Paeds · paediatric-dermatology
Acne vulgaris in adolescents
Also known as adolescent acne · common acne · comedonal acne · inflammatory acne · nodulocystic acne · acne vulgaris · adapalene · tretinoin · benzoyl peroxide · doxycycline · isotretinoin · acne fulminans
A fellowship approach to acne vulgaris in the adolescent: the comedones and the papules and the pustules over the sebum-rich skin of the face and the upper back and the chest that mark the androgen-driven pilosebaceous unit, the four drivers of the sebum and the Cutibacterium acnes and the follicular plugging and the inflammation that the treatment targets, the split between the comedonal and the inflammatory disease that frames the topical retinoid and the benzoyl peroxide and the oral doxycycline, the oral isotretinoin for the nodulocystic and the refractory disease with the pregnancy prevention and the lipid and the liver monitoring, the antibiotic stewardship that never prescribes the monotherapy and always pairs the antibiotic with the benzoyl peroxide, and the psychosocial and the scarring burden that the early and the effective treatment prevents.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fifteen-year-old boy is brought to the general practice by his mother, who has watched his forehead and his cheeks break out over the past year into the blackheads and the red papules and the occasional pustule, with a few deeper lumps now appearing on his jawline. He has become quieter, he has stopped swimming, and he admits the acne bothers him a great deal. On examination the face and the upper back carry the open and the closed comedones, the inflammatory papules, and a few tender nodules, with early atrophic marks over the cheeks. The picture is the moderate inflammatory acne vulgaris of the adolescent, and the plan is the topical retinoid and the benzoyl peroxide at night, the oral doxycycline for three months, the photoprotection, and the clear pathway to the isotretinoin if the nodulocystic disease or the scarring progresses. [2] [12]
The four drivers of acne — Sebum, Bugs, Block, Burn
Overview & Definition
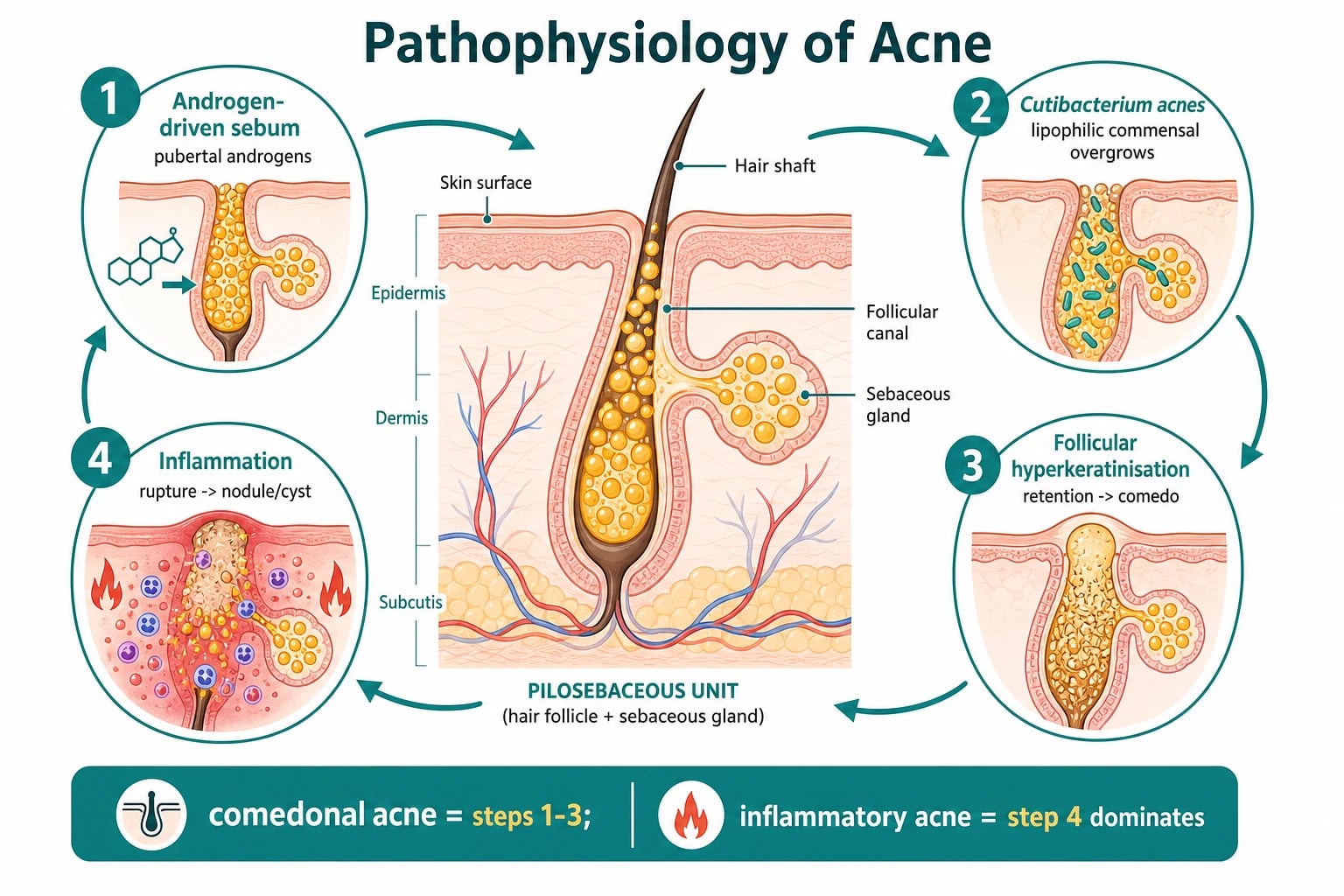
Picture the adolescent skin at the moment the sebaceous glands wake. Under the pubertal androgen surge, the glands enlarge and pour out the sebum, the hair follicles clog with the retained keratin and the lipid, and the resident Cutibacterium acnes thrives on the feast. The blocked follicle swells into the comedone, and when its wall gives way the immune system meets the follicular contents and the redness and the pus follow. That cascade, playing out over the face, the upper back, the chest, and the shoulders of the teenager, is acne vulgaris. [3] [8]
Acne vulgaris is the commonest skin disorder of adolescence, and the generalist meets it at every clinic. The definition the fellowship wants is operational rather than abstract: it is the chronic inflammatory disease of the pilosebaceous unit that produces the open and the closed comedones and the inflammatory lesions, on the sebum-rich skin, driven by the four factors of the sebum, the organism, the plugging, and the inflammation. The severity runs from the few comedones to the confluent nodulocystic disease, and the severity, not the name, governs the treatment. [1] [4]
Why the adolescent focus matters is that the disease, the distress, and the scarring all peak here. The onset tracks the adrenarche and the gonadarche between eleven and thirteen years, and the prevalence climbs to roughly four in five teenagers by the mid-teens. The generalist who recognises the severity, treats early, and escalates in time prevents the permanent scarring and the mood harm that no later treatment fully reverses. [2] [9]
Classification
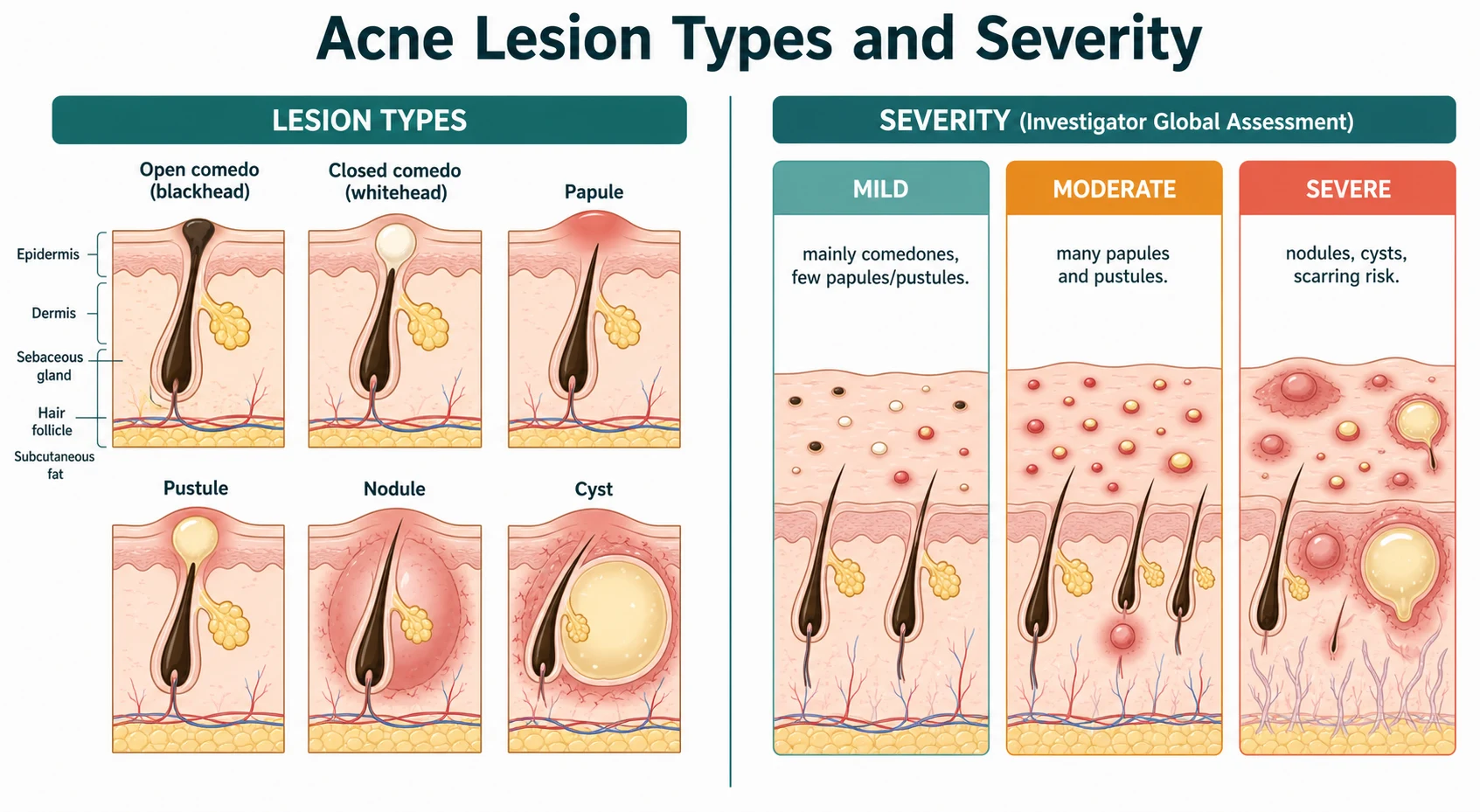
The classification that drives the treatment is the comedonal versus the inflammatory split, because the two answer to different drugs. The comedonal acne is the non-inflammatory disease of the open and the closed comedones — the blackhead, whose wide opening oxidises the keratin to the dark colour, and the whitehead, whose narrow closed neck keeps the contents pale. It is the disease of the plugged follicle, and the topical retinoid is its mainstay because the retinoid normalises the keratinocyte shedding and unblocks the follicle. [1] [2]
The inflammatory acne is the disease of the red papule, the pustule, the nodule, and the cyst. Here the follicle wall has ruptured and the immune reaction to the keratin, the sebum, and the bacterial antigens has set the cascade alight. The inflammatory disease adds the benzoyl peroxide, which kills the organism and reduces the inflammation, and when it is moderate it adds the oral antibiotic; when it is severe and nodulocystic it moves to the isotretinoin. The scar risk sits in the inflammatory end, which is why the severity, more than the label, sets the urgency. [3] [10]
The comedonal versus the inflammatory acne
Comedonal (non-inflammatory)
Mild inflammatory
Moderate inflammatory
Severe nodulocystic or refractory
Epidemiology & Risk Factors
Acne vulgaris is so common in adolescence that the absence, not the presence, is the surprise. The prevalence climbs through the early teens, and roughly four in five individuals between the ages of twelve and twenty-four experience some degree of the disease, with the peak severity in the mid-to-late teens. The onset mirrors the hormonal transition: the adrenarche raises the adrenal androgens first, the gonadarche adds the gonadal androgens, and the sebum output follows. The male adolescent tends to the more severe and the more sebum-heavy disease, and the trunk involvement is more common in him. [2] [12]
The risk factors cluster around the sebum and the follicle. The strong family history predicts the earlier and the more severe disease, and the genetic loading is one of the best predictors of the scarring. The occlusive cosmetics and the oily hair products worsen the plugging, and the friction from the helmets, the headbands, and the backpacks localises the lesions. The high-glycaemic diet and the skim-milk intake carry a modest and debated association, and the evidence is enough to counsel but not to prescribe a diet. The picking and the squeezing deepen the inflammation and the scarring. [1] [3]
The risk factor that changes the management is the hormonal pattern in the female. The flaring along the jawline and the lower face, the premenstrual worsening, and the resistance to the standard topical therapy raise the polycystic ovary syndrome and the hyperandrogenism. The irregular menses, the hirsutism, and the acanthosis nigricans complete the picture, and the female-pattern acne reframes the treatment toward the combined oral contraceptive and the spironolactone alongside the topicals. [4] [9]
Pathophysiology
The pathophysiology of acne is the story of the pilosebaceous unit driven off the rails by the androgen and the organism. The sebaceous gland, dormant in childhood, is switched on by the pubertal androgens — the testosterone and the dihydrotestosterone — and the sebum output rises sharply. The sebum is the substrate and the fuel, and the lipophilic Cutibacterium acnes, the commensal renamed from Propionibacterium acnes, metabolises the triglycerides into the free fatty acids that irritate the follicular wall. [3] [8]
The plugging comes next. The follicular keratinocyte, normally shed one by one, becomes cohesive and sticky, and the lining thickens into the microcomedone — the invisible precursor that is the true first lesion of acne. The retained keratin, the sebum, and the bacterial products distend the follicle into the visible open or the closed comedone. The organism forms a biofilm within the plug, a structure that shields it from the antibiotic and the immune attack, and that biofilm is the reason the resistance and the recurrence are so hard to dislodge. [7] [8]
The inflammation is the rupture. The distended follicle wall gives way, spilling the keratin, the sebum, and the bacterial antigens into the dermis, and the neutrophils and the T cells rush in. The papule, the pustule, and the painful nodule are the clinical face of that immune fire, and the deeper and the more repeated the rupture, the greater the destruction of the dermis and the more certain the scar. The four drivers — the sebum, the organism, the plugging, and the inflammation — are the four targets the treatment is built around. [1] [10]
Clinical Presentation
The adolescent presents with the lesions over the sebum-rich skin and the story of a gradual, fluctuating course. The face — the forehead, the cheeks, the nose, the chin — is the commonest site, and the upper back, the chest, and the shoulders carry the disease in the more sebum-heavy teenager. The open comedones sit as the dark pinpoint plugs, the closed comedones as the small pale bumps, and the inflammatory lesions as the red papules, the yellow-centred pustules, and the deep tender nodules. The course waxes and wanes over months, and the premenstrual flare is the signature of the hormonal pattern in the female. [2] [12]
The atypical presentations are the ones the fellowship tests. The sudden, severe, ulcerative eruption with the fever, the arthralgia, and the malaise in the adolescent boy is the acne fulminans, the dermatological emergency. The acne concentrated on the jawline and the lower face of the female, with the premenstrual flare and the resistance to the topical therapy, is the hormonal pattern that demands the endocrine review. The acne with the sudden worsening, the painful nodules, and the systemic features asks the examiner to step back from the routine and to reach for the escalation. [1] [4]
The presentation that is easy to under-weight is the psychosocial one. The teenager who has stopped the sport, avoided the photographs, and grown quiet under the acne is signalling the distress that the lesion count alone will never capture. The acne carries a measurable burden on the quality of life, and the severe disease is associated with the anxiety, the depression, and the impaired self-image. The clinician who asks about the impact, and who treats to the patient's concern rather than the lesion count, is the clinician who prevents the harm the skin score hides. [9] [11]
Differential Diagnosis
The adolescent with the papules and the pustules on the face is usually the acne vulgaris, but the fellowship demands the mimics held and excluded. Rosacea shares the central-face redness and the papules, but it lacks the comedones, it sits on the background of the flushing and the telangiectasia, and it is the disease of the older adult rather than the adolescent. The folliculitis presents the pustules centred on the hair follicles, often staphylococcal or malassezia, and it follows the shaving, the occlusion, or the hot humid exposure. The perioral dermatitis rings the mouth and the nose with the papules and the scale, classically after the topical steroid. [2] [3]
The drug-induced acneiform eruption is the mimic that the history catches. The systemic corticosteroid, the anabolic steroid, the lithium, the antiepileptics, and the halogens produce the monomorphic papules and the pustules without the comedones, and the onset tracks the drug. The occupational and the cosmetic occlusion produce the localised acne, and the chloracne, the rare persistent comedonal eruption of the dioxin exposure, is the extreme. The keratosis pilaris, the rough follicular papules of the outer upper arms and the thighs, is the dry keratinisation disorder rather than the sebum-driven disease, and it is managed with the emollients, not the acne drugs. [3] [12]
The endocrine mimic is the one the fellowship rewards. The female with the severe, sudden, or treatment-resistant acne, the irregular menses, the hirsutism, and the acanthosis nigricans raises the polycystic ovary syndrome, the non-classic congenital adrenal hyperplasia, and rarely the androgen-secreting tumour. The acne with the clitoromegaly, the deepening voice, or the rapid virilisation is the tumour until proven otherwise. The onset of the acne before the age of seven is the precocious adrenarche, and it needs the paediatric endocrinology review. [4] [9]
The mimics of adolescent acne
Acne vulgaris
Rosacea
Folliculitis
Drug-induced acneiform
Keratosis pilaris
Clinical & Bedside Assessment
The assessment is the history and the examination, because the diagnosis is clinical and no test confirms the routine case. The history asks the onset, the distribution, the flare factors, the prior treatments and their adherence, the menstrual link in the female, the diet and the cosmetics, the family history of the severe or the scarring disease, and — above all — the impact on the mood, the sleep, the school, and the social life. The treatment adherence and the patient's own goals frame the plan, because the acne that the teenager will not treat consistently will not improve. [1] [11]
The examination grades the disease and the scar risk. The clinician records the distribution, the lesion types, and the relative proportion of the comedonal and the inflammatory lesions, and grades the severity on a reproducible scale. The Investigator Global Assessment, a five-point scale from the clear to the severe, anchors the communication and the follow-up, and the lesion counts support it. The clinician looks for the scarring — the atrophic ice-pick, the boxcar, and the rolling scars, and the hypertrophic or the keloid scars — and for the post-inflammatory hyperpigmentation, which is more visible and more distressing in the darker skin. The truncal involvement is noted, because it changes the topical reach and the systemic decision. [2] [10]
The bedside assessment carries the safety-net. The clinician screens the mood and the self-harm risk in the adolescent whose acne distresses them, because the severe disease and the hopelessness are the dangerous pair. The female with the hormonal pattern is asked about the menstrual irregularity and examined for the hirsutism and the acanthosis, and the examination findings guide the endocrine workup. The red flags — the fulminans, the virilisation, the precocious onset, the suicidal ideation — are the features that move the assessment from the routine to the urgent. [4] [9]
Investigations
The routine acne needs no investigation, and the over-investigation is the mark of the uncertain clinician. The diagnosis is clinical, and the first-line treatment is begun on the history and the examination alone. The investigation enters when the presentation is atypical, the disease is refractory, the endocrine cause is suspected, or the isotretinoin is planned. [1] [11]
The endocrine workup is reserved for the female with the hormonal pattern. The severe, the sudden, or the treatment-resistant acne with the irregular menses, the hirsutism, or the virilisation warrants the early-morning free testosterone, the dehydroepiandrosterone sulphate, the luteinising hormone and the follicle-stimulating hormone, and the 17-hydroxyprogesterone to exclude the non-classic congenital adrenal hyperplasia. The markedly elevated testosterone or the dehydroepiandrosterone sulphate raises the androgen-secreting tumour and the paediatric endocrinology referral, and the polycystic ovary syndrome is a clinical and the biochemical diagnosis that the gynaecology and the endocrinology share. [4] [9]
The pre-isotretinoin panel is the baseline that every course begins with. The pregnancy test — the serum or the urine beta-human chorionic gonadotropin — is the non-negotiable first test in the female of the childbearing potential, and it is repeated at each visit under the pregnancy-prevention programme. The fasting lipids and the liver function tests screen for the hypertriglyceridaemia and the transaminitis that the isotretinoin can raise, and the full blood count completes the baseline. The lipids and the liver are repeated at one to two months and then as the course demands, and the patient is counselled on the dryness, the photosensitivity, the mood, and the teratogenicity before the first capsule. [5] [6]
Management — Resuscitation
There is no resuscitation in the routine acne, and the fellowship candidate who names this explicitly steadies the viva. The disease is chronic and the treatment is elective, and the first-line therapy is the topical combination begun at the outpatient visit. The resuscitation frame enters only at the two acute escalations, and the recognition of them is the test. [1] [3]
The acute dermatological emergency is the acne fulminans. The adolescent, most often the boy, presents the sudden onset of the severe, painful, ulcerative nodules and the crusted plaques over the face, the back, and the chest, with the fever, the malaise, the arthralgia, and sometimes the osteolytic bone lesions. The immediate management is the systemic corticosteroid — the oral prednisolone at 0.5 to 1 mg/kg per day — to suppress the systemic inflammation, and the low-dose isotretinoin is introduced gradually only as the inflammation settles. The abrupt isotretinoin or the oral antibiotic alone worsens the fulminans, and the referral to the dermatology is immediate. [1] [5]
The acute psychosocial emergency is the suicidal ideation in the adolescent whose acne has worn the hope down. The severe acne and the depression travel together, and the clinician who screens and finds the active intent or plan does not defer to the dermatology waitlist. The urgent psychosocial assessment, the safety planning, and the mental-health escalation run alongside the aggressive acne treatment, because the acne itself is the driver of the mood and the effective treatment is part of the safety. The isotretinoin, in this context, is not the cause to fear but the disease to treat. [9] [11]
Management — Definitive & Stepwise
The definitive treatment is the graded ladder, and each rung pairs the drug with the dose, the route, the timing, and the rationale. The foundation of every rung is the topical retinoid, because it fixes the microcomedone upstream and works as the maintenance long after the flare settles. The benzoyl peroxide is the antibacterial partner that no antibiotic should travel without. [1] [2]
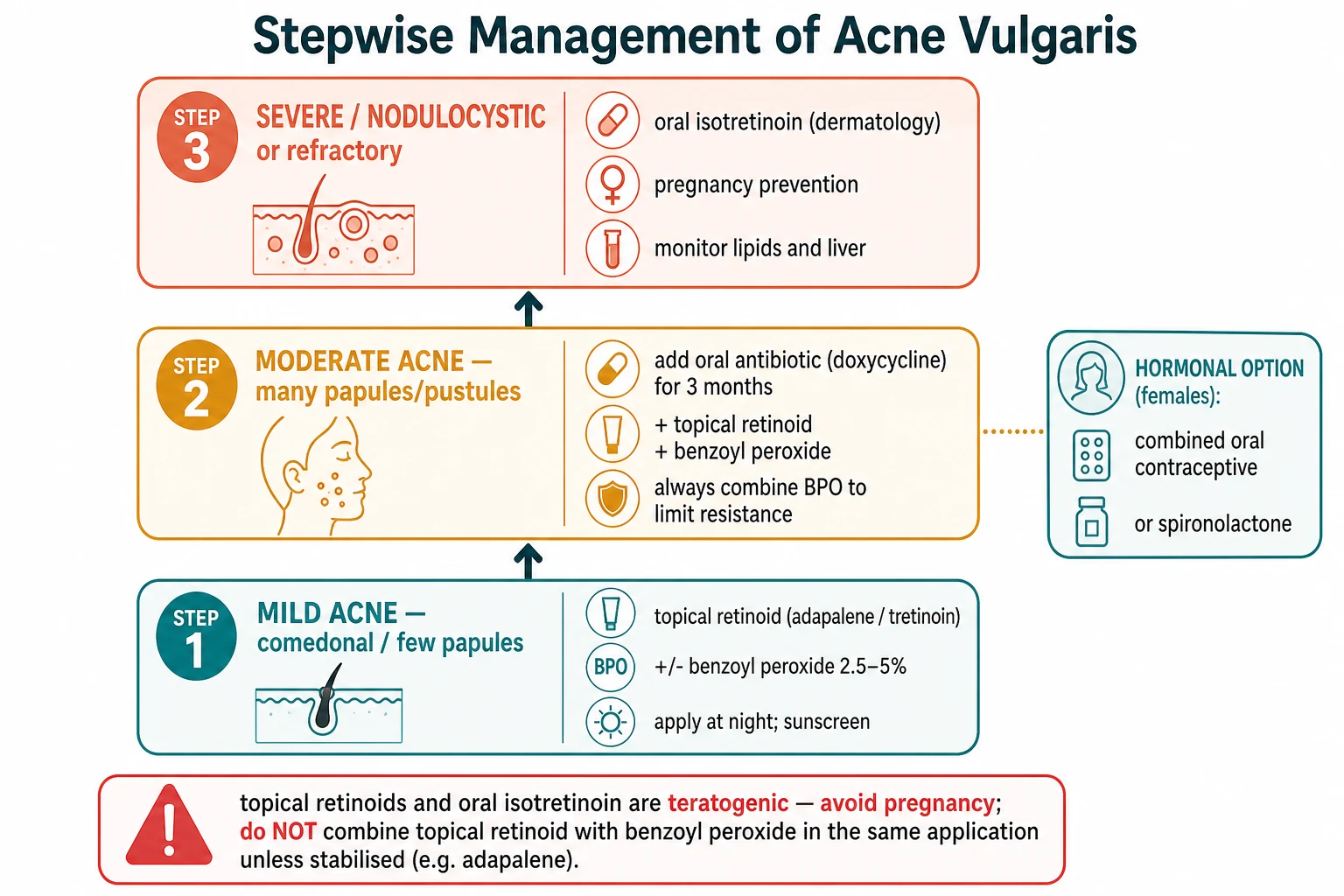
The mild comedonal disease answers to the topical retinoid and the benzoyl peroxide. The adapalene 0.1 per cent gel or cream is applied as a thin film to the whole affected area at night — not just the spots — and the benzoyl peroxide 2.5 per cent is applied once or twice daily; the 2.5 per cent strength matches the higher strengths with the less irritation. The tretinoin 0.025 per cent is the alternative retinoid, applied at night, but it is degraded by the benzoyl peroxide, so the two are separated in time or swapped for the adapalene, which is photostable and combines safely. The patient is warned of the dryness and the photosensitivity and counselled on the sunscreen, and the improvement is judged at six to eight weeks. [1] [11]
The moderate inflammatory disease adds the oral antibiotic. The doxycycline 50 to 100 mg once daily, or the lymecycline 300 to 408 mg once daily, is given for three months alongside the topical retinoid and the benzoyl peroxide, and never alone. The antibiotic course is capped — the guidelines advise the review and the stop by three to four months — because the prolonged monotherapy breeds the resistant Cutibacterium acnes. The benzoyl peroxide is always paired with the antibiotic to limit the resistance, and the topical retinoid carries the maintenance after the antibiotic stops. [1] [7]
The severe nodulocystic disease, the scarring disease, and the disease that fails three months of the combination therapy move to the oral isotretinoin. The isotretinoin is started at 0.5 mg/kg per day and titrated toward 1.0 mg/kg per day, with the cumulative dose target of 120 to 150 mg/kg over the four to eight month course that best predicts the durable remission. The mucocutaneous dryness, the lip and the eye dryness, the photosensitivity, the lipid and the liver monitoring, and the absolute teratogenicity are counselled at the outset. The tetracycline is stopped before the first capsule, because the combination raises the benign intracranial hypertension. The course is supervised by the dermatology, and the low-dose and the standard-dose regimens are both supported. [5] [6]
The graded acne ladder — the rungs
Mild, comedonal or few papules: topical adapalene 0.1 per cent at night plus benzoyl peroxide 2.5 per cent daily; counsel on the dryness, the photosensitivity, and the sunscreen; review at six to eight weeks.
Mild inflammatory: add a topical antibiotic such as clindamycin 1 per cent with the benzoyl peroxide or the retinoid; never the antibiotic alone; review the adherence and the irritation.
Moderate inflammatory: oral doxycycline once daily for three months with the topical retinoid and the benzoyl peroxide; cap the course and review at three months.
Severe, scarring, or refractory: refer to the dermatology for the oral isotretinoin; stop the tetracycline first; baseline the pregnancy test, the lipids, and the liver; counsel the teratogenicity.
Maintenance: continue the topical retinoid with or without the benzoyl peroxide long-term; the microcomedone recurs the moment the retinoid stops.
In Australasia, the isotretinoin is prescribed under the dermatology oversight with the contraception counselling and the repeated pregnancy testing, and the generalist initiates the topical and the oral antibiotic ladder and refers the severe or the refractory. The combined oral contraceptive and the spironolactone are the off-label or the shared-care hormonal options for the female-pattern disease, and the access to the dermatology and the isotretinoin is the equity issue in the rural and the remote adolescent. [11] [12]
Specific Subtypes & Scenarios
The acne fulminans is the severe subtype that commands its own protocol. The adolescent boy presents the acute onset of the ulcerative, crusted nodules over the back and the chest, with the fever, the arthralgia, the myalgia, and the malaise, and occasionally the painful osteolytic bone lesions. The aetiology is the explosive immune reaction to the Cutibacterium antigens, sometimes triggered by the high-dose testosterone or the anabolic steroid. The management is the oral prednisolone 0.5 to 1 mg/kg per day for several weeks to settle the systemic inflammation, followed by the gradual introduction of the low-dose isotretinoin at 0.5 mg/kg per day, titrated up. The referral is immediate, and the scarring is the long-term consequence the early control limits. [1] [5]
The hormonal or the female-pattern acne is the subtype that reframes the drugs. The flaring along the jawline and the lower face, the premenstrual worsening, and the resistance to the topical and the oral antibiotic therapy are the signature, and the irregular menses, the hirsutism, and the acanthosis nigricans complete the polycystic ovary syndrome. The combined oral contraceptive — the ethinylestradiol with the drospirenone or the norgestimate — and the spironolactone 50 to 100 mg per day, titrated toward 200 mg, are the anti-androgen mainstays, added to the topical retinoid and the benzoyl peroxide. The COC and the spironolactone are the options the female with the treatment-resistant disease benefits from, and they are prescribed with the contraception and the electrolyte counselling. [4] [9]
The acne in the transgender and the gender-diverse adolescent on the masculinising testosterone is the subtype the modern fellowship tests. The exogenous testosterone raises the sebum output and the acne severity, and the disease can be the nodulocystic and the refractory. The topical and the oral antibiotic ladder applies, and the isotretinoin is effective and safe in this group, with the contraception and the pregnancy-prevention considerations tailored to the anatomy and the hormone regimen. The respectful, the gender-affirming, and the evidence-based care is the standard. [1] [4]
Complications & Pitfalls
The scarring is the complication that no later treatment fully reverses, and its prevention is the justification for the early and the effective treatment. The atrophic scars — the ice-pick, the boxcar, and the rolling scars — follow the dermal destruction of the deep inflammatory lesion, and the hypertrophic and the keloid scars follow the exaggerated healing, more commonly on the chest, the back, and the darker skin. The post-inflammatory hyperpigmentation is the common and the distressing sequela in the darker skin type, and it adds months to the recovery. The Liu 2023 systematic review found the scarring prevalent and closely tied to the severity and the delay, which is why the severe and the scarring disease is the indication for the isotretinoin. [10] [11]
The isotretinoin carries the adverse-effect profile the fellowship demands verbatim. The teratogenicity is absolute, and the retinoid embryopathy — the craniofacial, the cardiac, and the thymic defects — is the reason for the pregnancy-prevention programme. The mucocutaneous effects — the cheilitis, the dry skin, the dry eyes, the epistaxis, and the photosensitivity — are near-universal and managed with the emollients and the lip balm. The lipids and the liver transaminases can rise, and the monitoring catches the hypertriglyceridaemia. The benign intracranial hypertension is the reason the tetracycline is stopped first. The mood and the inflammatory bowel disease associations remain debated, and the current evidence finds no consistent causal link for the depression, though the monitoring and the counselling stand. [5] [6]
The antibiotic resistance is the complication of the prescribing pattern, and the stewardship is the prevention. The prolonged antibiotic monotherapy, the topical or the oral, selects the resistant Cutibacterium acnes, and the Zhu 2025 systematic review documented the substantial resistance rates, especially to the erythromycin and the clindamycin. The rules are simple: never prescribe the antibiotic alone, always pair it with the benzoyl peroxide, cap the oral course at three to four months, and never combine the topical erythromycin with the topical clindamycin. The retinoid and the benzoyl peroxide carry the maintenance that the resistance-prone antibiotic cannot. [1] [7]
Prognosis & Disposition
The natural history of the adolescent acne is the slow remission over the late teens and the early twenties, but a substantial minority — and more often the female — carries the disease into the adulthood. The predictors of the persistence and the scarring are the severity, the nodulocystic disease, the truncal involvement, the strong family history, the delay in the effective treatment, and the picking. The early and the adequate treatment is the single most modifiable determinant of the outcome, and the generalist who treats to the scarring risk, not the lesion count, prevents the permanent harm. [2] [10]
The disposition follows the severity and the response. The mild and the moderate disease is managed in the primary care with the topical and the oral antibiotic ladder, and the review at six to eight weeks for the topical and at three months for the oral antibiotic. The referral to the dermatology is for the nodulocystic disease, the scarring or the high scar risk, the failure of three months of the combination therapy, the suspected endocrine cause, the significant psychosocial impact, and the isotretinoin candidacy. The acne fulminans and the suspected tumour are the immediate referrals. [1] [11]
The safety-net is the follow-up and the maintenance. The topical retinoid is continued — with or without the benzoyl peroxide — long after the lesions clear, because the microcomedone recurs the moment the treatment stops, and the maintenance is the half of the treatment the adolescent underestimates. The mood and the scarring are reviewed at each visit, and the transition to the adult care and the dermatology is planned for the severe and the persistent disease. [2] [9]
Special Populations
The adolescent female is the population the contraception and the teratogenicity frame. The isotretinoin and the topical retinoids are the teratogens, and the reliable contraception and the negative pregnancy test are the prerequisites for the isotretinoin, with the repeated testing under the pregnancy-prevention programme. The combined oral contraceptive serves the double duty of the contraception and the anti-androgen, and the spironolactone adds the anti-androgen with the potassium monitoring. The female with the hormonal pattern benefits from the endocrine review and the tailored hormonal therapy alongside the standard topicals. [4] [5]
The male adolescent carries the higher sebum load and the more truncal and the more severe disease, and the back and the chest involvement raise the topical-versus-systemic decision. The topical reach is limited on the trunk, and the moderate-to-severe truncal disease moves earlier to the oral antibiotic and the isotretinoin. The anabolic steroid and the supplement use is asked, because it drives the severe and the fulminant disease. [1] [12]
The indigenous, the rural-remote, and the socioeconomically disadvantaged adolescent is the population the access frames. The delay in the dermatology and the isotretinoin access, the cost of the topicals, and the photoprotection gaps widen the scarring burden, and the telehealth and the shared-care pathways are the equity levers. The transgender and the gender-diverse adolescent on the testosterone is the population the respectful and the tailored care serves, and the isotretinoin is the effective option with the anatomy-appropriate contraception counselling. [9] [11]
Evidence, Guidelines & Regional Differences
The guidelines converge on the graded ladder with the regional accents. The American Academy of Dermatology 2024 guideline, the Reynolds work, sets the contemporary standard: the topical retinoid and the benzoyl peroxide first, the oral antibiotic added for the moderate inflammatory disease and always paired with the benzoyl peroxide, and the oral isotretinoin for the severe, the scarring, and the refractory. The European guidance and the United Kingdom Drug and Therapeutics Bulletin 2023 align on the ladder and emphasise the antibiotic stewardship and the patient-centred severity. The Australasian Gebauer 2017 review carries the same structure for the primary care. [1] [11]
The isotretinoin-depression controversy is the evidence debate the fellowship tests. The early regulatory concern followed the case reports, but the systematic reviews and the Cochrane 2018 review found no consistent causal link between the isotretinoin and the depression, and the acne itself is the established driver of the mood harm. The current practice counsels and monitors the mood without withholding the effective treatment, and the shared decision and the documentation carry the medico-legal protection. [5] [6]
The diet controversy and the dosing debate round out the evidence. The high-glycaemic-load diet and the skim-milk intake carry a modest and debated association, enough to counsel but not to prescribe. The low-dose versus the standard-dose isotretinoin debate turns on the tolerability and the relapse: the lower dose extends the course to the cumulative target and reduces the acute flare, while the standard dose reaches the target sooner, and both achieve the durable remission at the 120 to 150 mg/kg cumulative dose. The prophylactic corticosteroid or the lower starting dose is used for the fulminans-prone and the severe nodulocystic disease. [5] [11]
Costa 2018 — Cochrane review of oral isotretinoin for acne
Population: Moderate-to-severe acne vulgaris
Key finding
Oral isotretinoin is effective for the severe nodulocystic and the refractory acne, with the cumulative dose the best predictor of the durable remission; the evidence on the head-to-head dosing and the adverse-event comparisons remains limited and the monitoring standard.
Practice change
The isotretinoin is the definitive therapy for the severe, the scarring, and the refractory disease, prescribed with the pregnancy prevention and the lipid and liver monitoring.
Exam Pearls
Hold the high-yield facts the examiner rewards. Never prescribe the antibiotic monotherapy, topical or oral — always pair it with the benzoyl peroxide, and cap the oral course at three to four months. The adapalene is the photostable retinoid that combines safely with the benzoyl peroxide; the tretinoin is degraded by it, so separate the two in time. The isotretinoin cumulative dose target of 120 to 150 mg/kg governs the relapse, and the tetracycline is stopped before the first capsule to avoid the benign intracranial hypertension. [1] [2]
Hold the acne fulminans protocol. The severe ulcerative eruption with the fever and the arthralgia is the emergency: the oral prednisolone 0.5 to 1 mg/kg per day first, then the gradual low-dose isotretinoin, never the abrupt isotretinoin or the antibiotic alone. The female with the jawline and the premenstrual flare, the irregular menses, and the hirsutism is the polycystic ovary syndrome until the workup, and the combined oral contraceptive and the spironolactone join the standard topicals. The topical retinoid is the maintenance, because the microcomedone recurs the moment it stops. [3] [9]
Hold the mimics and the red flags. The rosacea lacks the comedones, the folliculitis centres on the hair, the drug eruption is the monomorphic papule without the comedone, and the keratosis pilaris is the dry outer arm. The acne before the age of seven, or with the clitoromegaly and the rapid virilisation, is the endocrine red flag for the paediatric endocrinology. The post-inflammatory hyperpigmentation and the keloid are the commoner and the more visible sequela in the darker skin, and the early treatment is the prevention. [4] [10]
The five rules you must say aloud at the viva
One: the antibiotic is never alone. Two: the benzoyl peroxide always travels with the antibiotic. Three: the adapalene combines with the benzoyl peroxide; the tretinoin does not. Four: the isotretinoin target is the cumulative 120 to 150 mg/kg, and the tetracycline stops first. Five: the fulminans is the corticosteroid before the isotretinoin. Say these and the examiner moves on. [1] [7]
References
- [1]Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris Journal of the American Academy of Dermatology, 2024.PMID 38300170
- [2]Eichenfield DZ, Sprague J, Eichenfield LF. Management of Acne Vulgaris: A Review JAMA, 2021.PMID 34812859
- [3]Williams HC, Dellavalle RP, Garner S. Acne vulgaris Lancet, 2012.PMID 21880356
- [4]Eichenfield LF, Krakowski AC, Piggott C, et al. Evidence-based recommendations for the diagnosis and treatment of pediatric acne Pediatrics, 2013.PMID 23637225
- [5]Bagatin E, Costa CS. The use of isotretinoin for acne - an update on optimal dosing, surveillance, and adverse effects Expert Review of Clinical Pharmacology, 2020.PMID 32744074
- [6]Costa CS, Bagatin E, Martimbianco ALC, et al. Oral isotretinoin for acne Cochrane Database of Systematic Reviews, 2018.PMID 30484286
- [7]Zhu C, Wei B, Li Y, et al. Antibiotic resistance rates in Cutibacterium acnes isolated from patients with acne vulgaris: a systematic review and meta-analysis Frontiers in Microbiology, 2025.PMID 40535003
- [8]Dreno B, Pecastaings S, Corvec S, et al. Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates Journal of the European Academy of Dermatology and Venereology, 2018.PMID 29894579
- [9]Gieler U, Gieler T, Kupfer JP. Acne and quality of life - impact and management Journal of the European Academy of Dermatology and Venereology, 2015.PMID 26059729
- [10]Liu L, Xue Y, Chen Y, et al. Prevalence and risk factors of acne scars in patients with acne vulgaris Skin Research and Technology, 2023.PMID 37357642
- [11]Santer M, Burden-Teh E, Ravenscroft J. Managing acne vulgaris: an update Drug and Therapeutics Bulletin, 2023.PMID 38154809
- [12]Gebauer K. Acne in adolescents Australian Family Physician, 2017.PMID 29464224