Paeds · paediatric-dermatology
Alopecia and hair disorders in children
Also known as Alopecia areata · Hair loss in children · Trichotillomania · Telogen effluvium · Patchy hair loss
Fellowship guide to alopecia and hair disorders in children: the smooth non-scaly bald patch with exclamation-mark hairs of alopecia areata, an organ-specific autoimmune attack on the anagen hair bulb; the diffuse shedding two to three months after a trigger that marks telogen effluvium; the irregular patch of hairs broken to varying lengths that betrays trichotillomania; the hairline thinning of traction alopecia; and the scaly broken stubs and lymphadenopathy of tinea capitis. Bedside confirmation with dermoscopy, the hair pull test, potassium hydroxide microscopy and thyroid and iron studies. The stepwise ladder for alopecia areata from topical and intralesional corticosteroid and topical minoxidil through topical immunotherapy to systemic agents and JAK inhibitors, the habit-reversal and cognitive behavioural therapy that is first-line for trichotillomania, and the trigger removal and reassurance that settle most telogen effluvium.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eight-year-old girl whose mother has just noticed a coin-sized, completely bald, smooth patch behind her left ear. The skin looks normal, there is no scale and no redness, and around the edge are a few short hairs that taper to a fine point. This is alopecia areata, the archetypal non-scarring alopecia of childhood, and the smooth bald patch with those tapering exclamation-mark hairs is the single most useful clue that the cause is autoimmune rather than infectious or behavioural. [1]
Now picture a different child: a ten-year-old who, six weeks after a nasty febrile illness, finds handfuls of hair on her pillow and in the shower drain. There is no bald patch, just generalised thinning all over the scalp. This is telogen effluvium, the common reactive shedding that follows a trigger by two to three months, and the diffuse pattern and the timing point straight to a disturbance of the hair cycle rather than to a discrete scalp disease. [10]
A third child, a twelve-year-old boy, has an odd, irregular area of thinned hair over the crown with hairs of all different lengths sticking up, and the scalp beneath looks entirely normal. He denies pulling at it. This is trichotillomania, a body-focused repetitive behaviour, and the varying lengths on a normal scalp are the signature. [8]
Alopecia simply means loss of hair from where it normally grows, and classifying it turns on one question: is the follicle preserved or destroyed? In the common, non-scarring disorders the follicle survives, the skin surface is normal, and regrowth is possible. In the rare, scarring (cicatricial) disorders the follicle is permanently destroyed and the skin is altered. Most paediatric hair loss is non-scarring, so the central task is to recognise the pattern of each common form, to identify the few scarring causes early before the follicle is lost, and to choose treatment by the diagnosis rather than reaching for a generic hair lotion. [12]
Classification
The most useful first split in a child with hair loss is between non-scarring and scarring disease, because it predicts whether the loss is reversible and because it sets the urgency. [12]
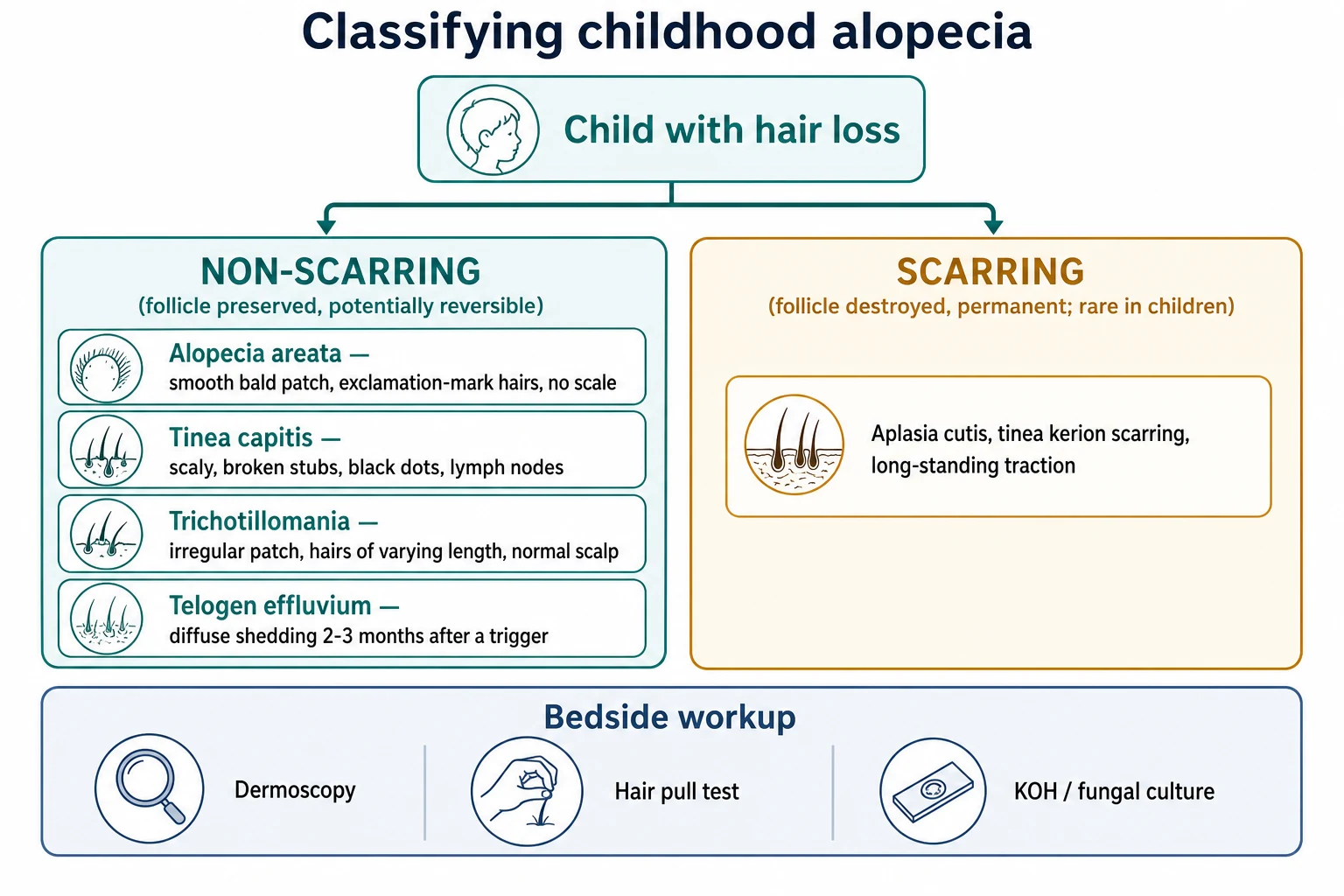
Within the non-scarring group, five disorders cover almost everything a fellowship candidate will meet. Alopecia areata is the autoimmune patchy or diffuse loss of anagen hairs. Telogen effluvium is diffuse reactive shedding after a trigger. Trichotillomania is mechanical hair-pulling. Traction alopecia is hairline loss from tight hairstyles. And tinea capitis is an infectious, treatable mimic that sits in the differential of any scaly bald patch. Androgenetic alopecia is patterned thinning that may appear in an older adolescent after puberty. [12]
A second axis, by mechanism, helps organise the differential: autoimmune (alopecia areata), infectious (tinea capitis), traumatic or behavioural (trichotillomania, traction), physiologic or reactive (telogen effluvium), androgen-dependent (androgenetic), and the rare congenital or structural causes such as aplasia cutis congenita, loose anagen syndrome and temporal triangular alopecia that appear in infants. [11]
Alopecia areata
autoimmune, non-scarring
- Smooth bald patch, no scale
- Exclamation-mark hairs at the edge
- Nail pitting or trachyonychia
- Autoimmune thyroid association
Tinea capitis
infectious, non-scarring
- Scaly broken stubs and black dots
- Occipital or cervical lymphadenopathy
- Potassium hydroxide positive
- Needs an oral antifungal
Trichotillomania
behavioural, non-scarring
- Irregular patch of varying-length hairs
- Normal scalp, no scale
- Pulling behaviour, often denied
- Habit-reversal therapy first-line
Telogen effluvium
reactive, non-scarring
- Diffuse generalised shedding
- Two to three months after a trigger
- Positive hair pull test
- Self-limiting once trigger resolves
The scarring group is uncommon in children but matters precisely because delay is irreversible. Aplasia cutis congenita presents at birth with a defect of skin, a long-standing or incised kerion can leave a permanent bald scar, and chronic traction can eventually scar the hairline. The teaching point is that a non-scarring pattern reassures, while any patch with loss of follicular openings, atrophy or active inflammation must reach dermatology before the follicle is gone. [12]
Epidemiology & Risk Factors
Alopecia areata is one of the most common non-scarring alopecias of childhood. Its lifetime prevalence is around two per cent, and roughly half of all cases begin before the age of twenty, so a fellowship candidate will meet it repeatedly. [4]
The risk factors and associations for alopecia areata are themselves high-yield. A family history is present in roughly ten to twenty per cent, atopy is over-represented, and the condition is more common in Down syndrome. The most important association is with other autoimmune disease, above all autoimmune thyroid disease, but also vitiligo and type 1 diabetes, which is why thyroid screening is built into the work-up. [4]
Telogen effluvium is a common, self-limiting cause of diffuse shedding in children, appearing two to three months after a high fever, a surgical illness, rapid weight loss or a crash diet, severe emotional stress, or the onset of a thyroid disorder. Trichotillomania often begins in childhood or adolescence and, after puberty, shows a female predominance. Tinea capitis peaks between three and seven years of age and is covered in detail in its own topic, but it appears here because it is the infectious mimic of every bald patch. [10] [8]
Pathophysiology
To understand why each alopecia looks the way it does, follow the hair follicle through its cycle. Each follicle moves through a long anagen growth phase measured in years, a short catagen regression phase of weeks, and a telogen resting phase of months, after which the club hair sheds and the cycle restarts. At any moment around ten per cent of scalp follicles are in telogen, which is the baseline against which telogen effluvium is measured. [10]
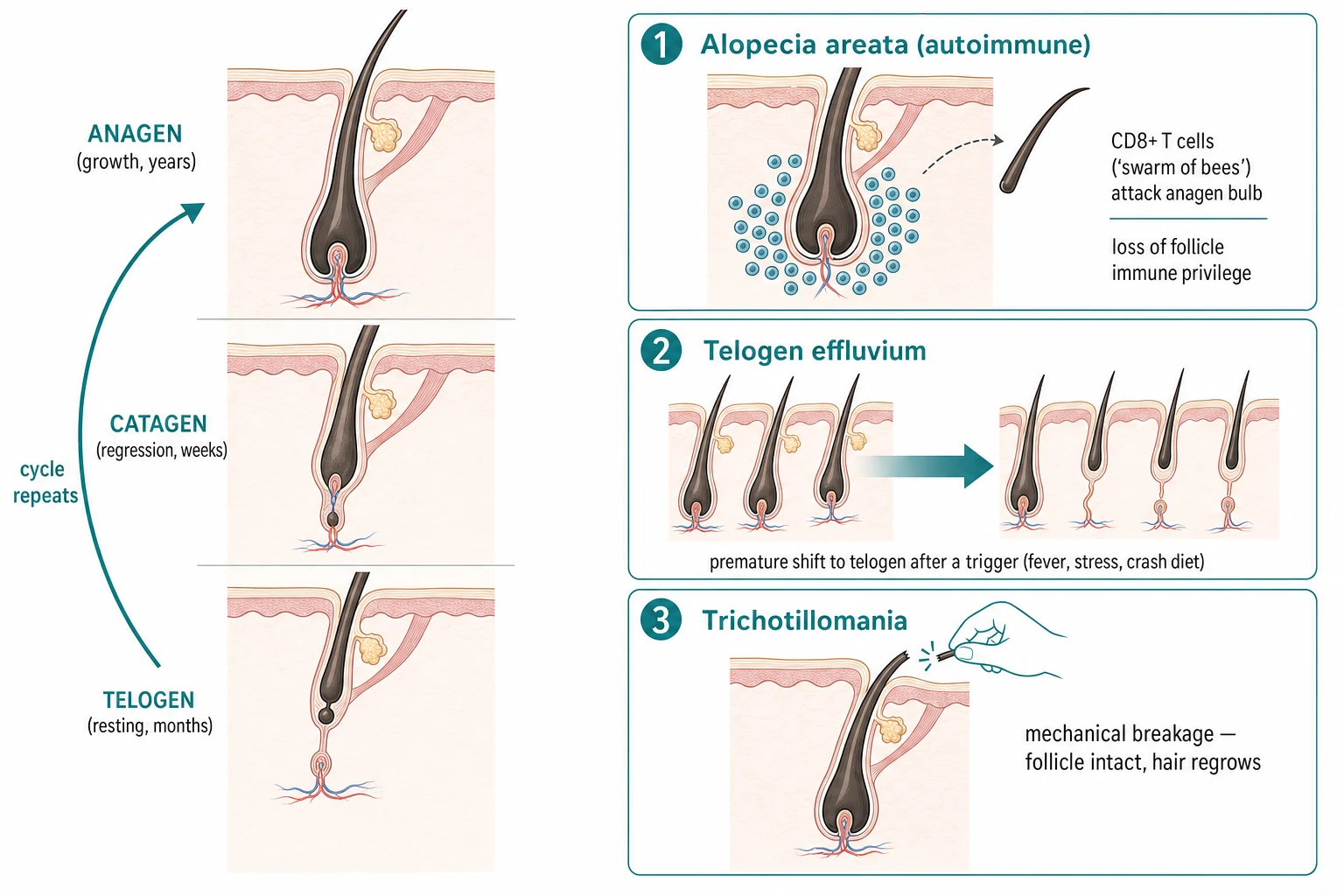
Alopecia areata is an organ-specific, T-cell-mediated autoimmune disease. The anagen hair bulb normally enjoys immune privilege, but when that privilege collapses, CD8-positive NKG2D-positive T cells cluster around the bulb in the perifollicular infiltrate that histologists call the swarm of bees. The attacked follicle is driven prematurely into a dystrophic catagen, the hair shaft narrows, and it breaks at the narrow point to produce the exclamation-mark hair. Because the follicle itself is not destroyed, regrowth remains possible once the immune attack is quieted. [7]
Telogen effluvium works by a different but related mechanism. A trigger drives an abnormally large fraction of anagen follicles prematurely into telogen, and two to three months later those follicles shed their club hairs together, producing the diffuse increase in daily shedding. The follicle is intact throughout, which is why the hair loss is diffuse and reversible once the trigger passes. [10]
Trichotillomania and traction alopecia are mechanical. The follicle is entirely healthy and the hair shaft is simply broken or pulled, so the scalp looks normal and the hair regrows once the behaviour stops or the hairstyle is loosened. The same logic explains why tinea capitis, though it causes hair loss, is fundamentally an infection of the hair shaft rather than a primary follicular disease, and why the broken stubs and scale point to fungus rather than to autoimmunity. [8] [12]
Clinical Presentation
The smooth bald patch of alopecia areata is hard to mistake once seen. It appears suddenly as one or more well-demarcated, completely bald, smooth and non-scaly patches with no inflammation. At the advancing edge, exclamation-mark hairs, short broken hairs that are narrower at the scalp than at the tip, are the pathognomonic sign. Most children present with limited patchy disease, but the pattern can extend into an ophiasis band across the occipital and temporal scalp, into alopecia totalis loss of the whole scalp, or into alopecia universalis loss of all body hair. Nail involvement such as pitting, trachyonychia or onychorrhexis occurs in around ten to fifteen per cent and is a useful clue. [1] [4]
Trichotillomania presents differently. The hair loss is patchy and irregular, with an ill-defined ragged or felted border, and the defining feature is hairs broken to wildly varying lengths on an otherwise completely normal scalp. It favours sites the child can easily reach, such as the crown and frontotemporal region, and may spare the back of the scalp. Children often deny the pulling, and a careful history may reveal that hair is eaten, which raises the risk of a trichobezoar. [8]
Telogen effluvium is diffuse rather than patchy. The child or parent describes increased daily shedding, often more than one hundred to one hundred and fifty hairs a day, with generalised thinning that typically spares the hairline. The hair pull test is positive, yielding multiple club hairs with their white bulbs. Traction alopecia shows the fringe sign of frontotemporal and hairline thinning in a child who wears tight braids, ponytails or extensions. And tinea capitis presents with the scaly, broken-stub, black-dot patch and the occipital or cervical lymphadenopathy that separate it from the non-infectious causes. [10] [12]
Differential Diagnosis
The differential for a bald patch is wide, and the discriminator is always at the edge of the lesion and on the surface of the scalp. The question to ask is whether the patch is smooth and non-scaly, pointing to alopecia areata, or scaly with broken stubs, pointing to tinea capitis. [12]
Alopecia areata
autoimmune
- Smooth, completely bald, non-scaly
- Exclamation-mark hairs
- No lymphadenopathy
- Autoimmune thyroid association
Tinea capitis
infectious
- Scaly broken stubs and black dots
- Occipital or cervical nodes
- Potassium hydroxide positive
- Oral antifungal, never steroid
Trichotillomania
behavioural
- Hairs of wildly varying length
- Normal scalp, no scale
- Sites the child can reach
- Pulling behaviour, often denied
Telogen effluvium
reactive
- Diffuse generalised shedding
- Trigger two to three months prior
- Positive pull test
- Spares the hairline
The pitfall that no candidate should miss is treating tinea capitis as alopecia areata. A topical corticosteroid applied to a scaly fungal patch suppresses the inflammation and itch, so the family is falsely reassured, but the fungus spreads unchecked in a modified form called tinea incognito. The broken stubs, the black dots and the lymphadenopathy are the features that redirect the diagnosis to tinea and the management to an oral antifungal. [12]
Two further mimics deserve respect. A boggy, purulent, painful scalp mass is a kerion, an intense hypersensitivity reaction to a dermatophyte rather than a bacterial abscess, and it needs an oral antifungal and corticosteroid rather than a knife. And any bald patch with loss of follicular openings, atrophy or active inflammation may be a scarring alopecia, and though these are rare in children, the cost of delay is a permanently bald scalp. [12]
Clinical & Bedside Assessment
Start with the story, because the history often gives the diagnosis before the examination. Ask when the loss began and how fast it has progressed, whether there was a recent fever, illness, surgery, rapid weight loss or severe stress, whether the thyroid is under question, what hair products and styles are used, and whether there is a family history of autoimmune disease or hair loss. Ask, sensitively and without judgement, about any hair-pulling, because trichotillomania is frequently denied and a direct, kind question is often the only way in. [8] [12]
Examine the whole scalp under good light. Note whether each patch is smooth or scaly, whether the hairs are intact or exclamation-mark shaped, whether the loss is focal, patchy, diffuse or band-like, and whether there is occipital or cervical lymphadenopathy. Perform the hair pull test by grasping a bundle of around fifty to sixty hairs close to the scalp and pulling gently outward; the test is positive if more than a few hairs come out, and it indicates active shedding, as in telogen effluvium. Look at the nails for pitting and trachyonychia, and examine the eyebrows and body hair if the loss is extensive. [1]
Dermoscopy, or trichoscopy, refines the bedside diagnosis and reduces the need for biopsy. Alopecia areata shows yellow dots, black dots, exclamation-mark hairs and short regrowing vellus hairs. Trichotillomania shows broken hairs of differing lengths with empty follicles and none of the exclamation-mark hairs of areata. The absence of scale and broken stubs distinguishes the autoimmune and behavioural causes from tinea capitis, which is then confirmed with potassium hydroxide microscopy. [12]
Investigations
Most non-scarring alopecia is a clinical diagnosis, and investigations are used to confirm the pattern and to exclude mimics rather than to biopsy routinely. [1]
For a scaly scalp, the first test is potassium hydroxide microscopy of a plucked hair or a scrape of the active border, looking for branching septate hyphae and arthroconidia that confirm tinea capitis. A Wood's lamp may show green fluorescence for some Microsporum species, but a negative lamp never excludes tinea, because Trichophyton tonsurans does not fluoresce. [12]
For diffuse shedding, send targeted bloods to find the trigger: a full blood count, ferritin or iron studies, and thyroid function tests to exclude iron deficiency and thyroid disease, both of which are common, treatable contributors to telogen effluvium and both worth screening when alopecia areata is accompanied by autoimmune thyroid risk. [10]
Reserve a scalp biopsy for the case that is not clarified at the bedside, and especially when a scarring alopecia is suspected. The histology of alopecia areata is a peribulbar lymphocytic infiltrate, the swarm of bees, around anagen follicles, and this, with dermoscopy and the pull test, will resolve the great majority of presentations without resort to tissue. [7]
Management — Resuscitation
Paediatric hair loss is rarely a time-critical emergency, but three situations need prompt action. A boggy, purulent, painful scalp mass is a kerion, an intense hypersensitivity reaction to a dermatophyte, and the longer the inflammation runs the greater the risk of a permanent scar, so start an oral antifungal early. Any bald patch with loss of follicular openings, atrophy or active inflammation may be a scarring alopecia, and though rare in children it must reach dermatology before the follicle is irreversibly lost. And when the pattern, history or accompanying findings raise concern for child maltreatment, act on safeguarding pathways rather than on the skin alone. [12]
For the well child with limited patchy alopecia areata there is no resuscitation step. The first move is reassurance that the condition is non-scarring and that regrowth is common, combined with a worked-up management plan and baseline thyroid screening, because the visible loss can be deeply distressing and a clear, honest plan is part of safe care. [1] [5]
Management — Definitive & Stepwise
The management of childhood alopecia is built around the diagnosis, and the ladder for alopecia areata is the most tested part. For limited patchy disease, first-line is a potent or ultrapotent topical corticosteroid, with or without topical minoxidil five per cent, applied to the patch and its margin. Intralesional triamcinolone acetonide, commonly five to ten milligrams per millilitre given in small volumes of around zero point zero five to zero point one millilitre per site every four to six weeks, is useful for a few discrete patches, with a lower concentration on the face. [1] [2]
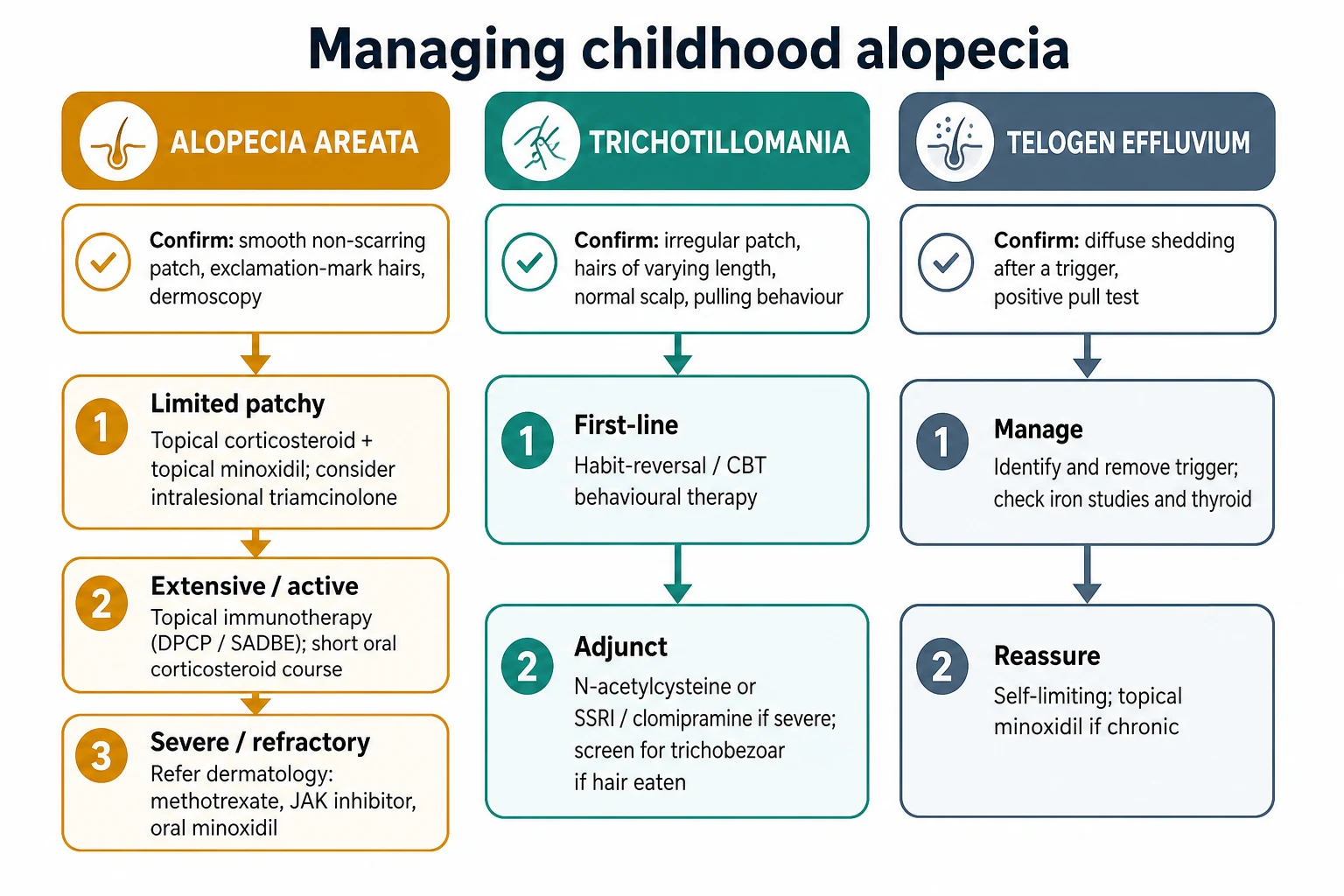
For extensive, rapidly progressive or refractory disease, escalate to topical immunotherapy with diphenylcyclopropenone or squaric acid dibutylester, and consider a short tapering course of oral corticosteroid to halt rapid shedding. Systemic therapy is given under specialist dermatology guidance and includes methotrexate, ciclosporin, low-dose oral minoxidil, and the JAK inhibitors such as baricitinib that are licensed in adults and emerging in adolescents. The oral minoxidil dosing used in the literature is low, for example zero point two five to five milligrams daily, and because it can cause hypertrichosis and, at higher doses, cardiovascular effects, it is reserved for specialist use. [3] [6]
Confirm the pattern and exclude tinea capitis with potassium hydroxide microscopy before any corticosteroid
For limited patchy alopecia areata start a potent topical corticosteroid with or without topical minoxidil, and consider intralesional triamcinolone for discrete patches
For extensive or active disease escalate to topical immunotherapy with diphenylcyclopropenone or squaric acid dibutylester, and a short oral corticosteroid course
Reserve systemic therapy, oral minoxidil and JAK inhibitors for refractory disease under dermatology guidance
Screen for autoimmune thyroid disease and arrange psychosocial support and review
The other disorders are managed by their own logic, not by the areata ladder. Trichotillomania is treated first-line with habit-reversal and cognitive behavioural therapy, because the behavioural driver must be addressed for any treatment to hold; pharmacotherapy with N-acetylcysteine, a selective serotonin reuptake inhibitor or clomipramine is an adjunct for severe cases, though the evidence is modest. Telogen effluvium is managed by identifying and removing the trigger, correcting iron deficiency and thyroid disease, and reassuring the family that acute shedding is self-limiting; topical minoxidil is reserved for the chronic form. Traction alopecia reverses with loosening of the hairstyle, provided it is caught before scarring sets in. [8] [9] [10]
Specific Subtypes & Scenarios
The prognosis of alopecia areata is decided by its subtype. Limited patchy disease is the majority and carries a high rate of spontaneous or treatment-assisted regrowth, especially in a first episode. The ophiasis pattern, and the totalis and universalis patterns, carry a worse prognosis, as do the features that predict a harder course: atopy, early childhood onset, nail involvement, long duration before treatment, extensive involvement, and a family history of the disease. Naming these features for a family sets honest expectations. [4]
Trichotillomania is classified among the obsessive-compulsive and related disorders as a body-focused repetitive behaviour. It often begins in childhood or adolescence, is frequently associated with anxiety or depression, and may be denied by the child. A specific risk is trichophagy, the eating of pulled hair, which can form a trichobezoar and, in its extension known as Rapunzel syndrome, cause gastric outlet or intestinal obstruction. Asking about hair eating is part of the assessment, and habit-reversal therapy is the evidence-based first-line treatment. [8]
Chronic telogen effluvium, lasting more than six months, is less common in children than the acute form and may overlap with or unmask androgenetic alopecia in an adolescent. In an infant, the structural and congenital causes come to the fore: aplasia cutis congenita presents at birth with a localized skin defect, loose anagen syndrome causes painless, easily pluckable thin hair in young children, and temporal triangular alopecia produces a stable lanc-shaped patch at the frontotemporal hairline. These are usually recognised clinically and managed expectantly or with surgical revision later where appropriate. [10] [11]
Complications & Pitfalls
The preventable complications of childhood alopecia are largely the cost of misdiagnosis and delay. The high relapse rate and occasional progression to totalis or universalis of alopecia areata, the permanent follicle loss of an untreated scarring alopecia or long-standing traction alopecia, and the trichobezoar of unrecognised trichophagy all carry real morbidity. The visible nature of the loss adds a heavy burden of psychosocial distress, anxiety, depression and reduced quality of life, which is itself a complication to manage, not a footnote. [5]
The defining diagnostic pitfalls are the misattributions. Treating tinea capitis as alopecia areata with a topical steroid causes tinea incognito and allows the fungus to spread. Incising a kerion as a bacterial abscess delays healing and scars the scalp. Attributing telogen effluvium to alopecia areata leads to needless immunosuppression. Missing the behavioural driver of trichotillomania leaves the root cause untouched. And over-using systemic immunosuppression or off-label JAK inhibition without specialist oversight exposes a child to harm for a condition that may have regrown on its own. [12]
The iatrogenic pitfalls are real too. Skin atrophy can follow over-use of a potent topical or intralesional corticosteroid, especially on the face, so concentrations and volumes are kept low and courses are limited. Oral minoxidil can cause hypertrichosis and, at higher doses, cardiovascular effects, so it is used in low doses under specialist guidance. These are the reasons that treatment is stepped and supervised rather than maximal from the outset. [6] [1]
Prognosis & Disposition
Limited patchy alopecia areata has a good prognosis, with spontaneous or treatment-assisted regrowth in many children, and the follicle is preserved so regrowth remains possible. The prognosis worsens with the ophiasis, totalis and universalis patterns and with the features of atopy, early onset, nail involvement, long duration and extensive disease, and relapse is common enough to set honest expectations early. [4]
Acute telogen effluvium is self-limiting and resolves once the trigger is removed or the iron and thyroid disturbance is corrected. Trichotillomania often waxes and wanes and responds to behavioural therapy over months. Traction alopecia is reversible in its early phase but becomes permanent if the hairstyle continues, which is why loosening it early is the whole of the treatment. [8] [10]
Disposition follows severity and complexity. Manage limited patchy alopecia areata, acute telogen effluvium and early traction alopecia in primary care or general paediatrics, with thyroid and iron screening as appropriate. Refer to dermatology for extensive or refractory alopecia areata, suspected scarring alopecia, paediatric androgenetic alopecia, severe trichotillomania, and any case needing systemic therapy, oral minoxidil or a JAK inhibitor. Refer to mental-health services for the child whose hair loss carries a heavy psychological load. [1] [5]
Special Populations
The autoimmune association is the single most important special-population point. Children with alopecia areata should be screened for autoimmune thyroid disease, with thyroid function tests and, where clinically indicated, thyroid antibodies, and the increased prevalence in Down syndrome and the association with vitiligo and type 1 diabetes should be kept in mind when the history is taken. [4]
In the adolescent, new androgenetic-pattern thinning after puberty is recognised, but pattern loss before puberty, or an atypical or rapidly progressive pattern, should prompt consideration of an endocrine cause before cosmetic treatment is offered. Hair-loss consultations are sensitive for teenagers, and the consultation should make space for embarrassment, privacy and the option of camouflage or a wig. [11]
The psychosocial dimension applies to every child and family. Visible hair loss carries stigma at school, and the burden is greater for children facing access barriers or cultural pressures around hair. Build camouflage, support organisations and low-threshold follow-up into the plan, give culturally safe advice around hairstyles for children at risk of traction alopecia, and ensure migrant, refugee and Indigenous families can complete treatment and review without transport, cost or language becoming the reason a curable condition is left untreated. [5]
Evidence, Guidelines & Regional Differences
The major guidance is concordant across regions. The British Association of Dermatologists living guideline for managing people with alopecia areata sets the standard: topical and intralesional corticosteroid, topical minoxidil and topical immunotherapy as first-line, with systemic therapy including JAK inhibitors for severe disease. The NICE Clinical Knowledge Summary on alopecia areata reaches the same conclusions, and Australasian practice aligns with both, with a clear threshold for specialist referral before systemic therapy. [1] [12]
The paediatric evidence base is thinner than the adult one, and that matters for how treatment is chosen. The systematic review of paediatric alopecia areata treatment found limited high-quality paediatric data, with much of practice extrapolated from adults, and the network meta-analysis of alopecia areata treatments confirms that the strongest evidence for newer agents, including the JAK inhibitors, sits in the adult literature. The practical consequence is a stepped approach in which first-line topical therapy is well supported and systemic therapy is specialist-led. [2] [3]
The active controversies are the role of oral minoxidil, whose benefits and risks have been summarised in recent recommendations, and the place of JAK inhibitors such as baricitinib, now licensed for adults and being explored in adolescents. For trichotillomania, the Cochrane review of pharmacotherapy found only modest evidence, which is why habit-reversal and cognitive behavioural therapy remain first-line. These are also the strongest arguments for involving a specialist before committing a child to systemic or off-label treatment. [6] [7] [9]
JAK inhibitors for alopecia areata and the emerging adolescent evidence
Phase three randomised trials in adults (for example baricitinib) and systematic reviews of paediatric treatment
Practice change
Use first-line topical therapy confidently; reserve JAK inhibitors and oral minoxidil for severe disease under specialist dermatology guidance
Exam Pearls
The exclamation-mark hair, a short broken hair narrower at the scalp than at the tip, is pathognomonic for alopecia areata, and the presence of scale, broken stubs and lymphadenopathy redirects the diagnosis to tinea capitis. [1] [12]
Alopecia areata is non-scarring, so regrowth is possible; the hair pull test is positive in active telogen effluvium; and hairs of wildly varying lengths on a normal scalp signal trichotillomania rather than alopecia areata. [10] [8]
HABIT
Autoimmune thyroid disease is the most common association of alopecia areata, the condition is more common in Down syndrome, and habit-reversal and cognitive behavioural therapy rather than drugs are first-line for trichotillomania. [4] [9]
References
- [1]Harries MJ, Ascott A, Asfour L, et al. British Association of Dermatologists living guideline for managing people with alopecia areata 2024. Br J Dermatol, 2025.PMID 39432739
- [2]Barton VR, Toussi A, Awasthi S, et al. Treatment of pediatric alopecia areata: A systematic review. J Am Acad Dermatol, 2022.PMID 33940103
- [3]Westerkam LL, McShane DB, Nieman EL, et al. Treatment Options for Alopecia Areata in Children and Adolescents. Paediatr Drugs, 2024.PMID 38466519
- [4]Lee HH, Gwillim E, Patel KR, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: A systematic review and meta-analysis. J Am Acad Dermatol, 2020.PMID 31437543
- [5]Toussi A, Barton VR, Le ST, et al. Psychosocial and psychiatric comorbidities and health-related quality of life in alopecia areata: A systematic review. J Am Acad Dermatol, 2021.PMID 32561373
- [6]Ong MM, Li Y, Lipner SR Oral Minoxidil for Alopecia Treatment: Risks, Benefits, and Recommendations. Am J Clin Dermatol, 2026.PMID 41118052
- [7]Dahabreh D, Jung S, Renert-Yuval Y, et al. Alopecia Areata: Current Treatments and New Directions. Am J Clin Dermatol, 2023.PMID 37606849
- [8]Harrison JP, Franklin ME Pediatric trichotillomania. Curr Psychiatry Rep, 2012.PMID 22437627
- [9]Hoffman J, Williams T, Rothbart R Pharmacotherapy for trichotillomania. Cochrane Database Syst Rev, 2021.PMID 34582562
- [10]Asghar F, Shamim N, Farooque U, et al. Telogen Effluvium: A Review of the Literature. Cureus, 2020.PMID 32607303
- [11]Griggs J, Burroway B, Tosti A Pediatric androgenetic alopecia: A review. J Am Acad Dermatol, 2021.PMID 31415838
- [12]Dakkak M, Forde KM, Lanney H Hair Loss: Diagnosis and Treatment. Am Fam Physician, 2024.PMID 39283847