Paeds · ophthalmology
Urgent ophthalmology referral and childhood vision loss
Also known as Red reflex abnormality · Childhood vision loss · Amblyopia and the sensitive period · Leukocoria · Painful red eye in a child · Sudden vision loss in a child · Papilloedema and raised intracranial pressure · Same-day ophthalmology referral
Fellowship guide to urgent ophthalmology referral and childhood vision loss, framed as a red-flag triage topic. Covers why childhood vision loss is time-critical through the amblyopia sensitive period, the abnormal red reflex and leukocoria as retinoblastoma until proven otherwise, the painful red eye and orbital cellulitis, the sudden painless vision loss from optic neuritis and cortical visual impairment, the papilloedema of raised intracranial pressure, the optic nerve hypoplasia of septo-optic dysplasia, the red reflex test at the newborn and well-child visits, and the tiered same-day, urgent and routine referral pathway that protects the eye and the developing visual brain.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A general practitioner checks the red reflex at the six-week check and finds a white pupil where there should be a warm orange-red. A parent photographs their infant and sees a white glow in the flash. A child wakes with a red, painful eye and a drooping lid. Each has crossed the threshold from a routine eye concern into an urgent ophthalmology problem, and the clinician who assigns the correct referral tier is the clinician who saves the eye and the developing visual brain. Urgent ophthalmology referral is the structured decision that matches the speed of the specialist assessment to the threat to the vision, the globe and the life. [1][4]
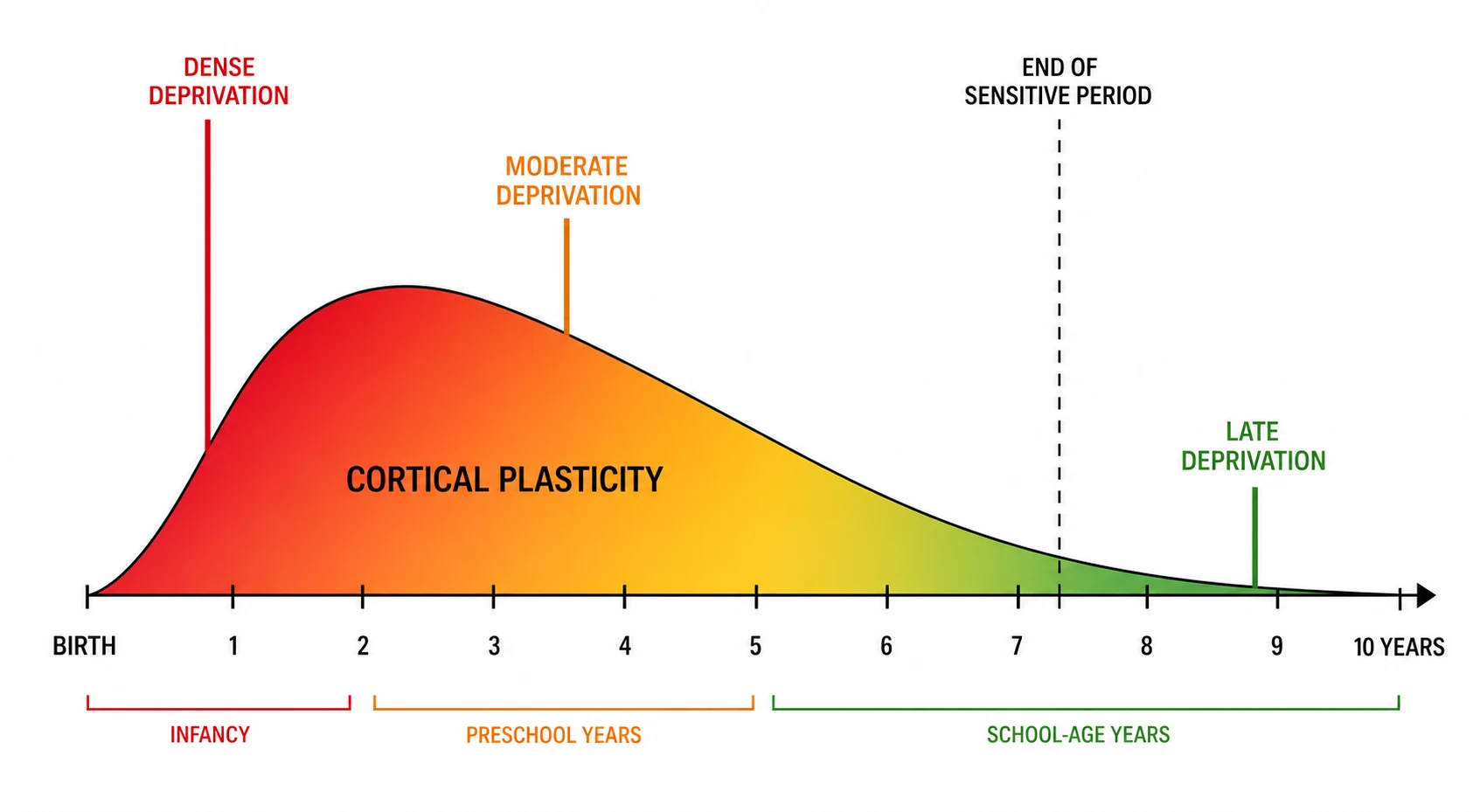
The reason childhood vision loss is time-critical, and the reason this topic exists as a triage framework rather than a single disease, is that the child's visual system is still being built. The image that falls on the retina travels to the visual cortex, and the cortex uses that image to wire its own architecture through a sensitive period that spans roughly the first seven to eight years. When the image is blurred, blocked or absent during this window, the cortex wires itself to a poor standard, and the deficit becomes amblyopia, a permanent reduction of vision that no later surgery or spectacle can fully recover. [11]
The fellow who frames the urgent referral around amblyopia and the sensitive period, and who holds the red-flag presentations in a single mental map, demonstrates the reasoning the boards reward. The abnormal red reflex, the leukocoria, the new strabismus, the painful red eye with proptosis and the sudden loss of vision are not five separate problems but five doors into the same principle that the delay costs the vision. The task of this topic is to build the triage pathway that places each presentation into the correct tier, from the immediate emergency through the same-day and the urgent reviews to the routine clinic. [1][11]
Classification
The clinician who frames the urgent referral correctly thinks in tiers, because the tier determines the speed, the setting and the safety. The presentation, not the diagnosis, drives the tier, and the candidate who can place a child into the correct tier from the bedside demonstrates the triage skill the examiner probes. The four tiers run from the immediate emergency, seen in the emergency department now, through the same-day ophthalmology review, the urgent one-to-two-day review and the routine clinic, and each carries a defined threat to the eye, the optic nerve and the visual brain. [1][4]
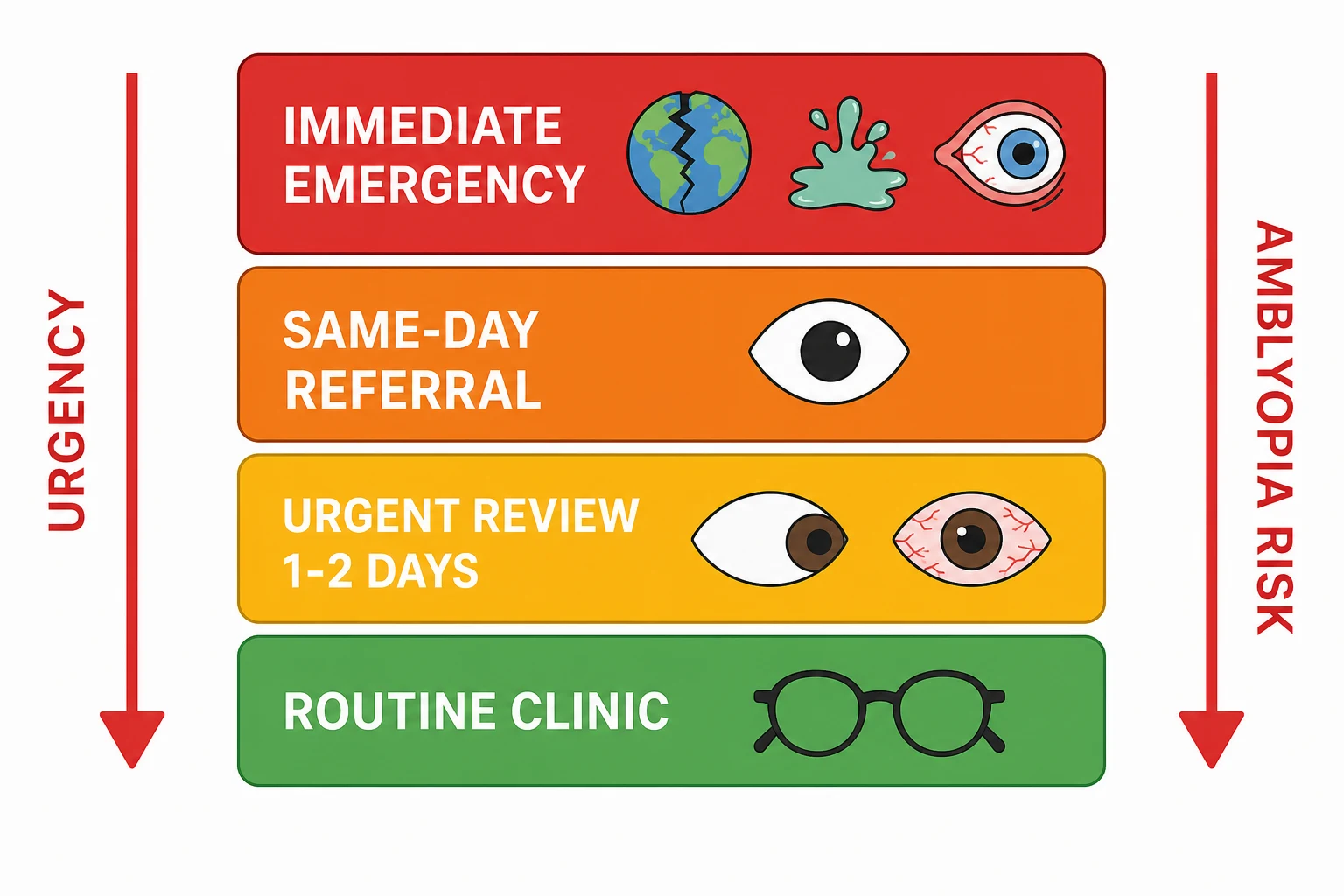
The immediate emergencies are the problems where minutes or hours decide whether the eye survives, and they bypass the outpatient pathway entirely. The suspected globe rupture, the chemical injury, the orbital cellulitis with proptosis and reduced vision, the acute angle-closure glaucoma and the raised intracranial pressure with papilloedema all belong here. Each is stabilised and sent to the emergency department for the immediate ophthalmology and, where needed, the neurosurgical or the ear-nose-throat input. The chemical injury is irrigated copiously first and the globe rupture is shielded, not examined, first, because the first aid protects the eye before the referral. [4][9]
The same-day tier is the tier of the red-flag presentations that threaten amblyopia or hide a malignancy, and it is the tier the generalist must never under-call. The leukocoria and the abnormal red reflex, the new strabismus under two years, the sudden painless loss of vision and the painful red eye without the proptosis all belong here. The child is seen by the ophthalmology service the same day, because the delay of weeks converts the curable into the irreversible. The urgent one-to-two-day tier catches the established but not sight-threatening problems, and the routine tier catches the stable refractive error and the surveillance. [5][6]
Immediate emergency
minutes to hours
- Suspected globe rupture, shield and do not examine
- Chemical injury, irrigate copiously first
- Orbital cellulitis with proptosis and reduced vision
- Raised intracranial pressure with papilloedema
- Acute angle-closure glaucoma
Same-day referral
today
- Leukocoria or abnormal red reflex
- New strabismus, particularly under two years
- Sudden painless loss of vision
- Painful red eye without proptosis
- Suspected optic neuritis
Urgent review
one to two days
- Preseptal cellulitis that fails first treatment
- Persistent discharge or watering
- Suspected corneal abrasion that is not healing
- New unequal vision on a screening test
Routine clinic
weeks
- Stable refractive error on a screening test
- Surveillance of a known stable condition
- Routine follow-up after a resolved problem
Epidemiology & Risk Factors
Childhood vision loss and blindness are uncommon in the high-income setting, but the conditions that cause them are the conditions the triage pathway is built to catch. Globally, an estimated one and a half million children are blind, and the causes divide sharply by the resource of the country. In the high-income setting, the lesions of the visual brain, the cortical visual impairment and the optic nerve disease dominate, alongside the retinopathy of prematurity in the survivors of neonatal intensive care. In the low-income setting, the vitamin A deficiency, the corneal scarring from the infection and the measles drive the blindness, and the cataract and the retinoblastoma present late with the proptosis. [1]
The single greatest risk factor for a poor outcome from a childhood eye problem is the delay in the referral, and the delay tracks the access to the care, the performance of the red reflex and the awareness of the red flags. The child who is referred the same day for the leukocoria keeps the eye and the vision, while the child who waits weeks presents with the extraocular retinoblastoma and the metastatic disease. The risk is concentrated in the preverbal child who cannot report the loss of vision, in the child with the complex neurology who cannot cooperate with the examination, and in the child in the remote community where the specialist is far. [1][6]
The risk of amblyopia, the irreversible legacy of the delayed referral, rises with the severity and the age at onset of the deprivation. A dense congenital cataract that is not removed in the first weeks of life produces a profound amblyopia that no later surgery recovers, while a strabismus that is treated in the sensitive period can be rescued. The fellow who names the delay, the access and the preverbal age as the three risk axes demonstrates the population reasoning the boards reward. [1][11]
Pathophysiology
The pathophysiology that makes childhood vision loss time-critical, and that justifies every tier of the referral ladder, is the development of the visual cortex through the sensitive period. The retinal image drives the competition between the two eyes for the cortical representation, and the eye that carries the clearer, more consistent image wins the cortical space. When one eye is blurred by a refractive error, occluded by a cataract or suppressed by a strabismus, it loses the competition, and the cortex dedicates its columns to the better eye. The result is amblyopia, a deficit of the cortical processing that persists even after the original problem in the eye is fixed. [11]
The sensitive period begins at birth, is densest through infancy and the preschool years, and tapers through the first seven to eight years, after which the cortical architecture becomes resistant to change. This is why a cataract removed at six weeks and at six years carry such different prognoses, and why the triage ladder weights the young child so heavily. The deprivation amblyopia of a dense cataract is the most aggressive form, because the cortex is denied any form vision at the height of its plasticity, and the reversal demands the surgery within weeks, not months. [11]
The same plasticity that makes the deprivation dangerous makes the treatment effective when it is timely. The patching of the better eye forces the cortex to re-engage the amblyopic eye, and the atropine penalisation blurs the better eye to the same end, but both work only while the cortex remains plastic. The fellow who holds the pathophysiology of the sensitive period in mind never under-calls a same-day referral, because the cortical clock is always running. [11]
Clinical Presentation
The clinical presentations that trigger the urgent referral are few enough to hold in a single map, and the candidate who can recite them by their red-flag features demonstrates the triage fluency the boards reward. The leukocoria, the white pupillary reflex, is the first and the most important, seen by the parent in the flash photograph or by the clinician on the red reflex test, and it is retinoblastoma or a congenital cataract until proven otherwise. The new strabismus, particularly the unilateral and the constant turn in the child under two years, is the second, because the tumour behind the fovea may present with the drift before the leukocoria. [5][6]
The painful red eye with the systemic toxicity, the proptosis, the reduced vision or the painful eye movement is the presentation that the generalist must never dismiss as conjunctivitis, because the conjunctivitis does not hurt, does not drop the vision and does not swell the lid. This is the door to the orbital cellulitis, the acute glaucoma and the corneal ulcer, and the proptosis with the restricted eye movement is the sign that the infection has crossed the orbital septum into the sight-threatening and the life-threatening compartment. [12][9]
The sudden loss of vision is the presentation that the boards use to separate the preverbal from the verbal child. The verbal child reports the blur, the field loss or the loss of the colour, while the preverbal child shows the poor visual behaviour, the roving eye movements, the loss of the social smile or the new head turn. Behind the sudden loss sits the optic neuritis with the pain on the eye movement and the relative afferent pupillary defect, the cortical visual impairment with the normal eye and the abnormal brain, the papilloedema of the raised intracranial pressure, and the traumatic or the vascular event. [7][10]
Differential Diagnosis
The differential diagnosis of the childhood vision loss is best organised by the presentation, because the presentation drives both the tier and the workup. The leukocoria opens the widest differential, and the retinoblastoma heads the list as the diagnosis that must never be missed, followed by the congenital cataract as the commonest cause of the unilateral leukocoria in the high-income setting. The Coats disease, the retinopathy of prematurity, the persistent fetal vasculature and the toxocariasis fill out the list, and the candidate who walks through them from the most dangerous to the commonest demonstrates the breadth the examiner rewards. [5]
The sudden painless loss of vision opens a different differential that the generalist must hold alongside the ophthalmology referral. The optic neuritis, often the first presentation of a demyelinating process in the older child, presents with the pain on the eye movement, the reduced colour vision and the relative afferent pupillary defect. The cortical visual impairment, the commonest cause of the bilateral vision impairment in the developed world, presents with the poor visual behaviour and the normal eye examination in a child with the perinatal hypoxic-ischaemic injury, the structural brain malformation or the prematurity. [7][10]
The optic nerve hypoplasia and the septo-optic dysplasia present with the poor vision, the small pale disc and the midline brain defects, and they carry the hidden endocrinopathy that the pituitary workup must uncover. The papilloedema of the raised intracranial pressure, whether from the idiopathic intracranial hypertension or the space-occupying lesion, presents with the headache, the vomiting, the transient visual obscurations and the swollen disc. The painful red eye carries the orbital cellulitis, the acute glaucoma, the corneal ulcer and the iritis, and the fellow who frames each differential by the tier demonstrates the integrated reasoning the boards reward. [8][9]
Leukocoria
retinoblastoma first
- Retinoblastoma, the mass with the calcification
- Congenital cataract, the lens opacity
- Coats disease, the exudative detachment
- Retinopathy of prematurity, the fibrotic scar
- Persistent fetal vasculature and toxocariasis
Sudden painless loss
optic nerve or brain
- Optic neuritis, the pain on eye movement
- Cortical visual impairment, the normal eye
- Papilloedema of the raised pressure
- Optic nerve hypoplasia and septo-optic dysplasia
- Vascular or traumatic event
Painful red eye
not conjunctivitis
- Orbital cellulitis with the proptosis
- Acute angle-closure glaucoma
- Corneal ulcer and the keratitis
- Anterior uveitis and the iritis
- Trauma, including the occult globe rupture
Clinical & Bedside Assessment
The bedside assessment that drives the triage tier is built from five tools that every generalist can perform, and the candidate who executes them in the correct order demonstrates the clinical fluency the boards reward. The first is the red reflex test, performed in the dim room with the direct ophthalmoscope at roughly thirty centimetres, with the ophthalmoscope set to zero or a low dioptre, and the light shone at both pupils simultaneously while the examiner compares the colour and the brightness. The normal reflex is the warm orange-red, symmetric and filling the pupil, and any white, black, absent or asymmetric reflex is abnormal. [2][4]
The red reflex test is performed at the newborn examination, at the six-week check and at every well-child visit, and it is the single tool that catches the leukocoria and the cataract before the amblyopia sets in. The sensitivity is modest and the specificity is imperfect, so a normal reflex in a child with a concerning history does not exclude the disease, and the examination under anaesthesia by the ophthalmology service remains the standard for the high-risk child. The systematic review of the neonatal red reflex confirmed its value as a screening tool and its limits as a diagnostic one. [2][3]
The second tool is the vision assessment, tailored to the age, from the fixing and following of the infant through the picture acuity of the toddler to the Snellen chart of the school-age child. The third is the cover test for the strabismus, the fourth is the pupil examination for the relative afferent pupillary defect, and the fifth is the fundus examination for the disc swelling, the pallor and the retinal lesion. The five tools together generate the picture that places the child into the correct referral tier, and the fellow who performs them in the dim room, calmly and completely, is the fellow who never under-calls the red flag. [4][7]
The five tools of the bedside triage
Investigations
The investigations in the urgent pathway are selected by the presentation and the tier, and the generalist who over-investigates before the referral loses the time that the child cannot afford. The leukocoria and the abnormal red reflex need no pre-referral imaging in the generalist's hands, because the examination under anaesthesia, the ocular ultrasound and the magnetic resonance imaging are the tools of the ophthalmology service. The computed tomography is avoided in the child because of the radiation and the second-malignancy risk in the heritable disease. [5][6]
The sudden loss of vision with the optic nerve signs prompts the magnetic resonance imaging of the brain and the orbits, with the contrast and the fat suppression, to characterise the optic neuritis and to screen for the demyelinating lesions. The papilloedema prompts the urgent neuroimaging to exclude the mass, the venous sinus thrombosis and the hydrocephalus before the lumbar puncture confirms the raised pressure and the idiopathic intracranial hypertension. The optic nerve hypoplasia and the septo-optic dysplasia prompt the magnetic resonance imaging of the midline and, crucially, the endocrine workup for the growth-hormone and the cortisol deficiency. [8][9]
The orbital cellulitis prompts the contrast-enhanced computed tomography of the orbits and the sinuses to define the abscess and the orbital extension, and the blood culture and the inflammatory markers guide the intravenous antibiotic. The generalist's role across all of these is to make the referral and to set the investigation in motion with the specialist, not to delay the child for the tests that the specialist will perform better. [9][12]
[5] [6]Management — Resuscitation
The resuscitation phase of the urgent pathway is where the generalist intervenes directly, because the first aid decides whether the eye survives the journey to the specialist. The chemical injury is irrigated copiously with the saline or the water for at least thirty minutes, with the lid retracted and the eye everted to clear the fornices, before and during the referral, because the alkali continues to penetrate the cornea until it is diluted. The suspected globe rupture is shielded, not patched and not examined, and the child is kept fasting and nil by mouth for the theatre. [4][12]
The orbital cellulitis with the proptosis and the reduced vision is started on the broad-spectrum intravenous antibiotic that covers the streptococcus, the staphylococcus and the Haemophilus, and the child is referred immediately for the imaging and the joint care. The raised intracranial pressure with the papilloedema, the depressed conscious state or the focal deficit is a neurosurgical emergency, and the child is stabilised, imaged and referred before the lumbar puncture, because the lumbar puncture in the obstructed flow can herniate the brainstem. [9]
The acute angle-closure glaucoma and the corneal ulcer are referred for the immediate ophthalmology care, and the generalist does not instil the drops or the ointments that might obscure the specialist's view, with the one exception of the copious irrigation for the chemical injury. The fellow who performs the first aid correctly and then makes the call demonstrates the resuscitation mindset that the boards reward. [4][12]
The immediate resuscitation before the referral
Chemical injury
Irrigate copiously for at least thirty minutes, evert the lids, check the pH, and refer immediately
Suspected globe rupture
Shield the eye, do not patch or examine, keep the child nil by mouth, and refer immediately
Orbital cellulitis
Start the broad-spectrum intravenous antibiotic, and refer immediately for the imaging and the joint care
Raised intracranial pressure
Stabilise and image before the lumbar puncture, and involve the neurosurgery
Management — Definitive & Stepwise
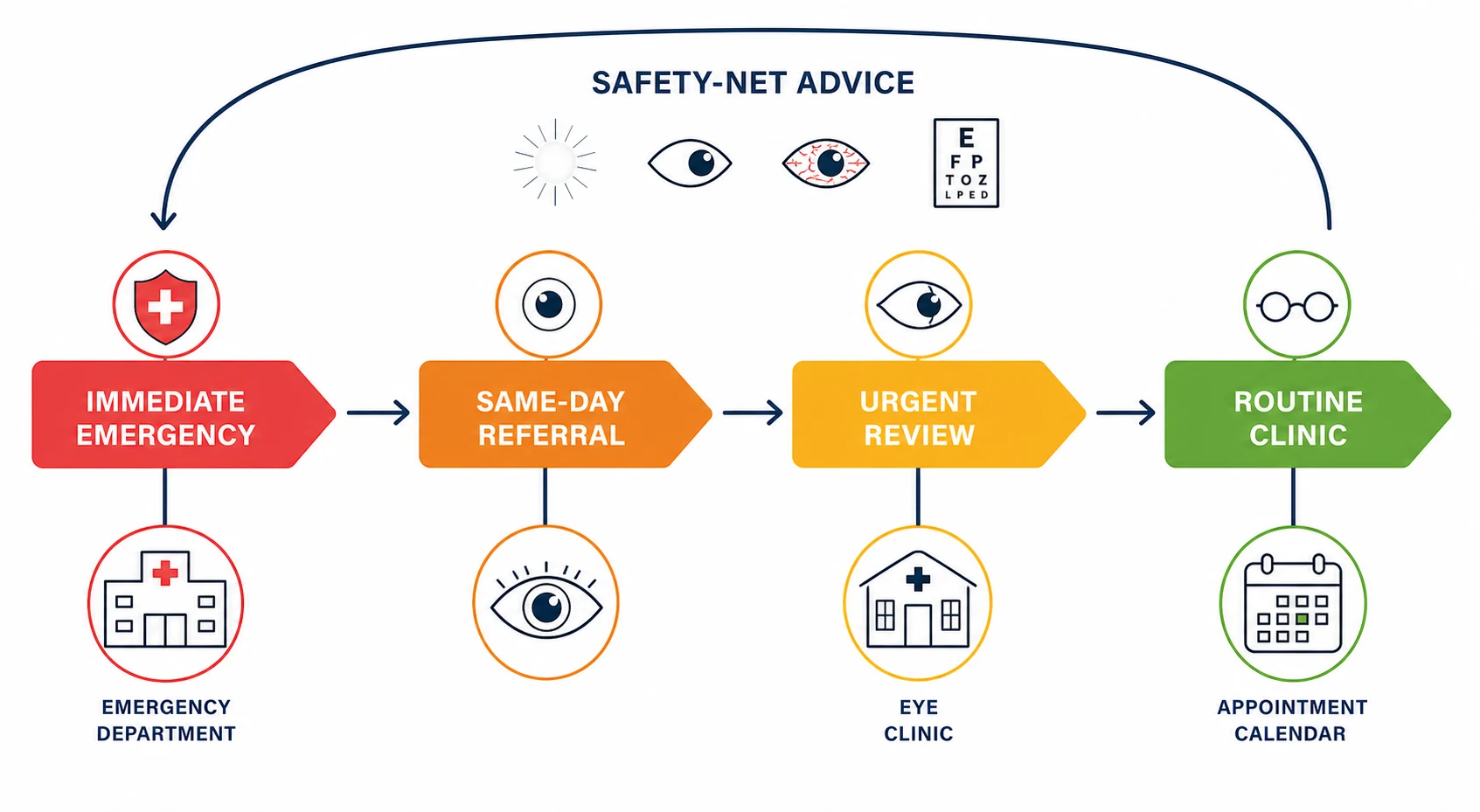
The definitive management is the execution of the tier, and the stepwise pathway runs from the referral call through the specialist assessment to the risk-adapted treatment. The immediate emergencies are sent to the emergency department with the first aid done and the specialist alerted, and the same-day referrals are called through to the ophthalmology service with the red-flag feature named. The generalist who names the red-flag feature in the referral call, rather than the vague eye problem, accelerates the specialist triage and protects the child. [4][6]
[4] [11]The same-day referral for the leukocoria leads to the examination under anaesthesia, the ocular ultrasound and the magnetic resonance imaging, and then to the risk-adapted treatment of the retinoblastoma or the cataract surgery within weeks for the deprivation. The same-day referral for the new strabismus under two years leads to the fundus examination that excludes the retinoblastoma before the amblyopia therapy. The same-day referral for the sudden loss of vision leads to the magnetic resonance imaging, the steroid protocol for the optic neuritis and the workup for the demyelination. [6][10]
The urgent and the routine tiers complete the pathway, with the preseptal cellulitis that fails the first treatment stepped up to the urgent review and the stable refractive error sent to the routine clinic. The safety-net advice, given to every family at every tier, names the features that should bring the child back sooner, because the preverbal child cannot report the deterioration. The fellow who closes the loop with the safety-net demonstrates the disposition skill that the boards reward. [11][12]
[4] [11]Specific Subtypes & Scenarios
The leukocoria scenario is the centrepiece of the urgent pathway, and the candidate who handles it flawlessly secures the marks. The white pupillary reflex, found on the red reflex test or the photograph, is retinoblastoma or a congenital cataract until proven otherwise, and the child is referred the same day to the ophthalmology service. The retinoblastoma presents as the cream-white mass behind the lens with the dilated vessels and the possible strabismus, the congenital cataract as the opacity within the lens, and the delay of weeks converts the curable intraocular tumour into the lethal extraocular disease. [5][6]
The painful red eye with the proptosis is the orbital cellulitis scenario, and the generalist must separate it from the benign preseptal cellulitis at the bedside. The proptosis, the painful and the restricted eye movement, the reduced vision, the relative afferent pupillary defect and the systemic toxicity are the signs that the infection has crossed the orbital septum, and the child is referred immediately for the imaging and the intravenous antibiotic. The conjunctivitis, by contrast, does not hurt, does not drop the vision and does not swell the lid, and the discharge alone points to the common, the self-limiting course. [12][9]
The sudden painless loss of vision is the scenario that brings the optic neuritis, the cortical visual impairment and the optic nerve hypoplasia into the same consultation. The optic neuritis presents with the pain on the eye movement, the reduced colour vision and the relative afferent pupillary defect, and the child needs the urgent magnetic resonance imaging and the steroid protocol. The cortical visual impairment presents with the poor visual behaviour and the normal eye in the child with the brain injury, and the optic nerve hypoplasia presents with the small disc and the risk of the endocrinopathy that the septo-optic dysplasia workup uncovers. [7][8]
The papilloedema of the raised intracranial pressure is the scenario where the eye carries the sign of the brain, and the optic nerve is being crushed by the pressure. The idiopathic intracranial hypertension presents with the headache, the transient visual obscurations, the pulsatile tinnitus and the swollen disc in the older, often the overweight, child, and the lumbar puncture confirms the raised pressure after the imaging excludes the mass. The space-occupying lesion presents with the focal deficit and the progressive course, and the urgency is absolute. [9][10]
A red-flag presentation walked through the tiers
Complications & Pitfalls
The complications of the delayed or the under-tiered referral are the irreversible amblyopia, the loss of the eye and, in the retinoblastoma, the loss of the life, and the fellow who names them in the order of their gravity demonstrates the safety reasoning the boards reward. The amblyopia is the legacy of the deprivation that the cortex could not recover, and the loss of the eye is the legacy of the orbital cellulitis or the globe rupture that the first aid did not protect. The pitfall of the under-called tier is the commonest source of the avoidable harm. [1][11]
The first pitfall is the dismissal of the red eye as the conjunctivitis, because the conjunctivitis does not hurt, does not drop the vision and does not swell the lid, and the orbital cellulitis hides behind the comfortable diagnosis. The second pitfall is the reassurance of the parent who saw the white glow, because the photograph leukocoria is retinoblastoma until proven otherwise, and the wait-and-see approach costs the eye and the life. The third pitfall is the failure to examine the fundus of the child with the new strabismus, because the tumour behind the fovea presents with the drift before the leukocoria. [5][12]
The fourth pitfall is the normal red reflex in the child with the concerning history, because the sensitivity of the test is modest and the examination under anaesthesia remains the standard for the high-risk child. The fifth pitfall is the computed tomography in the child with the leukocoria, because the radiation and the second-malignancy risk in the heritable disease make the magnetic resonance imaging the modality of choice. The fellow who names these five pitfalls demonstrates the defensive reasoning that protects the child. [2][6]
Prognosis & Disposition
The prognosis of the childhood vision loss is determined by the tier of the referral, the age of the child and the cause of the problem, and the disposition is the structured follow-up that the tier defines. The retinoblastoma referred the same day carries the survival above ninety-five percent in the high-income setting, while the retinoblastoma referred late, with the proptosis and the extraocular disease, carries the survival below forty percent. The amblyopia treated in the sensitive period recovers the vision, while the amblyopia treated late leaves the deficit. [1][6]
The cortical visual impairment carries a prognosis that tracks the underlying brain, with the improvement in the child with the recoverable injury and the stable deficit in the child with the structural malformation. The optic neuritis carries a good recovery of the vision in most children, but it carries the risk of the subsequent demyelination that the follow-up must screen for. The idiopathic intracranial hypertension carries the risk of the permanent visual loss if the pressure is not controlled, and the visual field monitoring is the cornerstone of the follow-up. [7][9]
The disposition is the tiered follow-up, with the immediate emergencies admitted, the same-day referrals seen in the clinic, the urgent reviews booked in one to two days and the routine referrals seen in weeks. The safety-net advice and the written instructions close the loop at every tier, because the family is the second pair of eyes on the preverbal child, and the prompt return is the safety that the system cannot otherwise guarantee. [9][11]
Special Populations
The preverbal child is the population in whom the vision loss hides, because the infant cannot report the blur, the field loss or the loss of the colour, and the clinician depends on the red reflex, the fixing and following and the parental concern. The fellow who weights the preverbal child heavily in the triage, and who trusts the parent who saw the white glow, demonstrates the population reasoning that protects the most vulnerable. [1][4]
The child with the complex neurology and the disability is the population in whom the cortical visual impairment and the optic nerve disease dominate, and the vision assessment is adapted to the cooperation and the communication. The child with the septo-optic dysplasia carries the hidden endocrinopathy, and the cortisol deficiency can decompensate the child in the stress, so the endocrine workup is never optional. The child in the remote community, where the specialist is far and the red reflex is not checked, is the population in whom the retinoblastoma presents with the proptosis and the amblyopia presents late. [7][8]
The child in the out-of-home care, the child of the migrant or the refugee family and the child in the socioeconomically disadvantaged household are the populations in whom the screening is missed and the awareness is low. The tiered pathway must reach them through the telehealth, the school screening and the primary-care vigilance. The fellow who names the equity dimension of the childhood vision loss demonstrates the public-health reasoning the boards reward. [1][11]
The high-income setting, with the red reflex at the newborn and the well-child visits and the accessible specialist, presents the retinoblastoma with the leukocoria and carries the survival above ninety-five percent. The low-income setting, without the screening and the specialist, presents the retinoblastoma with the proptosis and carries the survival below forty percent, because the national income determines the speed of the referral and the access to the care.
[1][6]Evidence, Guidelines & Regional Differences
The evidence base for the red reflex screening is anchored in the newborn and the neonatal studies that defined the sensitivity and the specificity of the test, and in the systematic review that consolidated them into the practice. The sensitivity is modest and the specificity is imperfect, so the red reflex is a screening tool that catches the leukocoria and the cataract but does not exclude the disease in the high-risk child, and the examination under anaesthesia remains the standard. The red reflex is performed at the newborn examination, the six-week check and every well-child visit across the high-income settings. [2][3]
The guidelines converge on the principle that the red-flag presentations, the leukocoria, the new strabismus under two years and the painful red eye with the proptosis, demand the same-day referral, and that the immediate emergencies, the globe rupture, the chemical injury and the raised intracranial pressure, demand the emergency-department care. The American Academy of Pediatrics, the American Academy of Ophthalmology and the Royal College of Paediatrics and Child Health align on the red reflex at the well-child visits and the prompt referral of the abnormal finding. [3][4]
The regional difference is the access, and the access is the determinant of the outcome. The high-income setting with the universal screening, the accessible specialist and the telehealth reaches the child in the remote community, while the low-income setting without the screening presents the disease late. The fellow who frames the evidence, the guidelines and the access as the three legs of the urgent pathway demonstrates the integrated reasoning the boards reward. [1][11]
Exam Pearls
The single highest-yield fact for the exam is that the white pupillary reflex, the absent or the asymmetric red reflex and the new strabismus under two years are retinoblastoma or a congenital cataract until proven otherwise. They demand the same-day referral, because the delay of weeks converts the curable into the irreversible and the survivable into the lethal. The second is that the painful red eye with the proptosis, the reduced vision or the relative afferent pupillary defect is the orbital cellulitis or the sight-threatening emergency, not the conjunctivitis. The conjunctivitis does not hurt, does not drop the vision and does not swell the lid. [4][6]
The third is that the childhood vision loss is time-critical through the amblyopia sensitive period of the first seven to eight years, because the cortex wires itself to the retinal image and the deprivation in the window becomes the permanent deficit. The fourth is that the red reflex test is performed in the dim room with the direct ophthalmoscope at thirty centimetres, at the newborn, the six-week check and every well-child visit, and any abnormality is referred the same day. The chemical injury is irrigated first, the globe rupture is shielded, and the raised intracranial pressure is imaged before the lumbar puncture. [2][11]
The fifth is that the cortical visual impairment is the commonest cause of the bilateral vision impairment in the developed world, and the optic nerve hypoplasia carries the hidden endocrinopathy of the septo-optic dysplasia. The candidate who holds the five red-flag presentations, the four tiers, the five bedside tools and the amblyopia sensitive period in a single mental map answers every question the examiner can ask from this topic. [7][8]
References
- [1]Solebo AL, Teoh L, Rahi J Epidemiology of blindness in children Arch Dis Child, 2017.PMID 28465303
- [2]Sun M, Ma A, Li F, et al Sensitivity and Specificity of Red Reflex Test in Newborn Eye Screening J Pediatr, 2016.PMID 27640356
- [3]Taksande A, Jameel PZ, Taksande B, et al Red reflex test screening for neonates: A systematic review and meta analysis Indian J Ophthalmol, 2021.PMID 34304165
- [4]McLaughlin C, Levin AV The red reflex Pediatr Emerg Care, 2006.PMID 16481935
- [5]Patel N, Salchow DJ, Materin M Differentials and approach to leukocoria Conn Med, 2013.PMID 23589950
- [6]Nag A, Khetan V Retinoblastoma - A comprehensive review, update and recent advances Indian J Ophthalmol, 2024.PMID 38804799
- [7]Ospina LH Cortical visual impairment Pediatr Rev, 2009.PMID 19884281
- [8]Kumar V, Karunakaran A, Valakada J Septo-optic dysplasia Int Ophthalmol, 2018.PMID 28050731
- [9]Gaier ED, Heidary G Pediatric Idiopathic Intracranial Hypertension Semin Neurol, 2019.PMID 31847041
- [10]Lehman SS, Lavrich JB Pediatric optic neuritis Curr Opin Ophthalmol, 2018.PMID 30096089
- [11]Levi DM Rethinking amblyopia 2020 Vision Res, 2020.PMID 32866759
- [12]Wong MM, Anninger W The pediatric red eye Pediatr Clin North Am, 2014.PMID 24852155