Paeds · ophthalmology
Visual development, amblyopia and vision screening in childhood
Also known as Amblyopia · Lazy eye · Childhood vision screening · Patching for amblyopia · Strabismic and anisometropic amblyopia
Fellowship guide to visual development, amblyopia and vision screening in childhood: the maturation of acuity from newborn 6/60 toward adult 6/6 across a sensitive period to about 7 to 9 years; amblyopia as a unilateral, rarely bilateral, cortical reduction in best-corrected acuity from abnormal visual experience in that window, classified as strabismic, anisometropic, stimulus-deprivation or bilateral ametropic; the cortical mechanism of suppression and reorganisation of ocular dominance columns that lets amblyopia both develop and be treated; the age-based screening programme from the newborn red reflex, through instrument photoscreening at 1 to 3 years, to monocular acuity at 4 to 5 years with the refer threshold of 0.2 logMAR or worse or a two-line interocular difference; and the management ladder of refractive correction first, then occlusion of the better eye two to six hours a day or atropine one per cent penalisation, supported by the PEDIG trials showing equivalence of two and six hours of patching and of atropine and patching for moderate amblyopia, with urgent referral of the red flags of leukocoria and absent red reflex.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old who sailed through her newborn and infant checks and sees perfectly with both eyes open, but who, at her school-entry vision test, can read only the top line with her left eye when the right is covered. The eye looks completely normal, there is no turn and no white pupil, yet acuity in that eye is poor and does not improve with a pinhole. This is amblyopia, and the key idea is that the problem is in the brain, not the eye: during the sensitive period of visual development the cortex received a blurred or competing image from that eye and learned to suppress it, so the neural machinery for sharp vision never developed. [2]
Normal visual development is a race against a closing window. A newborn sees at roughly 6/60 and refines acuity steadily through infancy and early childhood toward the adult 6/6, building the cortical circuits and binocular connections that depend on two clear, well-aligned images. That construction is most plastic in the first two to three years and tapers over the sensitive period to about seven to nine years of age, after which the cortex is much harder to remodel. The same plasticity is the reason amblyopia can be treated at all — forcing the weaker eye to work during the window lets the cortex recover — and the reason that, once the window closes, untreated amblyopia is largely permanent. [1] [11]
Amblyopia is defined as a unilateral, or occasionally bilateral, reduction in best-corrected visual acuity caused by abnormal visual experience during the sensitive period, in the absence of an organic lesion of the eye or visual pathway that would fully explain the deficit. It is common, affecting about one to three per cent of children, which makes it the leading cause of unilateral vision loss in this age group. Crucially, it is invisible to a both-eyes-open check, because the better eye hides the poorer one, so detection depends on testing each eye separately. [2]
Classification
The most useful way to classify amblyopia is by what the cortex received during the sensitive period, because the cause predicts how dense the deficit is, how urgent it is, and how well it responds to treatment. [2]
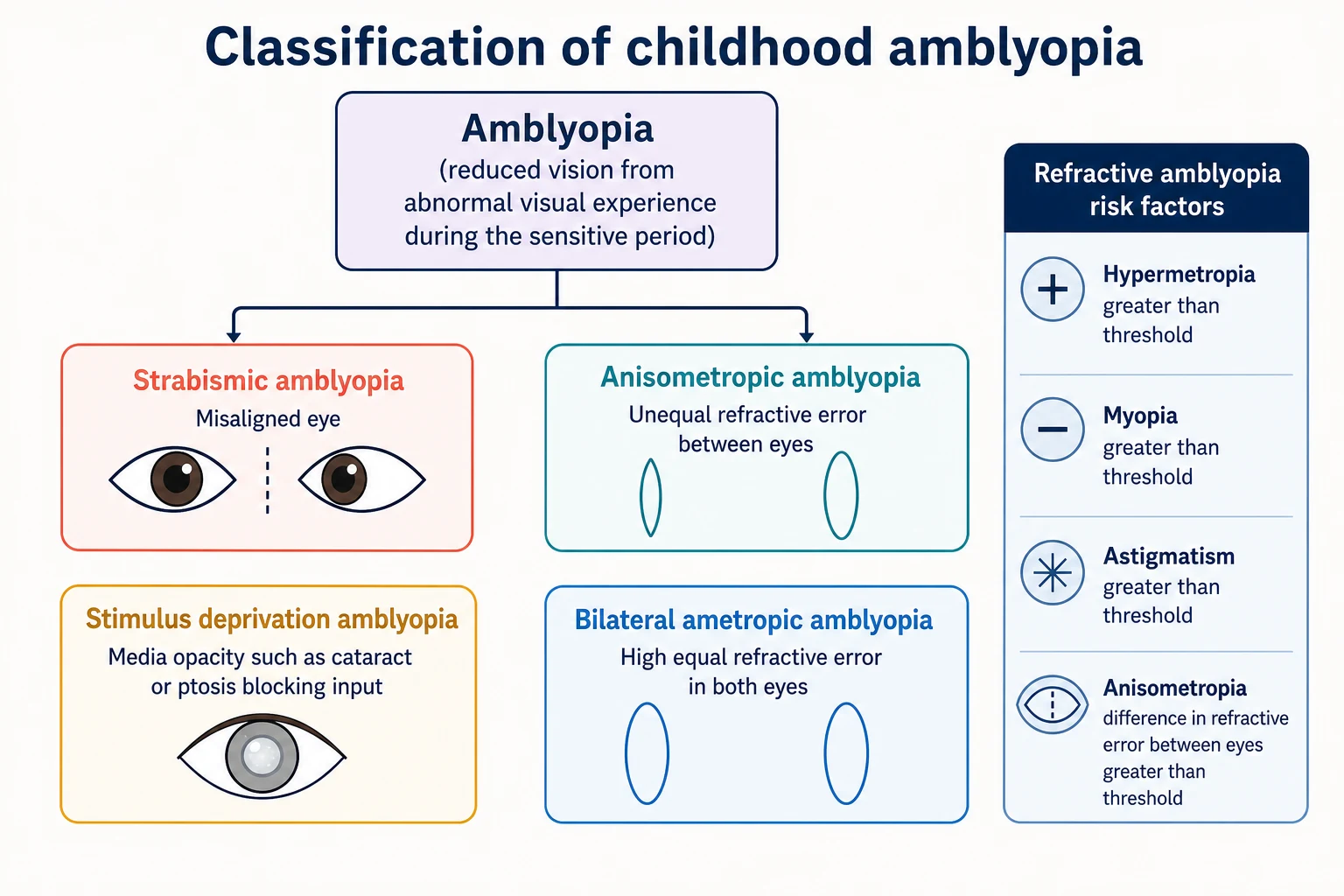
Four types cover the field. Strabismic amblyopia arises when a manifest turn of one eye forces the cortex to suppress that eye's image to avoid double vision. Anisometropic amblyopia arises when one eye has a substantially different refractive error, so its image is defocused relative to the other and the cortex suppresses it. Stimulus- or form-deprivation amblyopia is the least common but the densest, caused by anything that blocks the image entirely — a congenital cataract, a drooping lid, a corneal opacity — because removing input during the most plastic phase of the cortex causes the deepest deficit. Bilateral ametropic amblyopia arises when both eyes share a high but equal refractive error, so both images are defocused and acuity is reduced in both eyes. [2] [11]
The two commonest forms are strabismic and anisometropic, and they often coexist. The teaching point is that deprivation amblyopia, although rare, is the emergency of the group: because it removes input entirely during the peak of cortical plasticity, it causes the most treatment-resistant deficit and demands the most urgent correction of the cause. [2]
Strabismic
competing image suppressed
- Manifest turn of one eye
- Cortex suppresses to avoid diplopia
- Commonest combined with anisometropia
- Fix once acuity equalised
Anisometropic
unequal refractive error
- One eye defocused relative to the other
- Often asymptomatic until screening
- Spectacles first, then occlusion
- Good prognosis if caught early
Stimulus-deprivation
image blocked
- Cataract, ptosis or corneal opacity
- Densest and most urgent deficit
- Correct the cause within weeks
- Red-flag leukocoria pathway
Bilateral ametropic
high equal refractive error
- Both eyes defocused
- Reduced acuity in both eyes
- Bilateral spectacles, no patching
- Less common, often high hypermetropia
Epidemiology & Risk Factors
Amblyopia affects about one to three per cent of children, which is high enough that every general paediatrician will see it and low enough that no child should reach school age undetected. The leading antecedents are strabismus, most often esotropia, and significant refractive error, especially unilateral or asymmetric hypermetropia, astigmatism or anisometropia. [2]
The risk factors worth asking about cluster around the same themes: prematurity and low birth weight, a family history of amblyopia or strabismus (the heritability of refractive error and strabismus is real), significant refractive error, developmental delay, and any media opacity or ptosis that causes form deprivation. These are the children for whom an extra screening pass, or a lower threshold to refer, pays off. [1]
The population-level reason for screening is not the acuity deficit alone but its downstream risk. A child with untreated unilateral amblyopia relies on a single eye for life, and if that eye is later injured or diseased, the consequence is serious bilateral visual impairment. This elevated lifetime risk of vision loss is the economic and clinical argument that has underpinned universal preschool screening programmes. [7] [8]
Pathophysiology
To understand amblyopia, hold two facts together: the cortex builds sharp vision only from clear input, and it does this building only during a limited window. The visual cortex organises its ocular dominance columns — the sets of neurons that respond preferentially to one eye or the other — by competing the two retinal images against each other. When both images are clear and aligned, the columns develop in balanced balance and binocular connections form. When one image is blurred, turned or absent, the cortex suppresses it and reallocates cortical territory to the stronger eye. [11]
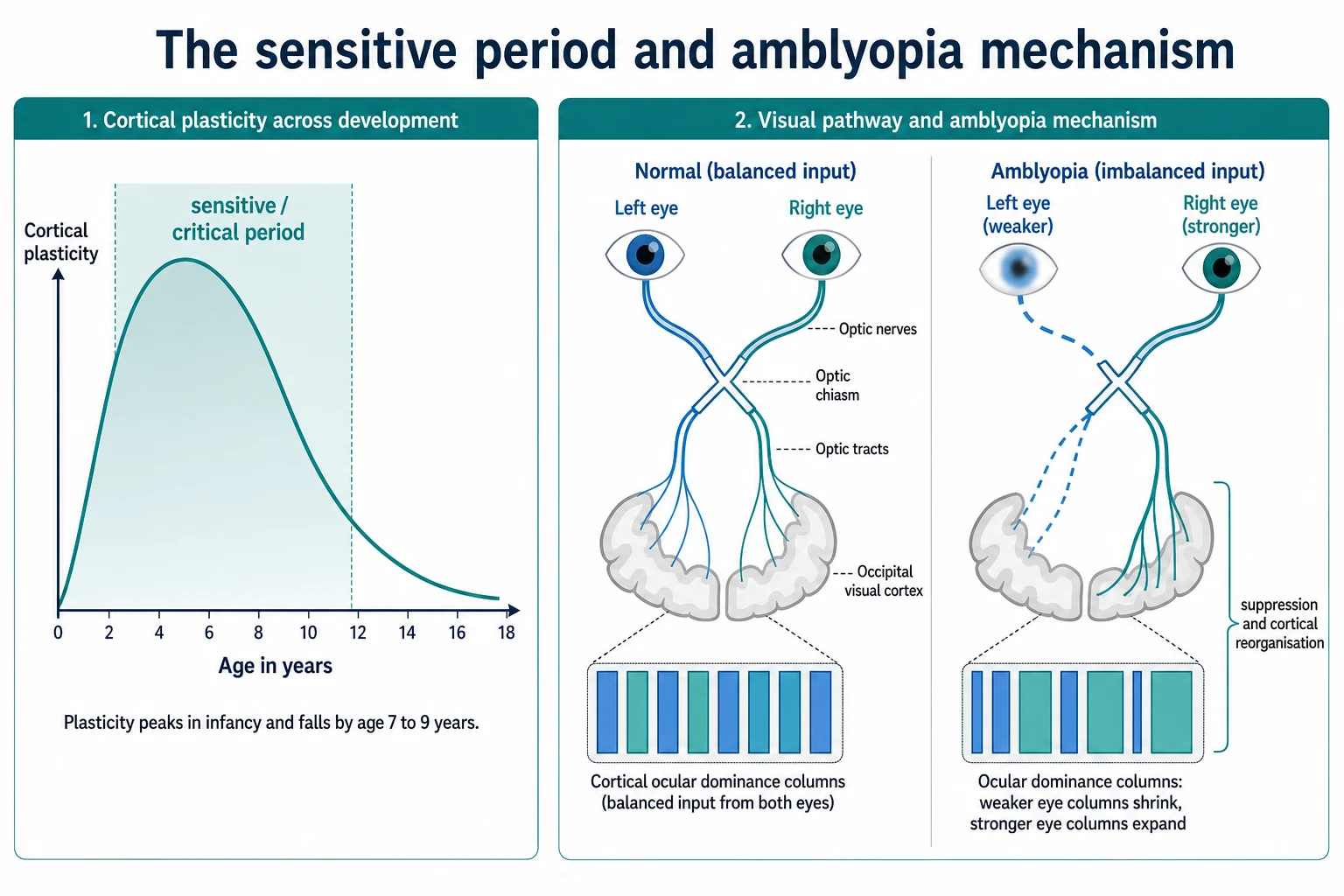
This competition is gated by age. Cortical plasticity is highest in infancy and early childhood and tapers across the sensitive period to about seven to nine years, mirroring the curve along which amblyopia can be both produced and treated. A congenital cataract blocks input at the very peak of plasticity, which is why deprivation amblyopia is so dense and so hard to reverse if the cause is not removed within weeks. A mild anisometropia acting later in the sensitive period produces a shallower deficit that responds well to refractive correction and occlusion. [2] [11]
The same plasticity is what makes treatment work. Occluding or penalising the better eye forces the cortex to use the suppressed image, and within the sensitive period the ocular dominance columns can recover some of the territory they lost. Once the window closes, that recovery becomes much harder, which is why treatment is front-loaded into the preschool years and why late diagnosis is the single biggest predictor of a poor outcome. [11]
Clinical Presentation
The archetypal presentation is the asymptomatic child. Amblyopia is silent because the better eye does all the work, so the child neither complains nor struggles, and the deficit appears only when each eye is tested on its own. A fellowship candidate should expect to find it at screening rather than in the history, which is exactly why monocular acuity testing is non-negotiable from age four. [2]
The features that point to a cause are more visible. A manifest turn of one eye, reported by a parent or found on cover test, points to strabismic amblyopia. A parental report of a squint that comes and goes, a head tilt, or a child who closes or favours one eye, raises the same suspicion. Leukocoria, a white pupil seen in a photograph or in dim light, is the red flag for a media opacity and demands same-day referral. A drooping lid points to ptosis and possible deprivation. [10]
Atypical presentations matter because they are the missed cases. The premature or developmentally delayed infant cannot report, so detection rests on the red reflex, fixation behaviour and instrument-based screening. The child with unilateral high refractive error may have no turn and no complaint, found only on photoscreening. And the older child whose amblyopia is detected late, at school-entry acuity testing, is the child for whom the window is already narrowing. [1]
Differential Diagnosis
When a child has reduced acuity in one eye, the first question is whether the deficit is amblyopia or an organic cause, because amblyopia is a diagnosis made only after the eye and pathway are shown to be structurally sound. Pure refractive error corrects fully with spectacles and is not amblyopia; retinal or optic nerve disease, cortical visual impairment, and structural lesions such as congenital cataract or retinoblastoma each have findings that amblyopia lacks. [2]
Amblyopia
functional, cortical
- Normal ocular structures
- Acuity improves with refractive correction
- No afferent pupillary defect
- Detected at screening
Refractive error (no amblyopia)
optical
- Fully corrects with spectacles
- No interocular suppression
- No turn on cover test
- Normal red reflex
Organic retinal or optic nerve disease
structural
- Acuity not explained by refractive error
- May have afferent pupillary defect
- Fundus findings on examination
- Refer urgently to ophthalmology
Cortical visual impairment
neurological
- Often bilateral, variable
- History of brain injury or prematurity
- Normal eye examination
- Multidisciplinary management
The can't-miss mimic of a white or poor red reflex is the group that every candidate must name on demand: congenital cataract, retinoblastoma, retinal detachment, Coats disease and persistent fetal vasculature. Each can present as leukocoria, each is sight- or life-threatening, and each requires urgent ophthalmology referral rather than waiting for screening. [10]
A common and reassuring distinction is pseudostrabismus. A wide, flat nasal bridge and prominent epicanthal folds can make a perfectly aligned eye appear turned, especially when the child looks to the side. The cover test is normal, the red reflex is symmetric, and the apparent turn disappears as the face grows. The trap is the reverse — accepting pseudostrabismus as the explanation for an apparent turn without performing a cover test and a red reflex, thereby missing a real strabismus and its amblyopia. [2]
Clinical & Bedside Assessment
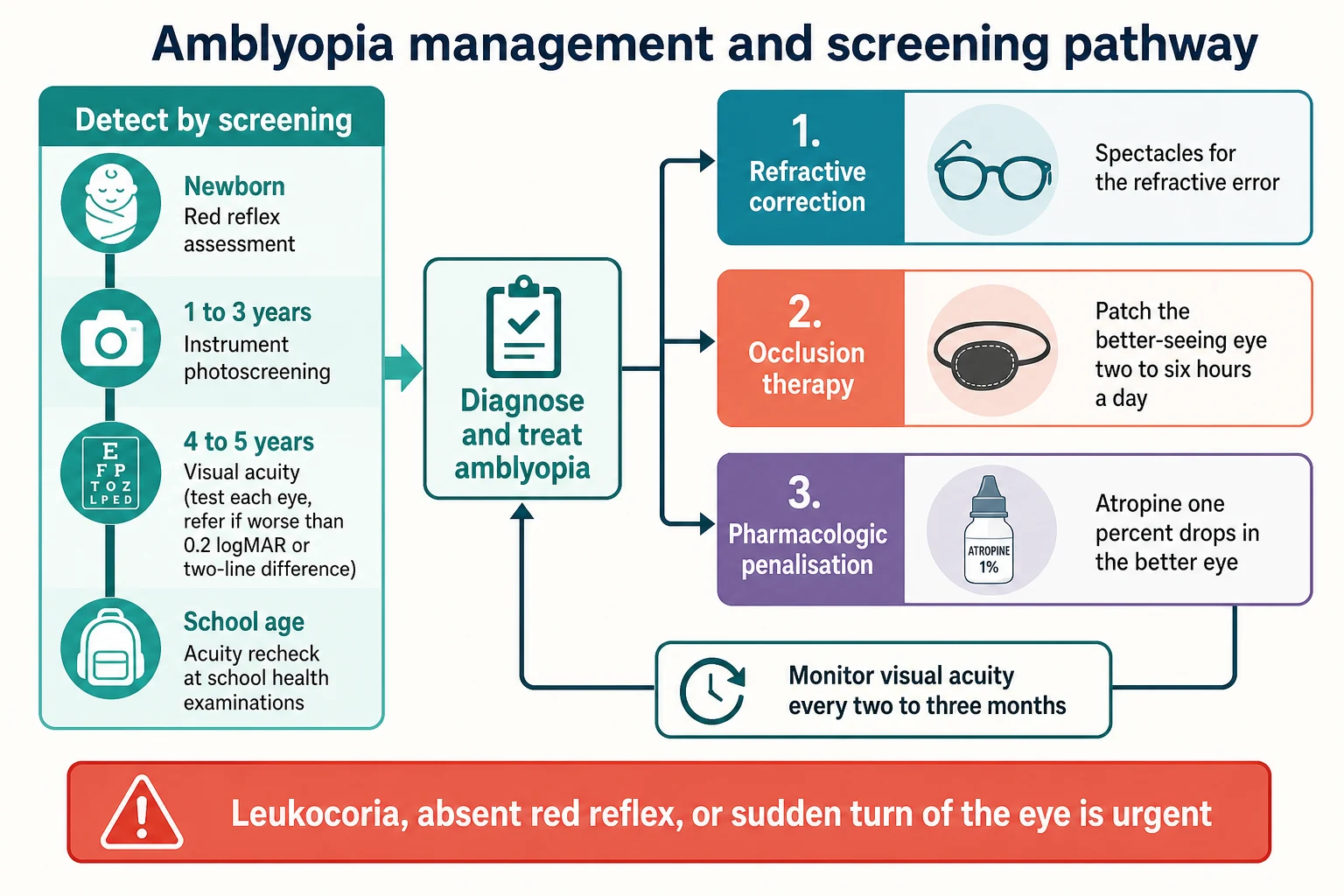
The paediatric eye examination is built around the child's age and ability, and the same child moves through different tests as they grow. At the newborn and six to eight week check, the examination is the red reflex and inspection for eye structure and lid position. From around six months, add the cover-uncover and alternate cover test for strabismus and an assessment of fixation. From age four to five, formal monocular acuity testing becomes possible and becomes the cornerstone of screening. [1]
The red reflex test is the single most useful bedside manoeuvre in infancy, and it is performed in a dim room with a direct ophthalmoscope held about 45 cm away, focused on the pupil, comparing the two eyes for a symmetric orange-red glow. A white, absent, dark or markedly asymmetric reflex is abnormal and urgent. This is the Bruckner technique, and it doubles as a sensitive screen for strabismus, because a deviating eye often reflects the light differently. [10]
Monocular acuity testing must be done with each eye separately and the other properly occluded, because anything less hides amblyopia. From age four, a logMAR or Snellen chart is used, and the screening refer thresholds are an acuity worse than 0.2 logMAR in either eye or a two-line (0.2 logMAR) difference between the eyes. A child who cannot yet name letters uses a matching or picture chart, and the preverbal child is screened with an instrument rather than a chart. [1]
Investigations
Most vision screening is done without laboratory tests, and the diagnostic pathway is by age-appropriate test rather than by blood panel. For the preverbal child, the investigations are the red reflex and instrument-based screening. Photoscreeners such as Spot and Plusoptix, and handheld autorefractors, detect the amblyopia risk factors — significant refractive error, anisometropia and strabismus — rather than amblyopia itself, and a systematic review and meta-analysis reports useful sensitivity and specificity that support their use from one to three years. [12]
The definitive assessment of refractive status is cycloplegic refraction, performed by ophthalmology after instilling a cycloplegic drop such as cyclopentolate to relax accommodation. It defines the hypermetropic, myopic, astigmatic or anisometropic contribution and tells the clinician whether spectacles alone, or spectacles plus occlusion, are needed. Validation of instruments against this gold standard underpins their use in screening. [9]
Imaging is reserved for the abnormal. A media opacity, leukocoria or suspected retinoblastoma is assessed with B-scan ultrasound and often an examination under anaesthesia, and the diagnosis of amblyopia itself remains clinical — made only after organic disease has been excluded and a persistent acuity deficit remains despite refractive correction. [10]
Management — Resuscitation
Childhood vision problems are rarely haemodynamic emergencies, but three situations are genuinely time-critical and must be acted on the same day. A white pupil, leukocoria or an absent or asymmetric red reflex in an infant is congenital cataract or retinoblastoma until proven otherwise and needs urgent ophthalmology referral, because a missed retinoblastoma is life-threatening and a missed cataract causes dense deprivation amblyopia within weeks. A new manifest strabismus persisting beyond four months is not a normal variant and needs assessment, because suppression sets up amblyopia within the sensitive period. And sudden visual loss in a child is an emergency until examined. [10]
Deprivation amblyopia from a congenital cataract is the clearest example of why urgency matters. Because the cortex is most plastic in the first months, removing the opacity early is the treatment, and the same cataract operated on at one year instead of one month leaves a far worse acuity. The take-home is that a red-flag red reflex is not a screening finding to watch — it is a referral. [2]
Management — Definitive & Stepwise
Once a red-flag cause is excluded, amblyopia is managed on a stepwise ladder, and the first step is almost always refractive correction. Prescribe the spectacles that fully correct the refractive error, then re-measure acuity after a period of refractive adaptation, because spectacle wear alone improves acuity in many children with anisometropic or bilateral ametropic amblyopia before any patching is begun. Occlusion is added only if a deficit persists. [2]
The second step is occlusion therapy, patching the better-seeing eye to force the cortex to use the amblyopic eye. The Pediatric Eye Disease Investigator Group randomised trial of two versus six hours of daily patching for moderate amblyopia showed broadly equivalent outcomes, which de-escalated practice from maximal occlusion toward two hours a day for moderate and up to six hours a day for severe amblyopia, sustained until acuity stops improving. [4] [3]
The alternative is pharmacologic penalisation, instilling atropine one per cent drops in the better-seeing eye to blur its near vision and force use of the amblyopic eye. The Pediatric Eye Disease Investigator Group trials showed that atropine gives equivalent outcomes to patching for moderate amblyopia, with the long-term follow-up confirming the effect persists to fifteen years of age. Penalisation suits families in whom patch compliance is poor and is a genuine alternative rather than a fallback. [5] [6]
Exclude red flags and organic disease, and confirm a persistent acuity deficit despite best refractive correction
Prescribe spectacles to fully correct the refractive error and re-measure acuity after refractive adaptation
Add occlusion of the better eye two hours a day for moderate and up to six hours a day for severe amblyopia, or atropine one per cent penalisation of the better eye
Review visual acuity every two to three months and continue treatment until acuity stops improving
Monitor the sound eye for reverse amblyopia and arrange shared-care follow-up with ophthalmology
The principles that govern the whole ladder are worth stating. Treatment works only within the sensitive period, so it is front-loaded into the preschool years. Compliance is the commonest determinant of success, so the choice between patching and atropine is partly a choice the family makes about what they can sustain. And the sound eye must be monitored, because over-occlusion can induce reverse amblyopia in the better eye. [2] [11]
Specific Subtypes & Scenarios
Each subtype of amblyopia is managed to its own logic. Strabismic amblyopia is treated with occlusion or atropine to equalise acuity, after which the residual deviation is addressed, often with strabismus surgery, so that the eyes are aligned and binocular vision has the best chance of developing. Anisometropic amblyopia is treated with spectacles first and occlusion or atropine second, and tends to respond well when caught early because the deficit is usually shallower than deprivation. [2]
Stimulus-deprivation amblyopia is the emergency of the group. A congenital cataract, a dense ptosis or a corneal opacity removes the image at the peak of cortical plasticity, so the cause is corrected within the first weeks to months of life and is followed by aggressive occlusion and optical correction, including aphakic correction after cataract surgery. This is the subtype for which delay is most damaging and for which the red-flag pathway exists. [10]
Bilateral ametropic amblyopia, from high but equal refractive error in both eyes, is managed with bilateral spectacles rather than occlusion, because there is no better eye to patch against. And the special case of the developmentally delayed or non-verbal child, in whom acuity cannot be charted, is managed with instrument-based screening and a low threshold for cycloplegic refraction and ophthalmology referral, because these children both depend on screening and are most likely to miss it. [1] [12]
Complications & Pitfalls
The chief complication of amblyopia is the permanent unilateral vision loss that follows if the sensitive period closes untreated, leaving the child dependent on a single seeing eye for life. The other is iatrogenic: over-occlusion of the better (sound) eye can induce reverse amblyopia, which is why the sound eye is monitored during treatment and why occlusion hours are calibrated to severity rather than maximal. [2]
The diagnostic pitfalls are the ones a fellowship candidate should rehearse. Missing amblyopia because the child sees well with both eyes open is the commonest — only monocular testing reveals it. Accepting pseudostrabismus as the explanation for an apparent turn, without a cover test and a red reflex, misses a real strabismus. And attributing a white pupil to a flash photograph or a benign cause misses a congenital cataract or a retinoblastoma. [10]
The management pitfalls matter as much. Prescribing occlusion without first giving spectacles misses the children whose acuity improves on refractive adaptation alone. Prescribing patching without compliance support wastes the window, because a patch that is not worn cannot work. And delaying referral of a deprivation cause so that treatment begins after the sensitive period closes converts a treatable problem into a permanent one. [11]
Prognosis & Disposition
Amblyopia treated within the sensitive period has a good prognosis, and most children gain useful acuity with refractive correction and occlusion or atropine. The prognosis worsens with a deeper deficit at presentation, older age at the start of treatment, a deprivation cause, and poor compliance. The yield of treatment falls steeply after about seven to nine years, although some improvement is still possible in selected older children, which is why screening is front-loaded into the preschool years. [2]
Disposition follows the severity and the subtype. Instrument screening, refractive correction and first-line occlusion or atropine can be shared between primary care, general paediatrics and ophthalmology, with acuity reviewed every two to three months. Same-day referral is reserved for the red flags of leukocoria, an absent or white red reflex, a new persistent strabismus, or sudden visual loss. [1] [10]
The wider case for screening is the lifetime risk it prevents. The economic evaluation that underpinned the UK screening programme weighed the cost of universal acuity screening at school entry against the lifetime burden of unilateral vision loss and the risk of losing the sole seeing eye, and concluded that a single well-targeted screen at four to five years was the efficient design. [7] [8]
Special Populations
The preverbal child, from infancy to about three years, cannot do acuity testing and so depends entirely on the red reflex, fixation behaviour and instrument-based screening for detection. For this group, the red reflex at the newborn and six to eight week check and photoscreening in the toddler years are not optional extras but the whole of detection, and missing them is how deprivation amblyopia is missed. [1]
The developmentally delayed or non-verbal child is a parallel case. Acuity cannot be charted reliably, so instrument-based screening and a low threshold for cycloplegic refraction and ophthalmology referral carry the diagnostic load. These children are also more likely to have significant refractive error and strabismus as part of their neurodevelopmental condition, which raises both the pre-test probability and the stakes of missing the deficit. [12]
The equity dimension is real and worth naming. Children in remote and low-access settings, and Aboriginal, Torres Strait Islander, Maori, migrant and refugee families, may miss screening and present late, often with a deprivation cause that has already closed the window. Outreach and telehealth-supported screening, and culturally safe follow-up that clears transport, cost and language barriers, are how the gap is narrowed and a curable condition is caught in time. [7]
Evidence, Guidelines & Regional Differences
The evidence base for amblyopia treatment is dominated by the Pediatric Eye Disease Investigator Group. The randomised trial of two versus six hours of daily patching for strabismic and anisometropic amblyopia showed broadly equivalent outcomes for moderate amblyopia, and the trials of atropine versus patching showed that pharmacologic penalisation matched occlusion. The fifteen-year follow-up confirmed that the benefit of treatment persisted into late adolescence. Together these trials de-escalated treatment from maximal occlusion toward a calibrated, compliance-friendly ladder. [4] [5] [6]
The screening evidence runs in parallel. The whole-population vision screening analysis and the systematic review and economic evaluation of screening programmes for amblyopia and strabismus up to four to five years together established that a single well-targeted acuity screen at school entry is effective and cost-effective, which is the foundation of the UK programme. The diagnostic accuracy of instrument-based photoscreeners was confirmed by a systematic review and meta-analysis, supporting their role in the preverbal years. [7] [8] [12]
PEDIG patching and atropine trials for moderate amblyopia
Randomised controlled trials and long-term follow-up by the Pediatric Eye Disease Investigator Group
Practice change
Treat moderate amblyopia with refractive correction plus two hours of patching a day or atropine one per cent penalisation, choosing by what the family can sustain
The active controversies are the upper age at which treatment remains worthwhile — with growing evidence that some older children and even teenagers respond, though the yield falls after the sensitive period — and the role of newer binocular and dichoptic therapies that aim to retrain binocular cooperation. These remain adjuncts to, rather than replacements for, established refractive correction, occlusion and penalisation. [11]
Exam Pearls
Amblyopia is the commonest cause of unilateral vision loss in children, it is cortical rather than ocular, and it can both develop and be treated only within the sensitive period to about seven to nine years — three facts that anchor every question on this topic. [2]
The screening acuity refer threshold is an acuity worse than 0.2 logMAR in either eye or a two-line interocular difference, and the four types are strabismic, anisometropic, stimulus-deprivation and bilateral ametropic. Leukocoria or an absent red reflex is a red flag requiring urgent referral, and pseudostrabismus is distinguished from a real turn by a normal cover test and a symmetric red reflex. [1] [10]
SCREEN
Refractive correction is always the first step before patching or atropine, the Pediatric Eye Disease Investigator Group trials showed equivalence of two and six hours of patching and of atropine and patching for moderate amblyopia, and the sound eye is monitored for reverse amblyopia during occlusion. [4] [5] [6]
References
- [1]Section on Ophthalmology, American Academy of Pediatrics Visual System Assessment in Infants, Children, and Young Adults by Pediatricians. Pediatrics, 2016.PMID 29756730
- [2]Holmes JM, Clarke MP Amblyopia. Lancet, 2006.PMID 16631913
- [3]Pediatric Eye Disease Investigator Group A randomized trial of increasing patching for amblyopia. Ophthalmology, 2013.PMID 23755872
- [4]Wallace DK, Pediatric Eye Disease Investigator Group A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology, 2006.PMID 16751033
- [5]Pediatric Eye Disease Investigator Group Atropine vs patching for treatment of moderate amblyopia: follow-up at 15 years of age of a randomized clinical trial. JAMA Ophthalmol, 2014.PMID 24789375
- [6]Pediatric Eye Disease Investigator Group Two-year follow-up of a 6-month randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Arch Ophthalmol, 2005.PMID 15710809
- [7]Solebo AL, Cumberland PM, Rahi JS Whole-population vision screening in children aged 4-5 years to detect amblyopia. Lancet, 2015.PMID 25499167
- [8]Carlton J, Karnon J, Czoski-Murray C, et al. The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4-5 years: a systematic review and economic evaluation. Health Technol Assess, 2008.PMID 18513466
- [9]Garry GA, Donahue SP Validation of Spot screening device for amblyopia risk factors. J AAPOS, 2014.PMID 25266832
- [10]Anderson J Don't Miss This! Red Flags in the Pediatric Eye Examination: Abnormal Red Reflex. J Binocul Vis Ocul Motil, 2019.PMID 31329054
- [11]Gopal SKS, Kelkar J, Kelkar A Simplified updates on the pathophysiology and recent developments in the treatment of amblyopia: A review. Indian J Ophthalmol, 2019.PMID 31436180
- [12]Zhang X, Wang J, Li Y, et al. Diagnostic test accuracy of Spot and Plusoptix photoscreeners in detecting amblyogenic risk factors in children: a systemic review and meta-analysis. Ophthalmic Physiol Opt, 2019.PMID 31236980