near vision and force the amblyopic eye to work. The landmark trial established that atropine and patching are comparable for moderate amblyopia, giving families a genuine alternative, especially where adherence to patching is poor. Refractive adaptation alone also improves acuity in many anisometropic children. [9] [10]
Childhood strabismus and amblyopia therapy ladder (confirm local formularies such as the BNF for Children)
Alignment is the final step. Strabismus surgery — recession (moving a muscle insertion back to weaken it) or resection (shortening a muscle to strengthen it), or a combined recession-resection — corrects the residual angle once refraction and amblyopia are addressed, with timing guided by binocular potential: infantile esotropia is typically aligned in infancy or early toddlerhood to give binocular cells a chance, while intermittent exotropia is operated when control deteriorates. Botulinum toxin injection into an extraocular muscle is a specialist alternative or adjunct in selected cases, including some infantile and acquired deviations. Prism relieves diplopia in some acquired incomitant deviations, and overminus lenses improve the short-term control of intermittent exotropia — though because they accelerate myopic progression, they are time-limited. [1] [8]
The stepwise childhood strabismus pathway
Detect the deviation with the cover-uncover and alternate-cover tests; measure the angle in prism dioptres and test comitance in all gaze positions.
Decide comitant versus incomitant: an acute comitant esotropia in an older child or any incomitant deviation earns urgent neuroimaging, not a surgical list.
Perform a cycloplegic refraction and a dilated fundus examination in every child to find the refractive error and exclude a sensory cause such as cataract or retinoblastoma.
Correct the refractive error with glasses — full hyperopic correction for accommodative esotropia, anisometropic correction for amblyopia, a bifocal add for a high accommodative convergence to accommodation ratio.
Treat amblyopia before surgery: occlusion of the sound eye or atropine one per cent penalisation, which are comparable for moderate amblyopia.
Choose alignment for the residual or non-refractive deviation: surgery (recession or resection) timed to binocular potential, botulinum toxin, prism or time-limited overminus lenses for intermittent exotropia.
Red flags — escalate: a new sixth or third nerve palsy, a painful third nerve palsy with a dilated pupil, papilloedema, or a sensory deviation from retinoblastoma all need imaging and urgent referral.
Specific Subtypes & Scenarios
An infant with a constant inward turn since birth (infantile esotropia). Confirm the large-angle esotropia with the cover test, perform a cycloplegic refraction (usually only mildly hyperopic) and a dilated fundus examination, and refer early to paediatric ophthalmology. Treat amblyopia if present, then plan surgical alignment in infancy or early toddlerhood to give the cortical binocular cells the best chance to develop, with botulinum toxin an alternative in some hands. Watch for the associated latent nystagmus, dissociated vertical deviation and inferior oblique overaction. [4] [6]
A three-year-old with a fluctuating inward turn (accommodative esotropia). Cycloplegic refraction reveals hyperopia, and full hyperopic glasses straighten the eyes in the refractive subtype. Re-measure the angle in glasses before deciding on surgery for any residual non-accommodative component, and use a bifocal add for a high accommodative convergence to accommodation ratio subtype with a large near angle. Treat amblyopia if the deviating eye has poorer acuity. Many of these children are managed entirely with glasses and never need surgery. [5] [2]
A preschool child who closes one eye in the sun (intermittent exotropia). Confirm the distance-dominant exodeviation and assess control, which may deteriorate over years. Options range from observation and part-time occlusion through overminus lenses (time-limited, because they accelerate myopia) and vision therapy to surgery (bilateral lateral rectus recession or a unilateral recession-resection) when control deteriorates and fusion is threatened. The decision to operate turns on documented loss of control and stereoacuity, not on the angle alone. [7] [8]
An older child with sudden double vision (acute acquired esotropia or a cranial nerve palsy). This is a red flag. An acute comitant esotropia in a previously straight older child, especially with no significant refractive error or new neurological signs, earns neuroimaging for a posterior fossa or brainstem lesion. A sixth nerve palsy with an abduction deficit, a third nerve palsy with the eye down and out, ptosis and a dilated pupil, or a fourth nerve palsy with a head tilt each demand imaging and urgent referral. Do not list these children for routine strabismus surgery. [6] [3]
A child with a head tilt and a vertical deviation (fourth nerve palsy or Brown syndrome). A congenital fourth nerve palsy presents with a long-standing head tilt to the opposite shoulder and a hypertropia worse on contralateral gaze and ipsilateral tilt, often with old family photographs confirming the tilt since infancy. Brown syndrome limits elevation in adduction from a tight superior oblique tendon. The head tilt is the sign that directs you to a vertical or oblique muscle problem rather than a horizontal one, and the gaze-dependent limitation marks the deviation as incomitant. [1] [3]
A child with variable ptosis and diplopia (childhood myasthenia). Myasthenia gravis causes fatigable, fluctuating ptosis and diplopia that worsen through the day and improve with rest — the variability is the key discriminator from a fixed cranial nerve palsy. An ice pack briefly applied to a ptotic lid may improve the ptosis. Refer for neurology assessment, serology and neurophysiology, because management (anticholinesterases, immunomodulation) is entirely different from strabismus surgery, and operating on a myasthenic deviation before it is controlled is futile. [1] [3]
Complications & Pitfalls
The first pitfall is missing amblyopia because the angle looks small. Even a small, constant unilateral deviation in a young child produces amblyopia, and the only way to detect it is to measure visual acuity in each eye. A child whose deviation looks cosmetically minor may still be losing cortical vision in that eye. The defence is to always assess monocular acuity and treat amblyopia before considering surgery, because operating on a suppressed eye does not restore fusion. [11] [9]
The second pitfall is operating before correcting the refractive error. An accommodative esotropia straightens with glasses, and a child sent to surgery without a cycloplegic refraction and a trial of full hyperopic correction may have an operation they never needed. The discipline is non-negotiable: cycloplegic refraction and refractive correction come first, always, and the residual angle in glasses is what is planned for surgery. [5] [1]
The third pitfall is labelling an acute or incomitant deviation as a routine squint. A new esotropia in an older child, an abduction deficit, a third nerve palsy with a dilated pupil, or a deviation with papilloedema are neurological emergencies. Listing such a child for elective strabismus surgery instead of imaging delays the diagnosis of a brainstem tumour, raised intracranial pressure or an aneurysm. The comitant-versus-incomitant fork and the onset history are what keep this error from happening. [6] [3]
The fourth pitfall is forgetting the dilated fundus examination. A sensory deviation from retinoblastoma, a cataract or an optic nerve lesion can present as a turned eye, and the fundus examination at the first visit is the step that finds it. Skipping the dilation and examining only the alignment is how a life-threatening tumour hides behind a benign-looking squint. Every child with strabismus gets a dilated fundus examination, without exception. [2] [1]
The fifth pitfall is dismissing pseudoesotropia as strabismus, or the reverse. Broad epicanthal folds create the illusion of a convergent turn that a normal cover test resolves in seconds, sparing a family unnecessary referral and anxiety. Conversely, accepting a parent's reassurance that the turn is "just the way he looks" without performing the cover test is how a true infantile esotropia is missed through the critical period. The cover test is the discriminator in both directions. [12] [1]
The sixth pitfall is ignoring the psychosocial and developmental burden. A visible squint, patching for amblyopia and the prospect of surgery affect a school-age child's confidence and friendships, and patching adherence is a major determinant of amblyopia outcome. Supporting adherence, involving the child in the plan, and addressing the self-image dimension are part of the management, not a footnote. [11] [10]
Prognosis & Disposition
The disposition for most childhood strabismus is outpatient and paediatric-ophthalmology-led, with the timing set by amblyopia risk and binocular potential. Infantile esotropia aligned in infancy can develop useful binocular function, accommodative esotropia often resolves with glasses alone, and intermittent exotropia watched and treated as control deteriorates generally does well. Setting the family's expectation around the sequence — refraction, glasses, amblyopia therapy, then surgery if needed — and the months-to-years timeline is part of the care. [1] [4]
Amblyopia is the outcome most sensitive to timing. Treatment within the critical period of the first seven years is most effective, but the window does not slam shut at seven — treatment can still improve acuity into the early teenage years, with diminishing returns. The decisive factor is adherence to occlusion or penalisation, which is why the amblyopia treatment index and family engagement matter as much as the dose of patching. Once the critical period closes, residual amblyopia is largely fixed, which is the whole reason for early detection. [11] [9]
The disposition hardens around the red flags. An acute comitant esotropia in an older child, a new cranial nerve palsy and a sensory deviation from retinoblastoma need urgent imaging and specialist referral, and their prognosis depends on the underlying cause rather than on strabismus surgery. At each review, re-measure the angle, re-check acuity, reinforce amblyopia therapy and adherence, and re-examine the fundus. The general paediatrician's role is detection, the cover test, timely referral and amblyopia adherence support. [6] [2]
Special Populations
Infants present with infantile esotropia, congenital incomitant disorders and, crucially, with sensory deviations from congenital cataract or retinoblastoma. The threshold to refer a baby with any turn is low, and the red-reflex and dilated fundus examination are mandatory at the first visit to exclude the sight- and life-threatening causes. Early alignment of infantile esotropia aims to preserve binocular potential within the critical period. [4] [2]
School-age children and adolescents carry intermittent exotropia, decompensating deviations and the psychosocial burden of a visible squint and patching. Address adherence, involve the young person in decisions about surgery, and screen mood and self-image when patching is a struggle, because adherence is the main determinant of amblyopia outcome. Acute acquired deviations in this age group are neurological until proven otherwise. [7] [11]
Children with cerebral palsy, Down syndrome and neurodevelopmental conditions have a much higher prevalence of both comitant and incomitant strabismus, and their refractive errors and amblyopia are often under-detected. Lower the threshold for cycloplegic refraction, amblyopia assessment and ophthalmology referral, because the visual contribution to development and quality of life is substantial and modifiable. Examine these children specifically and repeatedly. [3] [2]
Children in rural, remote and disadvantaged communities face real inequity of access to paediatric ophthalmology and orthoptics, and the delay can push amblyopia treatment beyond the critical period. Deliver as much as possible through primary-care screening, the cover test and telehealth-supported referral pathways, so that distance is not the reason a child with a turned eye loses binocular vision. Equity of access is a clinical issue, not an administrative one. [12] [2]
Aboriginal and Torres Strait Islander children and other Indigenous children in Australia and New Zealand carry a higher burden of refractive error and may face longer waits for specialist review. Embedding vision and alignment screening in child-health checks, with culturally safe referral pathways, is part of closing the gap in preventable childhood vision loss. The cover test in primary care is where equity begins. [2] [12]
Evidence, Guidelines & Regional Differences
The evidence base rests on a set of authoritative overviews and guidelines that frame the topic. The Donahue review of paediatric strabismus in the New England Journal of Medicine is the foundational general reference, and the American Academy of Ophthalmology Pediatric Eye Evaluations Preferred Practice Pattern sets the screening, referral and examination standards. The Mocan et al etiology-based classification scheme gives paediatricians a practical framework for comitant versus incomitant strabismus. These are the framing references for the approach. [1] [2] [3]
The disorder-specific evidence is anchored by Cochrane reviews and landmark trials. The Cochrane review of interventions for infantile esotropia (Mehner et al) and the Campos review of why the eyes cross set the mechanism and management of the esotropias, while the Lembo et al review covers accommodative esotropia in detail. The Cochrane review of interventions for intermittent exotropia (Pang et al) and the Pediatric Eye Disease Investigator Group overminus lens trial (2024) frame the exotropia evidence, including the myopic-shift caution of overminus therapy. [4] [6] [5] [7] [8]
Atropine vs patching for moderate amblyopia (PEDIG)
Population: Children with moderate amblyopia (visual acuity 20/40 to 20/100) randomised to patching of the sound eye versus atropine penalisation.
Key finding
Atropine one per cent penalisation and patching produced comparable improvement in visual acuity for moderate amblyopia, establishing pharmacologic penalisation as a genuine, adherence-friendly alternative to occlusion.
Practice change
The trial changed amblyopia practice by giving families a real choice, especially where patching adherence is poor, and underpins the modern amblyopia-first principle before strabismus surgery.
The amblyopia evidence is completed by the Holmes and Clarke Lancet review and the Li et al Cochrane review of conventional occlusion versus pharmacologic penalization, which together set the treatment principles and the comparable efficacy of the two main modalities. The Reedy-Cooper et al American Family Physician review of the childhood eye examination in primary care grounds the primary-care detection, cover-test and referral content. Together these references cover detection, mechanism, classification, the specific disorders, amblyopia and management. [11] [10] [12]
The regional policy structure is consistent in principle. Screening, cycloplegic refraction and amblyopia-first management are universal across the American Academy of Ophthalmology, RCOphth, RANZCO and primary-care guidance, including the Australian and New Zealand screening programmes. The threshold for neuroimaging in acute or incomitant strabismus is likewise universal. The genuine variation is one of access — the distance rural, remote and Indigenous families must travel for paediatric ophthalmology and orthoptics — which is why primary-care detection and telehealth-supported referral matter as much as the clinical content. [2] [12]
The controversies are real: the optimal timing and dose of patching and atropine; the role of vision therapy and overminus lenses for intermittent exotropia against the myopic-shift risk; the threshold for surgery versus observation in well-controlled intermittent exotropia; and the place of botulinum toxin against surgery in infantile esotropia. The defence against each is the same methodical approach — the cover test, cycloplegic refraction, amblyopia-first treatment, and a low threshold for imaging the red-flag deviation. [1] [8]
Exam Pearls
- The single most useful principle: decide comitant versus incomitant before anything else, because a comitant deviation is a childhood squint to refract and align while an incomitant deviation is a cranial nerve or restrictive problem to image. [1]
- The cover-uncover test finds the manifest tropia; the alternate-cover test breaks fusion and reveals the total deviation (tropia plus latent phoria), always larger; quantify in prism dioptres, or fall back on the Hirschberg corneal reflex where each millimetre of decentration is about seven degrees or fifteen prism dioptres. [1] [12]
- The management sequence is fixed: cycloplegic refraction, refractive correction, amblyopia therapy, then alignment. Operating on an eye that still suppresses will not give fusion, so treat amblyopia before surgery. [5] [9]
- Accommodative esotropia is hyperopia-driven and often resolves with full hyperopic glasses; the high accommodative convergence to accommodation ratio subtype has a larger near angle and uses a bifocal add. [5]
- Intermittent exotropia shows the classic closing of one eye in bright light and a distance-dominant angle; overminus lenses improve control but accelerate myopia, so they are time-limited. [7] [8]
- The red flags: acute comitant esotropia in an older child and any new incomitant deviation earn neuroimaging; a painful third nerve palsy with a dilated pupil is an emergency; a sixth nerve palsy can signal raised intracranial pressure. [6] [3]
- Every child with strabismus needs a dilated fundus examination to exclude a sensory cause — cataract, retinoblastoma, optic nerve disease — because the deviation may be the first clue to sight- or life-threatening disease. [2]
- Pseudoesotropia from broad epicanthal folds has a normal cover test and symmetrical corneal light reflexes; reassure the family. [12]
- Childhood myasthenia causes variable, fatigable ptosis and diplopia — the fluctuation separates it from a fixed cranial nerve palsy. [3]
- Atropine one per cent penalisation and patching are comparable for moderate amblyopia, giving families an adherence-friendly alternative. [9]
References
- [1]Donahue SP Clinical practice. Pediatric strabismus. N Engl J Med, 2007.PMID 17347457
- [2]Hutchinson AK; Morse CL; Hercinovic A; et al Pediatric Eye Evaluations Preferred Practice Pattern. Ophthalmology, 2023.PMID 36543602
- [3]Mocan MC; Pastapur A; Kaufman L Etiology-based strabismus classification scheme for pediatricians. Turk J Pediatr, 2022.PMID 35611422
- [4]Mehner L; Ng SM; Singh J Interventions for infantile esotropia. Cochrane Database Syst Rev, 2023.PMID 36645238
- [5]Lembo A; Serafino M; Strologo MD; et al Accommodative esotropia: the state of the art. Int Ophthalmol, 2019.PMID 29332227
- [6]Campos EC Why do the eyes cross? A review and discussion of the nature and origin of essential infantile esotropia, microstrabismus, accommodative esotropia, and acute comitant esotropia. J AAPOS, 2008.PMID 18550403
- [7]Pang Y; Gnanaraj L; Gayleard J; et al Interventions for intermittent exotropia. Cochrane Database Syst Rev, 2021.PMID 34516656
- [8]Writing Committee for the Pediatric Eye Disease Investigator Group; Chen AM; et al Refractive Error Change and Overminus Lens Therapy for Childhood Intermittent Exotropia. JAMA Ophthalmol, 2024.PMID 38536764
- [9]Pediatric Eye Disease Investigator Group A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol, 2002.PMID 11879129
- [10]Li T; Qureshi R; Taylor K Conventional occlusion versus pharmacologic penalization for amblyopia. Cochrane Database Syst Rev, 2019.PMID 31461545
- [11]Holmes JM; Clarke MP Amblyopia. Lancet, 2006.PMID 16631913
- [12]Reedy-Cooper A; Scartozzi C; Yurkonis T Childhood Eye Examination in Primary Care. Am Fam Physician, 2023.PMID 37440736