Paeds · ophthalmology
Uveitis in children
Also known as Iritis · Iridocyclitis · Anterior uveitis · Juvenile idiopathic arthritis uveitis · JIA-associated uveitis · Intermediate uveitis · Pars planitis · Ocular toxoplasmosis · Ocular toxocariasis
Fellowship topic on uveitis in children: the SUN anatomical classification of anterior, intermediate, posterior and panuveitis; the chronic silent anterior uveitis associated with juvenile idiopathic arthritis that is detected only by slit-lamp screening; the T-cell mediated autoimmune breakdown of the blood-aqueous barrier producing cells and flare; the 2019 ACR and Arthritis Foundation risk-stratified screening schedule based on JIA subtype, ANA status, age at onset and disease duration; the stepwise treatment from topical prednisolone acetate one percent and cycloplegia through systemic methotrexate to biologic anti-TNF adalimumab anchored by the SYCAMORE trial; the sight-threatening complications of band keratopathy, cataract, glaucoma, posterior synechiae and amblyopia; and the differential of non-infectious versus infectious uveitis including ocular toxoplasmosis and toxocariasis and TINU syndrome.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old girl with a swollen right knee for three months. She has oligoarticular juvenile idiopathic arthritis, ANA positive, diagnosed last month. Her eyes look completely normal. She has no eye pain, no redness, no photophobia, no visual complaint — yet her slit-lamp examination reveals grade 2+ cells and 1+ flare in both anterior chambers. This is the paradigm of childhood uveitis: the disease that blinds while the child looks and feels well, and the reason why slit-lamp screening exists. [3] [4]
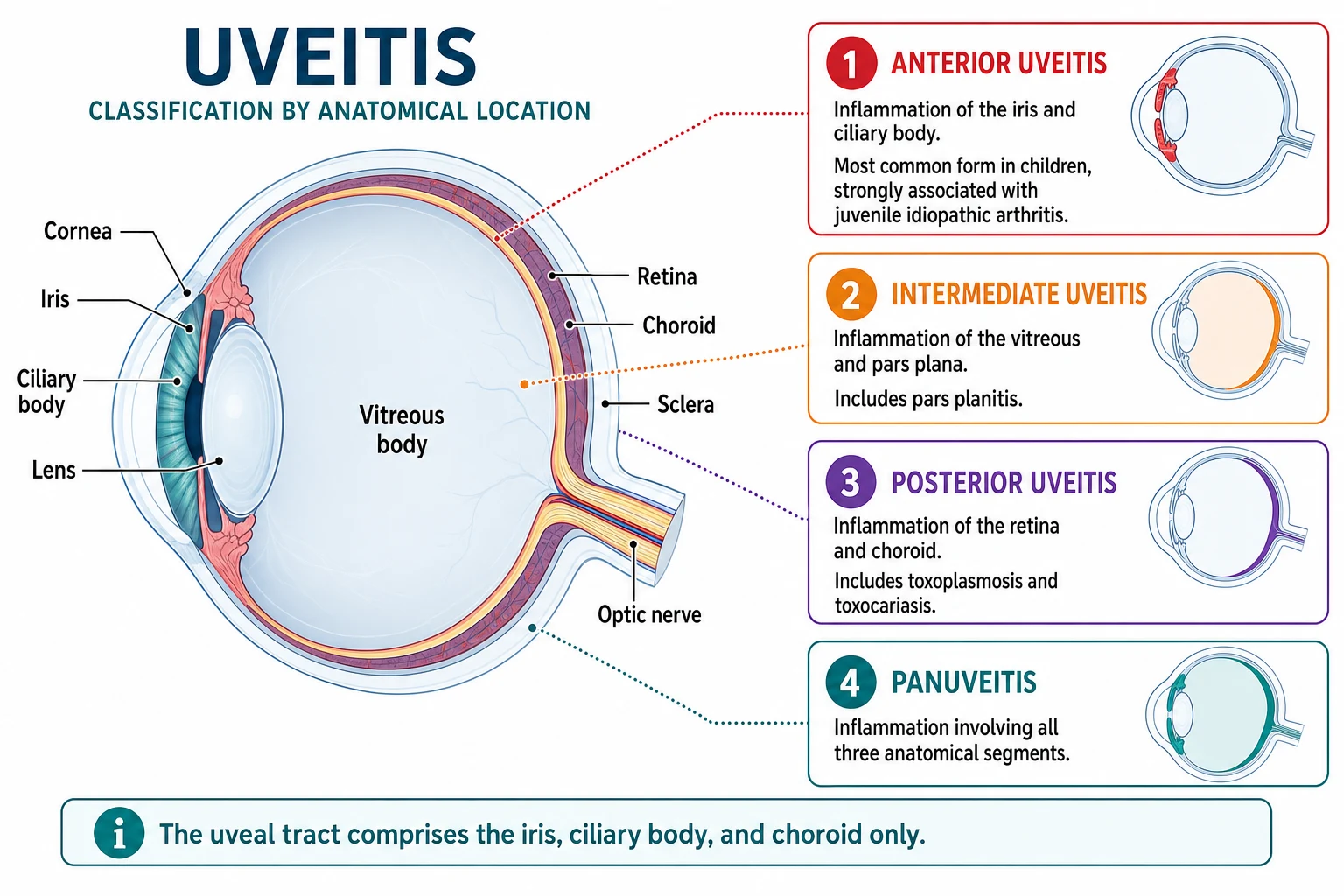
Uveitis is inflammation of the uveal tract — the iris, the ciliary body and the choroid. In practice the term extends to inflammation of adjacent structures, so anterior uveitis involves the iris and ciliary body, intermediate uveitis involves the vitreous and pars plana, and posterior uveitis involves the retina and choroid. The Standardization of Uveitis Nomenclature (SUN) working group formalised this anatomical classification in 2005 so that disease activity and treatment response could be reported consistently across centres. [1]
Why does this matter for the paediatrician? Because the single most important thing you can do for a child with JIA is to screen for uveitis. The disease is silent, the progression to irreversible structural damage is gradual, and the window for prevention closes once cataract, band keratopathy or amblyopia develop. Every child newly diagnosed with JIA needs a baseline slit-lamp examination and a planned surveillance schedule — this is non-negotiable, and it is the general paediatrician's responsibility to ensure it happens. [7] [3]
Classification
Classify childhood uveitis by anatomy, because the anatomical site predicts the cause, the clinical features and the treatment approach. The SUN anatomical scheme sorts uveitis into four zones, each defined by the primary site of inflammation visible on examination. [1] [9]
Anterior uveitis — inflammation of the iris and ciliary body (iritis or iridocyclitis) — is the commonest form in children. It is the form associated with JIA, and it accounts for the majority of paediatric uveitis in developed settings. The SUN system also grades anterior chamber inflammation: cells are counted per high-power field (0, 0.5+, 1+, 2+, 3+, 4+) and flare is graded by intensity (0 to 4+), giving a reproducible measure of disease activity that guides treatment decisions. [1]
Intermediate uveitis involves the vitreous and the pars plana, the peripheral retina where inflammatory exudates form a characteristic snowbank. The idiopathic form is called pars planitis. Posterior uveitis involves the retina and choroid, and in children it is dominated by infectious causes — toxoplasmosis producing focal necrotising retinochoroiditis, and toxocariasis producing a granulomatous choroidal mass. Panuveitis involves all three zones. [9] [10]
The second axis of classification is cause: non-infectious (autoimmune) versus infectious. Non-infectious uveitis includes the JIA-associated form, HLA-B27 acute anterior uveitis, sarcoidosis, Behcet disease, inflammatory bowel disease and TINU syndrome. Infectious uveitis includes toxoplasmosis, toxocariasis, tuberculosis, syphilis and viral retinitis. The cause dictates the treatment: immunosuppression for non-infectious disease, antimicrobials for infectious disease, and a careful combination when infection drives an immune response that also needs suppression. [8] [9]
Epidemiology & Risk Factors
Childhood uveitis is uncommon overall, but it is disproportionately sight-threatening because it strikes the visually immature eye during the amblyopia-sensitive years. The burden of disease and its complications fall heaviest on the youngest children, who have the least ability to report visual change and the most to lose from undetected inflammation. [3] [4]
The commonest childhood uveitis in developed settings is chronic anterior uveitis associated with JIA. Among children with JIA, roughly ten to twenty percent develop uveitis, and the disease is already present at or shortly after the arthritis diagnosis in the majority. The synthesis of the literature by Carvounis and colleagues established the incidence patterns and the visual outcomes that drove the creation of structured screening programmes. [4] [3]
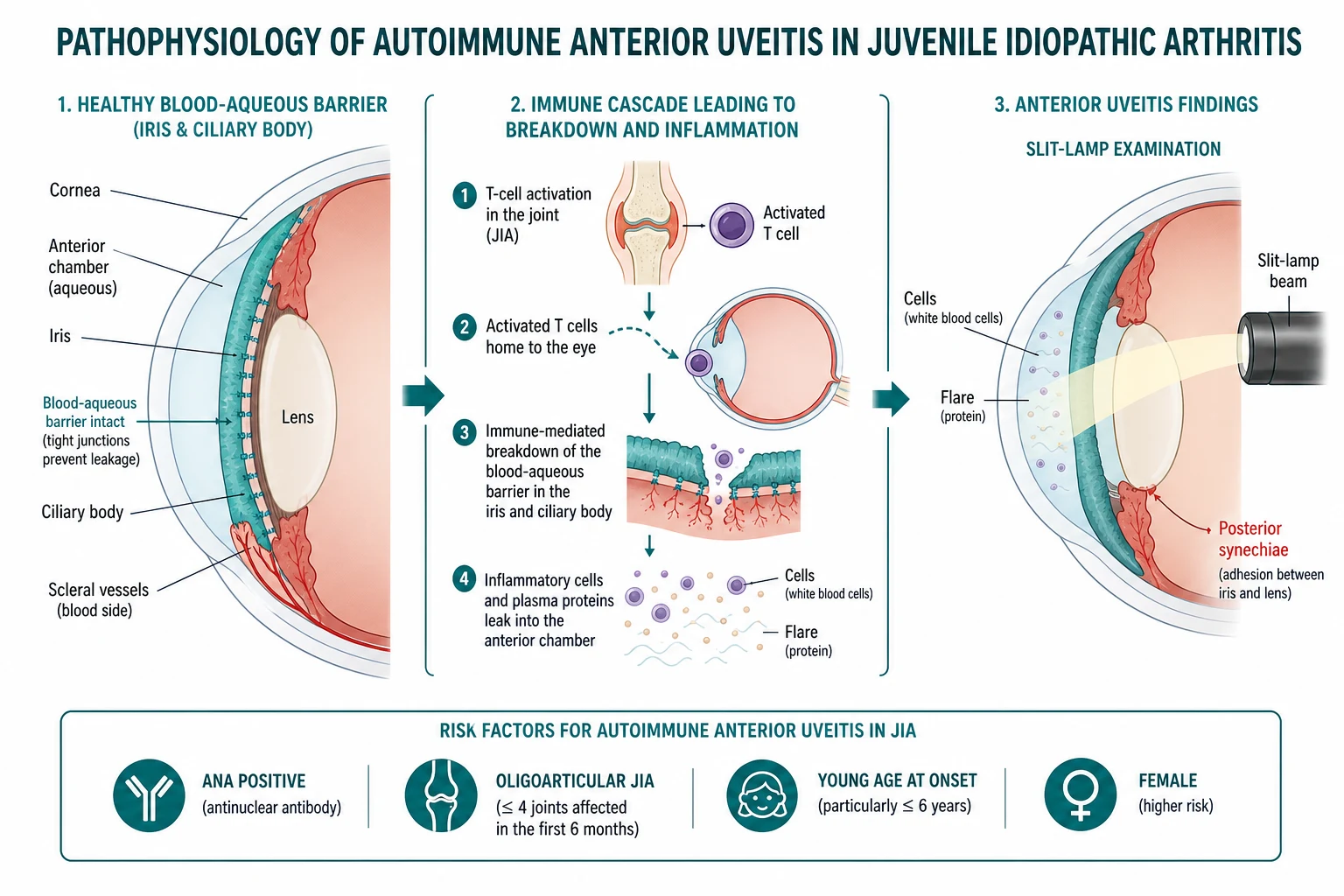
The risk factors for JIA-associated uveitis are the single highest-yield fact in this topic, because they determine the screening schedule. The high-risk profile is: ANA positive, oligoarticular JIA subtype (or rheumatoid-factor-negative polyarthritis), young age at onset (under seven years), and short disease duration (under four years from diagnosis). Female sex and the absence of systemic symptoms add to the risk. These children are the ones who need slit-lamp examination every three months. [7] [3]
JIA subtype and uveitis risk
Low
The JIA subtypes at low risk of uveitis are systemic JIA and rheumatoid-factor-positive polyarthritis — these children still need a baseline slit-lamp and less frequent surveillance. Importantly, uveitis may precede the arthritis in a minority of children: a child presenting with unexplained chronic anterior uveitis must be evaluated for JIA, because the eye disease may be the first manifestation. [7] [3]
In Australia and Aotearoa New Zealand, the burden of childhood uveitis and its complications is shaped by access to slit-lamp surveillance. Aboriginal and Torres Strait Islander, Maori and Pasifika children in rural and remote communities face the same disease risk with fewer opportunities for regular ophthalmology review, and the determinants — distance, transport, workforce and cultural safety — are what determine whether a high-risk child actually gets their three-monthly slit-lamp. The general paediatrician in these settings is often the linchpin of adherence, and telehealth-supported screening and regional outreach models are part of the solution. [7] [8]
Pathophysiology
Why does a child with a swollen knee develop silent inflammation inside the eye? The answer lies in a shared autoimmune mechanism that targets both the joint and the eye through a breakdown of the normal immune privilege of the anterior chamber. [3] [2]
Non-infectious anterior uveitis is a T-cell mediated autoimmune process. Autoreactive CD4-positive T-helper-1 and T-helper-17 lymphocytes directed against ocular antigens breach the blood-aqueous barrier — the tight junctional barrier between the iris and ciliary body vasculature and the anterior chamber that normally keeps the aqueous clear and cell-free. Once the barrier breaks, protein leaks into the aqueous (producing flare) and inflammatory cells enter (producing cells), and these slit-lamp findings are the direct readout of active inflammation. [2] [1]
The same persistent inflammation drives the structural complications that define the natural history of untreated disease. Fibrin in the anterior chamber causes the iris to adhere to the anterior lens surface, forming posterior synechiae that can seclude the pupil and block aqueous flow. Chronic inflammation deposits calcium hydroxyapatite in the corneal basement membrane, producing band keratopathy — the white plaque across the cornea that is a tell-tale sign of long-standing disease. The lens opacifies (cataract), the trabecular meshwork scars and inflames (secondary glaucoma), and cystoid macular oedema may develop in the posterior pole. [3] [4]
In the visually immature child, the stakes are higher than in the adult. Any media opacity — cataract, band keratopathy, or even dense flare — deprives the developing visual cortex of a clear image, and the result is amblyopia: permanent cortical visual impairment that persists even if the structural eye disease is later treated. This is why childhood uveitis blinds more readily than adult uveitis, and why the screening and early-treatment paradigm exists. [4] [9]
The infectious posterior uveitides follow a different mechanism. In ocular toxoplasmosis, Toxoplasma gondii establishes a focal necrotising retinitis with a secondary immune response, producing the characteristic fluffy white retinochoroidal lesion with overlying vitritis — the headlight-in-the-fog appearance. In ocular toxocariasis, the larva of Toxocara canis or Toxocara cati migrates to the choroid and produces a granulomatous mass, vitritis or an inflammatory pseudoglioma that mimics retinoblastoma in the young child. [10] [9]
Clinical Presentation
The clinical presentation of childhood uveitis depends on the form, and the contrast between the chronic anterior and the acute anterior forms is the key teaching point. [3] [9]
JIA-associated chronic anterior uveitis is asymptomatic. The eye is white, there is no pain, no redness, no photophobia, no discharge and no visual complaint. The child plays normally, reads normally and is entirely unaware of the inflammation inside both eyes. This is why the disease blinds: there is no symptom to prompt presentation, and the inflammation smoulders for months to years until a structural complication — band keratopathy, cataract, an irregular pupil from synechiae, or behavioural visual impairment — finally brings the child to attention, often too late to reverse the damage. The defence is slit-lamp screening, not symptom surveillance. [3] [4]
The red-flag features that suggest symptomatic or advanced disease at presentation deserve memorising. A small or irregular pupil suggests posterior synechiae. A white or grey corneal plaque is band keratopathy. A cloudy lens is cataract. Leukocoria, squinting, or behavioural visual change (sitting closer to the television, stumbling, declining school performance) signal that structural damage or amblyopia has developed. A red painful eye with photophobia in an adolescent suggests the acute anterior uveitis pattern of HLA-B27-associated disease — a very different tempo from the chronic JIA form, and one that does present with symptoms. [8] [9]
On slit-lamp examination, the active anterior uveitis signs are: cells (small inflammatory cells floating in the anterior chamber beam, graded 0 to 4+), flare (protein haze in the aqueous, graded 0 to 4+), keratic precipitates (clumps of inflammatory cells deposited on the corneal endothelium), and posterior synechiae (iris-to-lens adhesions). The intraocular pressure may be low from ciliary body shutdown or high from trabecular meshwork inflammation — secondary glaucoma. Intermediate uveitis produces floaters and snowbanking at the pars plana, and posterior uveitis produces reduced vision with focal retinitis or choroiditis and vitritis. [1] [9]
Differential Diagnosis
The differential diagnosis of childhood uveitis has two layers: first, separating uveitis from the other causes of a red or abnormal eye, and second, identifying the underlying cause of the uveitis itself. [8] [9]
For the child with a red eye, the critical distinction is between uveitis and the benign causes. Conjunctivitis produces discharge and grittiness without cells, flare, photophobia or visual loss. Keratitis produces a corneal staining defect with photophobia and pain. Acute angle-closure glaucoma produces a hazy cornea, a fixed mid-dilated pupil and a high pressure. Corneal abrasion follows trauma with a sudden foreign-body sensation. The feature that separates uveitis from all of these is the slit-lamp finding of cells and flare in the anterior chamber — but a red eye with photophobia must always be examined by slit-lamp with fluorescein before topical steroid, because herpes simplex keratitis mimics uveitis and is catastrophically worsened by steroid. [9] [1]
For the underlying cause of non-infectious anterior uveitis, the differential is the group of childhood autoimmune diseases: JIA (the commonest), juvenile spondyloarthritis and HLA-B27 (acute recurrent unilateral anterior uveitis with enthesitis and back pain), inflammatory bowel disease, psoriatic arthritis, sarcoidosis (with iris nodules — Koeppe and Busacca), Behcet disease (with oral and genital ulcers), and TINU syndrome (tubulointerstitial nephritis and uveitis, often after beta-lactam antibiotic exposure, with elevated creatinine and sterile pyuria). [8] [9]
For posterior uveitis, the differential is dominated by infection: ocular toxoplasmosis (focal necrotising retinochoroiditis, the commonest), ocular toxocariasis (granulomatous mass in a child with puppy or soil exposure), tuberculosis and syphilis. In the immunocompromised child, cytomegalovirus retinitis enters the differential with its characteristic pizza-pie appearance of haemorrhagic necrosis. Non-infectious posterior uveitis includes Vogt-Koyanagi-Harada disease (bilateral granulomatous panuveitis with meningismus and skin and hair changes). [10] [9]
[8] [9]Clinical & Bedside Assessment
The assessment of a child with suspected uveitis begins with the recognition that the definitive examination — the slit-lamp — is an ophthalmology skill, and the paediatrician's job is to screen, suspect, refer and coordinate. But every paediatrician can perform the bedside elements that frame the referral. [7] [9]
Take a focused history of any eye symptoms — and, critically, the absence of symptoms in a child with JIA, which is the expected pattern. Ask about the joint symptoms and their timing (morning stiffness, joint swelling, the JIA subtype), skin rashes (psoriasis, erythema nodosum), bowel symptoms (diarrhoea, abdominal pain, weight loss), oral and genital ulcers (Behcet), recent antibiotic exposure and urinary symptoms (TINU), and family history of autoimmune disease. Ask about puppy or soil exposure for toxocariasis, and congenital infection history for toxoplasmosis. [8] [10]
Perform the visual assessment. Check visual acuity in each eye with age-appropriate testing — a decline may be the first sign of amblyopia or macular oedema. Examine the pupils for irregularity, a small pupil, or a relative afferent pupillary defect that suggests optic nerve or retinal involvement. Inspect the eye externally for a white corneal plaque (band keratopathy), redness, an irregular pupil, or leukocoria. In the cooperative child, attempt to assess the red reflex — its asymmetry or absence suggests media opacity from cataract or vitritis. [9] [11]
BEDSIDE: the five things to check before the slit-lamp referral
Recognise that the definitive assessment — slit-lamp biomicroscopy by an ophthalmologist — is the gatekeeper test. It detects cells and flare, keratic precipitates and posterior synechiae that no bedside examination can reveal, and it is the examination that the screening schedule is built around. Every child with newly diagnosed JIA needs a slit-lamp at diagnosis and at planned intervals thereafter, and every child with suspected uveitis needs slit-lamp confirmation before treatment. Perform the full joint examination (swollen and tender joint count, enthesitis) and the systemic examination (fever, rash, lymphadenopathy, abdominal examination) to anchor the underlying diagnosis. [7] [3]
Investigations
The diagnosis of active anterior uveitis is clinical and slit-lamp-based — no blood test makes or excludes it. The cells and flare in the anterior chamber, the keratic precipitates and the posterior synechiae are the diagnosis, and the laboratory work-up serves the underlying cause, not the uveitis itself. [1] [9]
For the child with suspected non-infectious anterior uveitis, order the directed laboratory work-up guided by the clinical pattern. ANA is the key test for JIA risk stratification — a positive ANA in a child with oligoarticular arthritis places them in the high-risk screening group. HLA-B27 supports juvenile spondyloarthritis in the adolescent with acute recurrent anterior uveitis and enthesitis. Rheumatoid factor defines the JIA subtype. Additional tests — ANCA, ACE, lysozyme, angiotensin-converting enzyme — are ordered when vasculitis or sarcoidosis is suspected, not as a blanket screen. [7] [8]
For posterior uveitis, the infectious serology is essential. Send anti-Toxoplasma IgG and IgM for suspected ocular toxoplasmosis (IgG positive with a typical lesion is supportive). Send anti-Toxocara antibodies (serum, and sometimes aqueous humour) for suspected ocular toxocariasis. Send syphilis serology (treponemal and non-treponemal) and QuantiFERON-TB or tuberculin skin test when tuberculosis or syphilis is in the differential. In the immunocompromised child, CMV PCR of aqueous humour may be needed for CMV retinitis. [10] [9]
Reserve imaging for the ophthalmology-led assessment of complications and posterior segment disease. Optical coherence tomography (OCT) quantifies cystoid macular oedema. B-scan ultrasonography images the posterior segment when the view is obscured by cataract, vitritis or band keratopathy. Fluorescein angiography assesses retinal vasculitis, macular ischaemia and the activity of toxoplasmosis lesions. These are specialist tools that complement, not replace, the slit-lamp. [9] [11]
Management — Resuscitation
The time-critical scenarios in childhood uveitis are few but important, and each is an indication for urgent ophthalmology involvement before any treatment is started in the community. [7] [9]
The first is the child with acute severe anterior uveitis — a hypopyon (a layered collection of white cells in the anterior chamber), rapidly forming posterior synechiae, or severe pain and photophobia. This needs urgent ophthalmology and intensive topical corticosteroid with cycloplegia to prevent permanent synechiae, pupil seclusion and secondary glaucoma. A hypopyon may also signal Behcet disease or HLA-B27 disease, and the underlying diagnosis must be pursued in parallel. [8] [9]
The second, and the most dangerous error in all of paediatric ophthalmology, is the red eye that receives topical steroid before slit-lamp and fluorescein examination. Herpes simplex keratitis produces a dendritic ulcer that mimics uveitis with its redness and photophobia, and topical steroid causes corneal melting, thinning and perforation. The rule is absolute: no topical steroid to a red eye until herpes simplex keratitis is excluded by slit-lamp and fluorescein staining. If slit-lamp is not available, refer rather than prescribe. [9] [1]
The third is the child who presents late — with visual impairment, band keratopathy, cataract, or an irregular pupil from chronic undiagnosed uveitis. This is an ophthalmological emergency even though the eye may be white and painless, because the structural damage and the amblyopia may be irreversible without urgent treatment. The general paediatrician's role is recognition, immediate referral and the systemic immunosuppression that the ophthalmology treatment demands. [4] [7]
Management — Definitive & Stepwise
Definitive management is a stepwise ladder that escalates from topical therapy to systemic immunosuppression to biologic, with the goal of zero inflammation (not just reduced inflammation) at every step. The treatment is jointly managed by ophthalmology and paediatric rheumatology, and the general paediatrician coordinates the screening, the referral and the systemic medication adherence. [2] [7]
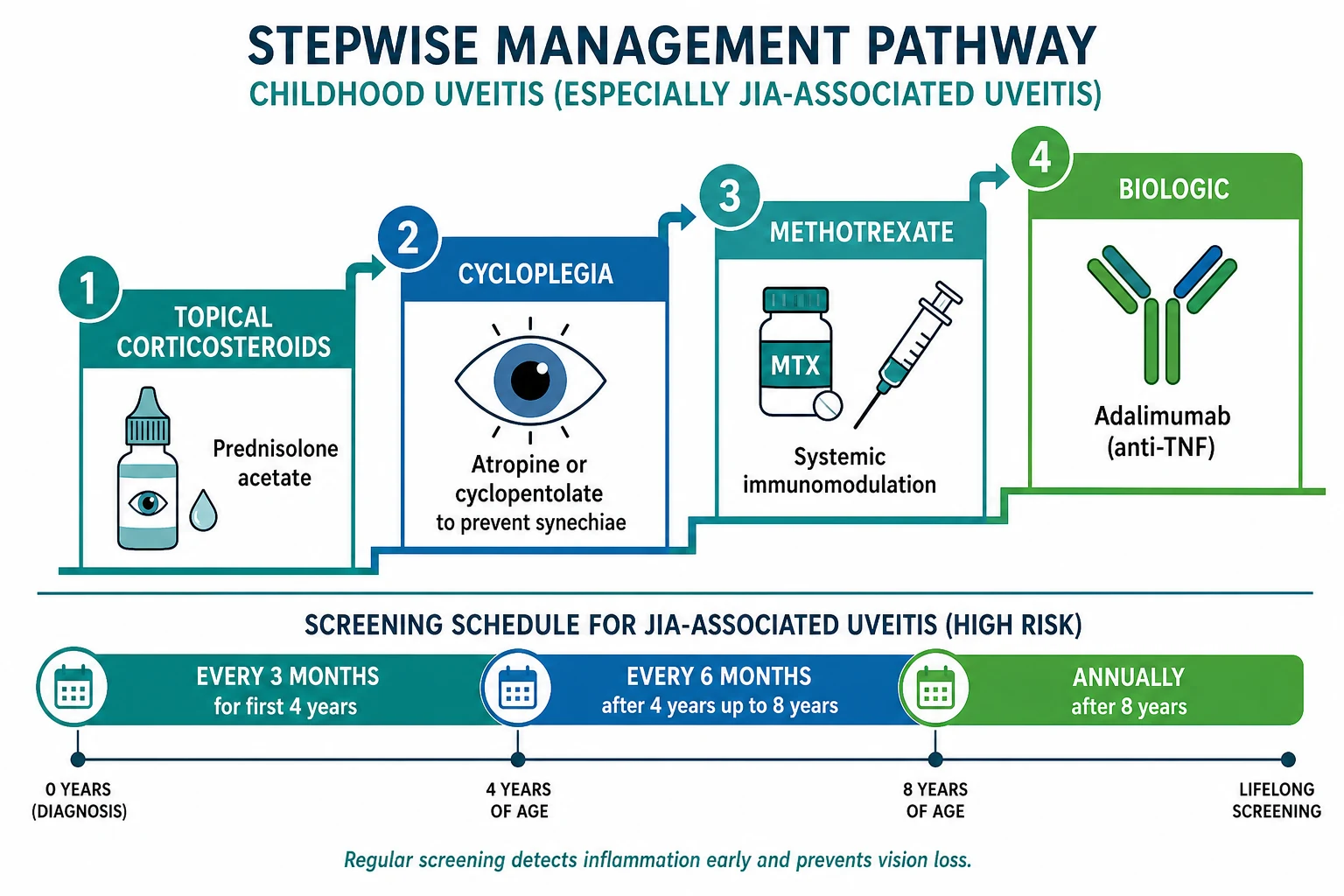
Step one: topical corticosteroid and cycloplegia. The first-line agent for active anterior uveitis is prednisolone acetate 1% eye drops. The frequency depends on severity — every one to two hours initially for moderate to severe disease, tapering as the inflammation settles on slit-lamp review. The essential companion is cycloplegia: atropine 1% or cyclopentolate 1% eye drops immobilise the iris and ciliary body, prevent and break posterior synechiae, and relieve ciliary spasm. Difluprednate 0.05% is a more potent alternative for severe disease. [2] [9]
Uveitis treatment ladder (ACR/AF 2019 and Heiligenhaus 2012 guidelines)
Step two: systemic methotrexate. When uveitis is not controlled by topical steroid alone, or when the child is corticosteroid-dependent or developing steroid complications, escalate to methotrexate 10 to 15 mg per square metre per week (oral or subcutaneous) with folic acid supplementation. Methotrexate is the conventional first-line systemic agent, and it may take two to three months to achieve full effect, so the topical steroid is continued and tapered as the systemic agent takes hold. [2] [8]
Step three: biologic anti-TNF. For uveitis resistant to or dependent on methotrexate, escalate to adalimumab — a monoclonal antibody against tumour necrosis factor alpha. The dose for JIA-associated uveitis in children aged two years and older is 24 mg per square metre subcutaneously every two weeks, up to a maximum of 40 mg per dose. The SYCAMORE trial established the evidence: adalimumab plus methotrexate significantly reduced the risk of treatment failure compared with methotrexate plus placebo in JIA-associated uveitis, making anti-TNF the standard second-line systemic therapy. Infliximab is an alternative anti-TNF agent for refractory disease. [5] [6]
SYCAMORE trial: Adalimumab plus Methotrexate for Uveitis in JIA
Population: Children with JIA-associated chronic anterior uveitis that was active despite methotrexate, randomised to adalimumab or placebo in addition to methotrexate.
Key finding
Adalimumab plus methotrexate significantly reduced the risk of treatment failure compared with methotrexate plus placebo, establishing anti-TNF therapy as the standard second-line systemic treatment for JIA-associated uveitis.
Practice change
Escalate to adalimumab for JIA uveitis that is uncontrolled on or dependent on methotrexate and topical steroid; the trial underpins the 2019 ACR/AF guideline recommendation for biologic therapy.
Step four: local steroid and refractory disease. For refractory unilateral or posterior disease, periocular or intravitreal triamcinolone injection or the fluocinolone acetonide intravitreal implant provides local anti-inflammatory control under specialist ophthalmology guidance. These carry their own risks of cataract and glaucoma, and they are reserved for disease that has failed the systemic ladder. Newer biologics — tocilizumab (anti-IL-6), abatacept, rituximab and golimumab — have emerging roles in anti-TNF-refractory disease. [8] [9]
The stepwise uveitis pathway
Screen first: every child with newly diagnosed JIA gets a baseline slit-lamp and a risk-stratified surveillance schedule (ACR/AF 2019) — high-risk children every 3 months.
Detect active anterior uveitis on slit-lamp: cells and flare, keratic precipitates, posterior synechiae — confirmed by ophthalmology before any treatment.
Exclude herpes simplex keratitis by slit-lamp and fluorescein before any topical steroid in a red eye.
Step one: topical prednisolone acetate 1% (every 1 to 2 hours for moderate to severe disease, tapering) plus cycloplegia with atropine 1% or cyclopentolate 1%.
Step two: systemic methotrexate 10 to 15 mg per square metre per week with folic acid for corticosteroid-dependent or resistant disease.
Step three: biologic adalimumab 24 mg per square metre every 2 weeks (max 40 mg) for methotrexate-resistant or dependent disease, per the SYCAMORE trial evidence.
Safety-net and monitor: slit-lamp review at intervals dictated by disease activity, intraocular pressure checks for steroid-induced glaucoma, and complication surveillance for cataract, band keratopathy and amblyopia.
Specific Subtypes & Scenarios
A four-year-old with oligoarticular ANA-positive JIA and grade 2+ cells on screening. This is the paradigm case. The uveitis was asymptomatic and detected only by the three-monthly screening slit-lamp that the ACR/AF schedule mandates. The management is topical prednisolone acetate 1% with cycloplegia, slit-lamp review at one to two weeks, and escalation to methotrexate if the inflammation does not settle or the child becomes steroid-dependent. The screening has done its job: the disease was caught before complications developed. [7] [3]
A fourteen-year-old boy with a sudden red painful right eye and photophobia. This is acute anterior uveitis, and the pattern — adolescent boy, acute unilateral onset, pain and photophobia — points to HLA-B27-associated spondyloarthritis. Examine by slit-lamp and fluorescein (excluding herpes simplex keratitis), confirm cells and flare, and treat with intensive topical prednisolone acetate 1% and cycloplegia. Refer to rheumatology for the underlying enthesitis-related arthritis: examine the sacroiliac joints, the Achilles tendon and plantar fascia insertions, and ask about inflammatory back pain and bowel symptoms. [8] [9]
A six-year-old with reduced vision and a focal white retinal lesion. This is likely ocular toxoplasmosis — the commonest infectious posterior uveitis. The focal necrotising retinochoroiditis with overlying vitritis gives the headlight-in-the-fog appearance on fundoscopy. Send anti-Toxoplasma serology, and treat sight-threatening lesions near the macula or optic disc with the classic regimen of oral sulfadiazine, pyrimethamine and folinic acid with systemic corticosteroid, under infectious disease and ophthalmology guidance. The old pigmented scar beside the active lesion is the signature of reactivation. [9] [10]
An eight-year-old with a unilateral granulomatous fundus mass and a new puppy. This is ocular toxocariasis — the ocular larva migrans syndrome. The Toxocara canis larva migrates to the choroid and produces a granulomatous mass, vitritis or an inflammatory pseudoglioma that can mimic retinoblastoma in the young child, so the distinction from malignancy is the first step (retinoblastoma is bilateral in a younger child with calcification on imaging). Send anti-Toxocara antibodies and treat with anti-helminthic therapy (albendazole) and systemic corticosteroid under specialist guidance. [10] [9]
A ten-year-old with uveitis, elevated creatinine and sterile pyuria after a course of antibiotics. This is TINU syndrome — tubulointerstitial nephritis and uveitis. The uveitis is typically bilateral anterior, the nephritis often follows a beta-lactam antibiotic or NSAID exposure, and the combination needs systemic corticosteroid for the renal disease alongside topical or systemic steroid for the uveitis. Co-management with nephrology is essential, because the interstitial nephritis may progress to chronic kidney disease if untreated. [8] [9]
A two-year-old with Kawasaki disease and a mildly red eye during the acute illness. This is the transient, self-limiting mild anterior uveitis of Kawasaki disease — bilateral, non-purulent, and resolving with the intravenous immunoglobulin and aspirin treatment of the Kawasaki disease itself. It does not need the chronic uveitis treatment ladder and does not carry the structural-complication risk of JIA uveitis, but it must be distinguished from JIA uveitis in the differential of childhood anterior uveitis. [8] [3]
Complications & Pitfalls
The complications of chronic undiagnosed or undertreated childhood uveitis are the five structural damages that the screening programme exists to prevent, and naming them at viva is expected. [4] [9]
Band keratopathy is the calcium hydroxyapatite plaque deposited in the corneal basement membrane by chronic anterior chamber inflammation. It appears as a white-grey band across the corneal surface, worst in the interpalpebral fissure, and it signals months to years of undetected disease. It may be treated by chelation with EDTA or superficial keratectomy once the inflammation is controlled, but the visual outcome depends on how much amblyopia has developed beneath it. [3] [11]
Cataract develops from both the chronic inflammation and the topical corticosteroid used to treat it — a double-hit. Secondary glaucoma results from trabecular meshwork inflammation and scarring, and it may also be worsened by topical steroid. Posterior synechiae seclude the pupil and can cause pupillary-block glaucoma. Cystoid macular oedema threatens central vision in intermediate and posterior disease. And amblyopia — cortical visual deprivation from any media opacity during the sensitive period — is the most devastating and the most preventable complication, because it is irreversible once the sensitive period closes. [4] [9]
The first pitfall is diagnosing JIA uveitis late because the eye is white and the child is asymptomatic. The defence is adherence to the slit-lamp screening schedule — not waiting for symptoms, and not assuming that a normal-looking eye means a normal anterior chamber. The second pitfall is giving topical steroid to a red eye that has not been examined by slit-lamp and fluorescein for herpes simplex keratitis. The third pitfall is undertreating — aiming for reduced inflammation rather than zero inflammation, which allows smouldering disease to produce complications. The fourth is failing to involve ophthalmology and rheumatology jointly, so that the topical and systemic treatments are uncoordinated. [7] [2]
The fifth pitfall is the complications of treatment itself. Topical and systemic corticosteroid cause cataract and ocular hypertension, so every child on steroid needs intraocular pressure monitoring and a clear taper plan. Methotrexate needs folic acid supplementation, regular blood count and liver function monitoring, and awareness of the slow onset of action. Adalimumab carries infection risks, needs screening for latent tuberculosis before commencement, and requires injection-site and adherence support. The treatment is as much a source of complications as the disease. [8] [2]
Prognosis & Disposition
The prognosis of childhood uveitis depends almost entirely on the timing of detection and the adequacy of sustained inflammation control. Children detected by screening before complications develop, and whose inflammation is suppressed to zero cells and flare with minimal steroid burden, do well. Children presenting with established band keratopathy, cataract, glaucoma or amblyopia may have irreversible visual loss despite the best subsequent treatment — and this is the entire justification for the screening programme. [4] [11]
The structural complications may be irreversible once established. Band keratopathy can be debrided but the amblyopia beneath it persists. Cataract surgery in a uveitic eye is higher-risk and needs the inflammation controlled for at least three months beforehand. Secondary glaucoma may need surgical management. Amblyopia, once the sensitive period closes, is permanent. These outcomes are what the screening and treatment ladder are designed to prevent — and the prevention works when it is applied early and sustained. [9] [3]
The disposition is joint paediatric-rheumatology and ophthalmology outpatient follow-up. The ophthalmology review sets the slit-lamp interval by disease activity — weekly to monthly during active inflammation, extending as the disease settles. The paediatric-rheumatology review manages the systemic immunosuppression (methotrexate or biologic), monitors for drug toxicity and tracks the underlying autoimmune disease. The general paediatrician coordinates the two services, ensures the screening schedule is kept, and supports the family through years of treatment. [7] [2]
Uveitis may remit, or it may run a relapsing or chronic course requiring years of immunosuppression. The transition to adult care must explicitly hand over the uveitis surveillance schedule, the current immunosuppression regimen, the intraocular pressure and complication monitoring, and the reproductive, adherence and psychosocial counselling for a young person living with chronic disease and chronic medication. A poorly planned transition is a common cause of disease recurrence and complication in early adulthood. [8] [9]
Special Populations
Children with JIA are the primary screening population. Apply the 2019 ACR and Arthritis Foundation risk-stratified schedule: high-risk children (ANA positive, oligoarticular or rheumatoid-factor-negative polyarticular JIA, onset under seven years, disease duration under four years) screened every three months for the first four years; the interval extends with longer disease duration and older age; lower-risk subtypes (systemic JIA, rheumatoid-factor-positive polyarthritis) screened less frequently but still requiring a baseline slit-lamp at diagnosis. [7] [3]
Indigenous, Maori, Pasifika, and refugee or migrant children face the same disease risk with fewer opportunities for regular slit-lamp surveillance. Distance, transport, workforce shortages, interpreter needs and cultural safety are the barriers that determine whether a high-risk child actually receives their three-monthly slit-lamp. The general paediatrician in rural, remote and cross-cultural settings is often the linchpin of adherence, and telehealth-supported screening and regional outreach models are part of the solution. The complication risk is not just biological — it is determined by access. [8] [7]
Immunocompromised children warrant a broader differential that includes opportunistic infectious uveitis — cytomegalovirus retinitis in HIV or post-transplant, fungal endophthalmitis, and other rare causes — alongside the autoimmune forms. Maintain a lower threshold for infectious work-up, aqueous humour PCR, and infectious disease and ophthalmology referral. The immunosuppressive treatment of autoimmune uveitis may need modification in the context of concurrent immunosuppression or transplant. [9] [10]
Adolescents transitioning to adult care need an explicit, structured handover of the uveitis surveillance schedule, the systemic immunosuppression regimen (methotrexate or biologic with its monitoring requirements), the intraocular pressure and complication surveillance, and the reproductive and adherence counselling. The transition is a high-risk period for treatment non-adherence and disease recurrence, and a coordinated paediatric-to-adult handover with a documented care plan reduces this risk. [8] [9]
Evidence, Guidelines & Regional Differences
The evidence base for childhood uveitis rests on four pillars: the SUN classification, the epidemiology and outcome studies, the treatment guidelines, and the SYCAMORE trial. [1] [5]
The SUN working group classification (Jabs et al., 2005) is the standard anatomical framework that makes disease activity and treatment response comparable across centres. It defined anterior, intermediate, posterior and panuveitis by anatomical site, and it introduced the grading of anterior chamber cells and flare that every slit-lamp report now uses. Its adoption unified a previously fragmented literature and enabled the multicentre treatment trials that followed. [1]
The 2019 ACR and Arthritis Foundation guideline (Angeles-Han et al.) is the screening and treatment standard. It replaced the earlier blanket schedules (which varied between the AAP, RCPCH and European recommendations) with a finer-grained, risk-stratified schedule based on JIA subtype, ANA status, age at onset and disease duration. It also set the treatment recommendations: topical corticosteroid for active anterior uveitis, methotrexate for disease uncontrolled on topical therapy, and adalimumab for disease resistant to or dependent on methotrexate. [7] [2]
The SYCAMORE trial (Ramanan et al., 2017, New England Journal of Medicine) is the landmark biologic evidence. In children with JIA-associated uveitis active despite methotrexate, adalimumab plus methotrexate significantly reduced the risk of treatment failure compared with methotrexate plus placebo. The trial was stopped early for efficacy, and it established anti-TNF as the standard second-line systemic therapy. The MERSI experience (Castiblanco et al., 2016) provided supporting real-world data on adalimumab in paediatric uveitis. [5] [6]
In Australia and Aotearoa New Zealand, the approach aligns with the ACR/AF 2019 guideline for screening and the Royal Australian and New Zealand College of Ophthalmologists and Royal Australasian College of Physicians position on joint care. The Therapeutic Guidelines and PBS access to adalimumab for JIA-associated uveitis frame the systemic treatment. The rural and remote challenge — access to slit-lamp surveillance for Indigenous and remote-community children — is addressed through regional outreach, telehealth-supported models and close coordination between the general paediatrician, rheumatology and visiting ophthalmology services. In the UK, the RCPCH and Royal College of Ophthalmologists guidance sets the screening schedule, and NICE and BNFc frame the drug choices. [7] [8]
The controversies are active. The optimal methotrexate route (subcutaneous versus oral) and dose, the timing of biologic escalation, the role of newer biologics (tocilizumab, abatacept, rituximab, golimumab) in anti-TNF-refractory disease, and the continuing debate between the ACR, RCPCH and European (SHARE) recommendations on screening intervals are all live. The universal principle beneath each controversy is the same: any screening schedule and any treatment ladder are useless without adherence, and the general paediatrician who ensures the slit-lamp happens is the person who prevents blindness. [8] [9]
Exam Pearls
- JIA-associated uveitis is the silent blinder: chronic, anterior, bilateral, asymptomatic, detected only by slit-lamp screening — the commonest childhood uveitis in developed settings. [3]
- The high-risk profile is ANA positive, oligoarticular subtype, onset under seven years, disease duration under four years — screen every three months. [7]
- The SUN anatomical classification: anterior (iritis or iridocyclitis), intermediate (pars planitis), posterior (retinitis or choroiditis), panuveitis — and the SUN grading of anterior chamber cells from 0 to 4+. [1]
- The treatment ladder: topical prednisolone acetate 1% and cycloplegia, then methotrexate 10 to 15 mg per square metre per week, then adalimumab 24 mg per square metre every two weeks — anchored by the SYCAMORE trial. [5] [2]
- Never give topical steroid to a red eye until herpes simplex keratitis is excluded by slit-lamp and fluorescein — steroid causes corneal melting and perforation in herpetic disease. [9]
- The five complications to name at viva: band keratopathy, cataract, secondary glaucoma, posterior synechiae and amblyopia — the structural damage that screening prevents. [4]
- Acute anterior uveitis in an adolescent boy with photophobia points to HLA-B27 spondyloarthritis — examine the entheses and ask about inflammatory back pain and bowel symptoms. [8]
- Posterior uveitis in a child is dominated by infection: ocular toxoplasmosis (focal retinochoroiditis, the commonest) and ocular toxocariasis (granulomatous mass, puppy or soil exposure). [10]
- TINU syndrome is uveitis with interstitial nephritis — check creatinine and urine for sterile pyuria, often after beta-lactam exposure, needing nephrology co-management. [9]
- Kawasaki disease causes a transient self-limiting mild anterior uveitis during the acute illness — it does not need the chronic uveitis treatment ladder but must be distinguished from JIA uveitis. [3]
References
- [1]Jabs DA; Nussenblatt RB; Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol, 2005.PMID 16196117
- [2]Heiligenhaus A; Minden K; Föll D; et al Evidence-based, interdisciplinary guidelines for anti-inflammatory treatment of uveitis associated with juvenile idiopathic arthritis. Rheumatol Int, 2012.PMID 22083610
- [3]Heiligenhaus A; Niewerth M; Ganser G; et al Review for disease of the year: epidemiology of juvenile idiopathic arthritis and its associated uveitis. Ocul Immunol Inflamm, 2013.PMID 23713827
- [4]Carvounis PE; Herman DC; Cha S; Burrus J; Moore J; Rosenbaum JT Incidence and outcomes of uveitis in juvenile rheumatoid arthritis, a synthesis of the literature. Graefes Arch Clin Exp Ophthalmol, 2006.PMID 16228217
- [5]Ramanan AV; Dick AD; Jones AP; McKay A; Williamson PR; Compeyrot-Lacassagne S; et al Adalimumab plus Methotrexate for Uveitis in Juvenile Idiopathic Arthritis. N Engl J Med, 2017.PMID 28445659
- [6]Castiblanco C; Foster CS; Di Chrstian M; et al Treatment of pediatric uveitis with adalimumab: the MERSI experience. J AAPOS, 2016.PMID 27079596
- [7]Angeles-Han ST; Yeh S; Vogel LB; Burnham J; Cooper AM; Magliya M; et al 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of Juvenile Idiopathic Arthritis-Associated Uveitis. Arthritis Care Res (Hoboken), 2019.PMID 31021540
- [8]Modrzejewska M; Grzybowski A; Misiuk-Hojło M; et al Uveitis in the Pediatric Population and Therapeutic Management: A Current Literature Review. Children (Basel), 2024.PMID 39062219
- [9]Modrzejewska M; Grzybowski A; Misiuk-Hojło M; et al Diagnosis and Treatment of Uveitis in Children: A Summary of the Latest Data from a 5-Year Literature Review. J Clin Med, 2024.PMID 38892808
- [10]Woodhall D; Starr MC; Montgomery SP; Jones JL; Lum F; Read RW; Moorthy RS Toxocariasis: A Review for Pediatricians. J Pediatric Infect Dis Soc, 2014.PMID 26625368
- [11]Lei B; Weng R; Wang Q; Liu Z; et al Pediatric Uveitis in a Tertiary Referral Center in East China: Clinical Patterns and Visual Outcomes. J Ophthalmol, 2024.PMID 39619646